
Quantitative Comparison of Hand Kinematics Measured with a Markerless Commercial Head-Mounted Display and a Marker-Based Motion Capture System in Stroke Survivors
 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
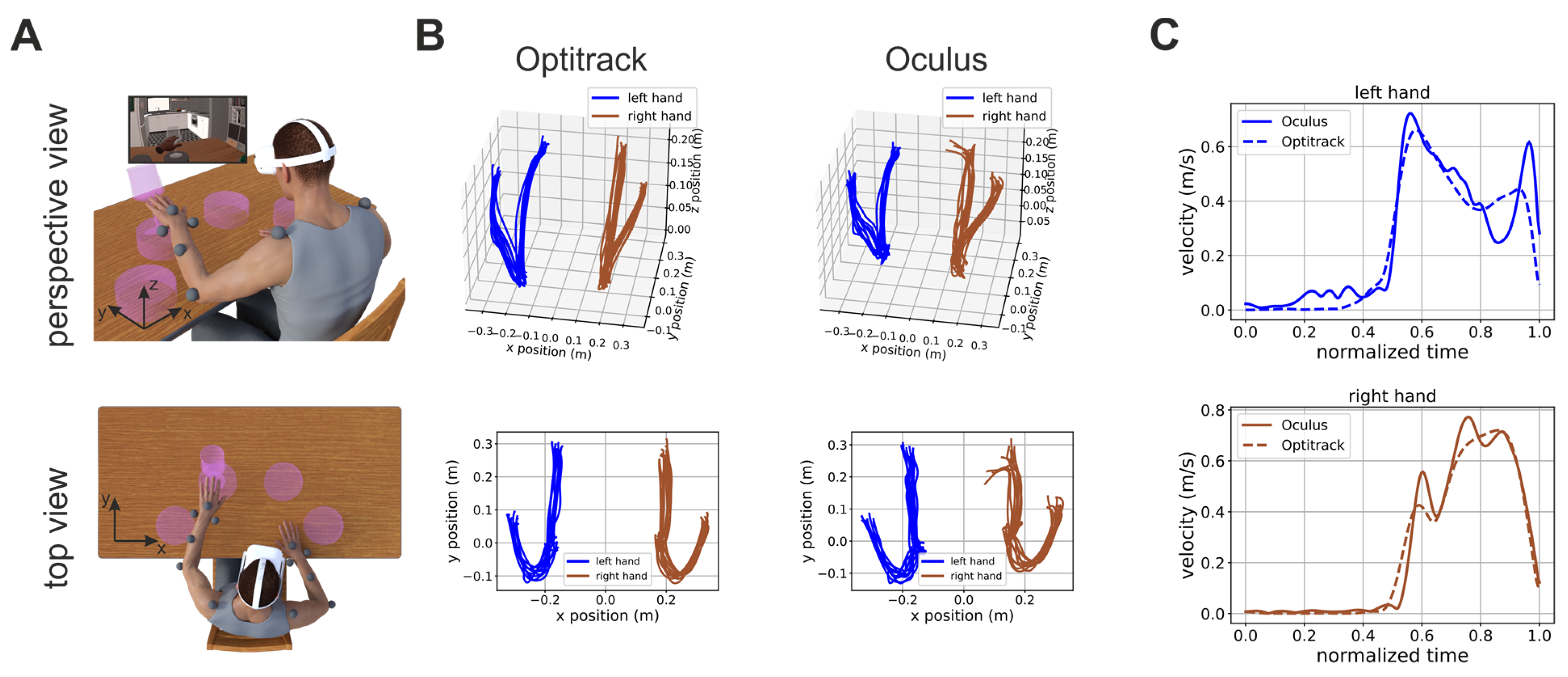
2.2. Experimental Procedures
2.3. Motion Capture
2.4. Data Analysis
2.5. Analysis of the Potential Spatial Dependence of Measurement Errors
2.6. Linear Regression Analysis
3. Results
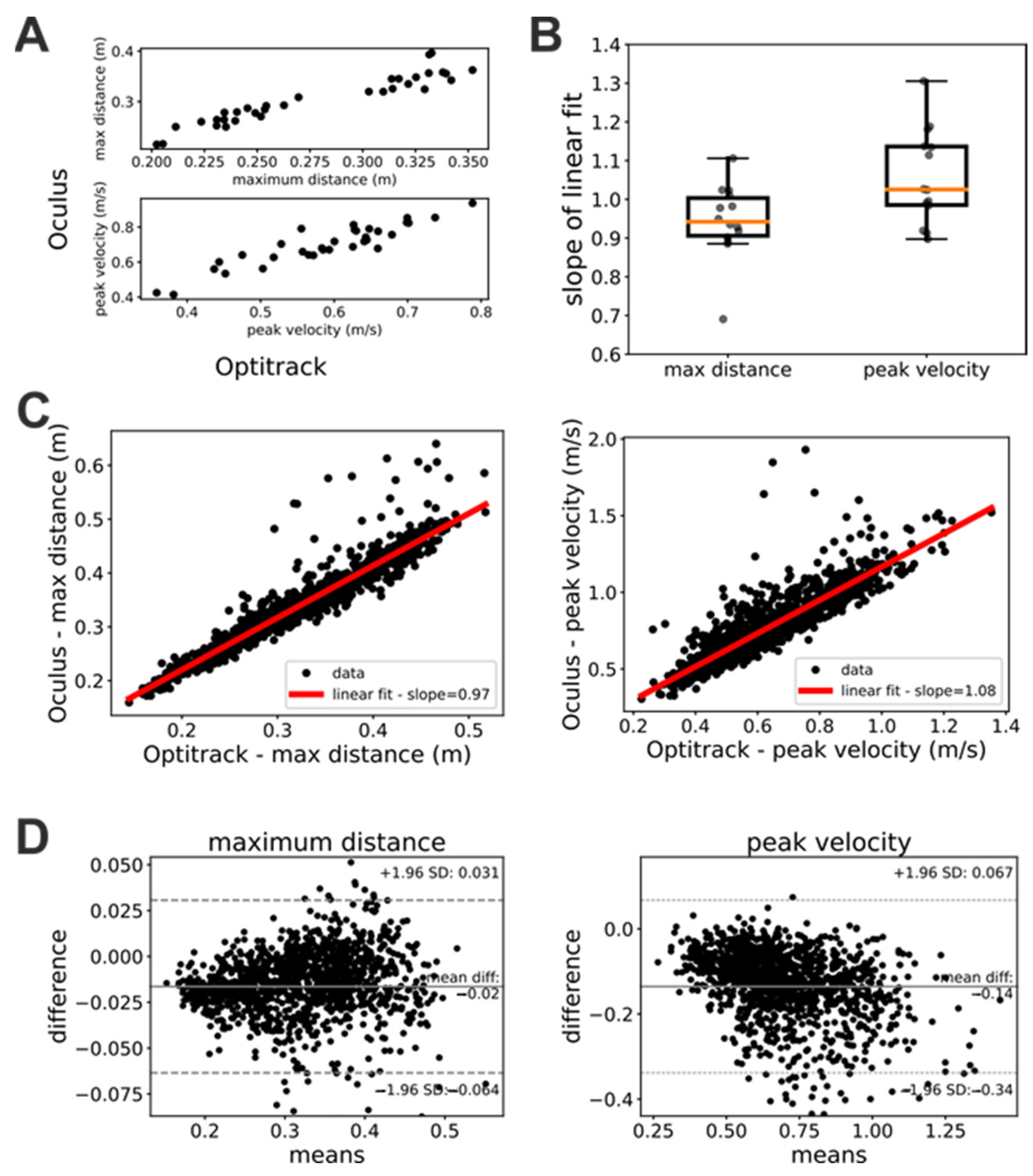
3.1. Oculus Estimates of Position and Velocity Are Linearly Related to Their Ground-Truth Values
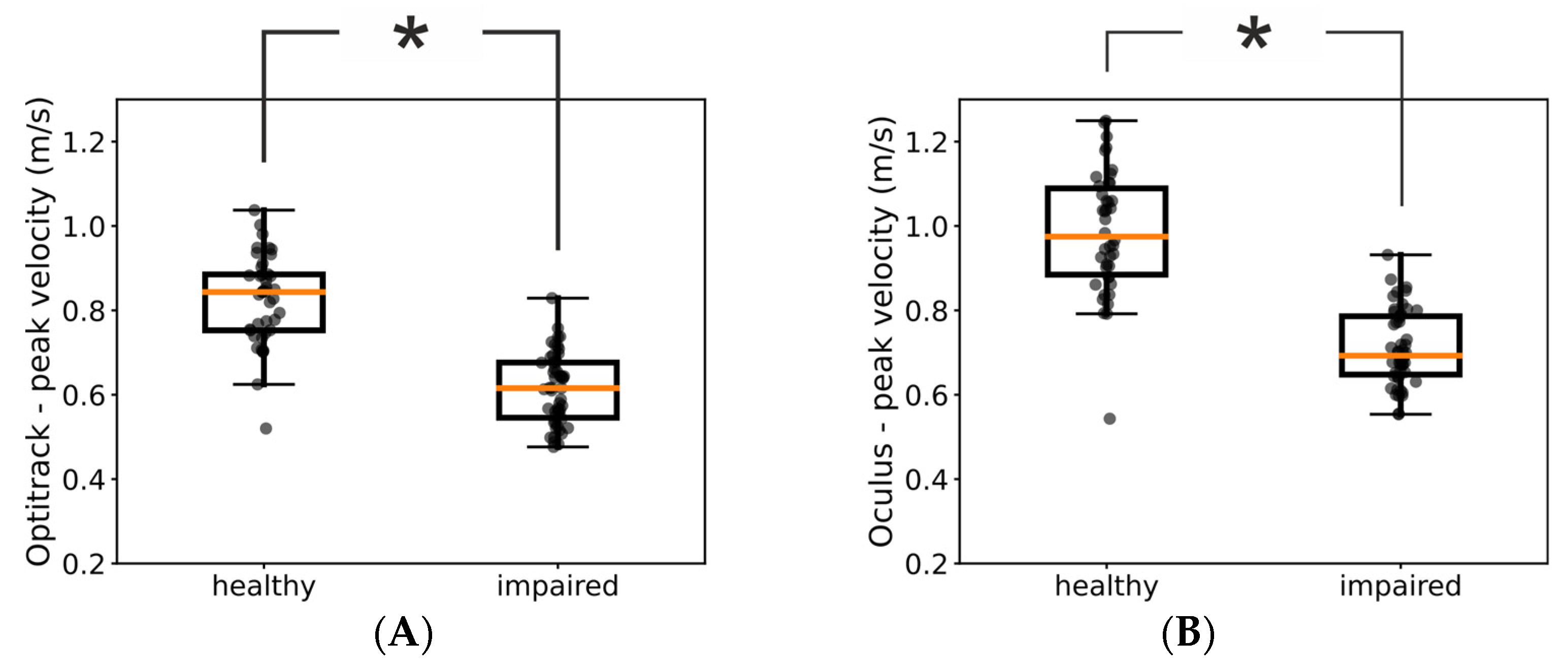
3.2. Oculus Kinematic Assessments Agree with the Same Assessments Based on Ground-Truth Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bonita, R.; Mendis, S.; Truelsen, T.; Bogousslavsky, J.; Toole, J.; Yatsu, F. The Global Stroke Initiative. Lancet Neurol. 2004, 3, 391–393. [Google Scholar] [CrossRef] [PubMed]
- Warlow, C.; Gijn, J.; Dennis, M.; Wardlaw, J.; Bamford, J.; Hankey, G.; Sandercock, P.; Rinkel, G.; Langhorne, P.; Sudlow, C.; et al. Stroke-Practical Management; Wiley-Blackwell: Oxford, UK, 2008; ISBN 978-1-4051-2766-0. [Google Scholar]
- World Health Organization. The World Health Report: 2003: Shaping the Future; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Wafa, H.A.; Wolfe, C.D.A.; Emmett, E.; Roth, G.A.; Johnson, C.O.; Wang, Y. Burden of Stroke in Europe: Thirty-Year Projections of Incidence, Prevalence, Deaths, and Disability-Adjusted Life Years. Stroke 2020, 51, 2418–2427. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.A.; Krishnamurthi, R.V.; Barker-Collo, S.; Forouzanfar, M.H.; Naghavi, M.; Connor, M.; Lawes, C.M.M.; Moran, A.E.; Anderson, L.M.; Roth, G.A.; et al. The Global Burden of Ischemic Stroke: Findings of the GBD 2010 Study. Glob. Heart 2014, 9, 107–112. [Google Scholar] [CrossRef]
- Luengo-Fernandez, R.; Violato, M.; Candio, P.; Leal, J. Economic Burden of Stroke across Europe: A Population-Based Cost Analysis. Eur. Stroke J. 2020, 5, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Nijland, R.H.M.; van Wegen, E.E.H.; Harmeling-van der Wel, B.C.; Kwakkel, G.; EPOS Investigators. Presence of Finger Extension and Shoulder Abduction within 72 Hours after Stroke Predicts Functional Recovery: Early Prediction of Functional Outcome after Stroke: The EPOS Cohort Study. Stroke 2010, 41, 745–750. [Google Scholar] [CrossRef]
- Dimyan, M.A.; Cohen, L.G. Neuroplasticity in the Context of Motor Rehabilitation after Stroke. Nat. Rev. Neurol. 2011, 7, 76–85. [Google Scholar] [CrossRef]
- Huang, J.; Ji, J.-R.; Liang, C.; Zhang, Y.-Z.; Sun, H.-C.; Yan, Y.-H.; Xing, X.-B. Effects of Physical Therapy-Based Rehabilitation on Recovery of Upper Limb Motor Function after Stroke in Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Ann. Palliat. Med. 2022, 11, 521–531. [Google Scholar] [CrossRef]
- van Lieshout, E.C.C.; van de Port, I.G.; Dijkhuizen, R.M.; Visser-Meily, J.M.A. Does Upper Limb Strength Play a Prominent Role in Health-Related Quality of Life in Stroke Patients Discharged from Inpatient Rehabilitation? Top. Stroke Rehabil. 2020, 27, 525–533. [Google Scholar] [CrossRef]
- Morris, J.H.; van Wijck, F.; Joice, S.; Donaghy, M. Predicting Health Related Quality of Life 6 Months after Stroke: The Role of Anxiety and Upper Limb Dysfunction. Disabil. Rehabil. 2013, 35, 291–299. [Google Scholar] [CrossRef]
- Kwakkel, G.; Lannin, N.A.; Borschmann, K.; English, C.; Ali, M.; Churilov, L.; Saposnik, G.; Winstein, C.; van Wegen, E.E.; Wolf, S.L.; et al. Standardized Measurement of Sensorimotor Recovery in Stroke Trials: Consensus-Based Core Recommendations from the Stroke Recovery and Rehabilitation Roundtable. Int. J. Stroke Off. J. Int. Stroke Soc. 2017, 12, 451–461. [Google Scholar] [CrossRef]
- Maura, R.M.; Rueda Parra, S.; Stevens, R.E.; Weeks, D.L.; Wolbrecht, E.T.; Perry, J.C. Literature Review of Stroke Assessment for Upper-Extremity Physical Function via EEG, EMG, Kinematic, and Kinetic Measurements and Their Reliability. J. Neuroeng. Rehabil. 2023, 20, 21. [Google Scholar] [CrossRef]
- Thrane, G.; Sunnerhagen, K.S.; Murphy, M.A. Upper Limb Kinematics during the First Year after Stroke: The Stroke Arm Longitudinal Study at the University of Gothenburg (SALGOT). J. Neuroeng. Rehabil. 2020, 17, 76. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, A.; Kanzler, C.M.; Lambercy, O.; Luft, A.R.; Veerbeek, J.M. Systematic Review on Kinematic Assessments of Upper Limb Movements After Stroke. Stroke 2019, 50, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Kwakkel, G.; Van Wegen, E.; Burridge, J.H.; Winstein, C.J.; van Dokkum, L.; Alt Murphy, M.; Levin, M.F.; Krakauer, J.W. Standardized Measurement of Quality of Upper Limb Movement after Stroke: Consensus-Based Core Recommendations from the Second Stroke Recovery and Rehabilitation Roundtable. Int. J. Stroke Off. J. Int. Stroke Soc. 2019, 14, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Cerfoglio, S.; Ferraris, C.; Vismara, L.; Amprimo, G.; Priano, L.; Pettiti, G.; Galli, M.; Mauro, A.; Cimolin, V. Kinect-Based Assessment of Lower Limbs during Gait in Post-Stroke Hemiplegic Patients: A Narrative Review. Sensors 2022, 22, 4910. [Google Scholar] [CrossRef]
- Lam, W.W.T.; Tang, Y.M.; Fong, K.N.K. A Systematic Review of the Applications of Markerless Motion Capture (MMC) Technology for Clinical Measurement in Rehabilitation. J. Neuroeng. Rehabil. 2023, 20, 57. [Google Scholar] [CrossRef]
- Wade, L.; Needham, L.; McGuigan, P.; Bilzon, J. Applications and Limitations of Current Markerless Motion Capture Methods for Clinical Gait Biomechanics. PeerJ 2022, 10, e12995. [Google Scholar] [CrossRef]
- Ganguly, A.; Rashidi, G.; Mombaur, K. Comparison of the Performance of the Leap Motion ControllerTM with a Standard Marker-Based Motion Capture System. Sensors 2021, 21, 1750. [Google Scholar] [CrossRef]
- Lahkar, B.K.; Muller, A.; Dumas, R.; Reveret, L.; Robert, T. Accuracy of a Markerless Motion Capture System in Estimating Upper Extremity Kinematics during Boxing. Front. Sports Act. Living 2022, 4, 939980. [Google Scholar] [CrossRef]
- Smeragliuolo, A.H.; Hill, N.J.; Disla, L.; Putrino, D. Validation of the Leap Motion Controller Using Markered Motion Capture Technology. J. Biomech. 2016, 49, 1742–1750. [Google Scholar] [CrossRef]
- Bonnechère, B.; Sholukha, V.; Omelina, L.; Van Sint Jan, S.; Jansen, B. 3D Analysis of Upper Limbs Motion during Rehabilitation Exercises Using the KinectTM Sensor: Development, Laboratory Validation and Clinical Application. Sensors 2018, 18, 2216. [Google Scholar] [CrossRef]
- Banakou, D.; Groten, R.; Slater, M. Illusory Ownership of a Virtual Child Body Causes Overestimation of Object Sizes and Implicit Attitude Changes. Proc. Natl. Acad. Sci. USA 2013, 110, 12846–12851. [Google Scholar] [CrossRef] [PubMed]
- Fodor, L.A.; Coteț, C.D.; Cuijpers, P.; Szamoskozi, Ș.; David, D.; Cristea, I.A. The Effectiveness of Virtual Reality Based Interventions for Symptoms of Anxiety and Depression: A Meta-Analysis. Sci. Rep. 2018, 8, 10323. [Google Scholar] [CrossRef] [PubMed]
- Keizer, A.; van Elburg, A.; Helms, R.; Dijkerman, H.C. A Virtual Reality Full Body Illusion Improves Body Image Disturbance in Anorexia Nervosa. PLoS ONE 2016, 11, e0163921. [Google Scholar] [CrossRef] [PubMed]
- Marini, M.; Casile, A. I Can See My Virtual Body in a Mirror: The Role of Visual Perspective in Changing Implicit Racial Attitudes Using Virtual Reality. Front. Psychol. 2022, 13, 989582. [Google Scholar] [CrossRef]
- Slater, M.; Sanchez-Vives, M.V. Enhancing Our Lives with Immersive Virtual Reality. Front. Robot. AI 2016, 3, 74. [Google Scholar] [CrossRef]
- Tassinari, M.; Aulbach, M.B.; Jasinskaja-Lahti, I. The Use of Virtual Reality in Studying Prejudice and Its Reduction: A Systematic Review. PLoS ONE 2022, 17, e0270748. [Google Scholar] [CrossRef]
- Yee, N.; Bailenson, J. The Proteus Effect: The Effect of Transformed Self-Representation on Behavior. Hum. Commun. Res. 2007, 33, 271–290. [Google Scholar] [CrossRef]
- Pau, M.; Porta, M.; Bertoni, R.; Mattos, F.G.M.; Cocco, E.; Cattaneo, D. Effect of Immersive Virtual Reality Training on Hand-to-Mouth Task Performance in People with Multiple Sclerosis: A Quantitative Kinematic Study. Mult. Scler. Relat. Disord. 2023, 69, 104455. [Google Scholar] [CrossRef]
- Demeco, A.; Zola, L.; Frizziero, A.; Martini, C.; Palumbo, A.; Foresti, R.; Buccino, G.; Costantino, C. Immersive Virtual Reality in Post-Stroke Rehabilitation: A Systematic Review. Sensors 2023, 23, 1712. [Google Scholar] [CrossRef]
- Marek, K.; Zubrycki, I.; Miller, E. Immersion Therapy with Head-Mounted Display for Rehabilitation of the Upper Limb after Stroke-Review. Sensors 2022, 22, 9962. [Google Scholar] [CrossRef] [PubMed]
- Patsaki, I.; Dimitriadi, N.; Despoti, A.; Tzoumi, D.; Leventakis, N.; Roussou, G.; Papathanasiou, A.; Nanas, S.; Karatzanos, E. The Effectiveness of Immersive Virtual Reality in Physical Recovery of Stroke Patients: A Systematic Review. Front. Syst. Neurosci. 2022, 16, 880447. [Google Scholar] [CrossRef] [PubMed]
- Jost, T.A.; Nelson, B.; Rylander, J. Quantitative Analysis of the Oculus Rift S in Controlled Movement. Disabil. Rehabil. Assist. Technol. 2021, 16, 632–636. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.M.; Stafford, J.; Egorova, A.; McCabe, C.; Matthews, M. Can We Use the Oculus Quest VR Headset and Controllers to Reliably Assess Balance Stability? Diagn. Basel Switz. 2022, 12, 1409. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Chen, K.B.; Lin, J.-H.; Radwin, R.G. The Accuracy of the Oculus Rift Virtual Reality Head-Mounted Display during Cervical Spine Mobility Measurement. J. Biomech. 2015, 48, 721–724. [Google Scholar] [CrossRef]
- Carnevale, A.; Mannocchi, I.; Sassi, M.S.H.; Carli, M.; De Luca, G.; Longo, U.G.; Denaro, V.; Schena, E. Virtual Reality for Shoulder Rehabilitation: Accuracy Evaluation of Oculus Quest 2. Sensors 2022, 22, 5511. [Google Scholar] [CrossRef]
- Fregna, G.; Schincaglia, N.; Baroni, A.; Straudi, S.; Casile, A. A Novel Immersive Virtual Reality Environment for the Motor Rehabilitation of Stroke Patients: A Feasibility Study. Front. Robot. AI 2022, 9, 906424. [Google Scholar] [CrossRef]
- Kim, G.J.; Parnandi, A.; Eva, S.; Schambra, H. The Use of Wearable Sensors to Assess and Treat the Upper Extremity after Stroke: A Scoping Review. Disabil. Rehabil. 2022, 44, 6119–6138. [Google Scholar] [CrossRef]
- Maceira-Elvira, P.; Popa, T.; Schmid, A.-C.; Hummel, F.C. Wearable Technology in Stroke Rehabilitation: Towards Improved Diagnosis and Treatment of Upper-Limb Motor Impairment. J. Neuroeng. Rehabil. 2019, 16, 142. [Google Scholar] [CrossRef]
- Liz, L.; da Silva, T.G.; Michaelsen, S.M. Validity, Reliability, and Measurement Error of the Remote Fugl-Meyer Assessment by Videoconferencing: Tele-FMA. Phys. Ther. 2023, 103, pzad054. [Google Scholar] [CrossRef]
- Yang, C.-L.; Simpson, L.A.; Eng, J.J. A Pilot Study for Remote Evaluation of Upper Extremity Motor Function After Stroke: The Arm Capacity and Movement Test (ArmCAM). Am. J. Occup. Ther. Off. Publ. Am. Occup. Ther. Assoc. 2023, 77, 7701205020. [Google Scholar] [CrossRef] [PubMed]
- Webster, D.; Celik, O. Systematic Review of Kinect Applications in Elderly Care and Stroke Rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 108. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, I.A.; da Fonseca, P.F.P.; Pinheiro, A.R.V.; Velhote Correia, M.F.P.; da Silva, C.I.C. Methodological Considerations for Kinematic Analysis of Upper Limbs in Healthy and Poststroke Adults Part II: A Systematic Review of Motion Capture Systems and Kinematic Metrics. Top. Stroke Rehabil. 2019, 26, 464–472. [Google Scholar] [CrossRef]
- Alt Murphy, M.; Willén, C.; Sunnerhagen, K.S. Kinematic Variables Quantifying Upper-Extremity Performance after Stroke during Reaching and Drinking from a Glass. Neurorehabil. Neural Repair 2011, 25, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, A.; Bhagubai, M.M.C.; Nies, S.H.G.; Held, J.P.O.; Veltink, P.H.; Buurke, J.H.; Luft, A.R. Characterization of Stroke-Related Upper Limb Motor Impairments across Various Upper Limb Activities by Use of Kinematic Core Set Measures. J. Neuroeng. Rehabil. 2022, 19, 2. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Sample (N = 14) | |
|---|---|
| Age (mean, SD) | 59 ± 15 |
| Sex | |
| Males | 10 (71%) |
| Females | 4 (29%) |
| Stroke Type | |
| Ischemic | 13 (93%) |
| Hemorrhagic | 1 (7%) |
| Stroke side | |
| Left | 5 (36%) |
| Right | 9 (64%) |
| Stroke timeframe | |
| <1 year | 6 (42%) |
| 1–3 years | 4 (29%) |
| >3 years | 4 (29%) |
| FMA-UE score (min-max) | 20–65 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Optitrack | 7.37 × 10−3 | 8.23 × 10−4 | 1.80 × 10−4 | 5.77 × 10−15 | 6.36 × 10−1 | 4.44 × 10−3 | 1.81 × 10−3 | 2.36 × 10−1 | 4.32 × 10−8 | 2.40 × 10−5 | 3.06 × 10−13 | 2.15 × 10−10 | 2.60 × 10−1 | 1.10 × 10−4 |
| Oculus | 5.35 × 10−1 | 7.02 × 10−3 | 3.69 × 10−2 | 8.24 × 10−13 | 2.84 × 10−1 | 1.27 × 10−3 | 8.73 × 10−4 | 1.44 × 10−1 | 1.16 × 10−6 | 1.12 × 10−2 | 1.02 × 10−13 | 1.02 × 10−5 | 1.43 × 10−1 | 4.56 × 10−4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casile, A.; Fregna, G.; Boarini, V.; Paoluzzi, C.; Manfredini, F.; Lamberti, N.; Baroni, A.; Straudi, S. Quantitative Comparison of Hand Kinematics Measured with a Markerless Commercial Head-Mounted Display and a Marker-Based Motion Capture System in Stroke Survivors. Sensors 2023, 23, 7906. https://doi.org/10.3390/s23187906
Casile A, Fregna G, Boarini V, Paoluzzi C, Manfredini F, Lamberti N, Baroni A, Straudi S. Quantitative Comparison of Hand Kinematics Measured with a Markerless Commercial Head-Mounted Display and a Marker-Based Motion Capture System in Stroke Survivors. Sensors. 2023; 23(18):7906. https://doi.org/10.3390/s23187906
Chicago/Turabian StyleCasile, Antonino, Giulia Fregna, Vittorio Boarini, Chiara Paoluzzi, Fabio Manfredini, Nicola Lamberti, Andrea Baroni, and Sofia Straudi. 2023. "Quantitative Comparison of Hand Kinematics Measured with a Markerless Commercial Head-Mounted Display and a Marker-Based Motion Capture System in Stroke Survivors" Sensors 23, no. 18: 7906. https://doi.org/10.3390/s23187906