

Assessing the Impact of Use and Trust in Different Sources of Information on COVID-19 Vaccination Uptake in Saudi Arabia (SA) Using the COVID-19 Vaccine Hesitancy and Resistance in SA (CoV-HERSA) Tool

Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodological Approach
2.2. Piloting the Questionnaire
2.3. Data Management
2.4. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Personal Medical Experience with COVID-19
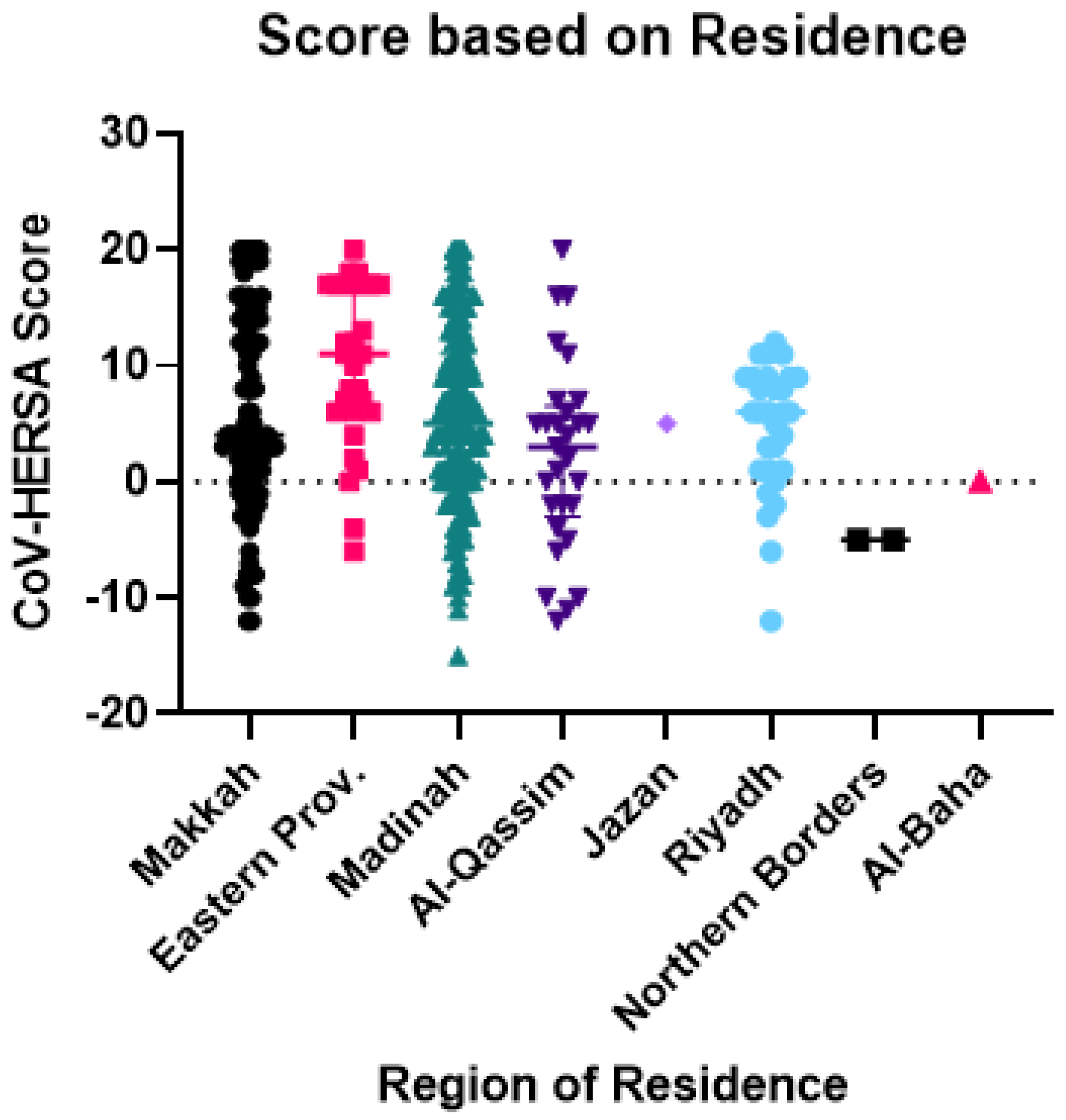
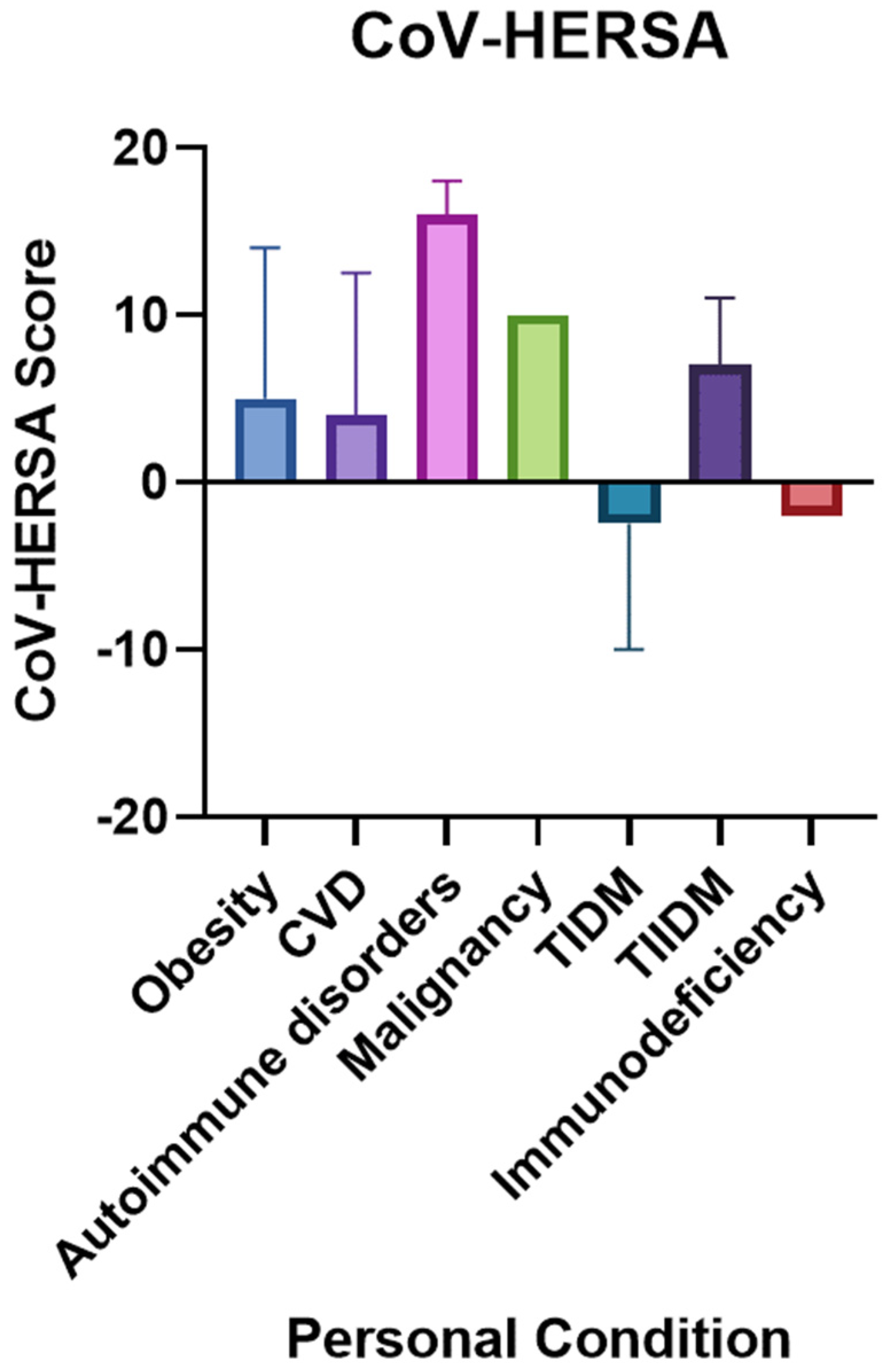
3.3. The Impact of Participants’ Characteristics and Experience with COVID-19 on Their CoV-HERSA Scores
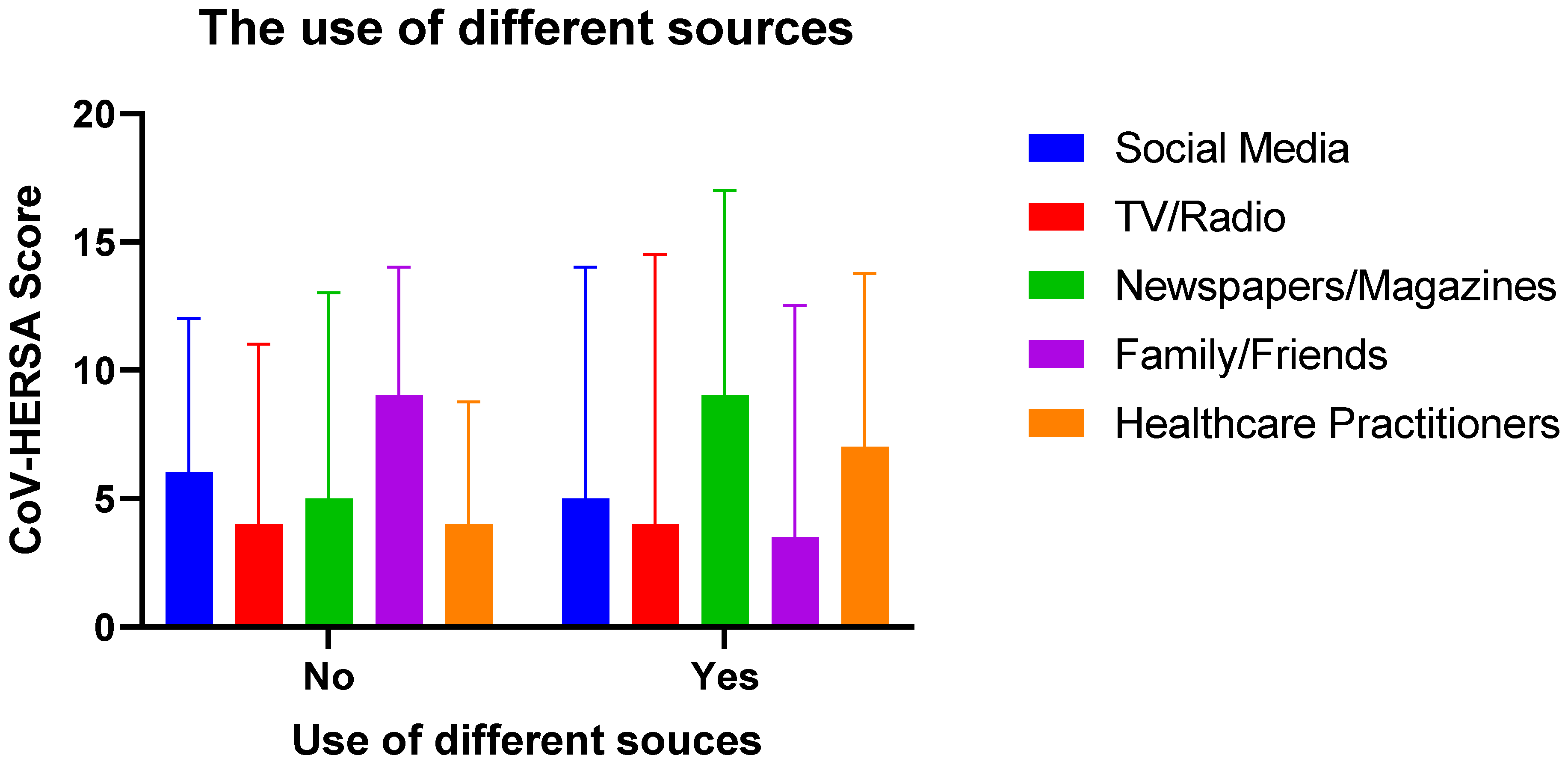
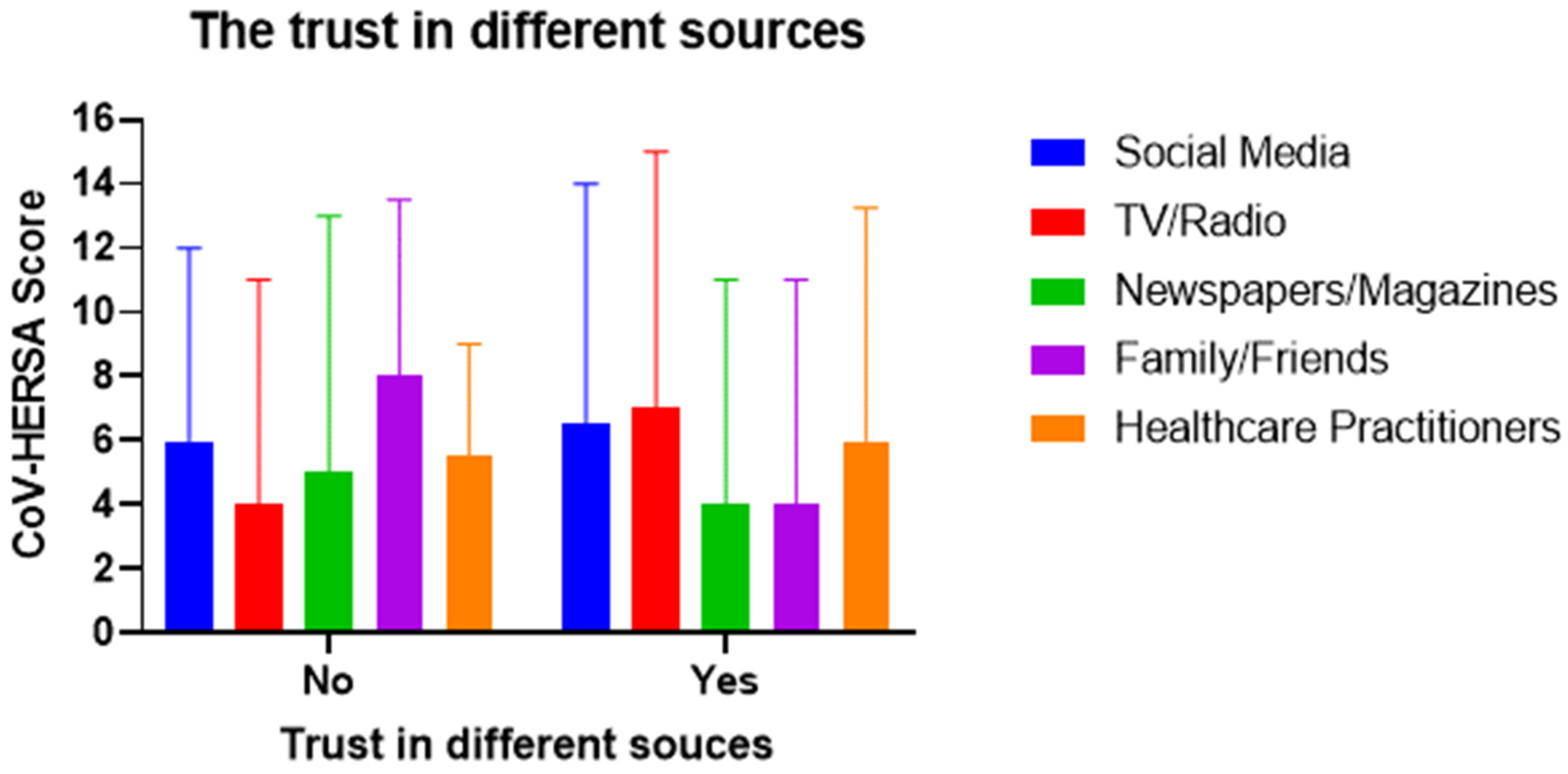
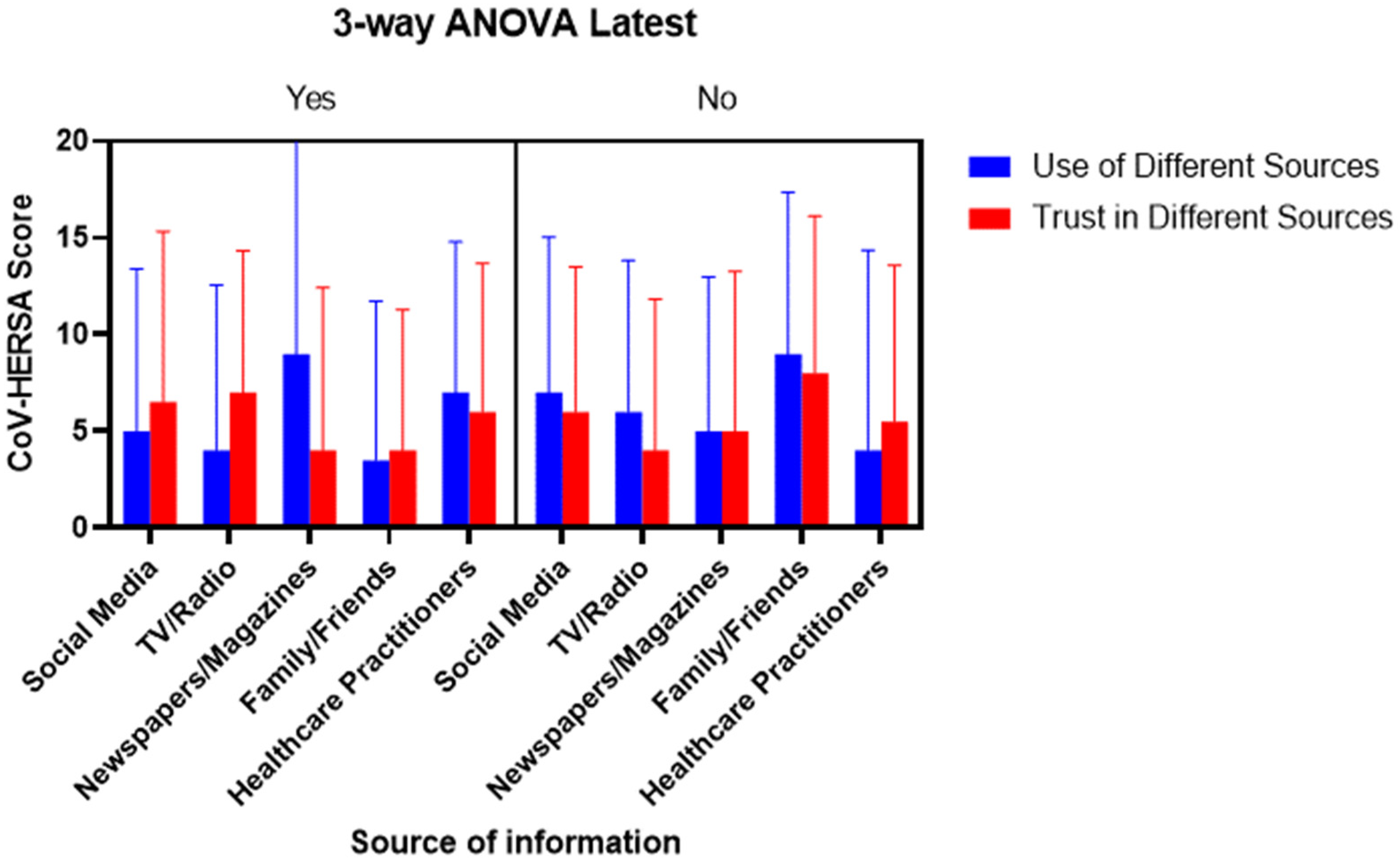
3.4. The Impact of the Use and Trust in Different Sources of Information on Participants’ CoV-HERSA Scores
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | Answer | Assigned Score |
|---|---|---|
| To what extent do you agree with the following statements: | ||
| (1) COVID-19 vaccine has been tested properly before its wide use in the vaccination program. | Strongly Disagree Disagree I Do Not Know Agree Strongly Agree | −2 −1 0 1 2 |
| (2) COVID-19 vaccine is safe to use. | Strongly Disagree Disagree I Do Not Know Agree Strongly Agree | −2 −1 0 1 2 |
| (3) I believe that COVID-19 vaccine will protect me from getting infected. | Strongly Disagree Disagree I Do Not Know Agree Strongly Agree | −2 −1 0 1 2 |
| (4) I believe that COVID-19 vaccine will protect me from having a severe COVID-19 infection. | Strongly Disagree Disagree I Do Not Know Agree Strongly Agree | −2 −1 0 1 2 |
| (5) I recommend my family/friends to get vaccinated with COVID-19 vaccine. | Strongly Disagree Disagree I Do Not Know Agree Strongly Agree | −2 −1 0 1 2 |
| (6) I believe that COVID-19 Vaccine is unsafe because it will alter/change my DNA. | Strongly Disagree Disagree I Do Not Know Agree Strongly Agree | 2 1 0 −1 −2 |
| (7) I believe that COVID-19 Vaccine is unsafe because it will prevent me/one of my family members/friends from becoming pregnant. | Strongly Disagree Disagree I Do Not Know Agree Strongly Agree | 2 1 0 −1 −2 |
| (8) I believe that COVID-19 Vaccine is unsafe because we do not know its long-term side-effects. | Strongly Disagree Disagree I Do Not Know Agree Strongly Agree | 2 1 0 −1 −2 |
| (9) I do not need to get vaccinated as long as I am wearing a face mask and maintaining social distancing. | Strongly Disagree Disagree I Do Not Know Agree Strongly Agree | 2 1 0 −1 −2 |
| (10) I will only get vaccinated if it becomes mandatory, e.g., for Umrah or travelling. | Strongly Disagree Disagree I Do Not Know Agree Strongly Agree | 2 1 0 −1 −2 |
References
- Sayed, A.A.; Allam, A.A.; Sayed, A.I.; Alraey, M.A.; Joseph, M.V. The use of neutrophil-to-lymphocyte ratio (NLR) as a marker for COVID-19 infection in Saudi Arabia. Saudi Med. J. 2021, 42, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Sayed, A.A. The Cost-Effectiveness of Requesting a Complete Blood Count (CBC) in the Management of COVID-19 in Saudi Arabia. Healthcare 2022, 10, 1780. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Sayed, A.A. The Progressive Public Measures of Saudi Arabia to Tackle COVID-19 and Limit Its Spread. Int. J. Environ. Res. Public Health 2021, 18, 783. [Google Scholar] [CrossRef]
- Allam, A.A.; Sayed, A.A. Active COVID-19 infection and transmission after the first dose of the BNT162b2 mRNA vaccination in Saudi Arabia: A case report. J. Infect. Public Health 2021, 14, 1123–1125. [Google Scholar] [CrossRef]
- Lee, S.A. Coronavirus Anxiety Scale: A brief mental health screener for COVID-19 related anxiety. Death Stud. 2020, 44, 393–401. [Google Scholar] [CrossRef] [Green Version]
- Martin, L.R.; Petrie, K.J. Understanding the Dimensions of Anti-Vaccination Attitudes: The Vaccination Attitudes Examination (VAX) Scale. Ann. Behav. Med. 2017, 51, 652–660. [Google Scholar] [CrossRef]
- Zeballos Rivas, D.R.; Lopez Jaldin, M.L.; Nina Canaviri, B.; Portugal Escalante, L.F.; Alanes Fernández, A.M.C.; Aguilar Ticona, J.P. Social media exposure, risk perception, preventive behaviors and attitudes during the COVID-19 epidemic in La Paz, Bolivia: A cross sectional study. PLoS ONE 2021, 16, e0245859. [Google Scholar] [CrossRef]
- Hennessy, C.M.; Smith, C.F.; Greener, S.; Ferns, G. Social media guidelines: A review for health professionals and faculty members. Clin. Teach. 2019, 16, 442–447. [Google Scholar] [CrossRef]
- Al-Mansour, K.; Alyahya, S.; AbuGazalah, F.; Alabdulkareem, K. Factors Affecting COVID-19 Vaccination among the General Population in Saudi Arabia. Healthcare 2021, 9, 1218. [Google Scholar] [CrossRef] [PubMed]
- AL-Mohaithef, M.; Padhi, B.K.; Ennaceur, S. Socio-Demographics Correlate of COVID-19 Vaccine Hesitancy During the Second Wave of COVID-19 Pandemic: A Cross-Sectional Web-Based Survey in Saudi Arabia. Front. Public Health 2021, 9, 698106. [Google Scholar] [CrossRef] [PubMed]
- Yahia, A.I.O.; Alshahrani, A.M.; Alsulmi, W.G.H.; Alqarni, M.M.M.; Abdulrahim, T.K.A.; Heba, W.F.H.; Alqarni, T.A.A.; Alharthi, K.A.Z.; Buhran, A.A.A. Determinants of COVID-19 vaccine acceptance and hesitancy: A cross-sectional study in Saudi Arabia. Hum. Vaccin. Immunother. 2021, 17, 4015–4020. [Google Scholar] [CrossRef] [PubMed]
- Alfageeh, E.I.; Alshareef, N.; Angawi, K.; Alhazmi, F.; Chirwa, G.C. Acceptability of a COVID-19 Vaccine among the Saudi Population. Vaccines 2021, 9, 226. [Google Scholar] [CrossRef]
- Aldakhil, H.; Albedah, N.; Alturaiki, N.; Alajlan, R.; Abusalih, H. Vaccine hesitancy towards childhood immunizations as a predictor of mothers’ intention to vaccinate their children against COVID-19 in Saudi Arabia. J. Infect. Public Health 2021, 14, 1497–1504. [Google Scholar] [CrossRef]
- Qattan, A.M.N.; Alshareef, N.; Alsharqi, O.; Al Rahahleh, N.; Chirwa, G.C.; Al-Hanawi, M.K. Acceptability of a COVID-19 Vaccine among Healthcare Workers in the Kingdom of Saudi Arabia. Front. Med. 2021, 8, 644300. [Google Scholar] [CrossRef]
- Al-Mohaithef, M.; Padhi, B.K. Determinants of COVID-19 vaccine acceptance in saudi arabia: A web-based national survey. J. Multidiscip. Healthc. 2020, 13, 1657–1663. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Alzahrani, S.H.; Baig, M.; Alrabia, M.W.; Algethami, M.R.; Alhamdan, M.M.; Alhakamy, N.A.; Asfour, H.Z.; Ahmad, T. Attitudes toward the SARS-CoV-2 Vaccine: Results from the Saudi Residents’ Intention to Get Vaccinated against COVID-19 (SRIGVAC) Study. Vaccines 2021, 9, 798. [Google Scholar] [CrossRef]
- Dhama, K.; Sharun, K.; Tiwari, R.; Dhawan, M.; Emran, T.B.; Rabaan, A.A.; Alhumaid, S. COVID-19 vaccine hesitancy—Reasons and solutions to achieve a successful global vaccination campaign to tackle the ongoing pandemic. Hum. Vaccin. Immunother. 2021, 17, 3495–3499. [Google Scholar] [CrossRef]
- Voramontri, D.; Klieb, L. Impact of social media on consumer behaviour. Int. J. Inf. Decis. Sci. 2019, 11, 209–233. [Google Scholar] [CrossRef] [Green Version]
- Rajamohan, S.; Bennett, E.; Tedone, D. The hazards and benefits of social media use in adolescents. Nursing 2019, 49, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Sujata, M.; Khor, K.-S.; Ramayah, T.; Teoh, A.P. The role of social media on recycling behaviour. Sustain. Prod. Consum. 2019, 20, 365–374. [Google Scholar] [CrossRef] [Green Version]
- Temsah, M.-H.; Alhuzaimi, A.N.; Aljamaan, F.; Bahkali, F.; Al-Eyadhy, A.; Alrabiaah, A.; Alhaboob, A.; Bashiri, F.A.; Alshaer, A.; Temsah, O.; et al. Parental Attitudes and Hesitancy About COVID-19 vs. Routine Childhood Vaccinations: A National Survey. Front. Public Health 2021, 9, 752323. [Google Scholar] [CrossRef] [PubMed]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccin. Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef] [PubMed]
- Li, H.O.-Y.; Bailey, A.; Huynh, D.; Chan, J. YouTube as a source of information on COVID-19: A pandemic of misinformation? BMJ Glob. Health 2020, 5, e002604. [Google Scholar] [CrossRef] [PubMed]
- Hou, Z.; Tong, Y.; Du, F.; Lu, L.; Zhao, S.; Yu, K.; Piatek, S.J.; Larson, H.J.; Lin, L. Assessing COVID-19 Vaccine Hesitancy, Confidence, and Public Engagement: A Global Social Listening Study. J. Med. Internet Res. 2021, 23, e27632. [Google Scholar] [CrossRef]






| Characteristics | Number (%) |
|---|---|
| Gender | Male = 193 (49.9%) Female = 194 (50.1%) |
| Smoking status | Smoker =324 (83.7%) Non-smoker = 63 (16.3%) |
| Age (years) | 34 (24–43) * |
| Level of education | Middle school 6 (1.6%) High school 85 (22%) Bachelor’s degree 249 (64.3%) Postgraduate degree 47 (12.1%) |
| Region of residence | Madinah 200 (51.7%) Makkah 94 (24.3%) Riyadh 30 (7.8%) Eastern Province 30 (7.8%) Qassim 29 (7.5%) Al-Baha 1 (0.3%) Jazan 1 (0.3%) Northern borders 2 (0.5%) |
| Nature of workplace | Educational establishment (student/staff) 192 (49.6%) Healthcare facility (Physician/nurse) 39 (9.8%) Nonmedical establishment (admin/clerk) 60 (15.5%) Field work (Engineer/technician) 21 (5.4%) Home (Housewife/retiree/jobseeker) 76 (19.6%) |
| Characteristics | Number (%) |
|---|---|
| Personal Medical History | Type I Diabetes 16 (4.1%) Type II Diabetes 15 (3.9%) Cardiovascular diseases 37 (9.6%) Immunodeficiency disorders 2 (0.5%) Autoimmune disorders 6 (1.6%) Malignancy 3 (0.8%) Obesity 74 (19.1%) Healthy 275 (71.1%) |
| Immediate Family/Friends’ Medical History | Type I Diabetes 157 (40.6%) Type II Diabetes 116 (30%) Cardiovascular diseases 163 (42.1%) Immunodeficiency disorders 9 (2.3%) Autoimmune disorders 46 (11.9%) Malignancy 46 (11.9%) Obesity 127 (32.8%) Healthy 96 (24.8%) |
| Pregnancy | 6 (3.1%) |
| Pregnant Immediate Family/Friends | Yes = 130 (33.6%) No = 257 (66.4%) |
| Previous Vaccination (Hep B/Influenza) | Yes = 244 (63%) No = 143 (37%) |
| Characteristics | Number (%) |
|---|---|
| Diagnosed with COVID-19 via a PCR test | Yes 42 (10.9%) No 345 (89.1%) |
| Immediate family/friends diagnosed with COVID-19 via a PCR test | Yes 295 (76.2%) No 92 (23.8%) |
| Hospital admission due to COVID-19 | Yes 2 (4.8%) No 40 (95.2) |
| Hospital admission of immediate family/friends due to COVID-19 | Yes 91 (30.8%) No 204 (69.2%) |
| Death of immediate family/friends due to COVID-19 | Yes 120 (40.7%) No 175 (59.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sayed, A.A. Assessing the Impact of Use and Trust in Different Sources of Information on COVID-19 Vaccination Uptake in Saudi Arabia (SA) Using the COVID-19 Vaccine Hesitancy and Resistance in SA (CoV-HERSA) Tool. Trop. Med. Infect. Dis. 2022, 7, 375. https://doi.org/10.3390/tropicalmed7110375
Sayed AA. Assessing the Impact of Use and Trust in Different Sources of Information on COVID-19 Vaccination Uptake in Saudi Arabia (SA) Using the COVID-19 Vaccine Hesitancy and Resistance in SA (CoV-HERSA) Tool. Tropical Medicine and Infectious Disease. 2022; 7(11):375. https://doi.org/10.3390/tropicalmed7110375
Chicago/Turabian StyleSayed, Anwar A. 2022. "Assessing the Impact of Use and Trust in Different Sources of Information on COVID-19 Vaccination Uptake in Saudi Arabia (SA) Using the COVID-19 Vaccine Hesitancy and Resistance in SA (CoV-HERSA) Tool" Tropical Medicine and Infectious Disease 7, no. 11: 375. https://doi.org/10.3390/tropicalmed7110375