1. Introduction
Movement coordination is an ability that allows smooth and efficient goal-directed movements involving several body parts. Due to its complexity, a coordinated gait requires the interaction between different body parts, various muscles to maintain balance, sensory inputs and proprioception [
1]. The cerebellum is an essential part of the coordination and planning of complex movements. It is well recognized that the cerebellum regulates postural equilibrium and muscle tone by interacting with the brainstem, basal ganglia, and cerebral cortex. The cerebellum also contributes to the cognitive aspects of postural control such as the maintenance of postural verticality and anticipatory postural adjustment [
2]. In particular, gait is an ability that starts to develop during the first year of life but maturity is only reached around 11 years of age [
3]. The maturity and development of coordinated gait movements are affected by movement and developmental disorders such as dystonia, early onset ataxia (EOA) and developmental coordination disorder (DCD). In this study, we focus on the distinction between EOA, DCD and typically developing (CTRL) children, based on gait.
Ataxia presenting before 25 years of age is denominated as early onset ataxia (EOA). EOA involves lack of coordination, impaired voluntary and goal-directed movements and loss of balance control [
4]. Distinguishing clinical features in EOA patients include dysdiadochokinesia, dysmetria, overshoot, impaired gait and posture, intention tremor, oculomotor dysfunction and speech abnormalities [
5]. The scale for the assessment and rating of ataxia (SARA) is one of the clinical tools commonly used to assess ataxia. In patients with movement disorders, the SARA was designed to identify and quantify ataxic characteristics [
6].
Developmental coordination disorder (DCD) is defined as an impairment in the coordination and execution of motor function which affects the child’s academic or social development, while no underlying neurological diagnosis or intellectual deficits, such as cerebral palsy, muscular dystrophy, visual impairment or intellectual disability, are present [
7,
8]. Mostly, the features consistent with DCD are identified by the parents when the children present delays in gross or fine motor milestones [
8]. Some of the most common symptoms in DCD patients are abnormal coordination, having motor coordination below expectations for their age as well as delays in early motor milestones, such as walking and crawling.
Patients with EOA and DCD may thus present with an overlap in clinical characteristics, hampering the clinical distinction between both [
5]. Reliable phenotypic recognition of EOA among other developmental disorders with coordination impairment, such as DCD, in relation to typically developing children is important for selecting the correct diagnostic algorithm, predicting familial recurrence risk, treating the child and/or, in case of typical development of an immature motor system, consolidation of the parents [
5]. However, in the context of ambiguous clinical descriptions and in the absence of clear clinical criterion standards, the clinical distinction between mildly initiating EOA features and DCD may be challenging [
5]. In the latter study, 5 out of 21 EOA and DCD patients were inhomogeneously phenotyped by three paediatric neurologists. The phenotypic interobserver agreements for the EOA, DCD and central hypotonia (sub)groups (Gwet’s agreement coefficient) were: EOA = 0.801 (
p < 0.001; substantial); DCD = 0.327 (
p = 0.037; fair); central hypotonia = 0.415 (
p = 0.005; moderate).
Several earlier studies compared the gait of typically developing children with DCD [
9,
10,
11] or with ataxia patients [
12,
13,
14]. However, to our knowledge, few studies have aimed to achieve the clinically more relevant goal of distinguishing between EOA, DCD and the immature motor behaviour of typically developing children, in a single study [
15,
16]. The reason for this may be that DCD is typically diagnosed by rehabilitation doctors, whereas EOA is typically diagnosed by paediatric neurologists. Since both patient groups are thus examined and treated by different specialists, a direct comparison between the groups may be hampered. In a recent study, DCD and typically developing children were asked to walk barefoot on a motor driven treadmill for 2 min, while their gait was assessed using a 3D motion capture system. The authors found that children with DCD exhibited more complexity in their shank movements and also greater variability in thigh and shank movements compared to age- and gender-matched typically developing participants [
9]. In another study, DCD and typically developing children were asked to walk up and down a flat 10-m-long pathway for 1 min, while the movement of their feet and trunk was recorded using motion analysis. The gait pattern of children with DCD was characterised by higher variability and an increased range of movement compared to their healthy peers [
17]. In a previous study from our own group, we aimed to distinguish between patients with EOA or DCD and typically developing children [
15]. Using inertial measurement units (IMUs), we collected data while the participants walked independently, and derived time and frequency domain-based, as well as statistical, information. Employing this information, we improved the classification performance compared to three expert evaluators. Although we achieved good accuracy, explainability of this classification model was low, i.e., we could not directly relate the distinguishing features to the clinical construct of impaired coordination. Knowing which interpretable features contribute most to classification is informative for doctors assessing these patients, as they may expose new, unstudied parameters distinguishing between the different groups. We have shown before, for upper limb SARA tasks, that informing clinicians of such distinguishing parameters, can help improve phenotypic assessment of EOA and DCD [
5].
In the present study, we therefore aimed to provide meaningful features as derived from the quantitative data of the two SARA gait tests to classify EOA and DCD patients and typically developing CTRL children. Our goal was to obtain features with better explainability on the one hand, while achieving similar or even better accuracy, on the other hand. To do so, we developed our features on the clinical premise that impaired gait coordination is characterised by irregularities in movement and loss of smoothness. We extracted gait features from IMU data collected during both SARA gait tests, accordingly.
2. Materials and Methods
The raw data used in this study consist of a data subset recorded for a larger project on the quantification of coordination impairment employing the SARA [
15,
16,
18,
19]. We followed the research and integrity codes of the University Medical Center Groningen (UMCG) and the principles of the declaration of Helsinki (2013). The SARA test battery is performed as part of clinical routine, therefore the Medical Ethical Committee of the UMCG provided a waiver for ethical approval of the study. It was also recognized that the attachment of IMUs to the participant’s body is non-invasive. Finally, parents and children 18 years or older were asked to sign informed consent and informed assent was given by minors 12 years or older.
2.1. Participants
We recruited participants between 2014 and 2019. EOA and DCD patients were asked to participate during routine visits to the outpatient clinic of the UMCG. All DCD patients received an independent neurological examination at the outpatient clinic to ensure that no underlying neurological or intellectual deficits were present. Both EOA and DCD patients fulfilled the official inclusion criteria [
7,
20]. Healthy participants were siblings of the included patients. They were declared to be healthy by their parents and had no other neurological or orthopaedic diagnosis that could theoretically interfere with coordinated motor performance. Intending to balance age, we tried to match the age of the participants in the three groups. None of the included children received medication with known negative side effects on motor coordination. Participants were excluded when they were unable to execute the SARA lower limb gait tests independently.
2.2. Clinical Assessment
We recorded gait and tandem gait SARA test performances using IMUs. During the gait test, participants were asked to walk independently for six meters, turn and walk back the same distance. The tandem gait test consisted of ten independently executed consecutive tandem steps.
2.3. Data Acquisition
Before the performance of both SARA gait tests, the participants were fitted with six lightweight IMUs (51 mm × 34 mm × 14 mm, 23.6 g, Shimmer3, Shimmer, Dublin, Ireland): one IMU was placed on the sternum, another one on the lower back close to the L3 vertebra, two were placed bilaterally halfway each upper leg over the quadriceps and two on the lateral side of the shanks, just above the malleolus. This set-up was chosen to enable various analyses including joint kinematics analysis during SARA motor test performance. For the goal of this study, only the data from a subset of IMUs were used.
Before attachment, the six Shimmer IMUs were calibrated and programmed to record inertial data into embedded SD cards. We configured each IMU to acquire 3D acceleration (±4 G), 3D angular velocity (±500 dps) and 3D magnetic data (±1.9 Ga), at a sampling frequency of 256 Hz. Additionally, we videotaped the start of recording by pressing a button on the multi-charger (Shimmer sensing, Dublin, Ireland) which resets the internal timer of each device so all devices, as well as full SARA gait test execution, are time-synchronised. This allowed later identification and delineation of each of the gait sequences, i.e., forward walking and turning.
2.4. Signal Preprocessing
We obtained six files per patient (one per Shimmer device), containing 3D inertial data. Subsequently, we created separate MATLAB (version R2020b, Mathworks, Natick, MA, USA) files for each test (gait and tandem gait) and each of the straight walking sections, before and after turning. Then, we synchronised the data from all devices, using a MATLAB script that employed the starting and ending time of each test to create a global timing for all devices. After synchronisation, we sorted the data from the sensors such that the x-axis corresponded to the vertical direction, the y-axis to the mediolateral direction and the z-axis to the anterior–posterior direction.
2.4.1. Gait Data Segmentation
After preprocessing, we plotted the mediolateral angular velocity (gyroscope) signals from the shimmers attached to each (right and left) shank. These signals are most representative of gait [
21]. By visual inspection, we then selected only those signals that had a similar pattern to that reported by Salarian et al. [
21] for gait, for further analysis.
Based on the algorithm described by Salarian et al. [
21], we created a MATLAB script to segment individual steps from each shank gait signal (left and right). First, we used a decimation technique to reduce the noise of the signal by increasing two bits of resolution [
22]. Then, we applied a zero-phase 0.5–5 Hz band-pass fourth-order Butterworth filter. This allowed identification of all positive peaks in the signal, which represent the mid-swing events. Subsequently, we identified the adjacent valleys to each peak, where the valley before the peak represents the moment of terminal contact (toe-off) and the valley after the peak represents the moment of initial contact (heel strike). Similar to Salarian et al. [
21], we searched for these peaks in time intervals of 0.5 s before and after mid-swing to automatically identify the toe-off and heel strike events, respectively. We only used the gait cycle data for which all three events could be identified. We identified the events for each shank (left and right) separately, but used the information from both shanks to extract temporal and spatial features (
Section 2.5).
2.4.2. Tandem Gait Data Segmentation
Similar to gait segmentation we first plotted the angular velocity recorded from the Shimmer IMUs attached to the shanks (left and right). By visual inspection, we identified the signals that were correctly acquired for further analysis.
For signal segmentation, we followed the same technique as we did for gait (
Section 2.4.1). Once each mid-swing event and the corresponding toe-off and heel-strike events were identified, we segmented each gait cycle from toe-off to toe-off instead of from heel-strike to heel-strike as we did in gait. We did this to have more usable tandem gait cycles per patient.
2.5. Feature Extraction
The extraction of gait and tandem gait features employed expert knowledge from clinicians and knowledge about gait characteristics as described in the literature. The latter were derived from IMU-based gait models [
23]. We aimed to derive gait features that reflected the gait characteristics clinicians look for during the evaluation of the SARA protocol, which include gait symmetry and regularity, as well as variability of gait performance. The use of such features instead of more general time or frequency domain-based or statistical features will allow for better explainability of the final model. This approach resulted in 36 extracted features. Details of the feature extraction are provided in
Appendix A.
2.6. Classification
For further processing, we combined the 36 extracted features (24 for gait and 12 for tandem gait) in a table, where each column represented one of the 36 features. One row of this table contained feature values from one complete gait cycle of gait and one tandem gait cycle, randomly chosen, thereby building a ‘combined movement’ per patient, for classification. Each patient was represented by 10 rows in this table.
We decided to use a random forest classifier since it performed well in a previous study with a similar application and allows the most relevant features in the model to be identified, thereby contributing to model explainability [
18]. For the classifier, we made an implementation pipeline using Python version 3.7 and scikit-learn 0.32. Random forest (RF) is an ensemble learning algorithm that combines several randomized decision trees and aggregates their predictions by averaging. It also returns estimates of feature importance, that we also report here. The latter characteristic of the method provides some insight into the most relevant features for classification which is of importance for the clinical interpretability of the classifier. Similar to a previous study from our group [
18], we used 300 trees to reduce the computational cost, and the default Gini index threshold hyperparameter in scikit-learn for our random forest classification, which was repeated 100 times. The average and standard deviation of the classification metrics were used to obtain an estimate of classification performance.
To deal with the imbalanced number of participants in our dataset (EOA = 18, DCD = 13 and CTRL = 29), we used the ADASYN algorithm, which synthetically oversamples the minority classes (EOA and DCD), to obtain a balanced dataset [
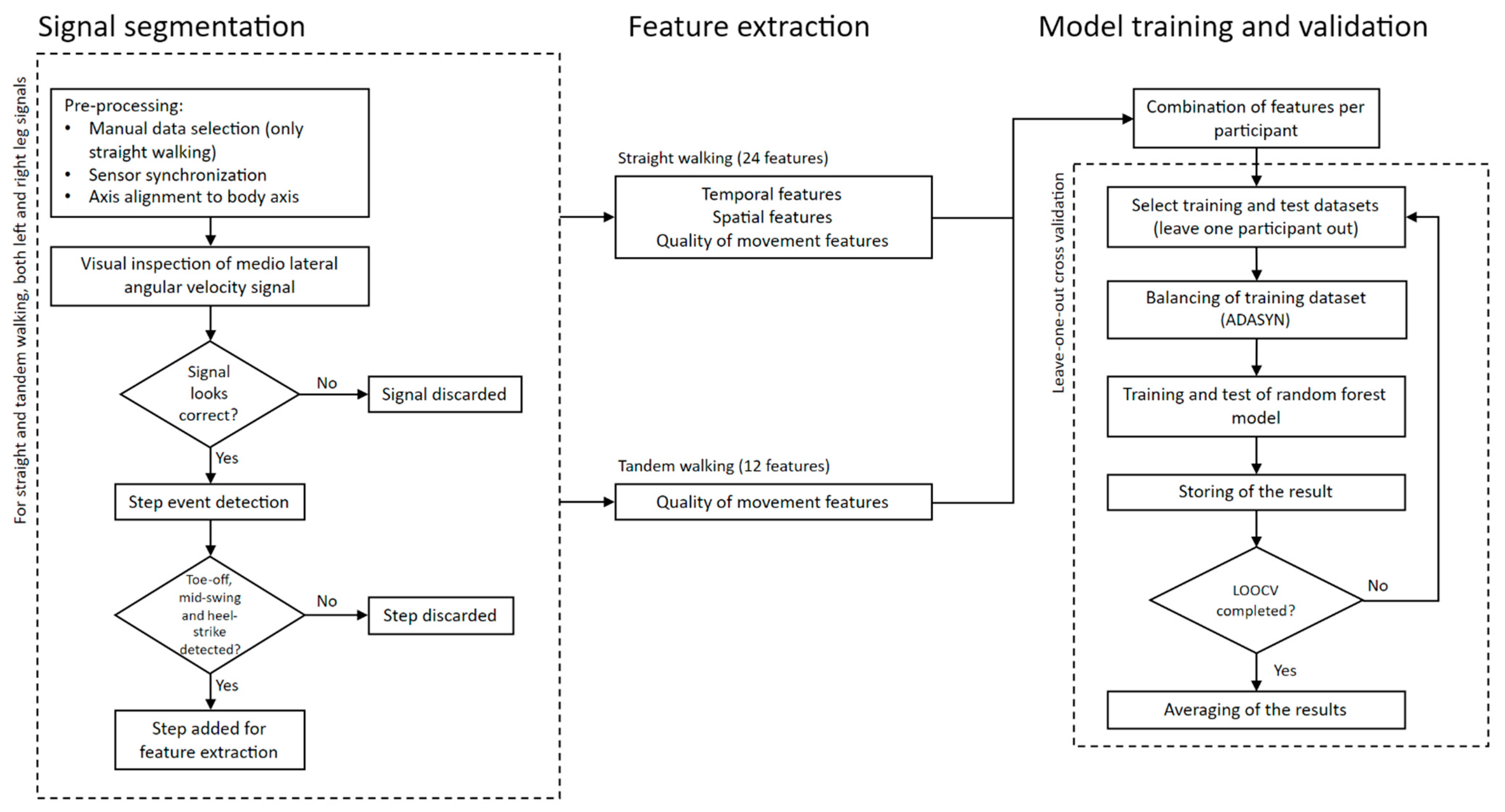
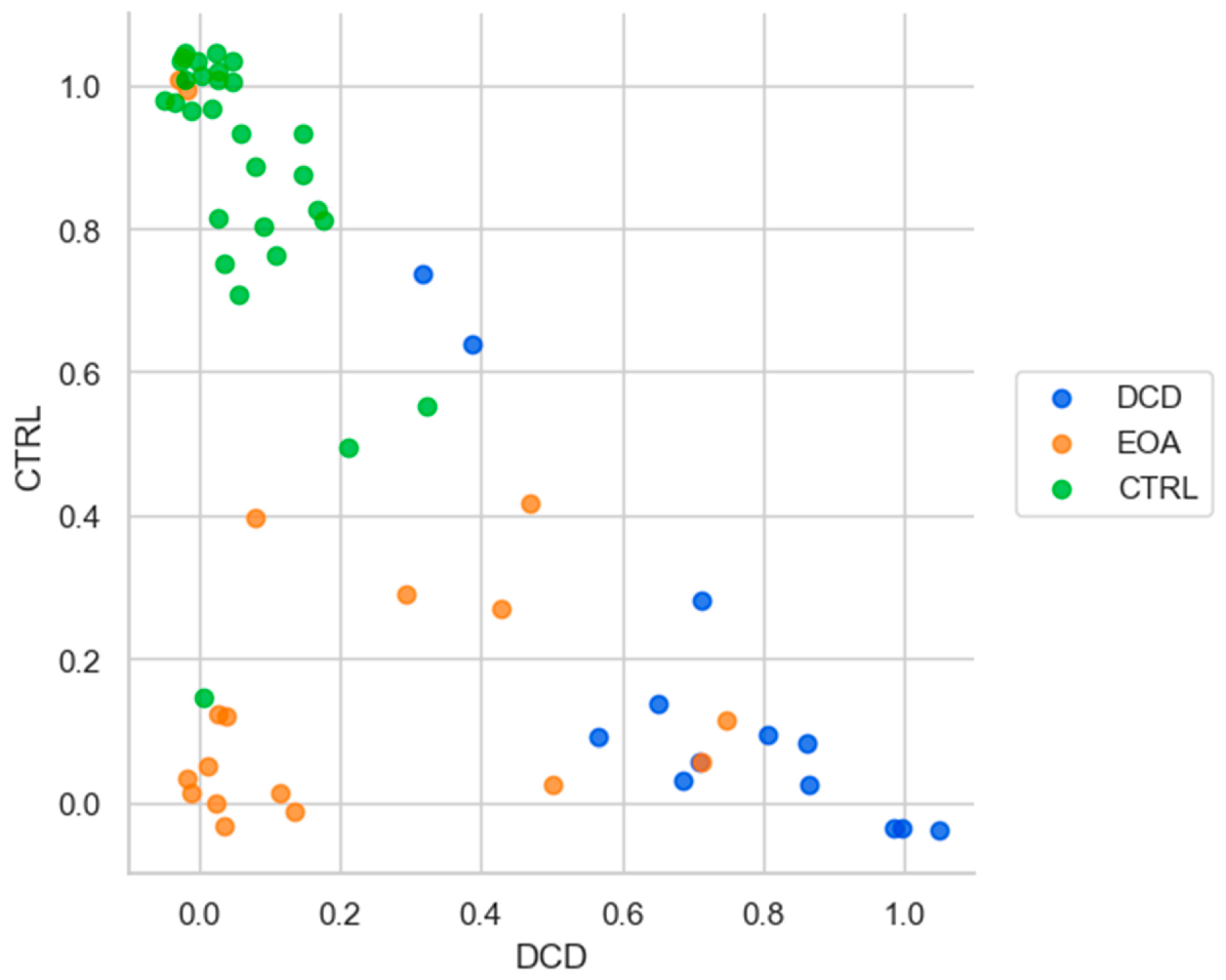
24]. In addition, aiming for a robust estimation (avoiding overfitting) and to overcome the relatively small number of samples we implemented leave-one-out cross validation. However, instead of leaving one instance (one row in the feature matrix) out, we took one participant (10 rows) out to be used as a test set, while keeping the remaining participants as a training set. Note that, for each LOOCV iteration, ADASYN was only applied to this training set. We classified each instance from each participant individually and used a majority vote strategy to obtain the classification per participant, per iteration. In case of a tie, the class was randomly determined from the two tied classes. Using this information over all 100 iterations, we also calculated and plotted the probability for each participant of being classified in one of the three classes. The entire procedure is outlined in the flowchart in
Figure 1.
Even though accuracy is one of the most used metrics to evaluate classification performance, the interpretation of the results could be misleading if there is imbalance in the number of participants per group (class). In such cases, precision and recall could be used as additional metrics to evaluate the performance of the classifier. In our case, as we have an imbalanced dataset (EOA = 18, DCD = 13 and CTRL = 29) we, therefore, decided to use these metrics to evaluate classifier performance in addition to accuracy. Precision (also known as positive predictive value) summarizes the number of positive predictions that actually belong to the positive class. Precision is simply the ratio of correct positive predictions out of all positive predictions made. In an imbalanced classification problem with more than two classes, precision is calculated as the sum of true positives across all classes divided by the sum of true positives and false positives across all classes. Precision thus quantifies the ratio of correct predictions across both positive classes (EOA and DCD).
Recall summarizes how well the positive class was predicted. Recall quantifies the number of positive class predictions in relation to all positive examples in the dataset. Unlike precision that only comments on the correct positive predictions out of all positive predictions, recall indicates missed positive predictions. In an imbalanced classification problem with more than two classes, recall is calculated as the sum of true positives across all classes divided by the sum of true positives and false negatives across all classes.
Precision and recall can be combined into a single score that seeks to balance both concerns, called the F-score or the F-measure. The F
1-measure, which weights precision and recall equally by taking their harmonic mean, is the variant most often used when learning from imbalanced data [
25].
4. Discussion
We used IMU data obtained during the execution of both SARA gait tests to extract meaningful features commonly used for gait analysis (e.g., step length and stride velocity) or for representing gait pattern variability (e.g., deviations from the mean). We employed these features for the classification of children with EOA or DCD and typically developing children. We slightly improved classification performance (0.82) when compared to clinical assessment (0.73) [
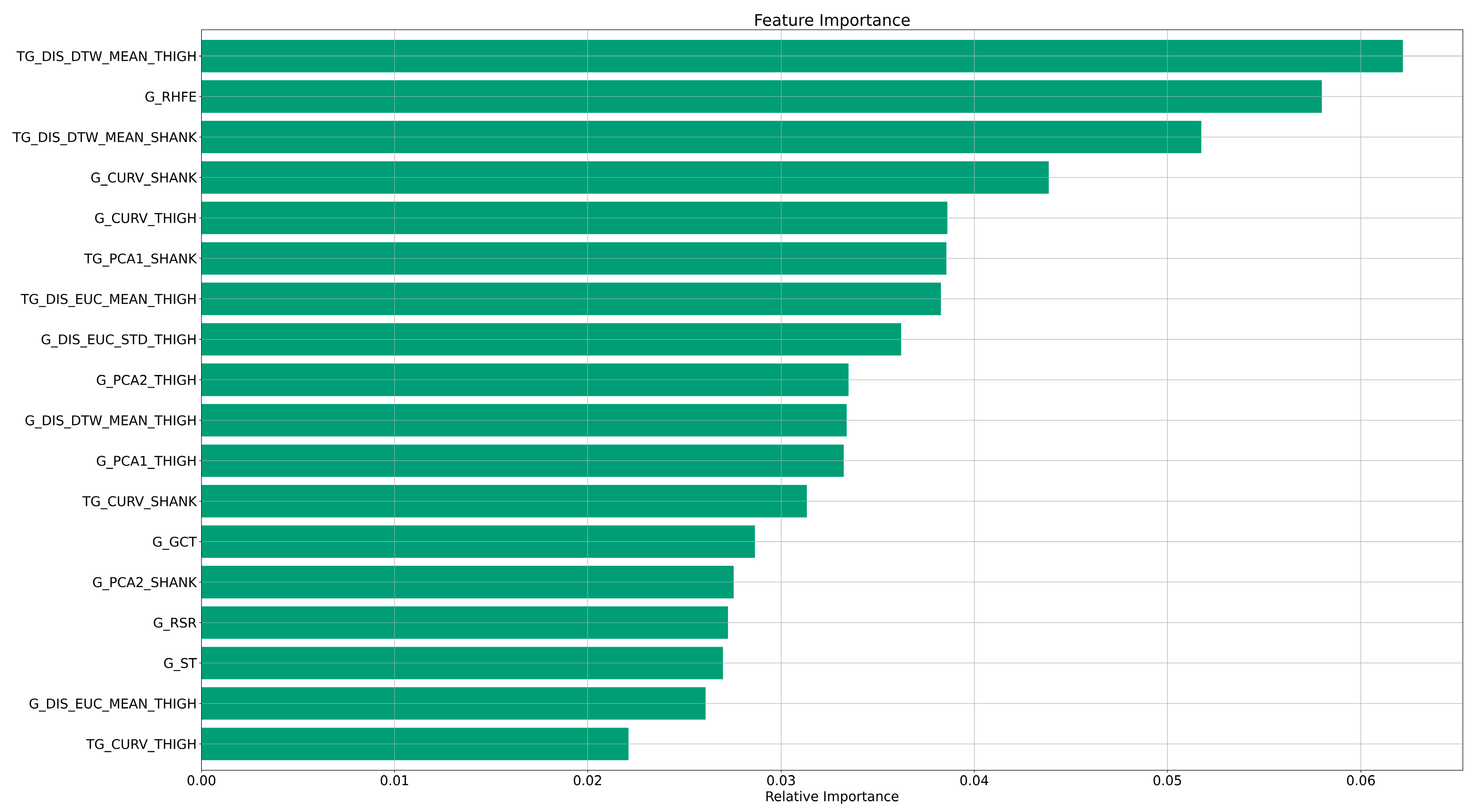
15], but more importantly, we identified the most contributing, meaningful, features, thereby increasing model explainability. We found that features that represent variability in gait are most relevant for classification using a random forest classifier, compared to temporal and spatial features, which contributed less.
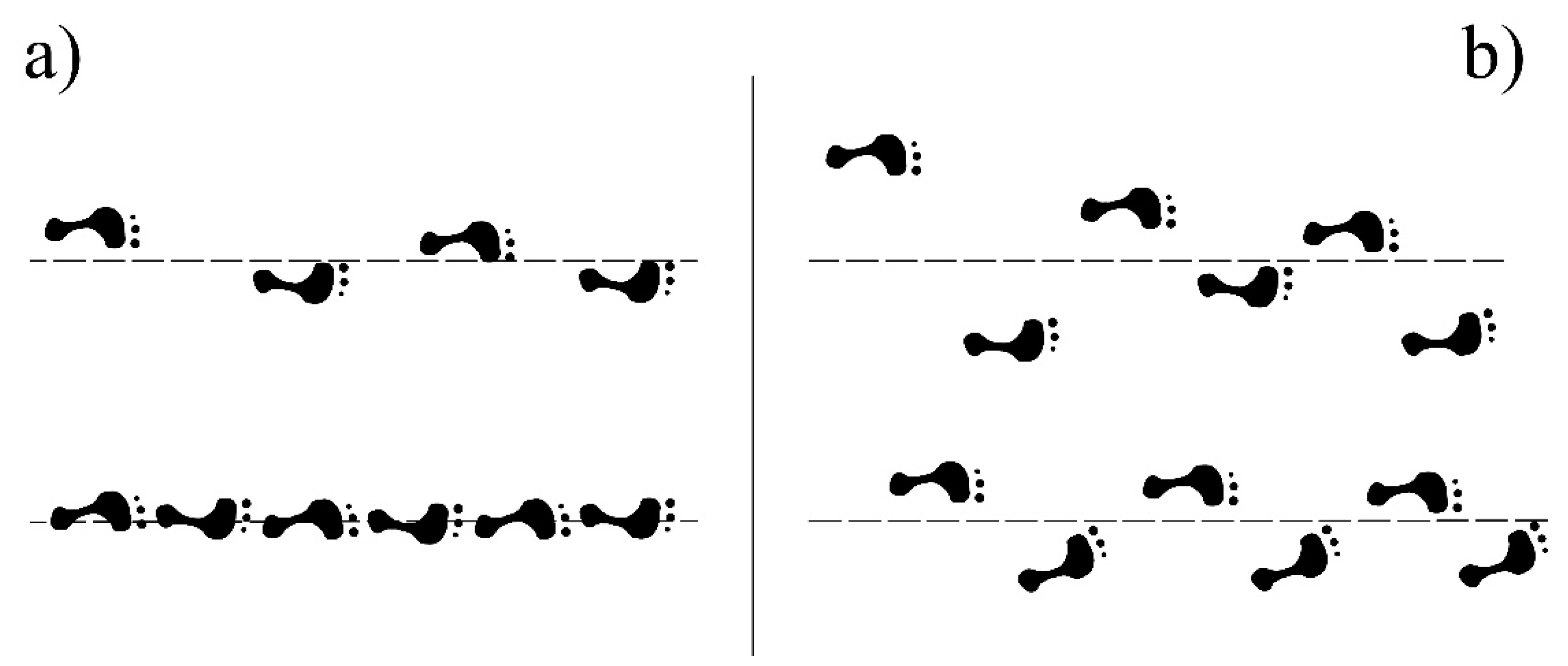
The most relevant features used by our random forest classifier were related with the range of the hip flexion–extension angle during gait or with variability of movement during tandem gait. This illustrates that the accurate classification of EOA, DCD and CTRL children depends on the incorporation of features representing variability, from both gait and tandem gait tests. This fits with our a priori hypothesis that abnormal gait is characterised by irregularities in movement and loss of smoothness, and also corresponds with the clinical concept of ataxic gait as visualized in
Figure 4.
As far as we know, there is limited literature on the automatic classification of EOA, DCD and CTRL children based on quantified movement data. Nevertheless, there are some studies aiming to distinguish between these groups. For example, in our previous study using information from gait only, we classified 80.0%, 85.7% and 70.0% of the CTRL, DCD and EOA children, respectively. Overall, that classifier correctly classified 78.4% of the participants [
15]. However, in that study we only used statistical features, that provide limited insight in the classification model. In the current study, we correctly classified 94.5%, 85.5% and 61.4% of the CTRL, DCD and EOA children, respectively. Overall, the random forest classifier correctly classified 82.0% of the participants. Not only did we achieve good classification performance, even slightly better than in our previous study, we also now derived knowledge-based features—related to how gait is assessed clinically, incorporating stride length and gait velocity, for example—instead of statistical features, thereby providing meaningful features that enhance the explainability of the classification model.
In the literature, there are some other studies aiming to distinguish between DCD patients and healthy participants using 3D motion capture systems [
9,
11,
16]. In a study aiming to examine the complexity and variability of gait, Rosengren et al. [
9] found that DCD patients performed movements with higher complexity, meaning that they had higher variability as well as asymmetry in their movement patterns compared to healthy children. In our study, in line with these findings, we found that the most relevant features used by the classifier to identify between groups are those related to the variability of gait (i.e., distance to the mean trajectory for thigh and shank sensors during tandem gait execution and the range of the hip flexion–extension angle during gait).
In another study, Woodruff et al. [
11], developed an index of walking performance to compare the gait patterns of children with DCD and healthy children. They combined four variables (percentage of cycle at opposite toe off, percentage of cycle of single stance, percentage of cycle at toe off and step length as a percentage of the gait cycle) to create a single index. DCD children showed abnormal gait patterns having larger variance in this index than healthy children. This is in line with our results, again suggesting that variability-based features are more meaningful for DCD distinction from healthy participants. To enhance the interpretability of our results, for the four most relevant features for our classification, we investigated if there was a significant difference between groups, by means of the Kruskal–Wallis H-test. These four features represented variability of movement, two measuring the distance of each gait cycle to the mean (TG_DIS_DTW_MEAN_THIGH, TG_DIS_DTW_MEAN_SHANK), one measuring the range of the angles during each gait cycle (G_RHFE) and one measuring the local curvature from the 3D angular velocity (G_CURV_SHANK). We calculated the median value per most relevant feature and group (see
Table 4 and the
Appendix A for an explanation of the features).
For the first three features, the medians are higher for the EOA group, lower for the CTRL group and values for the DCD group are in between, which is expected according to clinical experience. A possible explanation of the increased variability of gait parameters in DCD patients compared to CTRL children could be that DCD patients present increased coactivation, as suggested by Raynor [
27], meaning that DCD patients have not developed the same level of muscular organization compared to their healthy peers. Since motor incoordination in DCD patients is clinically associated with cerebellar dysfunction, patients may present with more complex movements, i.e., unskilled movements similar to those observed in typically developing children in the earlier stages of childhood [
28].
To the best of our knowledge, this is the first classification study using meaningful features based on the clinical construct of motor incoordination by combining information from the SARA gait and tandem gait tests. Although we obtained a good and insightful classification of EOA, DCD and CTRL children, there are some limitations to the study. First, we used a relatively small dataset (60 participants). However, it should be noted in that respect that, since EOA is a rare disorder, and we wanted to make sure that our labels were as accurate as possible, we carefully identified children with a formal diagnosis of having ataxia, validated by DNA analysis. This limited the number of children with ataxia eligible for our study. Another limitation is the use of inertial measurement units; we are aware that the use of even smaller and lighter sensors could further reduce any experienced restraint during the execution of the gait and tandem gait SARA tests. Hence, participants may not have walked as freely as during regular clinical examinations. However, we avoided pulling the Velcro bands too tight and the Shimmer IMUs only weigh 23.6 g each. Furthermore, we did not take the potential influence of height, cognitive processing, or other disease-independent participant characteristics on gait (variability) features into account. Yet, our results show that features that reflect gait variability during the straight walking part of both SARA gait tasks are most important for classifying the three participant groups. Hence, the potential noise added to these features due to disease-independent participant characteristics apparently does not hamper significant classification.
In the near future, we aim to include more data from the other SARA subtests, so that we can integrate all information for an improved classification of EOA, DCD and typically developing children. In this study, we aimed to distinguish between EOA, DCD and CTRL participants using meaningful information, deriving features similar to what clinicians look at when phenotypically evaluating patients. We expect that techniques such as deep learning may be helpful in further distinguishing hidden patterns, and can probably provide clinicians with new motor characteristics to consider. However, deep learning techniques typically require ample data, which should then first be collected.
We further hope that this study motivates other researchers to use wearable sensors for assessment of ataxia and other coordination disorders. Using this technology not only in the clinical environment but also during daily activities could potentially improve the early identification of ataxic signs.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}



