

The Acute and Long-Term Effects of Olympic Karate Kata Training on Structural and Functional Changes in the Body Posture of Polish National Team Athletes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
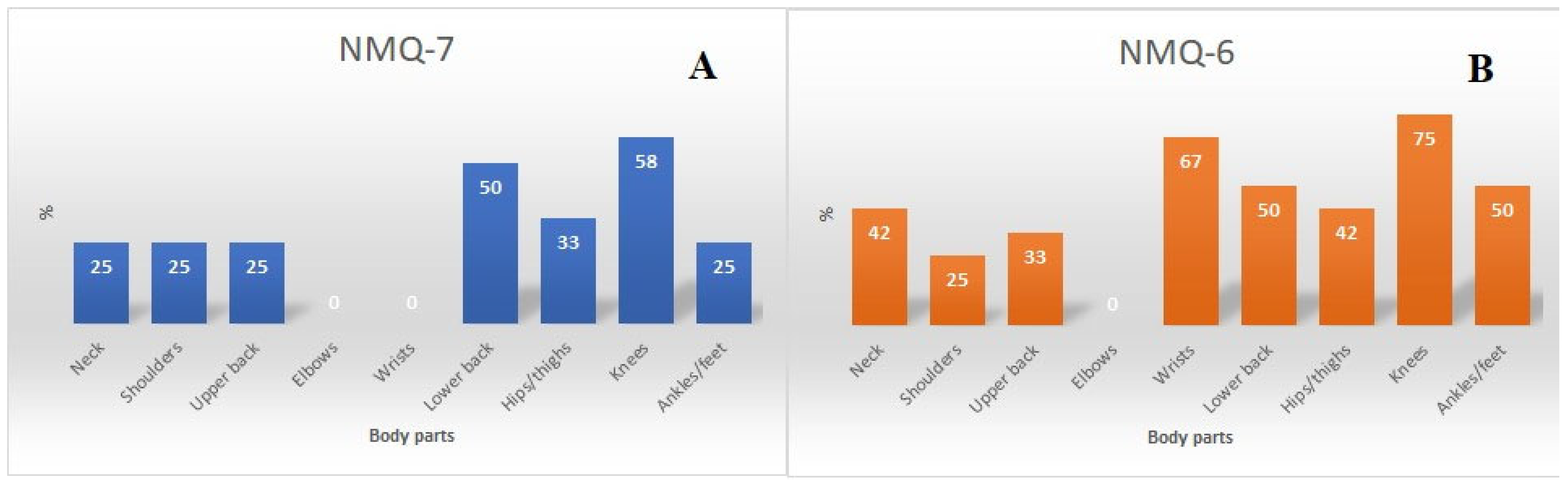
2.3. Prevalence and Locations of Musculoskeletal Pain
2.4. Anthropometric Measurements
2.5. Range of Motion Testing (microFET-3 Device)
2.6. Sagittal Spinal Curvatures and Spinal Mobility Testing
2.7. Natural Experiment
2.8. Statistical Analysis
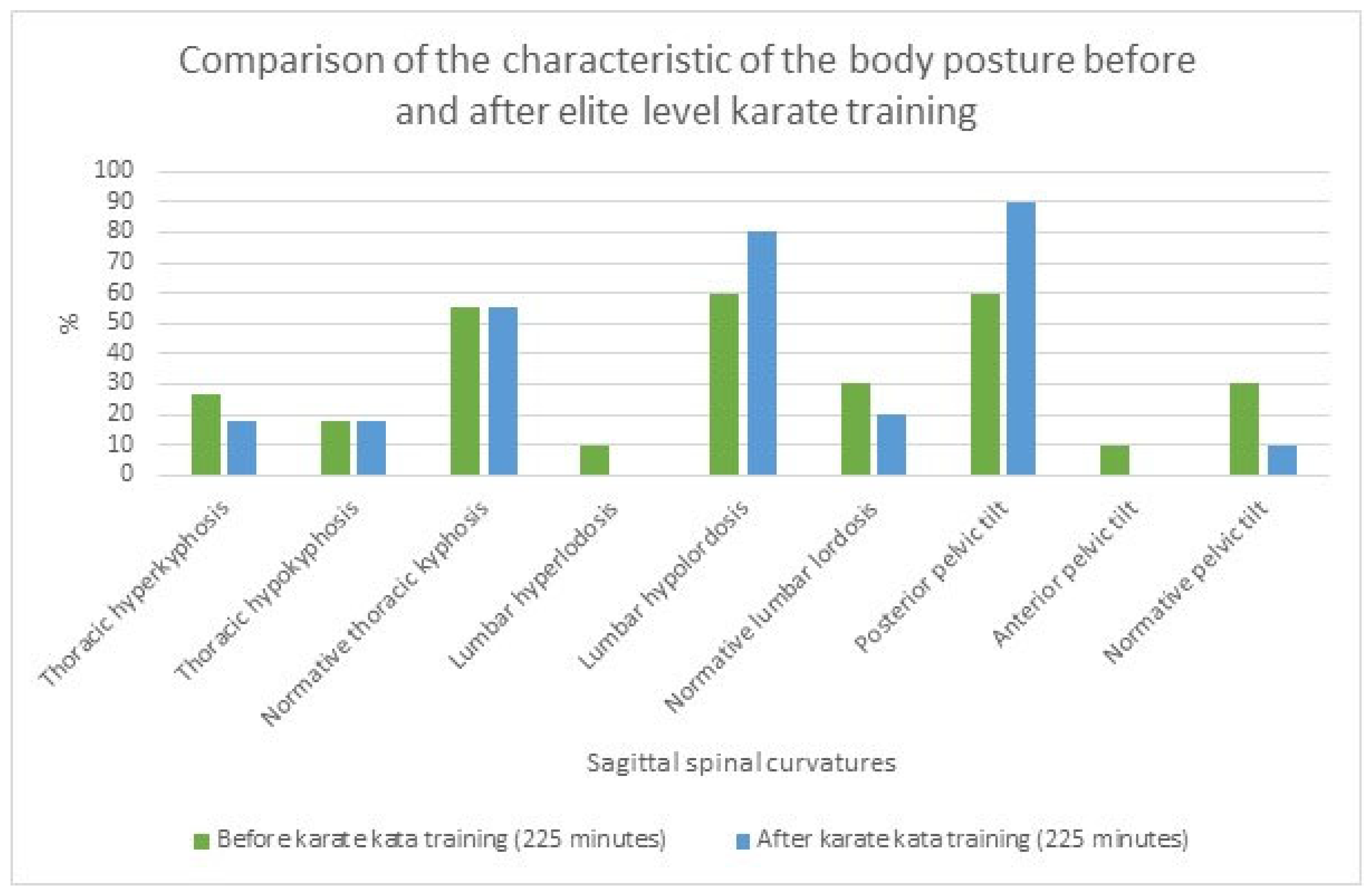
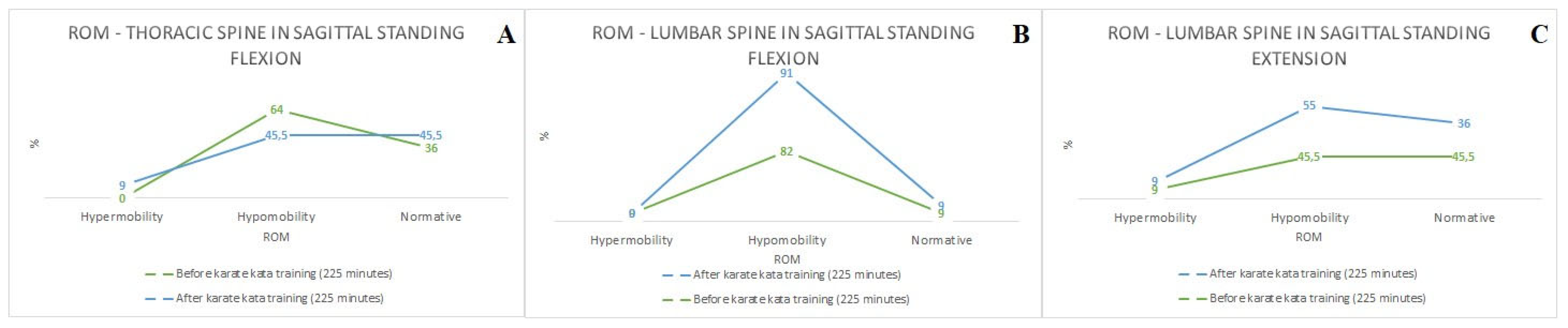
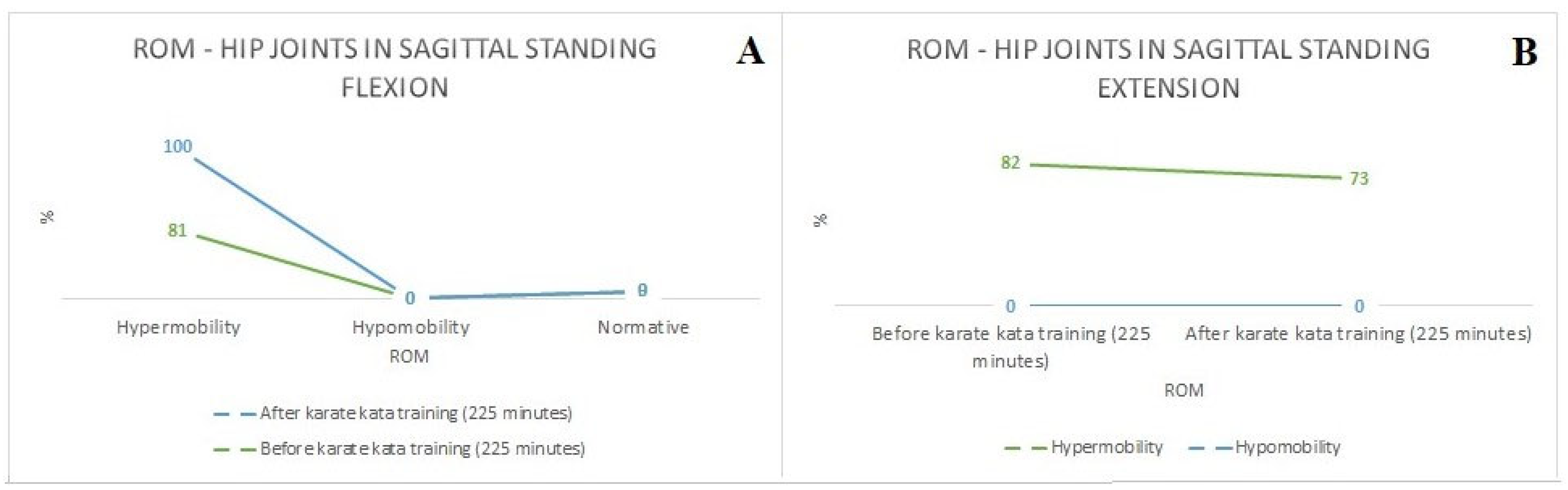
3. Results
4. Discussion
Limitations and Strengths of the Study
5. Conclusions
- Elite-level karate (Shotokan style) kata training induces both acute adaptations and long-term structural changes in the position and ROM of the lumbar spine and pelvic tilt;
- Kata stances and their movement pattern seem to be related to the occurrence of disturbances in the ROM of the internal and external rotations of the hip joints and decreased depth of lumbar lordosis, pelvic tilt, and their ROM;
- The locations of the long-term musculoskeletal complaints (assessed using the NMQ-6) seem to result from compensatory changes that occur in the musculoskeletal structures as a result of elite-level kata training;
- Mobility exercises for both internal and external rotation of the humeral and hip joints should be implemented in order to minimalize the risk of musculoskeletal complaints and injury of the abovementioned joints. Simultaneously applying mobility exercises for the lumbar spine could reduce the incidence of low back pain and disfunctions of the lumbar segments of the spine in karate athletes.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stamenković, A.; Manić, M.; Roklicer, R.; Trivić, T.; Malović, P.; Drid, P. Effects of Participating in Martial Arts in Children: A Systematic Review. Children 2022, 9, 1203. [Google Scholar] [CrossRef]
- Raczek, J. Antropomotoryka. In Teoria Motoryczności Człowieka w Zarysie; PZWL–Wydawnictwo Lekarskie: Warsaw, Poland, 2010; ISBN 9788320038453. [Google Scholar]
- Koropanovski, N.; Berjan, B.; Bozic, P.R.; Pazin, N.; Sanader, A.; Jovanovic, S.; Jaric, S. Anthropometric and physical performance profiles of elite karate kumite and kata competitors. J. Hum. Kinet. 2011, 30, 107–114. [Google Scholar] [CrossRef]
- Imamura, H.; Yoshimura, Y.; Uchida, K.; Nishimura, S.; Nakazawa, A.T. Maximal oxygen uptake, body composition and strength of highly competitive and novice karate practitioners. Appl. Hum. Sci. 1998, 17, 215–218. [Google Scholar] [CrossRef]
- Statutes and Rules of the World Karate Federation|WKF. Available online: https://www.wkf.net/structure-statutes-rules (accessed on 15 November 2023).
- Doria, C.; Veicsteinas, A.; Limonta, E.; Maggioni, M.A.; Aschieri, P.; Eusebi, F.; Fanò, G.; Pietrangelo, T. Energetics of karate (kata and kumite techniques) in top-level athletes. Eur. J. Appl. Physiol. 2009, 107, 603–610. [Google Scholar] [CrossRef]
- Chaabène, H.; Franchini, E.; Sterkowicz, S.; Tabben, M.; Hachana, Y.; Chamari, K. Physiological responses to karate specific activities. Sci. Sports 2015, 30, 179–187. [Google Scholar] [CrossRef]
- Tabben, M.; Conte, D.; Haddad, M.; Chamari, K. Technical and Tactical Discriminatory Factors Between Winners and Defeated Elite Karate Athletes. Int. J. Sports Physiol. Perform. 2019, 14, 563–568. [Google Scholar] [CrossRef]
- Drzał-Grabiec, J.; Truszczyńska, A. Evaluation of selected postural parameters in children who practice kyokushin karate. Biomed. Hum. Kinet. 2014, 6. [Google Scholar] [CrossRef]
- Carini, F.; Mazzola, M.; Fici, C.; Palmeri, S.; Messina, M.; Damiani, P.; Tomasello, G. Posture and posturology, anatomical and physiological profiles: Overview and current state of art. Acta Biomed. 2017, 88, 11–16. [Google Scholar]
- Zwierzchowska, A.; Tuz, J. Evaluation of The Impact of Sagittal Spinal Curvatures on Musculoskeletal Disorders in Young People/Ocena Wplywu Krzywizn Kregoslupa W Plaszczyznie Strzalkowej Na Dolegliwosci Miesniowo-Szkieletowe U Mlodych Osob. Med. Pr. 2018, 69, 29–37. [Google Scholar]
- Lugo, R.; Kung, P.; Ma, C.B. Shoulder biomechanics. Eur. J. Radiol. 2008, 68, 16–24. [Google Scholar] [CrossRef]
- Zwierzchowska, A.; Gawel, E.; Karpinski, J.; Maszczyk, A.; Zebrowska, A. The effect of swimming on the body posture, range of motion and musculoskeletal pain in elite para and able-bodied swimmers. BMC Sports Sci. Med. Rehabil. 2023, 15, 122. [Google Scholar] [CrossRef]
- Zwierzchowska, A.; Gaweł, E.; Maszczyk, A.; Roczniok, R. The importance of extrinsic and intrinsic compensatory mechanisms to body posture of competitive athletes a systematic review and meta-analysis. Sci. Rep. 2022, 12, 8808. [Google Scholar] [CrossRef]
- Hawrylak, A.; Chromik, K.; Barczyk-Pawelec, K.; Demczuk-Włodarczyk, E. The spine mobility of karate master class contenstants. Arch. Budo 2017, 13, 350–434. [Google Scholar]
- Katarzyna, W.C.; Ewa, S.; Agnieszka, G.; Mirosław, M.; Marta, N.; Paweł, O.; Iwona, T.B. Evaluation of Anterior-Posterior Spine Curvatures and Incidence of Sagittal Defects in Children and Adolescents Practicing Traditional Karate. Biomed Res. Int. 2019, 2019, 9868473. [Google Scholar] [CrossRef]
- Brzęk, A.; Knapik, A.; Brzęk, B.; Niemiec, P.; Przygodzki, P.; Plinta, R.; Szyluk, K. Evaluation of Posturometric Parameters in Children and Youth Who Practice Karate: Prospective Cross-Sectional Study. Biomed Res. Int. 2022, 2022, 5432743. [Google Scholar] [CrossRef]
- Hadad, A.; Ganz, N.; Intrator, N.; Maimon, N.; Molcho, L.; Hausdorff, J.M. Postural control in karate practitioners: Does practice make perfect? Gait Posture 2020, 77, 218–224. [Google Scholar] [CrossRef]
- Ansari, S.; Hosseinkhanzadeh, A.A.; AdibSaber, F.; Shojaei, M.; Daneshfar, A. The Effects of Aquatic Versus Kata Techniques Training on Static and Dynamic Balance in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2021, 51, 3180–3186. [Google Scholar] [CrossRef]
- Ryguła, I. Research Process in Sport Sciences [Proces Badawczy w Naukach o Sporcie]; AWF Katowice: Katowice, Poland, 2003; ISBN 83-87478-60-1. [Google Scholar]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sørensen, F.; Andersson, G.; Jørgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- Zwierzchowska, A.; Gawel, E.; Celebanska, D.; Rosolek, B. Musculoskeletal pain as the effect of internal compensatory mechanisms on structural and functional changes in body build and posture in elite Polish sitting volleyball players. BMC Sports Sci. Med. Rehabil. 2022, 14, 49. [Google Scholar] [CrossRef]
- Józefowski, P. Functional Diagnostics of the Musculoskeletal System with the Elements of Walking Verticalization and Reeducation [Diagnistyka Czynnościowa Narządu Ruchu z Elementami Pionizacji i Reedukacji Chodu]; MedPharm Polska: Wrocław, Poland, 2013; ISBN 978-83-7846-023-7. [Google Scholar]
- Frost, J. Introduction to Statistics: An Intuitive Guide for Analyzing Data and Unlocking Doveries; Statistics by Jim Publishing: State College, PA, USA, 2020; p. 255. ISBN 1735431109. [Google Scholar]
- Amiri Khorasani, A.; Amiri Khorasani, M.T.; Mohammadipour, F. Comparison of the Maximum Angular Velocity of Lower Limb Joints in Different Methods of Zenkutsu-dachi in Karate. J. Sport Biomech. 2020, 6, 12–21. [Google Scholar] [CrossRef]
- Cazeau, C.; Courtonne, C.; Delacroix, S.; Lescure, Y.; Piat, C.; Stiglitz, Y. Biomechanical study comparing the energy cost of human bipedalism versus zenkutsu-dachi stepping of a karateka. Int. Orthop. 2021, 45, 2435–2443. [Google Scholar] [CrossRef] [PubMed]
- Bober, T.; Zawadzki, J. Biomechanika Układu Ruchu Człowieka; Wydawnictwo BK: Wrocław, Poland, 2003; ISBN 83-910251-3-6. [Google Scholar]
- Lisowska, A.; Fryzowicz, A.; Mączyński, J.; Ogurkowska, M. The ground reaction forces in basic stances in shotokan karate as an effective indicator in the prevention of lower limb pain in competitive athletes. Arch. Budo 2021, 17, 177–184. [Google Scholar]
- Polechoński, J.; Gaweł, D.; Niestrój-Jaworska, M. The influence of different stretching techniques on the mobility of hip joints of karate competitors. In Physical Activity and Functional Efficiency; Wydawnictwo Wydawnictwo Wyższa Vot School: Racibórz, Poland, 2018; pp. 17–43. ISBN 978-83-947623-9-1. [Google Scholar]
- Zayed, M.A.; Aly, M.A.R. Relationship between biomechanical parameters of lower limb and velocity of arm strike during punch Gyaku Zuki performance in karate. Int. J. Sports Sci. Arts 2018, 8, 62–70. [Google Scholar] [CrossRef]
- Hofmann, M.; Witte, K.; Emmermacher, P. Biomechanical analysis of fist punch gyaku-zuki in karate. In Proceedings of the ISBS Conference 2008, Seoul, Republic of Korea, 14–18 July 2008. [Google Scholar]
- Zago, M.; Codari, M.; Iaia, F.M.; Sforza, C. Multi-segmental movements as a function of experience in karate. J. Sports Sci. 2017, 35, 1515–1522. [Google Scholar] [CrossRef]
- Vando, S.; Filingeri, D.; Maurino, L.; Chaabène, H.; Bianco, A.; Salernitano, G.; Foti, C.; Padulo, J. Postural adaptations in preadolescent karate athletes due to a one week karate training cAMP. J. Hum. Kinet. 2013, 38, 45–52. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | WKF Karate Kata Athletes (n = 12; nF = 4, nM = 8) | WKF Karate Kata Athletes (n = 12; nF = 4, nM = 8) | WKF Karate Kata Athletes—Females (n = 4) | WKF Karate Kata Athletes—Males (n = 8) | WKF Karate Kata Athletes (Males vs. Females) |
|---|---|---|---|---|---|
| Mean ± SD | p-Value | Mean ± SD | Mean ± SD | p-Value | |
| Age (years) | 17.63 ± 3.36 | 0.26 | 16.25 ± 2.95 | 18.25 ± 3.15 | 0.36 |
| Body Mass (kg) | 62.27 ± 9.87 | 0.41 | 54.75 ± 4.76 | 65.75 ± 9.11 | 0.65 |
| Body Height (m) | 1.69 ± 0.06 | 0.27 | 1.66 ± 0.04 | 1.7 ± 0.07 | 0.24 |
| Hip Circumference (cm) | 90.64 ± 6.84 | 1.0 | 87.5 ± 5.36 | 92.13 ± 6.55 | 0.29 |
| Waist Circumference (cm) | 73.73 ± 6.9 | 0.11 | 69.25 ± 5.26 | 75.86 ± 6.09 | 0.12 |
| BMI | 21.65 ± 2.17 | 0.13 | 19.95 ± 1.04 | 22.54 ± 1.93 | 0.05 |
| BAI (%) | 17.73 ± 2.18 | 0.08 | 17.29 ± 2.57 | 18.03 ± 1.76 | 0.6 |
| WHR | 0.81 ± 0.06 | 0.63 | 0.79 ± 0.06 | 0.82 ± 0.05 | 0.4 |
| Karate training experience (years) | 10.82 ± 2.8 | 0.66 | 9.25 ± 1.92 | 11.63 ± 2.64 | 0.18 |
| Number of karate kata training sessions per week | 4.2 ± 1.19 | 0.04 | 4.5 ± 1.12 | 4.5 ± 1.73 | 1.0 |
| Number of strength and conditioning sessions per week | 3.18 ± 1.53 | 0.005 | 4.0 ± 2.12 | 2.75 ± 0.66 | 0.19 |
| ROM OF THE HIP JOINT | ||
|---|---|---|
| ROM Trial | Initial Position | Movement |
| Flexion (A) * | Supine position, both lower limbs straight, upper limbs in the anatomical position | Upright movement of the tested limb up to the maximal ROM, non-tested limb on the floor |
| Flexion (B) ** | Supine position, tested lower limb flexed in the knee joint, non-tested limb straight, upper limbs in the anatomical position | Flexion of the tested limb towards the chest up to the maximal ROM |
| Extension | Prone position, both lower limbs straight, upper limbs crossed, under the forehead | Upright movement of the tested limb up to the maximal ROM, non-tested limb on the floor |
| External rotation | Sitting position, both lower limbs over the floor, upper limbs crossed on the chest | Maximal external rotational movement |
| Internal rotation | Sitting position, both lower limbs over the floor, upper limbs crossed on the chest | Maximal external rotational movement |
| ROM OF THE HUMERAL JOINT | ||
| Flexion | Habitual standing position, upper limbs straight | Upright movement of the tested limb up to the maximal ROM |
| Extension | Prone position, both upper and lower limbs straight, forehead touching the mat | Upright movement of the tested limb up to the maximal ROM |
| External rotation | Supine position, both lower limbs straight, tested upper limb upright, flexed at 90 degrees, non-tested upper limb in the anatomical position | Maximal external rotational movement |
| Internal rotation | As above | Maximal internal rotational movement |
| Spinal Curvature Measurements: Sagittal Plane | SG (n = 11 *) Mean ± SD (°) (First Measurement) | p-Value | p-Value (Males and Females) | SG (n = 12) Mean ± SD (°) (Second Measurement) | p-Value | p-Value (Males and Females) | Correlation | R–Value (p < 0.001 *** p < 0.01 ** p < 0.05 *) |
|---|---|---|---|---|---|---|---|---|
| THa—sagittal standing | 37.55 ± 14.15 | 0.98 | 0.36 | 36.91 ± 8.75 | 0.48 | 0.39 | Pearson’s correlation | |
| THa—sagittal standing flexion | 44.27 ± 16.62 | 0.12 | 0.64 | 45.82 ± 17.23 | 0.33 | 0.69 | ROM—lumbar spine (1) and age | R = (−0.7) * |
| THa—sagittal standing extension | 27.82 ± 18.04 | 0.15 | 0.45 | 25.73 ± 9.8 | 0.66 | 0.96 | ROM—lumbar spine (1) and WC | R = (−0.7) * |
| LLa—sagittal standing **** | 17.8 ± 16.84 | 0.09 | 0.11 | 9.7 ± 9.34 | 0.01 | 0.65 | ROM—lumbar spine (1) and WHR | R = (−0.7) * |
| Lla—sagittal standing flexion | 30.91 ± 8.55 | 0.95 | 0.2 | 36.92 ± 12.63 | 0.67 | 0.5 | ROM—Incl (2) and BAI | R = 0.7 * |
| Lla—sagittal standing extension | 23.45 ± 15.2 | 0.19 | 0.86 | 12.82 ± 10.43 | 0.05 | 0.08 | Spearman’s rank order correlation | |
| Incl—sagittal standing **** SL—sagittal standing **** | 2.18 ± 1.59 445.4 ± 34.08 | 0.47 0.64 | 0.17 0.72 | 1.64 ± 1.67 429.91 ± 49.75 | 0.04 0.65 | 0.3 0.76 | LLa (1)—sagittal standing and Incl (2) sagittal standing | R = 0.7 * |
| Incl—sagittal standing flexion SL—sagittal standing flexion | 127.82 ± 8.47 536.73 ± 51.76 | 0.02 0.48 | 0.4 0.21 | 135.18 ± 7.76 528.27 ± 63.77 | 0.001 0.65 | 0.35 0.5 | ROM—lumbar spine (1) and karate training sessions/week | R = (−0.6) * |
| Incl—sagittal standing extension SL—sagittal standing extension | 51.0 ± 13.03 397.91 ± 35.08 | 0.87 0.7 | 0.61 0.6 | 59.45 ± 11.96 365.91 ± 59.82 | 0.78 0.55 | 0.82 0.09 | ||
| ROM in the sagittal plane (thoracic spine) | 20.27 ± 11.69 | 0.83 | 0.2 | 23.18 ± 18.25 | 0.11 | 0.72 | ||
| ROM in the sagittal plane (lumbar spine) | 53.64 ± 12.51 | 0.31 | 0.6 | 48.09 ± 14.32 | 0.97 | 0.09 | ||
| ROM in the sagittal plane (inclination) | 180.64 ± 18.0 | 0.17 | 0.51 | 194.64 ± 16.76 | 0.07 | 0.75 |
| ROM OF THE HIP JOINT | ||||||||
|---|---|---|---|---|---|---|---|---|
| ROM Trial and ISOM Normal Values (°) | Mean ± SD (LJ) (°) | p-Value | p-Value (Males and Females) | Mean ± SD (RJ) (°) | p-Value | p-Value (Males and Females) | Pearson’s Correlation | R-Value (p < 0.001 *** p < 0.01 ** p < 0.05 *) |
| Flexion (A) (125°) | 107.33 ± 10.14 | 0.27 | 0.01 | 107.5 ± 14.2 | 0.99 | 0.24 | RJ flexion (A) (hip) and RJ flexion (humeral) | R = 0.7 * |
| Flexion (B) (125°) | 122.0.3 ± 8.67 | 0.41 | 0.34 | 125.5.38± | 0.54 | 0.83 | LJ flexion (B) (hip) and RJ internal rotation (humeral) | R = 0.6 * |
| Extension (15°) | 18.94 ± 4.7 | 0.001 | 0.78 | 18.41 ± 5.58 | 0.14 | 0.77 | RJ flexion (B) (hip) and age | R = (−0.6) * |
| External rotation (45°) | 33.39 ± 9.53 | 0.07 | 0.75 | 29.5 ± 7.24 | 0.3 | 0.46 | RJ flexion (B) (hip) and karate training experience | R = (−0.6) * |
| Internal rotation (45°) | 25.33 ± 7.88 | 0.39 | 0.76 | 26.75 ± 9.63 | 0.06 | 0.34 | RJ internal rotation (hip) and BH | R = (−0.6) * |
| ROM OF THE HUMERAL JOINT | RJ internal rotation (hip) and LJ extension (humeral) | R = 0.6 * | ||||||
| Flexion (170°) | 174.53 ± 2.66 | 0.88 | 0.66 | 172.67 ± 3.76 | 0.92 | 0.89 | RJ internal rotation (hip) and RJ extension (humeral) | R = 0.7 * |
| Extension (50°) | 45.53 ± 10.17 | 0.01 | 0.51 | 43.89 ± 7.66 | 0.94 | 0.21 | ROM THa (1) and LJ internal rotation (hip) | R = 0.6 * |
| External rotation (90°) | 86.55 ± 5.96 | 0.001 | 0.08 | 88.5 ± 3.38 | 0.001 | 0.17 | ROM LLa (1) and RJ flexion (B) (hip) | R = 0.7 * |
| Internal rotation (80°) | 65.14 ± 12.11 | 0.45 | 0.12 | 61.67 ± 12.84 | 0.27 | 0.29 | ROM Incl (1) and RJ internal rotation (humeral) | R = (−0.6) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaweł, E.; Zwierzchowska, A. The Acute and Long-Term Effects of Olympic Karate Kata Training on Structural and Functional Changes in the Body Posture of Polish National Team Athletes. Sports 2024, 12, 55. https://doi.org/10.3390/sports12020055
Gaweł E, Zwierzchowska A. The Acute and Long-Term Effects of Olympic Karate Kata Training on Structural and Functional Changes in the Body Posture of Polish National Team Athletes. Sports. 2024; 12(2):55. https://doi.org/10.3390/sports12020055
Chicago/Turabian StyleGaweł, Eliza, and Anna Zwierzchowska. 2024. "The Acute and Long-Term Effects of Olympic Karate Kata Training on Structural and Functional Changes in the Body Posture of Polish National Team Athletes" Sports 12, no. 2: 55. https://doi.org/10.3390/sports12020055