
Effects of High-Load Bench Press Training with Different Blood Flow Restriction Pressurization Strategies on the Degree of Muscle Activation in the Upper Limbs of Bodybuilders
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Methods
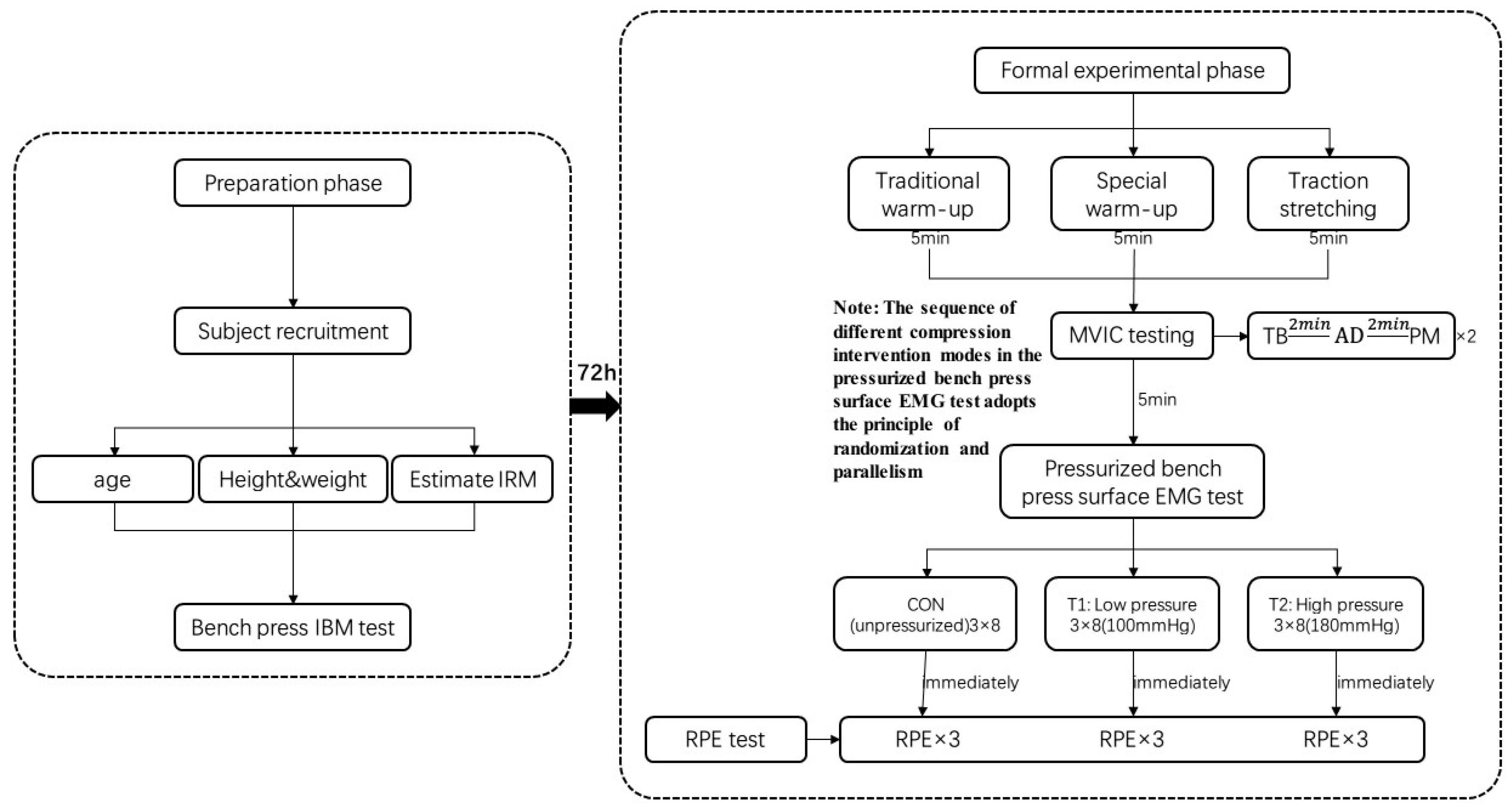
2.2.1. Experimental Design and Intervention Program
2.2.2. Testing of Experimental Indicators
- (1)
- Bench Press 1 RM Test
- (2)
- Maximum random isometric contraction (MVIC) test for target muscle groups of the upper limb
- (3)
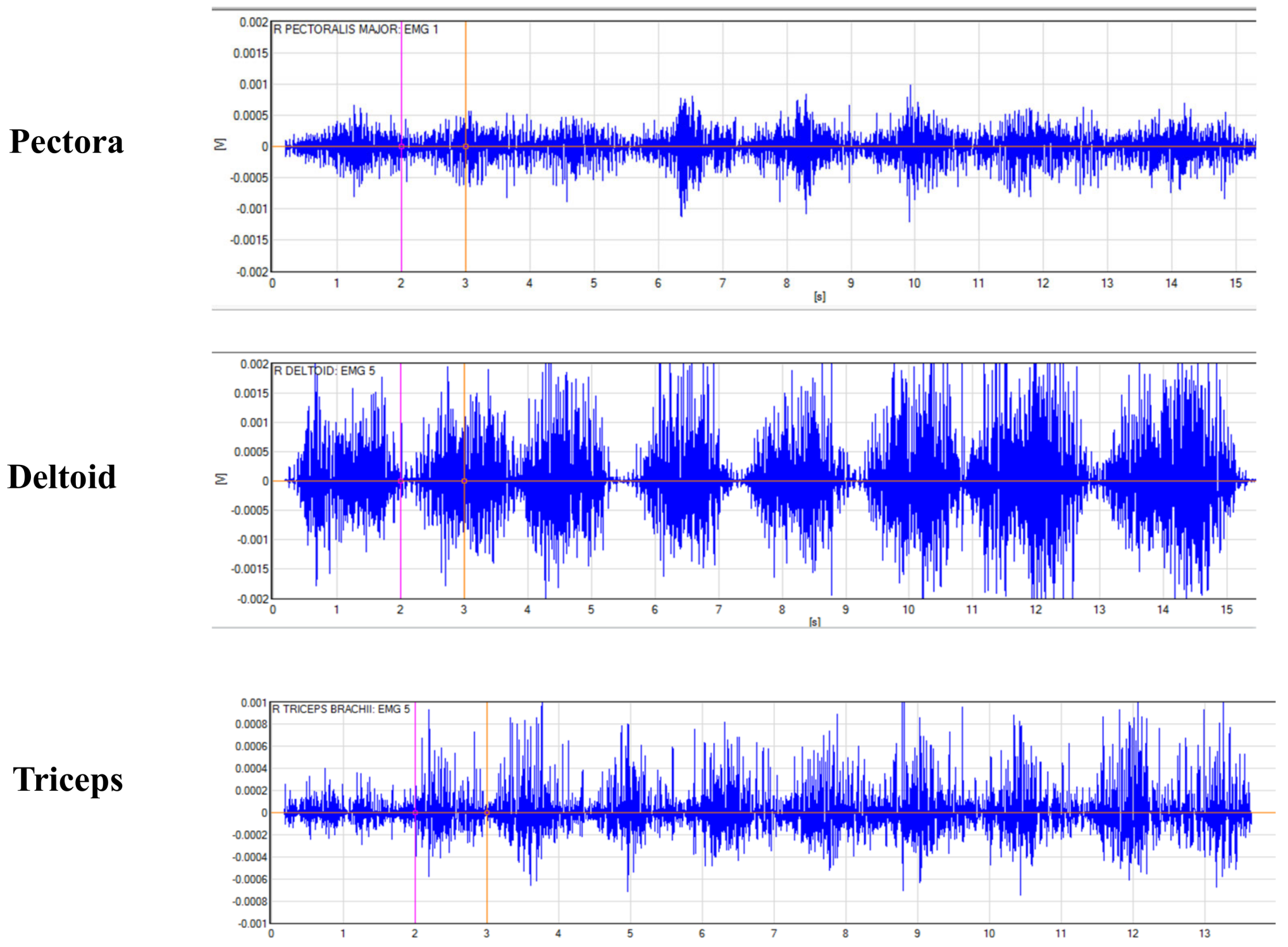
- Pressurized bench press training surface EMG test
- (4)
- Subjective fatigue (RPE) test
2.3. Statistical Methods
3. Results
3.1. Multiple Comparison Analysis
3.2. Changes in %MVIC Values of Target Muscles in Each Set of Bench Press Training in Different Pressurization Modes
3.3. Subjective Fatigue Results after High-Load Bench Press Training in Different Pressurization Modes
4. Discussion
- (1)
- Analysis of changes in the pectoralis major activation level
- (2)
- Analysis of changes in deltoid activation level
- (3)
- Analysis of changes in triceps activation
4.1. Analysis of Subjective Fatigue Test Results
4.2. Practical Application
4.3. Advantages of the Study
4.4. Study Limitations
4.5. Future Research Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Loenneke, J.P.; Thiebaud, R.S.; Abe, T.; Bemben, M.G. Blood flow restriction pressure recommendations: The hormesis hypothesis. Med. Hypotheses 2014, 82, 623–626. [Google Scholar] [CrossRef]
- Liu, S.; Wang, S.; Ji, W. Progress in the application and limitation of stress training. Chin. J. Rehabil. Med. 2022, 37, 6. [Google Scholar]
- Yu, L.; Wang, Z.; Gao, J.; Zhu, X. Effects of short-term pressure strength training on body composition and cardiovascular function in adult males. J. Beijing Sport Univ. 2022, 43, 132–139. [Google Scholar]
- Suga, T.; Okita, K.; Morita, N.; Yokota, T.; Hirabayashi, K.; Horiuchi, M.; Takada, S.; Takahashi, T.; Omokawa, M.; Kinugawa, S.; et al. Intramuscular metabolism during low-intensity resistance exercise with blood flow restriction. J. Appl. Physiol. (1985) 2009, 106, 1119–1124. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Liu, S.; Sun, P.; Li, W.; Lian, Z. Effects of different pressure blood flow restriction combined with low intensity resistance training on lower limb muscle and cardiopulmonary function of college students. Chin. J. Appl. Physiol. 2020, 36, 595–599. [Google Scholar]
- Christopher, A.F.; Jeremy, P.L.; Lindy, M.R.; Robert, S.T.; Michael, G.B. Methodological considerations for blood flow restricted resistance exercise. J. Trainology 2012, 1, 14–22. [Google Scholar]
- Yuan, W.T. Research on the effects of lower extremity pressurization combined with different resistance training on human function. Genom. Appl. Biol. 2018, 37, 8. [Google Scholar]
- Wei, J.; Li, B.; Feng, L.; Li, Y. Methodological factors and potential safety issues of blood flow restriction training. China Sports Sci. Technol. 2019, 55, 3–12. [Google Scholar]
- Torma, F.; Gombos, Z.; Fridvalszki, M.; Langmar, G.; Tarcza, Z.; Merkely, B.; Naito, H.; Ichinoseki-Sekine, N.; Takeda, M.; Murlasits, Z.; et al. Blood flow restriction in human skeletal muscle during rest periods after high-load resistance training down-regulates miR-206 and induces Pax7. J. Sport Health Sci. 2021, 10, 470–477. [Google Scholar] [CrossRef]
- Davids, C.J.; Næss, T.C.; Moen, M.; Cumming, K.T.; Horwath, O.; Psilander, N.; Ekblom, B.; Coombes, J.S.; Peake, J.; Raastad, T.; et al. Acute cellular and molecular responses and chronic adaptations to low-load blood flow restriction and high-load resistance exercise in trained individuals. J. Appl. Physiol. (1985) 2021, 131, 1731–1749. [Google Scholar] [CrossRef]
- Che, T.; Yang, T.; Liang, Y.; Li, Z. Effects of lower extremity low-intensity compression half-squat training on muscle activation and subjective fatigue of core muscle group. Sports Sci. 2021, 41, 59–66. [Google Scholar]
- Che, T.; Li, Z.; Zhao, Z.; Wei, W.; Sun, K.; Chen, C. Effects of low-intensity bench press training on muscle activation and subjective fatigue. J. Chengdu Univ. Phys. Educ. 2022, 48, 123–130. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human participants. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Sonkodi, B.; Kopa, Z.; Nyirády, P. Post Orgasmic Illness Syndrome (POIS) and Delayed Onset Muscle Soreness (DOMS): Do They Have Anything in Common? Cells 2021, 10, 14–28. [Google Scholar] [CrossRef]
- Konrad, P. The abc of emg. In A Pactical Introduction to Kinesiological Electromyography; Noraxon U.S.A. Inc.: Scottsdale, AZ, USA, 2005; Volume 1, pp. 30–35. [Google Scholar]
- Zourdos, M.C.; Goldsmith, J.A.; Helms, E.R.; Trepeck, C.; Halle, J.L.; Mendez, K.M.; Cooke, D.M.; Haischer, M.H.; Sousa, C.A.; Klemp, A.; et al. Proximity to Failure and Total Repetitions Performed in a Set Influences Accuracy of Intraset Repetitions in Reserve-Based Rating of Perceived Exertion. J. Strength Cond. Res. 2021, 35, S158–S165. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J.; Campos, Y.; Leitão, L.; Arriel, R.; Novaes, J.; Vianna, J. Does Acute Blood Flow Restriction with Pneumatic and Non-Pneumatic Non-Elastic Cuffs Promote Similar Responses in Blood Lactate, Growth Hormone, and Peptide Hormone? J. Hum. Kinet. 2020, 74, 85–97. [Google Scholar] [CrossRef]
- Zheng, B.; Zhang, Z. Study on the effects of different pressurized resistance training modes on human physiological and biomechanical characteristics after exercise. J. Southwest Norm. Univ. Nat. Sci. Ed. 2021, 46, 9. [Google Scholar]
- Zhao, Z.; Cheng, J.; Wei, W.; Sun, K.; Wang, M. Effects of pressure training and traditional muscle building training on some hormones and bioactive factors of elite male handball players. China Sports Sci. Technol. 2019, 55, 20–29. [Google Scholar]
- Yinghao, L.; Jing, Y.; Yongqi, W.; Jianming, Z.; Zeng, G.; Yiting, T.; Shuoqi, L. Effects of a blood flow restriction exercise under different pressures on testosterone, growth hormone, and insulin-like growth factor levels. J. Int. Med. Res. 2021, 49, 3000605211039564. [Google Scholar] [CrossRef]
- Li, Z.; Wei, W.; Zhao, Z.; Sun, K.; Gao, W.; Xiao, Z. Effects of different degree of blood flow restriction on serum growth hormone and testosterone secretion during low-intensity resistance exercise. China Sports Sci. Technol. 2020, 56, 38–43. [Google Scholar]
- Bemben, D.A.; Sherk, V.D.; Buchanan, S.R.; Kim, S.; Sherk, K.; Bemben, M.G. Acute and Chronic Bone Marker and Endocrine Responses to Resistance Exercise With and Without Blood Flow Restriction in Young Men. Front. Physiol. 2022, 13, 837631. [Google Scholar] [CrossRef]
- Lei, S.; Zhang, M.; Ma, C.; Gao, W.; Xia, X.; Dong, K. Muscle effect, dose-effect relationship and physiological mechanism of pressure resistance training. Chin. J. Tissue Eng. 2023, 27, 4254–4264. [Google Scholar]
- Schwiete, C.; Franz, A.; Roth, C.; Behringer, M. Effects of Resting vs. Continuous Blood-Flow Restriction-Training on Strength, Fatigue Resistance, Muscle Thickness, and Perceived Discomfort. Front. Physiol. 2021, 12, 663665. [Google Scholar] [CrossRef] [PubMed]
- Chernozub, A.; Manolachi, V.; Tsos, A.; Potop, V.; Korobeynikov, G.; Manolachi, V.; Sherstiuk, L.; Zhao, J.; Mihaila, I. Adaptive changes in bodybuilders in conditions of different energy supply modes and intensity of training load regimes using machine and free weight exercises. PeerJ 2023, 11, e14878. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Fahs, C.A.; Rossow, L.M.; Abe, T.; Bemben, M.G. The anabolic benefits of venous blood flow restriction training may be induced by muscle cell swelling. Med. Hypotheses 2012, 78, 151–154. [Google Scholar] [CrossRef]
- Lambert, B.; Hedt, C.; Daum, J.; Taft, C.; Chaliki, K.; Epner, E.; McCulloch, P. Blood Flow Restriction Training for the Shoulder: A Case for Proximal Benefit. Am. J. Sports Med. 2021, 49, 2716–2728. [Google Scholar] [CrossRef]
- Vieira, A.; Gadelha, A.B.; Ferreira-Junior, J.B.; Vieira, C.A.; Soares Ede, M.; Cadore, E.L.; Wagner, D.R.; Bottaro, M. Session rating of perceived exertion following resistance exercise with blood flow restriction. Clin. Physiol. Funct. Imaging 2015, 35, 323–327. [Google Scholar] [CrossRef]
- Suga, T.; Okita, K.; Morita, N.; Yokota, T.; Hirabayashi, K.; Horiuchi, M.; Takada, S.; Omokawa, M.; Kinugawa, S.; Tsutsui, H. Dose effect on intramuscular metabolic stress during low-intensity resistance exercise with blood flow restriction. J. Appl. Physiol. (1985) 2010, 108, 1563–1567. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age | Height (cm) | Body Mass (kg) | Shoulder Width (cm) | Bench Press 1 RM (kg) |
|---|---|---|---|---|
| 23.67± 1.73 | 174.22± 4.06 | 79.17 ± 8.28 | 44.50 ± 4.28 | 106.33 ± 10.48 |
| Pressurized Mode | Pectoralis Major Muscle (Across the Top of the Chest) | Deltoid Muscle (Over the Shoulder) | Triceps Brachii (Back of the Upper Arm) | |||
|---|---|---|---|---|---|---|
| F | P | F | P | F | P | |
| pectoralis major muscle (across the top of the chest) | 0.077 | 0.926 | 0.177 | 0.839 | 0.768 | 0.475 |
| deltoid muscle (over the shoulder) | 0.631 | 0.541 | 0.049 | 0.952 | 0.391 | 0.68 |
| triceps brachii (back of the upper arm) | 0.036 | 0.964 | 0.021 | 0.979 | 0.149 | 0.862 |
| Pectoralis Major Muscle (Across the Top of the Chest) | Deltoid Muscle (Over the Shoulder) | Triceps Brachii (Back of the Upper Arm) | ||||
|---|---|---|---|---|---|---|
| F | P | F | P | F | P | |
| Pressurized mode | 15.931 | 0.000 * | 57.209 | 0.000 * | 41.198 | 0.000 * |
| sports condition | 0.881 | 0.421 | 3.648 | 0.046 * | 3.251 | 0.047 * |
| interaction | 1.971 | 0.134 | 1.511 | 0.214 | 0.722 | 0.551 |
| Muscle Name | Pressurized Mode | 3 Sets of Bench Press Training (8 + 8 + 8) | ||
|---|---|---|---|---|
| Set I | Set II | Set III | ||
| pectoralis major muscle (across the top of the chest) | Sustained low pressure (T1) | 43.73 ± 19.97 *Δ | 46.30 ± 20.01 * | 47.33 ± 21.05 * |
| Intermittent high pressure (T2) | 61.21 ± 23.27 * | 53.46 ± 15.56 * | 44.79 ± 18.61 | |
| Unpressurized (C) | 34.33 ± 16.64 | 34.15 ± 19.98 | 36.28 ± 19.19 | |
| deltoid muscle (over the shoulder) | Sustained low pressure (T1) | 64.02 ± 15.09 * | 58.39 ± 13.66 *# | 58.56 ± 12.27 * |
| Intermittent high pressure (T2) | 73.85 ± 16.31 *§ | 75.40 ± 15.89 *§ | 65.85 ± 14.99 * | |
| Unpressurized (C) | 48.83 ± 12.56 | 48.63 ± 12.88 | 48.85 ± 15.08 | |
| triceps brachii (back of the upper arm) | Sustained low pressure (T1) | 46.42 ± 22.25 * | 56.85 ± 16.45 *§ | 32.27 ± 19.75 * |
| Intermittent high pressure (T2) | 54.64 ± 13.79 *§ | 57.62 ± 13.46 *§ | 33.41 ± 16.79 * | |
| Unpressurized (C) | 40.32 ± 17.43 | 47.46 ± 12.98 | 36.49 ± 18.37 | |
| Subjective Fatigue | Pressurized Mode | Training Group | ||
|---|---|---|---|---|
| Set I | Set II | Set III | ||
| RPE value | Sustained low pressure (T1) | 6.22 ± 0.67 *§ | 7.11 ± 1.17 *§# | 8.67 ± 1.22 * |
| Intermittent high pressure (T2) | 5.89 ± 1.05 § | 6.80 ± 1.12 §# | 8.00 ± 1.41 Δ | |
| Unpressurized (C) | 5.00 ± 1.00 § | 5.89 ± 0.60 §# | 7.11 ± 1.17 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, K.; Sun, Y.; Xiao, S.; Zhang, X.; Du, Z.; Zhang, Y. Effects of High-Load Bench Press Training with Different Blood Flow Restriction Pressurization Strategies on the Degree of Muscle Activation in the Upper Limbs of Bodybuilders. Sensors 2024, 24, 605. https://doi.org/10.3390/s24020605
He K, Sun Y, Xiao S, Zhang X, Du Z, Zhang Y. Effects of High-Load Bench Press Training with Different Blood Flow Restriction Pressurization Strategies on the Degree of Muscle Activation in the Upper Limbs of Bodybuilders. Sensors. 2024; 24(2):605. https://doi.org/10.3390/s24020605
Chicago/Turabian StyleHe, Kexin, Yao Sun, Shuang Xiao, Xiuli Zhang, Zhihao Du, and Yanping Zhang. 2024. "Effects of High-Load Bench Press Training with Different Blood Flow Restriction Pressurization Strategies on the Degree of Muscle Activation in the Upper Limbs of Bodybuilders" Sensors 24, no. 2: 605. https://doi.org/10.3390/s24020605