
Hearing and Seeing Nerve/Tendon Snapping: A Systematic Review on Dynamic Ultrasound Examination
 ,
,  , , and
, , and
Abstract
:1. Introduction
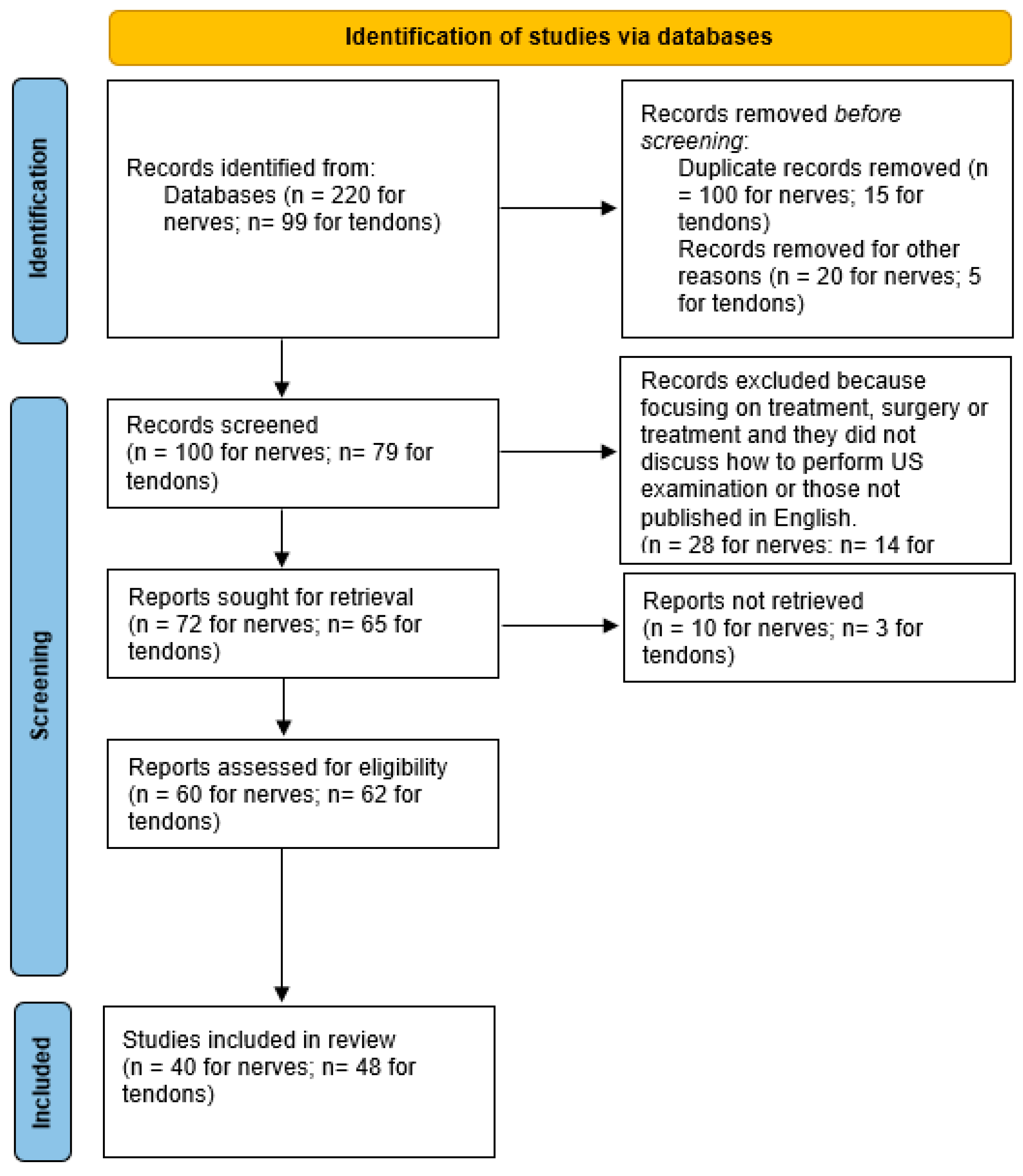
2. Materials and Methods
3. Results
4. Discussion
4.1. Nerve Snapping
4.2. Tendon Snapping
4.3. Future Perspectives Assessing Pros/Cons of Dynamic US Examination in the Evaluation of Nerve/Tendon Snapping
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marchand, A.J.; Proisy, M.; Ropars, M.; Cohen, M.; Duvauferrier, R.; Guillin, R. Snapping knee: Imaging findings with an emphasis on dynamic sonography. AJR Am. J. Roentgenol. 2012, 199, 142–150. [Google Scholar] [CrossRef]
- Pirri, C.; Stecco, C.; Güvener, O.; Mezian, K.; Ricci, V.; Jačisko, J.; Novotný, T.; Kara, M.; Chang, K.V.; Dughbaj, M.; et al. EURO-MUSCULUS/USPRM Dynamic Ultrasound Protocols for Knee. Am. J. Phys. Med. Rehabil. 2023, 102, e67–e72. [Google Scholar] [CrossRef] [PubMed]
- Mezian, K.; Ricci, V.; Güvener, O.; Jačisko, J.; Novotný, T.; Kara, M.; Chang, K.V.; Naňka, O.; Pirri, C.; Stecco, C.; et al. EURO-MUSCULUS/USPRM Dynamic Ultrasound Protocols for (Adult) Hip. Am. J. Phys. Med. Rehabil. 2022, 101, e162–e168. [Google Scholar] [CrossRef]
- Ricci, V.; Güvener, O.; Chang, K.V.; Wu, W.T.; Mezian, K.; Kara, M.; Leblebicioğlu, G.; Pirri, C.; Ata, A.M.; Dughbaj, M.; et al. EURO-MUSCULUS/USPRM Dynamic Ultrasound Protocols for Elbow. Am. J. Phys. Med. Rehabil. 2022, 101, e83–e92. [Google Scholar] [CrossRef] [PubMed]
- Çağlayan, G.; Özçakar, L.; Kaymak, S.U.; Kaymak, B.; Tan, A.A. Effects of Sono-feedback during aspiration of Baker’s cysts: A controlled clinical trial. J. Rehabil. Med. 2016, 48, 386–389. [Google Scholar] [PubMed] [Green Version]
- Cambon-Binder, A. Ulnar neuropathy at the elbow. Orthop. Traumatol. Surg. Res. 2021, 107, 102754. [Google Scholar] [CrossRef]
- Tsukada, K.; Yasui, Y.; Sasahara, J.; Okawa, Y.; Nakagawa, T.; Kawano, H.; Miyamoto, W. Ulnar Nerve Dislocation and Subluxation from the Cubital Tunnel Are Common in College Athletes. J. Clin. Med. 2021, 10, 3131. [Google Scholar] [CrossRef]
- Pisapia, J.M.; Ali, Z.S.; Hudgins, E.D.; Khoury, V.; Heuer, G.G.; Zager, E.L. Ultrasonography Detects Ulnar Nerve Dislocation Despite Normal Electrophysiology and Magnetic Resonance Imaging. World Neurosurg. 2017, 99, 809.e1–809.e5. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S.; Rosas, H.G.; Craig, J.G. Musculoskeletal ultrasound: Elbow imaging and procedures. Semin. Musculoskelet. Radiol. 2010, 14, 449–460. [Google Scholar] [CrossRef]
- Coraci, D.; Giovannini, S.; Imbimbo, I.; Santilli, V.; Padua, L. Ulnar Nerve Dislocation at the Elbow: The Role of Ultrasound. World Neurosurg. 2017, 103, 934–935. [Google Scholar] [CrossRef]
- Martinoli, C.; Bianchi, S.; Derchi, L.E. Tendon and nerve sonography. Radiol. Clin. N. Am. 1999, 37, 691–711. [Google Scholar] [CrossRef] [PubMed]
- Kakita, M.; Mikami, Y.; Ibusuki, T.; Shimoe, T.; Kamijo, Y.I.; Hoekstra, S.P.; Tajima, F. The prevalence of ulnar neuropathy at the elbow and ulnar nerve dislocation in recreational wheelchair marathon athletes. PLoS ONE 2020, 15, e0243324. [Google Scholar] [CrossRef] [PubMed]
- Martinoli, C.; Bianchi, S.; Dahmane, M.; Pugliese, F.; Bianchi-Zamorani, M.P.; Valle, M. Ultrasound of tendons and nerves. Eur. Radiol. 2002, 12, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Omejec, G.; Podnar, S. Does ulnar nerve dislocation at the elbow cause neuropathy? Muscle Nerve 2016, 53, 255–259. [Google Scholar] [CrossRef]
- Endo, F.; Tajika, T.; Kuboi, T.; Shinagawa, S.; Tsukui, T.; Nakajima, T.; Kogure, Y.; Chikuda, H. The ultrasonographic assessment of the morphologic changes in the ulnar nerve at the cubital tunnel in Japanese volunteers: Relationship between dynamic ulnar nerve instability and clinical symptoms. JSES Int. 2021, 5, 942–947. [Google Scholar] [CrossRef]
- Okamoto, M.; Abe, M.; Shirai, H.; Ueda, N. Morphology and dynamics of the ulnar nerve in the cubital tunnel. Observation by ultrasonography. J. Hand. Surg. Br. 2000, 25, 85–89. [Google Scholar] [CrossRef]
- Cornelson, S.M.; Sclocco, R.; Kettner, N.W. Ulnar nerve instability in the cubital tunnel of asymptomatic volunteers. J. Ultrasound 2019, 22, 337–344. [Google Scholar] [CrossRef]
- Kang, S.; Yoon, J.S.; Yang, S.N.; Choi, H.S. Retrospective study on the impact of ulnar nerve dislocation on the pathophysiology of ulnar neuropathy at the elbow. Peer J. 2019, 7, e6972. [Google Scholar] [CrossRef]
- Schertz, M.; Mutschler, C.; Masmejean, E.; Silvera, J. High-resolution ultrasound in etiological evaluation of ulnar neuropathy at the elbow. Eur. J. Radiol. 2017, 95, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Grechenig, W.; Clement, H.; Mayr, J.; Peicha, G. Ultrasound detection of dislocation of the ulnar nerve from the sulcus of the elbow joint. Praxis 2003, 92, 1129–1132. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.J.; Koh, S.B.; Park, K.W.; Kim, S.J.; Yoon, J.S. Pearls & Oy-sters: False positives in short-segment nerve conduction studies due to ulnar nerve dislocation. Neurology 2008, 70, e9–e13. [Google Scholar] [PubMed] [Green Version]
- Imao, K.; Miwa, H.; Tsubokawa, N.; Maki, Y.; Endo, N. Dislocation of the Medial Head of the Triceps With Ulnar Nerve Location Anterior to the Medial Epicondyle. J. Hand. Surg. Am. 2020, 45, 72.e1–72.e4. [Google Scholar] [CrossRef] [PubMed]
- Cesmebasi, A.; O’driscoll, S.W.; Smith, J.; Skinner, J.A.; Spinner, R.J. The snapping medial antebrachial cutaneous nerve. Clin. Anat. 2015, 28, 872–877. [Google Scholar] [CrossRef]
- Plaikner, M.; Loizides, A.; Loescher, W.; Spiss, V.; Gruber, H.; Djurdjevic, T.; Peer, S. Thickened hyperechoic outer epineurium, a sonographic sign suggesting snapping ulnar nerve syndrome? Ultraschall. Med. 2013, 34, 58–63. [Google Scholar] [CrossRef]
- Kim, B.J.; Date, E.S.; Lee, S.H.; Yoon, J.S.; Hur, S.Y.; Kim, S.J. Distance measure error induced by displacement of the ulnar nerve when the elbow is flexed. Arch. Phys. Med. Rehabil. 2005, 86, 809–812. [Google Scholar] [CrossRef]
- Yoo, M.J.; Kim, D.D.J.; Oh-Park, M. Exacerbation of habitual dislocation of ulnar nerve by concurrent dislocation of triceps muscle: Complementary role of dynamic ultrasonography to electrodiagnosis. Am. J. Phys. Med. Rehabil. 2007, 86, 1030. [Google Scholar] [CrossRef]
- Shimizu, H.; Beppu, M.; Arai, T.; Kihara, H.; Izumiyama, K. Ultrasonographic findings in cubital tunnel syndrome caused by a cubitus varus deformity. Hand Surg. 2011, 16, 233–238. [Google Scholar] [CrossRef]
- Hatem, M.; Martin, H.D.; Safran, M.R. Snapping of the Sciatic Nerve and Sciatica Provoked by Impingement Between the Greater Trochanter and Ischium: A Case Report. JBJS Case Connect. 2020, 10, e2000014. [Google Scholar] [CrossRef]
- Reisner, J.H.; Boettcher, B.J.; Johnson, A.C.; Cummings, N.M.; Jelsing, E.J. To Be or Not to Be (A Morton’s/Interdigital Neuroma): That Is the Question-A Case Series of Lateral Forefoot Pain Localized to the Proper Digital Nerve of the Fifth Toe. Clin. J. Sport Med. 2021, 31, e287–e289. [Google Scholar] [CrossRef] [PubMed]
- Chuang, H.J.; Hsiao, M.Y.; Wu, C.H.; Özçakar, L. Dynamic Ultrasound Imaging for Ulnar Nerve Subluxation and Snapping Triceps Syndrome. Am. J. Phys. Med. Rehabil. 2016, 95, e113–e114. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.H.; Joo, B.E.; Kim, K.H.; Park, B.K.; Cha, J.; Kim, D.H. Ultrasonographic and Electrophysiological Evaluation of Ulnar Nerve Instability and Snapping of the Triceps Medial Head in Healthy Subjects. Am. J. Phys. Med. Rehabil. 2017, 96, e141–e146. [Google Scholar] [CrossRef] [PubMed]
- Allen, G.; Wilson, D. Ultrasound of the upper limb: When to use it in athletes. Semin. Musculoskelet. Radiol. 2012, 16, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Bjerre, J.J.; Johannsen, F.E.; Rathcke, M.; Krogsgaard, M.R. Snapping elbow-A guide to diagnosis and treatment. World J. Orthop. 2018, 9, 65–71. [Google Scholar] [CrossRef]
- Chang, K.V.; Hung, C.Y.; Özçakar, L. Snapping Thumb and Superficial Radial Nerve Entrapment in De Quervain Disease: Ultrasound Imaging/Guidance Revisited. Pain. Med. 2015, 16, 2214–2215. [Google Scholar] [CrossRef]
- Jacobson, J.A.; Jebson, P.J.; Jeffers, A.W.; Fessell, D.P.; Hayes, C.W. Ulnar nerve dislocation and snapping triceps syndrome: Diagnosis with dynamic sonography--report of three cases. Radiology 2001, 220, 601–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yiannakopoulos, C.K. Imaging diagnosis of the snapping triceps syndrome. Radiology 2002, 225, 607–608, author reply 608. [Google Scholar] [CrossRef] [PubMed]
- Michael, A.E.; Young, P. Is triceps hypertrophy associated with ulnar nerve luxation? Muscle Nerve 2018, 58, 523–527. [Google Scholar] [CrossRef]
- Erez, O.; Khalil, J.G.; Legakis, J.E.; Tweedie, J.; Kaminski, E.; Reynolds, R.A. Ultrasound evaluation of ulnar nerve anatomy in the pediatric population. J. Pediatr. Orthop. 2012, 32, 641–646. [Google Scholar] [CrossRef]
- Granata, G.; Padua, L.; Celletti, C.; Castori, M.; Saraceni, V.M.; Camerota, F. Entrapment neuropathies and polyneuropathies in joint hypermobility syndrome/Ehlers-Danlos syndrome. Clin. Neurophysiol. 2013, 124, 1689–1694. [Google Scholar] [CrossRef]
- Tai, T.W.; Kuo, L.C.; Chen, W.C.; Wang, L.H.; Chao, S.Y.; Huang, C.N.; Jou, I.M. Anterior translation and morphologic changes of the ulnar nerve at the elbow in adolescent baseball players. Ultrasound Med. Biol. 2014, 40, 45–52. [Google Scholar] [CrossRef]
- Van Den Berg, P.J.; Pompe, S.M.; Beekman, R.; Visser, L.H. Sonographic incidence of ulnar nerve (sub)luxation and its associated clinical and electrodiagnostic characteristics. Muscle Nerve 2013, 47, 849–855. [Google Scholar] [CrossRef]
- Kawabata, M.; Miyata, T.; Tatsuki, H.; Naoi, D.; Ashihara, M.; Miyatake, K.; Kusaba, Y.; Watanabe, D.; Matsuzaki, M.; Suzuki, Y.; et al. Ultrasonographic prevalence of ulnar nerve displacement at the elbow in young baseball players. PMR 2022, 14, 955–962. [Google Scholar] [CrossRef]
- Konin, G.P.; Nazarian, L.N.; Walz, D.M. US of the elbow: Indications, technique, normal anatomy, and pathologic conditions. Radiographics 2013, 33, E125–E147. [Google Scholar] [CrossRef] [PubMed]
- Shen, P.C.; Chern, T.C.; Wu, K.C.; Tai, T.W.; Jou, I.M. The assessment of the ulnar nerve at the elbow by ultrasonography in children. J. Bone Joint. Surg. Br. 2008, 90, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Grechenig, W.; Mayr, J.; Peicha, G.; Boldin, C. Subluxation of the ulnar nerve in the elbow region--ultrasonographic evaluation. Acta Radiol. 2003, 44, 662–664. [Google Scholar]
- L’Heureux-Lebeau, B.; Odobescu, A.; Moser, T.; Harris, P.G.; Danino, M.A. Ulnar subluxation of the median nerve following carpal tunnel release: A case report. J. Plast. Reconstr. Aesthetic Surg. 2012, 65, e99–e101. [Google Scholar] [CrossRef] [PubMed]
- Filippou, G.; Mondelli, M.; Greco, G.; Bertoldi, I.; Frediani, B.; Galeazzi, M.; Giannini, F. Ulnar neuropathy at the elbow: How frequent is the idiopathic form? An ultrasonographic study in a cohort of patients. Clin. Exp. Rheumatol. 2010, 28, 63–67. [Google Scholar]
- Yen, Y.M.; Lewis, C.L.; Kim, Y.J. Understanding and Treating the Snapping Hip. Sports Med. Arthrosc. Rev. 2015, 23, 194–199. [Google Scholar] [CrossRef] [Green Version]
- Ooi, M.W.X.; Tham, J.L.; Al-Ani, Z. Role of dynamic ultrasound in assessment of the snapping elbow and distal biceps tendon injury. Ultrasound 2022, 30, 315–321. [Google Scholar] [CrossRef]
- Lee, K.S.; Rosas, H.G.; Phancao, J.P. Snapping hip: Imaging and treatment. Semin. Musculoskelet. Radiol. 2013, 17, 286–294. [Google Scholar]
- Janzen, D.L.; Partridge, E.; Logan, P.M.; Connell, D.G.; Duncan, C.P. The snapping hip: Clinical and imaging findings in transient subluxation of the iliopsoas tendon. Can. Assoc. Radiol. J. 1996, 47, 202–208. [Google Scholar] [PubMed]
- Blankenbaker, D.G.; Tuite, M.J. Iliopsoas musculotendinous unit. Semin. Musculoskelet. Radiol. 2008, 12, 13–27. [Google Scholar] [CrossRef]
- Shapiro, S.A.; Hernandez, L.O.; Montero, D.P. Snapping Pes Anserinus and the Diagnostic Utility of Dynamic Ultrasound. J. Clin. Imaging Sci. 2017, 7, 39. [Google Scholar] [CrossRef]
- Winston, P.; Awan, R.; Cassidy, J.D.; Bleakney, R.K. Clinical examination and ultrasound of self-reported snapping hip syndrome in elite ballet dancers. Am. J. Sports Med. 2007, 35, 118–126. [Google Scholar] [CrossRef]
- Chang, K.V.; Wu, W.T.; Özçakar, L. Ultrasound imaging and guided hydrodilatation for the diagnosis and treatment of internal snapping hip syndrome. Kaohsiung J. Med. Sci. 2019, 35, 582–583. [Google Scholar] [CrossRef]
- Nolton, E.C.; Ambegaonkar, J.P. Recognizing and Managing Snapping Hip Syndrome in Dancers. Med. Probl. Perform. Art. 2018, 33, 286–291. [Google Scholar] [CrossRef]
- Pesquer, L.; Guillo, S.; Poussange, N.; Pele, E.; Meyer, P.; Dallaudière, B. Dynamic ultrasound of peroneal tendon instability. Br. J. Radiol. 2016, 89, 20150958. [Google Scholar] [CrossRef] [PubMed]
- Lungu, E.; Michaud, J.; Bureau, N.J. US Assessment of Sports-related Hip Injuries. Radiographics 2018, 38, 867–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayhan, E.; Cevik, K. Triggering Thumb Is Not Always a Trigger Thumb. J. Hand. Surg. Glob. Online 2022, 4, 483–484. [Google Scholar] [CrossRef]
- Draghi, F.; Bortolotto, C.; Draghi, A.G.; Gitto, S. Intrasheath Instability of the Peroneal Tendons: Dynamic Ultrasound Imaging. J. Ultrasound Med. 2018, 37, 2753–2758. [Google Scholar] [CrossRef] [Green Version]
- Blankenbaker, D.G.; De Smet, A.A.; Keene, J.S. Sonography of the iliopsoas tendon and injection of the iliopsoas bursa for diagnosis and management of the painful snapping hip. Skeletal. Radiol. 2006, 35, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Erpala, F.; Ozturk, T. “Snapping” of the extensor carpi ulnaris tendon in asymptomatic population. BMC Musculoskelet. Disord. 2021, 22, 387. [Google Scholar] [CrossRef] [PubMed]
- Flanum, M.E.; Keene, J.S.; Blankenbaker, D.G.; Desmet, A.A. Arthroscopic treatment of the painful "internal" snapping hip: Results of a new endoscopic technique and imaging protocol. Am. J. Sports Med. 2007, 35, 770–779. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.S.; Cheng, Y.H.; Wu, C.H.; Özçakar, L. Dynamic ultrasound imaging for the iliotibial band/snapping hip syndrome. Am. J. Phys. Med. Rehabil. 2015, 94, e55–e56. [Google Scholar] [CrossRef]
- Piechota, M.; Maczuch, J.; Skupiński, J.; Kukawska-Sysio, K.; Wawrzynek, W. Internal snapping hip syndrome in dynamic ultrasonography. J. Ultrason. 2016, 16, 296–303. [Google Scholar] [CrossRef]
- Andronic, O.; Nakano, N.; Daivajna, S.; Board, T.N.; Khanduja, V. non-arthroplasty iliopsoas impingement in athletes: A narrative literature review. Hip. Int. 2019, 29, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Blankenbaker, D.G.; Tuite, M.J. The painful hip: New concepts. Skeletal. Radiol. 2006, 35, 352–370. [Google Scholar] [CrossRef] [PubMed]
- Asopa, V.; Douglas, R.J.; Heysen, J.; Martin, D. Diagnosing snapping sartorius tendon secondary to a meniscal cyst using dynamic ultrasound avoids incorrect surgical procedure. Case Rep. Radiol. 2013, 2013, 813232. [Google Scholar] [CrossRef] [Green Version]
- Fantino, O.; Borne, J.; Bordet, B. Conflicts, snapping and instability of the tendons. Pictorial essay. J. Ultrasound 2012, 15, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Lohrer, H.; Nauck, T. Posterior tibial tendon dislocation: A systematic review of the literature and presentation of a case. Br. J. Sports Med. 2010, 44, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, T.S.; Kuo, Y.J.; Chen, Y.P. Ultrasound-detected lateral band snapping syndrome in proximal interphalangeal joint of small finger-A rare case report. Int. J. Surg. Case Rep. 2019, 62, 73–76. [Google Scholar] [CrossRef]
- Greene, B.D.; Smith, S.E.; Smith, J.T. Snapping Plantaris Tendon: A Rare Case in a Competitive Dancer. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2021, 5, e21.00008. [Google Scholar] [CrossRef] [PubMed]
- Shukla, D.R.; Levy, B.A.; Kuzma, S.A.; Stuart, M.J. Snapping popliteus tendon within an osteochondritis dissecans lesion: An unusual case of lateral knee pain. Am. J. Orthop. 2014, 43, E210–E213. [Google Scholar] [PubMed]
- Tanaka, Y.; Gotani, H.; Yano, K.; Sasaki, K.; Miyashita, M.; Hamada, Y. Sonographic evaluation of effects of the volar plate on trigger finger. J. Orthop. Sci. 2015, 20, 999–1004. [Google Scholar] [CrossRef]
- Anderson, S.A.; Keene, J.S. Results of arthroscopic iliopsoas tendon release in competitive and recreational athletes. Am. J. Sports Med. 2008, 36, 2363–2371. [Google Scholar] [CrossRef]
- Deslandes, M.; Guillin, R.; Cardinal, E.; Hobden, R.; Bureau, N.J. The snapping iliopsoas tendon: New mechanisms using dynamic sonography. AJR Am. J. Roentgenol. 2008, 190, 576–581. [Google Scholar] [CrossRef]
- Raikin, S.M.; Elias, I.; Nazarian, L.N. Intrasheath subluxation of the peroneal tendons. J. Bone Joint Surg. Am. 2008, 90, 992–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacLennan, A.J.; Nemechek, N.M.; Waitayawinyu, T.; Trumble, T.E. Diagnosis and anatomic reconstruction of extensor carpi ulnaris subluxation. J. Hand. Surg. Am. 2008, 33, 59–64. [Google Scholar] [CrossRef]
- Pelsser, V.; Cardinal, E.; Hobden, R.; Aubin, B.; Lafortune, M. Extraarticular snapping hip: Sonographic findings. AJR Am. J. Roentgenol. 2001, 176, 67–73. [Google Scholar] [CrossRef]
- Cardinal, E.; Buckwalter, K.A.; Capello, W.N.; Duval, N. US of the snapping iliopsoas tendon. Radiology 1996, 198, 521–522. [Google Scholar] [CrossRef]
- De la Hera Cremades, B.; Escribano Rueda, L.; Lara Rubio, A. Snapping knee caused by the thickening of the medial hamstrings. Rev. Española De Cirugía Ortopédica Y Traumatol. 2017, 61, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Han, F.; Gartner, L.; Pearce, C.J. Snapping plantaris tendon: Case report. Foot Ankle Int. 2014, 35, 1358–1361. [Google Scholar] [CrossRef] [PubMed]
- Akagawa, M.; Kimura, Y.; Saito, H.; Kijima, H.; Saito, K.; Segawa, T.; Wakabayashi, I.; Kashiwagura, T.; Miyakoshi, N.; Shimada, Y. Snapping Pes Syndrome Caused by the Gracilis Tendon: Successful Selective Surgery with Specific Diagnosis by Ultrasonography. Case Rep. Orthop. 2020, 2020, 1783813. [Google Scholar] [CrossRef]
- Grandberg, C.; de Oliveira, D.P.; Gali, J.C. Superior peroneal retinaculum reattachment for an atraumatic peroneus brevis tendon subluxation: A case report. J. Med. Case Rep. 2022, 16, 239. [Google Scholar] [CrossRef]
- Smith, E.; Shrivastava, M.; Botchu, R. Snapping Sartorius tendon due to a medial knee ganglion: An unusual cause of medial knee pain. J. Ultrasound 2022, 25, 391–394. [Google Scholar] [CrossRef] [PubMed]
- Rainey, C.E.; Taysom, D.A.; Rosenthal, M.D. Snapping pes anserine syndrome. J. Orthop. Sports Phys. Ther. 2014, 44, 41. [Google Scholar] [CrossRef]
- Uemura, T.; Yano, K.; Miyashima, Y.; Konishi, S.; Nakamura, H. Posttraumatic triggering of the extensor pollicis brevis tendon in de Quervain’s disease successfully diagnosed with ultrasonography: A case report. J. Clin. Ultrasound 2021, 49, 398–400. [Google Scholar] [CrossRef]
- Hung, C.Y.; Chang, K.V.; Lam, S. Dynamic Sonography for Snapping Knee Syndrome Caused by the Gracilis Tendon. J. Ultrasound Med. 2018, 37, 803–804. [Google Scholar] [CrossRef] [Green Version]
- Karataglis, D.; Papadopoulos, P.; Fotiadou, A.; Christodoulou, A.G. Snapping knee syndrome in an athlete caused by the semitendinosus and gracilis tendons. A case report. Knee 2008, 15, 151–154. [Google Scholar] [CrossRef]
- Vidoni, A.; Shrivastava, M.; Botchu, R. Intrasynovial spindle cell lipoma of the deep flexor of the middle finger causing intermittent carpal tunnel syndrome-case report and review of the literature. J. Ultrasound 2020, 23, 419–423. [Google Scholar] [CrossRef]
- Guillin, R.; Mendoza-Ruiz, J.J.; Moser, T.; Ropars, M.; Duvauferrier, R.; Cardinal, E. Snapping biceps femoris tendon: A dynamic real-time sonographic evaluation. J. Clin. Ultrasound 2010, 38, 435–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Salazar, E.L.; Vicentini, J.R.T.; Johnson, A.H.; Torriani, M. Hallux saltans due to stenosing tenosynovitis of flexor hallucis longus: Dynamic sonography and arthroscopic findings. Skeletal. Radiol. 2018, 47, 747–750. [Google Scholar] [CrossRef] [PubMed]
- Fazekas, M.L.; Stracciolini, A. Snapping Pes Syndrome in a Pediatric Athlete. Curr. Sports Med. Rep. 2015, 14, 361–363. [Google Scholar] [CrossRef]
- Hashimoto, B.E.; Green, T.M.; Wiitala, L. Ultrasonographic diagnosis of hip snapping related to iliopsoas tendon. J. Ultrasound Med. 1997, 16, 433–435. [Google Scholar] [CrossRef] [PubMed]
- Stecco, C.; Pirri, C.; Fede, C.; Yucesoy; Can, A.; De Caro, R.; Stecco, A. Fascial or Muscle Stretching? A Narrative Review. Appl. Sci. 2021, 11, 307. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors and Year | Article Type | Participants | Sex | Age (y) | US Imaging | Maneuver/Movement | Nerve |
|---|---|---|---|---|---|---|---|
| Cambon-Binder, A. (2021) [7] | Review | - | - | - | B-mode | Elbow flexion/extension | Ulnar |
| Tsukada, K. et al. (2019) [8] | Retrospective study | 246 athletes | M | 19.5 ± 1.2 y. | B-mode | Elbow flexion/extension | Ulnar |
| Pisapia, J.M. et al. (2017) [9] | Case report | 1 | F | 15 y. | B-mode | Elbow flexion/extension | Ulnar |
| Lee, K.S. et al. (2010) [9] | Review | - | - | - | B-mode | - | Ulnar |
| Coraci, D. et al. (2017) [10] | Letter to editor | 1 | F | 41 y | B-mode, 18 MHz | 45° forearm flexion | Ulnar |
| Martinoli, C. et al. (1999) [11] | Review | - | - | - | B-mode | Elbow flexion/extension | Ulnar |
| Kakita, M. et al. (2012) [12] | Clinical trial | 38 | M | 50 ± 15 y. | B-mode | Elbow flexion/extension | Ulnar |
| Martinoli, C. et al. (2002) [13] | Review | - | - | - | B-mode | Elbow flexion/extension | Ulnar |
| Omejec, G. et al. (2016) [14] | Original article | 226 arms | M | 50 ± 14 y. | B-mode | Elbow flexion/extension | Ulnar |
| Endo, F. et al. (2021) [15] | Original article | 153 healthy participants | 44 M 112 F | 65.4 y. | B-mode | Maximal elbow flexion | Ulnar |
| Okamoto, M. et al. (2000) [16] | Original article | 100 heathy volunteers | 50 M 50 F | 20–69 y. | B-Mode, 7.5 MHz | Elbow flexion/extension | Ulnar |
| Cornelson, S.M. et al. (2019) [17] | Case reports | 42 | 25 M 17 F | 18–65 y. | B-Mode | Elbow in three different positions: extension, 45° flexion, and full flexion | Ulnar |
| Kang, S. et al. (2019) [18] | Original article | 65 | 65 M | 45 ± 14 y. | B-mode with 5–12 MHz linear array transducer | Elbow full extension to full flexion | Ulnar |
| Schertz, M. et al. (2017) [19] | Comparative study | 117 | 52 M 65 F | 47.3 y. | B-mode with linear probe 5–12 MHz | Starting from 90° flexion to complete flexion of the elbow | Ulnar |
| Grechenig, W. et al. (2003) [20] | Case reports | 2 | 2 M | 38 y. and 12 y. | B-mode | Elbow joint flexion | Ulnar |
| Kim, B.J. et al. (2008) [21] | Original article | 117 healthy volunteers | 52 M 65 F | 20–50 y. | B-mode with 7.5 to 12 MHz linear transducer. | At any angle during elbow flexion using real-time ultrasonography | Ulnar |
| Imao, K. et al. (2015) [22] | Case report | 1 | M | 43 y. | B-mode with | During elbow flexion more than 90° | Ulnar |
| Cesmebasi, A. et al. (2015) [23] | Case report | 4 | 1M 3 F | 18.5 y. | B-mode | Snapping over the medial epicondyle | Medial antebrachial cutaneous |
| Plaikner, M. et al. (2013) [24] | Retrospective study | 11 | 2 M 9 F | 28–82 y. | B-mode with linear probe L 17–5 MHz | During maximal extension and flexion of the elbow | Ulnar |
| Kim, B.J. et al. (2005) [25] | Original article | 39 | 19 M 20 F | 20–50 y. | B-Mod with linear probe 7.5 to 12MHz | Elbow extension and flexion | Ulnar |
| Yoo, M.J. et al. (2007) [26] | Case report | 1 | F | 50 y. | B-Mode with linear probe medium frequency of 10 MHz | At 70 degrees of elbow flexion; at 90 degrees elbow flexion | Ulnar |
| Shimizu, H. et al. (2011) [27] | Retrospective study | 8 | 4 F 4 M | 15–31 y. | B-Mode with linear probe medium frequency of 10 MHz | Elbow flexion/extension | Ulnar |
| Hatem, M. et al. (2020) [28] | Case report | 1 | F | 64 y. | B-Mode with curvilinear probe | Dislocation from the ischiofemoral space during hip mobilization from internal to external rotation | Sciatic |
| Reisner, J.H. et al. (2021) [29] | Case series | 2 | - | - | B-mode | - | Proper Digital of the Fifth Toe |
| Chuang, H.J. et al. (2016) [30] | Case report | 1 | M | 34 y. | B-mode | During active elbow flexion over 100 degrees | Ulnar |
| Kang, J.O. et al. (2017) [31] | Original article | 26 | 13 M 13 F | - | B-mode with 13-MHz high-frequency linear array transducer | Elbow in three different positions: extension, 90-degree flexion, and full flexion | Ulnar |
| Allen, G. et al. (2012) [32] | Review | - | - | - | B-mode | - | Ulnar |
| Bierre, J.J. et al. (2018) [33] | Case report | 2 | M | 16 y. | B-mode | Elbow flexion/extension | Ulnar |
| Chang, K.V. et al. (2017) [34] | Case report | 1 | F | 73 y. | B-mode | During extensor, pollicis brevis (EPB) tendon glided over the adjacent abductor pollicis longus (APL) tendon | Superficial Radial |
| Jacobson, J.A. et al. (2001) [35] | Case report | 3 | 3F | 17–52 y. | B-mode with 10-MHz linear transducer | Elbow flexion/extension | Ulnar |
| Yiannakopoulos, C.K. et al. (2002) [36] | Letter to editors | 2 | 1 F 1 M | 28–48 y. | B-mode | - | Ulna |
| Michael, A.E. et al. (2018) [37] | Cross-sectional study | 62 | 62 M | 18–60 y. | B-mode linear array transducer (15–7 MHz) | Cross-section image in elbow extension, 90-degree flexion, maximal flexion, and additionally in maximal flexion with isometric tension of the triceps | Ulnar |
| Erez, O. et al. (2012) [38] | Prospective study | 51 | - | 6 m.–18 y. | B-mode | Fully extended and flexed past 90 degrees | Ulnar |
| Granata, G. et al. (2013) [39] | Original article | 30 | 26 F 4 M | 15–58 y. | B-mode | Elbow flexion/extension | Ulnar |
| Tai, T.W. et al. (2014) [40] | Cross-sectional ultrasonographic study | 39 | M | 13 y. | B-mode with 5- to 10-MHz linear-array transducer | Elbow extended and at 45°, 90° and 120° of flexion | Ulnar |
| Van Den Berg, P.J. et al. (2013) [41] | Prospective study | 70 | 28 M 42 F | 19–79 y. | B-mode with a 7–18 MHz linear-array transducer | Patients were positioned supine, keeping the arm beside the head with the elbow flexed to 70 degrees | Ulnar |
| Kawabata, M. et al. (2022) [42] | Cross-sectional study. | 58 | 56 M 2 F | 10–12 | B-mode | Elbow flexion/extension | Ulnar |
| Konin, G.P. et al. (2013) [43] | Review | - | - | - | US B-mode with linear probe of 12–17 MHz | Elbow flexion/extension | Ulnar |
| Shen, P.C. et al. (2013) [44] | Original article | 237 | 108 F 129 M | 6–11 y. | B-mode with a 5 MHz to 10 MHz linear-array transducer | Elbow extended and at 45°, 90° and 120° of flexion | Ulnar |
| Grechenig, W. et al. (2003) [45] | Case report | 2 | M | 38 y. and 12 y. | B-mode | Elbow extension and flexion | Ulnar |
| L’Heureux-Lebeau, B. et al. (2012) [46] | Case report | 1 | M | 27 y. | B-mode | Subluxation of the median nerve from one side of the PL tendon during wrist flexion | Median |
| Filippou, G. et al. (2010) [47] | Original article | 91 | 49 M 42 F | 15–81 y. | B-mode | Elbow flexion/extension | Ulnar |
| Authors and Year | Type of Paper | Participants | Sex | Age (y) | US Imaging | Maneuver/Movement | Tendon |
|---|---|---|---|---|---|---|---|
| Yen, Y.M. et al. (2015) [48] | Review | - | - | - | B-mode | - | Iliopsoas |
| Ooi, M.W.X. et al. (2022) [49] | Original article | - | - | - | B-mode | Elbow flexion and extension | Distal biceps and brachialis |
| Lee, K.S. et al. (2013) [50] | Review | - | - | - | B-mode with linear probe 5–12 MHz. | During hip flexion, external rotation, and abduction | Iliopsoas, iliotibial band and gluteus maximus |
| Janzen, D.L. et al. (1996) [51] | Original article | 7 | - | 17–30 y. | B-mode linear probe 5–12 MHz | During hip flexion, external rotation, and abduction | Iliopsoas |
| Blankenbaker, D.G. et al. (2008) [52] | Review | - | - | - | B-mode | During hip flexion, external rotation, and abduction | Iliopsoas |
| Shapiro, S.A. et al. (2017) [53] | Case report | 2 | 1 M 1 F | 31 y. and 72 y. | B-mode | Repetitive flexion and extension of knee | Gracilis and semitendinosus |
| Winston, P. et al. (2007) [54] | Cross-sectional study | 87 | 30 M 57 F | 15 to 40 y. | B-mode | The subjects voluntarily reproduced the snap while the hips were scanned | Iliopsoas |
| Chang, K.V. et al. (2019) [55] | Case report | 1 | M | 42 y. | B-mode | Return from hip flexed and abducted in neutral position; during hip flexion and extension | Iliopsoas |
| Nolton, E.C. et al. (2018) [56] | Review | - | - | B-mode | During hip flexion and extension | Iliopsoas | |
| Pesquer, L. et al. (2016) [57] | Review | - | - | - | B-mode with high-frequency superficial probes | At different levels of motion in dorsi-flexion, also forced dorsi-flexion | Peroneal |
| Lungu, E. et al. (2018) [58] | Review | - | - | - | B-mode | During hip flexion and extension | Iliopsoas |
| Ayhan, E. et al. (2022) [59] | Case report | 1 | F | 18 y. | B-mode with linear probe L14-6 10-MHz | Finger flexion/extension | Extensor pollicis brevis |
| Draghi, F. et al. (2018) [60] | Review | - | - | - | B-mode with high-frequency | Dorsiflexion | Peroneal |
| Blankenbaker, D.G. et al. (2006) [61] | Retrospective study | 40 | 15 M 25 F | 15–72 y. | B-mode 7–4 MHz; 8–4 MHz, 10 MHz | During hip flexion and extension | Iliopsoas |
| Allen, G. et al. (2012) [32] | Review | - | - | - | B-mode | - | Rotator cuff, proximal long biceps, distal biceps, rotator cuff, the proximal long head of biceps, the distal biceps, the distal triceps, the flexor and extensor around the elbow and wrist, and the individual within the hand |
| Erpala, F. et al. (2021) [62] | Prospective randomized study | 775 | 340 M 415 F | 18–66 y. | B-mode | Participants were positioned on examination chair with wrist at flexion and forearm at supination (simulating provocation test) | Extensor Carpi ulnaris |
| Flanum, M.E. et al. (2007) [63] | Case series | 6 | 1 M 5 F | 24–48 y. | B-mode | During flexion/extension | Iliopsoas |
| Chang, K.S. et al. (2015) [64] | Case report | 1 | M | 34 y. | B-mode | Snapping of the ITB over the GT during hip flexion and extension | Iliotibial band |
| Chang, K.V. et al. (2015) [34] | Case report | 1 | F | 73 y. | B-mode | During extensor, pollicis brevis (EPB) tendon glided over the adjacent abductor pollicis longus (APL) tendon | Extensor pollicis brevis |
| Piechota, M. et al. (2016) [65] | Review | - | - | - | B-mode | Provocation test | Iliopsoas |
| Andronic, O. et al. (2019) [66] | Review | - | - | - | B-mode | FABER position, the tendon can be seen snapping over the iliopectineal eminence | Iliopsoas |
| Blankenbaker, D.G. et al. (2006) [67] | Review | - | - | - | B-mode 5–12 MHz | During flexion | Iliopsoas |
| Asopa, V. et al. (2013) [68] | Case report | 1 | M | 40 y. | B-mode | Knee flexion/extension | Sartorius |
| Marchand, A.J. et al. (2012) [1] | Review | - | - | - | B-mode | Knee flexion/extension | Biceps and popliteus |
| Fantino, O. et al. (2012) [69] | Review | - | - | - | B-mode | Specific tests | Posterior tibialis, peroneal; extensor carpi ulnaris, long head of the biceps muscle |
| Lohrer, H. et al. (2010) [70] | Review + case report | 1 | M | 58 y. | B-mode | Dislocated posterior tibial tendon over the right malleolus during flexion/extension | Posterior tibialis |
| Hsieh, T.S. et al. (2019) [71] | Case report | 1 | F | 43 y. | B-mode | During flexion/extension of PIP joint | Extensor digitorum |
| Greene, B.D. et al. (2021) [72] | Case report | 1 | F | 15 y. | B-mode | Plantar/dorsal flexion | Plantaris |
| Shukla, D.R. et al. (2014) [73] | Review | - | - | - | B-mode | During flexion/extension | Popliteus |
| Tanaka, Y. et al. (2015) [74] | Comparative study | 24 | 11 M 13 F | 26–74 y. | B-mode | During finger flexion/extension | Flexor digitorum |
| Anderson, S.A. et al. (2008) [75] | Case series | 15 | 4 M 11 F | 15–62 y. | B-mode | During hip flexion/extension | Iliopsoas |
| Deslandes, M. et al. (2008) [76] | Review and case series | 14 | 5 M 9 F | 13–50 y. | B-mode with 5–12 MHz | During hip flexion/extension | Iliopsoas |
| Raikin, S.M. et al. (2008) [77] | Original article | 57 | 15 M 42 F | - | B-mode | Ankle eversion/inversion | Peroneal |
| MacLennan, A.J. et al. (2008) [78] | Original article | 21 | 14 M 7 F | 14–44 y. | B-mode | Wrist flexion/extension | Extensor carpi ulnaris |
| Pelsser, V. et al. (2001) [79] | Original article | 20 | 3 M 17 F | 12–39 y. | B-mode with curvilinear probe | During hip flexion/extension | Iliopsoas |
| Cardinal, E. et al. (1996) [80] | Case reports | 3 | 1 M 2 F | 24–36 y. | B-mode | During hip flexion/extension | Iliopsoas |
| de la Hera Cremades, B. et al. (2017) [81] | Case report | 1 | F | 23 y. | B-mode | During hip flexion/extension | Iliopsoas |
| Han, F. et al. (2014) [82] | Case report | 1 | M | 30 y. | B-mode | During ankle plantar/dorsal flexion | Plantaris |
| Akagawa, M. et al. (2020) [83] | Case report | 1 | M | 26 y. | B-mode | During knee flexion/extension | Gracilis |
| Grandberg, C. et al. (2022) [84] | Case report | 1 | F | 25 y. | B-mode | Ankle eversion/inversion | Peroneals |
| Smith, E. et al. (2022) [85] | Case report | 1 | F | 70 y. | B-mode | Knee flexion/extension | Sartorius |
| Rainey, C.E. et al. (2015) [86] | Case report | 1 | M | 25 y. | B-mode | Knee flexion/extension | Pes anserinus |
| Uemura, T. et al. (2021) [87] | Case report | 1 | M | 52 y. | B-mode | Finger flexion/extension | Extensor pollicis brevis |
| Hung, C.Y. et al. (2018) [88] | Case report | 1 | M | 39 y. | B-mode | Knee flexion/extension | Gracilis |
| Karataglis, D. et al. (2008) [89] | Case report | 1 | M | 32 y. | B-mode | Knee flexion/extension | Semitendinosus and gracilis |
| Vidoni, A. et al. (2020) [90] | Case report | 1 | M | 26 y. | B-mode | Finger flexion/extension | Deep flexor digiti |
| Guillin, R. et al. (2010) [91] | Case report | 2 | 2 M | 25–44 y. | B-mode | Knee flexion/extension | Biceps femoris |
| Martinez-Salazar, E.L.et al. (2018) [92] | Case report | 1 | F | 42 y. | B-mode | Hallux flexion/extension | Flexor hallucis longus |
| Fazekas, M.L. et al. (2015) [93] | Case report | 1 | M | 14 y. | B-mode | Knee flexion/extension | Semitendinosus and gracilis |
| Hashimoto, B.E. et al. (1997) [94] | Case report | 1 | F | 14 y. | B-mode | During hip flexion/extension | Iliopsoas |
| Nerve | Tendon |
|---|---|
| Ulnar Medial antebrachial cutaneous Sciatic Proper digital (5th toe) Median | Iliopsoas Distal triceps brachii Iliotibial Peroneal Biceps femoris Semitendinosus and gracilis Sartorius Posterior tibialis Extensor pollicis brevis Extensor carpi ulnaris Proximal long biceps brachii Distal long biceps brachii Rotator cuff Deep flexor digiti tendon |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pirri, C.; Pirri, N.; Stecco, C.; Macchi, V.; Porzionato, A.; De Caro, R.; Özçakar, L. Hearing and Seeing Nerve/Tendon Snapping: A Systematic Review on Dynamic Ultrasound Examination. Sensors 2023, 23, 6732. https://doi.org/10.3390/s23156732
Pirri C, Pirri N, Stecco C, Macchi V, Porzionato A, De Caro R, Özçakar L. Hearing and Seeing Nerve/Tendon Snapping: A Systematic Review on Dynamic Ultrasound Examination. Sensors. 2023; 23(15):6732. https://doi.org/10.3390/s23156732
Chicago/Turabian StylePirri, Carmelo, Nina Pirri, Carla Stecco, Veronica Macchi, Andrea Porzionato, Raffaele De Caro, and Levent Özçakar. 2023. "Hearing and Seeing Nerve/Tendon Snapping: A Systematic Review on Dynamic Ultrasound Examination" Sensors 23, no. 15: 6732. https://doi.org/10.3390/s23156732