
The Role and Importance of Using Sensor-Based Devices in Medical Rehabilitation: A Literature Review on the New Therapeutic Approaches

 ,
, 
 and
and
Abstract
:1. Introduction
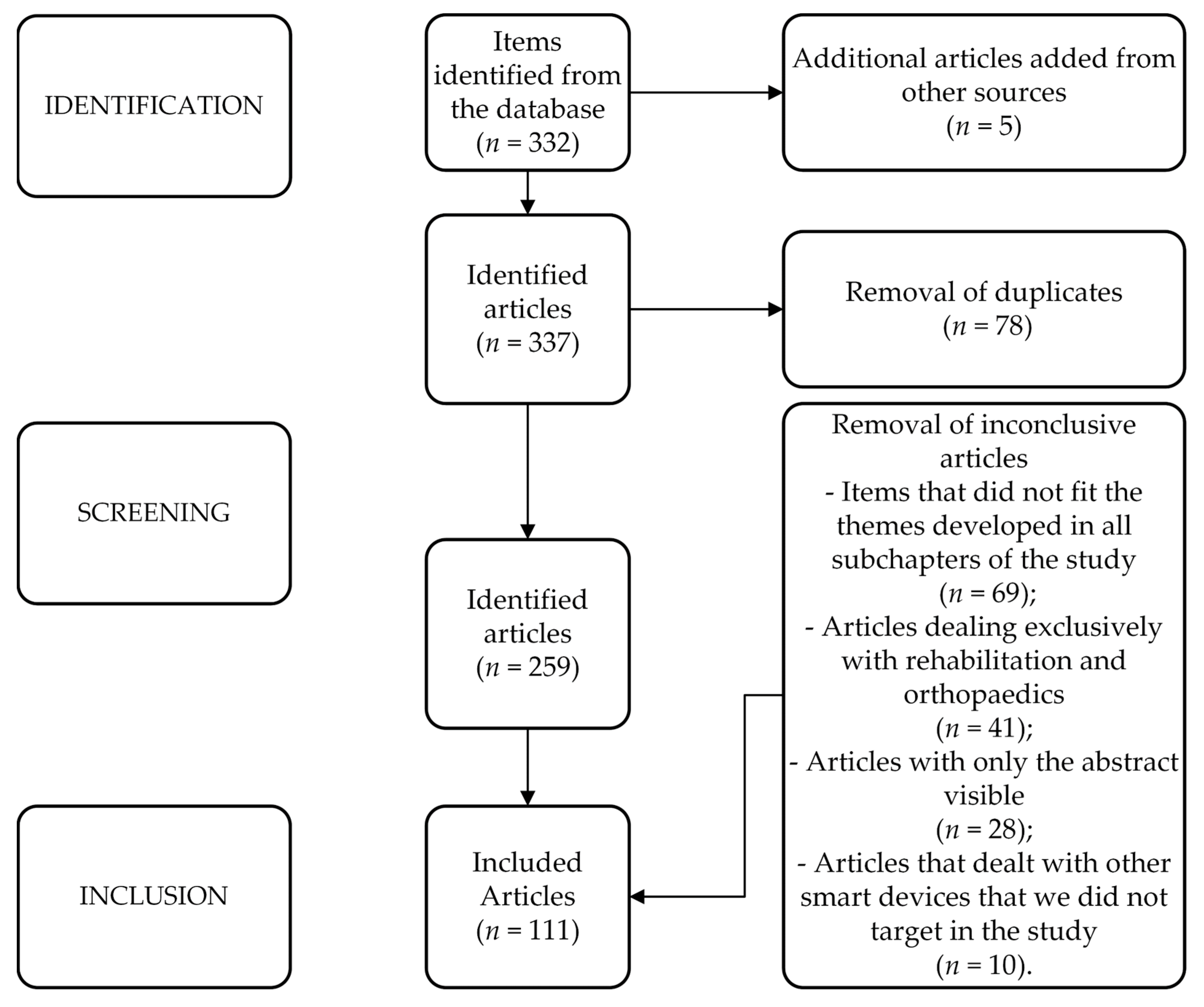
2. Materials and Methods
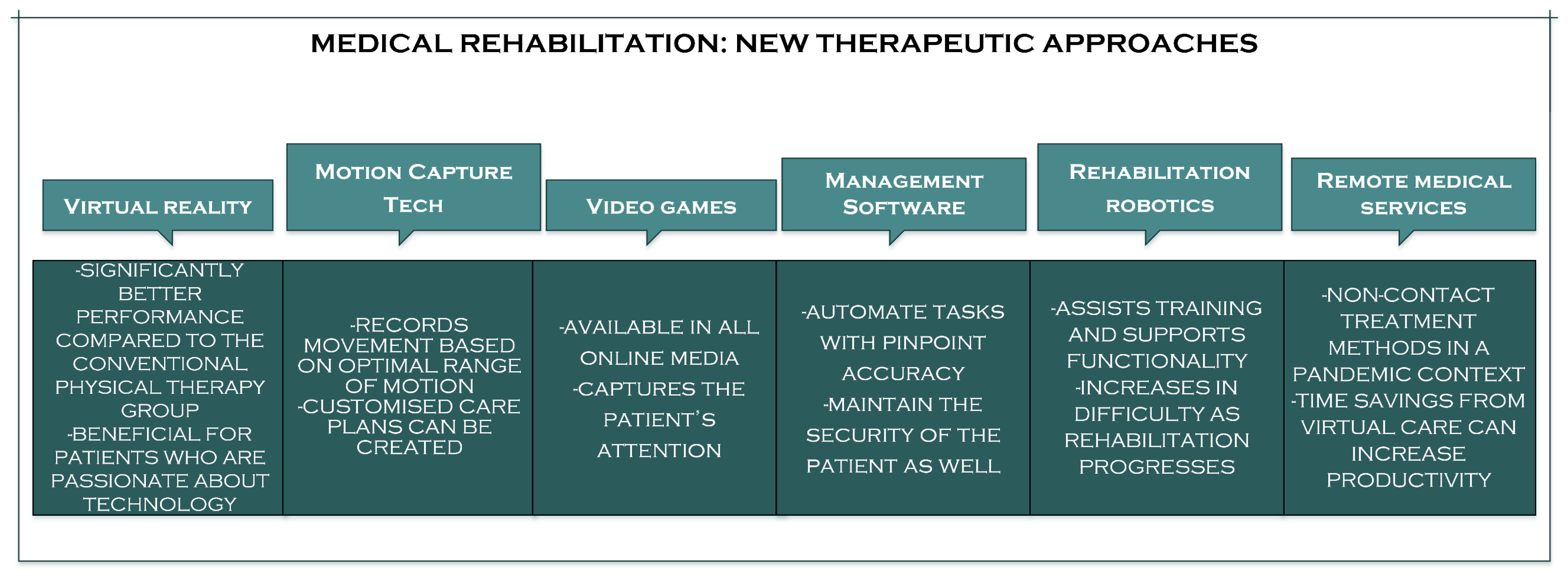
3. Medical Rehabilitation: New Therapeutic Approaches
3.1. Virtual Reality
3.2. Motion Capture Tech
3.3. Video Games
3.4. Physical Therapist Practice Management Software
3.5. Rehabilitation Robotics
3.6. Remote Medical Services

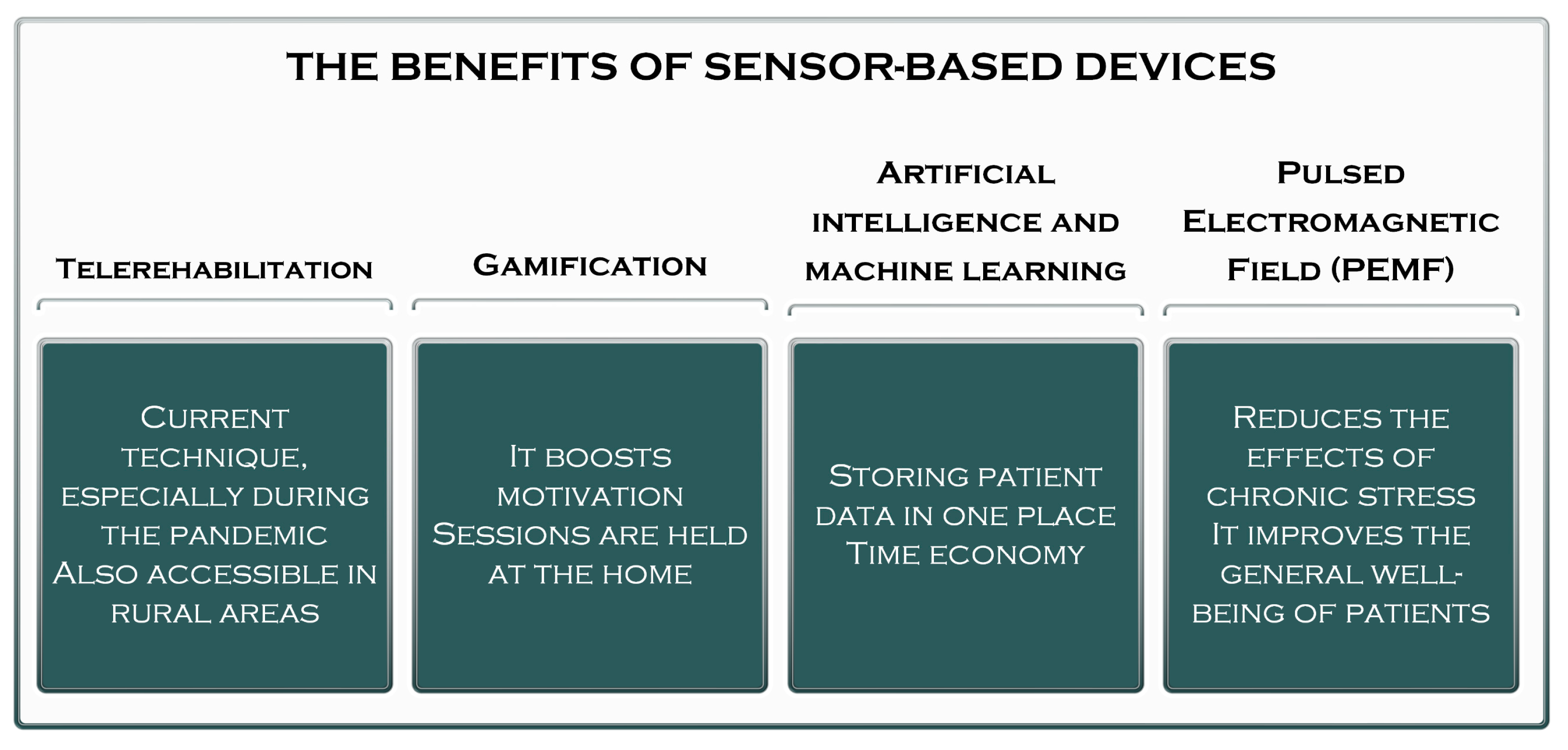
4. The Importance and Benefits of Using Sensor-Based Devices in Medical Rehabilitation
4.1. Telerehabilitation
4.2. Gamification
4.3. Artificial Intelligence and Machine Learning
4.4. Pulsed Electromagnetic Field (P.E.M.F.)

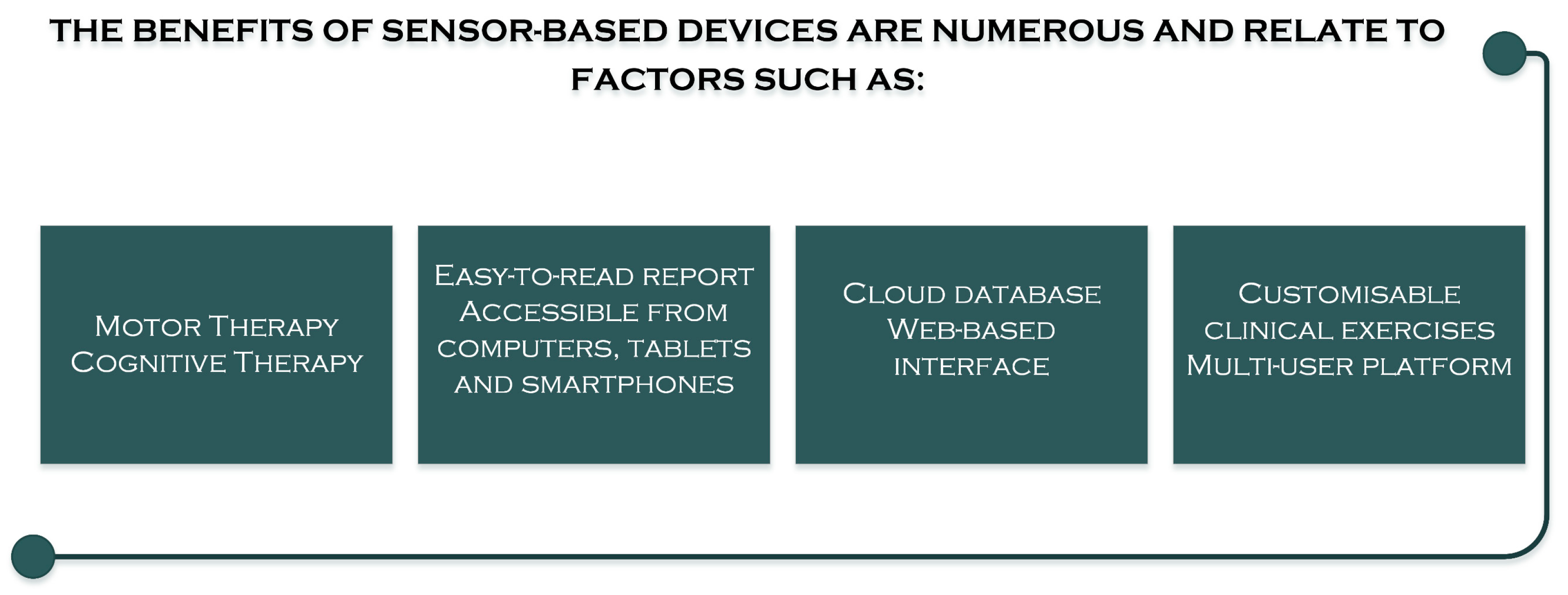
5. The Benefits of Using Sensor-Based Devices on Patients
The Quality of Rehabilitation of Lost Functions Using Sensor-Based Devices

6. The Impact of the Use of Sensor-Based Devices on Physiotherapists
7. Limitations of Using Sensor-Based Devices in Medical Rehabilitation
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zheng, W.; Liu, M.; Liu, C.; Wang, D.; Li, K. Recent Advances in Sensor Technology for Healthcare and Biomedical Applications (Volume II). Sensors 2023, 23, 5949. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Liu, B.; Li, H.; Li, M.; Song, Y.; Wang, R.; Wang, T.; Zhang, H. Flexible Wearable Sensors in Medical Monitoring. Biosensors 2022, 12, 1069. [Google Scholar] [CrossRef]
- Liu, Z.; Cascioli, V.; McCarthy, P.W. Healthcare Monitoring Using Low-Cost Sensors to Supplement and Replace Human Sensation: Does It Have Potential to Increase Independent Living and Prevent Disease? Sensors 2023, 23, 2139. [Google Scholar] [CrossRef] [PubMed]
- Canali, S.; Schiaffonati, V.; Aliverti, A. Challenges and recommendations for wearable devices in digital health: Data quality, interoperability, health equity, fairness. PLoS Digit. Health 2022, 1, e0000104. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Liu, C.; Zou, H.; Che, L.; Sun, P.; Yan, J.; Liu, W.; Xu, Z.; Yang, W.; Dong, L.; et al. Integrated wearable smart sensor system for real-time multi-parameter respiration health monitoring. Cell Rep. Phys. Sci. 2023, 4, 101191. [Google Scholar] [CrossRef]
- Vijayan, V.; Connolly, J.P.; Condell, J.; McKelvey, N.; Gardiner, P. Review of Wearable Devices and Data Collection Considerations for Connected Health. Sensors 2021, 21, 5589. [Google Scholar] [CrossRef]
- Al-Kahtani, M.S.; Khan, F.; Taekeun, W. Application of Internet of Things and Sensors in Healthcare. Sensors 2022, 22, 5738. [Google Scholar] [CrossRef]
- Berolo, S.; Wells, R.P.; Amick, B.C., 3rd. Musculoskeletal symptoms among mobile hand-held device users and their relationship to device use: A preliminary study in a Canadian university population. Appl. Ergon. 2011, 42, 371–378. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Re, T.S.; Zerbetto, R. The relationship between nomophobia and maladaptive coping styles in a sample of Italian young adults: Insights and implications from a cross-sectional study. JMIR Ment. Health 2019, 6, e13154. [Google Scholar] [CrossRef]
- Olczak, A.; Truszczyńska-Baszak, A.; Stępień, A. The Use of Armeo®Spring Device to Assess the Effect of Trunk Stabilization Exercises on the Functional Capabilities of the Upper Limb—An Observational Study of Patients after Stroke. Sensors 2022, 22, 4336. [Google Scholar] [CrossRef]
- Lai, C.H.; Sung, W.H.; Chiang, S.L.; Lu, L.H.; Lin, C.H.; Tung, Y.C.; Lin, C.H. Bimanual coordination deficits in hands following stroke and their relationship with motor and functional performance. J. Neuroeng. Rehabil. 2019, 16, 101. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.-H.; Zheng, D.; Liu, S.-Q.; Zeng, C.-Y.; Xu, Y.-F.; Li, X.-Q. Therapeutic effect of Peto method on the recovery of the motor function in children with cerebral palsy. Chin. J. Clin. Rehabil. 2004, 8, 2902–2903. [Google Scholar]
- Pérez-de la Cruz, S. Use of Robotic Devices for Gait Training in Patients Diagnosed with Multiple Sclerosis: Current State of the Art. Sensors 2022, 22, 2580. [Google Scholar] [CrossRef] [PubMed]
- Zaralieva, A.; Georgiev, G.P.; Karabinov, V.; Iliev, A.; Aleksiev, A. Physical Therapy and Rehabilitation Approaches in Patients with Carpal Tunnel Syndrome. Cureus 2020, 12, e7171. [Google Scholar] [CrossRef]
- Troev, T.; Zaralieva, A.; Lutskanova, S. The Application of Physical Medicine in Medical Practice. In Proceedings of the Second International Scientific and Practical Conference: Nature, Forest, Society. Nature and Habitats, Human Activity and Hunting, Alternative and Hunting Tourism. Problems and Interconnection, Belarus; 2014. [Google Scholar]
- Sconza, C.; Negrini, F.; Di Matteo, B.; Borboni, A.; Boccia, G.; Petrikonis, I.; Stankevičius, E.; Casale, R. Robot-Assisted Gait Training in Patients with Multiple Sclerosis: A Randomized Controlled Crossover Trial. Medicina 2021, 57, 713. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.; Dattola, V.; Logiudice, A.L.; Ciurleo, R.; Sessa, E.; De Luca, R.; Bramanti, P.; Bramanti, A.; Naro, A.; Calabrò, R.S. The role of Sativex in robotic rehabilitation in individuals with multiple sclerosis: Rationale, study design, and methodology. Medicine 2017, 96, 8826. [Google Scholar] [CrossRef]
- Pompa, A.; Morone, G.; Iosa, M.; Pace, L.; Catani, S.; Casillo, P.; Clemenzi, A.; Troisi, E.; Tonini, A.; Paolucci, S.; et al. Does robot-assisted gait training improve ambulation in highly disabled multiple sclerosis people? A pilot randomised control trial. Mult. Scler. 2017, 23, 696–703. [Google Scholar] [CrossRef]
- Drużbicki, M.; Guzik, A.; Przysada, G.; Phd, L.P.; Brzozowska-Magoń, A.; Cygoń, K.; Boczula, G.; Bartosik-Psujek, H. Effects of Robotic Exoskeleton-Aided Gait Training in the Strength, Body Balance, and Walking Speed in Individuals with Multiple Sclerosis: A Single-Group Preliminary Study. Arch. Phys. Med. Rehabil. 2021, 102, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Freivogel, S.; Mehrholz, J.; Schmalohr, D. Improved walking ability and reduced therapeutic stress with an electromechanical gait device. Rehab. Med. 2009, 41, 734–739. [Google Scholar] [CrossRef]
- Shin, J.C.; Jeon, H.R.; Kim, D.; Cho, S.I.; Min, W.K.; Lee, J.S.; Oh, D.S.; Yoo, J. Effects on the Motor Function, Proprioception, Balance, and Gait Ability of the End-Effector Robot-Assisted Gait Training for Spinal Cord Injury Patients. Brain Sci. 2021, 11, 1281. [Google Scholar] [CrossRef] [PubMed]
- Kouijzer, M.M.T.E.; Kip, H.; Bouman, Y.H.A.; Kelders, S.M. Implementation of virtual reality in healthcare: A scoping review on the implementation process of virtual reality in various healthcare settings. Implement. Sci. Commun. 2023, 4, 67. [Google Scholar] [CrossRef] [PubMed]
- Son, H.; Ross, A.; Mendoza-Tirado, E.; Lee, L.J. Virtual Reality in Clinical Practice and Research: Viewpoint on Novel Applications for Nursing. JMIR Nurs. 2022, 5, e34036. [Google Scholar] [CrossRef] [PubMed]
- Salisu, S.; Ruhaiyem, N.I.R.; Eisa, T.A.E.; Nasser, M.; Saeed, F.; Younis, H.A. Motion Capture Technologies for Ergonomics: A Systematic Literature Review. Diagnostics 2023, 13, 2593. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, L.V.; Nichols-Larsen, D.S.; Uswatte, G.; Strahl, N.; Simeo, M.; Proffitt, R.; Kelly, K.; Crawfis, R.; Taub, E.; Morris, D.; et al. Video game rehabilitation for outpatient stroke (VIGoROUS): A multi-site randomised controlled trial of in-home, self-managed, upper-extremity therapy. EClinicalMedicine 2021, 43, 101239. [Google Scholar] [CrossRef]
- Merolli, M.; Gray, K.; Choo, D.; Lawford, B.J.; Hinman, R.S. Use, and acceptability, of digital health technologies in musculoskeletal physical therapy: A survey of physical therapists and patients. Musculoskelet. Care 2022, 20, 641–659. [Google Scholar] [CrossRef]
- Giansanti, D. The Rehabilitation and the Robotics: Are They Going Together Well? Healthcare 2020, 9, 26. [Google Scholar] [CrossRef]
- Garske, C.A.; Dyson, M.; Dupan, S.; Nazarpour, K. Perception of game-based rehabilitation in upper limb prosthetic training: Survey of users and researchers. JMIR Serious Games 2021, 9, e23710. [Google Scholar] [CrossRef]
- Smolić, Š.; Blaževski, N.; Fabijančić, M. Remote Healthcare During the COVID-19 Pandemic: Findings for Older Adults in 27 European Countries and Israel. Front. Public Health 2022, 10, 921379. [Google Scholar] [CrossRef]
- Smith, A.C.; Thomas, E.; Snoswell, C.L.; Haydon, H.; Mehrotra, A.; Clemensen, J.; Caffery, L.J. Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19). J. Telemed. Telecare 2020, 26, 309–313. [Google Scholar] [CrossRef]
- Giansanti, D. The Social Robot in Rehabilitation and Assistance: What Is the Future? Healthcare 2021, 9, 244. [Google Scholar] [CrossRef]
- Sheridan, T.B. A review of recent research in social robotics. Curr. Opin. Psychol. 2020, 36, 7–12. [Google Scholar] [CrossRef]
- Atashzar, S.F.; Carriere, J.; Tavakoli, M. Review: How Can Intelligent Robots and Smart Mechatronic Modules Facilitate Remote Assessment, Assistance, and Rehabilitation for Isolated Adults With Neuro-Musculoskeletal Conditions? Front. Robot. AI 2021, 8, 610529. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.C. COVID-19 and the Advancement of Digital Physical Therapist Practice and Telehealth. Phys. Ther. 2020, 100, 1054–1057. [Google Scholar] [CrossRef] [PubMed]
- Pu, L.; Moyle, W.; Jones, C.; Todorovic, M. The effect of a social robot intervention on sleep and motor activity of people living with dementia and chronic pain: A pilot randomised controlled trial. Maturitas 2021, 144, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Lewis, T.T.; Kim, H.; Darcy-Mahoney, A.; Waldron, M.; Lee, W.H.; Park, C.H. Robotic Uses in Pediatric Care: A Comprehensive Review. J. Pediatr. Nurs. 2021, 58, 65–75. [Google Scholar] [CrossRef]
- Soares, E.E.; Bausback, K.; Beard, C.L.; Higinbotham, M.; Bunge, E.L.; Gengoux, G.W. Social Skills Training for Autism Spectrum Disorder: A Meta-analysis of In-person and Technological Interventions. J. Technol. Behav. Sci. 2021, 6, 166–180. [Google Scholar] [CrossRef]
- Sandgreen, H.; Frederiksen, L.H.; Bilenberg, N. Digital Interventions for Autism Spectrum Disorder: A Meta-analysis. J. Autism Dev. Disord. 2021, 51, 3138–3152. [Google Scholar] [CrossRef]
- Pires, I.M.; Lopes, E.; Villasana, M.V.; Garcia, N.M.; Zdravevski, E.; Ponciano, V. A Brief Review on the Sensor Measurement Solutions for the Ten-Meter Walk Test. Computers 2021, 10, 49. [Google Scholar] [CrossRef]
- Felizardo, V.; Sousa, P.; Sabugueiro, D.; Alexandre, C.; Couto, R.; Garcia, N.; Pires, I. E-Health: Current status and future trends. In Handbook of Research on Democratic Strategies and Citizen-Centered E-Government Services; I.G.I. Global: Hershey, PA, USA, 2015; pp. 302–326. [Google Scholar]
- Oniani, S.; Pires, I.M.; Garcia, N.M.; Mosashvili, I.; Pombo, N. A Review of Frameworks on Continuous Data Acquisition for E-Health and m-Health. In Proceedings of the 5th E.A.I. International Conference on Smart Objects and Technologies for Social Good, Valencia, Spain, 25–27 September 2019; pp. 231–234. [Google Scholar]
- Ureña, R.; Chiclana, F.; Gonzalez-Alvarez, A.; Herrera-Viedma, E.; Moral-Munoz, J.A. M-SFT: A Novel Mobile Health System to Assess the Elderly Physical Condition. Sensors 2020, 20, 1462. [Google Scholar] [CrossRef]
- Pires, I.M.; Marques, G.; Garcia, N.M.; Pombo, N.; Flórez-Revuelta, F.; Zdravevski, E.; Spinsante, S. A Review on the Artificial Intelligence Algorithms for the Recognition of Activities of Daily Living Using Sensors in Mobile Devices. In Handbook of Wireless Sensor Networks: Issues and Challenges in Current Scenario’s; Singh, P.K., Bhargava, B.K., Paprzycki, M., Kaushal, N.C., Hong, W.-C., Eds.; Advances in Intelligent Systems and Computing; Springer International Publishing: Cham, Germany, 2020; Volume 1132, pp. 685–713. ISBN 978-3-030-40304-1. [Google Scholar]
- Tavares, B.F.; Pires, I.M.; Marques, G.; Garcia, N.M.; Zdravevski, E.; Lameski, P.; Trajkovik, V.; Jevremovic, A. Mobile Applications for Training Plan Using Android Devices: A Systematic Review and a Taxonomy Proposal. Information 2020, 11, 343. [Google Scholar] [CrossRef]
- Ponciano, V.; Pires, I.M.; Fernandes, A.; Leithardt, V. The Importance of Software Development for the Monitoring of Training to High Competition. Braz. J. Dev. 2020, 6, 26005–26019. [Google Scholar] [CrossRef]
- Silva, J.; Sousa, I. Instrumented Timed up and Go: Fall Risk Assessment Based on Inertial Wearable Sensors. In Proceedings of the 2016 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Benevento, Italy, 15–18 May 2016; pp. 1–6. [Google Scholar]
- Cuesta-Vargas, A.I.; Pajares, B.; Trinidad-Fernandez, M.; Alba, E.; Roldan-Jiménez, C. Inertial Sensors Embedded in Smartphones as a Tool for Fatigue Assessment Based on Acceleration in Survivors of Breast Cancer. Phys. Ther. 2020, 100, 447–456. [Google Scholar] [CrossRef]
- Appelboom, G.; Camacho, E.; Abraham, M.E.; Bruce, S.S.; Dumont, E.L.; Zacharia, B.E.; D’Amico, R.; Slomian, J.; Reginster, J.Y.; Bruyère, O.; et al. Smart Wearable Body Sensors for Patient Self-Assessment and Monitoring. Arch. Public Health 2014, 72, 28. [Google Scholar] [CrossRef]
- Dimitrievski, A.; Zdravevski, E.; Lameski, P.; Trajkovik, V. Towards Application of Non-Invasive Environmental Sensors for Risks and Activity Detection. In Proceedings of the 2016 IEEE 12th International Conference on Intelligent Computer Communication and Processing (I.C.C.P.), Cluj-Napoca, Romania, 8–10 September 2016; pp. 27–33. [Google Scholar]
- Ponciano, V.; Pires, I.M.; Ribeiro, F.R.; Marques, G.; Villasana, M.V.; Garcia, N.M.; Zdravevski, E.; Spinsante, S. Identification of Diseases Based on the Use of Inertial Sensors: A Systematic Review. Electronics 2020, 9, 778. [Google Scholar] [CrossRef]
- Ponciano, V.; Pires, I.M.; Ribeiro, F.R.; Garcia, N.M.; Pombo, N.; Spinsante, S.; Crisóstomo, R. Smartphone-Based Automatic Measurement of the Results of the Timed-Up and Go Test. In Proceedings of the 5th E.A.I. International Conference on Smart Objects and Technologies for Social Good, Valencia, Spain, 25–27 September 2019; pp. 239–242. [Google Scholar]
- Ponciano, V.; Pires, I.M.; Ribeiro, F.R.; Marques, G.; Garcia, N.M.; Pombo, N.; Spinsante, S.; Zdravevski, E. Is The Timed-Up and Go Test Feasible in Mobile Devices? A Systematic Review. Electronics 2020, 9, 528. [Google Scholar] [CrossRef]
- Pires, I.M.; Ponciano, V.; Garcia, N.M.; Zdravevski, E. Analysis of the Results of Heel-Rise Test with Sensors: A Systematic Review. Electronics 2020, 9, 1154. [Google Scholar] [CrossRef]
- Pires, I.M.; Marques, D.; Pombo, N.; Garcia, N.M.; Marques, M.C.; Flórez-Revuelta, F. Measurement of the Reaction Time in the 30-S Chair Stand Test Using the Accelerometer Sensor Available in off-the-Shelf Mobile Devices. In Proceedings of the ICT4AWE 2018, Madeira, Portugal, 22–23 March 2018. [Google Scholar]
- Pires, I.M.; Garcia, N.M.; Zdravevski, E. Measurement of Results of Functional Reach Test with Sensors: A Systematic Review. Electronics 2020, 9, 1078. [Google Scholar] [CrossRef]
- Garcia, N.M. A roadmap to the design of a personal digital life coach. In Advances in Intelligent Systems and Computing; A.I.S.C.: Chicago, IL, USA, 2015. [Google Scholar]
- Goleva, R.I.; Ganchev, I.; Dobre, C.; Garcia, N.; Valderrama, C. Enhanced Living Environments: From Models to Technologies; I.E.T.: London, UK, 2017. [Google Scholar]
- Pires, I.M.; Garcia, N.M.; Pombo, N.; Flórez-Revuelta, F. Identification of activities of daily living using sensors available in off-the-shelf mobile devices: Research and hypothesis. In Advances in Intelligent Systems and Computing; A.I.S.C.: Chicago, IL, USA, 2016. [Google Scholar]
- Pires, I.M.; Teixeira, M.C.; Pombo, N.; Garcia, N.M.; Flórez-Revuelta, F.; Spinsante, S.; Goleva, R.; Zdravevski, E. Android Library for Recognition of Activities of Daily Living: Implementation Considerations, Challenges, and Solutions. Open Bioinform. J. 2018, 11, 61–88. [Google Scholar] [CrossRef]
- Merchán-Baeza, J.A.; González-Sánchez, M.; Cuesta-Vargas, A.I. Comparison of kinematic variables obtained by inertial sensors among stroke survivors and healthy older adults in the Functional Reach Test: Cross-sectional study. Biomed. Eng. Online 2015, 14, 49 . [Google Scholar] [CrossRef] [PubMed]
- Allen, B.; Derveloy, R.; Lowry, K.; Handley, H.; Fell, N.; Gasior, W.; Yu, G.; Sartipi, M. Evaluation of fall risk for post-stroke patients using bluetooth low-energy wireless sensor. In Proceedings of the 2013 IEEE Global Communications Conference (GLOBECOM), Atlanta, GA, USA, 9–13 December 2013; pp. 2598–2603. [Google Scholar]
- Itoh, T.; Kumagai, Y.; Morioka, I.; Mae, S.; Naka, T.; Uenishi, H.; Matsuoka, T. Development of a new instrument for evaluating leg motions using acceleration sensors (II). Environ. Health Prev. Med. 2012, 17, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.; He, L. GACEM: Genetic Algorithm Based Classifier Ensemble in a Multi-sensor System. Sensors 2008, 8, 6203–6224. [Google Scholar] [CrossRef] [PubMed]
- Bersch, S.D.; Azzi, D.; Khusainov, R.; Achumba, I.E.; Ries, J. Sensor data acquisition and processing parameters for human activity classification. Sensors 2014, 14, 4239–4270. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Xiong, D.; Guo, L.; Wang, J.A. Remote Quantitative Fugl-Meyer Assessment Framework for Stroke Patients Based on Wearable Sensor Networks. Comput. Methods Programs Biomed. 2016, 128, 100–110. [Google Scholar] [CrossRef]
- Hayward, K.S.; Eng, J.J.; Boyd, L.A.; Lakhani, B.; Bernhardt, J.; Lang, C.E. Exploring the Role of Accelerometers in the Measurement of Real World Upper-Limb Use After Stroke. Brain Impair. 2016, 17, 16–33. [Google Scholar] [CrossRef]
- Facciorusso, S.; Spina, S.; Reebye, R.; Turolla, A.; Calabrò, R.S.; Fiore, P.; Santamato, A. Sensor-Based Rehabilitation in Neurological Diseases: A Bibliometric Analysis of Research Trends. Brain Sci. 2023, 13, 724. [Google Scholar] [CrossRef]
- De Luca, C.J.; Chang, S.S.; Roy, S.H.; Kline, J.C.; Nawab, S.H. Decomposition of surface E.M.G. signals from cyclic dynamic contractions. J. Neurophysiol. 2015, 113, 1941–1951. [Google Scholar] [CrossRef]
- Kline, J.; Contessa, P.; Roy, S.; De Luca, G. Coordination of motor unit firings during cyclic activities of the upper-limb. In Proceedings of the ISB 2017 Congress XXVI, Brisbane, Australia, 23–27 July 2017. [Google Scholar]
- De Luca, C.J.; Kline, J.C.; Contessa, P. Transposed firing activation of motor units. J. Neurophysiol. 2014, 112, 962–970. [Google Scholar] [CrossRef]
- Porciuncula, F.; Roto, A.V.; Kumar, D.; Davis, I.; Roy, S.; Walsh, C.J.; Awad, L.N. Wearable Movement Sensors for Rehabilitation: A Focused Review of Technological and Clinical Advances. Pm&r 2018, 10, S220–S232, Erratum in Pm&r 2018, 10, 1437. [Google Scholar] [CrossRef]
- Roossien, C.C.; Baten, C.T.M.; van der Waard, M.W.P.; Reneman, M.F.; Verkerke, G.J. Automatically Determining Lumbar Load during Physically Demanding Work: A Validation Study. Sensors 2021, 21, 2476. [Google Scholar] [CrossRef] [PubMed]
- Regterschot, G.R.H.; Ribbers, G.M.; Bussmann, J.B.J. Wearable Movement Sensors for Rehabilitation: From Technology to Clinical Practice. Sensors 2021, 21, 4744. [Google Scholar] [CrossRef]
- Prasanth, H.; Caban, M.; Keller, U.; Courtine, G.; Ijspeert, A.; Vallery, H.; von Zitzewitz, J. Wearable Sensor-Based Real-Time Gait Detection: A Systematic Review. Sensors 2021, 21, 2727. [Google Scholar] [CrossRef] [PubMed]
- Mitternacht, J.; Hermann, A.; Carqueville, P. Acquisition of Lower-Limb Motion Characteristics with a Single Inertial Measurement Unit—Validation for Use in Physiotherapy. Diagnostics 2022, 12, 1640–1658. [Google Scholar] [CrossRef] [PubMed]
- Höher, J.; Lischke, B.; Petersen, W.; Mengis, N.; Niederer, D.; Stein, T.; Stoffels, T.; Prill, R.; Schmidt-Lucke, C. Sensor-based telerehabilitation system increases patient adherence after knee surgery. PLoS Digit. Health. 2023, 2, e0000175. [Google Scholar] [CrossRef]
- Tormene, P.; Bartolo, M.; De Nunzio, A.M.; Fecchio, F.; Quaglini, S.; Tassorelli, C.; Sandrini, G. Estimation of human trunk movements by wearable strain sensors and improvement of sensor’s placement on intelligent biomedical clothes. Biomed. Eng. Online 2012, 11, 95. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.; Horst, F.; Müller, S.; Steinberg, F.; Doppelmayr, M. Current State and Future Prospects of EEG and fNIRS in Robot-Assisted Gait Rehabilitation: A Brief Review. Front. Hum. Neurosci. 2019, 13, 172. [Google Scholar] [CrossRef]
- Shakti, D.; Mathew, L.; Kumar, N.; Kataria, C. Effectiveness of robo-assisted lower limb rehabilitation for spastic patients: A systematic review. Biosens. Bioelectron. 2018, 117, 403–415. [Google Scholar] [CrossRef]
- Todd, C.J.; Hubner, P.P.; Hubner, P.; Schubert, M.C.; Migliaccio, A.A. StableEyes—A Portable Vestibular Rehabilitation Device. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1223–1232. [Google Scholar] [CrossRef]
- Tannous, H.; Istrate, D.; Perrochon, A.; Daviet, J.-C.; Benlarbi-Delai, A.; Sarrazin, J.; Ho Ba Tho, M.-C.; Dao, T.T. GAMEREHAB@HOME: A new engineering system using serious game and multi-sensor fusion for functional rehabilitation at home. IEEE Trans. Games 2020, 13, 89–98. [Google Scholar] [CrossRef]
- Graybill, P.; Kiani, M. Eyelid Drive System: An Assistive Technology Employing Inductive Sensing of Eyelid Movement. IEEE Trans. Biomed. Circuits Syst. 2018, 13, 203–213. [Google Scholar] [CrossRef]
- Guy, V.; Soriani, M.-H.; Bruno, M.; Papadopoulo, T.; Desnuelle, C.; Clerc, M. Brain computer interface with the P300 speller: Usability for disabled people with amyotrophic lateral sclerosis. Ann. Phys. Rehabil. Med. 2018, 61, 5–11. [Google Scholar] [CrossRef]
- Zhihua, C.; Yun, X.; Xingyuan, H. Analyses of pedestrian’s head-to-windshield impact biomechanical responses and head injuries using a head finite element model. J. Mech. Med. Biol. 2019, 20, 1950063. [Google Scholar] [CrossRef]
- Jakob, I.; Kollreider, A.; Germanotta, M.; Benetti, F.; Cruciani, A.; Padua, L.; Aprile, I. Robotic and Sensor Technology for Upper Limb Rehabilitation. PMR 2018, 10, S189–S197. [Google Scholar] [CrossRef] [PubMed]
- Yap, H.K.; Ang, B.W.K.; Lim, J.H.; Goh, J.C.H.; Yeow, C.-H. A fabric-regulated soft robotic glove with user intent detection using E.M.G. and RFID for hand assistive application. In Proceedings of the 2016 IEEE International Conference on Robotics and Automation (I.C.R.A.), Stockholm, Sweden, 16 May 2016; pp. 3537–3542. [Google Scholar]
- Pan, S.; Lv, H.; Duan, H.; Pang, G.; Yi, K.; Yang, G.A. Sensor Glove for the Interaction with a Nursing-Care Assistive Robot. In Proceedings of the 2019 IEEE International Conference on Industrial Cyber Physical Systems (I.C.P.S.), Taipei, Taiwan, 6 May 2019; pp. 405–410. [Google Scholar]
- Han, J.; Shao, L.; Xu, D.; Shotton, J. Enhanced Computer Vision with Microsoft Kinect Sensor: A Review. IEEE Trans. Cybern. 2013, 43, 1318–1334. [Google Scholar] [CrossRef]
- Ju, J.; Shin, Y.; Kim, E. Vision based interface system for hands free control of an intelligent wheelchair. J. Neuroeng. Rehabil. 2009, 6, 33. [Google Scholar] [CrossRef] [PubMed]
- Kim, E. Wheelchair Navigation System for Disabled and Elderly People. Sensors 2016, 16, 1806. [Google Scholar] [CrossRef] [PubMed]
- Saravanakumar, D.; Reddy, R. A high performance asynchronous E.O.G. speller system. Biomed. Signal Process. Control 2020, 59, 101898. [Google Scholar] [CrossRef]
- Cio, Y.-S.L.-K.; Raison, M.; Leblond Menard, C.; Achiche, S. Proof of Concept of an Assistive Robotic Arm Control Using Artificial Stereovision and Eye-Tracking. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 2344–2352. [Google Scholar] [CrossRef]
- Aymaz, S.; Cavdar, T. Ultrasonic Assistive Headset for visually impaired people. In Proceedings of the 2016 39th International Conference on Telecommunications and Signal Processing (T.S.P.), Vienna, Austria, 27 June 2016; pp. 388–391. [Google Scholar]
- Jani, A.B.; Kotak, N.A.; Roy, A.K. Sensor Based Hand Gesture Recognition System for English Alphabets Used in Sign Language of Deaf-Mute People. In Proceedings of the 2018 IEEE SENSORS, New Delhi, India, 28 October 2018; pp. 1–4. [Google Scholar]
- Argent, R.; Slevin, P.; Bevilacqua, A.; Neligan, M.; Daly, A.; Caulfield, B. Wearable Sensor-Based Exercise Biofeedback for Orthopaedic Rehabilitation: A Mixed Methods User Evaluation of a Prototype System. Sensors 2019, 19, 432. [Google Scholar] [CrossRef]
- Kairy, D.; Lehoux, P.; Vincent, C.; Visintin, M. A systematic review of clinical outcomes, clinical process, healthcare utilisation and costs associated with telerehabilitation. Disabil. Rehabil. 2009, 31, 427–447. [Google Scholar] [CrossRef]
- Giggins, O.M.; Persson, U.; Caulfield, B. Biofeedback in rehabilitation. J. NeuroEng. Rehabil. 2013, 10, 60. [Google Scholar] [CrossRef]
- Chughtai, M.; Kelly, J.J.; Newman, J.M.; Sultan, A.A.; Khlopas, A.; Sodhi, N.; Bhave, A.; Kolczun, M.; Mont, M.A. The Role of Virtual Rehabilitation in Total and Unicompartmental Knee Arthroplasty. J. Knee Surg. 2019, 32, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Correia, F.D.; Nogueira, A.; Magalhães, I.; Guimarães, J.; Moreira, M.; Barradas, I.; Teixeira, L.; Tulha, J.; Seabra, R.; Lains, J.; et al. Home-based Rehabilitation with A Novel Digital Biofeedback System versus Conventional In-person Rehabilitation after Total Knee Replacement: A feasibility study. Sci. Rep. 2018, 8, 11299. [Google Scholar] [CrossRef]
- O’Reilly, M.; Caulfield, B.; Ward, T.; Johnston, W.; Doherty, C. Wearable Inertial Sensor Systems for Lower Limb Exercise Detection and Evaluation: A Systematic Review. Sports Med. 2018, 48, 1221–1246. [Google Scholar] [CrossRef] [PubMed]
- Giggins, O.M.; Sweeney, K.T.; Caulfield, B. Rehabilitation exercise assessment using inertial sensors: A cross-sectional analytical study. J. NeuroEng. Rehabil. 2014, 11, 158. [Google Scholar] [CrossRef]
- O’reilly, M.A.; Whelan, D.F.; Ward, T.E.; Delahunt, E.; Caulfield, B.M. Technology in Strength and Conditioning: Assessing Bodyweight Squat Technique with Wearable Sensors. J. Strength Cond. Res. 2017, 31, 2303–2312. [Google Scholar] [CrossRef] [PubMed]
- Bevilacqua, A.; Huang, B.; Argent, R.; Caulfield, B.; Kechadi, T. Automatic classification of knee rehabilitation exercises using a single inertial sensor: A case study. In Proceedings of the 2018 IEEE 15th International Conference on Wearable and Implantable Body Sensor Networks (B.S.N.), Las Vegas, NV, USA, 4–7 March 2018; pp. 21–24. [Google Scholar]
- Peake, J.M.; Kerr, G.; Sullivan, J.P. A Critical Review of Consumer Wearables, Mobile Applications, and Equipment for Providing Biofeedback, Monitoring Stress, and Sleep in Physically Active Populations. Front. Physiol. 2018, 9, 743. [Google Scholar] [CrossRef]
- Michie, S.; Yardley, L.; West, R.; Patrick, K.; Greaves, F. Developing and Evaluating Digital Interventions to Promote Behavior Change in Health and Health Care: Recommendations Resulting from an International Workshop. J. Med. Internet Res. 2017, 19, e232. [Google Scholar] [CrossRef] [PubMed]
- Argent, R.; Daly, A.; Caulfield, B. Patient Involvement with Home-Based Exercise Programs: Can Connected Health Interventions Influence Adherence? JMIR mHealth uHealth 2018, 6, e47. [Google Scholar] [CrossRef]
- O’Reilly, M.A.; Slevin, P.; Ward, T.; Caulfield, B. A Wearable Sensor-Based Exercise Biofeedback System: Mixed Methods Evaluation of Formulift. JMIR mHealth uHealth. 2018, 6, e33. [Google Scholar] [CrossRef]
- Bollen, J.; Dean, S.G.; Siegert, R.J.; Howe, T.E.; Goodwin, V.A.; Nepogodiev, D.; Chapman, S.J.; Glasbey, J.C.D.; Kelly, M.; Khatri, C.; et al. A systematic review of measures of self-reported adherence to unsupervised home-based rehabilitation exercise programmes, and their psychometric properties. BMJ Open. 2014, 4, 005044. [Google Scholar] [CrossRef]
- Steele, R.; Lo, A.; Secombe, C.; Wong, Y.K. Elderly persons’ perception and acceptance of using wireless sensor networks to assist healthcare. Int. J. Med. Inform. 2009, 78, 788–801. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.; Norman, K.; Saunders, S. The State of the Union: Trends and Drivers of Change in Physiotherapy in Ontario in 2014; Queen’s University: Kingston, ON, Canada, 2014. [Google Scholar]
- Cott, C.A.; Mandoda, S.; Landry, M.D. Models of integrating physical therapists into family health teams in Ontario, Canada: Challenges and opportunities. Physiother. Can. 2011, 63, 265–275. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Terms |
|---|---|
| PubMed | (Sensor-based devices) AND (Rehabilitation) AND (Medical) OR (Smart devices) AND (Rehabilitation) AND (Medical) OR (Video Games) AND (Rehabilitation) AND (Medical) OR (Rehabilitation robotics) OR (Artificial intelligence) AND (Rehabilitation) AND (Medical) OR (Virtual reality) OR (V.R.) AND (Rehabilitation) AND (Medical) OR (Medical rehabilitation) AND (New therapeutic approaches) OR (Physical therapy) AND (Software) OR (Medical rehabilitation) AND (Software) OR (Gamified rehabilitation). |
| Web of Science | (Virtual reality) OR (V.R.) AND (Rehabilitation) AND (Medical) OR (Medical rehabilitation) AND (New therapeutic approaches) OR (Physical therapy) AND (Software) OR (Medical rehabilitation) AND (Software) OR (Gamified rehabilitation) OR (Sensor-based devices) AND (Rehabilitation) AND (Medical) OR (Smart devices) AND (Rehabilitation) AND (Medical) OR (Video Games) AND (Rehabilitation) AND (Medical) OR (Rehabilitation robotics) OR (Artificial intelligence) AND (Rehabilitation) AND (Medical). |
| Scopus | (Video Games) AND (Rehabilitation) AND (Medical) OR (Rehabilitation robotics) OR (Artificial intelligence) AND (Rehabilitation) AND (Medical) OR (Virtual reality) OR (Sensor-based devices) AND (Rehabilitation) AND (Medical) OR (Smart devices) AND (Rehabilitation) AND (Medical) OR (V.R.) AND (Rehabilitation) AND (Medical) OR (Medical rehabilitation) AND (New therapeutic approaches) OR (Physical therapy) AND (Software) OR (Medical rehabilitation) AND (Software) OR (Gamified rehabilitation). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szabo, D.A.; Neagu, N.; Teodorescu, S.; Apostu, M.; Predescu, C.; Pârvu, C.; Veres, C. The Role and Importance of Using Sensor-Based Devices in Medical Rehabilitation: A Literature Review on the New Therapeutic Approaches. Sensors 2023, 23, 8950. https://doi.org/10.3390/s23218950
Szabo DA, Neagu N, Teodorescu S, Apostu M, Predescu C, Pârvu C, Veres C. The Role and Importance of Using Sensor-Based Devices in Medical Rehabilitation: A Literature Review on the New Therapeutic Approaches. Sensors. 2023; 23(21):8950. https://doi.org/10.3390/s23218950
Chicago/Turabian StyleSzabo, Dan Alexandru, Nicolae Neagu, Silvia Teodorescu, Mihaela Apostu, Corina Predescu, Carmen Pârvu, and Cristina Veres. 2023. "The Role and Importance of Using Sensor-Based Devices in Medical Rehabilitation: A Literature Review on the New Therapeutic Approaches" Sensors 23, no. 21: 8950. https://doi.org/10.3390/s23218950