

Dengue Incidence and Aedes Vector Collections in Relation to COVID-19 Population Mobility Restrictions

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Diagnosis and Reporting of Dengue in Sri Lanka
2.2. Data on Dengue Incidence and Rainfall
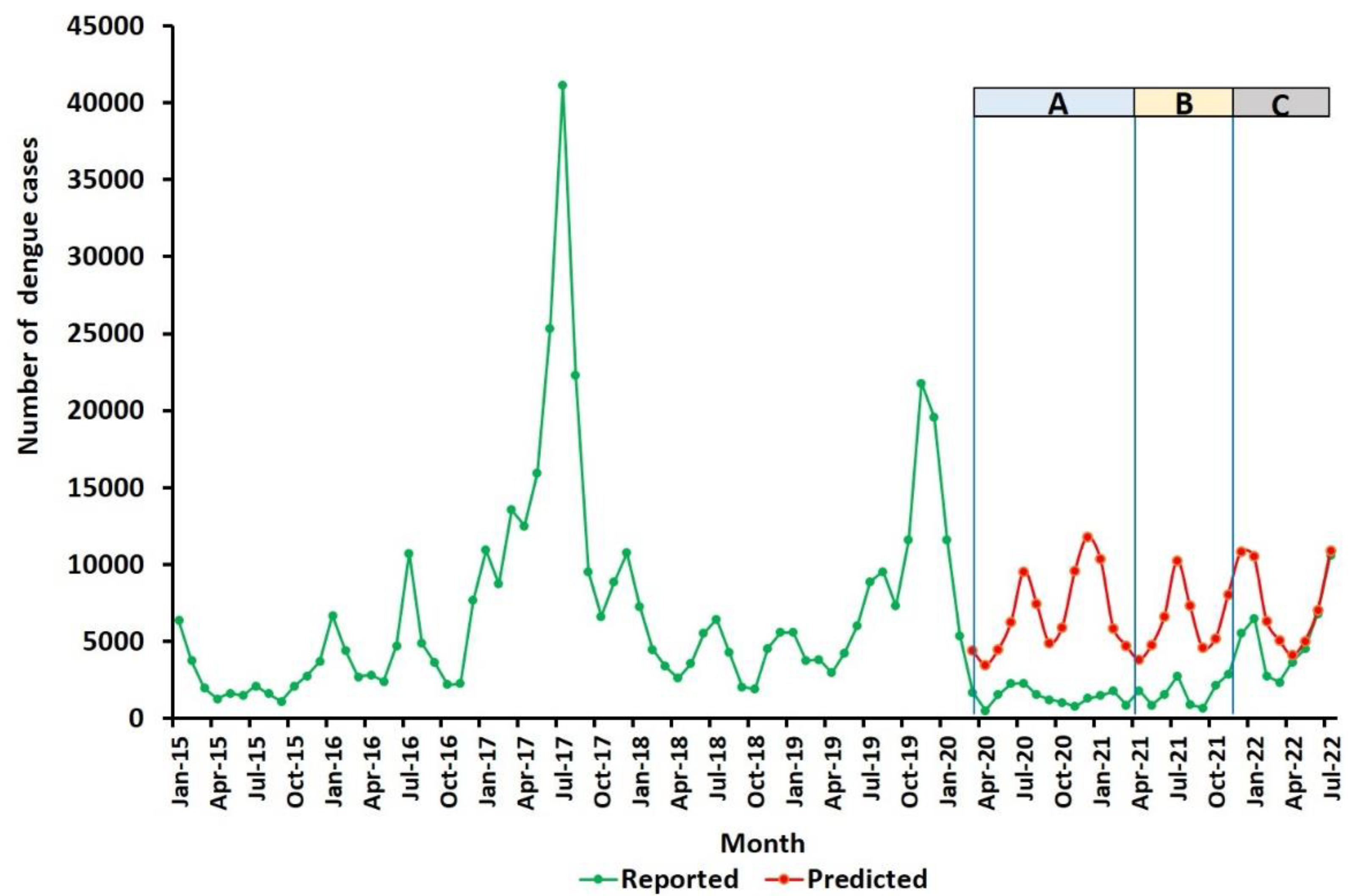
2.3. Prediction from Pre-Pandemic Data of the Expected Number of Monthly Dengue Cases from 1 May 2021 to 31 July 2022
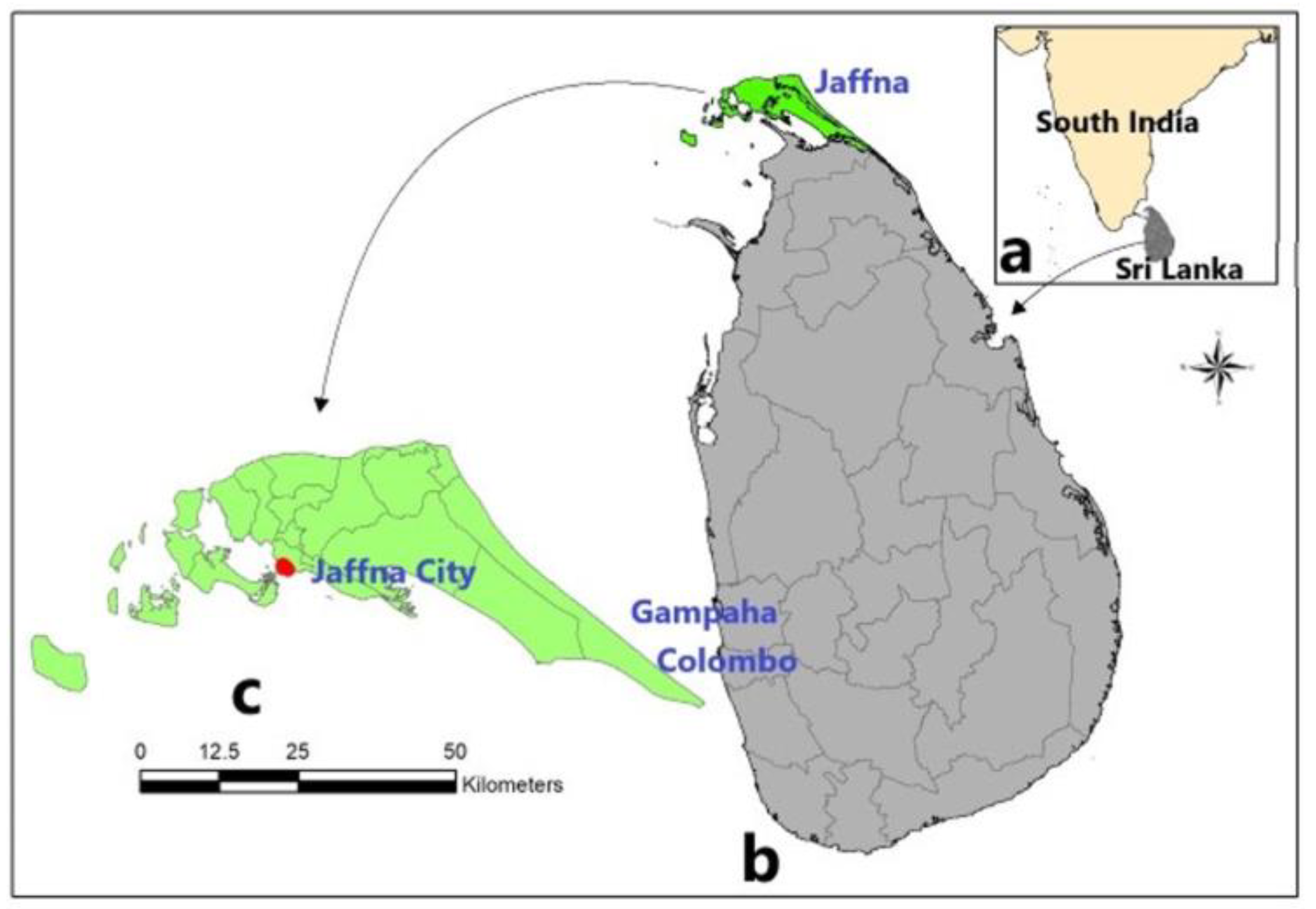
2.4. Ovitrap Collections of Aedes Larvae in Gurunagar, Jaffna
2.5. Statistical Analysis
3. Results
3.1. Dengue Incidence from 1 May 2021 to 31 July 2022 in All of Sri Lanka
3.2. Dengue Incidence from 1 May 2021 to 31 July 2022 in Each of the 25 Districts of Sri Lanka
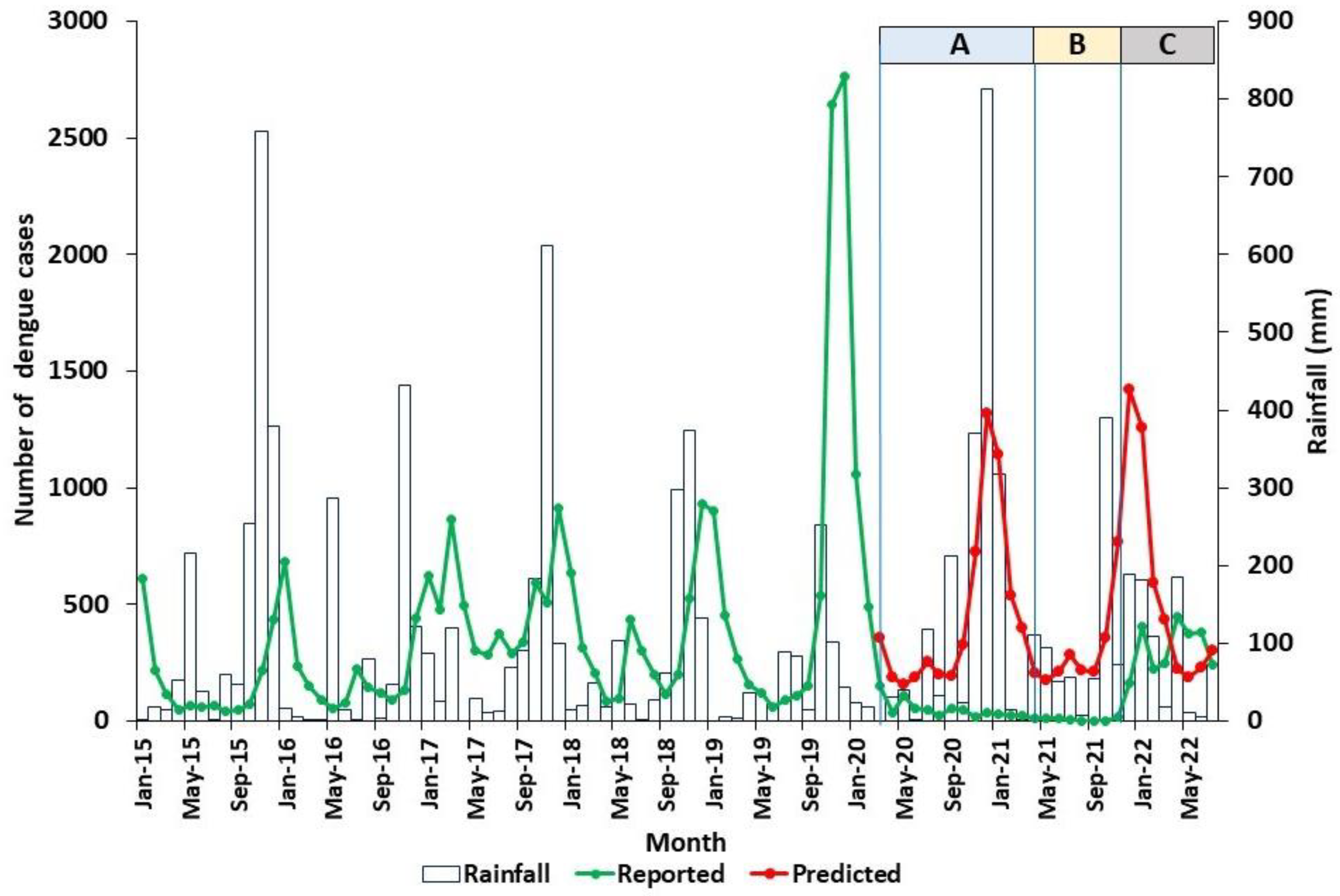
3.3. Dengue Incidence in Relation to Rainfall in the Jaffna District from 1 May 2021 to 31 July 2022
3.4. Aedes Larval Collections from Ovitraps from May 2021 to April 2022 in Gurunagar, Jaffna City
4. Discussion
- m = ratio of the number of vector mosquitoes to the number of humans;
- a = average number of human blood meals taken by a mosquito in a day;
- α = probability of transmission of pathogen from an infected human to a biting mosquito;
- β = probability of transmission of a pathogen from an infected mosquito to a non-immune human during feeding;
- p = daily probability of survival of the mosquito vector;
- n = duration in days from infection of a biting mosquito until the mosquito becomes capable of infecting humans after the pathogen undergoes obligatory development in the mosquito, also termed the extrinsic incubation period;
- r = recovery rate in humans (inverse of the average duration of infectiousness in days).
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Surendran, S.N.; Nagulan, R.; Sivabalakrishnan, K.; Arthiyan, S.; Tharsan, A.; Jayadas, T.T.P.; Raveendran, S.; Kumanan, T.; Ramasamy, R. Reduced dengue incidence during the COVID-19 movement restrictions in Sri Lanka from March 2020 to April 2021. BMC Public Health 2022, 22, 388. [Google Scholar] [CrossRef]
- Liyanage, P.; Rocklov, J.; Tissera, H.A. The impact of COVID-19 lockdown on dengue transmission in Sri Lanka. A natural experiment for understanding the influence of human mobility. PLoS Negl. Trop. Dis. 2021, 15, e0009420. [Google Scholar] [CrossRef] [PubMed]
- Ariyaratne, D.; Gomes, L.; Jayadas, T.T.P.; Kuruppu, H.; Kodituwakku, L.; Jeewandara, C.; Hetti, N.P.; Dheerasinghe, A.; Samaraweera, S.; Ogg, G.S.; et al. Epidemiological and virological factors determining dengue transmission in Sri Lanka during the COVID-19 pandemic. PLoS Glob. Public Health 2022, 2, e0000399. [Google Scholar] [CrossRef]
- Niriella, M.A.; Ediriweera, D.S.; De Silva, A.P.; Premarathna, B.H.R.; Jayasinghe, S.; de Silva, H.J. Dengue and leptospirosis infection during the coronavirus 2019 outbreak in Sri Lanka. Trans. Roy. Soc. Trop. Med. Hyg. 2021, 115, 944–946. [Google Scholar] [CrossRef]
- Epidemiology Unit, Sri Lanka. Dengue Trends. Available online: https://www.epid.gov.lk/web/index.php?option=com_casesanddeaths&Itemid=448&lang=en (accessed on 5 August 2022).
- Chen, Y.; Li, N.; Lourenço, J.; Wang, L.; Cazelles, B.; Dong, L.; Li, B.; Liu, Y.; Jit, M.; Bosse, N.I.; et al. Measuring the effects of COVID-19-related disruption on dengue transmission in southeast Asia and Latin America: A statistical modelling study. Lancet Infect. Dis. 2022, 22, 657–667. [Google Scholar] [CrossRef]
- Jayadas, T.T.P.; Kumanan, T.; Gomes, L.; Jeewandara, C.; Malavige, G.N.; Ranasinghe, D.; Jadi, R.S.; Ramasamy, R.; Surendran, S.N. Regional variation in dengue virus serotypes in Sri Lanka and its clinical and epidemiological relevance. Diagnostics 2021, 11, 2084. [Google Scholar] [CrossRef] [PubMed]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. Available online: https://ourworldindata.org/policy-responses-covid (accessed on 27 August 2022). [CrossRef]
- World Health Organisation. Fact sheet on Dengue and Severe Dengue. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue (accessed on 21 August 2022).
- Surendran, S.N.; Jayadas, T.T.P.; Thiruchenthooran, V.; Raveendran, S.; Tharsan, A.; Sandrasegaram, S.; Sivabalakrishnan, K.; Suthakar, K.; Ponnaiah, B.; Gomes, L.; et al. Aedes larval bionomics and implications for dengue control in the paradigmatic Jaffna peninsula in northern Sri Lanka. Parasit Vectors 2021, 14, 162. [Google Scholar] [CrossRef]
- Surendran, S.N.; Veluppillai, T.; Eswaramohan, T.; Sivabalakrishnan, K.; Noordeen, F.; Ramasamy, R. Salinity tolerant Aedes aegypti and Ae albopictus–infection with dengue virus and contribution to dengue transmission in a coastal peninsula. J. Vector Borne Dis. 2018, 55, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Epidemiology Unit, Ministry of Health, Sri Lanka. Guidelines on Management of Dengue Fever and Dengue Haemorrhagic Fever in Adults. National Guidelines. Revised and Expanded Edition 2012. Ministry of Health, Sri Lanka. Available online: http://www.epid.gov.lk/web/images/pdf/Publication/guidelines_for_the_management_of_df_and_dhf_in_adults.pdf (accessed on 19 August 2022).
- Ong, S.Q.; Ahmad, H.; Mohd Ngesom, A.M. Implications of the COVID-19 Lockdown on Dengue Transmission in Malaysia. Infect. Dis. Rep. 2021, 13, 148–160. [Google Scholar] [CrossRef] [PubMed]
- Stoddard, S.T.; Forshey, B.M.; Morrison, A.C.; Paz-Soldan, V.A.; Vazquez-Prokopec, G.M.; Astete, H.; Reiner, R.C., Jr.; Vilcarromero, S.; Elder, J.P.; Halsey, E.S.; et al. House-to-house human movement drives dengue virus transmission. Proc. Natl. Acad. Sci. USA 2013, 110, 994–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacDonald, G. The Epidemiology and Control of Malaria; Oxford University Press: London, UK, 1957. [Google Scholar]
- Ramasamy, R.; Surendran, S.N. Global climate change and its potential impact on disease transmission by salinity-tolerant mosquito vectors in coastal zones. Front Physiol. 2012, 19, 198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paramasivan, R.; Philip Samuel, P.; Pandian, R.S. Biting rhythm of vector mosquitoes in a rural ecosystem of South India. Int. J. Mosq. Res. 2015, 2, 106–113. [Google Scholar]
- Kusumawathie, P.H.D. Larval infestation of Aedes aegypti and Ae. albopictus in six types of institutions in a dengue transmission area in Kandy, Sri Lanka. Dengue Bull. 2005, 29, 165–168. [Google Scholar]
- Lim, J.T.; Chew, L.Z.X.; Choo, E.L.W.; Dickens, B.S.L.; Ong, J.; Aik, J.; Ng, L.C.; Cook, A.R. Increased dengue transmissions in Singapore attributable to SARS-CoV-2 social distancing measures. J. Infect. Dis. 2021, 223, 399–402. [Google Scholar] [CrossRef] [PubMed]
- Reegan, A.D.; Gandhi, M.R.; Asharaja, A.C.; Devi, C.; Shanthakumar, S.P. COVID-19 lockdown: Impact assessment on Aedes larval indices, breeding habitats, effects on vector control programme and prevention of dengue outbreaks. Heliyon 2020, 6, e05181. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, R.; Subanesan, N.; Wijesundere, A.; Fernando, N.K.; Ramasamy, M.S. Observations on malaria patients seeking treatment in hospitals in a rural and an urban area of Sri Lanka. Indian J. Malariol. 1992, 29, 29–34. [Google Scholar] [PubMed]
- Wijesundere, D.A.; Ramasamy, R. Analysis of historical trends and recent elimination of malaria from Sri Lanka and its applicability for malaria control in other countries. Front. Public Health 2017, 5, 212. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Period | Movement Restrictions | Affected Districts | a Reference Period Related to other Tables and Figures | b Stringency Index Range |
|---|---|---|---|---|
| 1-03-2020 to 30-04-2021 | Documented in [1] | Documented in [1] | A | 11–100 |
| 01–05-2021 to 21–10-2021 | All schools and educational institutions closed nationwide | All districts | B | 51–91 |
| 20-08-2021 to 01-10-2021 | Nationwide stay-at-home order, no public transport, other essential services functioned with limited staff. | All districts | ||
| 20-08-2021 to 31-10-2021 | Interprovincial travel restricted | All districts | ||
| 21-10-2021 | Partial opening of schools (grades 1–5) with fewer than 200 students | All districts | ||
| 31-10-2021 | Travel restrictions lifted | All districts | ||
| 08-11-2021 | Partial opening of schools (grades 10–13) | All districts | ||
| 22-11-2021 onward | Schools and public places opened with no movement restrictions | All districts | C | 54 |
| Comparison | Periods Compared | Species | Change and Probability (p) |
|---|---|---|---|
| Proportion of ovitraps with larvae out of all ovitraps placed. Chi square test | Period A vs. Pre-pandemic period | Ae. aegypti | Significantly reduced in period A χ2 = 121.93 p < 0.00001 |
| Ae. albopictus | Significantly reduced in period A χ2 = 27.32 p < 0.00001 | ||
| Periods B and C vs. Pre-pandemic period | Ae. aegypti | Significantly reduced in periods B and C χ2 = 29.01 p < 0.00001 | |
| Ae. albopictus | Significantly reduced in periods B and C χ2 = 11.40 p = 0.00073 | ||
| Period A vs. Periods B and C | Ae. aegypti | Significantly reduced in period A χ2 = 51.85 p < 0.00001 | |
| Ae. albopictus | Significantly reduced in period A χ2 = 5.43 p = 0.02 | ||
| Periods B and C | Ae. aegypti vs. Ae. albopictus | Significantly more ovitraps with Ae. aegypti χ2 = 10.58 p = 0.001 | |
| Numbers of larvae per ovitrap per month. Mann- Whitney U test | Pre-pandemic period vs. Period A | Ae. aegypti | Significantly more in pre-pandemic period p = 0.0003 |
| Ae. albopictus | Significantly more in pre-pandemic period p = 0.0048 | ||
| Pre-pandemic period vs. Periods B and C | Ae. aegypti | Significantly more in pre-pandemic period p = 0.0017 | |
| Ae. albopictus | Not significantly different, p = 0.1556 | ||
| Period A vs. Periods B and C | Ae. aegypti | Significantly more in periods B and C p = 0.0002 | |
| Ae. albopictus | Significantly more in periods B and C p = 0.0006 | ||
| Periods B and C | Ae. aegypti vs. Ae. albopictus | Tendency to be higher for Ae. aegypti p = 0.0561 | |
| Comparison of numbers of larvae collected per ovitrap | Period A vs. Pre-pandemic Period | Ae. aegypti | 96% reduced in Period A |
| Ae. albopictus | 79% reduced in Period A | ||
| Periods B & C vs. Pre-pandemic Period | Ae. aegypti | 46% reduced in Periods B & C | |
| Ae. albopictus | 29% reduced in Periods B & C | ||
| Period A vs. Periods B & C | Ae. aegypti | 93% reduced in Period A | |
| Ae. albopictus | 70% reduced in Period A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Surendran, S.N.; Nagulan, R.; Tharsan, A.; Sivabalakrishnan, K.; Ramasamy, R. Dengue Incidence and Aedes Vector Collections in Relation to COVID-19 Population Mobility Restrictions. Trop. Med. Infect. Dis. 2022, 7, 287. https://doi.org/10.3390/tropicalmed7100287
Surendran SN, Nagulan R, Tharsan A, Sivabalakrishnan K, Ramasamy R. Dengue Incidence and Aedes Vector Collections in Relation to COVID-19 Population Mobility Restrictions. Tropical Medicine and Infectious Disease. 2022; 7(10):287. https://doi.org/10.3390/tropicalmed7100287
Chicago/Turabian StyleSurendran, Sinnathamby Noble, Ratnarajah Nagulan, Annathurai Tharsan, Kokila Sivabalakrishnan, and Ranjan Ramasamy. 2022. "Dengue Incidence and Aedes Vector Collections in Relation to COVID-19 Population Mobility Restrictions" Tropical Medicine and Infectious Disease 7, no. 10: 287. https://doi.org/10.3390/tropicalmed7100287