
Are Posterior Oropharyngeal Saliva Specimens an Acceptable Alternative to Nasopharyngeal Sampling for the Monitoring of SARS-CoV-2 in Primary-Care Settings?

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
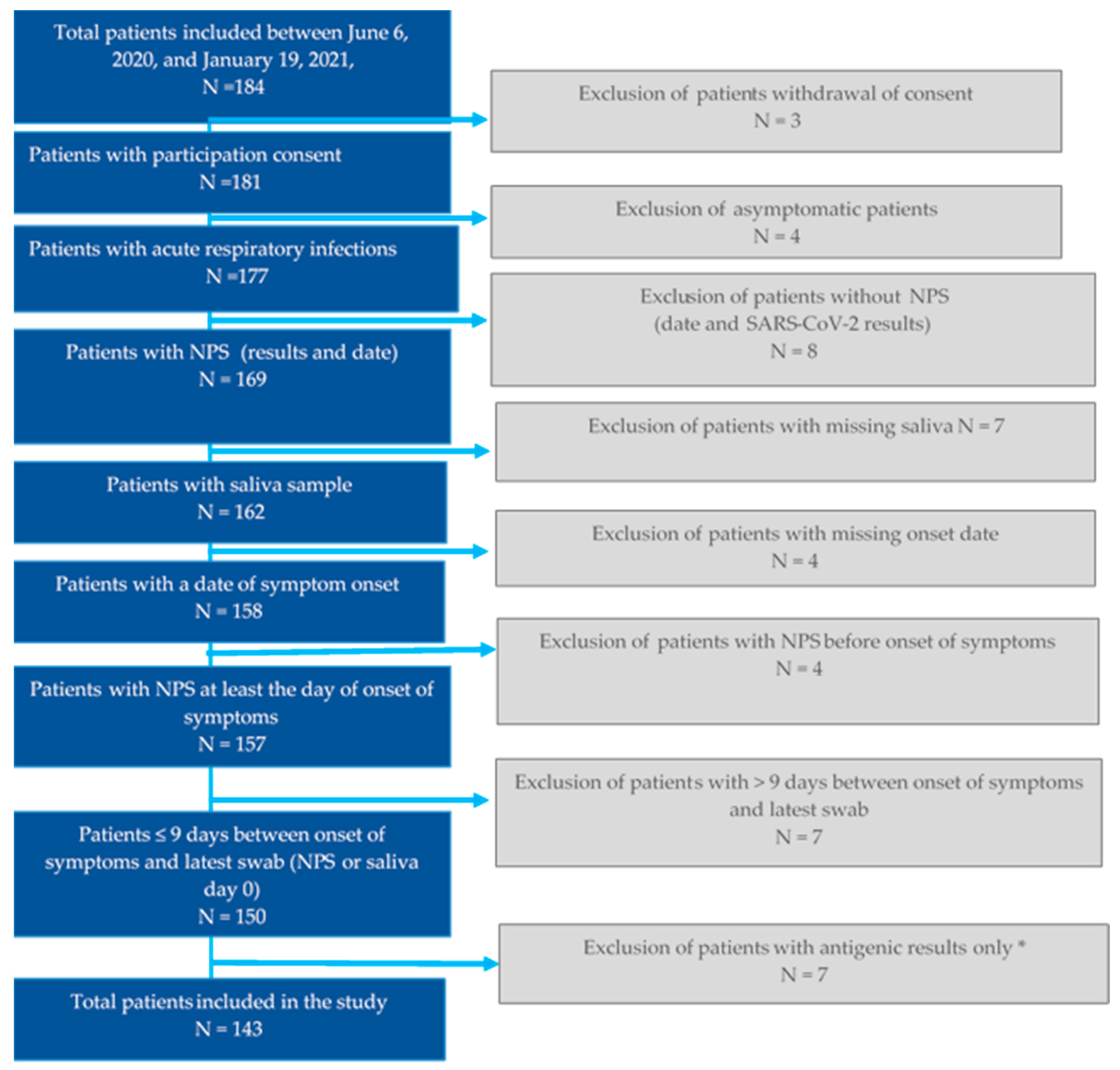
2.1. Study Design
2.2. Outcome
2.3. SARS-CoV-2 RNA Detection in Saliva Samples
2.4. Statistical Analysis
2.5. Ethics Approval
3. Results
3.1. Patient Characteristics
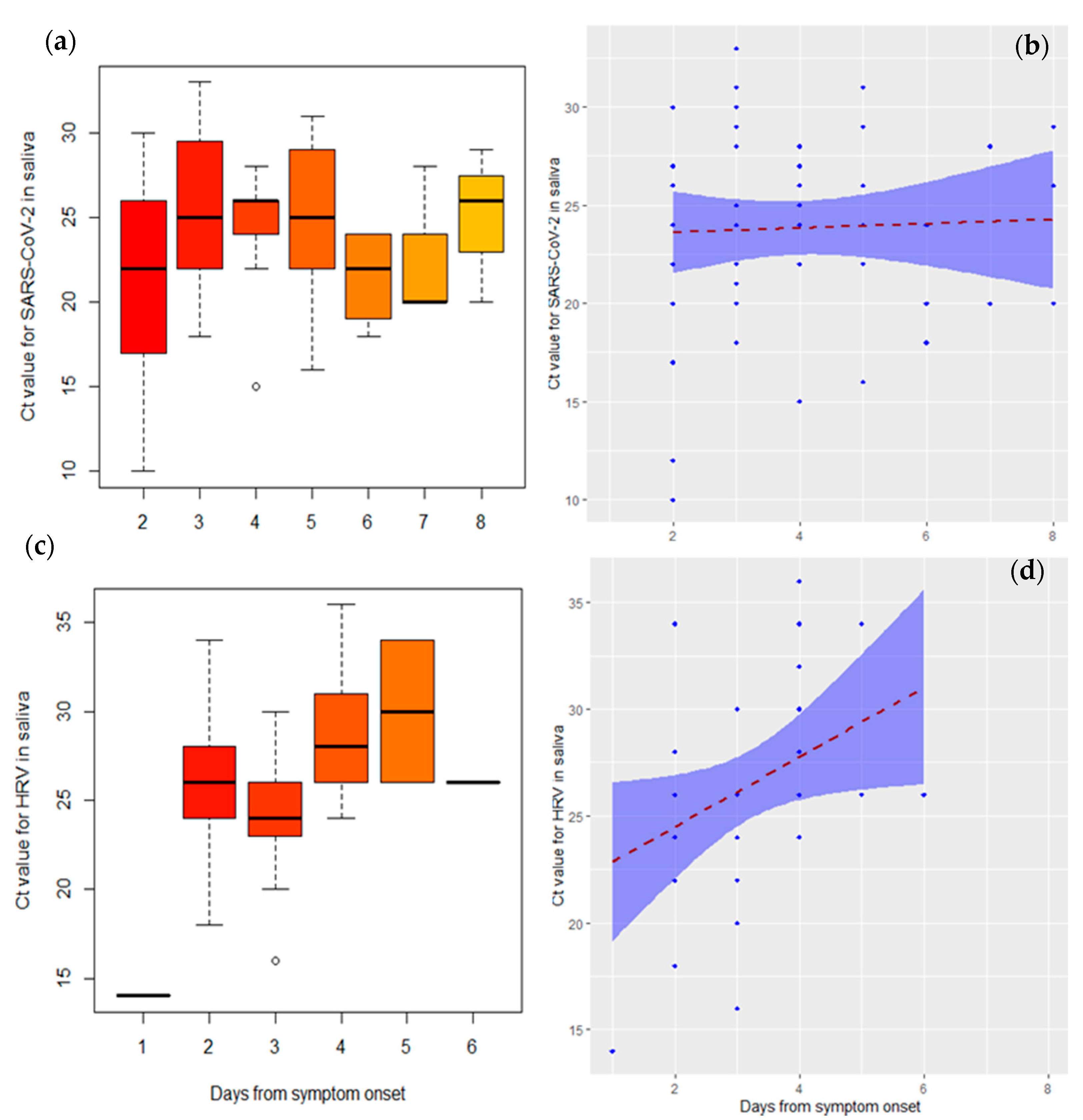
3.2. Virological Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Food and Drug Administration. FAQs on Testing for SARS-CoV-2. Available online: https://www.fda.gov/medical-devices/coronavirus-covid-19-and-medical-devices/faqs-testing-sars-cov-2 (accessed on 12 October 2020).
- Centers for Disease Control and Prevention. Information for Laboratories about Coronavirus (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/guidelines-clinical-specimens.html (accessed on 4 October 2020).
- Souty, C.; Masse, S.; Valette, M.; Behillil, S.; Bonmarin, I.; Pino, C.; Turbelin, C.; Capai, L.; Vilcu, A.M.; Lina, B.; et al. Baseline characteristics and clinical symptoms related to respiratory viruses identified among patients presenting with influenza-like illness in primary care. Clin. Microbiol. Infect. 2019, 25, 1147–1153. [Google Scholar] [CrossRef] [Green Version]
- Becker, D.; Sandoval, E.; Amin, A.; De Hoff, P.; Diets, A.; Leonetti, N.; Lim, Y.; Elliott, C.; Laurent, L.; Grzymski, J.; et al. Saliva is less sensitive than nasopharyngeal swabs for COVID-19 detection in the community setting. medRxiv 2020. [Google Scholar] [CrossRef]
- To, K.K.; Tsang, O.T.; Leung, W.S.; Tam, A.R.; Wu, T.C.; Lung, D.C.; Yip, C.C.; Cai, J.P.; Chan, J.M.; Chik, T.S.; et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: An observational cohort study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Sahajpal, N.S.; Mondal, A.K.; Njau, A.; Ananth, S.; Ghamande, S.; Hegde, M.; Chaubey, A.; Rojiani, A.M.; Kolhe, R. COVID-19 screening in a healthcare or community setting: Complexity of saliva as a specimen for PCR-based testing. Future Med. Chem. 2021, 13, 9–12. [Google Scholar] [CrossRef]
- Lee, R.A.; Herigon, J.C.; Benedetti, A.; Pollock, N.R.; Denkinger, C.M. Performance of Saliva, Oropharyngeal Swabs, and Nasal Swabs for SARS-CoV-2 Molecular Detection: A Systematic Review and Meta-analysis. J. Clin. Microbiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Flahault, A.; Blanchon, T.; Dorleans, Y.; Toubiana, L.; Vibert, J.F.; Valleron, A.J. Virtual surveillance of communicable diseases: A 20-year experience in France. Stat. Methods Med. Res. 2006, 15, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Procop, G.W.; Shrestha, N.K.; Vogel, S.; Van Sickle, K.; Harrington, S.; Rhoads, D.D.; Rubin, B.P.; Terpeluk, P. A Direct Comparison of Enhanced Saliva to Nasopharyngeal Swab for the Detection of SARS-CoV-2 in Symptomatic Patients. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [PubMed]
- Jamal, A.J.; Mozafarihashjin, M.; Coomes, E.; Powis, J.; Li, A.X.; Paterson, A.; Anceva-Sami, S.; Barati, S.; Crowl, G.; Faheem, A.; et al. Sensitivity of nasopharyngeal swabs and saliva for the detection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Cevik, M.; Tate, M.; Lloyd, O.; Maraolo, A.E.; Schafers, J.; Ho, A. SARS-CoV-2, SARS-CoV, and MERS-CoV viral load dynamics, duration of viral shedding, and infectiousness: A systematic review and meta-analysis. Lancet Microbe 2021, 2, e13–e22. [Google Scholar] [CrossRef]
- Miller, T.E.; Garcia Beltran, W.F.; Bard, A.Z.; Gogakos, T.; Anahtar, M.N.; Astudillo, M.G.; Yang, D.; Thierauf, J.; Fisch, A.S.; Mahowald, G.K.; et al. Clinical sensitivity and interpretation of PCR and serological COVID-19 diagnostics for patients presenting to the hospital. FASEB J. 2020, 34, 13877–13884. [Google Scholar] [CrossRef]
- Matsumura, Y.; Shimizu, T.; Noguchi, T.; Nakano, S.; Yamamoto, M.; Nagao, M. Comparison of 12 Molecular Detection Assays for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). J. Mol. Diagn. 2021, 23, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Pezzi, L.; Charrel, R.N.; Ninove, L.; Nougairede, A.; Molle, G.; Coutard, B.; Durand, G.; Leparc-Goffart, I.; de Lamballerie, X.; Thirion, L. Development and Evaluation of a duo SARS-CoV-2 RT-qPCR Assay Combining Two Assays Approved by the World Health Organization Targeting the Envelope and the RNA-Dependant RNA Polymerase (RdRp) Coding Regions. Viruses 2020, 12, 686. [Google Scholar] [CrossRef]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar] [PubMed]
- RDocumentation. ggplot2. Available online: https://rdocumentation.org/packages/ggplot2/versions/3.3.3 (accessed on 2 February 2020).
- Chambers, J.M.; Hastie, T.J. (Eds.) Linear Models, Chapter 4 of Statistical Models; Wadsworth & Brooks/Cole.: Pacific Grove, CA, USA, 1992. [Google Scholar]
- Butler-Laporte, G.; Lawandi, A.; Schiller, I.; Yao, M.; Dendukuri, N.; McDonald, E.G.; Lee, T.C. Comparison of Saliva and Nasopharyngeal Swab Nucleic Acid Amplification Testing for Detection of SARS-CoV-2: A Systematic Review and Meta-analysis. JAMA Intern Med. 2021, 181, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Hung, D.L.; Li, X.; Chiu, K.H.; Yip, C.C.; To, K.K.; Chan, J.F.; Sridhar, S.; Chung, T.W.; Lung, K.C.; Liu, R.W.; et al. Early-Morning vs Spot Posterior Oropharyngeal Saliva for Diagnosis of SARS-CoV-2 Infection: Implication of Timing of Specimen Collection for Community-Wide Screening. Open Forum Infect. Dis. 2020, 7, ofaa210. [Google Scholar] [CrossRef]
- Bonneton, M.; Antona, D.; Danis, K.; Ait-Belghiti, F.; Levy-Bruhl, D. Are vaccinated measles cases protected against severe disease? Vaccine 2020. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.; Cui, B.; Duan, X.; Zhang, P.; Zhou, X.; Yuan, Q. Saliva: Potential diagnostic value and transmission of 2019-nCoV. Int. J. Oral Sci. 2020, 12, 11. [Google Scholar] [CrossRef]
- Moreira, V.M.; Mascarenhas, P.; Machado, V.; Botelho, J.; Mendes, J.J.; Taveira, N.; Almeida, M.G. Diagnosis of SARS-Cov-2 Infection by RT-PCR Using Specimens Other Than Naso- and Oropharyngeal Swabs: A Systematic Review and Meta-Analysis. Diagnostics 2021, 11, 363. [Google Scholar] [CrossRef]
- Khiabani, K.; Amirzade-Iranaq, M.H. Are saliva and deep throat sputum as reliable as common respiratory specimens for SARS-CoV-2 detection? A systematic review and meta-analysis. Am. J. Infect. Control 2021. [Google Scholar] [CrossRef] [PubMed]
- Owusu, D.; Pomeroy, M.A.; Lewis, N.M.; Wadhwa, A.; Yousaf, A.R.; Whitaker, B.; Dietrich, E.; Hall, A.J.; Chu, V.; Thornburg, N.; et al. Persistent SARS-CoV-2 RNA Shedding without Evidence of Infectiousness: A Cohort Study of Individuals with COVID-19. J. Infect. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.; Lu, L.; Yip, C.C.; Poon, R.W.; Fung, A.M.; Cheng, A.; Lui, D.H.; Ho, D.T.; Hung, I.F.; Chan, K.H.; et al. Additional molecular testing of saliva specimens improves the detection of respiratory viruses. Emerg. Microbes Infect. 2017, 6, e49. [Google Scholar] [CrossRef] [Green Version]
- To, K.K.W.; Yip, C.C.Y.; Lai, C.Y.W.; Wong, C.K.H.; Ho, D.T.Y.; Pang, P.K.P.; Ng, A.C.K.; Leung, K.H.; Poon, R.W.S.; Chan, K.H.; et al. Saliva as a diagnostic specimen for testing respiratory virus by a point-of-care molecular assay: A diagnostic validity study. Clin. Microbiol. Infect. 2019, 25, 372–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boschi, C.; Hoang, V.T.; Giraud-Gatineau, A.; Ninove, L.; Lagier, J.C.; La Scola, B.; Gautret, P.; Raoult, D.; Colson, P. Coinfections with SARS-CoV-2 and other respiratory viruses in Southeastern France: A matter of sampling time. J. Med. Virol. 2021, 93, 1878–1881. [Google Scholar] [CrossRef]
- Hazra, A.; Collison, M.; Pisano, J.; Kumar, M.; Oehler, C.; Ridgway, J.P. Coinfections with SARS-CoV-2 and other respiratory pathogens. Infect Control Hosp. Epidemiol. 2020, 41, 1228–1229. [Google Scholar] [CrossRef]
- Kim, K.W.; Deveson, I.W.; Pang, C.N.I.; Yeang, M.; Naing, Z.; Adikari, T.; Hammond, J.M.; Stevanovski, I.; Beukers, A.G.; Verich, A.; et al. Respiratory viral co-infections among SARS-CoV-2 cases confirmed by virome capture sequencing. Sci. Rep. 2021, 11, 3934. [Google Scholar] [CrossRef] [PubMed]
- Kissling, E.; Hooiveld, M.; Brytting, M.; Vilcu, A.M.; de Lange, M.; Martinez-Baz, I.; Sigerson, D.; Enkirch, T.; Belhillil, S.; Meijer, A.; et al. Absence of association between 2019-20 influenza vaccination and COVID-19: Results of the European I-MOVE-COVID-19 primary care project, March-August 2020. Influenza Other Respir Viruses 2021. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | N = 143 |
|---|---|
| Sex (n; %) | |
| Female | 80 (56.0%) |
| Age (mean), years | 35.8 (8–74) |
| Age (median), years | 35 (22.5–49) |
| Age group (years) | |
| [8,15) | 20 (14.0%) |
| [15,35) | 51 (36.0%) |
| [35,45) | 26 (18.0%) |
| [45,55) | 24 (17.0%) |
| [55,65) | 15 (10.0%) |
| ≥65 | 7 (4.9%) |
| At least one chronic condition (n; %) | |
| Yes | 30 (21.0%) |
| Missing | 1 (0.7%) |
| Obesity (n; %) | |
| Yes | 21 (15.0%) |
| Missing | 3 (2.1%) |
| Smoking (n; %) | |
| Yes | 30 (21.0%) |
| Missing | 3 (2.1%) |
| Pregnancy (n; %) | |
| Yes | 1 (0.7%) |
| Missing | 5 (3.3%) |
| Health professional (n; %) | |
| Yes | 16 (11.0%) |
| Missing | 3 (2.1%) |
| Collection month (n; %) | |
| June | 8 (5.6%) |
| July | 4 (2.8%) |
| August | 1 (0.7%) |
| September | 25 (17.5%) |
| October | 46 (32.2%) |
| November | 44 (30.8%) |
| December | 8 (5.6%) |
| January | 7 (4.9%) |
| Days between onset of symptoms and saliva sampling (n; %) | |
| 1 | 6 (4.2%) |
| 2 | 38 (27.0%) |
| 3–4 | 71 (49.6%) |
| 5–6 | 17 (11.8%) |
| 7–8 | 11(7.7%) |
| Mean | 2.4 (0–7) |
| Median | 2 (1–3) |
| Days between onset of symptoms and NPS (n; %) | |
| 1 | 11 (7.7%) |
| 2 | 25 (17.0%) |
| 3–4 | 77 (53.8%) |
| 5–6 | 20 (13.9%) |
| 7–9 | 10 (7.0%) |
| Mean | 2.5 (0–8) |
| Median | 2 (1.5–3) |
| Days between collection of NPS and saliva sampling (n; %) | |
| From –5 to –1 | 31 (21.7%) |
| 0 | 56 (39.0%) |
| 1 | 44 (31.0%) |
| 2 | 11 (7.7%) |
| 3 | 1 (0.7%) |
| Median | 0 (0–3) |
| Virological Results | N = 143 |
|---|---|
| Detection in NPS | |
| SARS-CoV-2 | 56 (39.0%) |
| Detection in saliva sample | |
| Positive for at least one respiratory virus | 90 (63.0%) |
| SARS-CoV-2 | 53 (37.0%) |
| Positive for at least one respiratory virus other than SARS-CoV-2 | 40 (28.0%) |
| HRV | 36 (25.0%) |
| Human coronavirus HKU1 | 4 (2.8%) |
| Human parainfluenza 1 | 1 (0.7%) |
| Coinfection | 4 (2.8%) |
| HRV, human coronavirus HKU1 | 1 (0.7%) |
| SARS-CoV-2, human coronavirus HKU1 | 1 (0.7%) |
| SARS-CoV-2, human parainfluenza type 1 | 1 (0.7%) |
| SARS-CoV-2, HRV | 1 (0.7%) |
| NPS | Total | |||
|---|---|---|---|---|
| Positive | Negative | |||
| Saliva sample | Positive | 51 (96.2%) | 2 (3.8%) | 53 (100%) |
| Negative | 5 (5.6%) | 85 (94.4%) | 90 (100%) | |
| Total | 56 (39.2%) | 87 (60.8%) | 143 (100%) | |
| Cohen’s Kappa coefficient = 0.89, 95% confidence interval 0.82–0.97,p < 0.001 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masse, S.; Bonnet, C.; Vilcu, A.-M.; Benamar, H.; Swital, M.; van der Werf, S.; Carrat, F.; Hanslik, T.; Blanchon, T.; Falchi, A. Are Posterior Oropharyngeal Saliva Specimens an Acceptable Alternative to Nasopharyngeal Sampling for the Monitoring of SARS-CoV-2 in Primary-Care Settings? Viruses 2021, 13, 761. https://doi.org/10.3390/v13050761
Masse S, Bonnet C, Vilcu A-M, Benamar H, Swital M, van der Werf S, Carrat F, Hanslik T, Blanchon T, Falchi A. Are Posterior Oropharyngeal Saliva Specimens an Acceptable Alternative to Nasopharyngeal Sampling for the Monitoring of SARS-CoV-2 in Primary-Care Settings? Viruses. 2021; 13(5):761. https://doi.org/10.3390/v13050761
Chicago/Turabian StyleMasse, Shirley, Camille Bonnet, Ana-Maria Vilcu, Hayat Benamar, Morgane Swital, Sylvie van der Werf, Fabrice Carrat, Thomas Hanslik, Thierry Blanchon, and Alessandra Falchi. 2021. "Are Posterior Oropharyngeal Saliva Specimens an Acceptable Alternative to Nasopharyngeal Sampling for the Monitoring of SARS-CoV-2 in Primary-Care Settings?" Viruses 13, no. 5: 761. https://doi.org/10.3390/v13050761