1. Introduction
Globally, injuries account for approximately 10% of the world’s mortality burden [
1,
2]. Disability is the cause of more than half of the premature mortality worldwide, and low- and middle-income countries (LMICs) bear a disproportionate burden due to higher rates of trauma, lack of prehospital care services, limited post-traumatic injury care and rehabilitation services, or a combination of these factors [
3]. One study estimated the monetary value of disability-adjusted life years (DALYs) in East African countries to be nearly
$200 billion in 2015 [
4]. However, post-injury disability is under-measured in many LMICs, including in sub-Saharan Africa (SSA) with limited evidence on the best practices for how to assess disability. In Rwanda, a nationwide population study conducted in 2012 found that nearly a quarter of households reported having been affected by serious injuries [
5]. However, Rwanda’s overall burden of injury-related disability is not well understood.
The World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0) is a standardized tool to quantify physical, mental, and social disability and functioning post-injury [
6]. The WHODAS 2.0 has been widely utilized in a variety of settings and populations to measure impairment and disability after psychological trauma [
7,
8,
9,
10] as well as to measure functional status after surgical operations or physical trauma [
11]. In sub-Saharan Africa (SSA), the WHODAS 2.0 has been adapted and used to measure disability after road traffic incidents [
12], postoperative disability in surgical interventions [
13,
14], and to characterize severity of disability [
15]. The WHODAS 2.0 has also been adapted and validated for use in measuring psychological functional impairment in Rwandan children with psychosocial problems [
16]. These studies have demonstrated that the WHODAS 2.0 is feasible for assessment of functional status post-injury and has good cross-cultural adaptation. However, there remains a need for improved understanding of the impacts of injury and functional status in the adult Rwandan population, where an estimated 10% of disability-adjusted life-years (DALYs) are attributable to injury-related traumas, indicating a high economic burden [
4,
17].
The Katz Index of Activities of Daily Living (Katz ADL) is another commonly used measure for assessing disability and functional status post-injury [
18,
19]. While the Katz ADL has been used primarily in geriatric and chronically ill patient populations to evaluate functional capacity to independently perform activities typical in daily life, it has not been commonly studied among younger patient populations and those recovering from acute trauma [
20,
21,
22,
23]. One previous study comparing postoperative disability among surgical patients found correlation between the Katz ADL and WHODAS 2.0, suggesting that either could be useful in characterizing the functional status in such populations [
24].
In addition to existing formalized assessment tools, a pragmatic assessment of patients’ self-perception of their own functional status may help determine which scales are most appropriate for post-traumatic injury populations in LMICs (
Table A1). Additionally, self-perception of disability may help simplify screening and identification of patients in need for post-injury rehabilitation and support. Incorporating patients’ own perceived functional status could also serve to capture a patient’s lived experience post-injury in a culturally sensitive manner.
Determination of the most contextually appropriate approaches for evaluating patients’ functional status post-injury is necessary to better identify patient needs and allocate resources, and to design interventions to improve patients’ quality of life. The aim of this pilot study was to evaluate the functional status at hospital discharge and at 28-day follow-up of patients presenting for emergency care with significant acute injuries in Kigali, Rwanda and assess the correlation between the WHODAS 2.0, Katz ADL and the patients’ self-assessment of functional status.
2. Materials and Methods
2.1. Study Design and Setting
This is an a priori secondary analysis pilot evaluation of disability among patients experiencing injuries in Kigali, Rwanda comparing patients’ self-perception of functional status post-injury with standardized tools. The data used in this study were obtained from a prospective cohort study evaluating emergency care received by patients with significant injuries who presented to the emergency department (ED) of the Centre Hospitalier Universitaire de Kigali (CHUK) in Kigali, Rwanda from January to June 2020. Due to the COVID-19 pandemic, study activities were paused from March until June 2020, such that the data collection periods encompassed a pre-COVID-19 period from 27 January–21 March and a COVID-19 study period from 1–28 June [
24]. The study was approved by the CHUK ethics committee, the University of Rwanda College of Medicine and Health Sciences and the institutional review board of Rhode Island Hospital (Lifespan IRB00000396).
CHUK is a tertiary care hospital that serves the Rwandan population of approximately 12 million people and acts as the national public receiving center for all serious injuries [
25]. CHUK is an urban public tertiary care hospital with approximately 500 inpatient beds, teaching surgical and medical specialty consultant services. It is the one of the country’s largest injury referral centers and houses the country’s sole emergency medicine (EM) training program.
2.2. Study Population
Patients were eligible for inclusion if they met the following criteria: (1) age ≥ 15 years old, (2) presenting with acute injury (within 12 h of occurrence), (3) significant injury defined using a Kampala Trauma Score (KTS) ≤ 13 [
26,
27]. Patients with concurrent medical needs unrelated to the index injury, pregnant patients, age ≤ 14 years old, those unable or unwilling to provide informed consent, and any legal prisoner of the state were excluded from enrollment.
2.3. Data Collection and Management
All patients presenting for injury care that met inclusion criteria were continuously screened during the study recruitment periods. To avoid impeding clinical care, patients were screened after initial triage and stabilization. Screened patients meeting inclusion criteria and providing informed consent were enrolled. If a patient was unable to consent due to incapacity, informed consent was obtained from a legally authorized patient representative, which could include a parent, guardian, or caretaker. Enrolled participants were followed through their ED course, as inpatients and as outpatients post-discharge through 28-days after their injury event. Follow-up at 28 days was conducted in-person for participants still admitted to the hospital and via telephone for those discharged. If a patient was unable to respond their designated representative was contacted. Participants were given appropriate compensation for study involvement. If participants were unable to be reached after three attempts, the participant was deemed lost to follow-up. Study personnel trained in research protocols collected data using structured case reporting forms during the data collection periods.
2.4. Functional Status Assessments
A functional status evaluation of disability was conducted for each participant pre-injury, at time of discharge and at 28-days after the initial injury. Disability was assessed using the 12-item WHODAS 2.0 and Katz ADL scale, which have been demonstrated to have utility in disability assessments in both injury and non-injury pathologies [
6,
11,
12]. Additionally, a brief 6-item self-perception questionnaire was completed by all patients who were discharged from the hospital at 28-days.
The WHODAS 2.0 consists of 12 questions, each scaled from 0 (no difficulty) to 4 (extreme difficulty or unable to perform) regarding difficulties experienced in the past 30 days, with a total score ranging from 0–48, with 0 corresponding to no disability and 48 to complete disability. The Katz ADL index consists of 6 questions, each scaled as 0 (requires assistance) or 1 (able to perform activity without assistance) with a total score ranging from 0–6 (0 corresponding to completely dependent and 6 to completely independent) [
21]. The self-perception questionnaire was an adapted form of a previously used tool in East Africa [
28]. The self-perception questionnaire was completed by discharged patients at the final 28-day follow-up and included data on participants’ abilities to perform their pre-injury vocational activities (representing a patient and socio-culturally centered outcome) as well as a single item question for the patient’s own self-assessment of their overall functional status. The item on self-perceived overall functional status was scored from 1–4 corresponding to “fully recovered”, “partially recovered”, “same since leaving hospital”, or “worse since leaving hospital”. For patients still hospitalized at follow-up day 28, a general evaluation of neurologic-specific disability was assessed using the AVPU scale (an acronym from “alert, verbal, pain, unresponsive”), a simple scale used to record a patient’s level of consciousness, and the patient’s Glasgow Coma Scale (GCS) as documented on day 28. The GCS is a reliable scoring system used to describe the level of consciousness after traumatic brain injury.
2.5. Data Analysis
Descriptive analyses using frequencies with percentages, medians with interquartile ranges (IQR), or means with standard deviations (SD) were performed as appropriate for the continuous data variables. Comparisons were conducted with t-test, Mann–Whitney U test, Pearson’s chi-squared test, or Fisher’s exact test as appropriate. The primary outcome was descriptive profiles of the functional status at 28-days post-injury using the WHODAS 2.0 and ADL scale. Secondary outcomes included in-hospital complications (e.g., nosocomial infections, thromboembolic events, and respiratory decompensation) and length of stay. Additionally, for patients who were discharged from hospital, the functional status assessment scales were compared (single question on patients’ self-perceived functional status, Katz’ ADL, WHODAS 2.0) using Kendall’s (Tau) rank correlation coefficient. STATA Version 15.0 (Stata Corp; College Station, TX, USA) was used for all analyses.
3. Results
A total of 37 patients with serious injuries were enrolled during the study period. Of these patients, nine died while in the hospital, and four were lost to follow-up leaving 24 patients with complete discharge and 28-day follow-up data for analysis. A total of 21 (87.5%) patients were male and the median (IQR) age was 30.5 (24–33.5) years with an age range of 18–76 years. The most common mechanisms of injury were road traffic accidents (70.8%) and falls (8.3%). Head and face injuries were the most common (75%), followed by extremity (41.7%), chest (29.2%) and neck (25%) injuries; 58.3% were diagnosed with traumatic brain injury during hospitalization. Most patients (75%) reported they had no prior medical conditions prior to their injury. One-quarter of the patients were still hospitalized at day 28 follow-up (
Table 1).
Among the six patients still hospitalized at 28-day follow-up, none were categorized as “alert” using the AVPU scale, 3 (50%) could orient to voice, 1 (16.7%) could orient to pain, while 2 (33.3%) were unresponsive (
Table 2). The median GCS was 15 (IQR: 10–15) among those hospitalized (
Table 2).
Prior to their injury, no patients had reported any baseline functional disabilities in performing ADLs according to the Katz ADL scale and all patients reported going to work (91.7%) and/or school (12.5%) (
Table 2). Using the Katz ADL scale to assess ability to perform ADLs independently at 28-day follow-up, 20 (83.3%) could eat, 13 (54.2%) could bathe, 15 (62.5%) could use the toilet, and 20 (83.3%) were continent of bowel and bladder (
Table 2). Only 6 (25%) reported the ability to get out of bed without assistance.
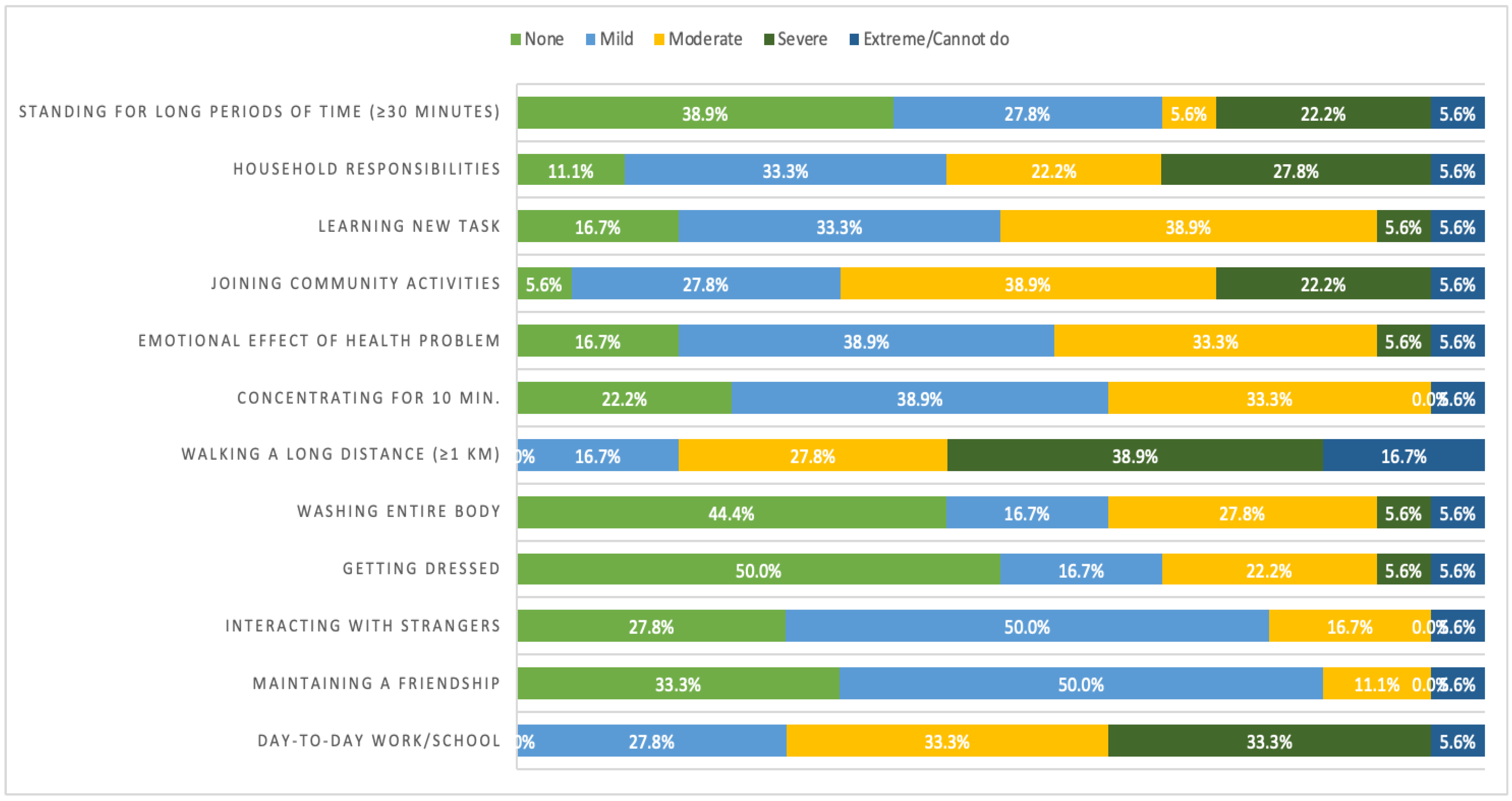
Among the 18 patients who had been discharged from the hospital, the median WHODAS 2.0 score was 16 (IQR: 9–24). Approximately one-third of patients reported severe or extreme difficulties in standing for more than 30 min (27.8%), completing household responsibilities (33.4%), or joining community activities (27.8%). None of the patients reported they had “no difficulties” in their day-to-day work/school or to walk more than one kilometer. The median number of days in the past 30 days in which the patient experienced difficulties with one or more of the listed activities was 25.5 days (IQR: 15–30). The distribution of responses for the WHODAS 2.0 questionnaire items are shown in
Figure 1.
Regarding the patient’s overall status at 28-day follow-up for those discharged, 15 (83.3%) patients reported being able to walk and 16 (88.9%) being able to speak; however, only 3 (16.7%) were able to return to work, 14 (77.8%) were still unable to work and one (5.6%) had not worked prior to the injury. Most patients reported that their health status was partially recovered (66.7%) or the same (22.2%) since discharge from the hospital (
Table 3) at day 28 post-injury. Only two (11.1%) patients reported that they had fully recovered by day 28 (
Table 3). The median number of days in the past 30 days requiring reduced activities or work was 8.5 (IQR: 5–14) days with 7.5 (IQR: 6–10) days of being totally unable to carry out tasks.
When comparing the different functional assessment scales (
Table 4), the Katz ADL Index and the WHODAS 2.0 were strongly correlated (τ = −0.63,
p = 0.001) and the self-perception item was strongly correlated with the WHODAS 2.0 (τ = 0.49,
p = 0.015). However, the self-perception item was not well correlated with the Katz’ ADL scale (τ = −0.27,
p = 0.247).
4. Discussion
This study evaluated the functional status at hospital discharge and at 28-day follow-up of patients presenting to a tertiary care emergency department with acute injuries in Kigali, Rwanda. Among this cohort of patients with severe injuries, post-injury morbidity was high with most patients having significant functional limitations at 28-days post-injury. The use of both a pragmatic and simple self-perception questionnaire and formalized evaluation tools was feasible with a strong correlation found between self-perception and the WHODAS 2.0.
While the WHODAS 2.0 and Katz’ ADL Index were well correlated with each other, the strong correlation between patient’s self-perceived functional status with the WHODAS 2.0 versus the poor correlation with the ADL scale suggest that the WHODAS 2.0 may be more appropriate for use in post-traumatic injury patient populations that are relatively young in comparison to the ADL scale. This finding also suggests that a single-item assessment of self-perceived functional status may be a much simpler alternative which may perform as well as more complex scales such as WHODAS 2.0 and better reflect patients’ own perceived needs. For instance, the Katz ADL and WHODAS 2.0 assessment scales did not always reflect a practical reality for patients who were discharged. The median WHODAS 2.0 score in our study was 16 (IQR: 9–24); however, despite this score indicating a mild disability status classification, many patients still reported significant impairment and impact on their quality of life: 77.8% of participants reported still being unable to return to work, and a median of 8.5 days of reduced daily activity at day 28. This finding is also consistent with previous research on functional status and disability after traumatic injury [
29,
30].
Notably, nearly three quarters of injuries in this study were caused by road traffic accidents (RTAs). In 2010, the United Nations General Assembly declared 2011–2020 the Decade of Action for Road Safety and outlined five categories in a framework for improvement. This included improving the post-crash response through the provision of post-injury rehabilitation [
31]. Despite this declaration, there has not been a significant amount of progress globally [
32]. A total of 93% of road traffic fatalities occur in LMICs, despite LMICs only having around 60% of the world’s vehicles. Sub-Saharan Africa bears a disproportionate burden of injury and death due to RTAs [
33,
34,
35], although there remains a paucity of comprehensive data on road traffic injuries in LMICs, and few studies have examined the relationship between long-term disability and road traffic injuries. One-quarter of patients still required hospitalization and most of those who were discharged reported an impaired functional status since discharge, which may reflect the severity of injuries as well as the relative lack of formal rehabilitation services and centers available.
Functional status after injury remains poorly characterized in LMIC settings, which has a direct impact on understanding rehabilitation service needs and resource allocation in these populations. This study has demonstrated that the WHODAS 2.0 and a single-item question on patient’s self-perceived functional status may be simple and useful tools in measuring functional status post-injury in similar settings. Both assessments are highly pragmatic for use in resource-constrained settings, as they take less than a few minutes to administer and can be conducted over the telephone or in-person and are therefore generally clinically acceptable for assessing functional status post-injury.
Previous studies have indicated a need for increased injury rehabilitation services in countries with high injury burdens [
31,
36,
37]. Given the unmet need for rehabilitation services in LMICs [
36], these scales can also help clinicians monitor their patients’ functional status to better assess patient needs after discharge and plan their care accordingly. As rehabilitation services are being developed, findings from this study demonstrate that the WHODAS 2.0 and self-perception questionnaires can be used to better characterize discharged injury patients’ needs and inform rehabilitation care and recovery after traumatic injuries.
5. Conclusions
This was a pilot study and therefore limited by small sample size; further evaluations of disability assessment scales in larger studies and across different levels of health facilities (e.g., district hospitals, ambulatory settings) in Rwanda and other LMICs are warranted. This study included only patients with a KTS score < 14 and therefore represents a subset of patients with severe injuries and cannot be generalized to patients with more minor injuries or those presenting to lower-level health facilities such as district hospitals. Additionally, although the WHODAS 2.0 and KATZ ADL have been validated in sub-Saharan African contexts, they may not fully capture what it means to be disabled in a Rwandan context.
This study did not specifically evaluate patient perceptions of the scales and assessments used. However, no patients declined to complete the phone assessments and assessments were successfully completed in a short amount of time via phone call. This indicates that evaluating disability can be feasibly conducted using telehealth and without requiring additional health facility visits. In this setting, using telehealth to conduct evaluations could save patients’ the time and expense associated with traveling to the clinic or hospital.
This study found that evaluating disability after injuries requiring emergency care in the Rwandan context was feasible via telehealth and without requiring additional visits by patients to healthcare facilities. The WHODAS 2.0 scale and self-perception questionnaire may be valuable for rapid post-injury functional assessment, as they were strongly correlated. These disability assessment tools may have utility in rehabilitation care in other settings in Africa, though further research is necessary.
Author Contributions
Conceptualization, C.G.M., S.C.G., E.O. and A.R.A.; methodology, A.R.A. and O.Y.T.; formal analysis, O.Y.T. and S.C.G.; data collection and patient enrollment A.B., D.U. and C.U.; writing—original draft preparation, S.C.G. and E.O.; writing—review and editing, E.O., C.G.M., S.C.G., A.H.S., D.U., C.U. and A.B.; supervision, A.R.A. and C.G.M.; funding acquisition, A.R.A. All authors have read and agreed to the published version of the manuscript.
Funding
Funding for this research was provided through Brown Physicians, Incorporated and Brown Emergency Medicine research grants.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the CHUK ethics committee, the University of Rwanda College of Medicine and Health Sciences and the institutional review board of Rhode Island Hospital (Lifespan IRB00000396).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ongoing analyses and reporting.
Acknowledgments
The authors would like to thank the Emergency Department staff and research personnel at the Centre Hospitalier Universitaire de Kigali for their help and support of the study.
Conflicts of Interest
The authors have no conflict of interest. The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the views of or any academic organizations. The funders played no role in the collection, analysis or reporting of the data.
Appendix A
Table A1.
Self-Perception Questionnaire.
Table A1.
Self-Perception Questionnaire.
| Self-Assessment Questionnaire | Response Options |
|---|
| Is the participant still alive? | No |
| Yes |
| Is the participant able to speak? | No |
| Yes |
| Is the participant able to walk? | No |
| Yes |
| Since the injury, has the participant been re-admitted to the hospital since being discharged? | No |
| Yes |
| What is the participant’s current health status after injury (self-assessment)? | Fully recovered (Ordinal value = 1) |
| Partially recovered (Ordinal value = 2) |
| The same since leaving the hospital (Ordinal value = 3) |
| Worse since leaving the hospital (Ordinal value = 4) |
| Since the injury, has the participant returned to work? | No |
| Yes |
| Did not work prior to injury |
| Since the injury, has the participant returned to school? | No |
| Yes |
| Did not attend school prior to injury |
| Since the injury, how many days (in the past 30 days) were you totally unable to carry out usual activities or work? | Continuous Integer |
| Excluding above days, how many days (in the past 30 days) did you reduce your usual activities or work? | Continuous Integer |
References
- Chandran, A.; Hyder, A.A.; Peek-Asa, C. The Global Burden of Unintentional Injuries and an Agenda for Progress. Epidemiol. Rev. 2010, 32, 110–120. [Google Scholar] [CrossRef] [Green Version]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Fact Sheet: Disability and Health. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/disability-and-health (accessed on 23 January 2022).
- Kirigia, J.M.; Mwabu, G.M. The Monetary Value of Disability-Adjusted-Life-Years Lost in the East African Community in 2015. Mod. Econ. 2018, 9, 1360–1377. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.C.; Byiringiro, J.C.; Ntakiyiruta, G.; Kyamanywa, P.; Irakiza, J.J.; Mvukiyehe, J.P.; Mutabazi, Z.; Vizir, J.P.; Ingabire, J.D.L.C.A.; Nshuti, S.; et al. Vital Statistics: Estimating Injury Mortality in Kigali, Rwanda. World J. Surg. 2015, 40, 6–13. [Google Scholar] [CrossRef]
- Ustun, T.B.; Kostanjesek, N.; Chatterji, S.; Rehm, J.; World Health Organization. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule (WHODAS 2.0). 2012. Available online: https://www.who.int/publications/i/item/measuring-health-and-disability-manual-for-who-disability-assessment-schedule-(-whodas-2.0) (accessed on 23 January 2022).
- Endsley, P.; Weobong, B.; Nadkarni, A. The psychometric properties of GHQ for detecting common mental disorder among community dwelling men in Goa, India. Asian J. Psychiatry 2017, 28, 106–110. [Google Scholar] [CrossRef]
- Hagaman, A.; Gallis, J.; Bhalotra, S.; Baranov, V.; Turner, E.L.; Sikander, S.; Maselko, J. Psychosocial determinants of sustained maternal functional impairment: Longitudinal findings from a pregnancy-birth cohort study in rural Pakistan. PLoS ONE 2019, 14, e0225163. [Google Scholar] [CrossRef]
- Jordans, M.; Rathod, S.; Fekadu, A.; Medhin, G.; Kigozi, F.; Kohrt, B.; Luitel, N.; Petersen, I.; Shidhaye, R.; Ssebunnya, J.; et al. Suicidal ideation and behaviour among community and health care seeking populations in five low- and middle-income countries: A cross-sectional study. Epidemiol. Psychiatr. Sci. 2017, 27, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Jordans, M.J.D.; Luitel, N.P.; Garman, E.; Kohrt, B.A.; Rathod, S.D.; Shrestha, P.; Komproe, I.H.; Lund, C.; Patel, V. Effectiveness of psychological treatments for depression and alcohol use disorder delivered by community-based counsellors: Two pragmatic randomised controlled trials within primary healthcare in Nepal. Br. J. Psychiatry 2019, 215, 485–493. [Google Scholar] [CrossRef] [Green Version]
- Federici, S.; Bracalenti, M.; Meloni, F.; Luciano, J.V. World Health Organization disability assessment schedule 2.0: An international systematic review. Disabil. Rehabil. 2017, 39, 2347–2380. [Google Scholar] [CrossRef] [PubMed]
- Denu, Z.A.; Yassin, M.O.; Azale, T.; Biks, G.A.; Gelaye, K.A. Do deaths from road traffic injuries follow a classical trimodal pattern in North West Ethiopia? A hospital-based prospective cohort study. BMJ Open 2021, 11, e051017. [Google Scholar] [CrossRef]
- Hendriks, T.; Botman, M.; de Haas, L.; Mtui, G.; Nuwass, E.; Jaspers, M.; Niemeijer, A.; Nieuwenhuis, M.; Winters, H.; van Zuijlen, P. Burn scar contracture release surgery effectively improves functional range of motion, disability and quality of life: A pre/post cohort study with long-term follow-up in a Low- and Middle-Income Country. Burns 2021, 47, 1285–1294. [Google Scholar] [CrossRef]
- White, M.C.; Randall, K.; Alcorn, D.; Greenland, R.; Glasgo, C.; Shrime, M.G. Measurement of patient reported disability using WHODAS 2.0 before and after surgical intervention in Madagascar. BMC Health Serv. Res. 2018, 18, 305. [Google Scholar] [CrossRef]
- Hamid, L.N.; Kobusingye, O.; Baine, S.O.; Mayora, C.; Bentley, J.A.; Chrispus, M. Disability Characteristics of Community-Based Rehabilitation Participants in Kayunga District, Uganda. Ann. Glob. Health 2017, 83, 478–488. [Google Scholar] [CrossRef] [Green Version]
- Scorza, P.; Stevenson, A.; Canino, G.; Mushashi, C.; Kanyanganzi, F.; Munyanah, M.; Betancourt, T. Validation of the “World Health Organization Disability Assessment Schedule for Children, WHODAS-Child” in Rwanda. PLoS ONE 2013, 8, e57725. [Google Scholar] [CrossRef] [Green Version]
- Odland, M.L.; Whitaker, J.; Nepogodiev, D.; Aling, C.A.; Bagahirwa, I.; Dushime, T.; Erlangga, D.; Mpirimbanyi, C.; Muneza, S.; Nkeshimana, M.; et al. Identifying, Prioritizing and Visually Mapping Barriers to Injury Care in Rwanda: A Multi-disciplinary Stakeholder Exercise. World J. Surg. 2020, 44, 2903–2918. [Google Scholar] [CrossRef]
- Galli, T.; Mirata, P.; Foglia, E.; Croce, D.; Porazzi, E.; Ferrario, L.; Ricci, E.; Garagiola, E.; Pagani, R.; Banfi, G. A comparison between WHODAS 2.0 and Modified Barthel Index: Which tool is more suitable for assessing the disability and the recovery rate in orthopedic rehabilitation? Clin. Outcomes Res. CEOR 2018, 5, 301–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent-Onabajo, G.; Joseph, E.; Musa, H.Y. Impact of balance on functional independence after stroke: A cross-sectional study at rehabilitation settings in Nigeria. NeuroRehabilitation 2018, 42, 499–504. [Google Scholar] [CrossRef]
- Hartley, T.; Burger, M.; Esterhuizen, T.M.; Inglis-Jassiem, G. Functional outcome of stroke inpatients according to human immunodeficiency virus status: A feasibility study. Afr. J. Disabil. 2020, 9, 9. [Google Scholar] [CrossRef] [Green Version]
- Katz, S. Assessing Self-maintenance: Activities of Daily Living, Mobility, and Instrumental Activities of Daily Living. J. Am. Geriatr. Soc. 1983, 31, 721–727. [Google Scholar] [CrossRef]
- Wallace, M.; Shelkey, M. Katz Index of Independence in Activities of Daily Living (ADL). Urol. Nurs. 2008, 108, 5. [Google Scholar]
- Mlinac, M.E.; Feng, M.C. Assessment of Activities of Daily Living, Self-Care, and Independence. Arch. Clin. Neuropsychol. 2016, 31, 506–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shulman, M.A.; Myles, P.S.; Chan, M.T.V.; McIlroy, D.R.; Wallace, S.; Ponsford, J. Measurement of Disability-free Survival after Surgery. Anesthesiology 2015, 122, 524–536. [Google Scholar] [CrossRef] [PubMed]
- Uwamahoro, C.; Marques, C.G.; Beeman, A.; Mutabazi, Z.; Twagirumukiza, F.R.; Jing, L.; Ndebwanimana, V.; Uwamahoro, D.; Nkeshimana, M.; Tang, O.Y.; et al. Injury burdens and care delivery in relation to the COVID-19 pandemic in Kigali, Rwanda: A prospective interrupted cross-sectional study. Afr. J. Emerg. Med. 2021, 11, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Akay, S.; Ozturk, A.M.; Akay, H. Comparison of modified Kampala trauma score with trauma mortality prediction model and trauma-injury severity score: A National Trauma Data Bank Study. Am. J. Emerg. Med. 2017, 35, 1056–1059. [Google Scholar] [CrossRef]
- Gardner, A.; Forson, P.K.; Oduro, G.; Stewart, B.; Dike, N.; Glover, P.; Maio, R.F. Diagnostic accuracy of the Kampala Trauma Score using estimated Abbreviated Injury Scale scores and physician opinion. Injury 2017, 48, 177–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mowafi, H.; Rice, B.; Nambaziira, R.; Nirere, G.; Wongoda, R.; James, M.; GECC Writing Group; Bisanzo, M.; Post, L. Household economic impact of road traffic injury versus routine emergencies in a low-income country. Injury 2021, 52, 2657–2664. [Google Scholar] [CrossRef]
- Haas, J.S.; Teixeira, C.; Cabral, C.R.; Fleig, A.H.D.; Freitas, A.P.R.; Treptow, E.C.; Rizzotto, M.I.; Machado, A.S.; Balzano, P.C.; Hetzel, M.P.; et al. Factors influencing physical functional status in intensive care unit survivors two years after discharge. BMC Anesthesiol. 2013, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Vesz, P.S.; Cremonese, R.V.; Rosa, R.; Maccari, J.G.; Teixeira, C. Impact of mechanical ventilation on quality of life and functional status after ICU discharge: A cross-sectional study. Rev. Assoc. Méd. Bras. 2018, 64, 47–53. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Plan for the Decade of Action for Road Safety 2011–2020; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Peden, M.M.; Puvanachandra, P. Looking back on 10 years of global road safety. Int. Health 2019, 11, 327–330. [Google Scholar] [CrossRef] [Green Version]
- Krebs, E.; Gerardo, C.J.; Park, L.P.; Vissoci, J.R.N.; Byiringiro, J.C.; Byiringiro, F.; Rulisa, S.; Staton, C.A.; Thielman, N.M. Mortality-Associated Characteristics of Patients with Traumatic Brain Injury at the University Teaching Hospital of Kigali, Rwanda. World Neurosurg. 2017, 102, 571–582. [Google Scholar] [CrossRef]
- Nickenig Vissoci, J.R.; Krebs, E.; Meier, B.; Vieira, I.F.; de Andrade, L.; Byiringiro, F.; Rulisa, S.; Staton, C.A. Road traffic crash experience among commercial motorcyclists in Kigali, Rwanda. Int. J. Inj. Control. Saf. Promot. 2020, 27, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Road Traffic Injuries. World Health Organization; 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/road-traffic-injuries (accessed on 20 December 2021).
- Rehabilitation 2030: A Call for Action. 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/331210/WHO-NMH-NVI-17.1-eng.pdf (accessed on 12 June 2022).
- Kinyanjui, B. Traumatic Brain Injury in Kenya: A Preliminary Review of the Literature. SAGE Open 2016, 6, 2158244016638392. [Google Scholar] [CrossRef] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 
{kind=link}
