1. Introduction
Condylar hyperplasia (CH, UCH) is a rare pathology related to the mandibular condyle. It is a self-limiting pathology without any clear etiology. Its progression can manifest in time and cause various forms of dentoalveolar and skeletal discrepancies if atypical progressive pathological growth is present. There are few known methods of classification. The first hyperplasias were described by Obwegeser as HH, HE, and rare mix-form HH-HE, followed further by the classification of CH (1–4) by Wolford [
1,
2]. Those related to primary condyle head tumors such as osteochondromas or others are quite less common. According to Obwegeser and Makek, in radiological assessments increased vertical height of the mandibular ramus or neck elongation are quite common symptoms of hemimandibular hyperplasia and elongation (HH, HE) [
1,
2,
3,
4]. Quite often (HH) is related to an atypical, abnormal self-limiting condyle growth factor with mandibular body overgrowth and asymmetry, while (HE) affects the condyle neck and is the most common asymmetry. A study by Wolford et al. described the condyle head shape, size, and enlargement variations with osteophytic formation visible on a panoramic radiograph, the occurrence of which should identify condylar hyperplasia or perhaps a benign or malignant bone-related pathology [
2,
4,
5,
6]. Some typical, atypical, and rare radiological symptoms found on routine panoramic radiographs should be reviewed and updated, and the presented paper is one of few known attempts on this topic.
An easy and accurate first step in any mandibular asymmetry evaluation is based on a routine radiograph. For an experienced clinician, some characteristic facial appearance followed by radiological features is sufficient enough to establish an accurate diagnosis. The degree of asymmetry and visible radiological features might vary. Nitzan et al. indicated that transverse asymmetry predominated in their study (52%), while a study by Alyamani and Abuzinada indicated that mandibular asymmetry might have various intensities not always corresponding with radiological data [
3,
4].
Some studies emphasize condylar hyperplasia is more often found in females, and slightly more present in the left condyle, while others estimate its occurrence quite equal without any predominant side. Alyamani and Abuzinada described 18 cases, where 15 were females [
4]. On the other hand, other authors also indicate slight female predominance [
5,
6,
7,
8,
9,
10,
11,
12,
13]. Etiological factors remain unknown, but many are taken into consideration, especially endocrinal and trauma followed by other factors such as genetic, hereditary, or perhaps even iatrogenic once in the close proximity of the joint [
5,
6,
7,
8]. Perhaps, other factors might be related to geographical regions and other possible individually driven factors. Nevertheless, occurrence age ranges from early childhood to fully grown adults, estimated at 11–35 years of age. Some reports might also describe older cases of patients (>40 years of age); however, most commonly during the time, the pathological growth has its tendency to reduce on its own. If growth is still present, then SPECT-CT evaluation might result in the necessity of a surgical intervention, namely one of the types of condylectomy, to remove the pathological growth within the joint. If radiological features of asymmetry are troublesome in full evaluation, a SPECT-CT evaluation of pathological bone growth is sensitive enough (86%) to confirm the diagnosis, which correlates with the study of Nolte et al. and others [
11,
13,
14]. SPECT-CT could have also a great amount of false positive results, which should be taken into consideration, and the study itself should be repeated in time [
8,
13,
15]. When pathological growth is present, a condylectomy procedure is scheduled. Its scope and involvement in TMJ muscles, disc, or other structures depend on many factors, especially surgeons’ preferences and the individuality of each case [
3,
4,
5,
13,
16].
Clinically, mandibular asymmetry might consist of simultaneously occurring maxillary asymmetry with horizontal plane deviation, which greatly depends on the condyle growth component. Quite commonly, HH is more frequent in one condyle, while HE mostly affects both sides with visible mandibular prognathism with laterognathia and asymmetry. Some mixed types (HH+HE) or a combination of both might also occur. Occurrence of skeletal class III is most common. Quite often, skeletal and dental features include asymmetrical angle skeletal class III malocclusion, which corresponds with other studies such as that by López et al. or Vernucci et al. [
8,
14,
16]. Clinically, a one-sided shifting chin is followed by overgrowth of the mandibular basis on the affected side, which also includes soft tissue changes in disproportion and asymmetry in mouth angle position and lip visualization. Inclined lower anterior teeth towards overgrowth are characteristic in hemimandibular hyperplasia. The dentoalveolar discrepancies remain mostly individual, but characteristic open bite in the anterior and premolar teeth is quite common. In lots of cases, the volume of bone overgrowth and the variety of asymmetry levels vary, because of patients’ age, growth component ratio, that they underwent orthodontic treatment, and the time from first symptoms to first accurate treatment [
6,
7,
8,
12,
17].
Most cases of asymmetry require first basic diagnostic steps which require a routine panoramic radiograph (panx) and lateral cephalograph (ceph). In cases of mandibular asymmetry, a diagnostic CBCT-3D and low-dose CT followed by SPECT examinations are quite good enough to establish any possible abnormal condyle growth. In some cases, SPECT and low-dose CT examinations are repeated every 6 months to establish the potential abnormal condyle growth or its progression or growth cessation to establish the best possible treatment plan [
1,
3,
6,
7,
8]. Studies by Sun et al. and Berlin et al. indicate that CT is a superior diagnostic tool in UCH [
10,
15]. Increased volume of asymmetry requires good high-quality diagnostics, especially in female patients whose facial appearance and balanced profile is the most important expected result from treatment [
3,
7,
15]. The retrospective study by Liu et al. indicated that a total of 21% of patients had increased progressive condyle growth, and more female patients are suffering from UCH; however, less than half (43%) of all studied cases showed regression towards normal growth [
9,
11,
16,
17,
18,
19].
More or fewer experienced clinicians should be aware and able to estimate the possible type of mandibular asymmetry by evaluating the panoramic radiographs and set further diagnostic steps that should be performed based on the features identified on the routine radiograph. The authors would like to point out a few key anatomical and radiological factors that might improve the first glimpse of eye diagnostics [
9]. More advanced diagnostics include CT/LDCT, MR, or other imaging protocols especially used for evaluating TMJ components and facial soft tissues, which for example can be present in craniofacial microsomia according to Kaban/OMENS classifications [
7,
8,
9].
The following paper consists of the following paragraphs: (1) introduction on UCH (presented above); (2) Materials and Methods (Go Moira! explanation and table data evaluation); (3) results on mandibular typical, atypical, and non-mandibular-related features on routine panoramic radiographs; (4) Discussion (with literature review, data evaluation, description of drawback, and future perspectives); and (5) detailed conclusions and policy implications.
The aim of this retrospective study is to evaluate routine panoramic radiographs of patients treated for, diagnosed with, or consulted about various forms of mandibular asymmetry, especially condyle hyperplasia, to estimate and evaluate the most common typical and atypical radiological manifestations of this pathology and establish the role of the acronym “Go Moira!” as a good diagnostic tool for distinguishing this type of asymmetry.
2. Materials and Methods
Patients’ pre-clinical data were gathered and consisted of cases consulted, treated, and operated by the authors. A total of 150 asymmetrical jaw radiographs were evaluated. A total of 46 were evaluated carefully and later on included in the study (
Table 1). A total of 46 panoramic radiographs, with a great predominance of female radiographs, were evaluated in the RadiAnt Dicom freeware viewer app. The authors wanted to summarize and described most typical HH symptoms present on routine panoramic radiographs in their own studied material. Inclusion criteria included full radiological, scintigraphic, orthodontic, surgical data and included only the most typical asymmetrical cases. Exclusion criteria were as follows: tumors/pseudotumors of jaws and TMJ ankylosis, trauma cases of fractured mandible condyle/head, and also other joint pathologies causing mandibular asymmetries, such as arthritic-related ones.
Gathered data were evaluated in STATISTICA v.13.3 (StatSoft, Inc., Tulsa, AK, USA). Values of p < 0.005 were considered as statistically significant. ANOVA and McNemara testing were used. All of the presented radiographical and clinical data were archived and evaluated in MeshLab (version:64 bit_v1.3.3—private license) and RadiAnt Dicom Image Viewer (private license).
Retrospective analysis of gathered panoramic radiographs based on individual anatomical, topographical, and radiological features was conducted. Studies on CT and CBCT-3D were not included in order to assess the most common panoramic radiograph features and their occurrence. Since condylar hyperplasia has its own well-known radiological features, the authors emphasize the use of selected radiographic features for early and accurate diagnostics based on a routine panoramic radiograph. This approach is quite easy and fast and does not require any radiograph standardization, since it only requires the evaluation of features described herein. A detailed comparison of most typical cases of asymmetries enabled the authors to investigate the most common radiological features of HH and establish the following acronym which is helpful in early diagnostics.
The authors established their own radiograph classification based on the used acronym ”Go, Moira!”. Moira, a female name, is an Anglicization of the Irish name Máire. Since hemimandibular hyperplasia is quite more common in females, therefore Moira’s name was chosen.
The typical anatomical and radiological landmarks presented herein were carefully selected based on known literature and the authors’ experience with their treatment. The main classifications “Go Moira!” acronym stands for:
- (1)
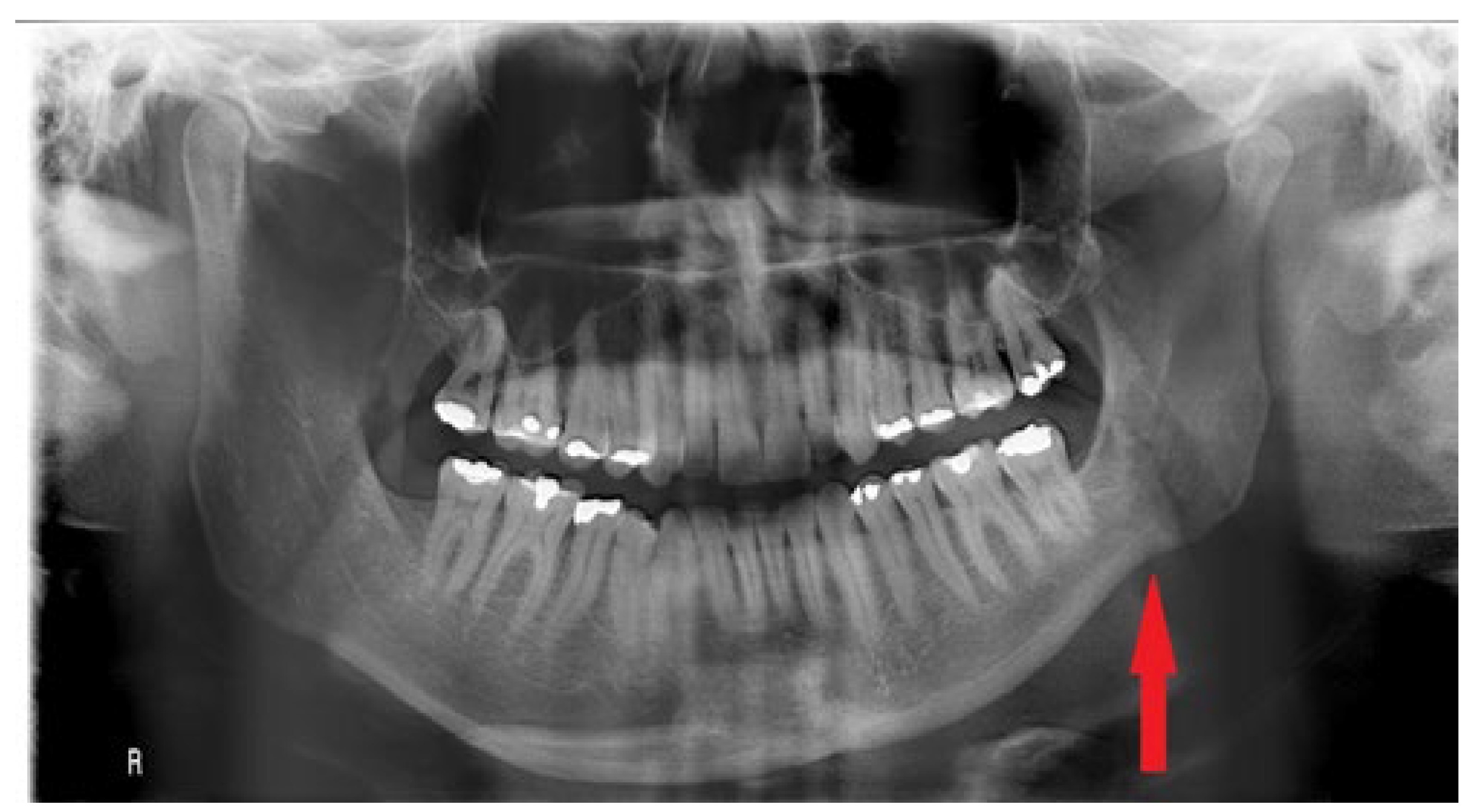
G—gonial angle, presence of antegonial notch (
Figure 1)—present on the contralateral side from the bone overgrowth in the mandible angle, manifested as angle curvature, rather than a smooth oval angle in the affected overgrowth side;
- (2)
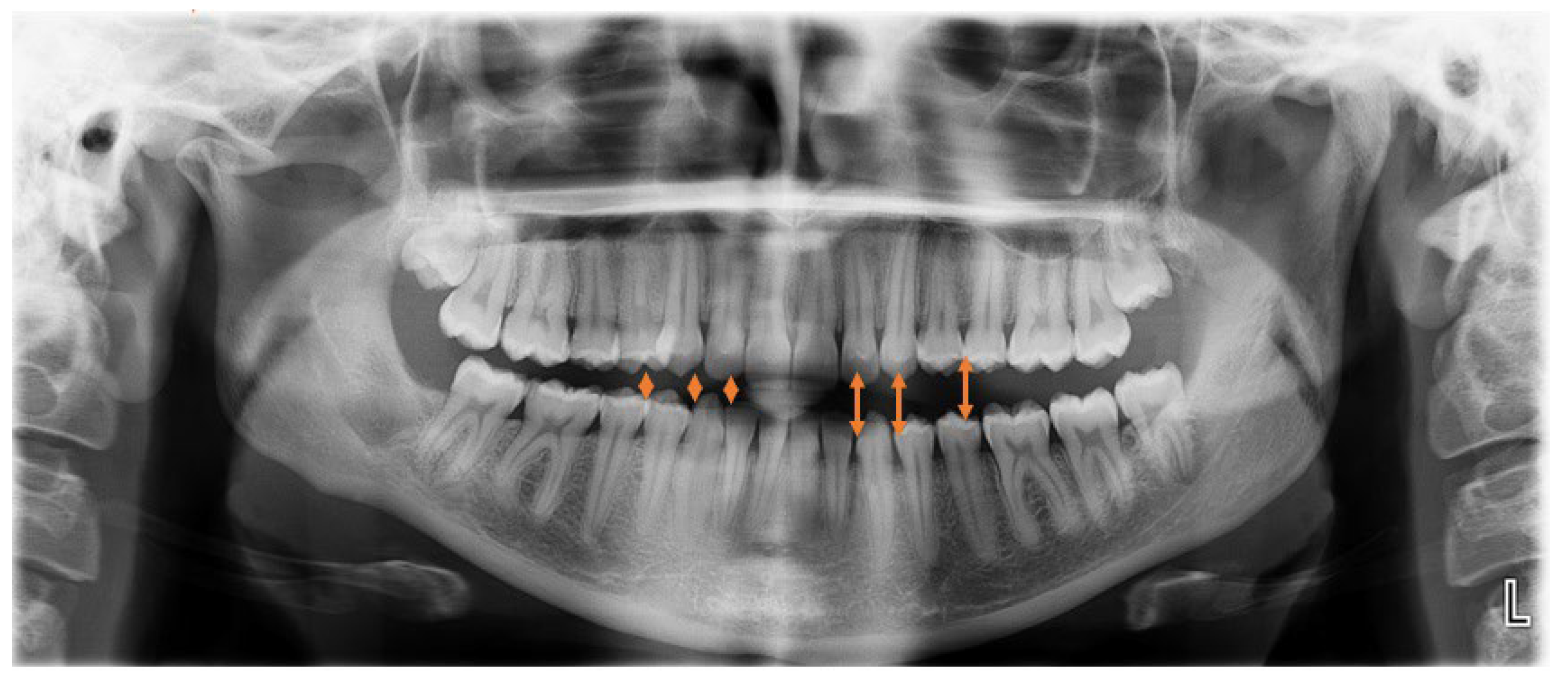
O—open bite at the canine, premolar area (
Figure 2)—visible in RTG as the enlarged distance from upper and lower dentition on the HH side;-greatly related to individual factors especially the degree and occurrence time of pathological growth;
- (3)
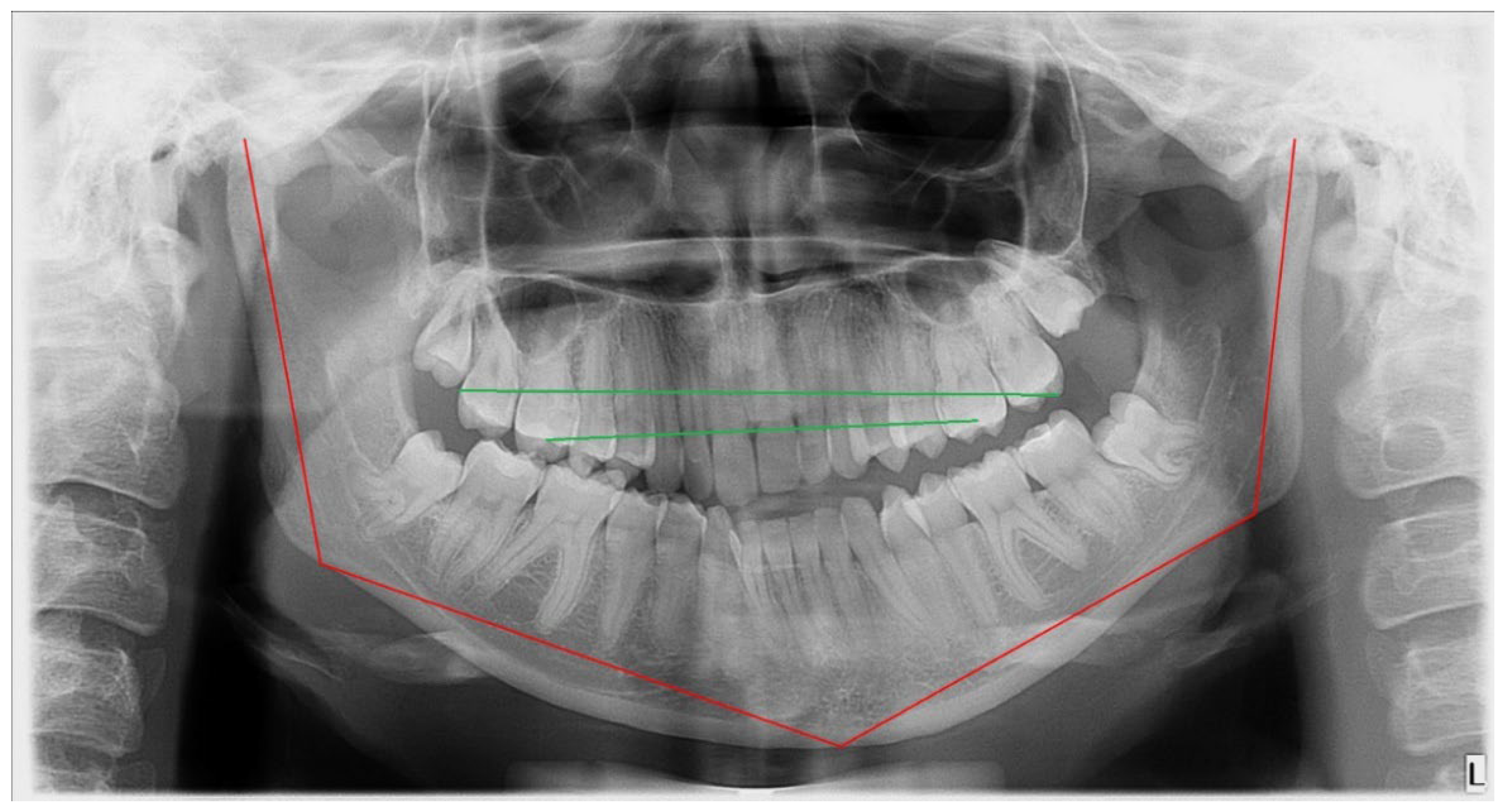
M—maxillary bones; low downward position of the maxilla on the affected side. Maxillary compensatory down growth = with or without maxillary cant deviated horizontal (transverse) occlusal plane (
Figure 3), also manifested as the asymmetrical position of part of the maxillary bone with or without sinus floor;
- (4)
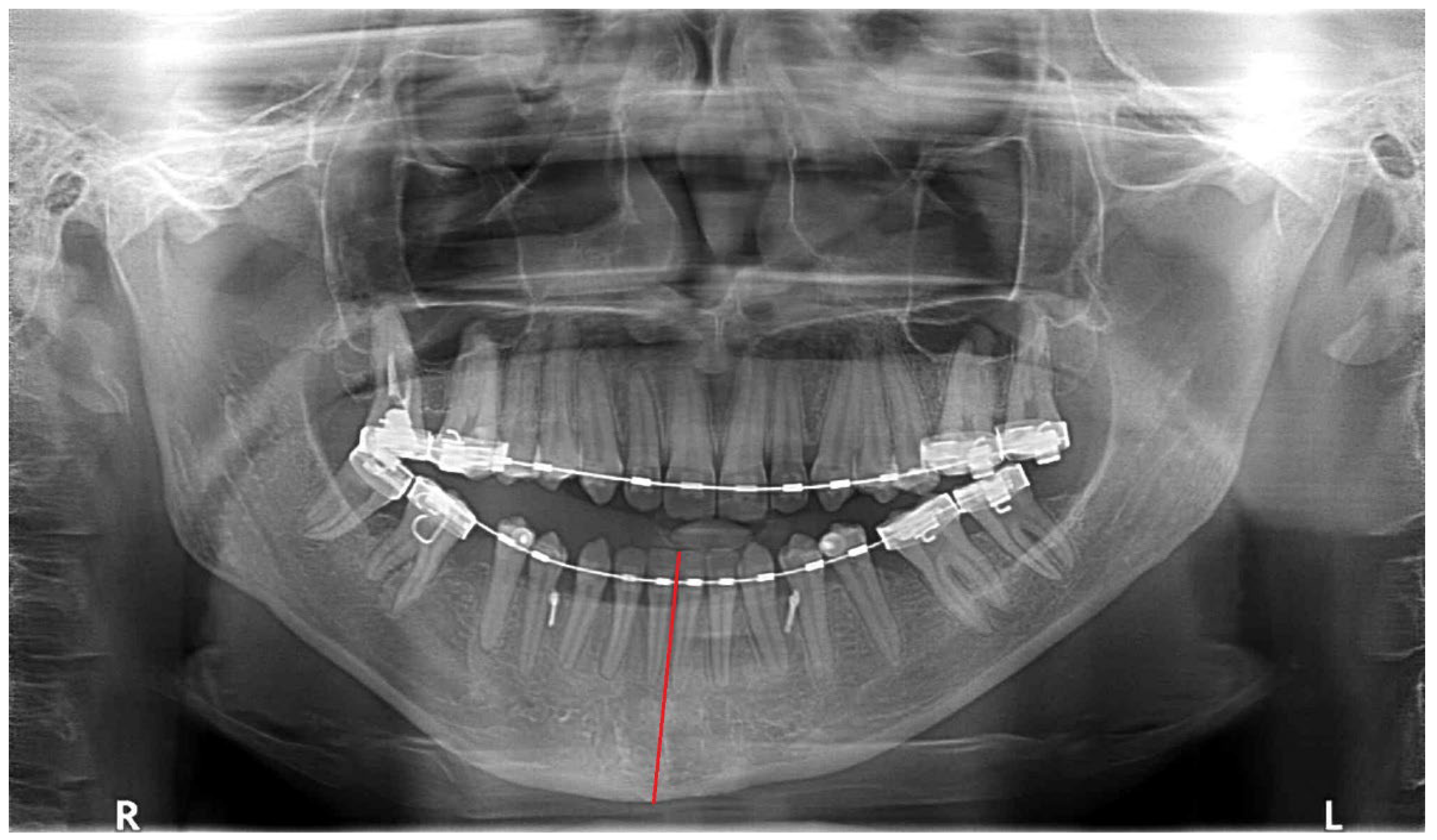
O—opposite side chin with normal position, chin shift towards the healthy side (
Figure 4), chin area shifted towards the healthy side or asymmetrically overgrown on affected side;
- (5)
I—inferior alveolar nerve, low position (
Figure 5)—typical in HH cases, mandibular canal situated inferiorly in the overgrowth mandibular body bone;
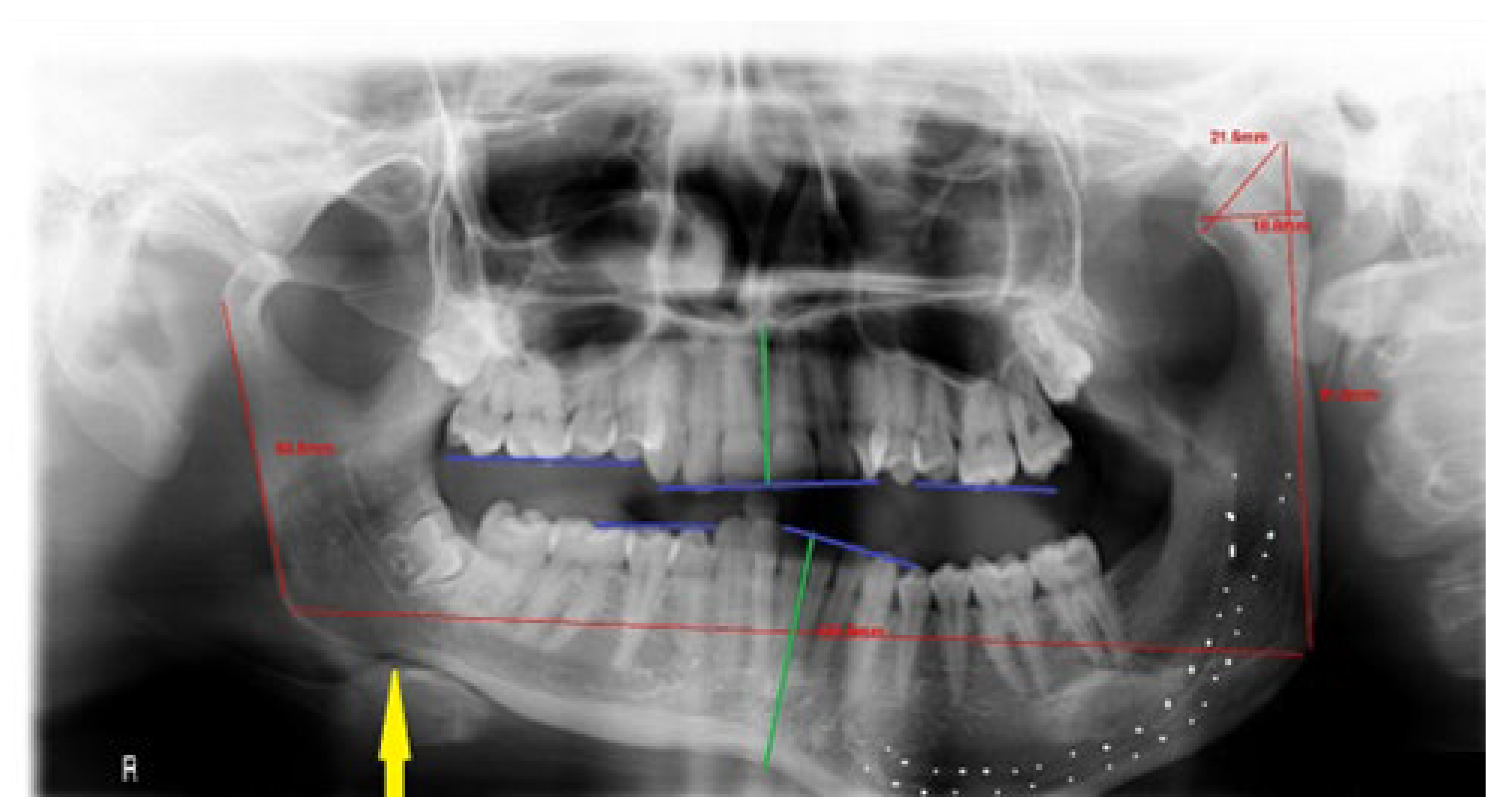
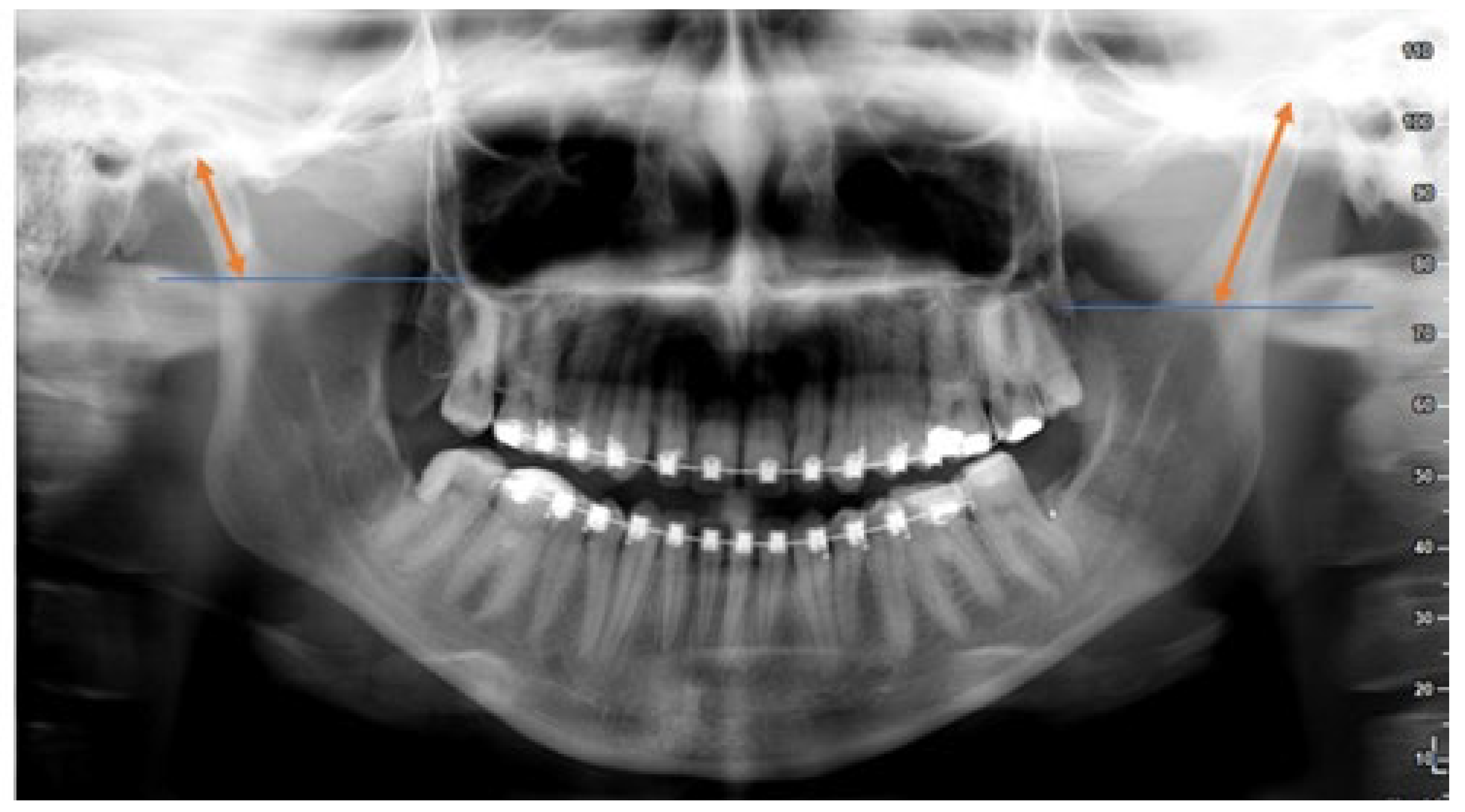
- (6)
R—ramus vertical height increased (
Figure 6)—the distance from the top of condyle head to gonial angle increased, typical for HH cases;
- (7)
A—anterior mandible = teeth midline shift towards the healthy side (
Figure 5), with or without teeth inclination’
- (8)
“!”—female to male ratio F:M = (
Figure 5) a classic female appearance of HH in panoramic radiograph with all features mentioned above.
The severity and presence of the following can be easily used to set a preliminary diagnosis just by the “first glimpse of eye” diagnostics. The amount of asymmetry and used anatomical and radiological features in the presented study should underline the possible form of condylar hyperplasia. Other forms, such as hemimandibular elongation (HE) (
Figure 7), have a decreased number of features, mostly found as an increased neck diameter or condyle elongation, which can be one or both sided, also causing mandibular prognathism with asymmetry.
3. Results
A total of 33 HH (25 F; 8 M) and 13 HE (12 F; 1 M) cases were evaluated (
Table 1). Other types of asymmetries were not included. The presented material revealed that increased vertical ramus height followed by anterior teeth midline shift was the most common effect (93.93%;
p < 0.05) in HH patients. The second most common one included open bite at the canine and premolar area followed by normal appearance of the chin on the contralateral, healthy side (87.87% vs. 81.81%;
p > 0.05). In a slow process, the teeth are able to accommodate and reach occlusion. That is why, based only on occlusion and open bite occurrence, it is quite predictable to assess the growth vector and its intensity in time. In a fast process, the teeth are unable to accommodate, and an open bite will develop. Long-standing slow progression of either HH or HE will typically have teeth in occlusion. For example, the presence/absence of an open bite is more a factor of the rate of elongation/hypertrophy. That is why, in the authors’ analyzed material, an open bite was more often found in the affected condyle related to typical HH form; however, this is not the first and only related radiological finding typical for hyperplasia.
Quite the opposite, the degree of a maxillary shift downward on the affected side and inferior alveolar nerve low position toward the mandibular basis was less common, but still present in more than 55% of all cases (p > 0.05). This finding might be related to the degree and rate of condyle growth in time. A similar result included the shape of the gonial angle, which greatly depends on the volume of bone overgrowth in time (p > 0.05). The degree of vertical ramus dimension did not correspond with the mandible body overgrowth. On the other hand, HE patients’ panoramic radiograph features mostly included anterior teeth midline asymmetry and visible chin deviation, which greatly included lateral prognathism of the mandible in various forms. The angulation of chin asymmetry is related with an increased diameter of the ramus. According to the authors’ acronym “Go Moira!”, all findings common for HH patients can be easily diagnosed. The aim of the presented acronym was to determine the existence of condylar hyperplasia and differentiate it from other mandibular asymmetry types only by a “glimpse of an eye” approach. Using it might improve clinicians’ early diagnostics; however, rare, atypical mixed forms of HH-HE or others might be troublesome. Therefore, further detailed diagnostics consisting of CT and SPECT are mandatory.
3.1. Atypical Signs
When evaluating routine panoramic radiographs, other atypical signs were also noticed. Because of the small number in the study group and a great variety of individual features of asymmetric mandible, some features were visible on a routine radiograph. Some of them might require additional clinical and radiological assessment, which might indicate their possible etiology and intensity. The rest of the features on the routine panoramic radiograph focused on HH/HE were less present and not statistically relevant (p > 0.05) features, such as:
Difference in the shape and curve of mandibular notch;
Depth and position of mandibular lingula and mandibular foramen;
Prominence and angulation of coronoid process;
Slight anterior condylar head position in the condylar fossa in affected overgrowth side;
Disruption in center condyle head position in the condylar fossa;
Posterior border of affected mandibular ramus in concave, convex, or straight shape;
Displacement of position of the mandibular foramen dislocated beyond half of the distance from height and width in affected ramus;
Decreased distance from anterior mandibular ramus on the affected side towards the mandibular lingula;
Increased distance from affected condyle head towards middle of the mandibular notch.
3.2. Other Non-Mandible-Related Factors
Other radiological factors noticed on a routine panoramic were non-mandible related. They were not evaluated in the gathered material but are worth remembering. They are especially helpful to estimate other asymmetries, such as those present in Goldenhar Syndrome and described by OMENS classifications, hemifacial microsomia (HCFM), or others. Those mentioned herein include other factors than mandibular-related ones, such as:
Position of inferior orbital rim;
Low positioned maxillary floor on the affected side;
Lack or underdeveloped anterior articular eminence;
Disrupted glenoid fossa shape;
External auditory meatus volume and presence;
Intranasal findings, such as: deviated septum, inferior nasal conchae enlargement, or anterior nares shape and width.
The typical manifestations of condylar hyperplasia mentioned herein are confirmed to be the most common ones. The atypical ones are greatly individually developed, based on the condylar growth vector and rate. The acronym “Go Moira!” seems to be a reasonable tool for a quick radiological assessment of any panoramic radiograph and distinguishing any type of condylar hyperplasia from other asymmetric pathologies within the mandible.
4. Discussion
The first look at a routine radiograph should be enough to establish some further diagnostic steps. In those cases, additional CT or SPECT will simply help to establish the type of condylar hyperplasia, its intensity, and indications for further treatment. In particular, planning for a condylectomy requires not only a routine RTG but a detailed CT-3D evaluation of the bone to estimate the degree of surgical excision.
Radiological evaluation of asymmetric mandible is quite useful. Panoramic radiograph is the first choice of imaging modality, due to that its good availability with low costs and good diagnostic performance and low dose is suitable enough for any first step diagnostics. In recent studies by Rizwana et al. and Maniskas et al., despite the superiority of CBCT/CT, a panoramic radiograph was still found to be a valuable diagnostic tool [
17,
20,
21,
22]. The evaluation of mandibular asymmetry requires some knowledge of key radiological and anatomical landmarks. Because of changes in the facial skeleton, some visible characteristic radiological signs can be easily visible on a routine radiograph. The positions, shapes, sizes, and bone anatomy later influence soft tissue expressions [
8,
17,
18,
19,
20]. Some forms of asymmetry might also manifest in facial soft tissues, the overall axial skeletal lack of balance, or even might cause some changes in the detailed facial bone architecture (eye socket or zygomatic bone underdevelopment, or others). It seems that radiographs and 2D evaluation can underline some major key characteristics of condylar hyperplasia [
1,
13,
14,
21]. When some atypical features or non-mandible-related factors occur on a routine panoramic radiograph, further radiological and clinical investigation is necessary. In addition to typical mandibular-related factors, such as a low positioned mandibular canal in the overgrowth bone and increased diameter of the vertical ramus, the condyle head can also be in various shapes, sizes, and positions among the glenoid fossa [
1,
2,
5,
9,
22]. When assessing routine panoramic radiographs features described herein are quite useful. Nevertheless, increased mandibular basis diameters with visible overgrowth and asymmetry towards the healthy side was the most common syndrome for condylar hyperplasia reported by most authors [
1,
2,
8,
10,
19,
20,
21,
22,
23]. Rare features might include joint or condylar process/head rare malignant or benign tumors, such as osteochondroma, which always require additional CT/CBCT for better differential diagnostics, as reported by Freidrich et al. [
24,
25]. Since 3D-CT is somehow a gold standard for each asymmetry evaluation, routine radiographs are also necessary for full data evaluation. Panoramic radiograph limitation does not allow full condylar head and glenoid fossa evaluation after a condylectomy, and also in some cases of asymmetry treated with surgery as a first approach more detailed and 3D data are mandatory [
8,
11,
13,
24]. On the other hand, currently 3D-CT/LDCT evaluation of both skeletal and soft tissue architecture grants more adequate diagnostics [
7,
9]. A study by Lemes et al. highlights the usage of CBCT for total horizontal and vertical measurements of overgrowth of the mandible, which is useful in surgery planning [
20]. Condylar position evaluation after a condylectomy is easily evaluated in CT/CBCT and even MRI to assess the lateral pterygoid muscle re-attachment to the new condylar bony stump in cases of condylar head re-shaping procedures [
13,
14,
15,
16,
25].
Firstly, since routine panoramic radiograph usage is somehow obsolete, and CBCT is considered a gold standard for each asymmetry evaluation, it is still worth it and recommended to perform a full radiographic evaluation of each patient. Full surgical and orthodontic data on each patient should include both radiographs and CBCT, especially in the evaluation of the presence or cessation of pathological growth in the affected condyles and the scope of skeletal overgrowths in time [
1,
2,
3,
4,
5,
9]. When condylar hyperplasia is confirmed based on their typical syndromes, other atypical features should be carefully estimated, because many surgical modalities could be used, such as a surgery-first approach, condylectomy, and orthodontics followed by late orthognathics [
7,
8,
13,
15]. Higginson et al. concluded that so far, no guidelines for the type of condylectomy, however a proportional condylectomy, should be considered regardless of the degree of overgrowth [
3,
24].
On the other hand, when some atypical or other mandible features are present on a routine panoramic radiograph more detailed radiological studies are mandatory [
1,
2,
3,
4,
5]. Differential diagnostics should include congenital (ex; genetic), acquired (trauma, tumors, developmental, inflammation), hereditary, or other factors. Study reviews by Nitzan et al. suggest that there is no detailed correlation between the radiologic findings and the clinical evaluation in UCH cases; however, in the present study the authors do not agree since most UCH cases have characteristic radiological symptoms which present themselves in different scopes in facial appearance, depending on the volume and time of the condyle hyperplastic growth [
3]. Nevertheless, most of the known articles include a basic panoramic radiograph in their study data as a valuable tool in estimating the first symptoms of UCH [
3,
5,
9,
16,
17,
18,
19,
20,
21,
22]. Each classic 2D radiograph has its limitations; however, still, each of them enables good early diagnostics which later influence the type of further scheduled radiological protocols [
15,
18,
21,
24]. In the authors’ data, the typical condylar hyperplasia syndromes noticeable on panoramic radiographs are described. They are described in various forms and intensities among published cases [
2,
7,
8,
9,
12,
20,
21,
22,
23,
24]. The most unpredictable factor remains the condylar head itself. Its growth factor and mass component greatly influence not only the type of condylectomy but also induce skeletal and dental changes among each patient [
13,
14,
15,
16]. The degree of overgrowth is individual in each case, therefore clinical and radiological assessment is mandatory.
There are some ways to evaluate and estimate mandibular and facial asymmetry. Patients’ clinical examination, followed by detailed RTG-panoramic radiograph, lateral cephalogram, computed tomography, and SPECT are useful [
4,
6,
8]. Not every mandibular asymmetry might be related to condylar hyperplasia. Features of the condylar hyperplasia might vary depending on their occurrence, intensity, and performed diagnostic procedures. In most cases, complete data consisting of clinical, radiological, CT/panx, orthodontic consult, and SPECT imaging are necessary [
12,
15,
17,
19]. An orthodontic consult is a mandatory approach, which is very helpful to establish the volume of dentoalveolar discrepancies and the scope of the open bite and anterior teeth inclination towards the affected side. Most authors describe vertical bone overgrowth with low positioned mandibular canal as a typical sign of this pathology [
1,
4,
9,
12,
15,
24]. In some cases, a mild form of asymmetry might be challenging to distinguish, especially when HH was present some time ago and caused some visible changes in the skeletal, bone, and teeth asymmetry and the condyle pathological growth can be absent. This finding is challenging, and according to the authors, first of all, SPECT and CT evaluation should estimate if the pathological growth in the condyle did really stop on its own and does not require any condylectomy or other surgical approach. If so, when the absence of pathological growth is confirmed, atypical mandibular overgrowth might be present among other various anatomical changes, related to the degree of bone activity. Some cases are not only related to the asymmetric mandible, but also the presence of an asymmetrical maxillary bone, which is quite commonly treated by orthognathic surgery in a variety of ways [
4,
5,
7,
15,
19]. On a routine panoramic radiograph, tilted maxillary occlusion and deviated plane are easy to evaluate [
10,
12,
16,
19].
Secondly, a careful examination of the mandibular body and soft tissue contour on a panoramic radiograph enables a quick look if the presented case is a hyperplasia or a tumor-like related pathology [
6,
7,
13,
15,
16,
21]. In improved diagnostics, a normal mandibular asymmetry can be confirmed and distinguished from condylar hyperplasia or joint tumors such as osteoma or osteochondroma. In addition, the presence of an enlarged condylar head with bone osteophytes and other bone formations along the condyle head might indicate the tumor-like formation. Since panoramic radiograph is just a simple diagnostic radiograph, the mandibular anatomy has major characteristics in distinguishing the type of condylar hyperplasia [
1,
2,
3,
4,
5]. An evaluation of both condyle head symmetry and bone volume followed by the vertical height of the ramus is the first diagnostic step. In the authors’ data, increased vertical ramus height did not always correspond with a low positioned mandibular canal, which is similar to other studies [
3,
7,
12,
15,
18,
21]. Furthermore, a comparison of the condyle neck and total ramus height: mandibular body dimension reveals the first data. A disruption in mentioned diameters should underline the first diagnostic steps. Sun et al. evaluated retrospective data on asymmetric mandibles and concluded that HH has some detailed characteristics which are less common in other asymmetries [
19,
21]. HE is mostly associated with an elongated condyle neck, while the rest of the features are less intense than in the classic HH form, which is commonly related to increase and overgrowth on one side of the mandible [
1,
2,
9]. The mandibular body overgrowth and its curvature with chin asymmetry seem to be the most common characteristics. On the other hand, a more complex bone analysis can be achieved in 3D-CT evaluation. In some radiological assessments, soft tissue features can be also evaluated. Further clinical examination might also include the occurrence of chin asymmetry and soft tissue discrepancies with a deviation of the facial midline noticeable in the soft tissues of lips, rima oris, the base of the nose, and philtrum, which is underlined in a study by Walters et al. [
21]. It is quite obvious that changes in the bone greatly impact the facial tissue soft tissue contour and asymmetry [
22,
23]. The presented study focused only on an easy and accessible acronym, the role of which is to quickly and accurately establish the type of asymmetry by evaluating key anatomical and radiological landmarks to easily establish the type of condylar hyperplasia, based on our own retrospective data.
Based on the results from the following panoramic radiographs, clinicians should know what radiological findings are more and less common in CH. Different relations might lead to establishing a proper diagnosis. A 2D analysis is also helpful but might have some limitations [
21]. On the other hand, it can be a useful diagnostic tool to establish important anatomical relations, such as ramus height, mandibular body overgrowth volume, and degree of maxillary canting. After gaining the following results, based on the authors’ “Go Moira!” acronym, it should be easy to investigate the type of asymmetry. Any other co-existing findings might include either vertical or horizontal bone overgrowth-related factors. It seems that not only chin asymmetry with mandibular basis overgrowth is quite inaesthetic, but also the deviation of the nose base related to condylar overgrowth. Therefore, the authors emphasize that nasal architecture plays the most important role in the facial perception of asymmetry [
10,
16].
Since CBCT/CT or PET/SPECT studies are more superior and more advanced than a routine panoramic radiograph, each panoramic radiograph has its limitations. Despite many factors including proper execution of such a radiograph, which can cause various disruptions, the main role of a panoramic radiograph is to ensure early diagnostics, which of course later should be enhanced with CT, SPECT, or other imaging tools [
5,
6,
7,
8,
9,
10,
19]. In condylar hyperplasia, each of the following vertical and horizontal bone relations is important to notice, despite the technique and quality of the radiograph. In addition, the position of clavicles and their relations with the mandibular body are helpful in establishing patients’ gender [
1,
8,
16,
20,
23]. In the authors’ data, all panoramic radiographs were sufficient enough to estimate the abovementioned main anatomical and radiological references, which greatly influence HH/HE evaluation. Regardless of their standardization, basic anatomical relations are the key to understanding selected mandibular pathologies.
The presented paper is probably one of few studies investigating routine panoramic radiographs in cases of UCH-related features. Thus far, each mandibular asymmetry with a positive SPECT result had been described as UCH. Great individuality in each case is related to the age of the UCH occurrence, growth potential, and dento-alveolar discrepancies; therefore, the authors tried to investigate typical and atypical mandibular features, as well as non-mandibular-related features found on routine panoramic radiographs, to improve early diagnostics. Major drawbacks include-: (1) cases with pathological growth cessation with a visibly asymmetric mandible as a result of the pathological growth which is no longer present; (2) trauma/inflammation cases resulting in normal condylar growth on the unaffected side and decreased normal growth on the affected side; (3) false positive SPECT results from other non-pathological growth condylar-related pathologies; and (4) missing data on possible UCH etiological factors, time of occurrence, and performed diagnostic approaches. Thus far, UCH treatment is case-based, with no detailed guidelines based on patients’ age, pathological growth factors, and present dento-alveolar discrepancies. This should be the main focus of future studies.
The main hypothesis of the authors assesses the probabilities of accurate evaluation of panoramic radiographs for the most common and typical features of asymmetric mandibles in condylar hyperplasia. The new type of approach presented based on an acronym should make it easier to indicate the presence of patients’ hemimandibular hyperplasia or elongation based on panoramic radiographs.


 ,
, 










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}