
Assessment of Spinal and Pelvic Kinematics Using Inertial Measurement Units in Clinical Subgroups of Persistent Non-Specific Low Back Pain

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
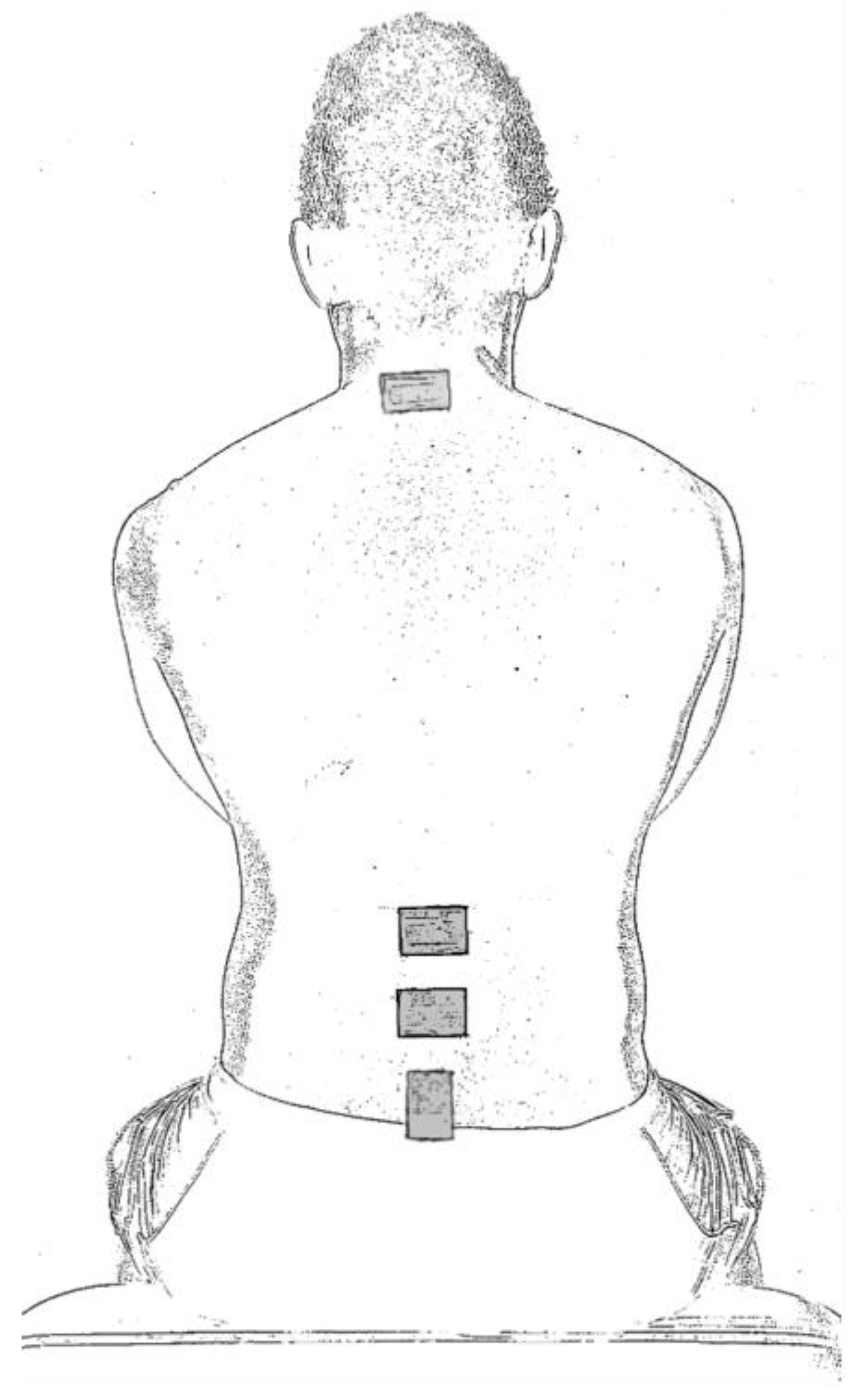
2.2. IMU Configuration
2.3. Testing Protocol
2.4. Data Acquisition and Processing
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
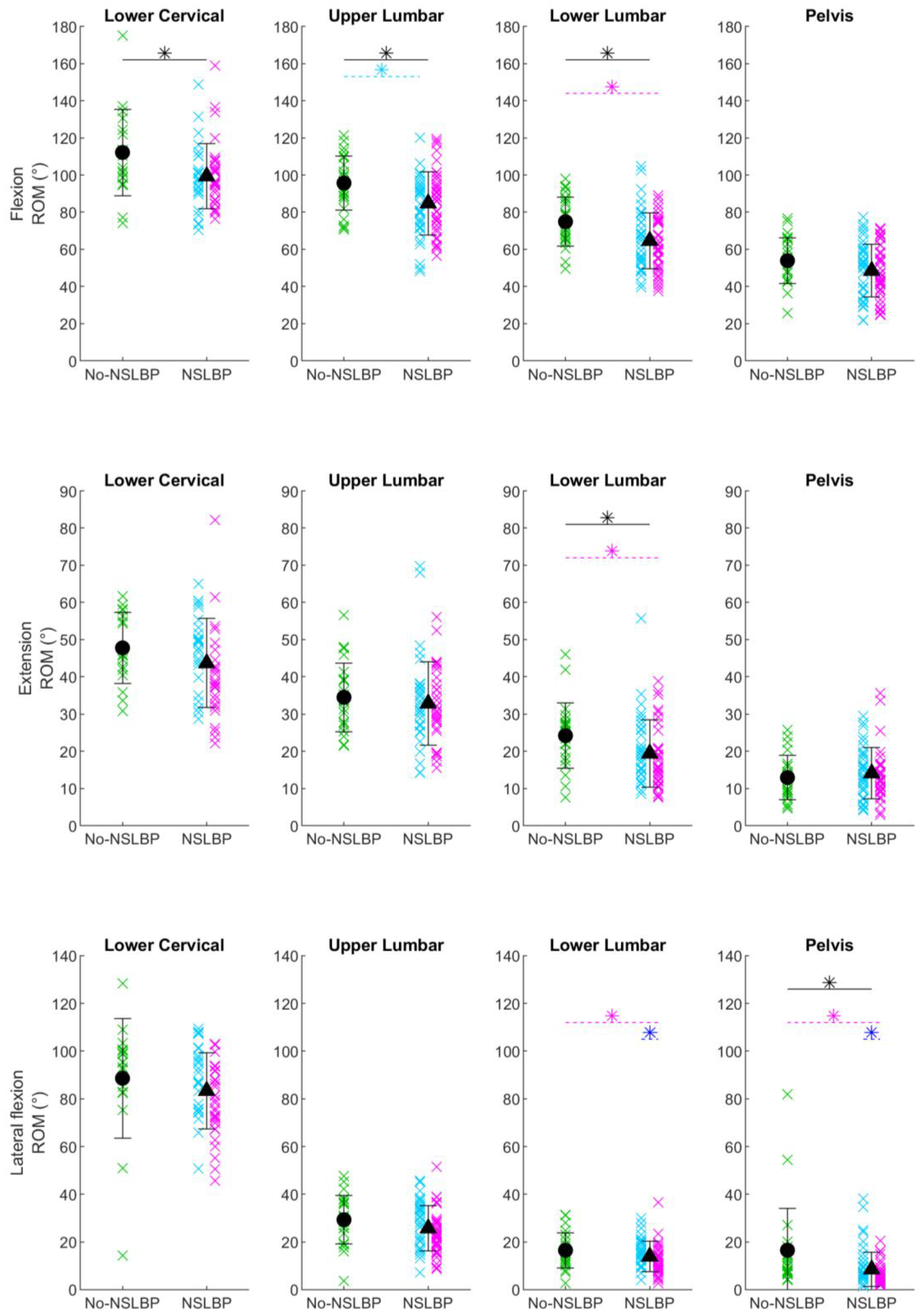
3.2. Between-Group Differences in Spinal and Pelvic Kinematics
3.2.1. NSLBP vs. no-NSLBP
3.2.2. No-NSLBP vs. EP-NSLBP vs. FP-NSLBP
4. Discussion
4.1. Trunk Kinematics
4.2. Upper and Lower Lumbar Spine and Pelvic Kinematics
4.3. Clinical Implications
4.4. Limitations
4.5. Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoy, D.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Bain, C.; Williams, G.; Smith, E.; Vos, T.; Barendregt, J.; et al. The global burden of low back pain: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 968–974. [Google Scholar] [CrossRef] [PubMed]
- Clark, S.; Horton, R. Low back pain: A major global challenge. Lancet 2018, 391, 2302. [Google Scholar] [CrossRef] [PubMed]
- Buchbinder, R.; van Tulder, M.; Öberg, B.; Costa, L.M.; Woolf, A.; Schoene, M.; Croft, P.; Hartvigsen, J.; Cherkin, D.; Foster, N.E.; et al. Low back pain: A call for action. Lancet 2018, 391, 2384–2388. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-specific low back pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef] [PubMed]
- Osumi, M.; Sumitani, M.; Otake, Y.; Nishigami, T.; Mibu, A.; Nishi, Y.; Imai, R.; Sato, G.; Nagakura, Y.; Morioka, S. Kinesiophobia modulates lumbar movements in people with chronic low back pain: A kinematic analysis of lumbar bending and returning movement. Eur. Spine J. 2019, 28, 1572–1578. [Google Scholar] [CrossRef] [PubMed]
- Panhale, V.P.; Gurav, R.S.; Nahar, S.K. Association of Physical Performance and Fear-Avoidance Beliefs in Adults with Chronic Low Back Pain. Ann. Med. Health Sci. Res. 2016, 6, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Park, S. The relationship between physical capacity and fear avoidance beliefs in patients with chronic low back pain. J. Phys. Ther. Sci. 2017, 29, 1712–1714. [Google Scholar] [CrossRef] [PubMed]
- Vlaeyen, J.W.S.; Linton, S.J. Fear-avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain 2000, 85, 317–332. [Google Scholar] [CrossRef]
- Oliveira, C.B.; Maher, C.G.; Pinto, R.Z.; Traeger, A.C.; Lin, C.-W.C.; Chenot, J.-F.; van Tulder, M.; Koes, B.W. Clinical practice guidelines for the management of non-specific low back pain in primary care: An updated overview. Eur. Spine J. 2018, 27, 2791–2803. [Google Scholar] [CrossRef]
- NICE. National Institute of Health and Care Excellence, Low Back Pain and Sciatica over 16s: Assessment and Management (NICE Guideline NG59); Last Updated 2020; NICE: London, UK, 2016. [Google Scholar]
- van Dieën, J.H.; Reeves, N.P.; Kawchuk, G.; van Dillen, L.R.; Hodges, P.W. Motor Control Changes in Low Back Pain: Divergence in Presentations and Mechanisms. J. Orthop. Sports Phys. Ther. 2019, 49, 370–379. [Google Scholar] [CrossRef]
- Hides, J.A.; Donelson, R.; Lee, D.; Prather, H.; Sahrmann, S.A.; Hodges, P.W. Convergence and Divergence of Exercise-Based Approaches That Incorporate Motor Control for the Management of Low Back Pain. J. Orthop. Sports Phys. Ther. 2019, 49, 437–452. [Google Scholar] [CrossRef] [PubMed]
- Fourney, D.R.; Andersson, G.; Arnold, P.M.; Dettori, J.; Cahana, A.; Fehlings, M.G.; Norvell, D.; Samartzis, D.; Chapman, J.R. Chronic Low Back Pain: A Heterogeneous Condition With Challenges for an Evidence-Based Approach. Spine 2011, 36, S1–S9. [Google Scholar] [CrossRef] [PubMed]
- Foster, N.E.; Hill, J.C.; O’Sullivan, P.; Hancock, M. Stratified models of care. Best Pract. Res. Clin. Rheumatol. 2013, 27, 649–661. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, P. Diagnosis and classification of chronic low back pain disorders: Maladaptive movement and motor control impairments as underlying mechanism. Man. Ther. 2005, 10, 242–255. [Google Scholar] [CrossRef] [PubMed]
- Sahrmann, S.A. Diagnosis and Treatment of Movement Impairment Syndromes; Mosby: St. Louis, MA, USA, 2002. [Google Scholar]
- McKenzie, R.; May, S. Lumbar Spine, Mechanical Diagnosis and Therapy; Spinal Publications Ltd: Waikanae, New Zealand, 2003. [Google Scholar]
- Lemeunier, N.; Jeoun, E.B.; Suri, M.; Tuff, T.; Shearer, H.; Mior, S.; Wong, J.J.; da Silva-Oolup, S.; Torres, P.; D’Silva, C.; et al. Reliability and validity of clinical tests to assess posture, pain location, and cervical spine mobility in adults with neck pain and its associated disorders: Part 4. A systematic review from the cervical assessment and diagnosis research evaluation (CADRE) collaboration. Musculoskelet. Sci. Pract. 2018, 38, 128–147. [Google Scholar] [CrossRef] [PubMed]
- Fedorak, C.; Ashworth, N.; Marshall, J.; Paull, H. Reliability of the Visual Assessment of Cervical and Lumbar Lordosis: How Good Are We? Spine 2003, 28, 1857–1859. [Google Scholar] [CrossRef] [PubMed]
- Astfalck, R.G.; O’Sullivan, P.B.; Straker, L.M.; Smith, A.J.; Burnett, A.; Caneiro, J.P.; Dankaerts, W. Sitting postures and trunk muscle activity in adolescents with and without nonspecific chronic low back pain: An analysis based on subclassification. Spine 2010, 35, 1387–1395. [Google Scholar] [CrossRef] [PubMed]
- Gombatto, S.P.; Collins, D.R.; Sahrmann, S.A.; Engsberg, J.R.; Van Dillen, L.R. Patterns of lumbar region movement during trunk lateral bending in 2 subgroups of people with low back pain. Phys. Ther. 2007, 87, 441–454. [Google Scholar] [CrossRef]
- Dankaerts, W.; O’Sullivan, P.; Burnett, A.; Straker, L. Differences in sitting postures are associated with nonspecific chronic low back pain disorders when patients are subclassified. Spine 2006, 31, 698–704. [Google Scholar] [CrossRef]
- Hemming, R.; Sheeran, L.; van Deursen, R.; Sparkes, V. Non-specific chronic low back pain: Differences in spinal kinematics in subgroups during functional tasks. Eur. Spine J. 2018, 27, 163–170. [Google Scholar] [CrossRef]
- Sheeran, L.; Sparkes, V.; Caterson, B.; Busse-Morris, M.; van Deursen, R. Spinal Position Sense and Trunk Muscle Activity During Sitting and Standing in Nonspecific Chronic Low Back Pain Classification Analysis. Spine 2012, 37, E486–E495. [Google Scholar] [CrossRef] [PubMed]
- Don, R.; Capodaglio, P.; Cimolin, V.; Benedetti, M.G.; D’Osualdo, F.; Frigo, C.; Vismara, L.; Negrini, S. Instrumental measures of spinal function: Is it worth? A state-of-the art from a clinical perspective. Eur. J. Phys. Rehabil. Med. 2012, 48, 255–273. [Google Scholar] [PubMed]
- Slater, H.; Briggs, A.M. Models of Care for musculoskeletal pain conditions: Driving change to improve outcomes. Pain Manag. 2017, 7, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Al-Amri, M.; Nicholas, K.; Button, K.; Sparkes, V.; Sheeran, L.; Davies, J.L. Inertial Measurement Units for Clinical Movement Analysis: Reliability and Concurrent Validity. Sensors 2018, 18, 719. [Google Scholar] [CrossRef]
- Giansanti, D.; Maccioni, G.; Benvenuti, F.; Macellari, V. Inertial measurement units furnish accurate trunk trajectory reconstruction of the sit-to-stand manoeuvre in healthy subjects. Med. Biol. Eng. Comput. 2007, 45, 969–976. [Google Scholar] [CrossRef]
- Ha, T.H.; Saber-Sheikh, K.; Moore, A.P.; Jones, M.P. Measurement of lumbar spine range of movement and coupled motion using inertial sensors—A protocol validity study. Man. Ther. 2012, 18, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Howarth, S.J.; Graham, R.B. Sensor positioning and experimental constraints influence estimates of local dynamic stability during repetitive spine movements. J. Biomech. 2015, 48, 1219–1223. [Google Scholar] [CrossRef] [PubMed]
- Beange, K.; Chan, A.; Graham, R. Wearable sensor performance for clinical motion tracking of the lumbar spine. CMBES Proc. 2019, 42. Available online: https://proceedings.cmbes.ca/index.php/proceedings/article/view/859 (accessed on 25 March 2024).
- Beange, K.H.; Chan, A.D.; Beaudette, S.M.; Graham, R.B. Concurrent validity of a wearable IMU for objective assessments of functional movement quality and control of the lumbar spine. J. Biomech. 2019, 97, 109356. [Google Scholar] [CrossRef]
- Bauer, C.M.; Heimgartner, M.; Rast, F.M.; Ernst, M.J.; Oetiker, S.; Kool, J. Reliability of lumbar movement dysfunction tests for chronic low back pain patients. Man. Ther. 2016, 24, 81–84. [Google Scholar] [CrossRef]
- Bauer, C.M.; Rast, F.M.; Ernst, M.J.; Oetiker, S.; Meichtry, A.; Kool, J.; Rissanen, S.M.; Suni, J.H.; Kankaanpää, M. Pain intensity attenuates movement control of the lumbar spine in low back pain. J. Electromyogr. Kinesiol. 2015, 25, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Bayartai, M.E.; Taulaniemi, A.; Tokola, K.; Vähä-Ypyä, H.; Parkkari, J.; Husu, P.; Kankaanpää, M.; Vasankari, T.; Michael Bauer, C.; Luomajoki, H. Role of the interaction between lumbar kinematics and accelerometer-measured physical activity in bodily pain, physical functioning and work ability among health care workers with low back pain. J. Electromyogr. Kinesiol. 2023, 69, 102744. [Google Scholar] [CrossRef] [PubMed]
- Graham, R.B.; Dupeyron, A.; van Dieën, J.H. Between-day reliability of IMU-derived spine control metrics in patients with low back pain. J. Biomech. 2020, 113, 110080. [Google Scholar] [CrossRef]
- Larivière, C.; Mecheri, H.; Shahvarpour, A.; Gagnon, D.; Shirazi-Adl, A. Criterion validity and between-day reliability of an inertial-sensor-based trunk postural stability test during unstable sitting. J. Electromyogr. Kinesiol. 2013, 23, 899–907. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Yoon, C.; Kim, K.; Cho, M.; Kim, H.C.; Chung, S.G. Lumbar Stability in Healthy Individuals and Low Back Pain Patients Quantified by Wall Plank-and-Roll Test. PM&R 2019, 11, 483–494. [Google Scholar] [CrossRef]
- Meinke, A.; Peters, R.; Knols, R.H.; Swanenburg, J.; Karlen, W. Feedback on Trunk Movements from an Electronic Game to Improve Postural Balance in People with Nonspecific Low Back Pain: Pilot Randomized Controlled Trial. JMIR Serious Games 2022, 10, e31685. [Google Scholar] [CrossRef] [PubMed]
- Mjøsund, H.L.; Boyle, E.; Kjaer, P.; Mieritz, R.M.; Skallgård, T.; Kent, P. Clinically acceptable agreement between the ViMove wireless motion sensor system and the Vicon motion capture system when measuring lumbar region inclination motion in the sagittal and coronal planes. BMC Musculoskelet. Disord. 2017, 18, 124. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, R.; Potter, M.N.; Carollo, J.J.; Howell, D.R.; Sweeney, E.A. Peak sagittal plane spine kinematics in female gymnasts with and without a history of low back pain. Clin. Biomech. 2020, 76, 105019. [Google Scholar] [CrossRef]
- Senington, B.; Lee, R.Y.; Williams, J.M. Biomechanical risk factors of lower back pain in cricket fast bowlers using inertial measurement units: A prospective and retrospective investigation. BMJ Open Sport Exerc. Med. 2020, 6, e000818. [Google Scholar] [CrossRef]
- Tanigawa, A.; Morino, S.; Aoyama, T.; Takahashi, M. Gait analysis of pregnant patients with lumbopelvic pain using inertial sensor. Gait Posture 2018, 65, 176–181. [Google Scholar] [CrossRef]
- Telles, G.F.; Ferreira, A.S.; Junior, P.M.P.; Lemos, T.; Bittencourt, J.V.; Nogueira, L.A.C. Concurrent validity of the inertial sensors for assessment of balance control during quiet standing in patients with chronic low back pain and asymptomatic individuals. J. Med. Eng. Technol. 2022, 46, 354–362. [Google Scholar] [CrossRef]
- Triantafyllou, A.; Papagiannis, G.; Stasi, S.; Gkrilias, P.; Kyriakidou, M.; Kampouroglou, E.; Skouras, A.Z.; Tsolakis, C.; Georgoudis, G.; Savvidou, O.; et al. Lumbar Kinematics Assessment of Patients with Chronic Low Back Pain in Three Bridge Tests Using Miniaturized Sensors. Bioengineering 2023, 10, 339. [Google Scholar] [CrossRef] [PubMed]
- Trinidad-Fernández, M.; Beckwée, D.; Cuesta-Vargas, A.; González-Sánchez, M.; Moreno, F.A.; González-Jiménez, J.; Joos, E.; Vaes, P. Validation, Reliability, and Responsiveness Outcomes Of Kinematic Assessment with an RGB-D Camera to Analyze Movement in Subacute and Chronic Low Back Pain. Sensors 2020, 20, 689. [Google Scholar] [CrossRef] [PubMed]
- Wattananon, P.; Kongoun, S.; Chohan, A.; Richards, J. The use of statistical parametric mapping to determine altered movement patterns in people with chronic low back pain. J. Biomech. 2023, 153, 111601. [Google Scholar] [CrossRef] [PubMed]
- Laird, R.A.; Keating, J.L.; Ussing, K.; Li, P.; Kent, P. Does movement matter in people with back pain? Investigating ‘atypical’ lumbo-pelvic kinematics in people with and without back pain using wireless movement sensors. BMC Musculoskelet. Disord. 2019, 20, 28. [Google Scholar] [CrossRef] [PubMed]
- Laird, R.A.; Kent, P.; Keating, J.L. How consistent are lordosis, range of movement and lumbo-pelvic rhythm in people with and without back pain? BMC Musculoskelet. Disord. 2016, 17, 403. [Google Scholar] [CrossRef] [PubMed]
- Laird, R.A.; Keating, J.L.; Kent, P. Subgroups of lumbo-pelvic flexion kinematics are present in people with and without persistent low back pain. BMC Musculoskelet. Disord. 2018, 19, 309. [Google Scholar] [CrossRef] [PubMed]
- Dankaerts, W.; O’Sullivan, P.; Burnett, A.; Straker, L.; Davey, P.; Gupta, R. Discriminating healthy controls and two clinical subgroups of nonspecific chronic low back pain patients using trunk muscle activation and lumbosacral kinematics of postures and movements: A statistical classification model. Spine 2009, 34, 1610–1618. [Google Scholar] [CrossRef]
- Bacon, Z.; Hicks, Y.; Al-Amri, M.; Sheeran, L. Automatic Low Back Pain Classification Using Inertial Measurement Units: A Preliminary Analysis. Procedia Comput. Sci. 2020, 176, 2822–2831. [Google Scholar] [CrossRef]
- Ferreira-Valente, M.A.; Pais-Ribeiro, J.L.; Jensen, M.P. Validity of four pain intensity rating scales. Pain 2011, 152, 2399–2404. [Google Scholar] [CrossRef]
- Fairbank, J.C.; Pynsent, P.B. The Oswestry Disability Index. Spine 2000, 25, 2940–2952. [Google Scholar] [CrossRef] [PubMed]
- Roelofs, J.; Goubert, L.; Peters, M.L.; Vlaeyen, J.W.S.; Crombez, G. The Tampa Scale for Kinesiophobia: Further examination of psychometric properties in patients with chronic low back pain and fibromyalgia. Eur. J. Pain 2004, 8, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Sheeran, L.; Robling, M. Spinal Function Assessment And Exercise Performance Framework For Low Back Pain. Orthop Procs. 2019, 101-B (Suppl. 9), 40. [Google Scholar]
- Waddell, G.; Somerville, D.; Henderson, I.; Newton, M. Objective clinical evaluation of physical impairment in chronic low back pain. Spine 1992, 17, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Mazzone, B.; Wood, R.; Gombatto, S. Spine Kinematics during Prone Extension in People with and without Low Back Pain and among Classification-Specific Low Back Pain Subgroups. J. Orthop. Sports Phys. Ther. 2016, 46, 571–579. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, M.J.; Smorenburg, N.T.; Heerkens, Y.F.; Mollema, J.; Kiers, H.; Nijhuis-van der Sanden, M.W.; Visser, B. Assessment instruments of movement quality in patients with non-specific low back pain: A systematic review and selection of instruments. Gait Posture 2020, 76, 346–357. [Google Scholar] [CrossRef] [PubMed]
- Errabity, A.; Calmels, P.; Han, W.-S.; Bonnaire, R.; Pannetier, R.; Convert, R.; Molimard, J. The effect of low back pain on spine kinematics: A systematic review and meta-analysis. Clin. Biomech. 2023, 108, 106070. [Google Scholar] [CrossRef] [PubMed]
- Laird, R.A.; Gilbert, J.; Kent, P.; Keating, J.L. Comparing lumbo-pelvic kinematics in people with and without back pain: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2014, 15, 229. [Google Scholar] [CrossRef]
- Matheve, T.; De Baets, L.; Bogaerts, K.; Timmermans, A. Lumbar range of motion in chronic low back pain is predicted by task-specific, but not by general measures of pain-related fear. Eur. J. Pain 2019, 23, 1171–1184. [Google Scholar] [CrossRef]
- Sadler, S.G.; Spink, M.J.; Ho, A.; De Jonge, X.J.; Chuter, V.H. Restriction in lateral bending range of motion, lumbar lordosis, and hamstring flexibility predicts the development of low back pain: A systematic review of prospective cohort studies. BMC Musculoskelet. Disord. 2017, 18, 179. [Google Scholar] [CrossRef]
- Riley, S.P.; Swanson, B.T.; Dyer, E. Are movement-based classification systems more effective than therapeutic exercise or guideline based care in improving outcomes for patients with chronic low back pain? A systematic review. J. Man. Manip. Ther. 2019, 27, 5–14. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Inclusion Criteria | |
|---|---|
| Age between 18 and 75 years | |
| Low back pain of non-specific nature for longer than 3 months | |
Clear mechanical basis for the pain disorder with a diagnosis of motor control impairment (MCI), characterised by unrestricted yet painful movement and pain-provoking behaviour in flexion or extension [15].
| |
| Able to speak and understand English well enough to complete questionnaires independently | |
| Exclusion Criteria | |
| Primary pain area different to lower back (from T12 to buttock line), e.g., leg pain, thoracic pain | |
| Acute exacerbation of pain at the time of testing, rendering the individual unable to undertake the testing procedure | |
| Specific diagnosis for pain (nerve root compression, radicular pain/radiculopathy, disc herniation, spondylolisthesis, spinal stenosis) | |
| Surgery (lower limb or abdominal surgery in last 6 months, any spinal surgery) | |
| Injection therapy for pain relief in the last 3 months | |
| Rheumatologic/inflammatory disease (e.g., psoriatic arthritis, rheumatoid arthritis, ankylosing spondylitis, Scheuermann’s disease), scoliosis (if a primary pain driver) | |
| Progressive neurological or neurodegenerative conditions (e.g., multiple sclerosis, Parkinson’s disease, motor neuron disease) | |
| Red flags/serious pathology (malignancy, acute trauma such as fracture, systemic infection, spinal cord compression, cauda equina syndrome) | |
| Pregnancy/breast feeding | |
| Assessment Test | Instruction |
|---|---|
| Flexion | From standing, bend your back forwards as far as is comfortable and return up to standing |
| Extension | From standing, bend your back backwards as far as is comfortable and return up to standing |
| Lateral flexion | From standing, bend sideways as far as is comfortable to the right/left, then back to the middle and sideways to the other side and back to the middle again |
| No NSLBP n = 26 | FP-NSLBP n = 38 | EP-NSLBP n = 43 | p Value | |
|---|---|---|---|---|
| Female | 16 (62%) | 13 (34%) | 32 (74%) † | 0.001 |
| Male | 10 (38%) | 25 (66%) | 11 (26%) † | |
| Age | 37.0 (12.2) [22–69] | 44.9 (12.3) [22–79] * | 46.6 (11.6) [25–698] * | 0.006 |
| BMI (kg/m2) | 24.7 (3.9) [19.0–34.4] | 27.2 (4.3) [18.9–37.6] | 28.4 (5.2) [19.8–37.3] * | 0.006 |
| VAS | - | 4.0 (1.3) [1.8–6.3] | 3.9 (1.2) [1–6.8] | 0.76 |
| ODI score | - | 19.6 (1.6) [2–44] | 19.3 (8.9) [4–37] | 0.88 |
| TSK score | - | 33.2 (6.5) [17–44] | 33.0 (6.9) [17–45] | 0.91 |
| Task | Region | No-NSLBP | NSLBP (All) | FP-NSLBP | EP-NSLBP | t-Test p Value | ANOVA Main Effect p Value | ANOVA Post Hoc Pairwise Comparisons (p Value) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| No-NSLBP v FP-NSLBP | No-NSLBP v EP-NSLBP | NSLBP-FP v NSLBP-EP | ||||||||
| Flexion ROM (°) | LCx | 112 (23) [102, 123] | 99 (18) [95, 104] | 99 (18) [93, 106] | 100 (18) [93, 106] | 0.01 | 0.05 | 0.11 | 0.10 | >0.99 |
| ULx | 96 (14) [90, 101] | 85 (17) [81, 89] | 84 (17) [78, 89] | 86 (17) [81, 91] | 0.005 | 0.02 | 0.02 | 0.06 | >0.99 | |
| LLx | 75 (13) [70, 80] | 65 (15) [61, 68] | 66 (16) [61, 71] | 63 (14) [59, 68] | 0.003 | 0.008 | 0.08 | 0.005 | >0.99 | |
| P | 54 (12) [49, 59] | 48 (14) [45, 52] | 49 (15) [44, 54] | 48 (13) [43, 52] | 0.09 | 0.21 | n/a | |||
| Extension ROM (°) | LCx | 48 (10) [43, 52] | 44 (12) [40, 47] | 47 (10) [43, 51] | 40 (13) [35, 45] | 0.21 | 0.04 | >0.99 | 0.14 | 0.11 |
| ULx | 34 (9) [30, 38] | 33 (11) [30, 36] | 33 (13) [29, 38] | 33 (10) [29, 36] | 0.53 | 0.80 | n/a | |||
| LLx | 24 (9) [21, 28] | 19 (9) [17, 22] | 21 (9) [17, 24] | 18 (9) [15, 21] | 0.03 | 0.05 | 0.48 | 0.04 | 0.87 | |
| P | 13 (6) [10, 15] | 14 (7) [12, 16] | 14 (7) [12, 17] | 14 (7) [11, 16] | 0.47 | 0.71 | n/a | |||
| Lateral Flexion ROM (°) | LCx | 89 (25) [76, 101] | 83 (16) [79, 88] | 89 (15) [83, 95] | 79 (15) [73, 85] | 0.31 | 0.08 | n/a | ||
| ULx | 29 (10) [25, 33] | 26 (9) [24, 28] | 28 (10) [25, 31] | 24 (9) [21, 26] | 0.13 | 0.04 | >0.99 | 0.07 | 0.11 | |
| LLx | 16 (7) [13, 19] | 14 (6) [12, 15] | 16 (6) [14, 18] | 12 (6) [10, 14] | 0.11 | 0.01 | >0.99 | 0.04 | 0.02 | |
| P | 17 (18) [9, 24] | 9 (7) [7, 10] | 11 (9) [8, 14] | 7 (4) [5, 8] | 0.003 | 0.003 | 0.39 | 0.005 | 0.04 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sheeran, L.; Al-Amri, M.; Sparkes, V.; Davies, J.L. Assessment of Spinal and Pelvic Kinematics Using Inertial Measurement Units in Clinical Subgroups of Persistent Non-Specific Low Back Pain. Sensors 2024, 24, 2127. https://doi.org/10.3390/s24072127
Sheeran L, Al-Amri M, Sparkes V, Davies JL. Assessment of Spinal and Pelvic Kinematics Using Inertial Measurement Units in Clinical Subgroups of Persistent Non-Specific Low Back Pain. Sensors. 2024; 24(7):2127. https://doi.org/10.3390/s24072127
Chicago/Turabian StyleSheeran, Liba, Mohammad Al-Amri, Valerie Sparkes, and Jennifer L. Davies. 2024. "Assessment of Spinal and Pelvic Kinematics Using Inertial Measurement Units in Clinical Subgroups of Persistent Non-Specific Low Back Pain" Sensors 24, no. 7: 2127. https://doi.org/10.3390/s24072127