
A New Dimension of Health Sustainability Model after Pandemic Crisis Using Structural Equation Model

1
Graduate School, University of the Thai Chamber of Commerce, 126/1 Vibhavadi Rangsit Road, Din Daeng, Bangkok 10400, Thailand
2
School of Engineering, University of the Thai Chamber of Commerce, 126/1 Vibhavadi Rangsit Road, Din Daeng, Bangkok 10400, Thailand
*
Author to whom correspondence should be addressed.
Sustainability 2023, 15(2), 1616; https://doi.org/10.3390/su15021616
Submission received: 5 October 2022
/
Revised: 7 January 2023
/
Accepted: 12 January 2023
/
Published: 13 January 2023
(This article belongs to the Special Issue Sustainable Development, Environment, and Health)
Abstract
:Since the coronavirus (COVID-19) pandemic, it has been clear that the health dimension (HEDm) has a severe impact on sustainability, which was originally considered from the pillars of society, environment and economy. Hence, the integration of the health dimension into the other three pillars is plausible to define guidelines and criteria for progress monitoring and policy assessment towards a health-sustainable city. The objective of this study aims to present The Health Sustainability Model (HSM), a four-dimensional model for health sustainability (health, economy, environment, and society), using the Del-phi method to determine potential indicators agreed by eighteen experts, including physicians who deeply understand issues on health sustainability, and assess complex dimensions of health in the context of sustainability. The researchers have found that 45 indicators, later grouped into 15 elements and 4 dimensions, have a high level of agreement with Kendall’s W (KW) at 0.36. The HSM was then examined by the structural equation model (SEM) with reliability and validity shown as follows: the absolute fit with CMIN/DF = 1.44, RMSEA = 0.033, GFI = 0.96, AGFI = 0.94, RMR = 0.025, and the incremental fit with NFI = 0.94, CFI = 0.98, TLI = 0.97, and IFI = 0.98. Based on the results, the model is valid, in line with the empirical data. For further application, the HSM is expected to support city planners and decision makers by identifying room for improvement in each dimension through the indicators employed in the model. In contrast to existing studies that mainly use qualitative data, by conducting quantitative assessment, the model enables policy makers to objectively evaluate conditions and appropriately design policies to improve residents’ well-being.
1. Introduction
Sustainable development (STD) was first introduced in the Brundtland Report in 1987. The term later came to denote a concept of sustainable development, receiving much attention globally [1]. From literature reviews, “sustainable development” has been defined by many scholars; however, the definition of sustainable development remains ambiguous because of its distinctive characteristics, [1] varying depending on the perspectives, goals, and contexts of cities [2,3]. Nonetheless, a sustainable city encompasses the two following aspects: enhancing human well-being and using ICT infrastructure in city management. The concept of STD with reference to “a development that meets the needs of the current generation without compromising the ability of future generations to meet their own needs” [4] is commonly used in three dimensions of development, society, environment, and economy [5], by primarily focusing on environmental development to reduce the impacts on society and economic growth [1,6]. Existing studies show that the three dimensions of STD are interrelated [7] and that promotion of STD activities is needed to conduct STD comprehensively, particularly in the social dimension (SODm) that interrelates with health dimension (HEDm) [8,9]. For the purpose of this study, STD means “development toward goals in consideration of the context of a city while strictly emphasizing the participation of all stakeholders and efficiently managing the effects on the health, environment, economy and society dimensions to achieve a new normal”. The definition used in the manuscript is consistent with the Brundtland Commission, stating that health is an integral part of social sustainability [10], making ‘Health for All’ an ultimate global goal after the World Health Assembly announced in 1977 that STD is the main goal of global development. Published in The Publication of the Brundtland Report in 1987, STD was turned to consider health development on the basis of equality, differently from the former concept that primarily focused on future generations and the environmental dimension (ENDm). The concept of health equality and STD was consequently introduced since 1989, marking a significant step for policy planning at national and local levels [11]. The concept of health promotion integrated with sustainable development was introduced through three models: (1) “The Mandala of Health: a model of the human ecosystem” studying the human ecosystem and the intersection between human culture and ecological environment. The model presents a belief that health depends on culture and the biosphere, (2) “Human development: focusing on the sustainable health”, presenting sustainable development with HEDm, ENDm, and an economic dimension (ECDm), (3) “Health and community ecosystem”, presenting a concept of the integration of health with the SODm, ENDm and ECDm in the context of healthy community [12]. Taking into account that health services are not only a single factor contributing to good health, the model also relates to other components such as the economy, lifestyle, behavior, and environment that may affect human health [13,14,15]. Later in 2000, the United Nations (UN) proposed the eight Millennium Development Goals (MDGs) to develop quality of life (QoL), namely; (1) to eliminate extreme poverty and hunger; (2) to achieve universal primary education; (3) to promote gender equality and empower women; (4) to reduce child mortality; (5) to promote maternal health; (6) to fight malaria, HIV/AIDS and other diseases; (7) to promote environmental sustainability and (8) to develop a universal partnership for development. The proposal was the official beginning of the integration of health and sustainability globally [15]. However, the MDGs ended in 2015 when the UN established “the Sustainable Development Goals (SDGs)” as a new target to drive global STD until August 2030 (a period of 15 years). The current SDGs are developed on three dimensions of sustainability: ECDm, SODm, and ENDm, encompassing 17 goals [16]. Nevertheless, the occurrence of COVID-19 has drawn a reconsideration as to whether the current concept of SDGs is sufficient [17]. The pandemic shows that HEDm substantially affects all three dimensions. Particularly, SODm is directly affected by social distancing to reduce the spread of infections, which consequently affects ECDm. In fact, the lack of socialization, travelling discontinuity and supply chain disruption in all affect the economy globally. Furthermore, ENDm has been affected by the disposal of a large amount of infectious and hazardous waste during the epidemic [7]. Considering the fact that, during the pandemic, each country has had to inevitably manage its healthcare system and resources sufficiency to control the spread of the coronavirus [18], healthcare was in a critical state around the world. Therefore, the integration of HEDm into the three pillars of STD is a plausible step to determine guidelines and criteria for progress monitoring and policies assessment to prepare a health-sustainable city for possible future outbreaks [13].
Table 1 shows the literature reviews of a sustainability model with health dimension. The study was firstly presented as “the three ecological models”, a descriptive model demonstrating interrelations among health, environment, economy and sustainable development [13,15]. As it primarily aimed to present a conceptual model, the indicators were not sufficiently considered, which makes the model difficult to use for further application and quantitative monitoring. Later, academics proposed a framework to rely on standard indicators as a Sustainable Model Measurement (SMM). The indicators were, namely, “ISO37120: Sustainable development Indicators” for city services and quality of life in communities. The ISO37210 relates to quality of urban life by using indicators for sustainable development [19], identifying indicators for city development [20] and applying the indicators into the plan of municipal level regulatory submitted to SEA in Chile. [21]. With the rise of the smart city concept, “ISO37122: Indicators for smart cities” and “ISO37123: Indicators for resilient cities” were introduced in model building as the standards in relation to the concept of smart city and urban renewal, mentioned in “Application of Open Government Data to Sustainable City Indicators: A Megacity Case Study [22]”. At the time, SMM was frequently used as a sustainability assessment model with multi-criteria discission making (MCDM) when evaluating the level of sustainable development [1,23,24,25,26,27,28,29,30,31,32]. Our literature reviews have also found that while the existing studies aim to present SMM with three sustainable dimensions, they have not described SMM with health sustainability. Furthermore, the indicators, though selected by a group of experts, lacked consensus on verification of validity and reliability. Hence, there is a possibility that the selection was conducted with biases such that a verification on compliance with empirical data to confirm the accuracy of the proposed SMM becomes necessary.
To fulfil this academic gap, this research presents a general model of health sustainability as an assessment tool that integrates the health dimension with the other three sustainability dimensions. The model is composed of standard indicators such as ISO37120, ISO37122, ISO37123 and U4SSC that were agreed through the Del-phi technique with experts from various fields. Then, the model is examined for its accuracy and generalized by the structural equation model. As the researchers also consider the context of Thailand, the model is designed to be functionable with quantitative indicators and to be able to use in MCDM, the model is expected to support strategy formulation for sustainable city development by identifying room for improvement on residents’ well-being in all related dimensions. For more details, the paper is structured into four sections with the aim to present a new model of sustainability. First, Section 1 introduces a literature review. Section 2 elaborates on methodologies of the study, starting from establishing indicators and expert panels and ending with the HSM structural equation analysis. Then, Section 3 shows the results of the study. Lastly, Section 4 conclude the study with a discussion on limitations and future research.
2. Materials and Methods
2.1. Delphi Method (DM)
DM is adopted to thoroughly investigate in-depth issues and generate a consensus from an expert panel. So, it does not need a large sample size [16], and mainly conducts investigation with the help of experts. Purposive sampling is used. The experts verify the structural validity, interpretation and variable classification [33], and generate a consensus towards the complex issues by cooperating using the questionnaires [34], and anonymity of experts [35] is enforced to avoid acquiescence of the experts from the beginning to the end of the study. The effectiveness of DM is contingent on selecting quality experts because this may alter the outcomes and accuracy [33,36]; it therefore takes into account the related information on education, experience, and competence of the experts importantly [37] with respect to the consistency with the respective topics studied [38], and diversified expertise and the in-depth data of the area studied should be inclusive to ensure data clarity in all dimensions [39]. In this study, a structured questionnaire was used to analyze the indicators derived from the literature review and standard indicators expected to have a relationship that may affect the 45 indicators. The procedures are as follows:
2.1.1. Establishing Indicators & Expert Panels
- While the number of experts for the DM should be contingent on 7-8 persons in theory [44], the researchers requested 18 experts to provide their opinions. The group of experts included physicians with in-depth understanding of overall health and sustainability issues at both the national and local level. For reference, The CVs of each expert are shown in Table A1.
2.1.2. Delphi Procedures & Consensus Indicators
First, we contacted qualified experts to request support as a sample participating in the research study. Next, the questionnaires were distributed for the first time. This was the Item-Objective Congruence (IOC) closed-ended developed questionnaire [45], including 45 indicators validated by the experts for accuracy and appropriateness that will be used to set the HSM (−1 = inappropriate) (0 = uncertainly) (+1 = appropriate). Each indicator must be close to 1, and the minimum value must be ≥0.05 or higher, but if the minimum value is ≤0.05, item adjustment or elimination may be needed [45]. The closed-ended questionnaire with qualified indicators is distributed for the second time. The experts expressed their opinion on the indicators by 5-point Linkert rating scale [46] (from 5 = very important to 1 = least important), halting the study when the expert consensus was consistent. The following statistical tests were conducted, finding as follows: Median (MD) ≥ 4 “highly important” [47], Interquartile Range (IQR) ≤ 1 and Standard Deviation (SD) < 1 [48]. KW ≤ 0.5 was used to test the degree of consensus in answering questions [49].
2.2. Structural Equation Model (SEM)
Over the past decades, SEM has been very popular in all academic arenas, including science, engineering, medicine, marketing, and education. SEM is a statistical analysis tool simultaneously encompassing the multivariate analysis techniques, focusing on examining the modification of the theoretical model [50], and the main goal of using SEM is to test the hypothesis through a causal relationship line [51], combining factor analysis and path analysis. It includes two main components (1) measurement model (MM) and (2) structural model (SM) [52]. The process of analyzing structural equations typically starts with exploratory factor analysis (EFA) to examine the structural relationship between variables to reduce the number of elements through grouping of elements into dimensions. If the structural relationship between variables is known from the review of literature, theories, or hypotheses based on studies, confirmatory factor analysis (CFA) may not be necessary. CFA is often used to confirm the relation between a theoretical variable or a given assumption [53]. The result of CFA is called the measurement model; afterwards, it is used to analyze SM by Regression Analysis, called ‘SEM’. The analysis is conducted using statistical programs such as SPSS for EFA analysis, and AMOS for CFA and SEM
SEM Procedure & Consensus Criteria
- The research instrument was designed after the analysis with DM where the final variables were concluded by the consensus from experts in 4 dimensions and 15 elements. To obtain a rating from the experts, a closed-ended 5-point Likert scale questionnaire [46] was presented to check for consistency and validity. An indicator was deemed acceptable when the IOC value was 0.5 or higher [45]. Next, the researchers tested the reliability of the questionnaires (40 questionnaires) where Cronbach’s Alpha must be 0.7 or higher [54]. Finally, the questionnaires were distributed to the samples, for which the number was determined with reference to Taro Yamane’s Sample Size Table [55]. The distribution of the questionnaire was conducted using the Snowball Sampling method, where the first group of samples or the experts refer to and nominate similar individuals who were qualified and suitable to complete the questionnaire.
- Factor Analysis (FA) is a process where the data obtained from the questionnaires are put into testing for the suitability with a statistical program. When the Kaiser–Meyer–Olkin (KMO) value ≥ 0.7 [56], the data would be suitable for EFA to determine the structural relationship between elements. To reduce the number of elements, the researchers have grouped them into dimensions, and CFA analysis was conducted to confirm theoretical variable relations and check the hypothetical model’s fit with the empirical data using two groups of statistics, namely 1) Absolute fit index, including CMIN/DF, RMSEA, GFI, AGFI, and RMR, and 2) Incremental fit index, including NFI, TLI, CFI, IFI. Finally, SM analysis was performed to test the research hypothesis.
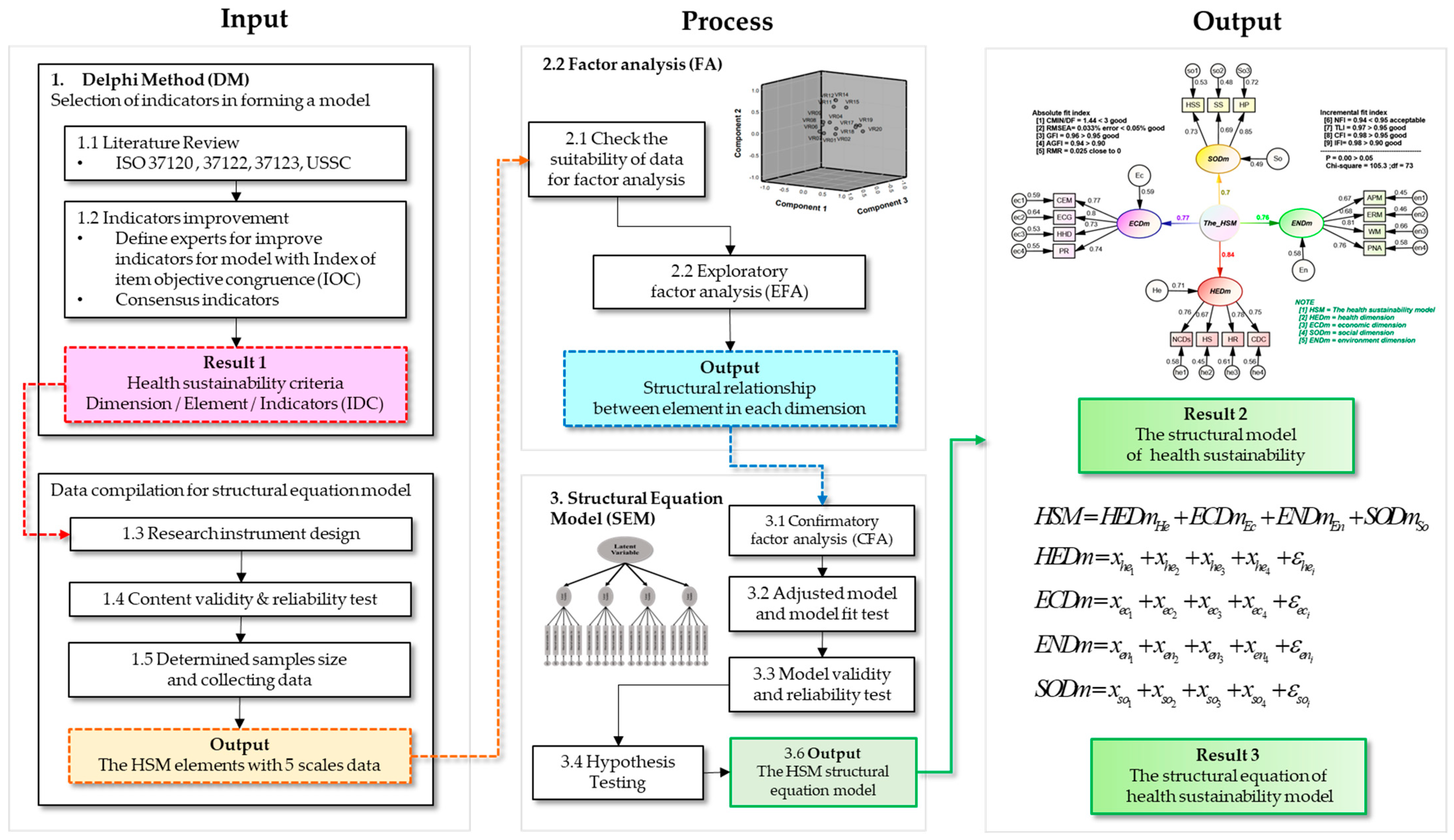
- Model validity and reliability: After completing the factor analysis, the researchers had verified the reliability convergent validity of the model with Composite Reliability (C.R.) to assess the accuracy of elements and latent variables. The preferable C.R. is above 0.7 and more than the value of AVE, where is standardized factor loading and is the number of items. The C.R., calculated from the squared sum of factor loading , is often applied in SEM models. The C.R. was then used to construct the sum of the error variance, shown as , which can be calculated from (1). The Average Variance Extracted (AVE), the average variance of the extracted variables, was calculated per formula (2). While the AVE should be more than 0.5, the Cronbach’s Alpha, which measures the internal consistency of the variables calculated by the SPSS program, should be more than 0.7. Furthermore, maximum shared variance (MSV) was tested on the relations between latent variables. MSV is the square of the highest correlation coefficient between latent constructs, where the acceptable MSV should be less than the value of AVE [56]. The above procedure is shown as a conceptual framework in Figure 1.
3. Results
3.1. Del-Phi Reliability
As shown in Table 2, it was found that the 18 experts had a consensus on all 45 indicators overall, IQR = 0.93, S.D. = 0.58, and M.D. = 4.3, and on each variable. Based on the results in Table 2, all indicators have IQR ≤ 1, M.D. ≥ 4, and S.D. < 1 where, in the DM study, all variables should have IQR ≤ 1 and S.D. < 1. Hence, it can be interpreted that the experts had a consensus on consistency, with all indicators of high significance [45]. When KW = 0.30 < 0.50, the answers were unanimous [46]. The results of the DM analysis can be summarized in Table 2.
3.2. The Health Sustainability Model (HSM)
The HSM encompasses four dimensions and 15 elements as follows:
3.2.1. Health Dimension (HEDm)
Table 2 reflects the basis of good health. Being perfect physically & mentally healthy since birth, including main disease control and the urban health service resources that result in urban public service from birth to the end of life, health status, and well-being are the heart of to human happiness and contribute greatly to economic and social development, consisting of four elements as follows:
- Health Status (HS) is one’s health status from birth to the end of life that affects longevity and health; it is influenced by several factors, including genetics, behavior, environment, health service system. and social factors, consisting of five indicators; VR01–VR05. Within HS, life expectancy has the highest average of five, implying that life expectancy is absolutely agreed to be an indicator for HS.
- Communicable Disease Control (CDC) reflects health promotion by protecting the general public from the effects of major communicable diseases. The goal is to monitor and control the cause of germs’ spread to minimize new infected cases and risk of recurrent and severe disease, consisting of four indicators; VR06–VR09. Table 2 shows that, within CDC, HIV/AIDS mortality has the highest average of 4.56, implying that is largely considered as an indicator for CDC.
- Non-Communicable Disease Control (NCDs) reflects the broad exposure to risk factors causing chronic diseases which are a major public health problem around the world because they cause sickness, disability, and premature death. The monitoring of chronic disease situations can reflect the health risk factors that have been emerging in the cities in a certain way, for instance, the tendency in urban populations to die from lung cancer mostly, etc.; it consists of six indicators, VR10–VR15. On the indicator of NCDs, Cancer mortality is widely agreed to be an indicator, with an average of 4.89.
- Health Resource: (HR) reflects efficiency and fundamental resources in the delivery of health services to the public and society; for instance, medical personnel on duty either directly or indirectly contact with patients, ward beds, ambulances, etc. The standard health service should possess resources in an adequate quantity to meet the demand, which affects the quality of public health services in the wider society. It consists of seven indicators, VR16–VR22. Among the seven indicators, the rate of physicians is largely agreed to be an indicator with an average of 4.56.
3.2.2. Environment Dimension (ENDm)
ENDm reflects the natural resources situation and urban environment, focusing on the environmental management of specific problems such as water pollution, air pollution, and environmental risk factors that are significant to human life. Urban communities affect well-being as well as the health and integrity of the ecosystem. The dimension consists of four elements as follows:
- Environment Risk Management (ERM) reflects the physical management factors, including the use of chemicals, biological and work that impact health, pollution, radiation, noise, land use patterns, and a working environment that impacts climate change, except for natural disasters beyond human control. These risks are attributed to non-health sectors such as energy, industry, agriculture, and transportation, which affect the incidence of chronic diseases (NCDs), consisting of one indicator, VR23.
- Air Pollution (APM) reflects air contamination by chemicals, dust, fumes, and pollution. It is a major public health concern, including particulate matter (PM), carbon monoxide (CO), ozone (O3), and nitrogen dioxide (NO2). Sulfur dioxide (SO2) affects morbidity and mortality from respiratory diseases and subsequent chronic diseases. It consists of one indicator, VR24.
- Protected Natural Areas (PNA) reflect protected natural areas, including plants and wildlife that are diverse in ecosystems on land, underwater and in wetlands; such areas can slow the loss of biodiversity because the areas are not disturbed by humans. It consists of one indicator, namely VR25.
- Water Management (WM) reflects eight dimensions of sustainable water management, namely water management costs, water management for consumption and usage, water security for development, water consumption cost, water quality and environment management, water disaster management, watershed forest conservation, and water resources management, consisting of one indicator, VR26.
3.2.3. Social Dimension (SODm)
SODm reflects the quality-of-life status, enhancing safety and health promotion in society, consisting of 3 elements as follows:
- Health Service Standard (HSS) reflects the standards established to implement the health service system and to measure the success of quality management as per standards, including building and environmental standards, medical equipment, and behavioral health education implementation to the public to deliver quality services that are trusted by the public and society, consisting of six indicators, VR27–VR32. Within the HSS element, health resource management has the highest average of 4.56, implying that the experts consider health resource management as an important indicator.
- Social Security (SS) reflects the quality of social security affected by events that occur in society as caused by human behavior, thereby consequently affecting the safety of life and property, injury and death; for instance, crime problems, substance use, accidents, or incidents that may occur if a person in society behaves recklessly, affecting physical health, mental health, quality of life and public peace. It consists of five indicators; VR33–VR36. Among the four indicators, traffic accident mortality receives the highest average of 4.56, which means the experts significantly consider traffic accident mortality as an indicator.
- Health Promotion (HP) reflects the control performance promotion and basic personal health improvement in attaining ultimate well-being. Health promotion is a process that encourages people to attain self-improvement on health and self-care, such as via exercise, etc., by reducing the behavioral risk factors that may cause diseases. It consists of five indicators; VR37–VR41. Among the five indicators, universal health coverage service achieves the highest average of 4.67, implying that universal health coverage service is a significant indicator.
3.2.4. Economic Dimension (ECDm)
ECDm reflects the income distribution and economic growth; economics is an element in meeting human basic needs and well-being, and ECDm reflects the improved quality of life in terms of public wealth and healthy well-being. It consists of four elements as follows:
- City’s Employment (CEM) reflects economic power; weak economy, sluggish economy, people’s lack of income, poverty, and discontinuity of private expenditure may affect quality of life, and poverty problems usually resulting from the low employment rate, consisting of one indicator, VR42.
- Poverty Reduction (PR) reflects economic policy and humanity, aiming at eradicating poverty as it is a harmful obstacle to social development, physical health, and mental health, as well as shortening the life expectancy of people in society. Most of them are remedied by economic empowerment and humanitarian policy. Poverty alleviation can improve the quality of life. It consists of one indicator, VR43.
- Household Debt reflects the household debt burden to pay interest or principal sum to the creditors on the due date. The incremental household debt affects private consumption and suspends economic growth in the long term. Liabilities and debts can also affect the happiness of people in society, particularly mental health, which may influence and press an individual’s attitudes to the extent of suicide decisions eventually. It consists of one indicator, VR44.
- Economic Growth reflects economic expansion including land, labor, capital, and entrepreneurs. Economic growth has resulted from the people in society having been employed by the business sector, while the government sector receives more income tax to spend on public services in society. Economic growth can enhance the standard of living; that is, when the public’s income is higher, the greater spending power in various areas results, for example, health care, education, consumption, etc. It consists of one indicator, VR45.
3.3. Reliability and Sampling Adequacy Results
The number of respondents for the questionnaire is 442, with 54% having a graduate degree, 27% having an undergraduate degree and the other 19% having a doctoral degree. From the affiliation perspective, 58% work in the public sector, 34% work in the private sector, 6% work in state enterprise sand the last 2% work in other sectors. Looking at the roles, 36% of the correspondents work in health issues, 35% work in environmental issues, 20% in economic issues and 6% in social issues. When considering work experience, 49% of the correspondents had work experience of 10 years or more while the other 51% had work experience of less than 10 years. Based on residency, 23% of the correspondents live in the northeastern area, 22% live in Bangkok, 22% live in the central area and 12% live in the southern area. Prior to conducting FA, a reliability analysis was performed for the suitability of the data sets. In the SEM analysis, it was found that Cronbach’s Alpha was 0.87 > 0.70, indicating that the instrument and variables used in the research meet the criteria, and KMO and Bartlett’s Test (BT) showed the KMO was 0.88 > 0.50 and BT was 0.00 < 0.05, indicating that all variables were marvelous, with high suitability for the factor analysis [56] After the confidence and suitability test, the EFA process followed.
3.4. Exploratory Factor Analysis (EFA)
In EFA, 15 elements derived by calculation were used. The indicators in the groups shown in Table 2 were new variables, including VR01–VR05 to HS, VR06–VR09 to CDC, VR10–VR15 to NCDs, VR16–VR22 to HR, VR27–VR32 to HSS, VR33–VR36 to SS, VR37–VR41 to HP. As for the elements containing one indicator, the former name was used, including VR23–VR26 to ERM, APM, PNA, WM, VR42–VR45 to CEM, PR, HHD, ECG respectively. Next, element extraction was performed using the principal component analysis method. The number of factors was determined based on eigenvalue > 1 and factor rotation was performed using the Varimax method. The results showed that the commonalities value and factor loading of all variables were > 0.50, indicating that all variables were suitable for factor analysis and consistent with the experts’ variables grouping in Table 2. In the EFA analysis, all 15 elements were classified into four dimensions: HS, CDC, NCDs, HR to HEDm, ERM, APM, PNA, WM to ENDm, HSS, SS, HP to SODm, and CEM, PR, HHD, ECG to ECDm. After that, the elements were examined through the CFA, as shown in Table 3.
3.5. Confirmatory Factor Analysis (CFA)
The purpose of the EFA was to examine the structural relationship between variables in each group to reduce the number of variables and check the suitability of the variables in the structural model analysis; however, it could not test the hypothesis based on the structural relationship between variables. Thus, CFA was required to assert the elements’ relationships or hypotheses to see whether they met the criteria defined or not. The EFA analysis data were transferred from the SPSS program to the AMOS program. The analysis results are shown in Table 3. It was found that all elements of the measurement model in CFA were statistically significant. (***) corresponding to the EFA grouping, the critical ratio (C.r.) was ≥1, greater than the expected minimum value, indicating that the indicators are suitable to represent as dimension. In contrast, C.r. was <1, indicating that the variables were not suitable to represent the dimension [56]. Next, the model suitability testing is performed with test statistical values of two groups as shown in Table 4; it was found that Group 1 had Absolute fit, consisting of test statistics, CMIN/DF = 1.44, indicating that the model fit with the empirical data as whole, and RMSEA = 0.033, GFI = 0.96, AGFI = 0.94, RMR = 0.025, all test statistic values for Group 1 were of a good level. Group 2—Incremental fit, consisting of test statistics, NFI = 0.94, CFI = 0.98, TLI = 0.97, and IFI = 0.98, all statistical values for Group 2 were of a good level, except for NFI, which was of an acceptable level. To conclude, the model was a good fit with the empirical data; although the Chi-square p was 0.00 not significant, it can be explained that because Chi-square depends on the sample size, if the sample size is large, the Chi-square value is greater accordingly. In this study, the sample size was 400, with >200 being considered a large sample. Testing Chi-square may also conclude that the model is not a good fit with the empirical data. Therefore, a correction follows Bollen’s [57] recommendations; CMIN/DF < 3 was considered instead of the Chi-square value in testing the model fit with the empirical data.
Validity and Reliability in the CFA Analysis
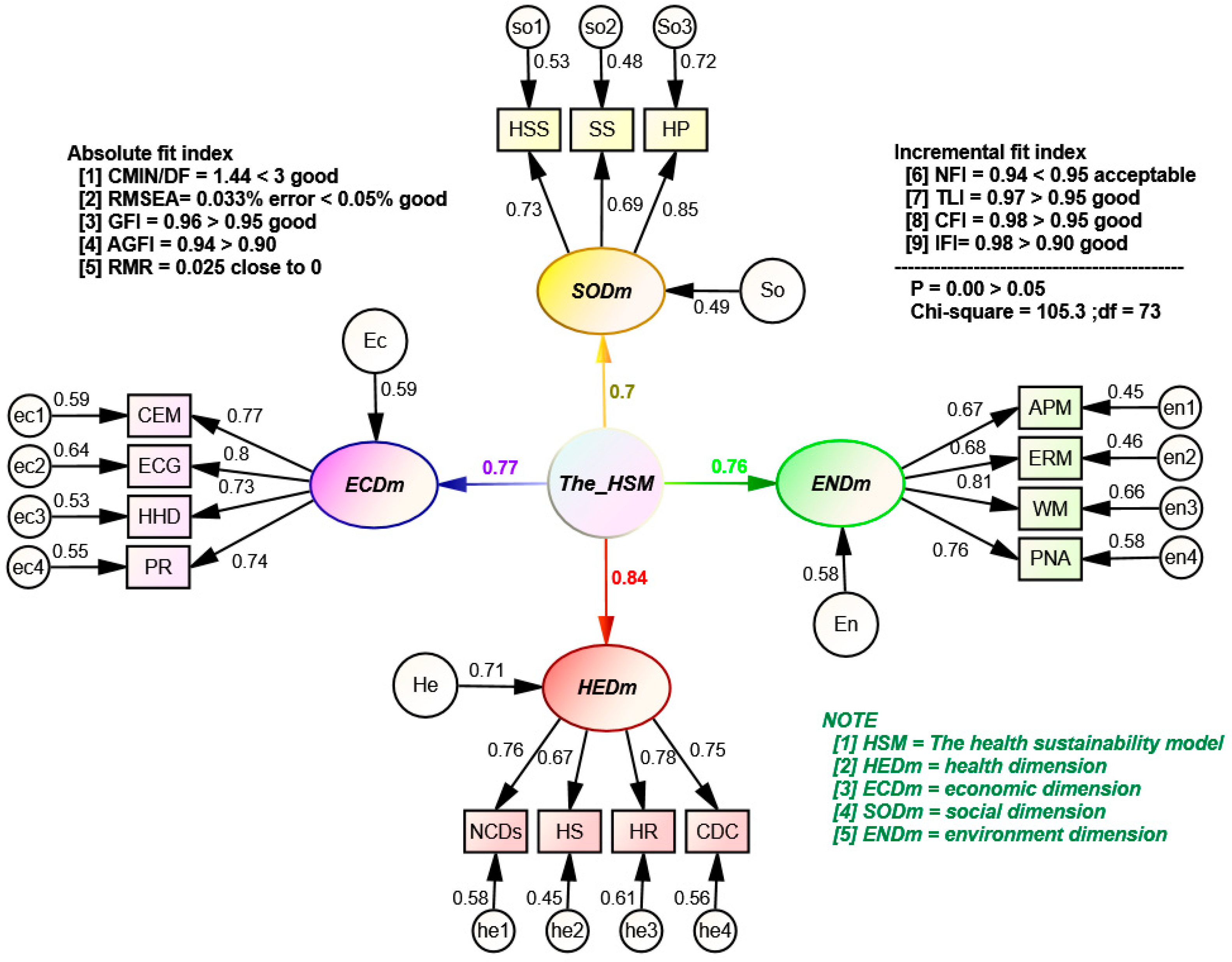
Table 5 shows that the validity and reliability for both the model toward the four pillars and the four pillars towards the elements are of a satisfactory level, with the AVE less than the C.R., where C.R. must be more than 0.7 to be considered acceptable. As the AVE is more than 0.5 and the C.A. is more than 0.7, it can be concluded that the proposed HSM is valid and reliable. Then, the researchers conducted a study on the model structure by considering and reported in the order of maximum to miminum. Among the four dimensions in the HSM, HEDm has the largest with a value of 0.84. Looking into the HEDm dimension, it is found that the of HR, NCDs, CDC and HS are 0.78, 0.76, 0.75 and 0.67. Next, the dimension with the second highest is ECDm with a value of 0.77. Within the dimension, the of ECG, CEM, PR and HHD are 0.80, 0.77, 0.74 and 0.73, respectively. Then, the third highest is ENDm, with a value of 0.76. Within the ENDm, the of WM, PNA, ERM and APM are 0.81, 0.76, 0.68 and 0.67 accordingly. Lastly, in the social dimension, the of SODm is 0.70 with the of HP, HSS and SS are 0.85, 0.73 and 0.69. All indicators of each element are shown in Table 2; the structural model is illustrated as Figure 2.
SM presents a structural of the HSM’s measurement model as required to test the hypothesis for the full structural model, as shown in Figure 2, consisting of an assumption as follows:
- H1: The HSM structural model is consistent with empirical data (Accepted). Because this is a hypothetical testing of the structural model, various types of testing were adopted in the study. The statistics in Table 4 were used to analyze the data. Thus, H1 is accepted. The hypothesis testing can be summarized as a structural equation as shown in Figure 2 as follows:
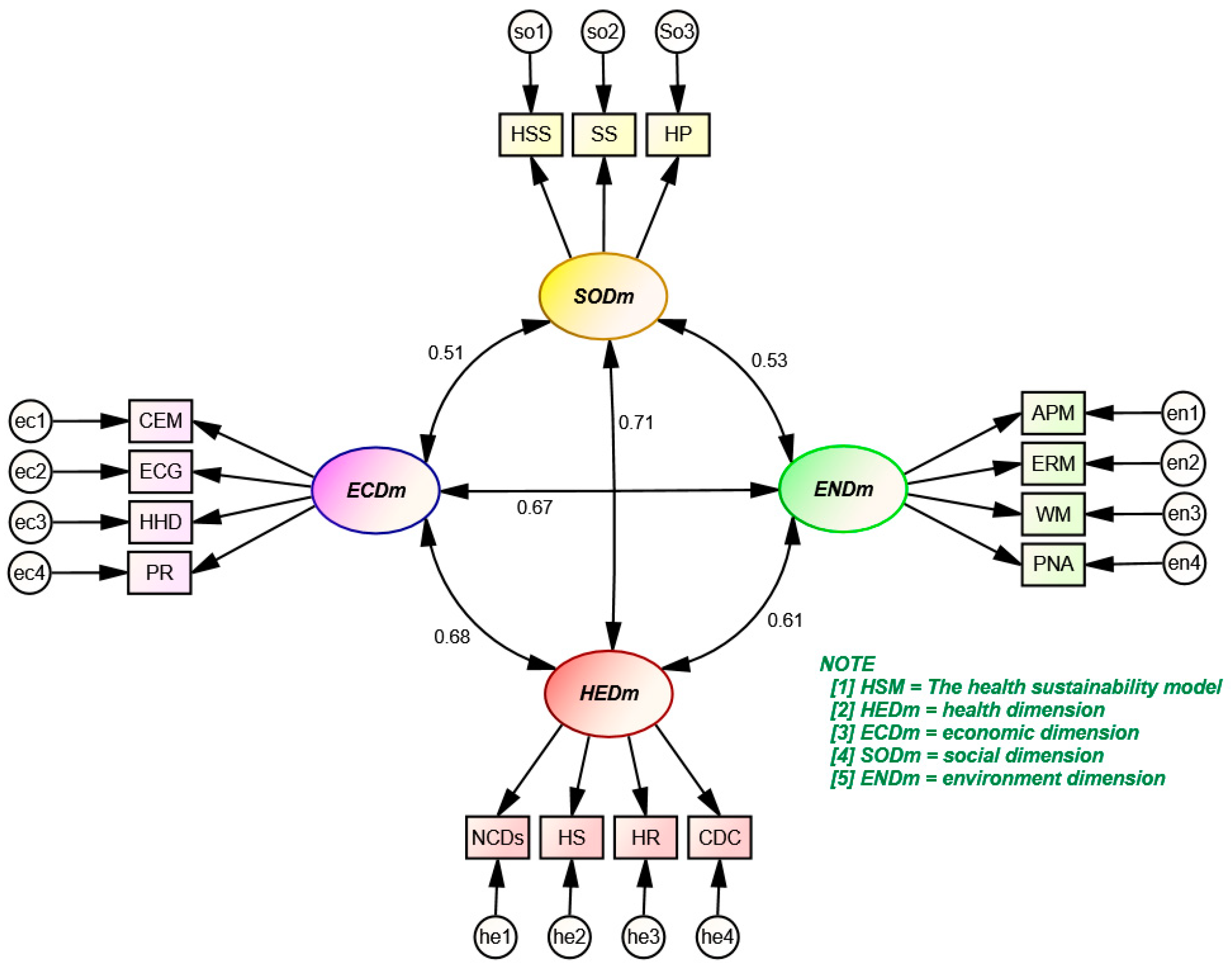
Table 6 shows that the P value of all tests are ***, interpreted as all dimensions being interrelated. Hence, all assumptions are accepted. Moreover, since MSV is less than AVE from Table 5 for all relations, we can conclude that the model is valid and reliable. The interrelations among the four dimensions and its illustration are shown in Figure 3.
Figure 3 presents interrelation among the four dimensions after testing an assumption on interrelation among each dimension. To verify the hypotheses, the researchers have set assumptions as follows.
- H:2 health dimension interrelates with social dimension (accepted)
- H:3 economic dimension interrelates with social dimension (accepted)
- H:4 environmental dimension interrelates with social dimension (accepted)
- H:5 economic dimension interrelates with environmental dimension (accepted)
- H:6 health dimension interrelates with environmental dimension (accepted)
- H:7 economic dimension interrelates with health dimension (accepted)
The causal relations can be depicted as below.
The HSM as shown in Figure 4 represents a four-dimensional sustainability model with each relationship overlapping and affecting human health directly and indirectly, including the dimensions of health, economy, environment, and society. Currently, sustainable urban development focuses on three main dimensions and often views health as small issues within SODm, while health is defined by medical services only. The concept of The HSM is that sustainable health determinants do not depend on SODm only. Thus, HEDm is separated from SODm. Being healthy is not just determined by health services, but all overlapping dimensions directly and indirectly affect health. Therefore, integration of the dimensions is needed to achieve overall health sustainability.
Health and well-being are linked to two implications. Firstly, the implications on health, including (1) physical health is the existence of a healthy body and being free from physical ailments, (2) mental health is the mental capacity, good mental health, and emotional stability to tackle difficulties and failure in life without contributions to stress, anxiety or depression causing deteriorating physical health. Thus, it can be concluded that a good physical condition and good mental health are the primary basis for normal happy lives in a society, and consequently, the feeling of social safety. Secondly, the implications on well-being, including (1) objective well-being—the basic physiological needs that human beings must have met, including food, health, shelter and safety and security needs from dangers, career stability, adequate emergency savings, etc., leading to the wider economic development; (2) subjective well-being—emotional need and responses, including belonging being loved by neighboring people and society (for example, having a family, being accepted and recognized by the society), being respected (esteem needs), including rank, position, competency; all these have affected the quality of life of the people.
Physical and mental well-being makes it possible for individuals to live their life to the fullest, consequently resulting in improved performance, a better quality of life, and improved economic stability when people in society are satisfied with their welfare. Community health development comprises three components: (1) health promotion, (2) health protection, including vaccinations, mental support counseling for quitting drugs, disease screening, etc., (3) health services, including nutrition counseling, treatment, and disease prevention information to the extent that quality is met adequately by the government to increase control and self-improvement on health, generally provided by the government from public health service investment to public health quality standards to support urban expansion appropriately as well as the equality and equity of access. Sustainability development in HEDm and ECDm at the same time is called “human development”.
Livable Development constitutes improving and adjusting the ecosystem into equilibrium, making changes such as a smaller number of patients and improved delivery of comprehensive public health services, clean living environment, such as air quality, water quality, and safety conditions, ability to coexist with nature, awareness and respect for all in the food chain, encouraging sharing the city, and developing a variable transportation option to support walking and cycling to reduce pollution, accidents and traffic congestion, and encourage urban people to share social activities, thus reducing the impact on the ecosystem as a whole (ecological footprint reduction).
Environmental wellness represents the state of physical well-being as a result of a pleasant environment supporting well-being and encourage interaction with nature. Sustainability can be achieved with the cooperation of the economic sector, which is a sector that directly impacts environmental health. The economic sector must be aware (environment awareness) of the environmental vulnerability and the importance of environmental protection, and implement environment policy that is designed to prevent and reduce the harmful impacts (carbon footprint reduction) generated by human activities on the environment; for example, educating the community on environmental protection, the control of chemicals, noise, pollution, waste, water resources, as well as energy-saving measures and reuse, etc. The HSM can be summarized as a diagram as shown in Figure 4.
4. Discussion
The research presents a model considering health sustainability. While precedent research does not consider the health dimension, our proposed model integrates the health dimension into the existing three sustainability dimensions. Based on the agreement from the experts and the factor analysis, the model contains 45 indicators, grouped into 15 elements and four dimensions, respectively. Model fit is tested by SEM and it was found that both the absolute fit index and the incremental fit index achieve a favorable result, consistent with the empirical data. Afterwards, the researchers conducted validity and reliability tests and found that the elements in all dimensions satisfied the preset criteria, consistent with the agreement from the experts. In the final step, the researchers tested the assumptions on interrelation among four dimensions and found that all dimensions have a positive interrelation. Hence, a change occurring in one dimension will cause a direct variation in other dimensions.
At present, the sustainability assessment model in Thailand is built only to measure at the national level. There has been no development of a concrete model to measure at the provincial level, leaving a space for the proposed model to implement. In the application, the model is crucial as it enables a city planner to formulate a strategy driving toward health sustainability and improving residents’ well-being in all dimensions. The HSM is designed to be a general assessment model, suitable for the context of Thailand to apply quantitative indicators and support the assessment with MCDM, and is expected to facilitate the assessment not only in any specific province, but in all 77 provinces of Thailand. For more details on the applicability of the HSM, the readers can refer to our research in Part 2: The Dynamic Evaluation Model of Health Sustainability under MCDM Benchmarking Health Indicator Standards [59].
Limitations and Future Research
- The research aims to propose a model to assess sustainability from four dimensions. While the integrity among the dimensions has been tested with the SEM, the relationships within elements and dimensions have yet been verified, leaving room for future research to conduct path analysis to test both direct and indirect effects. In future research, multiple regression analysis and descriptive statistics can be elaborated to provide in-depth understanding for each dimension and element.
- The research only presents an assessment model without any application with real data. Future research can conduct a sustainability assessment of a city by applying the model with MCDM.
- The sample mentioned in the study is gathered via a snowball sampling method. As a result, there is limitation in controlling the demographics of the sample. Future research should identify the demographics and expected composition of the sample to maintain its integrity.
Author Contributions
Conceptualization, V.V.; Methodology, V.V.; Formal analysis, N.R.; Investigation, N.R.; Writing—original draft, N.R.; Writing—review & editing, W.R.; Supervision, V.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Human Research Ethics Committee of University of the Thai Chamber of Commerce (protocol code UTCCEC/Excemp057/2022 and date of approval 17 October 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to express their gratitude to the Logistics Research and Development Institute team, Wararat Theerasak, Thanaporn Srisuk, Kulsurat Muangthong, and Natthakrit Bamrungwong for their support throughout the study, the 18 experts for kindly cooperating and willfully providing their invaluable opinions, and Mode Vasuaninchita and Yuth Kraiwan for advice on structural equation model analysis. We also would like to thank Nuttun pongpanit, Thayika kasiwit amnuai, Krissana Piaratisit, Nattawut pumpugsri, Bumrung Nokkaew, AIongkorn Piaphong and Anupong inprom for coordinating throughout the study. Lastly, we appreciate all reviewers for your sincere comments and invaluable recommendations to improve our edition to be completed as our readers have scrolled up to now.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HSM | Health Sustainability Model |
| SMM | Sustainable Model Measurement |
| STD | Sustainable development |
| SDGs | Sustainable Development Goals |
| MCDM | Multi criteria discission making |
| HEDm | Health dimension |
| SODm | Social dimension |
| ENDm | Environmental dimension |
| ECDm | Economic dimension |
| DM | Del-phi method |
| EFA | Exploratory Factory Analysis |
| CFA | Confirmatory Factor Analysis |
| QoL | Quality of life |
| C.r. | Critical Ratio |
| C.R. | Composite (construct) Reliability |
| IOC | Item-Objective Congruence |
| SM | Structural model |
| MM | Measurement model |
| SEM | Structural Equation Model |
| FA | Factor analysis |
| KMO | Kaiser-Meyer-Olkin test |
| K.W. | Kendall’s W |
| IQR. | The Interquartile Range |
| S.D. | Standard Deviation |
| M.D. | Median |
| CMIN/DF | Relative Chi-Square |
| RMSEA | Root means square error of approximation |
| GFI | Goodness of Fit index |
| AGFI | Adjusted goodness of fit index |
| RMR | Root of mean square residuals |
| NFI | Normed Fit Index |
| TLI | Non-Normed-fit index (Tucker-Lewis) |
| CFI | The comparative fit index |
| IFI | Incremental fit index |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table A1.
Experts profile & qualification.
| Number | Title | Experience | Expertise |
|---|---|---|---|
| 1 | M.D. |
| Pulmonary medicine and pulmonary critical care, emergency medicine, community medicine, environmental medicine, internal medicine Specialty: Respiratory Disease |
| 2 | M.D. |
| Surgery, emergency medicine, pathology |
| 3 | M.D. |
| Maternal Nursing Infants and Midwifery, community medicine, environmental medicine |
| 4 | M.D. |
| Internal medicine, rheumatology and rheumatism, community medicine |
| 5 | M.D. |
| Emergency management, disease control planning, animal science |
| 6 | Dr. |
| Health promotion, community health |
| 7 | Dr. |
| Nutrition ology and dietetics, food science for health, sanitary |
| 8 | Dr. |
| Macro & micro economic policies analysis, international economy |
| 9 | Dr. |
| Analyze and plan work to drive economic and social development. |
| 10 | - |
| Social welfare system, human and social development policy. |
| 11 | - |
| City planning analysis and development. |
| 12 | Dr. |
| Smart sustainable city, smart city, sustainability, economic, sustainable development. |
| 13 | Dr. |
| Smart city, smart city characteristics, smart city project analysis, economic |
| 14 | Dr. |
| Carbon footprint, water quality, air quality, noise, toxic substances, environmental quality standards. |
| 15 | Dr. |
| Plan and control environment, environment risk factor examine. |
| 16 | Dr. |
| Sustainable development, environmental Science |
| 17 | Dr. |
| Sustainable measurement, Sociology and Anthropology |
| 18 | Dr. |
| Social Science, Sustainable Development |
References
- Tang, J.; Zhu, H.-L.; Liu, Z.; Jia, F.; Zheng, X.-X. Urban Sustainability Evaluation under the Modified TOPSIS Based on Grey Relational Analysis. Int. J. Environ. Res. Public Health 2019, 16, 256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banamar, I.; Yves De, S. An extension of PROMETHEE II to temporal evaluations. Int. J. Multicriteria Decis. Mak. 2018, 7, 298–325. [Google Scholar] [CrossRef]
- Kondepudi, S.N.; Ramanarayanan, V.; Jain, A.; Singh, G.N.; Nitin Agarwal, N.K.; Kumar, R.; Singh, R.; Bergmark, P.; Hashitani, T.; Gemma, P. Smart Sustainable Cities Analysis of Definitions; The ITU-T Focus Group for Smart Sustainable Cities: Geneva, Switzerland, 2014. [Google Scholar]
- Brundtland Commission. Brundtland Report: Our Common Future WCED: World Commission on the Environment Development; Oxford University Press: Oxford, UK, 1987. [Google Scholar]
- Hairet, T.; Yang, Z.F.; Wang, H.D. Reflection on theory of urban sustainable development. Environ. Sci 1998, 18, 13–18. [Google Scholar]
- Hamilton, A.; Mitchell, G.; Yli-Karjanmaa, S. The BEQUEST toolkit: A decision support system for urban sustainability. Build. Res. Inf. 2002, 30, 109–115. [Google Scholar] [CrossRef]
- Prajapati, D.; Agarwal, S.; Murtaza, Q. Impact of COVID-19 on Sustainability Enablers and Evaluation of Performance Index. Mater. Today Proc. 2022, 56, 3790–3796. [Google Scholar] [CrossRef] [PubMed]
- UN Centre for Human Settlements (Habitat). The State of the World’s Cities Report. 2006/2007: The Millennium Development Goals and Urban Sustainability: 30 Years of Shaping the Habitat Agenda; Earthscan: London, UK, 2006. [Google Scholar]
- World Health Organization. Ottawa Charter for Health Promotion; World Health Organization, Regional Office for Europe: København, Denmark, 1986. [Google Scholar]
- Brundtland Commission. Our Common Future; Oxford University Press: Oxford, UK, 1987. [Google Scholar]
- Mori, K.; Christodoulou, A. Review of sustainability indices and indicators: Towards a new City Sustainability Index (CSI). Environ. Impact Assess. Rev. 2012, 32, 94–106. [Google Scholar] [CrossRef]
- Trevor, H.; Perkins, F. The mandala of health. Health Educ. 1985, 24, 8–10. [Google Scholar]
- Trevor, H. Health, human development and the community ecosystem: Three ecological models. Health Promot. Int. 1993, 8, 41–47. [Google Scholar]
- WHO and the Government of South Australia. The Adelaide Statement on Health in All Policies: Moving towards a shared governance for health and well-being. Health Promot. Int. 2010, 25, 258–260. [Google Scholar] [CrossRef]
- Kjærgård, B.; Land, B.; Pedersen, K.B. Health and sustainability. Health Promot. Int. 2013, 29, 558–568. [Google Scholar] [CrossRef] [Green Version]
- Fukuda-Parr, S. From the Millennium Development Goals to the Sustainable Development Goals: Shifts in purpose, concept, and politics of global goal setting for development. Gend. Dev. 2016, 24, 43–52. [Google Scholar] [CrossRef]
- Rai, P.K.; Sonne, C.; Song, H.; Kim, K.-H. The effects of COVID-19 transmission on environmental sustainability and human health: Paving the way to ensure its sustainable management. Sci. Total Environ. 2022, 838, 156039. [Google Scholar] [CrossRef] [PubMed]
- An, X.; Xiao, L.; Yang, X.; Tang, X.; Lai, F.; Liang, X.-H. Economic burden of public health care and hospitalisation associated with COVID-19 in China. Public Health 2022, 203, 65–74. [Google Scholar] [CrossRef]
- Przybyłowski, A.; Kałaska, A.; Przybyłowski, P. Quest for a Tool Measuring Urban Quality of Life: ISO 37120 Standard Sustainable Development Indicators. Energies 2022, 15, 2841. [Google Scholar] [CrossRef]
- Lehner, A.; Erlacher, C.; Schlögl, M.; Wegerer, J.; Blaschke, T.; Steinnocher, K. Can ISO-Defined Urban Sustainability Indicators Be Derived from Remote Sensing: An Expert Weighting Approach. Sustainability 2018, 10, 1268. [Google Scholar] [CrossRef] [Green Version]
- Reicher, O.; Delgado, V.; Arumi, J.-L. Use of Indicators in Strategic Environmental Assessments of Urban-Planning Instruments: A Case Study. Sustainability 2021, 13, 12639. [Google Scholar] [CrossRef]
- Takiya, H.; Negreiros, I.; Yamamura, C.L.K.; Quintanilha, J.A.; Machado, C.A.S.; Abiko, A.; de Campos, C.I.; Pessoa, M.S.D.P.; Berssaneti, F.T. Application of Open Government Data to Sustainable City Indicators: A Megacity Case Study. Sustainability 2022, 14, 8802. [Google Scholar] [CrossRef]
- Ding, L.; Shao, Z.; Zhang, H.; Xu, C.; Wu, D. A Comprehensive Evaluation of Urban Sustainable Development in China Based on the TOPSIS-Entropy Method. Sustainability 2016, 8, 746. [Google Scholar] [CrossRef] [Green Version]
- Dang, W.V.-T.; Wang, J.; Dang, V.-T. An Integrated Fuzzy AHP and Fuzzy TOPSIS Approach to Assess Sustainable Urban Development in an Emerging Economy. Int. J. Environ. Res. Public Health 2019, 16, 2902. [Google Scholar] [CrossRef] [Green Version]
- Zavadskas, E.K.; Cavallaro, F.; Podvezko, V.; Ubarte, I.; Kaklauskas, A. MCDM Assessment of a Healthy and Safe Built Environment According to Sustainable Development Principles: A Practical Neighborhood Approach in Vilnius. Sustainability 2017, 9, 702. [Google Scholar] [CrossRef] [Green Version]
- Wątróbski, J.; Bączkiewicz, A.; Ziemba, E.; Sałabun, W. Sustainable cities and communities assessment using the DARIA-TOPSIS method. Sustain. Cities Soc. 2022, 83, 103926. [Google Scholar] [CrossRef]
- Paz, T.D.S.R.; Caiado, R.G.G.; Quelhas, O.L.G.; Gavião, L.O.; Lima, G.B.A. Assessment of sustainable development through a multi-criteria approach: Application in brazilian municipalities. J. Environ. Manag. 2021, 282, 111954. [Google Scholar] [CrossRef] [PubMed]
- Long, R.; Li, H.; Wu, M.; Li, W. Dynamic evaluation of the green development level of China’s coal-resource-based cities using the TOPSIS method. Resour. Policy 2021, 74, 102415. [Google Scholar] [CrossRef]
- Stachura, P.; Kuligowska, K. Multi-criteria analysis of urban policy for sustainable development decision-making: A case study for Warsaw city, Poland. Procedia Comput. Sci. 2021, 192, 259–269. [Google Scholar] [CrossRef]
- Boggia, A.; Massei, G.; Pace, E.; Rocchi, L.; Paolotti, L.; Attard, M. Spatial multicriteria analysis for sustainability assessment: A new model for decision making. Land Use Policy 2018, 71, 281–292. [Google Scholar] [CrossRef] [Green Version]
- Paolotti, L.; Gomis, F.D.C.; Torres, A.A.; Massei, G.; Boggia, A. Territorial sustainability evaluation for policy management: The case study of Italy and Spain. Environ. Sci. Policy 2019, 92, 207–219. [Google Scholar] [CrossRef]
- Hély, V.; Antoni, J.-P. Combining indicators for decision making in planning issues: A theoretical approach to perform sustainability assessment. Sustain. Cities Soc. 2019, 44, 844–854. [Google Scholar] [CrossRef]
- Okoli, C.; Pawlowski, S.D. The Delphi method as a research tool: An example, design considerations and applications. Inf. Manag. 2004, 42, 15–29. [Google Scholar] [CrossRef] [Green Version]
- Linstone, H.A.; Turoff, M. Delphi: A brief look backward and forward. Technol. Forecast. Soc. Chang. 2011, 78, 1712–1719. [Google Scholar] [CrossRef]
- Musa, H.D.; Yacob, M.R.; Abdullah, A.M.; Ishak, M.Y. Delphi Method of Developing Environmental Well-being Indicators for the Evaluation of Urban Sustainability in Malaysia. Procedia Environ. Sci. 2015, 30, 244–249. [Google Scholar] [CrossRef] [Green Version]
- Donohoe Holly, M. Defining culturally sensitive ecotourism: A Delphi consensus. Curr. Issues Tour. 2011, 14, 27–45. [Google Scholar] [CrossRef]
- Monica, R.; Maria, J.; Maaret, C.; Leif, S.; Dan, G.; Anders, R. Essential key indicators for disaster medical response suggested to be included in a national uniform protocol for documentation of major incidents: A Delphi study. Scand. J. Trauma Resusc. Emerg. Med. 2013, 21, 68. [Google Scholar]
- Saud Ali, A.; Yacine, R.; Haijiang, L. Delphi-based consensus study into a framework of community resilience to disaster. Nat. Hazards 2015, 75, 2221–2245. [Google Scholar]
- Jeste Dilip, V.; Monika, A.; Dan, B.; Kraemer Helena, C.; George, V.; Meeks Thomas, W. Expert consensus on characteristics of wisdom: A Delphi method study. Gerontologist. 2010, 50, 668–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Organization for Standardization. Sustainable Cities and Communities: Indicators for City Services and Quality of Life; International Organization for Standardizaiton: Geneva, Switzerland, 2018. [Google Scholar]
- International Organization for Standardization. Sustainable Cities and Communities—Indicators for Smart Cities; International Organization for Standardization: Geneva, Switzerland, 2019. [Google Scholar]
- International Organization for Standardization. Sustainable Cities and Communities—Indicators for Resilient Cities; International Organization for Standardization: Geneva, Switzerland, 2018. [Google Scholar]
- The United for Smart Sustainable Cities (U4SSC). Collection Methodology for Key Performance Indicators for Smart Sustainable Cities; The United for Smart Sustainable Cities: Geneva, Switzerland, 2017. [Google Scholar]
- Amr, S.; Mu, S. The Delphi method: Review and use in construction management research. Int. J. Constr. Educ. Res. 2015, 11, 54–76. [Google Scholar]
- Rovinelli Richard, J.; Hambleton Ronald, K. On the Use of Content Specialists in the Assessment of Criterion-Referenced Test Item Validity; ERIC: Tinton Falls, NJ, USA, 1976.
- Rensis, L. A technique for the measurement of attitudes. Arch. Psychol. 1932, 22, 55. [Google Scholar]
- Horner, K.; Islam, M.; Flygare, L.; Tsiklakis, K.; Whaites, E. Basic principles for use of dental cone beam computed tomography: Consensus guidelines of the European Academy of Dental and Maxillofacial Radiology. Dentomaxillofac. Radiol. 2009, 38, 187–195. [Google Scholar] [CrossRef]
- Geist Monica, R. Using the Delphi method to engage stakeholders: A comparison of two studies. Eval. Program Plan. 2010, 33, 147–154. [Google Scholar] [CrossRef]
- Maurice, G.K.; Babington, S.B. The problem of m rankings. Ann. Math. Stat. 1939, 10, 275–287. [Google Scholar]
- Anderson James, C.; Gerbing David, W. Structural equation modeling in practice: A review and recommended two-step approach. Psychol. Bull. 1988, 103, 411. [Google Scholar] [CrossRef]
- Pui-Wa, L.; Qiong, W. Introduction to structural equation modeling: Issues and practical considerations. Educ. Meas. Issues Pract. 2007, 26, 33–43. [Google Scholar]
- Rebecca, W.; Gore Jr, P.A. A brief guide to structural equation modeling. Couns. Psychol. 2006, 34, 719–751. [Google Scholar]
- Hair Joseph, F.; Anderson Rolph, E.; Babin Barry, J.; Black Wiiliam, C. Multivariate Data Analysis: A Global Perspective; Pearson Education: London, UK, 2010; Volume 7. [Google Scholar]
- Mohsen, T.; Reg, D. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53. [Google Scholar]
- Yamane, T. Statistics: An Introductory Analysis, 3rd ed.; Harper & Row: Manhattan, NY, USA, 1973. [Google Scholar]
- Dejan, D.; Darja, T. Introduction to structural equation modeling: Review, methodology and practical applications. In Proceedings of the International Conference on Logistics & Sustainable Transport, Celje, Slovenia, 19–21 June 2014; pp. 19–21. [Google Scholar]
- Bollen Kenneth, A.; Scott, L.J. Testing Structural Equation Models; Sage: Southend Oaks, CA, USA, 1993; Volume 154. [Google Scholar]
- Schumacker Randall, E.; Lomax Richard, G. A Beginner’s Guide to Structural Equation Modeling; Psychology Press: Hove, UK, 2004. [Google Scholar]
- Ritmak, N.; Rattanawong, W.; Vongmanee, V. The Dynamic Evaluation Model of Health Sustainability under MCDM Benchmarking Health Indicator Standards. Int. J. Environ. Res. Public Health 2023, 20, 259. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Conceptual framework.

Figure 2.
Structural Model of The HSM.

Figure 3.
The interrelation among the four dimensions.

Figure 4.
The health sustainable model diagram.

Table 1.
Literature reviews matrix.
| Objective | Initial Factors | Sustainability Dimension Focus | Result | Ref. | ||||
|---|---|---|---|---|---|---|---|---|
| Soc. | Eco. | Env. | Hea. | Etc. | ||||
| Investigate the possibility of comparing, in a transparent way, urban quality of life using sustainable development indicators | ISO37120 | ✓ | ✓ | ✓ | IDS | [19] | ||
| Identify indicators for the sustainable development of cities that have the greatest potential for their underlying data to be measured by means of remote sensing. | ISO37120 | ✓ | ✓ | IDS | [20] | |||
| Analyze the indicators of the São Paulo City Observatory (Observa Sampa), confronting them with the ISO 3712x series (sustainable, smart, and resilient cities) standards | ISO37120 ISO37122 ISO37123 | ✓ | ✓ | ✓ | IDS | [22] | ||
| Applied indicators at municipal-level regulatory plans submitted to SEA in Chile. | ISO37120 | ✓ | IDS | [21] | ||||
| (1) The three ecological models are the links between health, environment and economy (2) All models link the social, environmental and economic dimensions of a healthy and sustainable community. | - | ✓ | ✓ | ✓ | ✓ | CM | [13] | |
| Understanding the linkages between health promotion and sustainable development for health and food | - | ✓ | ✓ | ✓ | CM | [15] | ||
| Evaluates the sustainable development level with the phenomenon of a spatial clustering case study in China | LR | ✓ | ✓ | ✓ | EM | [23] | ||
| Evaluation of urban sustainability with grey relation analysis is used to reduce the uncertainty existing in the process of an evaluation case study in China | LR | ✓ | ✓ | ✓ | EM | [1] | ||
| Assess Sustainable Urban Development in an Emerging Economy with Fuzzy-TOPSIS in a case case study in Vietnam lacking clear data | LR | ✓ | ✓ | ✓ | EM | [24] | ||
| Assess a healthy and safe built environment with integrated MCDM methods in a case study in Lithuania | LR/Unitednation | ✓ | ✓ | ✓ | EM | [25] | ||
| Sustainability assessment method that integrates the MCDM approach with the variability of the alternatives’ performance measurement in a case study in Europe | LR | ✓ | ✓ | ✓ | EM | [26] | ||
| Verify the performance of Brazilian municipalities in the three dimensions of sustainability in a case study in Brazil | LR | ✓ | ✓ | ✓ | EM | [27] | ||
| Developed an evaluation index system that satisfies the requirements of green development in coal-resource-based cities by considering four dimensions in a case study in China | LR | ✓ | ✓ | ✓ | ✓ | EM | [28] | |
| Evaluate the progress of a single city towards the concept of sustainable development in a case study in Poland | Warsaw policy | ✓ | ✓ | ✓ | EM | [29] | ||
| Present a new model, called Geo Umbria SUIT, integrating Multicriteria Analysis and Geographic Information Systems, specifically developed for helping Decision Makers to take policy decisions about sustainability in planning in a case study in Malta | the Geo Umbria Suite | ✓ | ✓ | ✓ | EM | [30] | ||
| The tested model, Geo Umbria SUIT, was found very suitable for territorial sustainability assessment, for evaluating sustainability at the territorial level in two different European countries, i.e., Italy and Spain. | National Statistics Office | ✓ | ✓ | ✓ | EM | [31] | ||
| Assessment of localizations in the Besancon area in terms of sustainable urban development; case study in France | GIS grid | ✓ | ✓ | ✓ | EM | [32] | ||
| This paper: presents a new general model of health sustainability that integrates the health dimension with the other three sustainability dimensions for a Thai context. | ISO37120 ISO37122 ISO37123 U4SSC | ✓ | ✓ | ✓ | ✓ | SEM SMM | ||
Note: Literature review (LR); Social (Soc.); Economic (Eco.); Environment (Env.); Health (Hea.); indicator set (IDS); conceptual model (CM); Structural equation model (SEM); Sustainable measurement model (SMM); evaluation model with MCDM (EM).
Table 2.
Del-phi Results.
| Dimension | Element | Indicators | Unit | IQR | M.D. | AVR. | S.D. | CODE |
|---|---|---|---|---|---|---|---|---|
| Health | Health Status (HS) | Life expectancy | Year | 0 | 5 | 5.00 | 0.00 | VR01 |
| Low-birth-weight newborns | % | 1 | 4 | 3.56 | 0.50 | VR02 | ||
| Number of deaths (rate) | 1 K | 1 | 4 | 4.00 | 0.67 | VR03 | ||
| Infant mortality livebirth (rate) | 1 K | 1 | 4 | 3.56 | 0.50 | VR04 | ||
| Suicide mortality (rate) | 100 K | 1 | 4 | 4.22 | 0.63 | VR05 | ||
| Communicable Disease Control (CDC) | HIV/AIDS mortality (rates) | 100 K | 1 | 5 | 4.56 | 0.68 | VR06 | |
| Tuberculosis mortality (rates) | 100 K | 1 | 4 | 3.78 | 0.63 | VR07 | ||
| Pneumonia mortality (rates) | 100 K | 1 | 4 | 3.44 | 0.68 | VR08 | ||
| Diarrhea mortality (rates) | 100 K | 1 | 4 | 3.56 | 0.50 | VR09 | ||
| Non communicable Disease Control (NCDs) | Cancer mortality (rates) | 100 K | 0 | 5 | 4.89 | 0.31 | VR10 | |
| Stroke mortality (rate) | 100 K | 1 | 4 | 3.67 | 0.67 | VR11 | ||
| Ischemic heart disease Mortality (rate) | 100 K | 1 | 4 | 4.33 | 0.67 | VR12 | ||
| Diabetes mellitus mortality (rate) | 100 K | 1 | 5 | 4.56 | 0.50 | VR13 | ||
| Chronic obstructive pulmonary disease mortality (rate) | 100 K | 1 | 4 | 4.22 | 0.63 | VR14 | ||
| Chronic kidney disease mortality (rate) | 100 K | 1 | 4 | 3.44 | 0.68 | VR15 | ||
| Health Resource (HS) | Physicians (rate) | 100 K | 1 | 5 | 4.56 | 0.68 | VR16 | |
| Hospital beds (rate) | 100 K | 1 | 4 | 4.33 | 0.67 | VR17 | ||
| Nursing & midwifery personnel (rate) | 100 K | 1 | 4 | 4.33 | 0.67 | VR18 | ||
| Psychiatric physicians (rate) | 100 K | 1 | 5 | 4.44 | 0.68 | VR19 | ||
| Total Health worker (rate) | 100 K | 1 | 4 | 3.56 | 0.50 | VR20 | ||
| Ambulance (rate) | 100 K | 1 | 4 | 4.00 | 0.67 | VR21 | ||
| Electronic Medical Records | % | 1 | 4 | 4.44 | 0.50 | VR22 | ||
| Environment | Environment Risk Management (ERM) | Environmental risk Management | % | 1 | 4 | 4.33 | 0.47 | VR23 |
| Air pollution management (APM) | Average of AQI Index | Index | 1 | 4 | 3.44 | 0.68 | VR24 | |
| Protected Natural Areas (PNA) | Forest area rate | % | 1 | 5 | 4.56 | 0.50 | VR25 | |
| Water Management (WM) | Water management Index | Index | 1 | 5 | 4.56 | 0.50 | VR26 | |
| Social | Health Service Standard (HSS) | Health resource management | % | 1 | 5 | 4.56 | 0.50 | VR27 |
| Transparency in public health | % | 1 | 4 | 4.33 | 0.67 | VR28 | ||
| Green & Clean hospital administration | % | 1 | 4 | 3.56 | 0.50 | VR29 | ||
| Management of public health crises | % | 1 | 4 | 3.44 | 0.68 | VR30 | ||
| Community hospital quality | % | 1 | 4 | 3.56 | 0.50 | VR31 | ||
| Control of acute infectious diseases | % | 1 | 4 | 4.00 | 0.67 | VR32 | ||
| Social security (SS) | Smoking mortality (rate) | 100 K | 1 | 4 | 3.56 | 0.50 | VR33 | |
| Alcohol drinking mortality (rate) | 100 K | 1 | 4 | 4.00 | 0.67 | VR34 | ||
| Traffic accident mortality (rate) | 100 K | 1 | 5 | 4.56 | 0.50 | VR35 | ||
| Crime mortality (rate) | % | 1 | 5 | 4.44 | 0.68 | VR36 | ||
| Health Promotion(HP) | Universal Health Coverage Service | % | 1 | 4 | 4.67 | 0.68 | VR37 | |
| Desirable health behaviors | % | 1 | 4 | 4.33 | 0.67 | VR38 | ||
| Obesity (BMI > 30.0 kg/m2) | % | 1 | 4 | 3.67 | 0.67 | VR39 | ||
| Management of Glycemic control | % | 1 | 4 | 4.00 | 0.67 | VR40 | ||
| Management of Blood pressure control | % | 1 | 4 | 3.67 | 0.67 | VR41 | ||
| Economic | City’s Employment (CEM) | Unemployment rate | % | 1 | 5 | 4.44 | 0.68 | VR42 |
| Poverty Reduction (PR) | Population living in poverty | % | 0 | 4 | 4.11 | 0.31 | VR43 | |
| Household debt (HHD) | Household debt per income ratio | % | 1 | 4 | 4.33 | 0.67 | VR44 | |
| Economic growth(ECG) | Gross Provincial Product growth rate | % | 1 | 5 | 4.44 | 0.68 | VR45 | |
| Summary | 0.93 | 4.30 | - | 0.58 | 45 | |||
| KW = 0.36/Sig 0.00/N 18 | ||||||||
Note: 1 K = 1000 Population; the Interquartile Range (IQR); median (M.D.); average (AVR.); standard division (S.D.); Kendall’s Coefficient of Concordance (KW); Level of significance; number of expert (N).
Table 3.
CFA Factor Loading Statistics.
| The Standardized Factor Loading ( ) | Hypothesis Testing | |||||||
|---|---|---|---|---|---|---|---|---|
| Element | ECDm | HEDm | ENDm | SODm | Estimate | S.E. | C.r. | p |
| HHD | 0.73 | 1.17 | 0.11 | 9.64 | *** | |||
| ECG | 0.80 | 0.96 | 0.11 | 9.46 | *** | |||
| CEM | 0.77 | 0.96 | 0.10 | 9.46 | *** | |||
| PR | 0.74 | 1.09 | 0.12 | 9.43 | *** | |||
| CDC | 0.75 | 0.95 | 0.09 | 10.02 | *** | |||
| HR | 0.78 | 1.00 | 0.10 | 10.02 | *** | |||
| HS | 0.67 | 1.03 | 0.09 | 8.92 | *** | |||
| NCDs | 0.76 | 0.97 | 0.10 | 9.47 | *** | |||
| APM | 0.67 | 1.02 | 0.08 | 12.58 | *** | |||
| ERM | 0.68 | 0.98 | 0.08 | 12.58 | *** | |||
| WM | 0.81 | 1.19 | 0.10 | 12.17 | *** | |||
| PNA | 0.76 | 1.19 | 0.10 | 11.94 | *** | |||
| SS | 0.69 | 0.86 | 0.10 | 8.62 | *** | |||
| HP | 0.85 | 0.96 | 0.13 | 8.62 | *** | |||
| HSS | 0.73 | 0.88 | 0.11 | 9.03 | *** | |||
Notes: Standard Error (S.E.); Critical Ratio (C.r.); Unstandardized. p < 0.001 for all coefficients (***).
Table 4.
Measurement of model fit.
| Index | Recommended Value | Estimated Value | Type | Ref. |
|---|---|---|---|---|
| CMIN/DF | 3 good 5 permissible | 1.44 good | Absolute fit | [56] |
| RMSEA | 0.05 good –0.08 moderate 0.8 bad | 0.033 good | Absolute fit | [58] |
| GFI | good acceptable | 0.96 good | Absolute fit | [56] |
| AGFI | good | 0.94 good | Absolute fit | [58] |
| RMR | Close to 0 | 0.025 | Absolute fit | [56] |
| NFI | good acceptable | 0.94 acceptable | Incremental fit | [56] |
| CFI | 0.98 good | Incremental fit | [56] | |
| TLI | good acceptable | 0.97 good | Incremental fit | [56] |
| IFI | good | 0.98 good | Incremental fit | [57] |
| P | significant | 0.00 | - | [57] |
| CMIN | 0 | 105.3 | - | [57] |
| DF | - | 73 | - | - |
Table 5.
The HSM validity and reliability.
| Dimensions/Element | C.R. | AVE. | C.A. | |||||
|---|---|---|---|---|---|---|---|---|
| The HSM | ---> | ECDm | 0.77 | 0.59 | 0.41 | 0.85 * | 0.59 * | 0.87 * |
| ---> | HEDm | 0.84 | 0.71 | 0.29 | ||||
| ---> | ENDm | 0.76 | 0.58 | 0.42 | ||||
| ---> | SODm | 0.70 | 0.49 | 0.51 | ||||
| ECDm | ---> | HHD | 0.73 | 0.53 | 0.47 | 0.85 * | 0.58 * | 0.78 * |
| ---> | ECG | 0.80 | 0.64 | 0.36 | ||||
| ---> | CEM | 0.77 | 0.59 | 0.41 | ||||
| ---> | PR | 0.74 | 0.55 | 0.45 | ||||
| HEDm | ---> | CDC | 0.75 | 0.56 | 0.44 | 0.83 * | 0.55 * | 0.77 * |
| ---> | HR | 0.78 | 0.61 | 0.39 | ||||
| ---> | HS | 0.67 | 0.45 | 0.55 | ||||
| ---> | NCDs | 0.76 | 0.58 | 0.42 | ||||
| ENDm | ---> | APM | 0.67 | 0.45 | 0.55 | 0.82 * | 0.54 * | 0.83 * |
| ---> | ERM | 0.68 | 0.46 | 0.54 | ||||
| ---> | WM | 0.81 | 0.66 | 0.34 | ||||
| ---> | PNA | 0.76 | 0.58 | 0.42 | ||||
| SODm | ---> | SS | 0.69 | 0.48 | 0.52 | 0.80 * | 0.58 * | 0.79 * |
| ---> | HP | 0.85 | 0.72 | 0.28 | ||||
| ---> | HSS | 0.73 | 0.53 | 0.47 | ||||
Note: the standardized factor loading (); variance (); the error variance 1 − (); Composite (construct) Reliability (C.R.); Average Variance Extracted (AVE.); Cronbach’s Alpha (C.A.); Acceptable (*).
Table 6.
The validity test of the interrelated dimensions.
| Relation between Dimensions | Cor. | MSV | Cov. | S.E. | C.R. | p | ||
|---|---|---|---|---|---|---|---|---|
| HEDm | <--> | SODm | 0.71 | 0.50 | 0.29 | 0.03 | 8.88 | *** |
| ECDm | <--> | SODm | 0.51 | 0.26 | 0.21 | 0.03 | 6.91 | *** |
| ENDm | <--> | SODm | 0.53 | 0.28 | 0.28 | 0.04 | 7.12 | *** |
| ECDm | <--> | ENDm | 0.67 | 0.45 | 0.38 | 0.04 | 9.17 | *** |
| HEDm | <--> | ENDm | 0.61 | 0.37 | 0.36 | 0.04 | 8.58 | *** |
| ECDm | <--> | HEDm | 0.68 | 0.46 | 0.3 | 0.03 | 8.86 | *** |
Notes: Correlations (Cor.); Covariances (Cov.); Maximum Shared Variance (MSV); Standard error (S.E); Critical ratio (C.R.); Unstandardized. p < 0.001 for all coefficients significant (***).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ritmak, N.; Rattanawong, W.; Vongmanee, V. A New Dimension of Health Sustainability Model after Pandemic Crisis Using Structural Equation Model. Sustainability 2023, 15, 1616. https://doi.org/10.3390/su15021616
AMA Style
Ritmak N, Rattanawong W, Vongmanee V. A New Dimension of Health Sustainability Model after Pandemic Crisis Using Structural Equation Model. Sustainability. 2023; 15(2):1616. https://doi.org/10.3390/su15021616
Chicago/Turabian StyleRitmak, Nutthawut, Wanchai Rattanawong, and Varin Vongmanee. 2023. "A New Dimension of Health Sustainability Model after Pandemic Crisis Using Structural Equation Model" Sustainability 15, no. 2: 1616. https://doi.org/10.3390/su15021616
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.