Outcomes of Community-Based Systematic Screening of Household Contacts of Patients with Multidrug-Resistant Tuberculosis in Myanmar

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.2.1. Country Setting
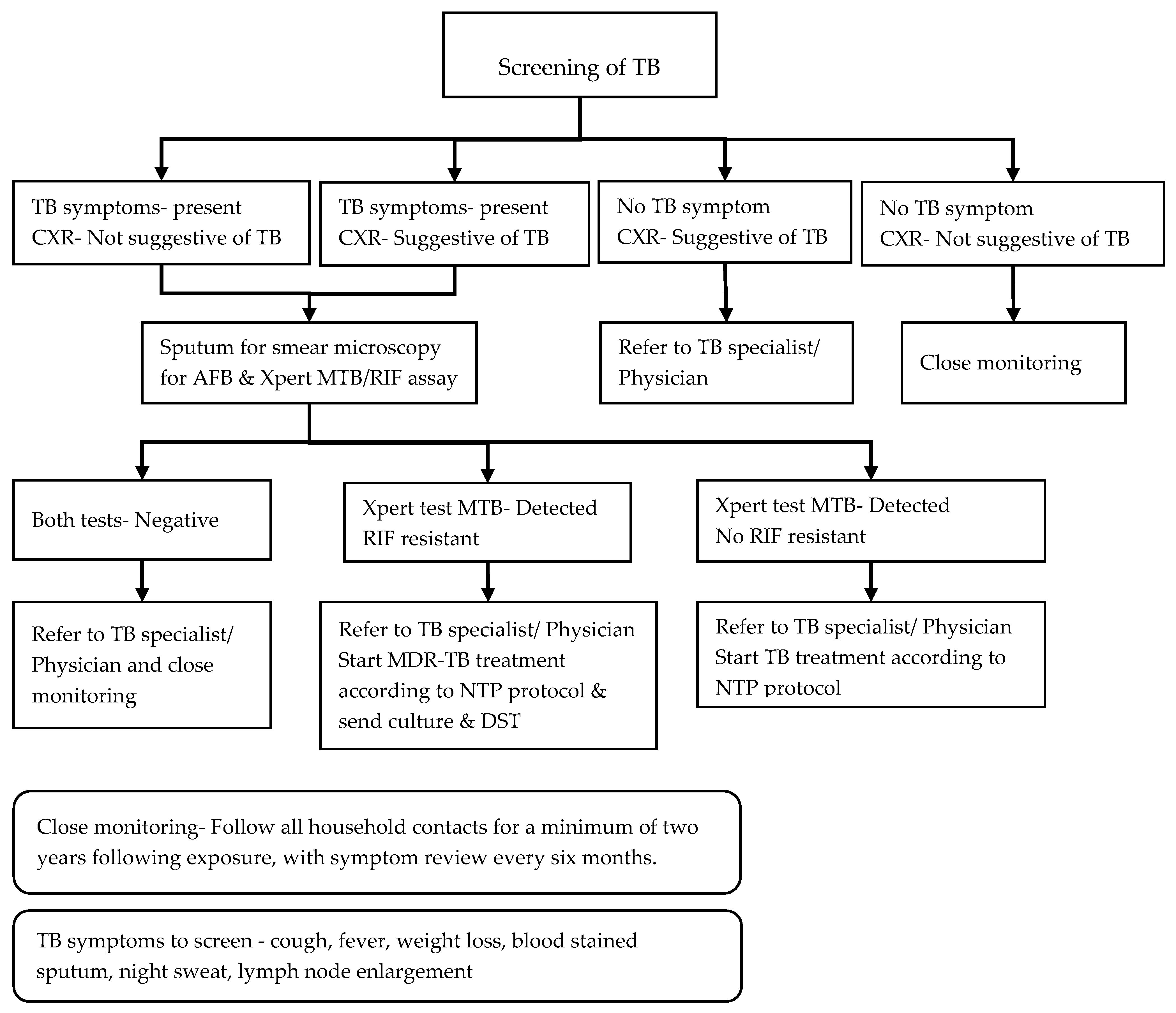
2.2.2. Project Description and the Implementation of Systematic Screening
2.3. Study Sites and Population
2.4. Sources of Data, Data Variables, and Data Collection
2.5. Analysis and Statistics
2.6. Ethics
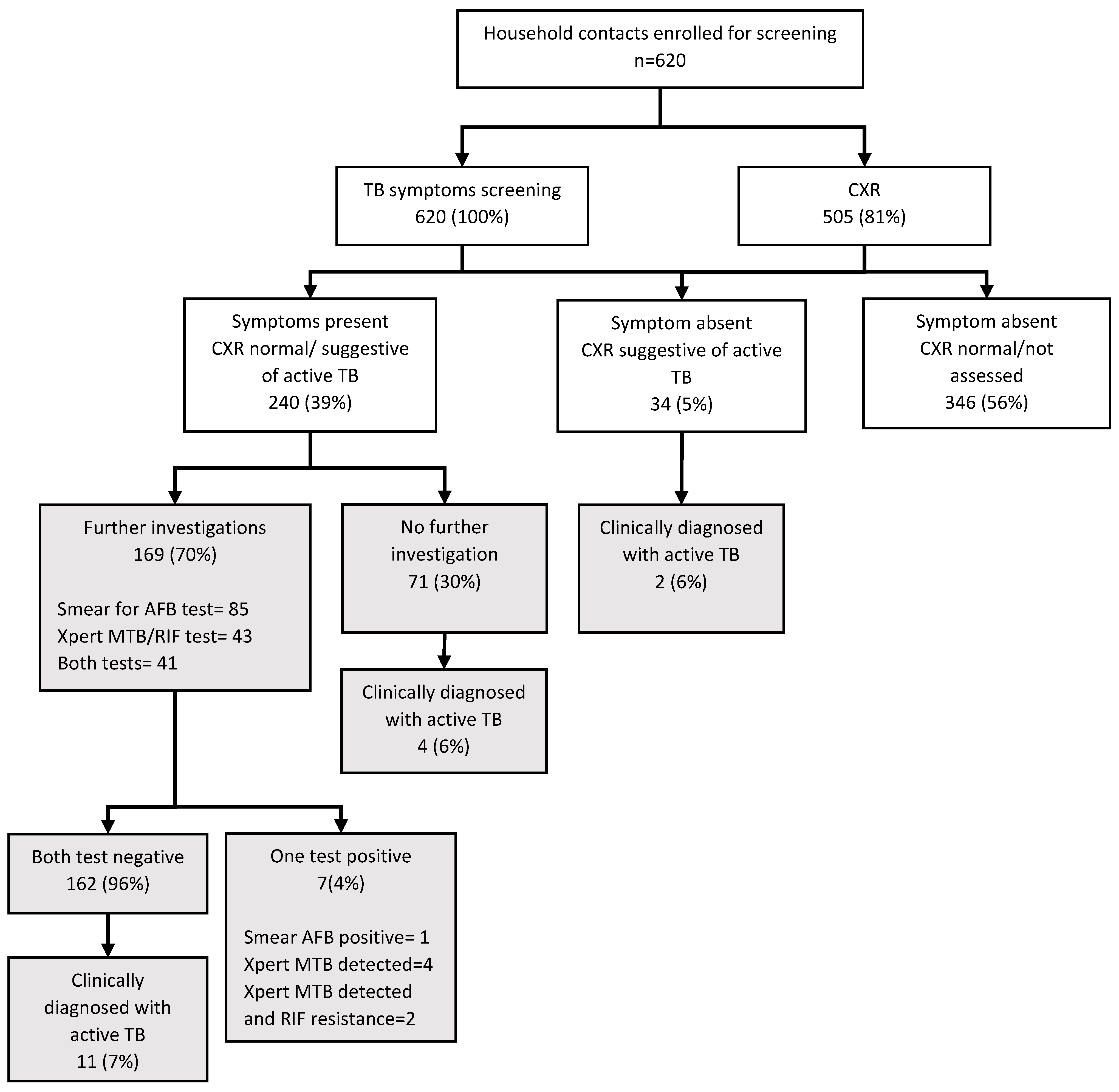
3. Results
3.1. Characteristics Associated with Following the Systematic Screening Algorithm among Symptomatic Contacts
3.2. Characteristics Associated with Diagnosed with Active TB among Registered Contacts
4. Discussion
Policy and Practice Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2018. Available online: http://www.who.int/tb/publications/global_report/en/ (accessed on 29 December 2018).
- World Health Organization. Guidelines for Treatment of Drug-Susceptible Tuberculosis and Patient Care. Available online: http://www.who.int/tb/publications/2017/dstb_guidance_2017/en/ (accessed on 3 May 2017).
- World Health Organization. Systematic Screening for Active Tuberculosis: Principles and Recommendations. Available online: https://www.who.int/tb/tbscreening/en/ (accessed on 11 October 2019).
- Fox, G.J.; Barry, S.E.; Britton, W.J.; Marks, G.B. Contact investigation for tuberculosis: A systematic review and meta-analysis. Eur. Respir. J. 2013, 41, 140–156. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.S.; Yuen, C.M.; Heo, M.; Tolman, A.W.; Becerra, M.C. Yield of contact investigations in households of patients with drug-resistant tuberculosis: Systematic review and meta-analysis. Clin. Infect. Dis. 2014, 58, 381–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-Resistant Tuberculosis. 2014. Available online: http://www.who.int/tb/publications/pmdt_companionhandbook/en/ (accessed on 5 December 2016).
- National Tuberculosis Programme Five Year National Strategic Plan for Tuberculosis Control 2011–2015. Available online: http://www.searo.who.int/myanmar/documents/en/ (accessed on 3 December 2018).
- National Tuberculosis Programme National Strategic Plan for Tuberculosis 2016. Available online: http://mohs.gov.mm/Main/content/publication/list?pagenumber=1&pagesize=9 (accessed on 3 December 2018).
- National Tuberculosis Programme Guidelines for the Management of Multi-Drug Resistant Tuberculosis (MDR-TB) in Myanmar. Available online: http://www.searo.who.int/myanmar/areas/tuberculosis/en/ (accessed on 27 May 2017).
- Wai, P.P.; Shewade, H.D.; Kyaw, N.T.T.; Thein, S.; Thu, A.S.; Kyaw, K.W.Y.; Aye, N.N.; Phyo, A.M.; Maung, H.M.W.; Soe, K.T.; et al. Community-based MDR-TB care project improves treatment initiation in patients diagnosed with MDR-TB in Myanmar. PLoS ONE 2018, 13, e0194087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Chest Radiography in Tuberculosis Detection. Available online: http://www.who.int/tb/publications/chest-radiography/en/ (accessed on 2 July 2017).
- Kigozi, N.G.; Heunis, J.C.; Engelbrecht, M.C. Yield of systematic household contact investigation for tuberculosis in a high-burden metropolitan district of South Africa. BMC Public Health 2019, 19, 867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong-Hough, M.; Turimumahoro, P.; Meyer, A.J.; Ochom, E.; Babirye, D.; Ayakaka, I.; Mark, D.; Ggita, J.; Cattamanchi, A.; Dowdy, D.; et al. Drop-out from the tuberculosis contact investigation cascade in a routine public health setting in urban Uganda: A prospective, multi-center study. PLoS ONE 2017, 12, e0187145. [Google Scholar] [CrossRef] [Green Version]
- Fox, G.J.; Loan, L.P.; Nhung, N.V.; Loi, N.T.; Sy, D.N.; Britton, W.J.; Marks, G.B. Barriers to adherence with tuberculosis contact investigation in six provinces of Vietnam: A nested case–control study. BMC Infect. Dis. 2015, 15, 103. [Google Scholar] [CrossRef] [Green Version]
- Ayakaka, I.; Ackerman, S.; Ggita, J.M.; Kajubi, P.; Dowdy, D.; Haberer, J.E.; Fair, E.; Hopewell, P.; Handley, M.A.; Cattamanchi, A.; et al. Identifying barriers to and facilitators of tuberculosis contact investigation in Kampala, Uganda: A behavioral approach. Implement. Sci. 2017, 12, 33. [Google Scholar] [CrossRef] [Green Version]
- Durovni, B.; Saraceni, V.; Hof, S.V.D.; Trajman, A.; Cordeiro-Santos, M.; Cavalcante, S.; Menezes, A.; Cobelens, F. Impact of Replacing Smear Microscopy with Xpert MTB/RIF for Diagnosing Tuberculosis in Brazil: A Stepped-Wedge Cluster-Randomized Trial. PLoS Med. 2014, 11, e1001766. [Google Scholar] [CrossRef]
- Churchyard, G.J.; Stevens, W.S.; Mametja, L.D.; McCarthy, K.M.; Chihota, V.; Nicol, M.P.; Erasmus, L.K.; Ndjeka, N.O.; Mvusi, L.; Vassall, A.; et al. Xpert MTB/RIF versus sputum microscopy as the initial diagnostic test for tuberculosis: A cluster-randomised trial embedded in South African roll-out of Xpert MTB/RIF. Lancet Glob. Health 2015, 3, e450–e457. [Google Scholar] [CrossRef] [Green Version]
- Nwachukwu, N.O.; Onyeagba, R.A.; Nwaugo, V.O.; Ononiwu, H.A.; Okafor, D.C. Diagnostic Accuracy of Xpert MTB/RIF Assay in Diagnosis of Pulmonary Tuberculosis. J. Infect. Dis. Treat. 2016, 2, 1–3. [Google Scholar]
- Van Kampen, S.C.; Tursynbayeva, A.; Koptleuova, A.; Murzabekova, Z.; Bigalieva, L.; Aubakirova, M.; Pak, S.; Hof, S.V.D. Effect of Introducing Xpert MTB/RIF to Test and Treat Individuals at Risk of Multidrug-Resistant Tuberculosis in Kazakhstan: A Prospective Cohort Study. PLoS ONE 2015, 10, e0132514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grandjean, L.; Gilman, R.H.; Martin, L.; Soto, E.; Castro, B.; López, S.; Coronel, J.; Castillo, E.; Alarcón, V.; Lopez, V.; et al. Transmission of Multidrug-Resistant and Drug-Susceptible Tuberculosis within Households: A Prospective Cohort Study. PLoS Med. 2015, 12, e1001843. [Google Scholar] [CrossRef] [PubMed]
- Singla, N.; Singla, R.; Jain, G.; Habib, L.; Behera, D. Tuberculosis among household contacts of multidrug-resistant tuberculosis patients in Delhi, India. Int. J. Tuberc. Lung Dis. 2011, 15, 1326–1330. [Google Scholar] [CrossRef] [PubMed]
- Titiyos, A.; Jerene, D.; Enquselasie, F. The yield of screening symptomatic contacts of multidrug-resistant tuberculosis cases at a tertiary hospital in Addis Ababa, Ethiopia. BMC Res. Notes 2015, 8, 501. [Google Scholar] [CrossRef] [Green Version]
- Chamie, G.; Wandera, B.; Luetkemeyer, A.; Bogere, J.; Mugerwa, R.D.; Havlir, D.V.; Charlebois, E.D. Household ventilation and tuberculosis transmission in Kampala, Uganda. Int. J. Tuberc. Lung Dis. 2013, 17, 764–770. [Google Scholar] [CrossRef]
- World Health Organization. WHO Policy on TB Infection Control in Health-Care Facilities, Congregate Settings and Households. Available online: https://www.who.int/tb/publications/2009/9789241598323/en/ (accessed on 11 October 2019).
- Puryear, S.; Seropola, G.; Ho-Foster, A.; Arscott-Mills, T.; Mazhani, L.; Firth, J.; Goldfarb, D.M.; Ncube, R.; Bisson, G.P.; Steenhoff, A.P. Yield of contact tracing from pediatric tuberculosis index cases in Gaborone, Botswana. Int. J. Tuberc. Lung Dis. 2013, 17, 1049–1055. [Google Scholar] [CrossRef]
- Amanullah, F.; Ashfaq, M.; Khowaja, S.; Parekh, A.; Salahuddin, N.; Lotia-Farrukh, I.; Khan, A.J.; Becerra, M.C. High tuberculosis prevalence in children exposed at home to drug-resistant tuberculosis. Int. J. Tuberc. Lung Dis. 2014, 18, 520–527. [Google Scholar] [CrossRef]
- Becerra, M.C.; Franke, M.F.; Appleton, S.C.; Joseph, J.K.; Bayona, J.; Atwood, S.S.; Mitnick, C.D. Tuberculosis in Children Exposed at Home to Multidrug-resistant Tuberculosis. Pediatr. Infect. Dis. J. 2013, 32, 115–119. [Google Scholar] [CrossRef] [Green Version]
- Chheng, P.; Nsereko, M.; Malone, L.L.; Okware, B.; Zalwango, S.; Joloba, M.; Boom, W.H.; Mupere, E.; Stein, C.M. Tuberculosis case finding in first-degree relative contacts not living with index tuberculosis cases in Kampala, Uganda. Clin. Epidemiol. 2015, 7, 411–419. [Google Scholar]
- Padmapriyadarsini, C.; Das, M.; Burugina Nagaraja, S.; Rajendran, M.; Kirubakaran, R.; Chadha, S.; Tharyan, P. Is Chemoprophylaxis for Child Contacts of Drug-Resistant TB Patients Beneficial? A Systematic Review. Tuberc. Res. Treat. 2018, 2018, 3905890. [Google Scholar] [CrossRef] [Green Version]
- Seddon, J.A.; Hesseling, A.C.; Finlayson, H.; Fielding, K.; Cox, H.; Hughes, J.; Godfrey-Faussett, P.; Schaaf, H.S. Preventive Therapy for Child Contacts of Multidrug-Resistant Tuberculosis: A Prospective Cohort Study. Clin. Infect. Dis. 2013, 57, 1676–1684. [Google Scholar] [CrossRef] [PubMed]
- Seddon, J.A.; Godfrey-Faussett, P.; Hesseling, A.C.; Gie, R.P.; Beyers, N.; Schaaf, H.S. Management of children exposed to multidrug-resistant Mycobacterium tuberculosis. Lancet Infect. Dis. 2012, 12, 469–479. [Google Scholar] [CrossRef]
- Moore, D.A.J. What can we offer to 3 million MDRTB household contacts in 2016? BMC Med. 2016, 14, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Total | Followed the Systematic Screening Algorithm | ||||
|---|---|---|---|---|---|---|
| n | (%) † | n | (%) § | OR | (95% CI) * | |
| Total | 240 | (100) | 169 | (70.4) | ||
| Sex | ||||||
| Male | 105 | (43.7) | 70 | (66.7) | Ref | |
| Female | 135 | (56.3) | 99 | (73.3) | 0.7 | (0.3–1.5) |
| Age | ||||||
| <5 years | 16 | (6.7) | 2 | (12.5) | 0.3 | (0.0–0.2) |
| 5–14 years | 44 | (18.3) | 15 | (34.1) | 0.2 | (0.0–0.4) |
| 15–49 years | 117 | (48.8) | 95 | (81.2) | Ref | |
| >49 years | 58 | (24.2) | 56 | (96.5) | 6.5 | (2.2–18.9) |
| Missing | 5 | (2.1) | 1 | (20.0) | 0.1 | (0.0–0.8) |
| History of previous TB | ||||||
| Yes | 11 | (4.6) | 9 | (81.8) | 1.9 | (0.5–6.6) |
| No | 229 | (95.4) | 160 | (69.9) | Ref | |
| HIV status | ||||||
| Positive | 3 | (1.3) | 3 | (1.8) | NA | |
| Unknown | 237 | (98.7) | 166 | (98.2) | ||
| History of diabetes mellitus | ||||||
| Yes | 2 | (0.8) | 1 | (50.0) | 0.4 | (0.0–6.8) |
| Unknown | 238 | (99.2) | 168 | (70.6) | Ref | |
| Characteristics | Total | Diagnosed with Active TB | |||||
|---|---|---|---|---|---|---|---|
| n | (%) † | n | % | (95% CI) §,* | PR | (95% CI) * | |
| Total | 610 | 100 | 24 | 3.9 | (2.3–6.5) | - | |
| Sex | |||||||
| Male | 258 | (41.6) | 12 | 4.7 | (1.9–10.8) | 1.4 | (0.6–3.4) |
| Female | 362 | (58.4) | 12 | 3.3 | (2.1–5.2) | ref | |
| Age | |||||||
| <5 years | 40 | (6.5) | 4 | 10.0 | (3.6–24.7) | 3.7 | (1.2–11.4) |
| 5–14 years | 98 | (15.8) | 4 | 4.1 | (1.2–13.4) | 1.5 | (0.4–5.5) |
| 15–49 years | 337 | (54.4) | 8 | 2.7 | (1.4–5.1) | ref | |
| >49 years | 137 | (22.1) | 5 | 4.4 | (1.8–10.0) | 1.6 | (0.6–4.6) |
| Missing | 8 | (1.3) | 1 | 12.5 | (1.3–60.7) | 4.7 | (0.6–34.9) |
| History of previous TB | |||||||
| Yes | 17 | (2.7) | 0 | - | |||
| No | 603 | (97.3) | 24 | 4.0 | (2.3–6.7) | NA | |
| HIV status | |||||||
| Positive | 6 | (1.0) | 1 | 16.7 | (1.8–67.9) | 4.4 | (0.6–32.0) |
| Unknown | 614 | (99.0) | 23 | 3.7 | (2.2–6.4) | ref | |
| History of diabetes mellitus | |||||||
| Yes | 3 | (0.5) | 0 | - | |||
| Unknown | 617 | (99.5) | 24 | 3.9 | (2.3–6.6) | NA | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kyaw, N.T.T.; Sithu, A.; Satyanarayana, S.; Kumar, A.M.V.; Thein, S.; Thi, A.M.; Wai, P.P.; Lin, Y.N.; Kyaw, K.W.Y.; Tun, M.M.T.; et al. Outcomes of Community-Based Systematic Screening of Household Contacts of Patients with Multidrug-Resistant Tuberculosis in Myanmar. Trop. Med. Infect. Dis. 2020, 5, 2. https://doi.org/10.3390/tropicalmed5010002
Kyaw NTT, Sithu A, Satyanarayana S, Kumar AMV, Thein S, Thi AM, Wai PP, Lin YN, Kyaw KWY, Tun MMT, et al. Outcomes of Community-Based Systematic Screening of Household Contacts of Patients with Multidrug-Resistant Tuberculosis in Myanmar. Tropical Medicine and Infectious Disease. 2020; 5(1):2. https://doi.org/10.3390/tropicalmed5010002
Chicago/Turabian StyleKyaw, Nang Thu Thu, Aung Sithu, Srinath Satyanarayana, Ajay M. V. Kumar, Saw Thein, Aye Myat Thi, Pyae Phyo Wai, Yan Naing Lin, Khine Wut Yee Kyaw, Moe Myint Theingi Tun, and et al. 2020. "Outcomes of Community-Based Systematic Screening of Household Contacts of Patients with Multidrug-Resistant Tuberculosis in Myanmar" Tropical Medicine and Infectious Disease 5, no. 1: 2. https://doi.org/10.3390/tropicalmed5010002