

The Impact of an Outdoor Motor–Cognitive Exercise Programme on the Health Outcomes of Older Adults in Community Settings: A Pilot and Feasibility Study


Abstract
:1. Introduction
1.1. Promoting and Maintaining Health in Older Age through Physical Activity
1.2. Influencing Factors and Suitable Settings for Implementing Regular Physical Activity in Old Age
1.3. Reflection and Consequences
- What impact does a 12-week outdoor motor–cognitive exercise programme have on OAs’ physical and cognitive function?
- Are there any age- and sex-related differences in terms of the motor–cognitive exercise programme’s impact?
- How is the feasibility of and satisfaction with the outdoor motor–cognitive exercise programme within the target group?
2. Methodological Approach
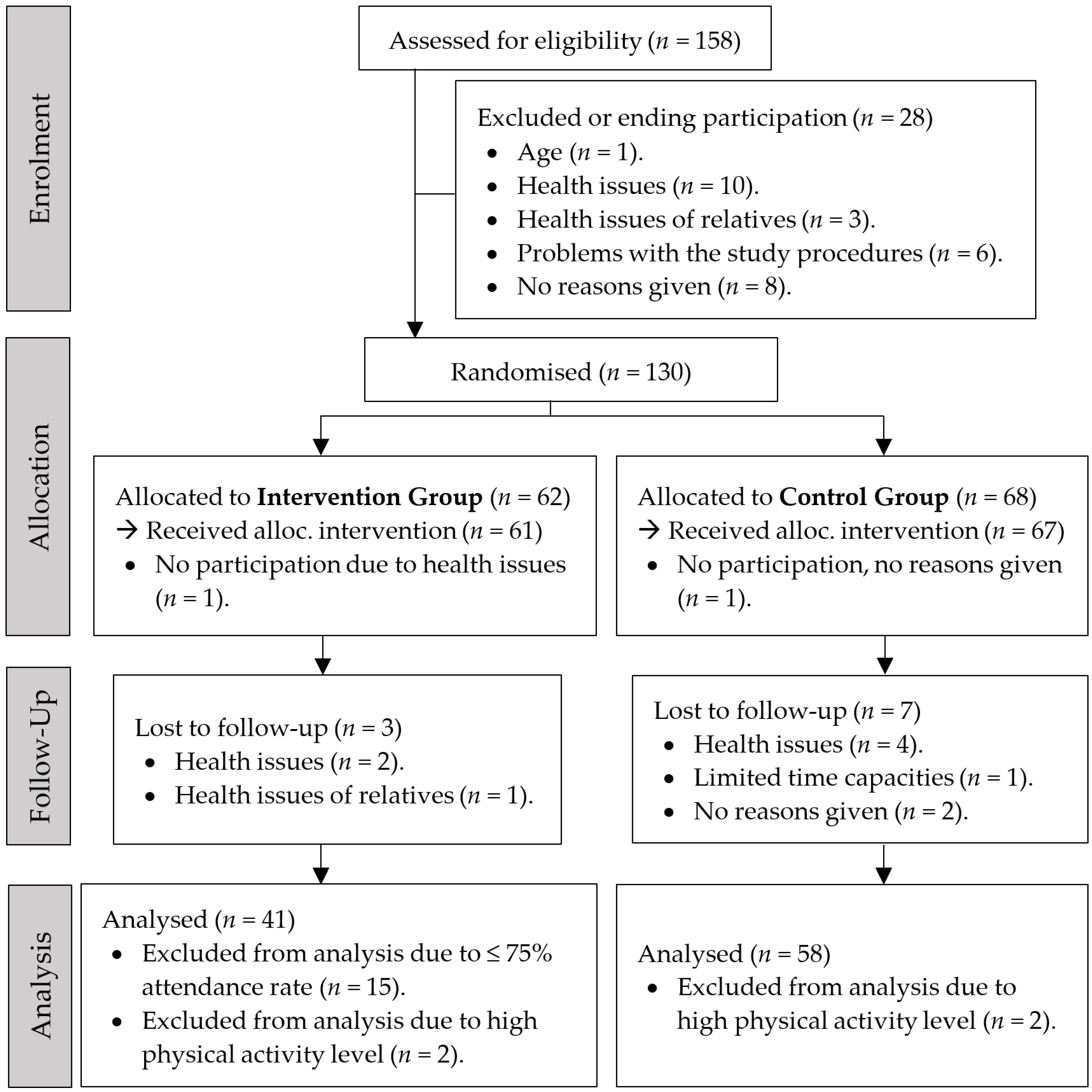
2.1. Trial Design
2.2. Sample Size Estimate/Power Calculations
2.3. Study Setting and Participants
2.4. Randomisation and Assignment to Intervention Group
2.5. Characteristics of Participants
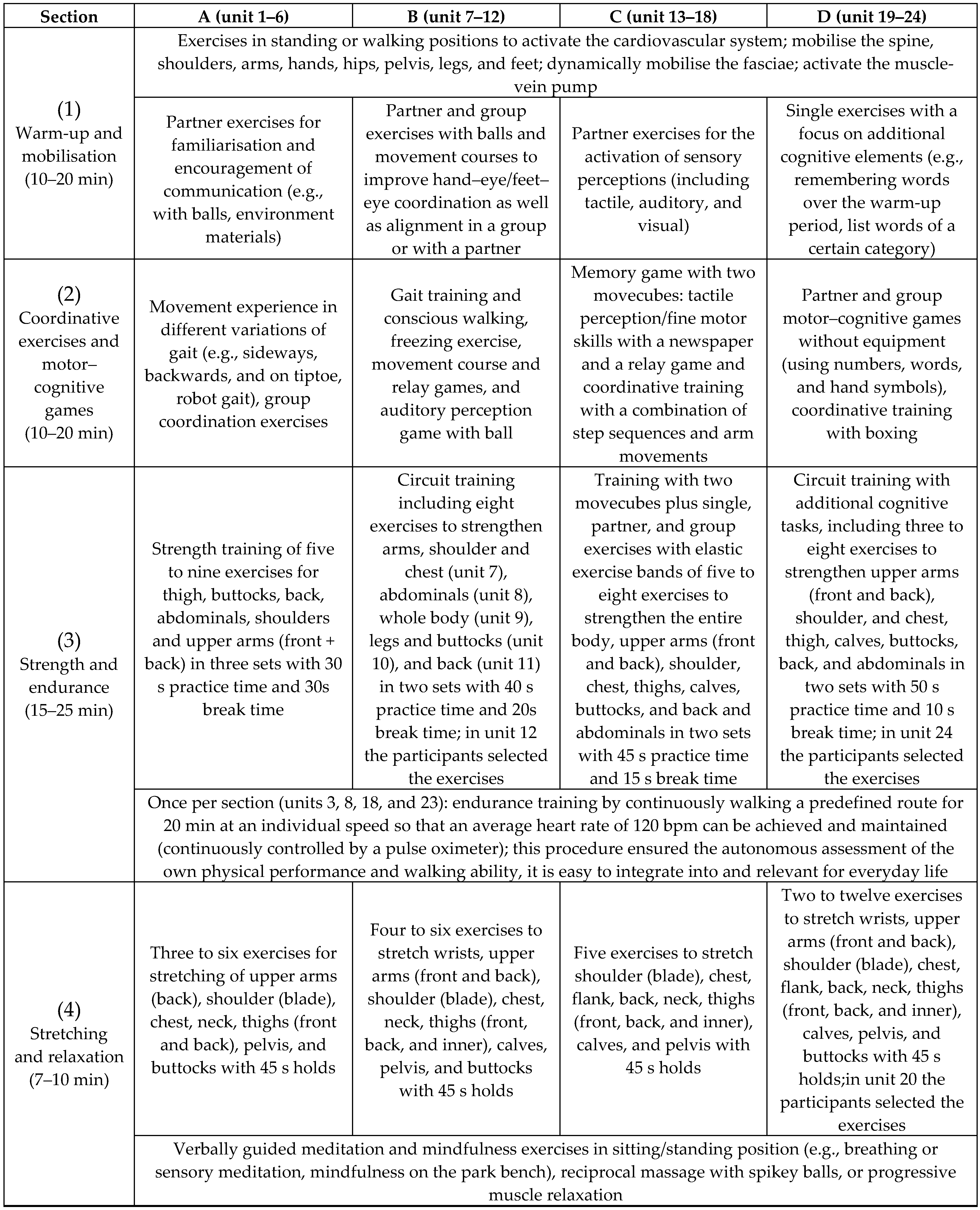
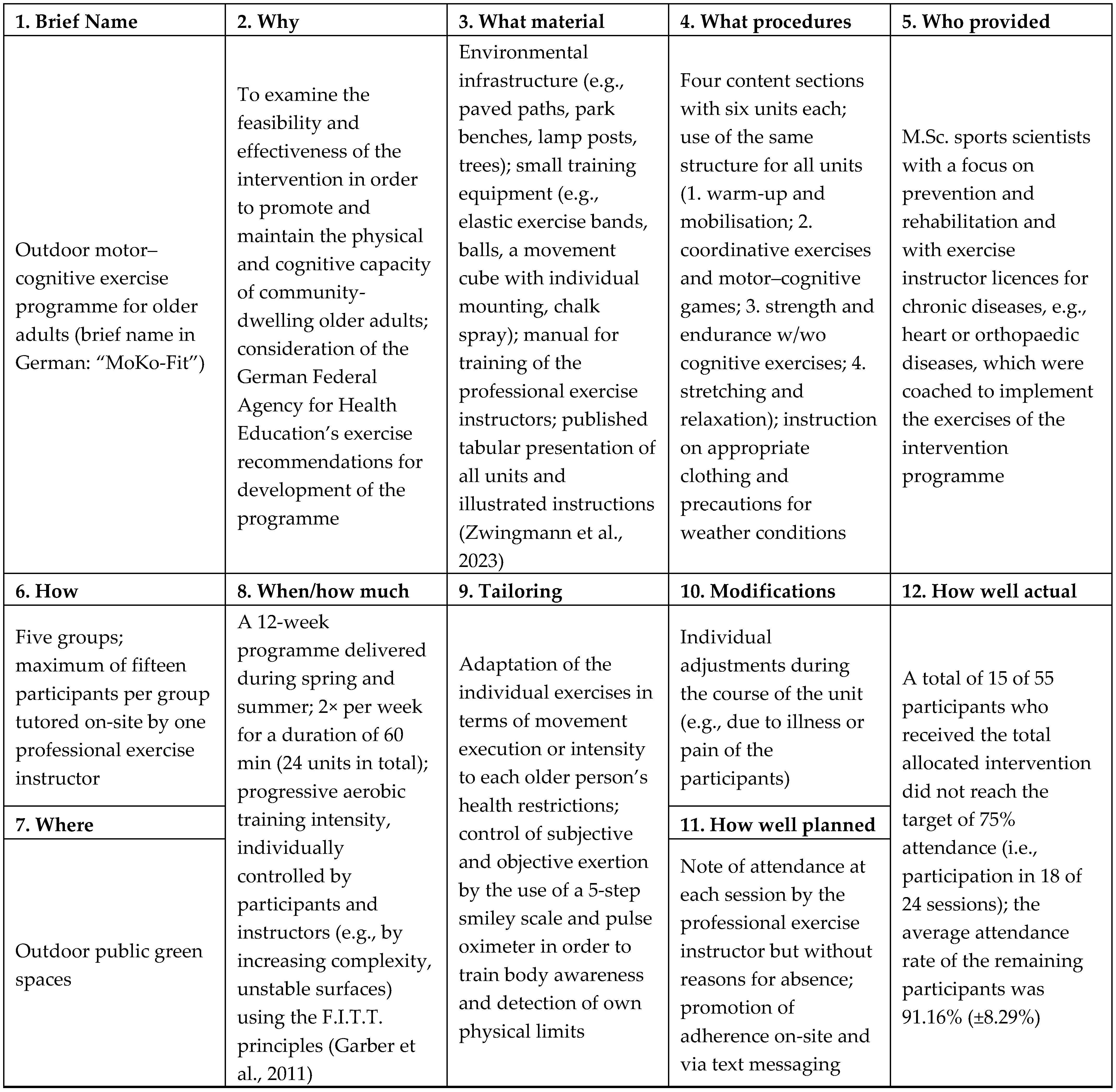
2.6. Design and Procedure of Intervention
2.7. Outcome Measures and Analyses
2.7.1. Procedure of Data Collection
2.7.2. Demographic, Feasibility, Psychosocial, Physical, and Cognitive Outcomes
2.8. Statistical Analysis
3. Results
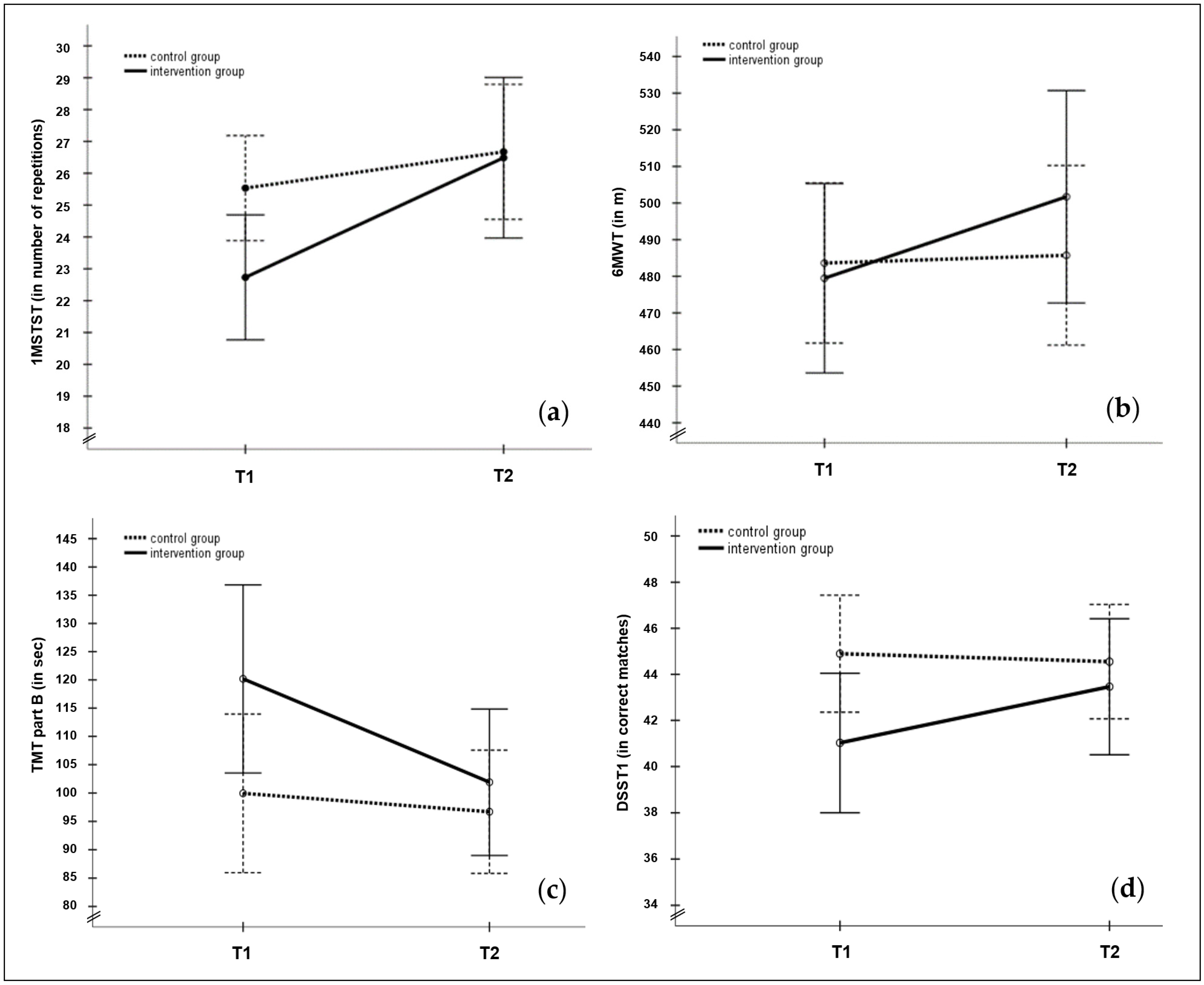
3.1. Functional Performance of the Lower Limbs
3.2. Functional Exercise Capacity
3.3. Hand Grip Strength
3.4. Neurocognitive Performance
3.5. Memory
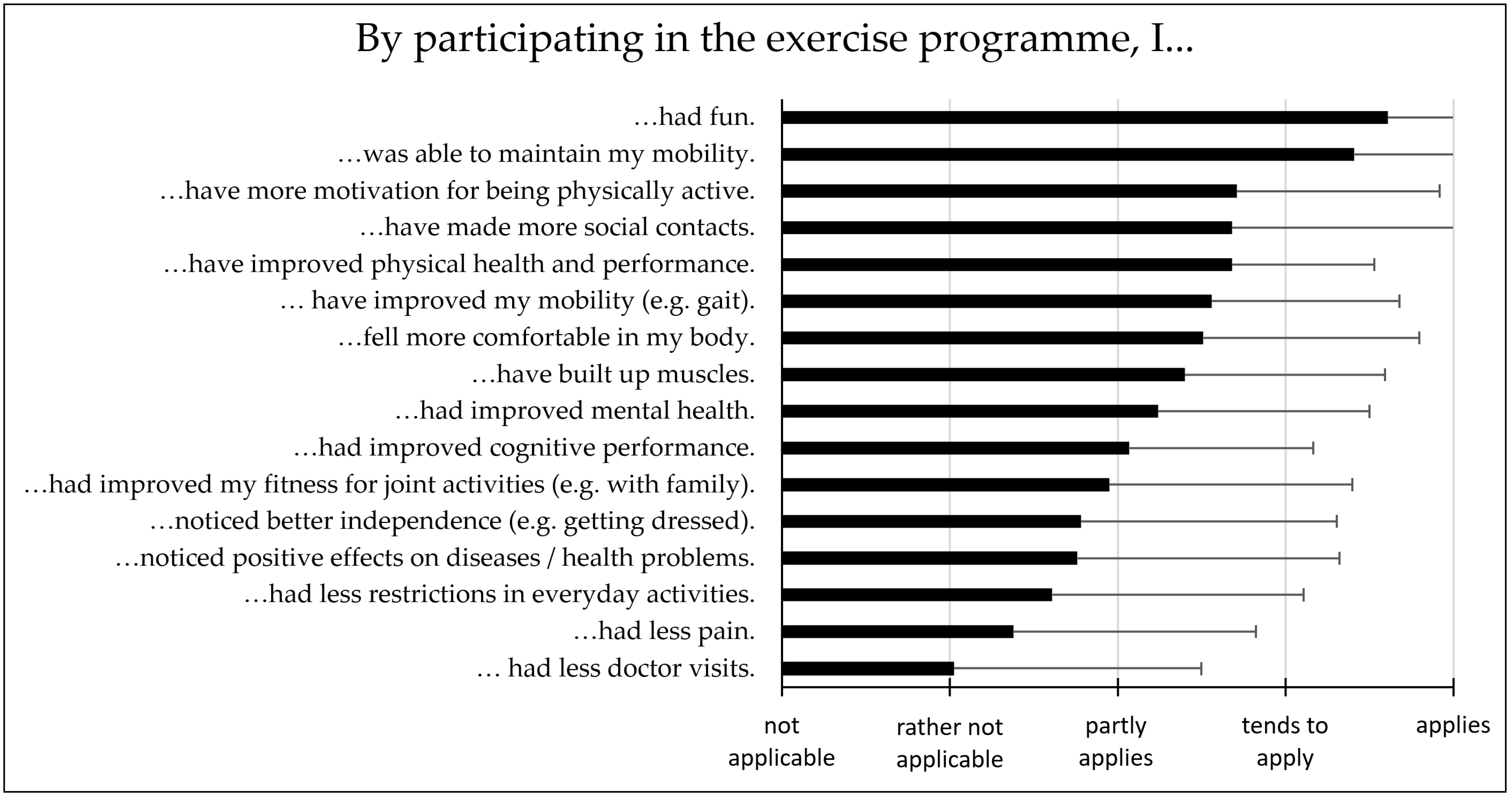
3.6. Feasibility
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Functional performance of the lower limbs (1MSTST; number of repetitions) | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | male | 16 | 23.56 ± 4.89 | 27.38 ± 10.28 | 3.724 | 0.061 | 0.087 | ||||
| female | 25 | 22.20 ± 5.39 | 25.92 ± 7.60 | 5.540 | 0.024 * | 0.124 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 0.660 | 0.421 | 0.017 | 0.271 | 0.606 | 0.007 | ||||||
| CG | male | 22 | 25.95 ± 5.78 | 26.00 ± 6.66 | 0.003 | 0.959 | 0.000 | ||||
| female | 36 | 25.28 ± 7.73 | 27.08 ± 8.42 | 6.771 | 0.012 * | 0.108 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 0.126 | 0.724 | 0.002 | 0.263 | 0.610 | 0.005 | ||||||
| Functional exercise capacity (6MWT; walking distance in m) | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | male | 15 | 505.13 ± 100.87 | 561.30 ± 73.06 | 5.547 | 0.024 * | 0.127 | ||||
| female | 25 | 464.07 ± 90.90 | 465.96 ± 106.45 | 0.000 | 0.919 | 0.000 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 1.763 | 0.192 | 0.044 | 9.341 | 0.004 * | 0.197 | ||||||
| CG | male | 21 | 506.41 ± 64.17 | 515.01 ± 65.70 | 0.612 | 0.437 | 0.011 | ||||
| female | 35 | 469.94 ± 73.06 | 468.15 ± 86.68 | 0.044 | 0.835 | 0.001 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 3.575 | 0.064 | 0.062 | 4.553 | 0.037 * | 0.078 | ||||||
| Hand grip strength (dominant hand; in kg) | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | male | 16 | 37.38 ± 8.78 | 36.08 ± 8.62 | 3.233 | 0.080 | 0.077 | ||||
| female | 25 | 21.96 ± 6.10 | 21.87 ± 5.86 | 0.001 | 0.881 | 0.001 | |||||
| F-statistics between: | F | F | p | ||||||||
| 44.147 | <0.001 ** | 0.531 | 39.584 | <0.001 ** | 0.504 | ||||||
| CG | male | 22 | 35.10 ± 7.47 | 34.28 ± 5.87 | 1.290 | 0.261 | 0.023 | ||||
| female | 35 | 21.42 ± 4.44 | 22.19 ± 4.19 | 1.824 | 0.182 | 0.032 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 75.440 | <0.001 ** | 0.578 | 82.401 | <0.001 ** | 0.600 | ||||||
| Neurocognitive performance: TMT A (in s) | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | male | 16 | 52.65 ± 21.00 | 47.97 ± 22.20 | 0.711 | 0.404 | 0.018 | ||||
| female | 25 | 51.63 ± 20.62 | 47.80 ± 14.48 | 0.742 | 0.394 | 0.019 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 0.024 | 0.879 | 0.001 | 0.001 | 0.977 | 0.000 | ||||||
| CG | male | 22 | 53.41 ± 22.14 | 59.30 ± 37.81 | 2.122 | 0.151 | 0.037 | ||||
| female | 36 | 41.18 ± 9.04 | 40.45 ± 12.40 | 0.053 | 0.819 | 0.001 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 8.699 | 0.005 * | 0.134 | 7.674 | 0.008 * | 0.121 | ||||||
| Neurocognitive performance: TMT B (in s) | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | male | 16 | 123.92 ± 89.47 | 107.50 ± 46.93 | 1.299 | 0.261 | 0.032 | ||||
| female | 25 | 117.79 ± 53.76 | 98.33 ± 32.92 | 2.851 | 0.099 | 0.068 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 0.075 | 0.785 | 0.002 | 0.541 | 0.466 | 0.014 | ||||||
| CG | male | 22 | 119.55 ± 45.88 | 118.55 ± 54.88 | 0.027 | 0.869 | 0.000 | ||||
| female | 36 | 87.98 ± 30.37 | 83.35 ± 28.58 | 0.962 | 0.331 | 0.017 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 9.967 | 0.003 * | 0.151 | 10.315 | 0.002 * | 0.156 | ||||||
| Neurocognitive performance: TMT B/A ratio | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | male | 16 | 2.44 ± 1.26 | 2.31 ± 0.68 | 0.100 | 0.754 | 0.003 | ||||
| female | 25 | 2.49 ± 1.48 | 2.21 ± 0.98 | 0.690 | 0.411 | 0.017 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 0.009 | 0.924 | 0.000 | 0.134 | 0.716 | 0.003 | ||||||
| CG | male | 22 | 2.38 ± 0.89 | 2.14 ± 0.63 | 2.086 | 0.154 | 0.036 | ||||
| female | 36 | 2.16 ± 0.67 | 2.12 ± 0.62 | 0.085 | 0.771 | 0.002 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 1.159 | 0.286 | 0.020 | 0.010 | 0.923 | 0.000 | ||||||
| Neurocognitive performance: DSST1 (number of correct matches) | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | male | 16 | 40.31 ± 8.87 | 43.56 ± 10.77 | 8.049 | 0.007 * | 0.171 | ||||
| female | 25 | 41.48 ± 8.51 | 43.40 ± 9.08 | 4.389 | 0.043 * | 0.101 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 0.178 | 0.676 | 0.005 | 0.003 | 0.959 | 0.000 | ||||||
| CG | male | 22 | 40.27 ± 8.22 | 40.09 ± 9.60 | 0.019 | 0.892 | 0.000 | ||||
| female | 36 | 47.72 ± 10.84 | 47.28 ± 8.34 | 0.183 | 0.670 | 0.003 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 7.669 | 0.008 * | 0.120 | 9.011 | 0.004 * | 0.139 | ||||||
| Memory: DSST2 (number of correct matches) | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | male | 16 | 3.06 ± 1.29 | 3.81 ± 1.91 | 1.969 | 0.200 | 0.042 | ||||
| female | 25 | 3.40 ± 2.22 | 4.60 ± 2.63 | 6.783 | 0.013 * | 0.148 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 0.303 | 0.585 | 0.008 | 1.252 | 0.270 | 0.031 | ||||||
| CG | male | 22 | 3.73 ± 2.21 | 4.45 ± 2.44 | 5.600 | 0.021 * | 0.091 | ||||
| female | 36 | 4.67 ± 2.44 | 4.67 ± 2.18 | 0.000 | 1.000 | 0.000 | |||||
| F-statistics between: | F | p | F | p | |||||||
| 2.174 | 0.146 | 0.037 | 0.118 | 0.732 | 0.002 | ||||||
| Functional performance of the lower limbs (1MSTST; number of repetitions) | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | younger | 22 | 24.50 ± 5.47 | 28.27 ± 10.13 | 5.014 | 0.031 * | 0.114 | ||||
| older | 19 | 20.68 ± 4.16 | 24.42 ± 6.17 | 4.448 | 0.046 * | 0.098 | |||||
| F-statistics between | F | p | F | p | |||||||
| 6.161 | 0.017 * | 0.136 | 2.076 | 0.158 | 0.051 | ||||||
| CG | younger | 30 | 26.63 ± 7.72 | 28.47 ± 8.48 | 5.745 | 0.020 * | 0.093 | ||||
| older | 28 | 24.36 ± 6.07 | 24.75 ± 6.50 | 0.246 | 0.622 | 0.004 | |||||
| F-statistics between | F | p | F | p | |||||||
| 1.544 | 0.219 | 0.027 | 3.474 | 0.068 | 0.058 | ||||||
| Functional exercise capacity (6MWT; walking distance in m) | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | younger | 22 | 505.02 ± 103.18 | 527.85 ± 123.38 | 1.239 | 0.273 | 0.032 | ||||
| older | 18 | 448.24 ± 77.12 | 469.77 ± 68.10 | 0.901 | 0.349 | 0.023 | |||||
| F-statistics between | F | p | F | p | |||||||
| 3.735 | 0.061 | 0.089 | 3.184 | 0.082 | 0.077 | ||||||
| CG | younger | 29 | 492.87 ± 58.03 | 500.10 ± 64.18 | 0.598 | 0.443 | 0.011 | ||||
| older | 27 | 473.67 ± 83.63 | 470.29 ± 96.64 | 0.122 | 0.728 | 0.002 | |||||
| F-statistics between | F | p | F | p | |||||||
| 1.008 | 0.320 | 0.018 | 1.874 | 0.177 | 0.034 | ||||||
| Hand grip strength (dominant hand; in kg) | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | younger | 22 | 29.81 ± 12.31 | 29.58 ± 11.19 | 0.136 | 0.715 | 0.003 | ||||
| older | 19 | 25.86 ± 7.57 | 24.91 ± 7.65 | 1.965 | 0.169 | 0.048 | |||||
| F-statistics between | F | p | F | p | |||||||
| 1.469 | 0.233 | 0.036 | 2.345 | 0.134 | 0.057 | ||||||
| CG | younger | 29 | 27.06 ± 8.60 | 27.12 ± 7.50 | 0.008 | 0.928 | 0.000 | ||||
| older | 28 | 26.32 ± 9.21 | 26.58 ± 7.98 | 0.158 | 0.692 | 0.003 | |||||
| F-statistics between | F | p | F | p | |||||||
| 0.099 | 0.754 | 0.002 | 0.070 | 0.739 | 0.001 | ||||||
| Neurocognitive performance: TMT A (in s) | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | younger | 22 | 48.12 ± 17.35 | 46.12 ± 13.61 | 0.181 | 0.673 | 0.005 | ||||
| older | 19 | 56.54 ± 23.31 | 49.90 ± 21.59 | 1.725 | 0.197 | 0.042 | |||||
| F-statistics between | F | p | F | p | |||||||
| 1.750 | 0.194 | 0.043 | 0.461 | 0.501 | 0.012 | ||||||
| CG | younger | 30 | 44.94 ± 15.00 | 41.57 ± 14.00 | 0.994 | 0.323 | 0.017 | ||||
| older | 28 | 46.76 ± 17.88 | 54.06 ± 34.60 | 4.369 | 0.041 * | 0.072 | |||||
| F-statistics between | F | p | F | p | |||||||
| 0.178 | 0.674 | 0.003 | 3.326 | 0.074 | 0.056 | ||||||
| Neurocognitive performance: TMT B (in s) | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | younger | 22 | 109.41 ± 55.71 | 90.61 ± 30.88 | 2.341 | 0.134 | 0.057 | ||||
| older | 19 | 132.66 ± 81.34 | 115.00 ± 43.32 | 1.784 | 0.189 | 0.044 | |||||
| F-statistics between | F | p | F | p | |||||||
| 1.167 | 0.287 | 0.029 | 4.398 | 0.043 * | 0.101 | ||||||
| CG | younger | 30 | 90.94 ± 33.19 | 84.62 ± 33.84 | 1.509 | 0.224 | 0.026 | ||||
| older | 28 | 109.61 ± 44.34 | 109.64 ± 49.62 | 0.000 | 0.995 | 0.000 | |||||
| F-statistics between | F | p | F | p | |||||||
| 3.325 | 0.074 | 0.056 | 5.095 | 0.028 * | 0.083 | ||||||
| Neurocognitive performance: TMT B/A ratio | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | younger | 22 | 2.46 ± 1.51 | 2.07 ± 0.73 | 1.210 | 0.278 | 0.030 | ||||
| older | 19 | 2.49 ± 1.25 | 2.46 ± 0.98 | 0.004 | 0.984 | 0.000 | |||||
| F-statistics between | F | p | F | p | |||||||
| 0.004 | 0.949 | 0.000 | 2.147 | 0.151 | 0.052 | ||||||
| CG | younger | 30 | 2.09 ± 0.67 | 2.09 ± 0.59 | 0.001 | 0.971 | 0.000 | ||||
| older | 28 | 2.41 ± 0.83 | 2.18 ± 0.66 | 2.491 | 0.120 | 0.043 | |||||
| F-statistics between | F | p | F | p | |||||||
| 2.677 | 0.107 | 0.046 | 0.320 | 0.574 | 0.006 | ||||||
| Neurocognitive performance: DSST1 (number of correct matches) | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | younger | 22 | 41.77 ± 7.09 | 44.59 ± 9.20 | 8.217 | 0.007 * | 0.174 | ||||
| older | 19 | 40.16 ± 10.13 | 42.16 ± 10.23 | 3.574 | 0.066 | 0.084 | |||||
| F-statistics between | F | p | F | p | |||||||
| 0.357 | 0.553 | 0.009 | 0.643 | 0.427 | 0.016 | ||||||
| CG | younger | 30 | 47.93 ± 11.97 | 46.40 ± 8.76 | 1.896 | 0.174 | 0.033 | ||||
| older | 28 | 41.64 ± 7.61 | 42.57 ± 9.91 | 0.649 | 0.424 | 0.011 | |||||
| F-statistics between | F | p | F | p | |||||||
| 5.612 | 0.021 * | 0.091 | 2.438 | 0.124 | 0.042 | ||||||
| Memory: DSST2 (number of correct matches) | F-statistics within | ||||||||||
| n | T1 (M ± SD) | T2 (M ± SD) | F | p | |||||||
| IG | younger | 22 | 3.55 ± 2.02 | 4.41 ± 2.26 | 3.080 | 0.087 | 0.073 | ||||
| older | 19 | 2.95 ± 1.75 | 4.16 ± 2.19 | 5.227 | 0.028 * | 0.118 | |||||
| F-statistics between | F | p | F | p | |||||||
| 1.013 | 0.320 | 0.025 | 0.129 | 0.721 | 0.003 | ||||||
| CG | younger | 30 | 4.43 ± 2.60 | 4.67 ± 2.40 | 0.741 | 0.393 | 0.013 | ||||
| older | 28 | 4.18 ± 2.16 | 4.50 ± 2.15 | 1.312 | 0.257 | 0.023 | |||||
| F-statistics between | F | p | F | p | |||||||
| 0.164 | 0.687 | 0.003 | 0.077 | 0.782 | 0.001 | ||||||
References
- Eurostat. Ageing Europe. Looking at the Lives of Older People in the EU, 2020th ed.; Publications Office of the European Union: Luxembourg, 2020. [Google Scholar] [CrossRef]
- State Statistical Office of Saxony. Statistical Yearbook Saxony 2019, 28th ed.; State Statistical Office of Saxony: Kamenz, Germany, 2019; Available online: https://www.statistischebibliothek.de/mir/servlets/MCRFileNodeServlet/SNHeft_derivate_00008934/jahrbuch_statistik-sachsen_insgesamt.pdf (accessed on 15 December 2023).
- Robert Koch-Institute. Health in Germany—The Most Important Trends. Federal Health Reporting. Jointly Provided by RKI and Destatis; Robert Koch-Institute: Berlin, Germany, 2016. [Google Scholar] [CrossRef]
- Dallmeyer, S.; Wicker, P.; Breuer, C. How an aging society affects the economic costs of inactivity in Germany: Empirical evidence and projections. Eur. Rev. Aging Phys. Act. 2017, 14, 18. [Google Scholar] [CrossRef] [PubMed]
- Blüher, S.; Böhm, A.; Geuter, G.; Grossmann, B.; Herweck, R.; Huber, H.P.; Kuhlmey, A.; Kümpers, S.; Nitsche-Neumann, L.; Nowossadeck, S.; et al. Nationales Gesundheitsziel—Gesund Älter Werden; Federal Ministry of Health: Berlin, Germany, 2012. [Google Scholar]
- Schwingel, A.; Chodzko-Zajko, W.J. Role of Physical Activity in the Health and Wellbeing of Older Adults. In Lifestyle Medicine, 3rd ed.; Rippe, J.M., Ed.; CRC Press: Boca Raton, FL, USA, 2019. [Google Scholar] [CrossRef]
- Cunningham, C.; O’Sullivan, R.; Caserotti, P.; Tully, M.A. Consequences of physical inactivity in older adults: A systematic review of reviews and meta-analyses. Scand. J. Med. Sci. Sports 2020, 30, 816–827. [Google Scholar] [CrossRef]
- Daskalopoulou, C.; Stubbs, B.; Kralji, C.; Koukounari, A.; Prince, M.; Prina, A.M. Physical activity and healthy ageing: A systematic review and meta-analysis of longitudinal cohort studies. Ageing Res. Rev. 2017, 38, 6–17. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.R.; Bredin, S.S.D. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Müller, K.; Voelcker-Rehage, C. Gesund durch Bewegung. In Bewegung und Mobilitätsförderung, Praxishandbuch für Pflege- und Gesundheitsberufe, 1st ed.; Schlesselmann, E., Ed.; Hogrefe: Bern, Germany, 2019; pp. 25–49. [Google Scholar]
- DiPietro, L.; Campbell, W.W.; Buschner, D.M.; Erickson, K.I.; Kenneth, E.P.; Bloodgood, B.; Hughes, T.; Day, K.R.; Piercy, K.L.; Vaux-Bjerke, A.; et al. Physical Activity, Injurious Falls, and Physical Function in Aging: An Umbrella Review. Med. Sci. Sports Exerc. 2019, 51, 1303–1313. [Google Scholar] [CrossRef]
- Freiberger, E.; Siebert, C.C.; Kerb, R. Mobility in Older Community-Dwelling Persons: A Narrative Review. Front. Physiol. 2020, 11, 881. [Google Scholar] [CrossRef]
- Peralta, M.; Martins, J.; Chávez, F.G.; Almanzar, P.C.; Marques, A. Self-rated wellbeing and physical activity associations in European older adults. Eur. J. Sport. Sci. 2018, 18, 1038–1044. [Google Scholar] [CrossRef]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef]
- Jeong, S.W.; Kim, S.H.; Kang, S.H.; Kim, H.J.; Yoon, C.H.; Youn, T.J.; Chae, I.H. Mortality reduction with physical activity in patients with and without cardiovascular disease. Eur. Heart J. 2019, 40, 3547–3555. [Google Scholar] [CrossRef]
- Emerson, K.G.; Gay, J. Physical Activity and Cardiovascular Disease Among Older Adults: The Case of Race and Ethnicity. J. Aging Phys. Act. 2017, 25, 505–509. [Google Scholar] [CrossRef]
- Falck, R.S.; Davis, J.C.; Best, J.R.; Crockett, R.A.; Liu-Ambrose, T. Impact of exercise training on physical and cognitive function among older adults: A systematic review and meta-analysis. Neurobiol. Aging 2019, 79, 119–130. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Edwards, M.K.; Crush, E.; Ikuta, T.; Del Arco, A. Dose–Response Association Between Physical Activity and Cognitive Function in a National Sample of Older Adults. Am. J. Health Promot. 2018, 32, 554–560. [Google Scholar] [CrossRef]
- McDowell, C.P.; Dishman, R.K.; Gordon, B.R.; Herring, M.P. Physical Activity and Anxiety: A Systematic Review and Meta-analysis of Prospective Cohort Studies. Am. J. Prev. Med. 2019, 57, 545–556. [Google Scholar] [CrossRef]
- Jeckel, S.; Sudeck, G. Sport activities in daily routine. Situational associations between individual goals, activity characteristics, and affective well-being. Ger. J. Exerc. Sport. Res. 2018, 48, 26–39. [Google Scholar] [CrossRef]
- Wu, F.; Zhang, J.; Yang, H.; Jiang, J. The Effect of Physical Exercise on the Elderly’s Anxiety: Based on Systematic Reviews and Meta-Analysis. Comput. Math. Methods Med. 2022, 2022, 4848290. [Google Scholar] [CrossRef]
- Lauenroth, A.; Ioannidis, A.E.; Teichmann, B. Influence of combined physical and cognitive training on cognition: A systematic review. BMC Geriatr. 2016, 16, 141. [Google Scholar] [CrossRef]
- Varela-Vásquez, L.A.; Minobes-Molina, E.; Jerez-Roig, J. Dual-task exercises in older adults: A structured review of the current literature. J. Frailty Sarcopenia Falls 2020, 5, 31–37. [Google Scholar] [CrossRef]
- Herold, F.; Hamacher, D.; Schega, L.; Müller, N.G. Thinking While Moving or Moving While Thinking—Concepts of Motor-Cognitive Training for Cognitive Performance Enhancement. Front. Aging Neurosci. 2018, 10, 228. [Google Scholar] [CrossRef]
- Wollesen, B.; Voelcker-Rehage, C. Training effects on motor-cognitive dual-task performance in older adults. A systematic review. Eur. Rev. Aging Phys. Act. 2014, 11, 5–24. [Google Scholar] [CrossRef]
- Budde, H.; Voelcker-Rehage, C.; Pietraßyk-Kendziorra, S.; Ribeiro, P.; Tidow, G. Acute coordinative exercise improves attentional performance in adolescents. Neurosci. Lett. 2008, 441, 219–223. [Google Scholar] [CrossRef]
- Gheysen, F.; Poppe, L.; DeSmet, A.; Swinnen, S.; Cardon, G.; De Bourdeaudhuij, I.; Chastin, S.; Fias, W. Physical activity to improve cognition in older adults: Can physical activity programs enriched with cognitive challenges enhance the effects? A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 63. [Google Scholar] [CrossRef]
- Wollesen, B.; Wildbredt, A.; van Schooten, K.S.; Lim, M.L.; Delbare, K. The effects of cognitive-motor training interventions on executive functions in older people: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2020, 17, 9. [Google Scholar] [CrossRef]
- Eggenberger, P.; Schumacher, V.; Angst, M.; Theill, N.; de Bruin, E. Does multicomponent physical exercise with simultaneous cognitive training boost cognitive performance in older adults? A 6-month randomized controlled trial with a 1-year follow-up. Clin. Interv. Aging 2015, 10, 1335–1349. [Google Scholar] [CrossRef]
- Eigenschenk, B.; Thomann, A.; McClure, M.; Davies, L.; Gregory, M.; Dettweiler, U.; Inglés, E. Benefits of Outdoor Sports for Society. A Systematic Literature Review and Reflections on Evidence. Int. J. Environ. Res. Public Health 2019, 16, 937. [Google Scholar] [CrossRef]
- Boakye, K.A.; Amram, O.; Schuna, J.M.; Duncan, G.E.; Hystad, P. GPS-based built environment measures associated with adult physical activity. Health Place 2021, 70, 102602. [Google Scholar] [CrossRef]
- Säumel, I.; Weber, F.; Kowarik, I. Toward livable and healthy urban streets: Roadside vegetation provides ecosystem services where people live and move. Environ. Sci. Policy 2016, 62, 6. [Google Scholar] [CrossRef]
- Bowler, D.; Buyung-Ali, L.; Knight, T.M.; Pullin, A.S. The importance of nature for health: Is there a specific benefit of contact with green space? Environ. Evid. 2010, 40. Available online: www.environmentalevidence.org/SR40.html (accessed on 15 December 2023).
- Kelley, C.; Mack, D.E.; Wilson, P.M. Does Physical Activity in Natural Outdoor Environments Improve Wellbeing? A Meta-Analysis. Sports 2022, 10, 103. [Google Scholar] [CrossRef]
- Thompson Coon, J.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors? A systematic review. Environ. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef]
- Lahart, I.; Darcy, P.; Gidlow, C.; Calogiuri, G. The Effects of Green Exercise on Physical and Mental Wellbeing: A Systematic Review. Int. J. Environ. Res. Public. Health 2019, 16, 1352. [Google Scholar] [CrossRef]
- World Health Organization/WHO. WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/handle/10665/336656 (accessed on 15 December 2023).
- Krug, S.; Jordan, S.; Mensink, G.B.M.; Müters, S.; Finger, J.D.; Lampert, T. Körperliche Aktivität. Ergebnisse der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1). Bundesgesundheitsbl 2013, 56, 765–771. [Google Scholar] [CrossRef]
- Pfeifer, K.; Banzer, B.; Ferrari, N.; Füzéki, E.; Geidl, W.; Graf, C.; Hartung, V.; Klamroth, S.; Völker, K.; Vogt, L. Empfehlungen für Bewegung. In Nationale Empfehlungen für Bewegung und Bewegungsförderung; Rütten, A., Pfeiffer, K., Eds.; FAU Erlangen-Nürnberg: Erlangen-Nürnberg, Germany, 2016; pp. 17–64. Available online: https://www.sport.fau.de/files/2016/05/Nationale-Empfehlungen-f%C3%BCr-Bewegung-und-Bewegungsf%C3%B6rderung-2016.pdf (accessed on 15 December 2023).
- Faß, E.; Schlesinger, T. The Relation of Physical Activity and Self-Rated Health in Older Age—Cross Country Analysis Results from SHARE. Popul. Ageing 2020, 13, 347–364. [Google Scholar] [CrossRef]
- Hoebel, J.; Finger, J.D.; Kuntz, B.; Lampert, T. Sozioökonomische Unterschiede in der körperlich-sportlichen Aktivität von Erwerbstätigen im mittleren Lebensalter. Welche Rolle spielen Bildung, Beruf und Einkommen? Bundesgesundheitsbl 2016, 59, 188–196. [Google Scholar] [CrossRef]
- Franken, G. Allein Lebende Personen mit Demenz; Dialog- und Transferzentrum Demenz: Witten, Germany, 2017; Available online: http://dzd.blog.uni-wh.de/wp-content/uploads/2018/01/Allein-lebende-Menschen-mit-Demenz_final_171204.pdf (accessed on 15 December 2023).
- Wille, E.; Schrappe, M.; Gerlach, F.M.; Glaeske, G.; Haubitz, M.; Kuhlmey, A.; Rosenbrock, R. Coordination and Integration—Health Care in an Ageing Society; Special Report; Advisory Council on the Assessment of Developments in the Health Care System: Stuttgart, Germany, 2009; Available online: https://www.svr-gesundheit.de/fileadmin/Gutachten/Sondergutachten_2009/Kurzfassung_engl_2009.pdf (accessed on 15 December 2023).
- Lis, K.; Olbermann, E.; von Koenen, C.; Wisniewski, G. Gesundheitsförderung für Ältere Menschen in Sozial Benachteiligten Lebenslagen im Setting Stadtbezirk; Ein Leitfaden mit Praktischen Handlungsempfehlungen; Institut für Gerontologie: Dortmund, Germany, 2011; Available online: https://www.bundesgesundheitsministerium.de/fileadmin/Dateien/5_Publikationen/Gesundheit/Broschueren/Praxishandbuch_Aelter_werden_in_Eving.pdf (accessed on 15 December 2023).
- Spiteri, K.; Broom, D.; Bekhet, A.H.; de Caro, J.X.; Laventure, B.; Grafton, K. Barriers and Motivators of Physical Activity Participation in Middle-aged and Older-adults—A Systematic Review. J. Aging Phys. Act. 2019, 27, 929–944. [Google Scholar] [CrossRef]
- Yarmohammadi, S.; Saadati, H.M.; Ghaffari, M.; Ramezankhani, A. A systematic review of barriers and motivators to physical activity in elderly adults in Iran and worldwide. Epidemiol. Health 2019, 41, e2019049. [Google Scholar] [CrossRef]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef]
- Sansano-Nadal, O.; Giné-Garriga, M.; Brach, J.S.; Wert, D.M.; Jerez-Roig, J.; Guerra-Balic, M.; Oviedo, G.; Fortuño, J.; Gómara-Toldrà, N.; Soto-Bagaria, L.; et al. Exercise-Based Interventions to Enhance Long-Term Sustainability of Physical Activity in Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2019, 16, 2527. [Google Scholar] [CrossRef]
- Langhammer, B.; Bergland, A.; Rydwik, E. The Importance of Physical Activity Exercise among Older People. Biomed. Res. Int. 2018, 2018, 7856823. [Google Scholar] [CrossRef]
- Lin, Y.-H.; Chen, Y.-C.; Tseng, Y.-C.; Tsai, S.-T.; Tseng, Y.-H. Physical activity and successful aging among middle-aged and older adults: A systematic review and meta-analysis of cohort studies. Aging 2020, 12, 7704–7716. [Google Scholar] [CrossRef]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef]
- Brand, T.; Gansefort, D. Bewegungsförderung im Quartier—Was braucht es? In Vielfalt im Alter mit Vielfalt Begegnen: Herausforderungen und Strategien in der Gesundheitsförderung; Landesvereinigung für Gesundheit Bremen e.V.: Bremen, Germany, 2017; pp. 13–14. [Google Scholar]
- Abu-Omar, K.; Gelius, P.; Rütten, A. Prävalenz der körperlichen (In-)Aktivität als Basis für eine setting- und zielgruppenspezifische Bewegungsförderung. In Gesundheit Durch Bewegung Fördern. Empfehlungen für Wissenschaft und Praxis. LIGA.Fokus 12; LIGA.NRW: Düsseldorf, Germany, 2011; pp. 23–26. Available online: https://www.lzg.nrw.de/_php/login/dl.php?u=/_media/pdf/liga-fokus/LIGA_Fokus_12.pdf (accessed on 15 December 2023).
- Kühnemund, C.; Kümpers, S. Health promotion for older people in the neighbourhood. Public. Health Forum 2018, 26, 123–126. [Google Scholar] [CrossRef]
- Di Lorito, C.; Long, A.; Byrne, A.; Harwood, R.H.; Gladman, J.R.F.; Schneider, S.; Logan, P.; Bosco, A.; van der Wardt, V. Exercise interventions for older adults: A systematic review of meta-analyses. J. Sport. Health Sci. 2021, 10, 29–47. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. Consort 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Weiser, U. Stadtteile Chemnitz. Versuch Eines Soziökonomischen Rankings; FOG-Institut für Markt- und Sozialforschung: Chemnitz, Germany, 2018; Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwia0LKvw4P9AhXI3KQKHb3gCIUQFnoECAsQAQ&url=https%3A%2F%2Fs628a60337583afbe.jimcontent.com%2Fdownload%2Fversion%2F1589891346%2Fmodule%2F13982116623%2Fname%2FStadtteil-Ranking%2520Chemnitz_Ergebnisbericht.pdf&usg=AOvVaw1Ey34ubCP9AsDr0oF0If7S (accessed on 15 December 2023).
- Frey, I.; Berg, A.; Grathwohl, D.; Keul, J. Freiburger Fragebogen zur körperlichen Aktivität—Entwicklung, Prüfung und Anwendung. Soz. Präventivmed. 1999, 44, 55–64. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Hoebel, J.; Müters, S.; Kuntz, B.; Lange, C.; Lampert, T. Messung des subjektiven sozialen Status in der Gesundheitsforschung mit einer deutschen Version der MacArthur Scale. Bundesgesundheitsbl 2015, 58, 749–757. [Google Scholar] [CrossRef]
- Kıskaç, M.; Soysal, P.; Smith, L.; Capar, E.; Zorlu, M. What is the Optimal Body Mass Index Range for Older Adults? Ann. Geriatr. Med. Res. 2022, 26, 49–57. [Google Scholar] [CrossRef]
- Voigt-Radloff, S.; Blümle, A.; Meerpohl, J. Die TIDieR Checkliste und Anleitung—Ein Instrument für eine verbesserte Interventionsbeschreibung und Replikation (Better Reporting of Interventions: Template for Intervention Description and Replication (TIDieR) Checklist and Guide). Gesundheitswesen 2016, 78, 175–188. [Google Scholar] [CrossRef]
- Zwingmann, K.; Schlesinger, T.; Müller, K. Körperliche Aktivität von Älteren Personen im Rahmen der kommunalen Gesundheitsförderung. In Darstellung Eines Motorisch-Kognitiven Bewegungskonzeptes im Außenbereich, 1st ed.; Feldhaus: Hamburg, Germany, 2023. [Google Scholar]
- Älter Werden in Balance. Available online: https://www.gesund-aktiv-aelter-werden.de/ (accessed on 23 October 2023).
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance for Prescribing Exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Müller, K.; Wagner, P. Trainermanual zum Programm “Aktiv Gegen Atemnot”, 1st ed.; Dustri-Verlag Dr. Karl Feistle: München, Germany, 2022. [Google Scholar]
- Bohannon, R.W.; Crouch, R. 1-Minute sit-to-stand test: Systematic review of procedures, performance, and clinimetric properties. J. Cardiopulm. Rehabil. Prev. 2019, 39, 2–8. [Google Scholar] [CrossRef]
- Crapo, R.; Enright, P.; Zeballos, R. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Akter, S. Measurement of Hand Grip Strength by Digital Jamar Hand Dynamometer: A Study on CRP Staffs & BHPI Students. Ph.D. Thesis, University of Dhaka, Dhaka, Bangladesh, 2018. [Google Scholar]
- Reitan, R.M.; Wolfson, D. Category Test and Trail Making Test as measures of frontal lobe functions. Clin. Neuropsychol. 1995, 9, 50–56. [Google Scholar] [CrossRef]
- Drane, D.L.; Yuseph, R.L.; Huthwaite, J.S.; Klingler, L.K. Demographic Characteristics and Normative Observations for Derived-Trail Making Test Indices. Neuropsychiatry Neuropsychol. Behav. Neurol. 2002, 15, 39–43. [Google Scholar] [CrossRef]
- Jaeger, J. Digit symbol substitution test: The case for sensitivity over specificity in neuropsychological testing. J. Clin. Psychopharm. 2018, 38, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Strassmann, A.; Steurer-Stey, C.; Lana, K.D.; Zoller, M.; Turk, A.J.; Suter, P.; Puhan, M.A. Population-based reference values for the 1-min sit-to-stand test. Int. J. Public. Health 2013, 58, 949–953. [Google Scholar] [CrossRef]
- Chen, Y.-L.; Tseng, C.-H.; Lin, H.-T.; Wu, P.-Y.; Chao, H.-C. Dual-task multicomponent exercise–cognitive intervention improved cognitive function and functional fitness in older adults. Aging Clin. Exp. Res. 2023, 35, 1855–1863. [Google Scholar] [CrossRef]
- Lipardo, D.S.; Tsang, W.W.N. Effects of combined physical and cognitive training on fall prevention and risk reduction in older persons with mild cognitive impairment: A randomized controlled study. Clin. Rehabil. 2020, 34, 773–782. [Google Scholar] [CrossRef]
- Rezola-Pardo, C.; Arrieta, H.; Gil, S.M.; Zarrazquin, I.; Yanguas, J.J.; López, M.A.; Irazusta, J.; Rodriguez-Larrad, A. Comparison between multicomponent and simultaneous dual-task exercise interventions in long-term nursing home residents: The Ageing-ONDUAL-TASK randomized controlled study. Age Ageing 2019, 48, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Schoene, D.; Kiesswetter, E.; Sieber, C.C.; Freiberger, E. Musculoskeletal factors, sarcopenia and falls in old age [Skelettmuskuläre Faktoren, Sarkopenie und Stürze im Alter]. Z. Gerontol. Geriat. 2019, 52, 37–44. [Google Scholar] [CrossRef]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.M.; Tausif, F.; Aziz, N.; Hussain, S.M. 6 Minute Walk Test (6MWT) for Healthy Adult Volunteers. J. Rawalpindi Med. Coll. 2021, 25, 333–338. [Google Scholar] [CrossRef]
- Enright, P.L.; Sherrill, D.L. Reference Equations for the Six-Minute Walk in Healthy Adults. Am. J. Respir. Crit. Care Med. 1998, 158, 1384–1387. [Google Scholar] [CrossRef]
- Illig, C.; Pfeffer, I. Is a multidimensional exercise program able to enhance cognitive and motor functions in older adults? (“Fördert ein multidimensionales Gesundheitssportprogramm kognitive und motorische Fähigkeiten im höheren Erwachsenenalter?”). Sportwissenschaft 2010, 40, 110–119. [Google Scholar] [CrossRef]
- Gouveia, É.R.; Smailagic, A.; Ihle, A.; Marques, A.; Gouveia, B.R.; Cameirão, M.; Sousa, H.; Kliegel, M.; Siewiorek, D. The Efficacy of a Multicomponent Functional Fitness Program Based on Exergaming on Cognitive Functioning of Healthy Older Adults: A Randomized Controlled Trial. J. Aging Phys. Act. 2021, 29, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, F.; Amaro, N.; Matos, R.; Mendes, D.; Monteiro, D.; Morouço, P. The impact of an exercise intervention using low-cost equipment on functional fitness in the community-dwelling older adults: A pilot study. Front. Physiol. 2022, 13, 1039131. [Google Scholar] [CrossRef]
- Brooks, D.; Solway, S.; Weinacht, K.; Wang, D.; Thomas, S. Comparison Between an Indoor and an Outdoor 6-Minute Walk Test Among Individuals with Chronic Obstructive Pulmonary Disease. Arch. Phys. Med. Rehabil. 2003, 84, 873–876. [Google Scholar] [CrossRef] [PubMed]
- Soto, M.E.; Pérez-Torres, I.; Rubio-Ruiz, M.E.; Cano-Martínez, A.; Manzano-Pech, L.; Guarner-Lans, V. Frailty and the Interactions between Skeletal Muscle, Bone, and Adipose Tissue-Impact on Cardiovascular Disease and Possible Therapeutic Measures. Int. J. Mol. Sci. 2023, 24, 4534. [Google Scholar] [CrossRef]
- Albrecht, B.M.; Stalling, I.; Bammann, K. Sex- and age-specific normative values for handgrip strength and components of the Senior Fitness Test in community-dwelling older adults aged 65–75 years in Germany: Results from the OUTDOOR ACTIVE study. BMC Geriatr. 2021, 21, 273. [Google Scholar] [CrossRef]
- Tombaugh, T.N. Trail Making Test A and B: Normative data stratified by age and education. Arch. Clin. Neuropsychol. 2004, 19, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, J.; Thaikruea, L.; Wongpakaran, N.; Munkhetvit, P.; Kittisares, A.; Varnado, P. Effects of Combined Physical Movement Activity and Multifaceted Cognitive Training in Older People with Mild Neurocognitive Disorder in a Rural Community: A Randomized Control Trial. Dement. Geriatr. Cogn. Disord. 2020, 49, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Hiyamizu, M.; Morioka, S.; Shomoto, K.; Shimada, T. Effects of dual task balance training on dual task performance in elderly people: A randomized controlled trial. Clin. Rehabil. 2011, 26, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Law, L.L.F.; Mok, V.C.T.; Yau, M.M.K. Effects of functional tasks exercise on cognitive functions of older adults with mild cognitive impairment: A randomized controlled pilot trial. Alzheimers Res. Ther. 2019, 11, 98. [Google Scholar] [CrossRef]
- Gaudino, E.A.; Geisler, M.W.; Squires, N.K. Construct validity in the trail making test: What makes part B harder? J. Clin. Exp. Neuropsychol. 1995, 17, 529–535. [Google Scholar] [CrossRef]
- Gurvich, C.; Le, J.; Thomas, N.; Thomas, E.H.X.; Kulkarni, J. Sex hormones and cognition in aging. Vitam. Horm. 2021, 115, 511–533. [Google Scholar] [CrossRef]
- Royer, F.L. Sex Differences in Symbol-Digit Substitution Task Performance. Intelligence 1978, 2, 145–151. [Google Scholar] [CrossRef]
- Eckhardt, N.; Braun, C.; Kibele, A. Instability Resistance Training improves Working Memory, Processing Speed and Response Inhibition in Healthy Older Adults: A Double-Blinded Randomised Controlled Trial. Sci. Rep. 2020, 10, 2506. [Google Scholar] [CrossRef]
- Jeong, M.K.; Park, K.W.; Ryu, J.K.; Kim, G.M.; Jung, H.H.; Park, H. Multi-Component Intervention Program on Habitual Physical Activity Parameters and Cognitive Function in Patients with Mild Cognitive Impairment: A Randomized Controlled Trial. Int. J. Environ. Res. Public. Health 2021, 18, 6240. [Google Scholar] [CrossRef] [PubMed]
- Nishiguchi, S.; Yamada, M.; Tanigawa, T.; Sekiyama, K.; Kawagoe, T.; Suzuki, M.; Yoshikawa, S.; Abe, N.; Otsuka, Y.; Nakai, R.; et al. A 12-Week Physical and Cognitive Exercise Program Can Improve Cognitive Function and Neural Efficiency in Community-Dwelling Older Adults: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2015, 63, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Santos, P.C.; Machado, D.R.L.; Abdalla, P.P.; Santos, C.V.; Lopes, S.; Martins, A.C.; Mota, J.; Mesquita, C. Otago Exercise Program Plus Cognitive Dual-task can Reduce Fall Risk, Improve Cognition and Functioning in Older Adults. Curr. Aging Sci. 2022, 16, 65–74. [Google Scholar] [CrossRef]
- Levin, O.; Netz, Y.; Ziv, G. The beneficial effects of different types of exercise interventions on motor and cognitive functions in older age: A systematic review. Eur. Rev. Aging Phys. Act. 2017, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Zhidong, C.; Wang, X.; Yin, J.; Song, D.; Chen, Z. Effects of physical exercise on working memory in older adults: A systematic and meta-analytic review. Eur. Rev. Aging Phys. Act. 2021, 18, 18. [Google Scholar] [CrossRef] [PubMed]
- Müller, B. 2.4.4. Höheres und hohes Alter. In Online Lehrbuch der Medizinischen Psychologie und Medizinischen Soziologie; Deinzer, R., von dem Knesebeck, O., Eds.; German Medical Science GMS Publishing House: Berlin, Germany, 2018. [Google Scholar] [CrossRef]
- Morris, S.; Guell, C.; Pollard, T.M. Group walking as a “lifeline”: Understanding the place of outdoor walking groups in women’s lives. Soc. Sci. Med. 2019, 238, 112489. [Google Scholar] [CrossRef] [PubMed]



| Total (n = 99, 61 Female) | IG (n = 41, 25 Female) | CG (n = 58, 36 Female) | F | p | |||||
|---|---|---|---|---|---|---|---|---|---|
| M ± SD | M ± SD | M ± SD | |||||||
| Min | Max | Min | Max | Min | Max | ||||
| Age (years) | 74.32 ± 7.28 | 72.46 ± 6.21 | 75.64 ± 7.73 | 4.748 | 0.032 * | 0.047 | |||
| 63 | 91 | 63 | 86 | 65 | 91 | ||||
| BMI (kg/m2) | 27.00 ± 3.73 | 27.26 ± 4.28 | 26.82 ± 3.32 | 0.332 | 0.566 | 0.003 | |||
| 18.37 | 37.99 | 20.21 | 37.99 | 18.37 | 33.76 | ||||
| ACCI | 3.50 ± 1.35 | 3.17 ± 1.22 | 3.64 ± 1.33 | 3.155 | 0.079 | 0.032 | |||
| 2 | 8 | 2 | 6 | 2 | 8 | ||||
| SSES (ladder steps) | 5.64 ± 1.29 | 5.46 ± 1.45 | 5.77 ± 1.15 | 1.377 | 0.243 | 0.014 | |||
| 1 | 8 | 1 | 8 | 1 | 8 | ||||
| MoCA (points) | 26.23 ± 2.37 | 25.66 ± 2.54 | 26.64 ± 2.17 | 4.244 | 0.042 * | 0.042 | |||
| 21 | 30 | 21 | 30 | 21 | 30 | ||||
| Outcome | Instrument | |
|---|---|---|
| Subjective socio-economic status (SSES) | MacArthur ladder scale (German version) [62] via questionnaire | |
| Physical activity | Freiburg questionnaire for physical activity (“Freiburger Fragebogen für körperliche Aktivität“/FFkA) [59] | |
| Functional performance of the lower limbs measured in completed repetitions within 1 minute | 1-Minute-Sit-to-Stand-Test/1MSTST [69] | |
| Functional exercise capacity measured in total walking distance in meters | 6-Minute-Walking-Test/6MWT [70] | |
| Hand grip strength measured in kilogramme (mean of three trials of the dominant hand) | Dynamometer by JAMAR (JAMAR R SmartHand Dynamometer, Performance Health Supply Inc, Cedarburg, USA) [71] | |
| Neurocognitive performance (i.e., sustained attention, executive dysfunction, and visual exploratory capacity, processing speed, set shifting) | measured in time for completion in seconds | Trail Making Test/TMT A and B [72] + ratio of TMT B/A [73] |
| measured in correct number–symbol matches within 90 seconds | Digit Symbol Substitution Test part 1/DSST1 [74] | |
| Memory measured in correct number–symbol matches | Digit Symbol Substitution Test part 2/DSST2 [74] | |
| Functional performance of the lower limbs (1MSTST; number of repetitions) | ||||||||||
| n | T1 | F-statistics T1 | T2 | F-statistics T1–T2 | ||||||
| M ± SD | F | p | M ± SD | F | p | |||||
| IG | 41 | 22.73 ± 5.22 | 4.712 | 0.032 * | 0.046 | 26.49 ± 8.65 | Time | 1.148 | 0.287 | 0.012 |
| CG | 58 | 25.53 ± 7.00 | 26.67 ± 7.75 | Group | 3.028 | 0.085 | 0.031 | |||
| Sex | 0.489 | 0.486 | 0.005 | |||||||
| Age | 8.223 | <0.001 ** | 0.307 | |||||||
| Time × Group | 3.709 | 0.057 | 0.038 | |||||||
| Time × Sex | 0.484 | 0.489 | 0.005 | |||||||
| Time × Age | 0.637 | 0.427 | 0.007 | |||||||
| Functional exercise capacity (6MWT; walking distance in m) | ||||||||||
| n | T1 | F-statistics T1 | T2 | F-statistics T1–T2 | ||||||
| M ± SD | F | p | M ± SD | F | p | |||||
| IG | 40 | 479.47 ± 95.62 | 0.072 | 0.789 | 0.001 | 501.71 ± 105.24 | Time | 0.383 | 0.537 | 0.004 |
| CG | 56 | 483.62 ± 71.52 | 485.72 ± 82.08 | Group | 0.156 | 0.694 | 0.002 | |||
| Sex | 14.263 | <0.001 ** | 0.134 | |||||||
| Age | 12.069 | <0.001 ** | 0.116 | |||||||
| Time × Group | 1.612 | 0.207 | 0.017 | |||||||
| Time × Sex | 3.663 | 0.059 | 0.038 | |||||||
| Time × Age | 0.058 | 0.810 | 0.001 | |||||||
| Hand grip strength (dominant hand; in kg) | ||||||||||
| n | T1 | F-statistics T1 | T2 | F-statistics T1–T2 | ||||||
| M ± SD | F | p | M ± SD | F | p | |||||
| IG | 41 | 27.98 ± 10.45 | 0.418 | 0.519 | 0.004 | 27.42 ± 9.88 | Time | 0.385 | 0.537 | 0.004 |
| CG | 57 | 26.70 ± 8.84 | 26.85 ± 7.67 | Group | 0.022 | 0.882 | 0.000 | |||
| Sex | 152.422 | <0.001 ** | 0.619 | |||||||
| Age | 16.056 | <0.001 ** | 0.146 | |||||||
| Time × Group | 1.000 | 0.320 | 0.011 | |||||||
| Time × Sex | 4.794 | 0.031 * | 0.049 | |||||||
| Time × Age | 0.098 | 0.755 | 0.001 | |||||||
| TMT A (in s) | ||||||||||
| n | T1 | F-statistics T1 | T2 | F-statistics T1–T2 | ||||||
| M ± SD | F | p | M ± SD | F | p | |||||
| IG | 41 | 52.02 ± 20.51 | 2.803 | 0.097 | 0.028 | 47.87 ± 17.62 | Time | 3.687 | 0.058 | 0.037 |
| CG | 58 | 45.82 ± 16.33 | 47.60 ± 26.58 | Group | 1.354 | 0.247 | 0.014 | |||
| Sex | 5.540 | 0.021 * | 0.055 | |||||||
| Age | 2.078 | 0.153 | 0.021 | |||||||
| Time × Group | 0.985 | 0.323 | 0.010 | |||||||
| Time × Sex | 0.358 | 0.551 | 0.004 | |||||||
| Time × Age | 3.949 | 0.050 | 0.040 | |||||||
| TMT B (in s) | ||||||||||
| n | T1 | F-statistics T1 | T2 | F-statistics T1–T2 | ||||||
| M ± SD | F | p | M ± SD | F | p | |||||
| IG | 41 | 120.19 ± 68.88 | 3.409 | 0.068 | 0.034 | 101.91 ± 38.69 | Time | 1.309 | 0.255 | 0.014 |
| CG | 58 | 99.95 ± 39.75 | 96.70 ± 43.68 | Group | 3.919 | 0.051 | 0.040 | |||
| Sex | 5.609 | 0.020 * | 0.056 | |||||||
| Age | 5.683 | 0.019 * | 0.056 | |||||||
| Time × Group | 2.183 | 0.143 | 0.022 | |||||||
| Time × Sex | 0.069 | 0.793 | 0.001 | |||||||
| Time × Age | 0.937 | 0.335 | 0.010 | |||||||
| TMT B/A ratio | ||||||||||
| n | T1 | F-statistics T1 | T2 | F-statistics T1–T2 | ||||||
| M ± SD | F | p | M ± SD | F | p | |||||
| IG | 41 | 2.47 ± 1.38 | 1.073 | 0.303 | 0.011 | 2.25 ± 0.87 | Time | 0.044 | 0.835 | 0.000 |
| CG | 58 | 2.25 ± 0.76 | 2.13 ± 0.62 | Group | 2.528 | 0.115 | 0.026 | |||
| Sex | 0.142 | 0.707 | 0.001 | |||||||
| Age | 2.913 | 0.091 | 0.030 | |||||||
| Time × Group | 0.234 | 0.630 | 0.002 | |||||||
| Time × Sex | 0.034 | 0.855 | 0.000 | |||||||
| Time × Age | 0.134 | 0.716 | 0.001 | |||||||
| DSST1 (number of correct matches) | ||||||||||
| n | T1 | F-statistics T1 | T2 | F-statistics T1–T2 | ||||||
| M ± SD | F | p | M ± SD | F | p | |||||
| IG | 41 | 41.02 ± 8.56 | 3.789 | 0.054 | 0.038 | 43.46 ± 9.64 | Time | 0.818 | 0.368 | 0.009 |
| CG | 58 | 44.90 ± 10.51 | 44.55 ± 9.45 | Group | 2.783 | 0.099 | 0.028 | |||
| Sex | 4.861 | 0.030 * | 0.049 | |||||||
| Age | 2.796 | 0.098 | 0.029 | |||||||
| Time × Group | 6.943 | 0.010 * | 0.068 | |||||||
| Time × Sex | 0.219 | 0.641 | 0.002 | |||||||
| Time × Age | 1.349 | 0.248 | 0.014 | |||||||
| Memory (DSST2; number of correct matches, range: 0–9) | ||||||||||
| n | T1 | F-statistics T1 | T2 | F-statistics T1–T2 | ||||||
| M ± SD | F | p | M ± SD | F | p | |||||
| IG | 41 | 3.27 ± 1.90 | 5.424 | 0.022 * | 0.053 | 4.29 ± 2.21 | Time | 0.097 | 0.756 | 0.001 |
| CG | 58 | 4.31 ± 2.38 | 4.59 ± 2.26 | Group | 2.986 | 0.097 | 0.030 | |||
| Sex | 1.630 | 0.205 | 0.017 | |||||||
| Age | 0.495 | 0.483 | 0.005 | |||||||
| Time × Group | 3.717 | 0.057 | 0.038 | |||||||
| Time × Sex | 0.359 | 0.551 | 0.004 | |||||||
| Time × Age | 0.006 | 0.936 | 0.000 | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zwingmann, K.; Schlesinger, T.; Müller, K. The Impact of an Outdoor Motor–Cognitive Exercise Programme on the Health Outcomes of Older Adults in Community Settings: A Pilot and Feasibility Study. Sports 2024, 12, 49. https://doi.org/10.3390/sports12020049
Zwingmann K, Schlesinger T, Müller K. The Impact of an Outdoor Motor–Cognitive Exercise Programme on the Health Outcomes of Older Adults in Community Settings: A Pilot and Feasibility Study. Sports. 2024; 12(2):49. https://doi.org/10.3390/sports12020049
Chicago/Turabian StyleZwingmann, Katharina, Torsten Schlesinger, and Katrin Müller. 2024. "The Impact of an Outdoor Motor–Cognitive Exercise Programme on the Health Outcomes of Older Adults in Community Settings: A Pilot and Feasibility Study" Sports 12, no. 2: 49. https://doi.org/10.3390/sports12020049