
Effect of Self-Myofascial Release of the Lower Back on Myofascial Gliding, Lumbar Flexibility, and Abdominal Trunk Muscle Strength: A Crossover Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ethics
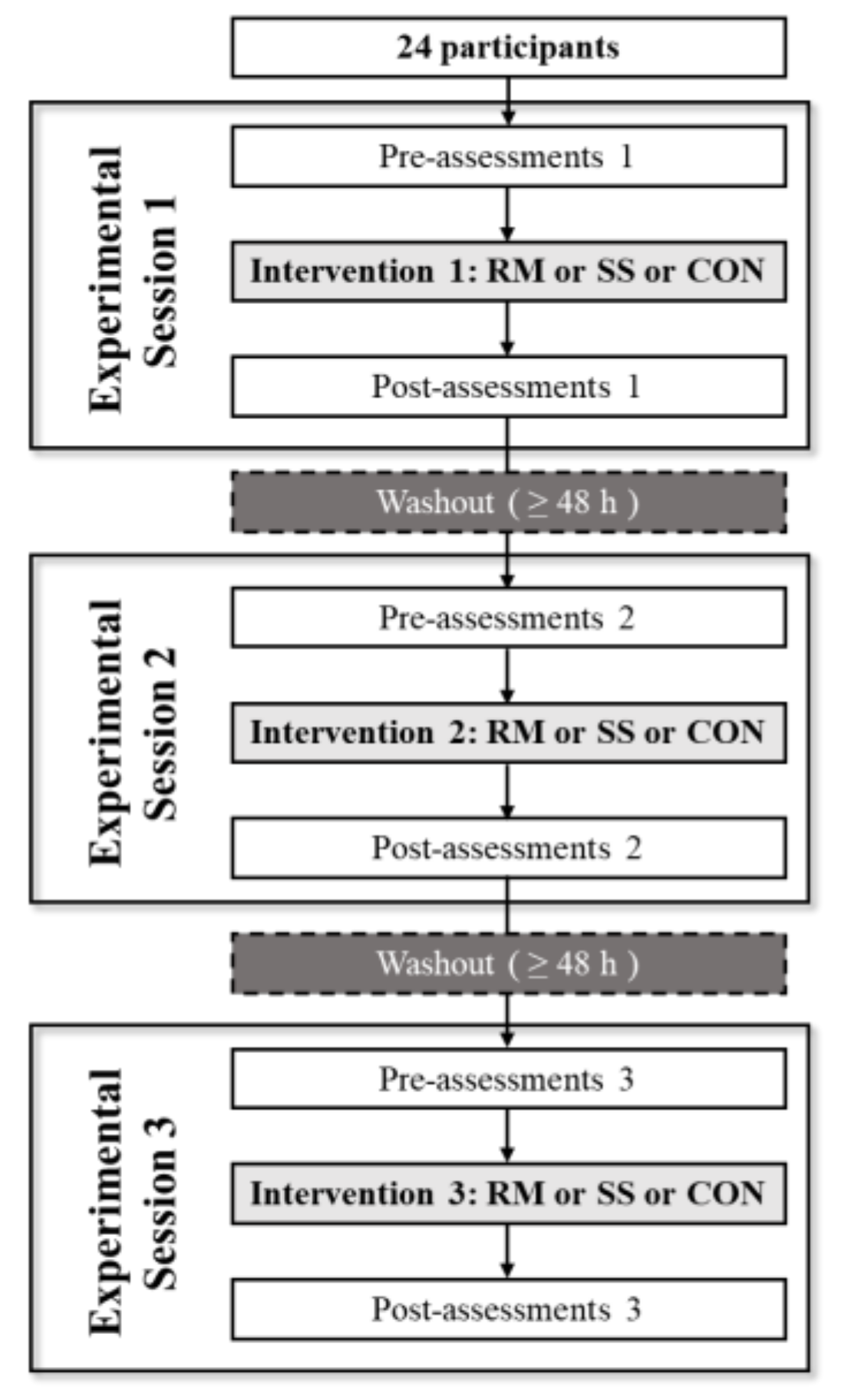
2.3. Procedures
2.4. Intervention
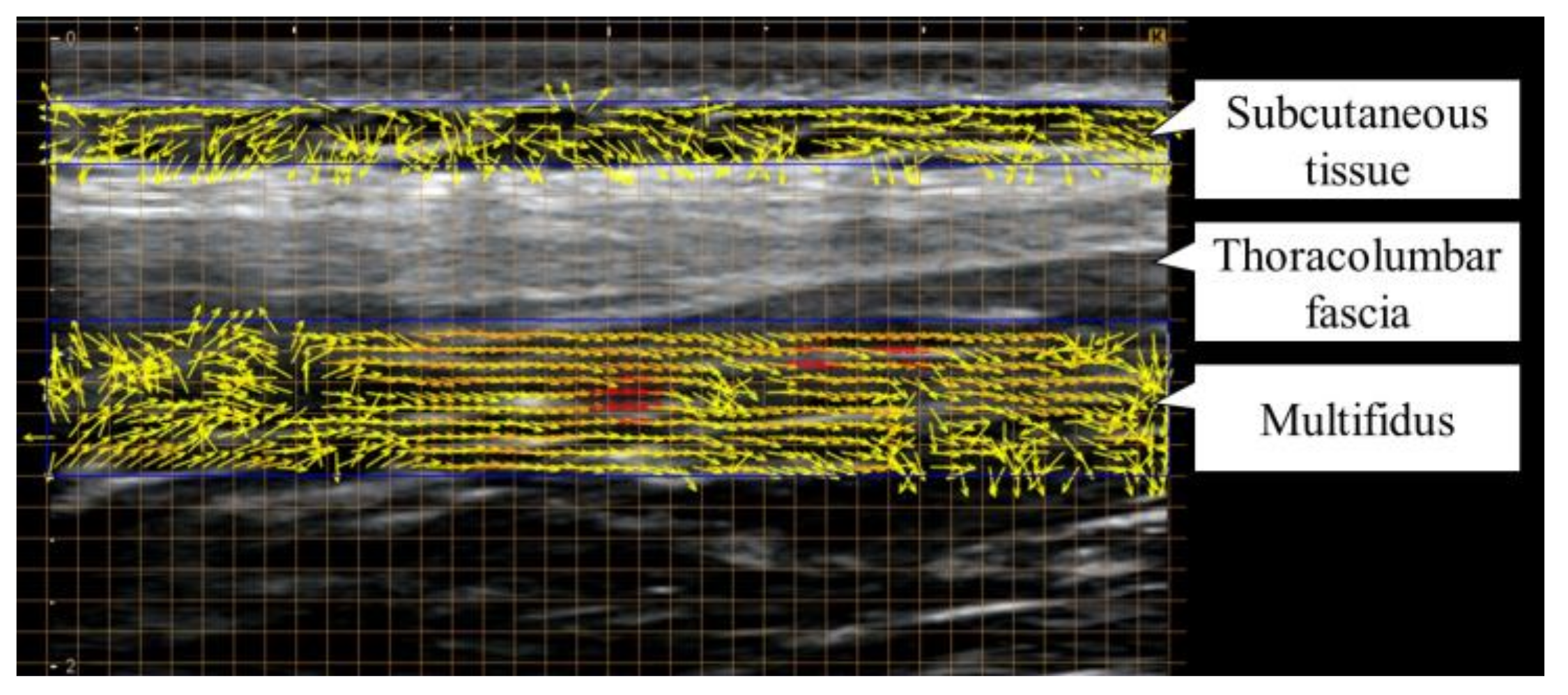
2.5. Measurement Method of Lumbar Myofascial Gliding
2.6. Measurement Method of Flexibility
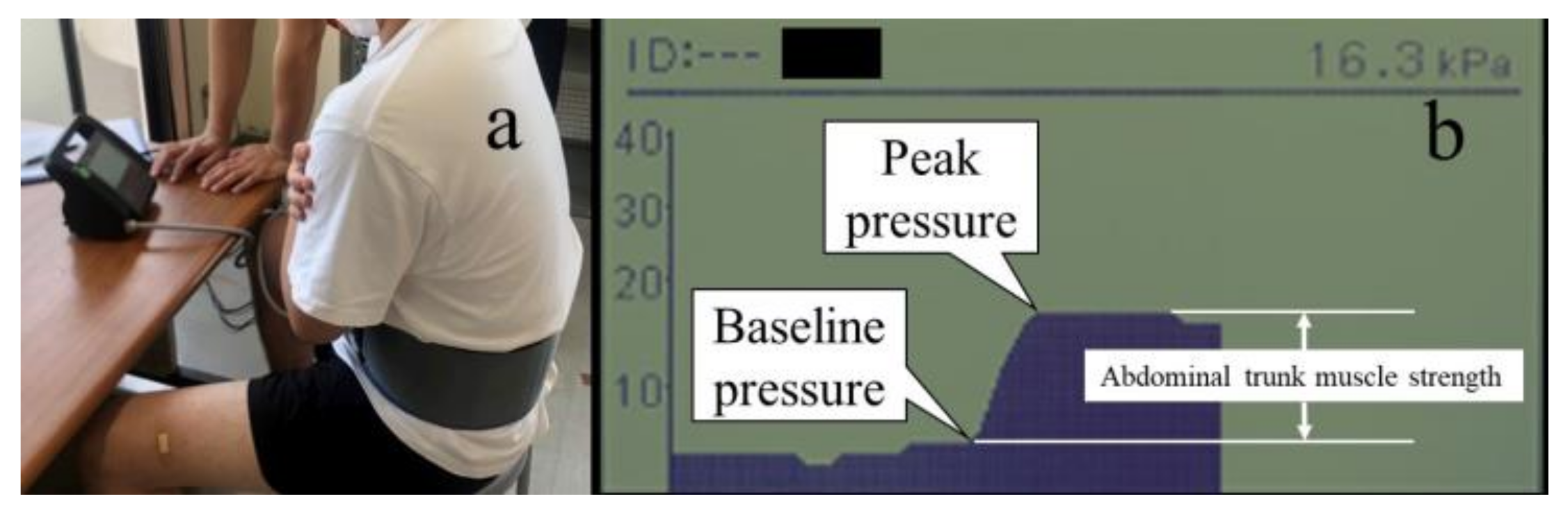
2.7. Measurement Method of Abdominal Trunk Muscle Strength
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heneweer, H.; Staes, F.; Aufdemkampe, G.; van Rijn, M.; Vanhees, L. Physical Activity and Low Back Pain: A Systematic Review of Recent Literature. Eur. Spine J. 2011, 20, 826–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortazavi, J.; Zebardast, J.; Mirzashahi, B. Low Back Pain in Athletes. Asian J. Sport. Med. 2015, 6, e24718. [Google Scholar] [CrossRef] [Green Version]
- Cheatham, S.W.; Kolber, M.J.; Cain, M.; Lee, M. The Effects of Self-Myofascial Release Using a Foam Roll or Roller Massager on Joint Range of Motion, Muscle Recovery, and Performance: A Systematic Review. Int. J. Sport. Phys. Ther. 2015, 10, 827–838. [Google Scholar]
- Ajimsha, M.S.; Shenoy, P.D. Improving the Quality of Myofascial Release Research—A Critical Appraisal of Systematic Reviews. J. Bodyw. Mov. Ther. 2019, 23, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Beardsley, C.; Škarabot, J. Effects of Self-Myofascial Release: A Systematic Review. J. Bodyw. Mov. Ther. 2015, 19, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Weerapong, P.; Hume, P.A.; Kolt, G.S. The Mechanisms of Massage and Effects on Performance, Muscle Recovery and Injury Prevention. Sport. Med. 2005, 35, 235–256. [Google Scholar] [CrossRef]
- McHugh, M.P.; Cosgrave, C.H. To Stretch or Not to Stretch: The Role of Stretching in Injury Prevention and Performance. Scand. J. Med. Sci. Sport. 2010, 20, 169–181. [Google Scholar] [CrossRef]
- Behm, D.G.; Blazevich, A.J.; Kay, A.D.; McHugh, M. Acute Effects of Muscle Stretching on Physical Performance, Range of Motion, and Injury Incidence in Healthy Active Individuals: A Systematic Review. Appl. Physiol. Nutr. Metab. 2016, 41, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Fonta, M.; Tsepis, E.; Fousekis, K.; Mandalidis, D. Acute Effects of Static Self-Stretching Exercises and Foam Roller Self-Massaging on the Trunk Range of Motions and Strength of the Trunk Extensors. Sports 2021, 9, 159. [Google Scholar] [CrossRef]
- Ozsoy, G.; Ilcin, N.; Ozsoy, I.; Gurpinar, B.; Buyukturan, O.; Buyukturan, B.; Kararti, C.; Sas, S. The Effects of Myofascial Release Technique Combined with Core Stabilization Exercise in Elderly with Non-specific Low Back Pain: A Randomized Controlled, Single-Blind Study. Clin. Interv. Aging 2019, 14, 1729–1740. [Google Scholar] [CrossRef] [Green Version]
- Maganaris, C.N.; Baltzopoulos, V.; Sargeant, A.J. In Vivo Measurement-Based Estimations of the Human Achilles Tendon Moment Arm. Eur. J. Appl. Physiol. 2000, 83, 363–369. [Google Scholar] [CrossRef]
- Masaki, M.; Ji, X.; Yamauchi, T.; Tateuchi, H.; Ichihashi, N. Effects of the Trunk Position on Muscle Stiffness That Reflects Elongation of the Lumbar Erector Spinae and Multifidus Muscles: An Ultrasonic Shear Wave Elastography Study. Eur. J. Appl. Physiol. 2019, 119, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Whatman, C.; Knappstein, A.; Hume, P. Acute Changes in Passive Stiffness and Range of Motion Post-stretching. Phys. Ther. Sport 2006, 7, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Konrad, A.; Kiyono, R.; Sato, S.; Yahata, K.; Yoshida, R.; Yasaka, K.; Murakami, Y.; Sanuki, F.; Wilke, J. Local and Non-local Effects of Foam Rolling on Passive Soft Tissue Properties and Spinal Excitability. Front. Physiol. 2021, 12, 702042. [Google Scholar] [CrossRef]
- Willard, F.H.; Vleeming, A.; Schuenke, M.D.; Danneels, L.; Schleip, R. The Thoracolumbar Fascia: Anatomy, Function and Clinical Considerations. J. Anat. 2012, 221, 507–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halperin, I.; Aboodarda, S.J.; Button, D.C.; Andersen, L.L.; Behm, D.G. Original Research Roller Massager Improves Range of Motion of Plantar Flexor Muscles without Subsequent. Int. J. Sport. Phys. Ther. 2014, 9, 92–102. [Google Scholar]
- Krause, F.; Wilke, J.; Niederer, D.; Vogt, L.; Banzer, W. Acute Effects of Foam Rolling on Passive Stiffness, Stretch Sensation and Fascial Sliding: A Randomized Controlled Trial. Hum. Mov. Sci. 2019, 67, 102514. [Google Scholar] [CrossRef]
- Behm, D.G.; Kibele, A. Effects of Differing Intensities of Static Stretching on Jump Performance. Eur. J. Appl. Physiol. 2007, 101, 587–594. [Google Scholar] [CrossRef]
- Masaki, M.; Aoyama, T.; Murakami, T.; Yanase, K.; Ji, X.; Tateuchi, H.; Ichihashi, N. Association of Low Back Pain with Muscle Stiffness and Muscle Mass of the Lumbar Back Muscles, and Sagittal Spinal Alignment in Young and Middle-Aged Medical Workers. Clin. Biomech. 2017, 49, 128–133. [Google Scholar] [CrossRef] [Green Version]
- Farnebäck, G.; Motion, T.-F. Two-Frame Motion Estimation Based on Polynomial Expansion. In Image Analysis; Lecture Notes in Computer Science; Springer: Berlin/Heidelberg, Germany, 2003; Volume 2749, pp. 363–370. ISBN 978-3-540-40601-3. [Google Scholar]
- Yamashita, T.; Ozawa, K.; Gamada, K. Validity and Reliability of Velocity Measurements on Ultrasonography Using Custom Software with an Optical-Flow Algorithm. J. Phys. Ther. Sci. 2020, 32, 130–139. [Google Scholar] [CrossRef]
- Kawanishi, K.; Kudo, S.; Yokoi, K. Relationship between Gliding and Lateral Femoral Pain in Patients with Trochanteric Fracture. Arch. Phys. Med. Rehabil. 2020, 101, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Hui, S.S.; Yuen, P.Y. Validity of the Modified Back-Saver Sit-and-Reach Test: A Comparison with Other Protocols. Med. Sci. Sport. Exerc. 2000, 32, 1655–1659. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Murakami, H.; Inaki, A.; Mochizuki, T.; Demura, S.; Nakase, J.; Yoshioka, K.; Yokogawa, N.; Igarashi, T.; Takahashi, N.; et al. Innovative Exercise Device for the Abdominal Trunk Muscles: An Early Validation Study. PLoS ONE 2017, 12, e0172934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Science; Routledge: London, UK, 1988; ISBN 9781134742707. [Google Scholar]
- Richardson, J.T.E. Eta Squared and Partial Eta Squared as Measures of Effect Size in Educational Research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Nakajima, H.; Imanishi, N.; Minabe, T.; Kishi, K.; Aiso, S. Anatomical Study of Subcutaneous Adipofascial Tissue: A Concept of the Protective Adipofascial System (PAFS) and Lubricant Adipofascial System (LAFS). Scand. J. Plast. Reconstr. Surg. Hand Surg. 2004, 38, 261–266. [Google Scholar] [CrossRef]
- Stecco, C.; Stern, R.; Porzionato, A.; Macchi, V.; Masiero, S.; Stecco, A.; De Caro, R. Hyaluronan within Fascia in the Etiology of Myofascial Pain. Surg. Radiol. Anat. 2011, 33, 891–896. [Google Scholar] [CrossRef]
- Cowman, M.K.; Schmidt, T.A.; Raghavan, P.; Stecco, A. Viscoelastic Properties of Hyaluronan in Physiological Conditions. F1000Research 2015, 4, 622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, J.D.; Spence, A.J.; Behm, D.G. Roller Massage Decreases Spinal Excitability to the Soleus. J. Appl. Physiol. 2018, 124, 950–959. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.H.; Chai, H.M.; Shau, Y.W.; Wang, C.L.; Wang, S.F. Increased Sliding of Transverse Abdominis during Contraction after Myofascial Release in Patients with Chronic Low Back Pain. Man. Ther. 2016, 23, 69–75. [Google Scholar] [CrossRef]
- Claus, A.P.; Hides, J.A.; Moseley, G.L.; Hodges, P.W. Different Ways to Balance the Spine in Sitting: Muscle Activity in Specific Postures Differs between Individuals with and without a History of Back Pain in Sitting. Clin. Biomech. 2018, 52, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Ożóg, P.; Weber-Rajek, M.; Radzimińska, A.; Goch, A. Analysis of Muscle Activity Following the Application of Myofascial Release Techniques for Low-Back Pain-A Randomized-Controlled Trial. J. Clin. Med. 2021, 10, 4039. [Google Scholar] [CrossRef]
- Kozanek, M.; Wang, S.; Passias, P.G.; Xia, Q.; Li, G.; Bono, C.M.; Wood, K.B.; Li, G. Range of Motion and Orientation of the Lumbar Facet Joints In Vivo. Spine 2009, 34, E689–E696. [Google Scholar] [CrossRef] [PubMed]
- McGill, S.M.; Santaguida, L.; Stevens, J. Measurement of the Trunk Musculature from T5 to L5 Using MRI Scans of 15 Young Males Corrected for Muscle Fibre Orientation. Clin. Biomech. 1993, 8, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Hides, J.; Stanton, W.; Mendis, M.D.; Sexton, M. The Relationship of Transversus Abdominis and Lumbar Multifidus Clinical Muscle Tests in Patients with Chronic Low Back Pain. Man. Ther. 2011, 16, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Bergmark, A. Stability of the Lumbar Spine. Acta Orthop. Scand. 1989, 60, 1–54. [Google Scholar] [CrossRef]
- Vleeming, A.; Schuenke, M.D.; Danneels, L.; Willard, F.H. The Functional Coupling of the Deep Abdominal and Paraspinal Muscles: The Effects of Simulated Paraspinal Muscle Contraction on Force Transfer to the Middle and Posterior Layer of the Thoracolumbar Fascia. J. Anat. 2014, 225, 447–462. [Google Scholar] [CrossRef]
- Cervera-Cano, M.; López-González, L.; Valcárcel-Linares, D.; Fernández-Carnero, S.; Achalandabaso-Ochoa, A.; Andrés-Sanz, V.; Pecos-Martín, D. Core Synergies Measured with Ultrasound in Subjects with Chronic Non-specific Low Back Pain and Healthy Subjects: A Systematic Review. Sensors 2022, 22, 8684. [Google Scholar] [CrossRef]
- Puentedura, E.J.; Buckingham, S.J.; Morton, D.; Montoya, C.; Fernandez de Las Penas, C. Immediate Changes in Resting and Contracted Thickness of Transversus Abdominis after Dry Needling of Lumbar Multifidus in Healthy Participants: A Randomized Controlled Crossover Trial. J. Manip. Physiol. Ther. 2017, 40, 615–623. [Google Scholar] [CrossRef]
- Wilke, J.; Schleip, R.; Yucesoy, C.A.; Banzer, W. Not Merely a Protective Packing Organ? A Review of Fascia and Its Force Transmission Capacity. J. Appl. Physiol. 2018, 124, 234–244. [Google Scholar] [CrossRef]
- Drust, B.; Atkinson, G.; Gregson, W.; French, D.; Binningsley, D. The Effects of Massage on Intra Muscular Temperature in the Vastus Lateralis in Humans. Int. J. Sport. Med. 2003, 24, 395–399. [Google Scholar] [CrossRef]
- De Ruiter, C.J.; De Haan, A. Temperature Effect on the Force/Velocity Relationship of the Fresh and Fatigued Human Adductor Pollicis Muscle. Pflugers Arch. 2000, 440, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Racinais, S.; Oksa, J. Temperature and Neuromuscular Function. Scand. J. Med. Sci. Sport. 2010, 20, 1–18. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre-Intervention | Post-Intervention | Change Value [95% CI] | ES | Interaction | ES | |||
|---|---|---|---|---|---|---|---|---|
| d | F | P | Partial η2 | |||||
| Gliding | RM | 0.73 ± 0.13 | 0.65 ± 0.15 | −0.08 ± 0.12 ** [−0.13, −0.03] | 0.66 | 5.358 | 0.008 ** | 0.189 |
| SS | 0.71 ± 0.11 | 0.70 ± 0.11 | −0.01 ± 0.12 [−0.06, 0.04] | 0.08 | ||||
| CON | 0.70 ± 0.13 | 0.72 ± 0.13 | 0.01 ± 0.09 [−0.03, 0.05] | 0.15 | ||||
| Lumber flexibility (cm) | RM | 37.0 ± 10.6 | 38.3 ± 10.1 | 1.27 ± 1.65 ** [0.57, 1.96] | 0.77 | 5.135 | 0.010 * | 0.183 |
| SS | 37.8 ± 10.4 | 38.5 ± 10.3 | 0.67 ± 1.70 [−0.05, 1.38] | 0.39 | ||||
| CON | 37.6 ± 10.3 | 37.3 ± 10.0 | −0.23 ± 1.31 [−0.78, 0.32] | 0.18 | ||||
| Abdominal trunk muscle strength (kPa) | RM | 20.4 ± 6.2 | 22.0 ± 6.2 | 1.56 ± 1.82 ** [0.79, 2.33] | 0.85 | 6.081 | 0.005 ** | 0.209 |
| SS | 21.6 ± 6.3 | 22.1 ± 6.0 | 0.54 ± 1.56 [−0.12, 1.20] | 0.34 | ||||
| CON | 21.5 ± 5.6 | 21.2 ± 5.9 | −0.24 ± 1.92 [−1.05, 0.57] | 0.13 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakai, Y.; Oe, K.; Matsuno, R.; Kiyama, R.; Kawada, M.; Takeshita, Y.; Miyazaki, T.; Araki, S. Effect of Self-Myofascial Release of the Lower Back on Myofascial Gliding, Lumbar Flexibility, and Abdominal Trunk Muscle Strength: A Crossover Study. Sports 2023, 11, 147. https://doi.org/10.3390/sports11080147
Nakai Y, Oe K, Matsuno R, Kiyama R, Kawada M, Takeshita Y, Miyazaki T, Araki S. Effect of Self-Myofascial Release of the Lower Back on Myofascial Gliding, Lumbar Flexibility, and Abdominal Trunk Muscle Strength: A Crossover Study. Sports. 2023; 11(8):147. https://doi.org/10.3390/sports11080147
Chicago/Turabian StyleNakai, Yuki, Katsutoshi Oe, Ryuko Matsuno, Ryoji Kiyama, Masayuki Kawada, Yasufumi Takeshita, Takasuke Miyazaki, and Sota Araki. 2023. "Effect of Self-Myofascial Release of the Lower Back on Myofascial Gliding, Lumbar Flexibility, and Abdominal Trunk Muscle Strength: A Crossover Study" Sports 11, no. 8: 147. https://doi.org/10.3390/sports11080147