
Partial Clipping and Multilayered Wrapping Using Collagen Matrix for Partially Thrombosed Basilar Trunk Aneurysm: A Technical Case Report
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
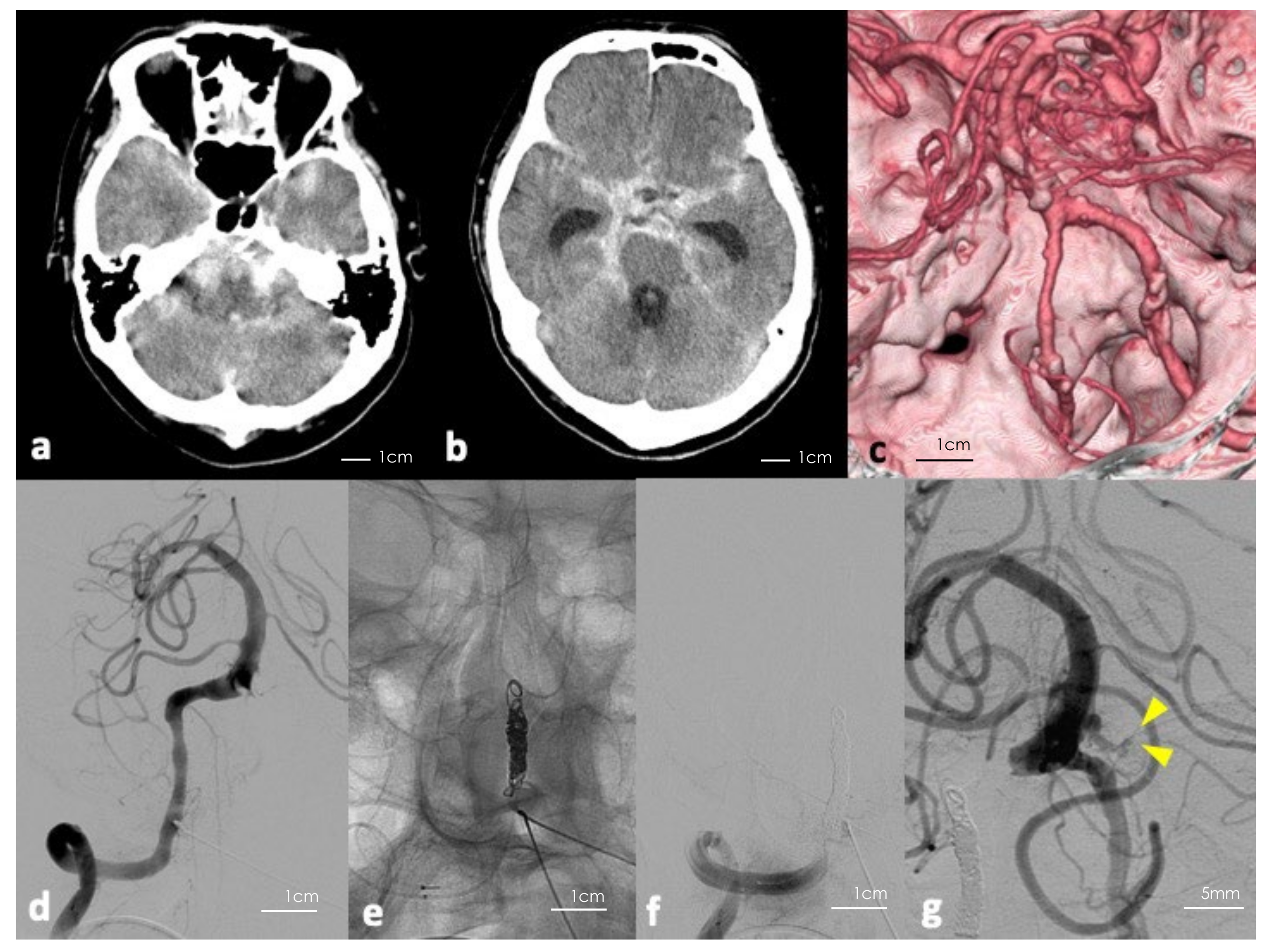
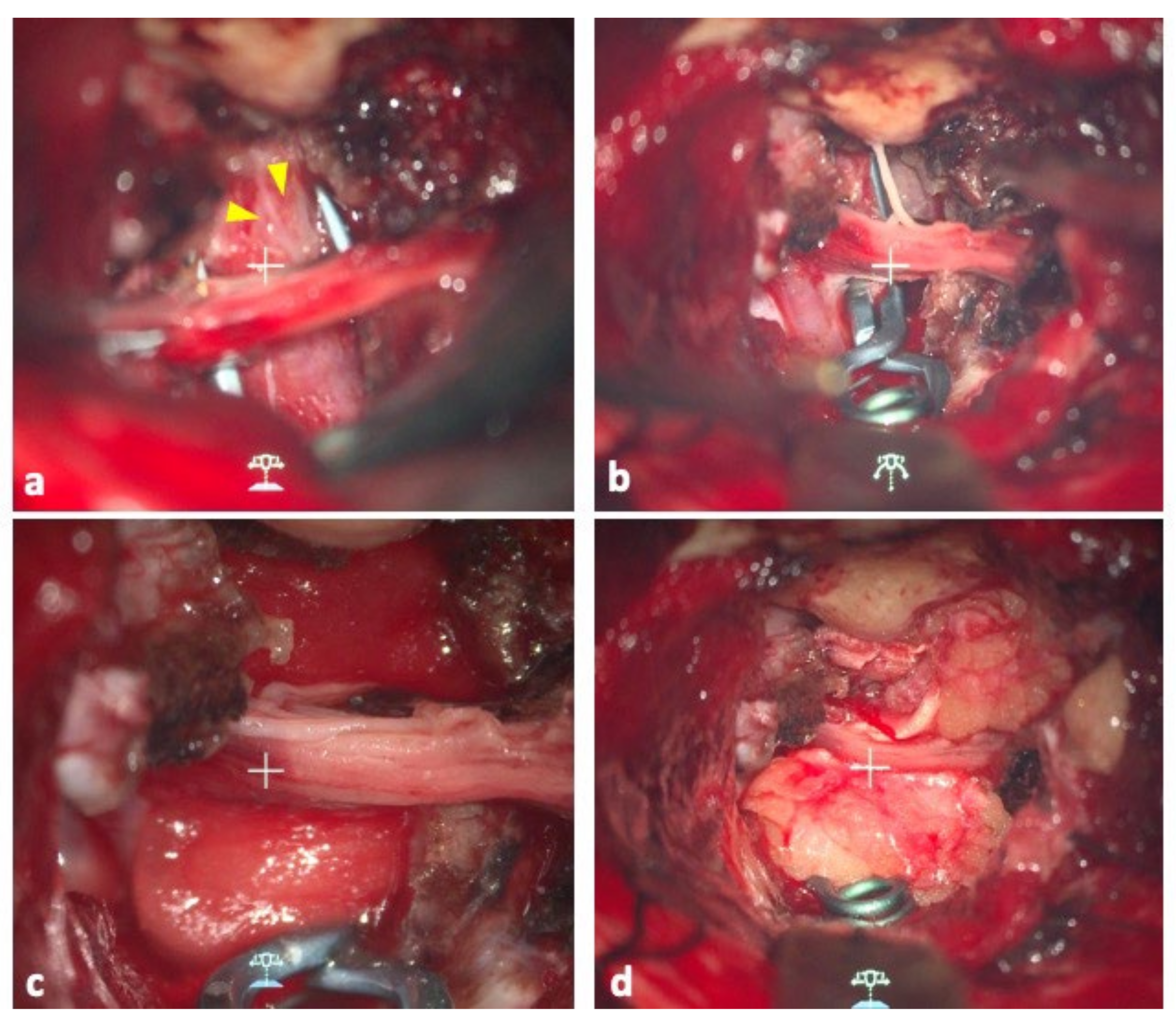
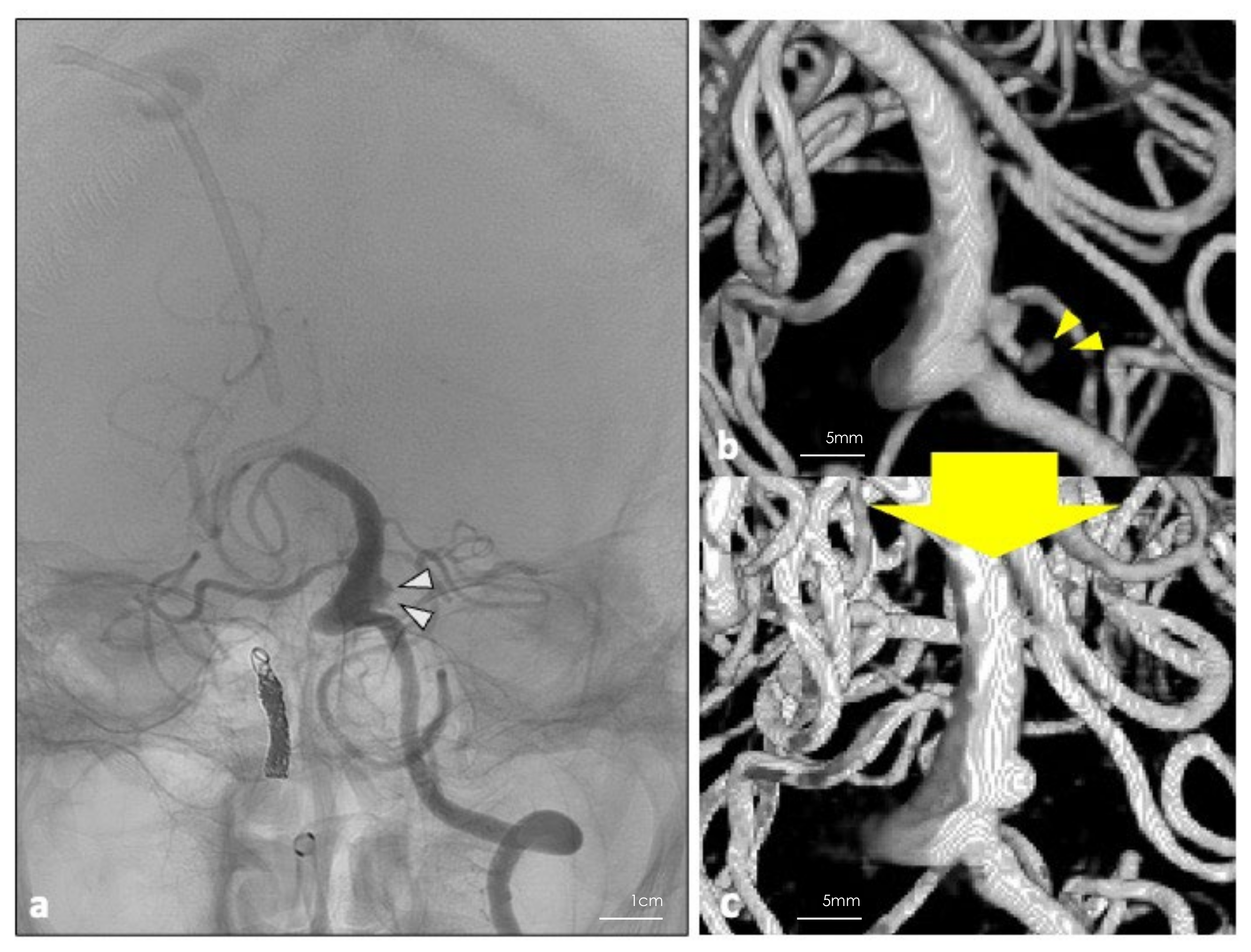
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Higa, T.; Ujiie, H.; Kato, K.; Kamiyama, H.; Hori, T. Basilar artery trunk saccular aneurysms: Morphological characteristics and management. Neurosurg. Rev. 2009, 32, 181–191, discussion 191. [Google Scholar] [CrossRef] [PubMed]
- Mizoi, K.; Yoshimoto, T.; Takahashi, A.; Ogawa, A. Direct clipping of basilar trunk aneurysms using temporary balloon occlusion. J. Neurosurg. 1994, 80, 230–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Xu, K.; Song, J.; Yu, J. Endovascular Therapy for Basilar Arterial Trunk Aneurysms. Front. Neurol. 2021, 12, 625909. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, S.; Shojima, M.; Iijima, A.; Oya, S.; Matsui, T.; Yoshikawa, G.; Tsutsumi, K.; Nakatomi, H.; Saito, N. Stent-assisted Coiling for Ruptured Basilar Artery Dissecting Aneurysms: An Initial Experience of Four Cases. Neurol. Med. Chir. 2016, 56, 43–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.-B.; Shi, W.-W.; Zhang, G.-X.; Lu, H.-C.; Ma, J. Flow diverter treatment of posterior circulation aneurysms. A meta-analysis. Neuroradiology 2016, 58, 391–400. [Google Scholar] [CrossRef] [Green Version]
- Kulcsár, Z.; Ernemann, U.; Wetzel, S.G.; Bock, A.; Goericke, S.; Panagiotopoulos, V.; Forsting, M.; Ruefenacht, D.A.; Wanke, I. High-profile flow diverter (silk) implantation in the basilar artery: Efficacy in the treatment of aneurysms and the role of the perforators. Stroke 2010, 41, 1690–1696. [Google Scholar] [CrossRef]
- Kawase, T.; Toya, S.; Shiobara, R.; Mine, T. Transpetrosal approach for aneurysms of the lower basilar artery. J. Neurosurg. 1985, 63, 857–861. [Google Scholar] [CrossRef] [Green Version]
- Saliou, G.; Sacho, R.H.; Power, S.; Kostynskyy, A.; Willinsky, R.A.; Tymianski, M.; Terbrugge, K.G.; Rawal, S.; Krings, T. Natural History and Management of Basilar Trunk Artery Aneurysms. Stroke 2015, 46, 948–953. [Google Scholar] [CrossRef] [Green Version]
- Graziano, F.; Ganau, M.; Iacopino, D.G.; Boccardi, E. Vertebro-Basilar Junction Aneurysms: A Single Centre Experience and Meta-Analysis of Endovascular Treatments. Neuroradiol. J. 2014, 27, 732–741. [Google Scholar] [CrossRef] [Green Version]
- Lauridsen, S.V.; Hvas, C.L.; Sandgaard, E.; Gyldenholm, T.; Mikkelsen, R.; Obbekjær, T.; Sunde, N.; Tønnesen, E.K.; Hvas, A.M. Thromboelastometry Shows Early Hypercoagulation in Patients with Spontaneous Subarachnoid Hemorrhage. World Neurosurg. 2019, 130, e140–e149. [Google Scholar] [CrossRef]
- Winkler, E.A.; Lee, A.; Yue, J.K.; Raygor, K.P.; Rutledge, W.C.; Rubio, R.R.; Josephson, S.A.; Berger, M.S.; Raper, D.M.S.; Abla, A.A. Endovascular embolization versus surgical clipping in a single surgeon series of basilar artery aneurysms: A complementary approach in the endovascular era. Acta Neurochir. 2021, 163, 1527–1540. [Google Scholar] [CrossRef] [PubMed]
- Ricci, G.; Ricci, A.; Gallucci, M.; Zotta, D.; Scogna, A.; Costagliola, C.; Galzio, R. Combined endovascular and microsurgical approach in the treatment of giant paraclinoid and vertebrobasilar aneurysms. J. Neurosurg. Sci. 2005, 49, 1–6. [Google Scholar] [PubMed]
- Deshmukh, V.R.; Kakarla, U.K.; Figueiredo, E.G.; Zabramski, J.M.; Spetzler, R.F. Long-term Clinical and Angiographic Follow-up of Unclippable Wrapped Intracranial Aneurysms. Neurosurgery 2006, 58, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Safavi-Abbasi, S.; Moron, F.; Sun, H.; Wilson, C.; Frock, B.; Oppenlander, M.E.; Xu, D.S.; Ghafil, C.; Zabramski, J.M.; Spetzler, R.F.; et al. Techniques and Outcomes of Gore-Tex Clip-Wrapping of Ruptured and Unruptured Cerebral Aneurysms. World Neurosurg. 2016, 90, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Pelissou-Guyotat, I.; Deruty, R.; Mottolese, C.; Amat, D. The use of Teflon as wrapping material in aneurysm surgery. Neurol. Res. 1994, 16, 224–227. [Google Scholar] [CrossRef] [PubMed]
- McFadzean, R.M.; Hadley, D.M.; McIlwaine, G.G. Optochiasmal arachnoiditis following muslin wrapping of ruptured anterior communicating artery aneurysms. J. Neurosurg. 1991, 75, 393–396. [Google Scholar] [CrossRef]
- Felsberg, G.J.; Tien, R.D.; Haplea, S.; Osumi, A.K. Muslin-induced optic arachnoiditis (“gauzoma”): Findings on CT and MR. J. Comput. Assist. Tomogr. 1993, 17, 485–487. [Google Scholar] [CrossRef]
- Prabhu, S.S.; Keogh, A.J.; Parekh, H.C.; Perera, S. Optochiasmal arachnoiditis induced by muslin wrapping of intracranial aneurysms. A report of two cases and a review of the literature. Br. J. Neurosurg. 1994, 8, 471–476. [Google Scholar] [CrossRef]
- Kirollos, R.W.; Tyagi, A.K.; Marks, P.V.; Van Hille, P.T. Muslin induced granuloma following wrapping of intracranial aneurysms: The role of infection as an additional precipitating factor. Acta Neurochir. 1997, 139, 411–415. [Google Scholar] [CrossRef]
- Brochert, A.; Reynolds, T.; Baker, R. MRI in a case of muslin-induced granuloma. Neuroradiology 2003, 45, 82–84. [Google Scholar] [CrossRef]
- Goldsberry, D.H.; Ross, I.B.; Dhillon, G.; Corbett, J.J. Visual Dysfunction Caused by Gauze Wrapping of an Intracranial Aneurysm. J. Neuro-Ophthalmol. 2004, 24, 42–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.W.; Binning, M.J.; Shanmugam, V.K.; Schmidt, R.H.; Couldwell, W.T.; Meyer, M.; Cupps, T.; Douglas, A.; McGrail, K. Muslin-induced intracranial vasculopathic stenosis: A report of two cases. Clin. Neurol. Neurosurg. 2012, 114, 63–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamura, R.; Kuranari, Y.; Orikasa, H.; Katayama, M. Meningioma Cell Invasion into DuraGen-Derived Dura Mater: A Case Report. Medicines 2022, 9, 30. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sayanagi, T.; Kuranari, Y.; Katayama, M.; Tamura, R. Partial Clipping and Multilayered Wrapping Using Collagen Matrix for Partially Thrombosed Basilar Trunk Aneurysm: A Technical Case Report. Surgeries 2022, 3, 357-363. https://doi.org/10.3390/surgeries3040038
Sayanagi T, Kuranari Y, Katayama M, Tamura R. Partial Clipping and Multilayered Wrapping Using Collagen Matrix for Partially Thrombosed Basilar Trunk Aneurysm: A Technical Case Report. Surgeries. 2022; 3(4):357-363. https://doi.org/10.3390/surgeries3040038
Chicago/Turabian StyleSayanagi, Taichi, Yuki Kuranari, Makoto Katayama, and Ryota Tamura. 2022. "Partial Clipping and Multilayered Wrapping Using Collagen Matrix for Partially Thrombosed Basilar Trunk Aneurysm: A Technical Case Report" Surgeries 3, no. 4: 357-363. https://doi.org/10.3390/surgeries3040038