


Mental Health and Quality of Life among University Students with Disabilities: The Moderating Role of Religiosity and Social Connectedness

 ,
,  , and
, and
Abstract
:1. Introduction
2. Literature Review
2.1. Depression and the QOL
2.2. Anxiety and the QOL
2.3. Stress and the QOL
2.4. The Moderated Role of Religiosity and Social Connectedness
3. Materials and Methods
3.1. Dealing with Missing Value, CMV, and Non-Response Bias
3.2. Model Evaluation
4. Results
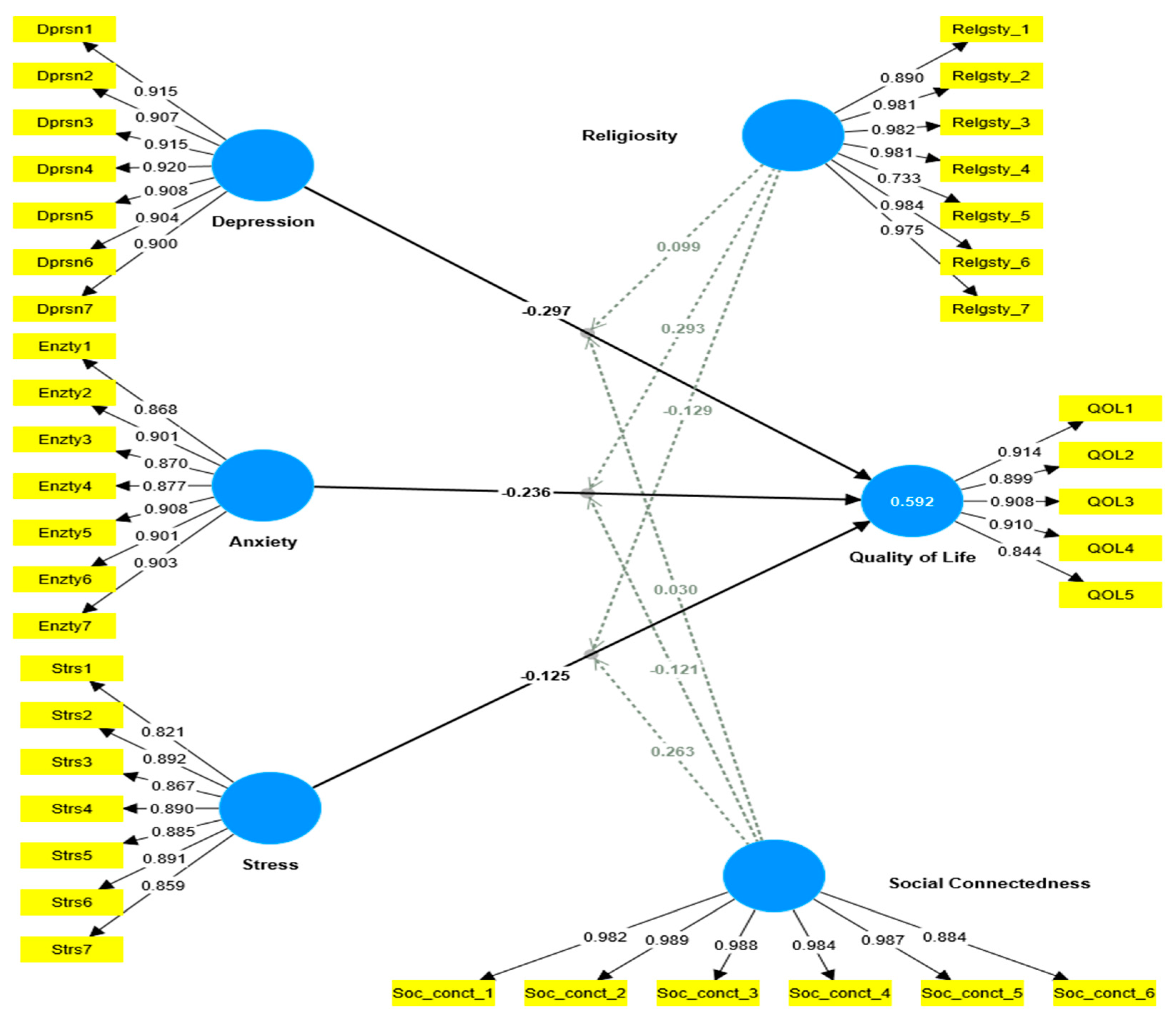
4.1. Outer Model Estimation
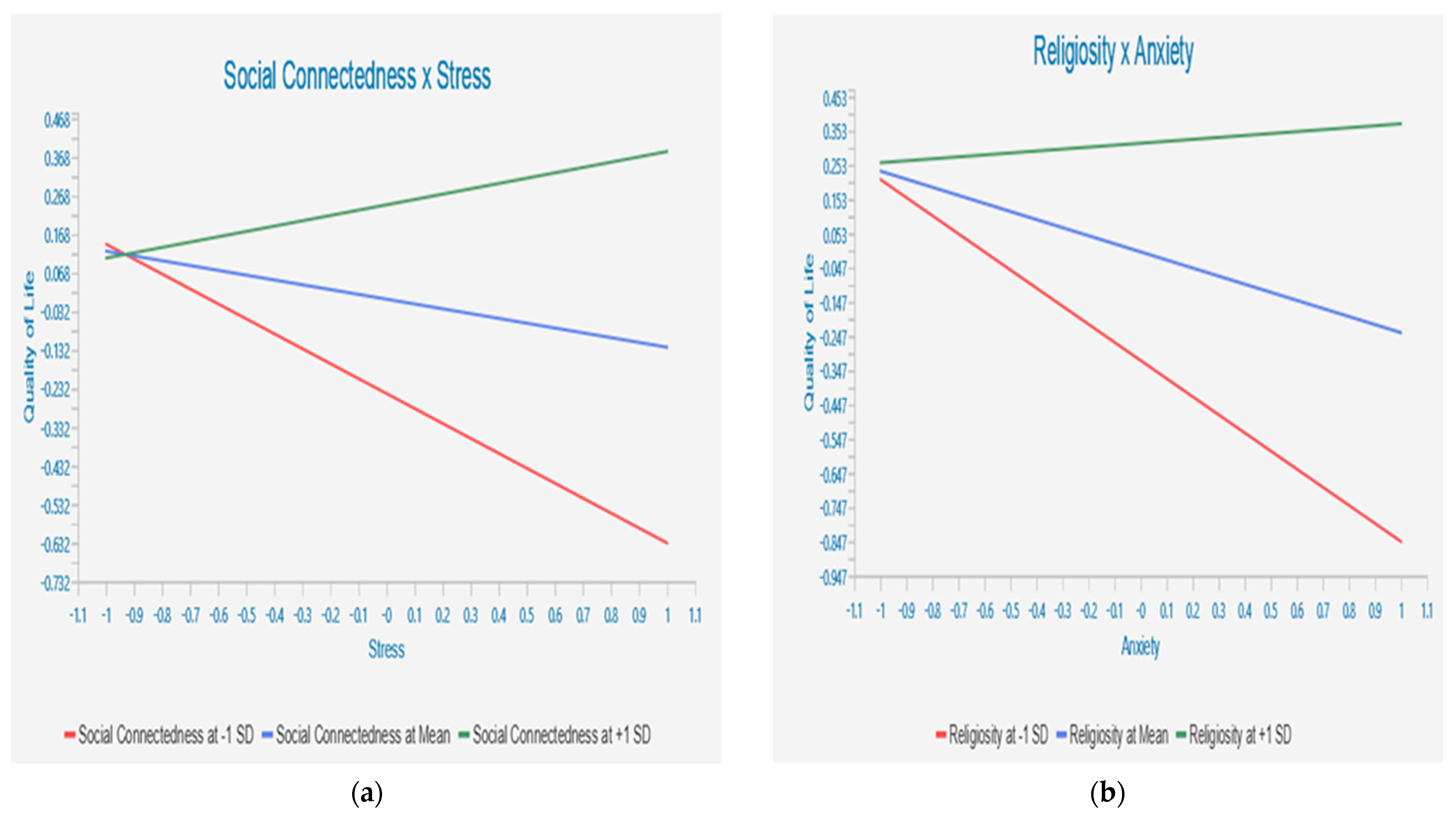
4.2. Structural (Inner) Model and Hypotheses Testing
5. Discussion and Conclusions
6. Limitations and Further Study Opportunities
7. Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Howden-Chapman, P.; Siri, J.; Chisholm, E.; Chapman, R.; Doll, C.N.; Capon, A. SDG 3: Ensure Healthy Lives and Promote Wellbeing for All at All Ages; A Guide to SDG Interactions: From Science to Implementation; International Council for Science: Paris, France, 2017; pp. 81–126. [Google Scholar]
- Leontopoulou, S. Aftermath of the COVID-19 pandemic: Resilience and mental health of emerging adult university students. Int. J. Environ. Res. Public Health 2023, 20, 6911. [Google Scholar] [CrossRef]
- Bantjes, J.; Kessler, M.; Lochner, C.; Breet, E.; Bawa, A.; Roos, J.; Davids, C.; Muturiki, M.; Kessler, R.C.; Stein, D.J. The mental health of university students in South Africa: Results of the National student survey. J. Affect. Disord. 2023, 321, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Thapar, A.; Eyre, O.; Patel, V.; Brent, D. Depression in young people. Lancet 2022, 400, 617–631. [Google Scholar] [CrossRef] [PubMed]
- Milsom, A.; DeWeese, M. Fostering Strengths and Supporting the Needs of Students with Disabilities. In Strengthening School Counselor Advocacy and Practice for Important Populations and Difficult Topics; IGI Global: Hershey, PA, USA, 2021; pp. 193–213. [Google Scholar]
- Perez, R.J. Disability Identities and Student Development. In Case Studies for Student Development Theory; Routledge: London, UK, 2019; pp. 89–100. [Google Scholar]
- Group, W. The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar]
- Meeks, L.M.; Mechaber, H.F.; Schroth, S.; Gupta, R.; Murray, J.F. The Student with a Psychological Disability: Rhonda Rapp, a Fourth-Year Medical Student with Depression and PTSD. In Disability as Diversity: A Case Studies Companion Guide; Springer: Cham, Switzerland, 2021; pp. 37–45. [Google Scholar]
- Fleming, A.R.; Plotner, A.J.; Oertle, K.M. College Students with Disabilities: The Relationship between Student Characteristics, the Academic Environment, and Performance. J. Postsecond. Educ. Disabil. 2017, 30, 209–221. [Google Scholar]
- Pedro, E.; Leitão, J.; Alves, H. Does the quality of academic life matter for students’ performance, loyalty and university recommendation? Appl. Res. Qual. Life 2016, 11, 293–316. [Google Scholar] [CrossRef]
- Lumley, S.; Ward, P.; Roberts, L.; Mann, J.P. Self-reported extracurricular activity, academic success, and quality of life in UK medical students. Int. J. Med. Educ. 2015, 6, 111. [Google Scholar] [CrossRef]
- O’Shea, A.; Kaplan, A. Disability identity and use of services among college students with psychiatric disabilities. Qual. Psychol. 2018, 5, 358. [Google Scholar] [CrossRef]
- Assana, S.; Laohasiriwong, W.; Rangseekajee, P. Quality of life, mental health and educational stress of high school students in the northeast of Thailand. J. Clin. Diagn. Res. JCDR 2017, 11, VC01. [Google Scholar] [CrossRef]
- Dyrbye, L.N.; Thomas, M.R.; Shanafelt, T.D. Systematic review of depression, anxiety, and other indicators of psychological distress among US and Canadian medical students. Acad. Med. 2006, 81, 354–373. [Google Scholar] [CrossRef]
- Yusoff, M.S.B.; Rahim, A.F.A.; Baba, A.A.; Ismail, S.B.; Pa, M.N.M. Prevalence and associated factors of stress, anxiety and depression among prospective medical students. Asian J. Psychiatry 2013, 6, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Yeshaw, Y.; Mossie, A. Depression, anxiety, stress, and their associated factors among Jimma University staff, Jimma, Southwest Ethiopia, 2016: A cross-sectional study. Neuropsychiatr. Dis. Treat. 2017, 13, 2803–2812. [Google Scholar] [CrossRef]
- Ramón-Arbués, E.; Gea-Caballero, V.; Granada-López, J.M.; Juárez-Vela, R.; Pellicer-García, B.; Antón-Solanas, I. The prevalence of depression, anxiety and stress and their associated factors in college students. Int. J. Environ. Res. Public Health 2020, 17, 7001. [Google Scholar] [CrossRef] [PubMed]
- Bujang, M.A.; Musa, R.; Liu, W.J.; Chew, T.F.; Lim, C.T.; Morad, Z. Depression, anxiety and stress among patients with dialysis and the association with quality of life. Asian J. Psychiatry 2015, 18, 49–52. [Google Scholar] [CrossRef]
- Papathanasiou, I.V.; Kelepouris, K.; Valari, C.; Papagiannis, D.; Tzavella, F.; Kourkouta, L.; Tsaras, K.; Fradelos, E.C. Depression, anxiety and stress among patients with hematological malignancies and the association with quality of life: A cross-sectional study. Med. Pharm. Rep. 2020, 93, 62. [Google Scholar] [CrossRef] [PubMed]
- Riddell, S.; Tinklin, T.; Wilson, A. Disabled Students in Higher Education: Perspectives on Widening Access and Changing Policy; Routledge: London, UK, 2005. [Google Scholar]
- Chernomas, W.M.; Shapiro, C. Stress, depression, and anxiety among undergraduate nursing students. Int. J. Nurs. Educ. Scholarsh. 2013, 10, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Freitas, P.H.B.d.; Meireles, A.L.; Ribeiro, I.K.d.S.; Abreu, M.N.S.; Paula, W.d.; Cardoso, C.S. Symptoms of depression, anxiety and stress in health students and impact on quality of life. Rev. Lat.-Am. Enferm. 2023, 31, e3884. [Google Scholar] [CrossRef]
- Al-Zoubi, E. Quality of life and its relationship with cognitive flexibility among higher education students. J. Educ. Soc. Res. 2020, 10, 156–167. [Google Scholar] [CrossRef]
- Fényes, H.; Pusztai, G.; Engler, Á. Gender role attitudes and religiosity among higher education students. J. Study Relig. Ideol. 2020, 19, 69–84. [Google Scholar]
- Maredpour, A. The Relationship between Religiosity and Mental Health in High School Students Using the Mediating Role of Social Support. Health Spiritual. Med. Ethics J. 2017, 4, 47. [Google Scholar]
- Dickinson, H.; Smith, C.; Yates, S.; Tani, M. The importance of social supports in education: Survey findings from students with disability and their families during COVID-19. Disabil. Soc. 2023, 38, 1304–1326. [Google Scholar] [CrossRef]
- Christiano, K.J.; Swatos, W.H., Jr.; Kivisto, P. Sociology of Religion: Contemporary Developments; Rowman & Littlefield: Lanham, MD, USA, 2015. [Google Scholar]
- Krok, D. Religiousness and social support as predictive factors for mental health outcomes. Arch. Psychiatry Psychother. 2014, 4, 65–76. [Google Scholar] [CrossRef]
- Hansson, L. Quality of life in depression and anxiety. Int. Rev. Psychiatry 2002, 14, 185–189. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV; American Psychiatric Association: Washington, DC, USA, 1994; Volume 4. [Google Scholar]
- Alsubaie, M.M.; Stain, H.J.; Webster, L.A.D.; Wadman, R. The role of sources of social support on depression and quality of life for university students. Int. J. Adolesc. Youth 2019, 24, 484–496. [Google Scholar] [CrossRef]
- James, R.; Baldwin, G.; Coates, H.; Krause, K.-L.; McInnis, C. Analysis of Equity Groups in Higher Education 1991–2002; Centre for the Study of Higher Education, The University of Melbourne: Parkville, Australia, 2004; p. 114. [Google Scholar]
- Chen, L.; Wang, L.; Qiu, X.H.; Yang, X.X.; Qiao, Z.X.; Yang, Y.J.; Liang, Y. Depression among Chinese university students: Prevalence and socio-demographic correlates. PLoS ONE 2013, 8, e58379. [Google Scholar]
- Larcombe, W.; Finch, S.; Sore, R.; Murray, C.M.; Kentish, S.; Mulder, R.A.; Lee-Stecum, P.; Baik, C.; Tokatlidis, O.; Williams, D.A. Prevalence and socio-demographic correlates of psychological distress among students at an Australian university. Stud. High. Educ. 2016, 41, 1074–1091. [Google Scholar] [CrossRef]
- Bukhari, S.R.; Afzal, F. Perceived social support predicts psychological problems among university students. Int. J. Indian Psychol. 2017, 4, 18–27. [Google Scholar]
- Yasin, M.A.S.M. The Relationship between Social Support and Psychological Problems among Students. 2010. Available online: http://umt-ir.umt.edu.my:8080/handle/123456789/4230 (accessed on 15 October 2023).
- Al-Qaisy, L.M. The relation of depression and anxiety in academic achievement among group of university students. Int. J. Psychol. Couns 2011, 3, 96–100. [Google Scholar]
- Fernandes, M.d.S.V.; Mendonca, C.R.; da Silva, T.M.V.; Noll, M. The relationship between depression and quality of life in students and the academic consequences: Protocol for a systematic review with meta-analysis. Int. J. Educ. Res. 2021, 109, 101812. [Google Scholar] [CrossRef]
- Gómez-Delgado, G.; Almaraz-Vega, E.; Ramírez-Mireles, J.E.; Gutiérrez-Paredes, M.E.; Padilla-Galindo, M.d.R. Health-related quality of life and depressive symptomatology in high school students during the lockdown period due to SARS-CoV-2. Int. J. Environ. Res. Public Health 2022, 19, 8780. [Google Scholar] [CrossRef]
- Hagell, P.; Westergren, A. The significance of importance: An evaluation of Ferrans and Powers’ quality of life index. Qual. Life Res. 2006, 15, 867–876. [Google Scholar] [CrossRef]
- Wechsler, H.; Lee, J.E.; Kuo, M.; Lee, H. College binge drinking in the 1990s: A continuing problem results of the Harvard School of Public Health 1999 College Alcohol Study. J. Am. Coll. Health 2000, 48, 199–210. [Google Scholar] [CrossRef]
- Ratnani, I.J.; Vala, A.U.; Panchal, B.N.; Tiwari, D.S.; Karambelkar, S.S.; Sojitra, M.G.; Nagori, N.N. Association of social anxiety disorder with depression and quality of life among medical undergraduate students. J. Fam. Med. Prim. Care 2017, 6, 243. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Accelerated Action for the Health of Adolescents (AA-HA!): Guidance to Support Country Implementation. 2017. Available online: https://policycommons.net/artifacts/546125/global-accelerated-action-for-the-health-of-adolescents-aa-ha/1523736/ (accessed on 15 December 2023).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Washington, DC, USA, 2013; Volume 5. [Google Scholar]
- Ansseau, M.; Dierick, M.; Buntinkx, F.; Cnockaert, P.; De Smedt, J.; Van Den Haute, M.; Vander Mijnsbrugge, D. High prevalence of mental disorders in primary care. J. Affect. Disord. 2004, 78, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Dahlin, M.; Joneborg, N.; Runeson, B. Stress and depression among medical students: A cross-sectional study. Med. Educ. 2005, 39, 594–604. [Google Scholar] [CrossRef]
- Rezaei, O.; Mokhayeri, Y.; Haroni, J.; Rastani, M.J.; Sayadnasiri, M.; Ghisvand, H.; Noroozi, M.; Armoon, B. Association between sleep quality and quality of life among students: A cross sectional study. Int. J. Adolesc. Med. Health 2017, 32, 20170111. [Google Scholar] [CrossRef]
- Berghöfer, A.; Martin, L.; Hense, S.; Weinmann, S.; Roll, S. Quality of life in patients with severe mental illness: A cross-sectional survey in an integrated outpatient health care model. Qual. Life Res. 2020, 29, 2073–2087. [Google Scholar] [CrossRef] [PubMed]
- Hancock, D.R. Effects of test anxiety and evaluative threat on students’ achievement and motivation. J. Educ. Res. 2001, 94, 284–290. [Google Scholar] [CrossRef]
- Van Hout, H.P.; Beekman, A.T.; De Beurs, E.; Comijs, H.; Van Marwijk, H.; De Haan, M.; Van Tilburg, W.; Deeg, D.J. Anxiety and the risk of death in older men and women. Br. J. Psychiatry 2004, 185, 399–404. [Google Scholar] [CrossRef]
- Eum, K.; Rice, K.G. Test anxiety, perfectionism, goal orientation, and academic performance. Anxiety Stress Coping 2011, 24, 167–178. [Google Scholar] [CrossRef]
- Machin, A.R.; Babatunde, O.; Haththotuwa, R.; Scott, I.; Blagojevic-Bucknall, M.; Corp, N.; Chew-Graham, C.A.; Hider, S.L. The association between anxiety and disease activity and quality of life in rheumatoid arthritis: A systematic review and meta-analysis. Clin. Rheumatol. 2020, 39, 1471–1482. [Google Scholar] [CrossRef] [PubMed]
- Nuriyyatiningrum, N.A.H.; Zikrinawati, K.; Lestari, P.; Madita, R. Quality of life of college students: The effects of state anxiety and academic stress with self-control as a mediator. Psikohumaniora J. Penelit. Psikol. 2023, 8, 87–102. [Google Scholar] [CrossRef]
- Wilmer, M.T.; Anderson, K.; Reynolds, M. Correlates of quality of life in anxiety disorders: Review of recent research. Curr. Psychiatry Rep. 2021, 23, 77. [Google Scholar] [CrossRef]
- Davies, E.; Read, J.; Shevlin, M. The impact of adverse childhood experiences and recent life events on anxiety and quality of life in university students. High. Educ. 2022, 84, 211–224. [Google Scholar] [CrossRef]
- Warnecke, A.J. First Semester Academic Functioning of College Students: The Role of Stressful and Traumatic Life Events. 2018. Available online: https://digitalcommons.georgiasouthern.edu/ij-sotl/vol13/iss2/8/ (accessed on 15 December 2023).
- Milošević Marković, M.; Latas, M.B.; Milovanović, S.; Poznanović, S.T.; Lazarević, M.M.; Karišik, M.J.; Đorđević, J.; Mandinić, Z.; Jovanović, S. Mental health and quality of life among dental students during COVID-19 pandemic: A cross-sectional study. Int. J. Environ. Res. Public Health 2022, 19, 14061. [Google Scholar] [CrossRef]
- Martinsen, K.D.; Neumer, S.-P.; Holen, S.; Waaktaar, T.; Sund, A.M.; Kendall, P.C. Self-reported quality of life and self-esteem in sad and anxious school children. BMC Psychol. 2016, 4, 45. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Making Every School a Health-Promoting School: Country Case Studies. 2021. Available online: https://pesquisa.bvsalud.org/portal/resource/pt/who-341909 (accessed on 15 December 2023).
- Carter, J.S.; Garber, J.; Ciesla, J.A.; Cole, D.A. Modeling relations between hassles and internalizing and externalizing symptoms in adolescents: A four-year prospective study. J. Abnorm. Psychol. 2006, 115, 428. [Google Scholar] [CrossRef]
- Reschly, A.L.; Huebner, E.S.; Appleton, J.J.; Antaramian, S. Engagement as flourishing: The contribution of positive emotions and coping to adolescents’ engagement at school and with learning. Psychol. Sch. 2008, 45, 419–431. [Google Scholar] [CrossRef]
- Ribeiro, Í.J.; Pereira, R.; Freire, I.V.; de Oliveira, B.G.; Casotti, C.A.; Boery, E.N. Stress and quality of life among university students: A systematic literature review. Health Prof. Educ. 2018, 4, 70–77. [Google Scholar] [CrossRef]
- Austin, E.J.; Saklofske, D.H.; Mastoras, S.M. Emotional intelligence, coping and exam-related stress in Canadian undergraduate students. Aust. J. Psychol. 2010, 62, 42–50. [Google Scholar] [CrossRef]
- Lin, J.-D.; Hu, J.; Yen, C.-F.; Hsu, S.-W.; Lin, L.-P.; Loh, C.-H.; Chen, M.-H.; Wu, S.-R.; Chu, C.M.; Wu, J.-L. Quality of life in caregivers of children and adolescents with intellectual disabilities: Use of WHOQOL-BREF survey. Res. Dev. Disabil. 2009, 30, 1448–1458. [Google Scholar] [CrossRef]
- Wallace, D.D.; Boynton, M.H.; Lytle, L.A. Multilevel analysis exploring the links between stress, depression, and sleep problems among two-year college students. J. Am. Coll. Health 2017, 65, 187–196. [Google Scholar] [CrossRef]
- Opoku-Acheampong, A.; Kretchy, I.A.; Acheampong, F.; Afrane, B.A.; Ashong, S.; Tamakloe, B.; Nyarko, A.K. Perceived stress and quality of life of pharmacy students in University of Ghana. BMC Res. Notes 2017, 10, 115. [Google Scholar] [CrossRef] [PubMed]
- Orines, R.D.; Dy, M.T.Q.; Huen, K.H.; Maligaya, K.N.B.; Pangan, J.M.G.; Paulino, N.D.; Racimo, K.M.Y. Stress and Avoidant Coping: Predictors of Quality of Life among Filipino Graduating Students. Eur. J. Psychol. Educ. Res. 2023, 6, 77–83. [Google Scholar]
- Henning, M.A.; Krägeloh, C.; Thompson, A.; Sisley, R.; Doherty, I.; Hawken, S.J. Religious affiliation, quality of life and academic performance: New Zealand medical students. J. Relig. Health 2015, 54, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Harlianty, R.A.; Paramastri, I. The role of religious coping as a moderator of the relationship between psychological burden and quality of life among caregiver of women with breast cancer. J. Psychol. Perspect. 2020, 2, 71–78. [Google Scholar] [CrossRef]
- Mosqueiro, B.P.; da Rocha, N.S.; de Almeida Fleck, M.P. Intrinsic religiosity, resilience, quality of life, and suicide risk in depressed inpatients. J. Affect. Disord. 2015, 179, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Joseph, R.A.; Kim, J.J.; Akers, S.W.; Turner, T.; Whorley, E.; Lumpkin, K.; Rosa, J.; McElroy, C. COVID-19 related stress, quality of life, and intrinsic religiosity among college students during the global pandemic: A cross-sectional study. Cogent Psychol. 2023, 10, 2195091. [Google Scholar] [CrossRef]
- Tempski, P.; Bellodi, P.L.; Paro, H.B.; Enns, S.C.; Martins, M.A.; Schraiber, L.B. What do medical students think about their quality of life? A qualitative study. BMC Med. Educ. 2012, 12, 106. [Google Scholar] [CrossRef]
- Panayiotou, G.; Karekla, M. Perceived social support helps, but does not buffer the negative impact of anxiety disorders on quality of life and perceived stress. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 283–294. [Google Scholar] [CrossRef]
- Nitschke, J.P.; Forbes, P.A.; Ali, N.; Cutler, J.; Apps, M.A.; Lockwood, P.L.; Lamm, C. Resilience during uncertainty? Greater social connectedness during COVID-19 lockdown is associated with reduced distress and fatigue. Br. J. Health Psychol. 2021, 26, 553–569. [Google Scholar] [CrossRef]
- Yoo-Jeong, M.; Nguyen, A.L.; Waldrop, D. Social network size and its relationship to domains of quality-of-life among older persons living with HIV. AIDS Care 2023, 35, 600–607. [Google Scholar] [CrossRef]
- Sujarwoto; Saputri, R.A.M.; Yumarni, T. Social media addiction and mental health among university students during the COVID-19 pandemic in Indonesia. Int. J. Ment. Health Addict. 2023, 21, 96–110. [Google Scholar] [CrossRef]
- Achat, H.; Kawachi, I.; Levine, S.; Berkey, C.; Coakley, E.; Colditz, G. Social networks, stress and health-related quality of life. Qual. Life Res. 1998, 7, 735–750. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.B.; McCullough, M.E.; Poll, J. Religiousness and depression: Evidence for a main effect and the moderating influence of stressful life events. Psychol. Bull. 2003, 129, 614. [Google Scholar] [CrossRef]
- Lee, M.; Nezu, A.M.; Nezu, C.M. Positive and negative religious coping, depressive symptoms, and quality of life in people with HIV. J. Behav. Med. 2014, 37, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Przepiorka, A.; Sobol-Kwapinska, M. Religiosity moderates the relationship between time perspective and life satisfaction. Personal. Individ. Differ. 2018, 134, 261–267. [Google Scholar] [CrossRef]
- Oei, T.P.; Sawang, S.; Goh, Y.W.; Mukhtar, F. Using the depression anxiety stress scale 21 (DASS-21) across cultures. Int. J. Psychol. 2013, 48, 1018–1029. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Diener, E.; Larsen, R.J.; Levine, S.; Emmons, R.A. Intensity and frequency: Dimensions underlying positive and negative affect. J. Personal. Soc. Psychol. 1985, 48, 1253. [Google Scholar] [CrossRef]
- Lombardi, A.; Gerdes, H.; Murray, C. Validating an assessment of individual actions, postsecondary, and social supports of college students with disabilities. J. Stud. Aff. Res. Pract. 2011, 48, 104–123. [Google Scholar] [CrossRef]
- Roussel, P.; Wacheux, F. Management des Ressources Humaines: Méthodes de Recherche en Sciences Humaines et Sociales. 2005. Available online: https://cir.nii.ac.jp/crid/1130000796973682688 (accessed on 15 December 2023).
- Krejcie, R.V.; Morgan, D.W. Determining sample size for research activities. Educ. Psychol. Meas. 1970, 30, 607–610. [Google Scholar] [CrossRef]
- Taherdoost, H. Sampling methods in research methodology; how to choose a sampling technique for research. How to choose a sampling technique for research (10 April 2016). Int. J. Acad. Res. Manag. (IJARM) 2016, 5, 18–27. [Google Scholar]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.-Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, S.B.; Podsakoff, P.M. Common method bias in marketing: Causes, mechanisms, and procedural remedies. J. Retail. 2012, 88, 542–555. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling. Can. Stud. Popul. 2018, 45, 188–195. [Google Scholar] [CrossRef]
- Reio, T.G., Jr. The threat of common method variance bias to theory building. Hum. Resour. Dev. Rev. 2010, 9, 405–411. [Google Scholar] [CrossRef]
- Michie, S.; Marteau, T.M. The choice to have a disabled child. Am. J. Hum. Genet. 1999, 65, 1204–1207. [Google Scholar] [CrossRef]
- Menachemi, N. Assessing response bias in a web survey at a university faculty. Eval. Res. Educ. 2011, 24, 5–15. [Google Scholar] [CrossRef]
- Gopalan, A.; Mannor, S.; Mansour, Y. Thompson sampling for complex online problems. In Proceedings of the International Conference on Machine Learning, PMLR, Beijing, China, 21–26 June 2014. [Google Scholar]
- Bowling, A. Research Methods in Health: Investigating Health and Health Services; McGraw-Hill Education (UK): London, UK, 2014. [Google Scholar]
- Ritchie, J.; Lewis, J.; Nicholls, C.M.; Ormston, R. Qualitative Research Practice: A Guide for Social Science Students and Researchers; Sage: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Lin, I.-F.; Schaeffer, N.C. Using survey participants to estimate the impact of nonparticipation. Public Opin. Q. 1995, 59, 236–258. [Google Scholar] [CrossRef]
- Gudergan, S.P.; Ringle, C.M.; Wende, S.; Will, A. Confirmatory tetrad analysis in PLS path modeling. J. Bus. Res. 2008, 61, 1238–1249. [Google Scholar] [CrossRef]
- Hair, J.F., Jr.; Matthews, L.M.; Matthews, R.L.; Sarstedt, M. PLS-SEM or CB-SEM: Updated guidelines on which method to use. Int. J. Multivar. Data Anal. 2017, 1, 107–123. [Google Scholar] [CrossRef]
- Anderson, J.C.; Gerbing, D.W. Structural equation modeling in practice: A review and recommended two-step approach. Psychol. Bull. 1988, 103, 411. [Google Scholar] [CrossRef]
- Chin, W.W. How to write up and report PLS analyses. In Handbook of Partial Least Squares: Concepts, Methods and Applications; Springer: Berlin/Heidelberg, Germany, 2009; pp. 655–690. [Google Scholar]
- Ringle, C.M.; Sarstedt, M.; Schlittgen, R. Finite mixture and genetic algorithm segmentation in partial least squares path modeling: Identification of multiple segments in complex path models. In Advances in Data Analysis, Data Handling and Business Intelligence: Proceedings of the 32nd Annual Conference of the Gesellschaft für Klassifikation eV, Joint Conference with the British Classification Society (BCS) and the Dutch/Flemish Classification Society (VOC), Helmut-Schmidt-University, Hamburg, Germany, 16–18 July 2008; Springer: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Bagozzi, R.P.; Yi, Y.; Phillips, L.W. Assessing construct validity in organizational research. Adm. Sci. Q. 1991, 36, 421–458. [Google Scholar] [CrossRef]
- Hair, J.F.; Ringle, C.M.; Sarstedt, M. PLS-SEM: Indeed a silver bullet. J. Mark. Theory Pract. 2011, 19, 139–152. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Hair, J.F.; Astrachan, C.B.; Moisescu, O.I.; Radomir, L.; Sarstedt, M.; Vaithilingam, S.; Ringle, C.M. Executing and interpreting applications of PLS-SEM: Updates for family business researchers. J. Fam. Bus. Strategy 2021, 12, 100392. [Google Scholar] [CrossRef]
- Jagpal, H.S. Multicollinearity in structural equation models with unobservable variables. J. Mark. Res. 1982, 19, 431–439. [Google Scholar] [CrossRef]
- Hair, J.; Alamer, A. Partial Least Squares Structural Equation Modeling (PLS-SEM) in second language and education research: Guidelines using an applied example. Res. Methods Appl. Linguist. 2022, 1, 100027. [Google Scholar] [CrossRef]
- Yuliana, S.; Yu, E.; Rias, Y.A.; Atikah, N.; Chang, H.J.; Tsai, H.T. Associations among disability, depression, anxiety, stress, and quality of life between stroke survivors and their family caregivers: An Actor-Partner Interdependence Model. J. Adv. Nurs. 2023, 79, 135–148. [Google Scholar] [CrossRef]
- Zile, I.; Bite, I.; Krumina, I.; Folkmanis, V.; Tzivian, L. Association between Anxiety, Quality of Life and Academic Performance of the Final-Year-Students in Latvia. Int. J. Environ. Res. Public Health 2021, 18, 5784. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.R.; Cosgrove, M.; Judd, C.; Scott, K.; Loughlin, A.M.; O’Keane, V. Mood matters: A national survey on attitudes to depression. Ir. J. Med. Sci. 2019, 188, 1317–1327. [Google Scholar] [CrossRef] [PubMed]
- Lundy, B.L.; Drouin, M. From social anxiety to interpersonal connectedness: Relationship building within face-to-face, phone and instant messaging mediums. Comput. Hum. Behav. 2016, 54, 271–277. [Google Scholar] [CrossRef]
- Schwadel, P. Individual, congregational, and denominational effects on church members’ civic participation. J. Sci. Study Relig. 2005, 44, 159–171. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Category | Group | Frequency (N = 390) | % |
|---|---|---|---|
| Gender | Male | 218 | 56.0 |
| Female | 172 | 44.0 | |
| Age group | 17–20 | 156 | 40.0 |
| 21–23 | 195 | 50.0 | |
| 24–25 | 39 | 10.0 | |
| study year | Frist year | 68 | 17.4 |
| Second year | 103 | 26.4 | |
| Third year | 177 | 45.5 | |
| Fourth year | 42 | 10.7 | |
| Disability | Physical disability | 129 | 33 |
| Visual disability | 137 | 35 | |
| Hearing disability | 66 | 17 | |
| Speech disability | 58 | 15 | |
| Academic discipline | Art | 156 | 40 |
| Education | 137 | 35 | |
| Business Administration | 58 | 15 | |
| Agricultural and Food Sciences | 39 | 10 |
| Conructs | α | CR | AVE | Loadings | T | VIF | |
|---|---|---|---|---|---|---|---|
| Mental health disorders (Lovibond and Lovibond, 1995) [82] | |||||||
| Depression | 0.965 | 0.968 | 0.828 | ||||
| X1 * | “I was unable to feel any happiness or positive emotions”. | 0.915 | 75.121 | 4.569 | |||
| X2 | “I struggled to start tasks and take initiative”. | 0.907 | 57.382 | 4.151 | |||
| X3 | “I saw no reason to be optimistic or have hope”. | 0.915 | 57.713 | 4.762 | |||
| X4 | “I felt sad and depressed”. | 0.920 | 59.265 | 4.265 | |||
| X5 | “I didn’t feel good about myself or my worth”. | 0.908 | 50.273 | 4.455 | |||
| X6 | “I was unable to get excited or passionate about anything”. | 0.904 | 49.704 | 4.182 | |||
| X7 | “I felt that life had no purpose or significance”. | 0.900 | 55.352 | 3.886 | |||
| Anxiety | 0.956 | 0.963 | 0.792 | ||||
| X8 | “I noticed my mouth was dry”. | 0.868 | 61.218 | 3.961 | |||
| X9 | “I had trouble breathing (such as rapid or shortness of breath without exertion)”. | 0.901 | 93.160 | 4.552 | |||
| X10 | “I felt shaking in my hands”. | 0.870 | 66.811 | 3.764 | |||
| X11 | “I was concerned about potentially panicking and embarrassing myself”. | 0.877 | 73.648 | 4.569 | |||
| X12 | “I felt close to a panic attack”. | 0.908 | 94.754 | 4.265 | |||
| X13 | “I felt scared without a clear reason”. | 0.901 | 75.765 | 4.003 | |||
| X14 | “I became aware of my heartbeat without any physical activity (such as feeling my heart rate increase or skipping a beat)”. | 0.903 | 96.912 | 4.268 | |||
| Stress | 0.948 | 0.960 | 0.761 | ||||
| X15 | “I had trouble calming down and relaxing”. | 0.821 | 35.456 | 2.459 | |||
| X16 | “I tended to have extreme reactions to events”. | 0.892 | 62.585 | 4.627 | |||
| X17 | “I felt I was employing a lot of nervous energy”. | 0.867 | 55.020 | 4.293 | |||
| X18 | “I became easily irritated”. | 0.890 | 65.880 | 3.983 | |||
| X19 | “I had difficulty finding relaxation”. | 0.885 | 55.035 | 3.682 | |||
| X20 | “I became easily frustrated by anything that disrupted my plans”. | 0.891 | 76.941 | 4.121 | |||
| X21 | “I felt I was easily upset or quick to anger”. | 0.859 | 48.103 | 3.573 | |||
| QOL (Diener et al., 1985) [83] | 0.938 | 0.938 | 0.802 | ||||
| Y1 | “In most ways my life is ideal”. | 0.914 | 83.180 | 4.276 | |||
| Y2 | “I am satisfied with my life”. | 0.899 | 57.046 | 3.673 | |||
| Y3 | “The conditions of my life are excellent”. | 0.908 | 76.308 | 3.929 | |||
| Y4 | “So far, I have gotten the important things I want in life”. | 0.910 | 74.371 | 3.752 | |||
| Y5 | “If I could live my life over, I would change almost nothing”. | 0.844 | 41.624 | 2.307 | |||
| Religiosity (Lombardi et al., 2011) [84] | 0.975 | 0.982 | 0.877 | ||||
| M1 | “I experience God’s presence in my life”. | 0.890 | 67.377 | 3.492 | |||
| M2 | “My faith permeates my entire existence”. | 0.981 | 221.909 | 4.203 | |||
| M3 | “I am a religious one who allows religious considerations to impact my daily life | 0.982 | 234.735 | 4.644 | |||
| M4 | “My religious beliefs are the foundation of my entire life philosophy”. | 0.981 | 232.826 | 2.112 | |||
| M5 | “Nothing is more important to me than serving God to the best of my ability”. | 0.733 | 4.365 | 1.812 | |||
| M6 | “When making important decisions, one should seek God’s guidance”. | 0.984 | 260.789 | 3.162 | |||
| M7 | “I strive to incorporate my religion into every aspect of my life”. | 0.975 | 172.363 | 2.908 | |||
| Social connectedness Alsubaie et al. [31] | 0.987 | 0.990 | 0.940 | ||||
| M8 | “I feel more comfortable when someone from my family is constantly with me”. | 0.982 | 195.092 | 2.279 | |||
| M9 | “My life is incomplete without a buddy beside me”. | 0.989 | 356.517 | 3.112 | |||
| M10 | “It’s hard for me to use my skills and talents without someone beside me”. | 0.988 | 367.445 | 3.026 | |||
| M11 | “I stick to my friends and family like glue”. | 0.984 | 219.822 | 2.303 | |||
| M12 | “I join groups more for friendship than the activity itself”. | 0.987 | 335.613 | 3.886 | |||
| M13 | “I wish to find someone who can be with me all the time” | 0.884 | 66.817 | 3.531 | |||
| I | II | III | IV | V | VI | |
|---|---|---|---|---|---|---|
| Anxiety | 0.890 | |||||
| Depression | 0.653 | 0.910 | ||||
| Quality of Life | −0.460 | −0.406 | 0.895 | |||
| Religiosity | 0.309 | 0.477 | 0.257 | 0.936 | ||
| Social Connectedness | 0.325 | 0.513 | 0.191 | 0.852 | 0.970 | |
| Stress | 0.603 | 0.339 | −0.359 | 0.103 | 0.158 | 0.873 |
| Anxiety | Depression | Quality of Life | Religiosity | Social Connectedness | Stress | ||
|---|---|---|---|---|---|---|---|
| X1 * | 0.607 | 0.915 | −0.370 | 0.448 | 0.458 | 0.341 | 0.607 |
| X2 | 0.569 | 0.907 | −0.398 | 0.443 | 0.461 | 0.290 | 0.569 |
| X3 | 0.621 | 0.915 | −0.367 | 0.419 | 0.444 | 0.326 | 0.621 |
| X4 | 0.585 | 0.920 | −0.323 | 0.466 | 0.495 | 0.300 | 0.585 |
| X5 | 0.567 | 0.908 | −0.335 | 0.447 | 0.478 | 0.263 | 0.567 |
| X6 | 0.575 | 0.904 | −0.366 | 0.393 | 0.439 | 0.292 | 0.575 |
| X7 | 0.625 | 0.900 | −0.411 | 0.426 | 0.492 | 0.337 | 0.625 |
| X8 | 0.868 | 0.559 | −0.382 | 0.232 | 0.249 | 0.456 | 0.868 |
| X9 | 0.901 | 0.595 | −0.500 | 0.203 | 0.221 | 0.525 | 0.901 |
| X10 | 0.870 | 0.571 | −0.373 | 0.360 | 0.369 | 0.528 | 0.870 |
| X11 | 0.877 | 0.571 | −0.348 | 0.325 | 0.341 | 0.555 | 0.877 |
| X12 | 0.908 | 0.620 | −0.381 | 0.359 | 0.352 | 0.572 | 0.908 |
| X13 | 0.901 | 0.565 | −0.426 | 0.239 | 0.263 | 0.528 | 0.901 |
| X14 | 0.903 | 0.587 | −0.419 | 0.246 | 0.263 | 0.596 | 0.903 |
| Y1 | −0.370 | −0.351 | 0.914 | 0.238 | 0.182 | −0.282 | −0.370 |
| Y2 | −0.405 | −0.374 | 0.899 | 0.194 | 0.169 | −0.319 | −0.405 |
| Y3 | −0.404 | −0.351 | 0.908 | 0.228 | 0.174 | −0.294 | −0.404 |
| Y4 | −0.403 | −0.384 | 0.910 | 0.220 | 0.151 | −0.295 | −0.403 |
| Y5 | −0.465 | −0.356 | 0.844 | 0.267 | 0.179 | −0.408 | −0.465 |
| M1 | 0.261 | 0.454 | 0.280 | 0.890 | 0.838 | 0.075 | 0.261 |
| M2 | 0.307 | 0.461 | 0.242 | 0.981 | 0.823 | 0.104 | 0.307 |
| M3 | 0.307 | 0.472 | 0.250 | 0.982 | 0.823 | 0.091 | 0.307 |
| M4 | 0.307 | 0.460 | 0.247 | 0.981 | 0.826 | 0.105 | 0.307 |
| M5 | 0.250 | 0.325 | 0.188 | 0.733 | 0.582 | 0.099 | 0.250 |
| M6 | 0.300 | 0.459 | 0.241 | 0.984 | 0.826 | 0.106 | 0.300 |
| M7 | 0.292 | 0.472 | 0.220 | 0.975 | 0.821 | 0.099 | 0.292 |
| M8 | 0.301 | 0.500 | 0.164 | 0.829 | 0.982 | 0.148 | 0.301 |
| M9 | 0.305 | 0.488 | 0.193 | 0.831 | 0.989 | 0.151 | 0.305 |
| M10 | 0.322 | 0.490 | 0.198 | 0.826 | 0.988 | 0.164 | 0.322 |
| M11 | 0.323 | 0.500 | 0.189 | 0.832 | 0.984 | 0.142 | 0.323 |
| M12 | 0.326 | 0.486 | 0.192 | 0.824 | 0.987 | 0.164 | 0.326 |
| M13 | 0.311 | 0.524 | 0.173 | 0.820 | 0.884 | 0.149 | 0.311 |
| X15 | 0.636 | 0.422 | −0.335 | 0.160 | 0.214 | 0.821 | 0.636 |
| X16 | 0.490 | 0.251 | −0.282 | 0.089 | 0.109 | 0.892 | 0.490 |
| X17 | 0.395 | 0.193 | −0.224 | 0.042 | 0.086 | 0.867 | 0.395 |
| X18 | 0.552 | 0.335 | −0.294 | 0.155 | 0.200 | 0.890 | 0.552 |
| X19 | 0.515 | 0.287 | −0.277 | 0.119 | 0.175 | 0.885 | 0.515 |
| X20 | 0.578 | 0.316 | −0.403 | 0.038 | 0.095 | 0.891 | 0.578 |
| X21 | 0.454 | 0.218 | −0.318 | 0.029 | 0.083 | 0.859 | 0.454 |
| Hypotheses | β | STDEV | T-Value | p | Conclusion | |
|---|---|---|---|---|---|---|
| Depression → QOL | −0.29 | 0.06 | 4.40 | 0.000 | Supporting H1 | |
| Anxiety → QOL | −0.23 | 0.076 | 3.101 | 0.002 | Supporting H2 | |
| Stress → QOL | −0.12 | 0.063 | 1.982 | 0.048 | Supporting H3 | |
| Moderating paths | ||||||
| Social Connectedness x Depression → QOL | 0.030 | 0.155 | 0.197 | 0.844 | Rejecting H4 | |
| Social Connectedness x Anxiety → QOL | −0.12 | 0.186 | 0.646 | 0.518 | Rejecting H5 | |
| Social Connectedness x Stress → QOL | 0.263 | 0.120 | 2.198 | 0.028 | Supporting H6 | |
| Religiosity x Depression → QOL | 0.099 | 0.158 | 0.628 | 0.530 | Rejecting H7 | |
| Religiosity x Anxiety → QOL | 0.293 | 0.196 | 3.496 | 0.035 | Supporting H8 | |
| Religiosity x Stress → QOL | −0.12 | 0.122 | 1.051 | 0.293 | Rejecting H9 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Shaer, E.A.; Aliedan, M.M.; Zayed, M.A.; Elrayah, M.; Moustafa, M.A. Mental Health and Quality of Life among University Students with Disabilities: The Moderating Role of Religiosity and Social Connectedness. Sustainability 2024, 16, 644. https://doi.org/10.3390/su16020644
Al-Shaer EA, Aliedan MM, Zayed MA, Elrayah M, Moustafa MA. Mental Health and Quality of Life among University Students with Disabilities: The Moderating Role of Religiosity and Social Connectedness. Sustainability. 2024; 16(2):644. https://doi.org/10.3390/su16020644
Chicago/Turabian StyleAl-Shaer, Ebrahim A., Meqbel M. Aliedan, Mohamed A. Zayed, Musaddag Elrayah, and Mohamed A. Moustafa. 2024. "Mental Health and Quality of Life among University Students with Disabilities: The Moderating Role of Religiosity and Social Connectedness" Sustainability 16, no. 2: 644. https://doi.org/10.3390/su16020644