
Design and Evaluation of a Potential Non-Invasive Neurostimulation Strategy for Treating Persistent Anosmia in Post-COVID-19 Patients
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
- Inclusion criteria: (1) patients who suffered loss of smell after infection by SARS-COV-2 (confirmed through positive PCR); (2) age between 18 and 55 years old; and (3) normal examination without clinic or exploratory data that hint at neurodegenerative diseases.
- Exclusion criteria: (1) fluctuating or paroxysmal loss of smell; (2) smoking; (3) use of drugs that could affect the sense of smell; (4) history in first-degree relatives of neurodegenerative diseases; (5) diseases that could affect the sense of smell; (6) pregnancy; and (7) use of an artificial pacemaker.
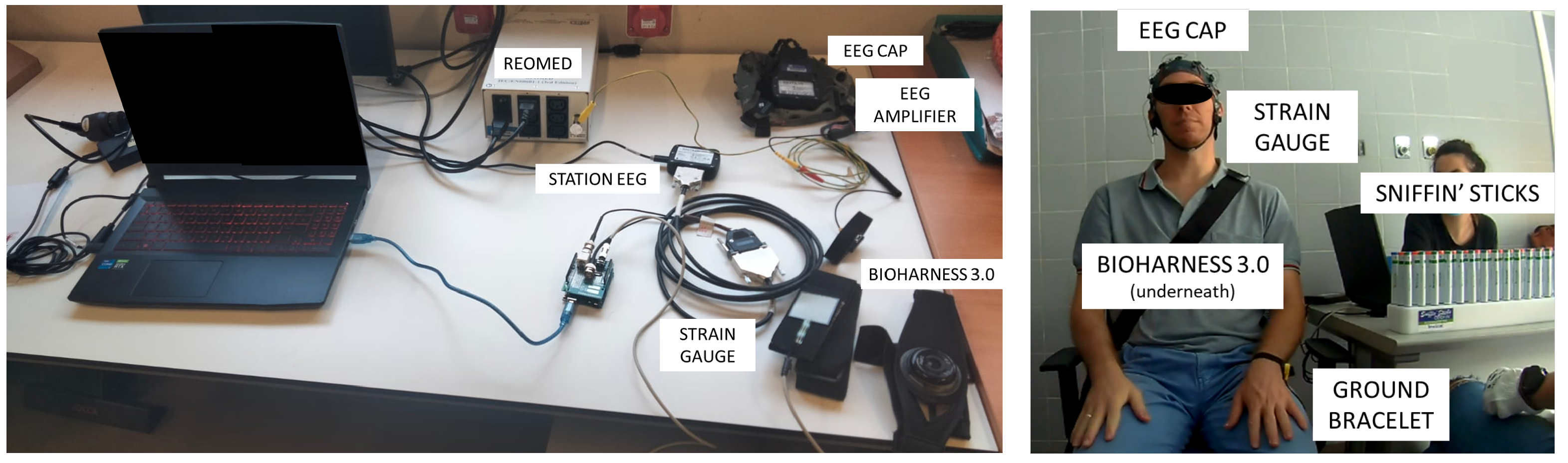
2.2. Devices
- A threshold test conducted with 48 Sniffin’ Sticks (32 blanks and 16 dilutions of 2-phenylethanol with different concentrations. Stick number 16 was the one with the lowest fragrance concentration, and stick number 1 had the highest concentration).
- A discrimination test conducted with 48 Sniffin’ Sticks (16 triplets, in which each one has two sticks with the same odor, while the other one is a different scent and is thus the target).
- An identification test conducted with 16 Sniffin’ Sticks (with different everyday smells).
2.3. Procedure
2.3.1. Initial Olfactory Test
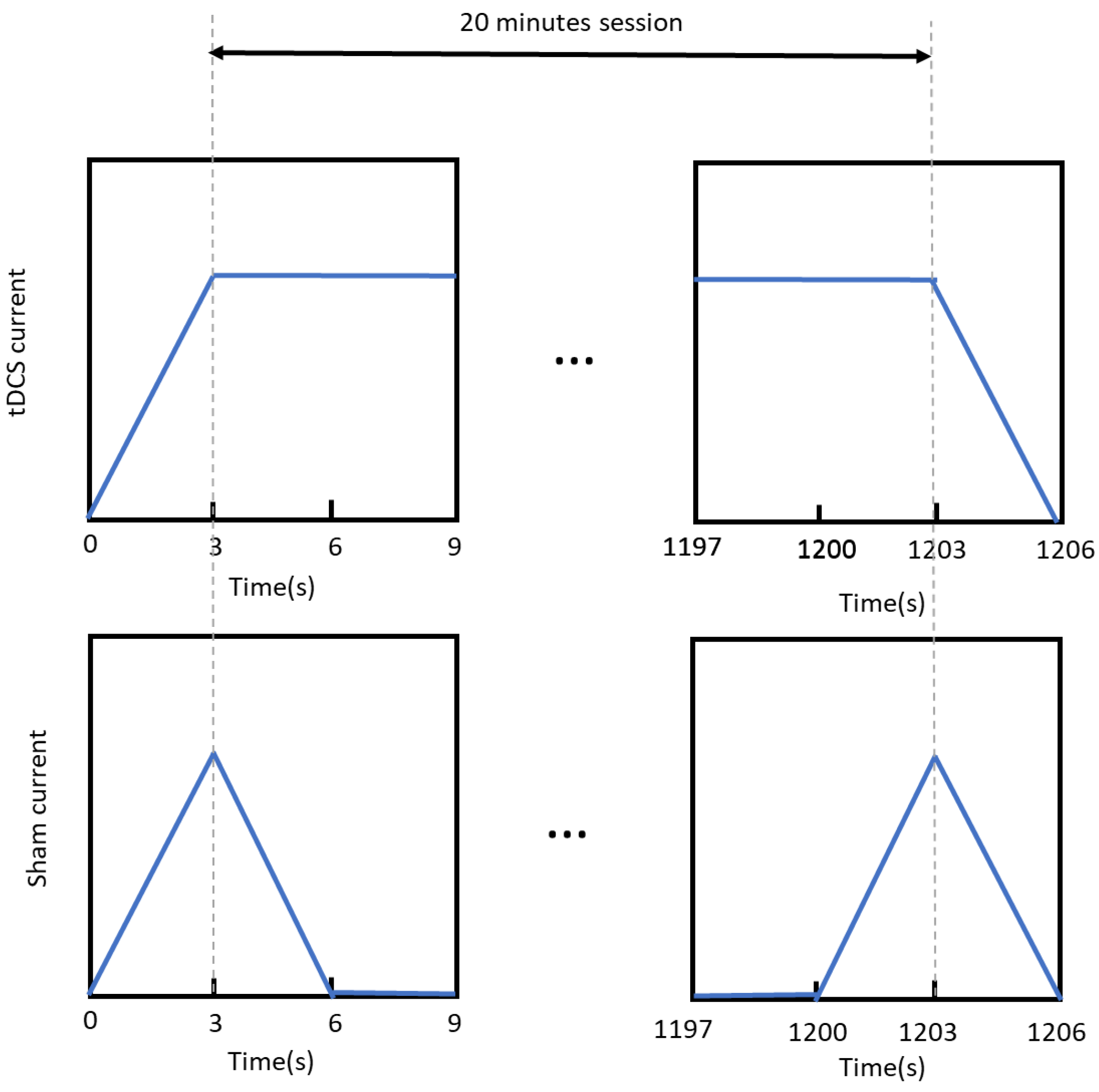
2.3.2. Stimulation Sessions
2.3.3. Final Olfactory Test
2.4. Data Analysis
2.4.1. Initial Olfactory Assessment
2.4.2. Final Olfactory Assessment
2.4.3. EEG Data
2.4.4. Stimulation
3. Results
3.1. Initial Olfactory Assessment
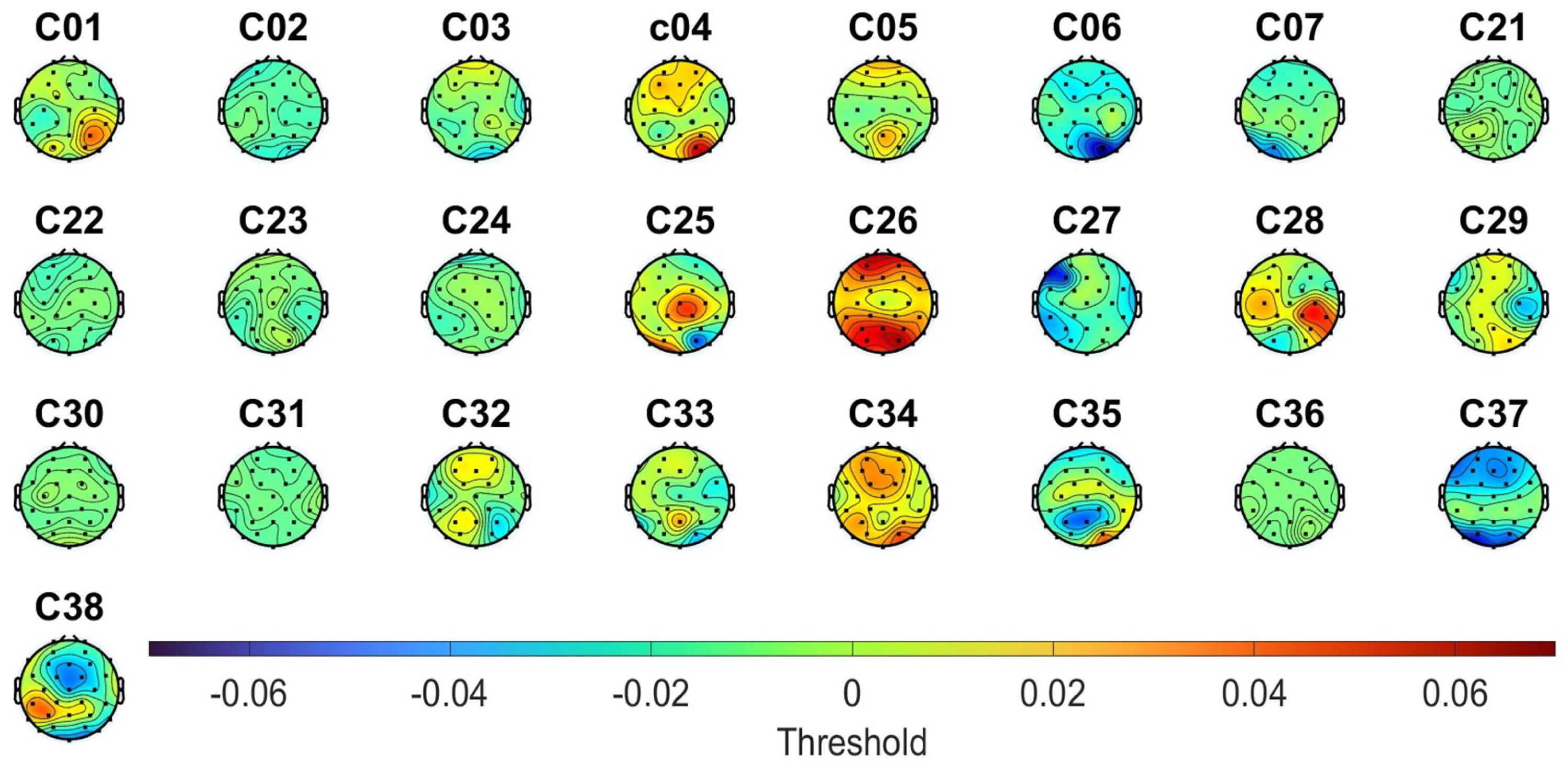
3.2. EEG Data from Initial Olfactory Assessment
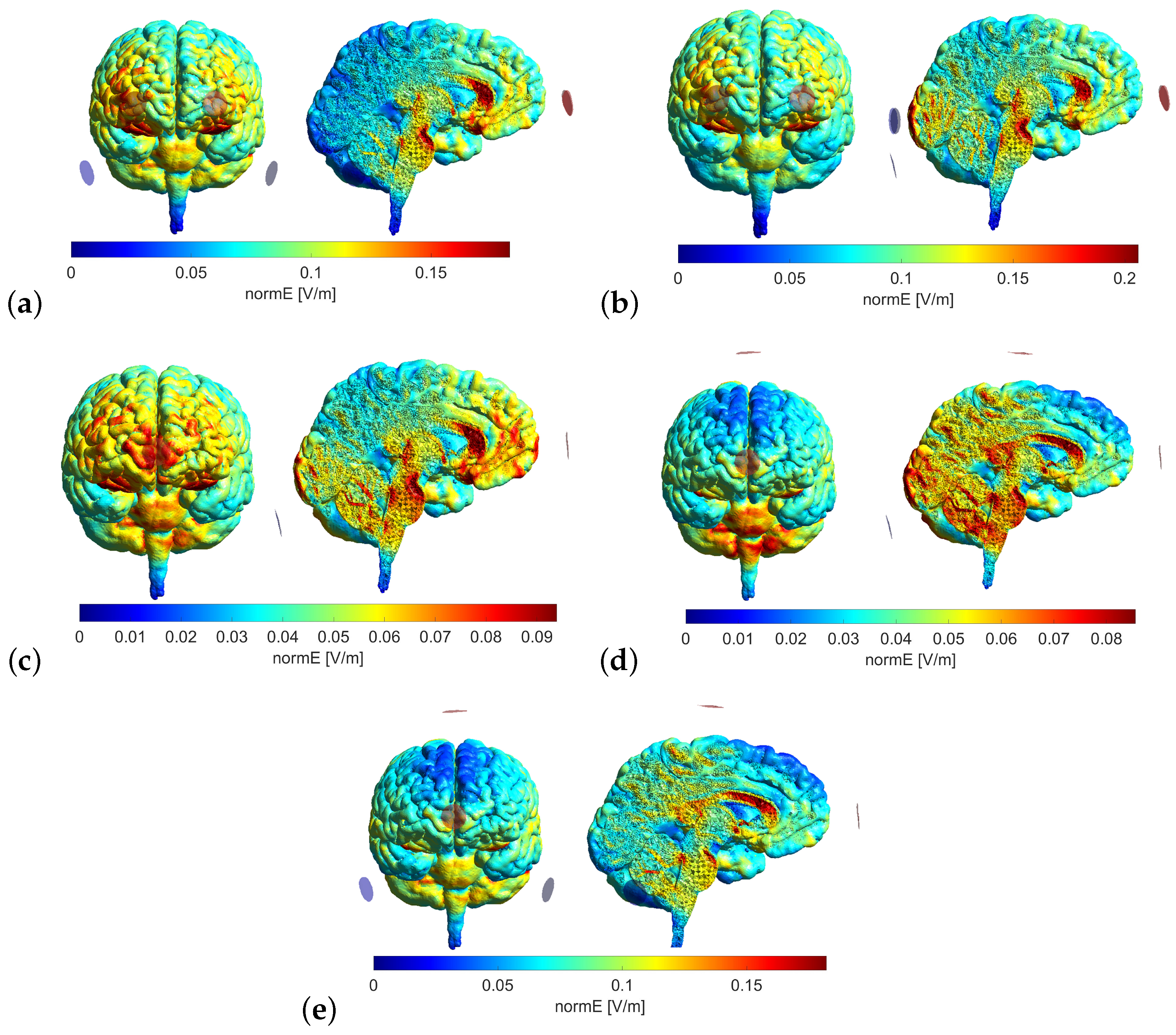
3.3. Stimulation
- Model 1: Anode electrodes, FP1 and FP2; cathode electrodes, P9 and P10.
- Model 2: Anode electrodes, FP1 and FP2; cathode electrodes, O1, O2, and IZ.
- Model 3: Anode electrodes, FPZ; cathode electrodes, IZ.
- Model 4: Anode electrodes, FPZ and CZ; cathode electrodes, IZ.
- Model 5: Anode electrodes, FPZ and CZ; cathode electrodes, P9 and P10.
3.4. Final Olfactory Assessment
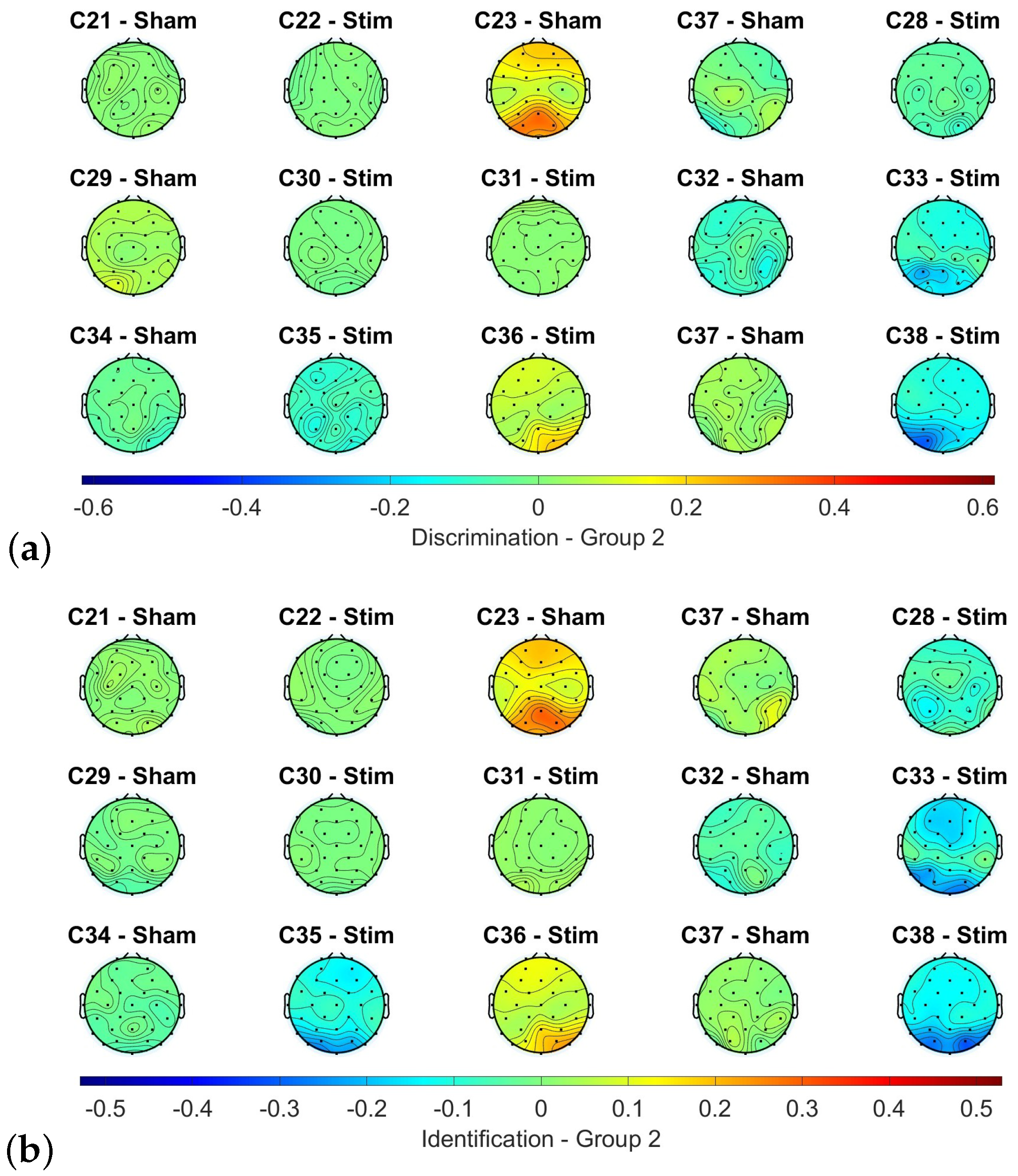
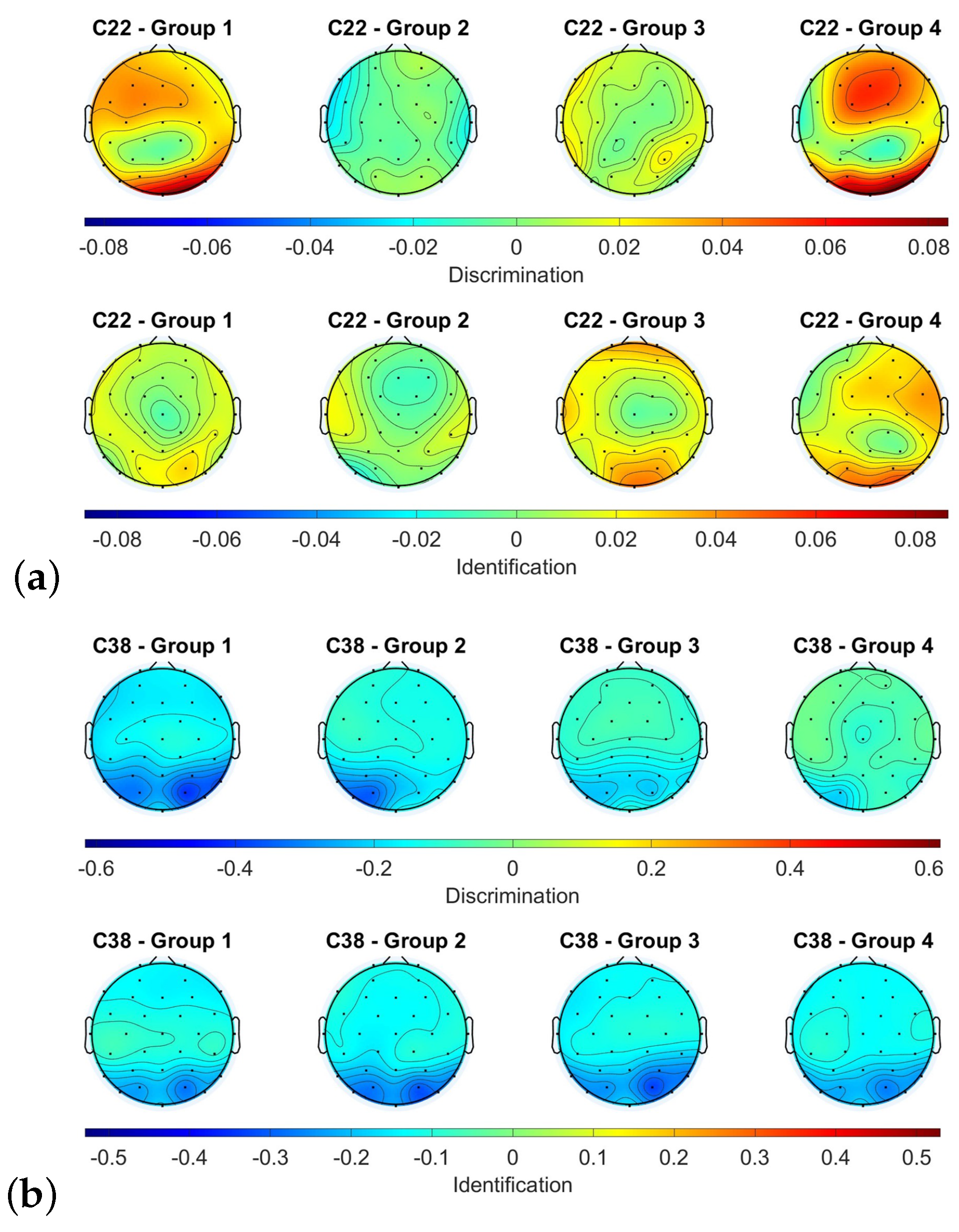
3.5. EEG Data from Final Olfactory Assessment
4. Discussion
4.1. Olfactory Assessments
4.2. EEG Data
4.3. Stimulation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Sample Availability
References
- Vellieux, G.; Sonneville, R.; Vledouts, S.; Jaquet, P.; Rouvel-Tallec, A.; D’Ortho, M.P. COVID-19-Associated Neurological Manifestations: An Emerging Electroencephalographic Literature. Front. Physiol. 2021, 11, 622466. [Google Scholar] [CrossRef] [PubMed]
- Galanopoulou, A.S.; Ferastraoaru, V.; Correa, D.J.; Cherian, K.; Duberstein, S.; Gursky, J.; Hanumanthu, R.; Hung, C.; Molinero, I.; Khodakivska, O.; et al. EEG findings in acutely ill patients investigated for SARS-CoV-2/COVID-19: A small case series preliminary report. Epilepsia Open 2020, 5, 314–324. [Google Scholar] [CrossRef]
- Agyeman, A.A.; Chin, K.L.; Landersdorfer, C.B.; Liew, D.; Ofori-Asenso, R. Smell and Taste Dysfunction in Patients with COVID-19: A Systematic Review and Meta-analysis. Mayo Clin. Proc. 2020, 95, 1621–1631. [Google Scholar] [CrossRef] [PubMed]
- Coelho, D.H.; Reiter, E.R.; French, E.; Costanzo, R.M. Decreasing Incidence of Chemosensory Changes by COVID-19 Variant. Otolaryngol. Neck Surg. 2022, 168, 704–706. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.K.J.; Han, R.; Zhao, J.J.; Tan, N.K.W.; Quah, E.S.H.; Tan, C.J.W.; Chan, Y.H.; Teo, N.W.Y.; Charn, T.C.; See, A.; et al. Prognosis and persistence of smell and taste dysfunction in patients with covid-19: Meta-analysis with parametric cure modelling of recovery curves. BMJ 2022, 378, e069503. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; Beckers, E.; Mustin, V.; Ducarme, M.; Journe, F.; Marchant, A.; Jouffe, L.; Barillari, M.R.; Cammaroto, G.; et al. Prevalence and 6-month recovery of olfactory dysfunction: A multicentre study of 1363 COVID-19 patients. J. Intern. Med. 2021, 290, 451–461. [Google Scholar] [CrossRef]
- Cho, R.H.; To, Z.W.; Yeung, Z.W.; Tso, E.Y.; Fung, K.S.; Chau, S.K.; Leung, E.Y.; Hui, T.S.; Tsang, S.W.; Kung, K.N.; et al. COVID-19 Viral Load in the Severity of and Recovery From Olfactory and Gustatory Dysfunction. Laryngoscope 2020, 130, 2680–2685. [Google Scholar] [CrossRef]
- Aragão, M.F.; Leal, M.C.; Cartaxo Filho, O.Q.; Fonseca, T.M.; Valença, M.M. Anosmia in COVID-19 associated with injury to the olfactory bulbs evident on MRI. Am. J. Neuroradiol. 2020, 41, 1703–1706. [Google Scholar] [CrossRef]
- Eliezer, M.; Hamel, A.L.; Houdart, E.; Herman, P.; Housset, J.; Jourdaine, C.; Eloit, C.; Verillaud, B.; Hautefort, C. Loss of smell in patients with COVID-19: MRI data reveal a transient edema of the olfactory clefts. Neurology 2020, 95, e3145–e3152. [Google Scholar] [CrossRef] [PubMed]
- Laurendon, T.; Radulesco, T.; Mugnier, J.; Gérault, M.; Chagnaud, C.; El Ahmadi, A.A.; Varoquaux, A. Bilateral transient olfactory bulb edema during COVID-19-related anosmia. Neurology 2020, 95, 224–225. [Google Scholar] [CrossRef]
- Meinhardt, J.; Radke, J.; Dittmayer, C.; Franz, J.; Thomas, C.; Mothes, R.; Laue, M.; Schneider, J.; Brünink, S.; Greuel, S.; et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat. Neurosci. 2021, 24, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Moein, S.T.; Hashemian, S.M.R.; Tabarsi, P.; Doty, R.L. Prevalence and reversibility of smell dysfunction measured psychophysically in a cohort of COVID-19 patients. Int. Forum Allergy Rhinol. 2020, 10, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, C.; Surda, P.; Whitehead, E.; Kumar, B.N. Early recovery following new onset anosmia during the COVID-19 pandemic—An observational cohort study. J. Otolaryngol.-Head Neck Surg. 2020, 49, 26. [Google Scholar] [CrossRef] [PubMed]
- Renaud, M.; Thibault, C.; Le Normand, F.; McDonald, E.G.; Gallix, B.; Debry, C.; Venkatasamy, A. Clinical Outcomes for Patients with Anosmia 1 Year after COVID-19 Diagnosis. JAMA Netw. Open 2021, 4, e2115352. [Google Scholar] [CrossRef] [PubMed]
- McWilliams, M.P.; Coelho, D.H.; Reiter, E.R.; Costanzo, R.M. Recovery from Covid-19 smell loss: Two-years of follow up. Am. J. Otolaryngol. 2022, 43, 103607. [Google Scholar] [CrossRef]
- Mullol, J.; Alobid, I.; Mariño-Sánchez, F.; Quintó, L.; de Haro, J.; Bernal-Sprekelsen, M.; Valero, A.; Picado, C.; Marin, C. Furthering the understanding of olfaction, prevalence of loss of smell and risk factors: A population-based survey (OLFACAT study). BMJ Open 2012, 2, e001256. [Google Scholar] [CrossRef] [Green Version]
- Boesveldt, S.; Postma, E.M.; Boak, D.; Welge-Luessen, A.; Schöpf, V.; Mainland, J.D.; Martens, J.; Ngai, J.; Duffy, V.B. Anosmia—A clinical review. Chem. Sci. 2017, 42, 513–523. [Google Scholar] [CrossRef] [Green Version]
- Khurana, K.; Singh, C.V. Management of Anosmia in COVID-19: A Comprehensive Review. Cureus 2022, 14, e30425. [Google Scholar] [CrossRef]
- Scaturro, D.; Vitagliani, F.; Di Bella, V.E.; Falco, V.; Tomasello, S.; Lauricella, L.; Letizia Mauro, G. The Role of Acetyl-Carnitine and Rehabilitation in the Management of Patients with Post-COVID Syndrome: Case-Control Study. Appl. Sci. 2022, 12, 4084. [Google Scholar] [CrossRef]
- Deems, D.A.; Doty, R.L.; Settle, R.G.; Moore-Gillon, V.; Shaman, P.; Mester, A.F.; Kimmelman, C.P.; Brightman, V.J.; Snow, J.B., Jr. Smell and Taste Disorders, A Study of 750 Patients From the University of Pennsylvania Smell and Taste Center. Arch.-Otolaryngol. Head Neck Surg. 1991, 117, 519–528. [Google Scholar] [CrossRef]
- Douaud, G.; Lee, S.; Alfaro-Almagro, F.; Arthofer, C.; Wang, C.; McCarthy, P.; Lange, F.; Andersson, J.L.; Griffanti, L.; Duff, E.; et al. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature 2022, 604, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Bhatia-Dey, N.; Heinbockel, T. The Olfactory System as Marker of Neurodegeneration in Aging, Neurological and Neuropsychiatric Disorders. Int. J. Environ. Res. Public Health 2021, 18, 6976. [Google Scholar] [CrossRef] [PubMed]
- Straschill, M.; Stahl, H.; Gorkisch, K. Effects of electrical stimulation of the human olfactory mucosa. Appl. Neurophysiol. 1983, 46, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Cakmak, Y.O.; Nazim, K.; Thomas, C.; Datta, A. Optimized Electrode Placements for Non-invasive Electrical Stimulation of the Olfactory Bulb and Olfactory Mucosa. Front. Neurosci. 2020, 14, 581503. [Google Scholar] [CrossRef]
- Brooks, J.; Teng, S.Y.; Wen, J.; Nith, R.; Nishida, J.; Lopes, P. Stereo-Smell via Electrical Trigeminal Stimulation. In Proceedings of the 2021 CHI Conference on Human Factors in Computing Systems, New York, NY, USA, 8–13 May 2021. [Google Scholar] [CrossRef]
- Chen, H.; Huo, D.; Zhang, J. Gas Recognition in E-Nose System: A Review. IEEE Trans. Biomed. Circuits Syst. 2022, 16, 169–184. [Google Scholar] [CrossRef]
- Holbrook, E.H.; Puram, S.V.; See, R.B.; Tripp, A.G.; Nair, D.G. Induction of smell through transethmoid electrical stimulation of the olfactory bulb. Int. Forum Allergy Rhinol. 2019, 9, 158–164. [Google Scholar] [CrossRef]
- Lefaucheur, J.P.; Antal, A.; Ayache, S.S.; Benninger, D.H.; Brunelin, J.; Cogiamanian, F.; Cotelli, M.; De Ridder, D.; Ferrucci, R.; Langguth, B.; et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin. Neurophysiol. 2017, 128, 56–92. [Google Scholar] [CrossRef]
- Mondino, M.; Bennabi, D.; Poulet, E.; Galvao, F.; Brunelin, J.; Haffen, E. Can transcranial direct current stimulation (tDCS) alleviate symptoms and improve cognition in psychiatric disorders? World J. Biol. Psychiatry 2014, 15, 261–275. [Google Scholar] [CrossRef]
- Kuo, M.F.; Paulus, W.; Nitsche, M.A. Therapeutic effects of non-invasive brain stimulation with direct currents (tDCS) in neuropsychiatric diseases. NeuroImage 2014, 85, 948–960. [Google Scholar] [CrossRef]
- Azabou, E.; Bao, G.; Heming, N.; Bounab, R.; Moine, P.; Chevallier, S.; Chevret, S.; Resche-Rigon, M.; Siami, S.; Sharshar, T.; et al. Randomized Controlled Study Evaluating Efficiency of Low Intensity Transcranial Direct Current Stimulation (tDCS) for Dyspnea Relief in Mechanically Ventilated COVID-19 Patients in ICU: The tDCS-DYSP-COVID Protocol. Front. Med. 2020, 7, 372. [Google Scholar] [CrossRef]
- Silva-Filho, E.; Moura, S.; Santos, A.; Brasileiro-Santos, M.; Albuquerque, J. Transcranial direct current stimulation as a strategy to manage COVID-19 pain and fatigue. Rev. Assoc. Méd. Bras. 2021, 67, 26–28. [Google Scholar] [CrossRef] [PubMed]
- Castelo-Branco, L.; Fregni, F. Home-Based Transcranial Direct Current Stimulation (tDCS) to Prevent and Treat Symptoms Related to Stress: A Potential Tool to Remediate the Behavioral Consequences of the COVID-19 Isolation Measures? Front. Integr. Neurosci. 2020, 14, 46. [Google Scholar] [CrossRef]
- Rumeau, C.; Nguyen, D.T.; Jankowski, R. How to assess olfactory performance with the Sniffin’ Sticks test. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2016, 133, 203–206. [Google Scholar] [CrossRef]
- Eluecque, H.; Nguyen, D.T.; Jankowski, R. Influence of random answers on interpretation of the Sniffing Stick identification test in nasal polyposis. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2015, 132, 13–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oleszkiewicz, A.; Schriever, V.A.; Croy, I.; Hähner, A.; Hummel, T. Updated Sniffin’ Sticks normative data based on an extended sample of 9139 subjects. Eur. Arch. Otorhinolaryngol. 2019, 276, 719–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iravani, B.; Arshamian, A.; Ohla, K.; Wilson, D.A.; Lundström, J.N. Non-invasive recording from the human olfactory bulb. Nat. Commun. 2020, 648. [Google Scholar] [CrossRef] [Green Version]
- Ishimaru, T.; Shimada, T.; Sakumoto, M.; Miwa, T.; Kimura, Y.; Furukawa, M. Olfactory Evoked Potential Produced by Electrical Stimulation of the Human Olfactory Mucosa. Chem. Senses 1997, 22, 77–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seta, N.; Koizuka, I.; Takemoto, I.; Matsunaga, T.; Tonoike, M. A Test Of Olfactory Evoked Potentials Using Odor Stimulation. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Orlando, FL, USA, 31 October–3 November 1991; Volume 13, pp. 541–542. [Google Scholar] [CrossRef]
- Guo, Y.; Wu, D.; Sun, Z.; Yao, L.; Liu, J.; Wei, Y. Prognostic value of olfactory evoked potentials in patients with post-infectious olfactory dysfunction. Eur. Arch.-Oto-Rhino-Laryngol. 2021, 278, 3839–3846. [Google Scholar] [CrossRef]
- James Evans, W.; Cui, L.; Starr, A. Olfactory event-related potentials in normal human subjects: Effects of age and gender. Electroencephalogr. Clin. Neurophysiol. 1995, 95, 293–301. [Google Scholar] [CrossRef] [Green Version]
- Evans, W.; Starr, A. Stimulus parameters and temporal evolution of the olfactory evoked potential in rats. Chem. Senses 1992, 17, 61–77. [Google Scholar] [CrossRef]
- Arpaia, P.; Cataldo, A.; Criscuolo, S.; De Benedetto, E.; Masciullo, A.; Schiavoni, R. Assessment and Scientific Progresses in the Analysis of Olfactory Evoked Potentials. Bioengineering 2022, 9, 252. [Google Scholar] [CrossRef] [PubMed]
- Caminiti, F.; De Salvo, S.; De Cola, M.C.; Russo, M.; Bramanti, P.; Marino, S.; Ciurleo, R. Detection of Olfactory Dysfunction Using Olfactory Event Related Potentials in Young Patients with Multiple Sclerosis. PLoS ONE 2014, 9, e103151. [Google Scholar] [CrossRef] [Green Version]
- Thielscher, A.; Antunes, A.; Saturnino, G.B. Field modeling for transcranial magnetic stimulation: A useful tool to understand the physiological effects of TMS? In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 222–225. [Google Scholar] [CrossRef]
- Foerster, Á.S.; Rezaee, Z.; Paulus, W.; Nitsche, M.A.; Dutta, A. Effects of Cathode Location and the Size of Anode on Anodal Transcranial Direct Current Stimulation Over the Leg Motor Area in Healthy Humans. Front. Neurosci. 2018, 12, 443. [Google Scholar] [CrossRef]
- Bikson, M.; Grossman, P.; Thomas, C.; Zannou, A.L.; Jiang, J.; Adnan, T.; Mourdoukoutas, A.P.; Kronberg, G.; Truong, D.; Boggio, P.; et al. Safety of Transcranial Direct Current Stimulation: Evidence Based Update 2016. Brain Stimul. 2016, 9, 641–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landis, B.; Hummel, T.; Hugentobler, M.; Giger, R.; Lacroix, J. Ratings of Overall Olfactory Function. Chem. Senses 2003, 28, 691–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vestito, L.; Mori, L.; Trompetto, C.; Bagnasco, D.; Canevari, R.F.; Ponzano, M.; Subbrero, D.; Cecchella, E.; Barbara, C.; Clavario, P.; et al. Impact of tDCS on persistent COVID-19 olfactory dysfunction: A double-blind sham-controlled study. J. Neurol. Neurosurg. Psychiatry 2022, 94, 87–88. [Google Scholar] [CrossRef]
- Moradi, K. Clinical Trial Protocol Evaluation of the Effectiveness of TDCS (Transcranial Direct Current Stimulation) in the Treatment of Hyposmia in Patients with COVID-19. Available online: https://www.irct.ir/trial/53545 (accessed on 10 June 2022).
- Gardner-O’Kearny, W. SWFT—Shapiro-Wilk/Shapiro-Francia Tests. 2021. Available online: https://www.mathworks.com/matlabcentral/fileexchange/88778-swft-shapiro-wilk-shapiro-francia-tests (accessed on 12 June 2023).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Threshold | Discrimination | Identification | TDI | Classification | Percentile |
|---|---|---|---|---|---|---|
| C01 | 10.5 | 13 | 11 | 34.5 | Normosmia | 50–75% |
| C02 | 12.5 | 15 | 12 | 39.5 | Normosmia | 75–90% |
| C03 | 12.5 | 12 | 14 | 38.5 | Normosmia | 75% |
| C04 | 1 | 11 | 11 | 23 | Hyposmia | 0–5% |
| C05 | 11.75 | 12 | 13 | 36.75 | Normosmia | 50–75% |
| C06 | 6.25 | 13 | 14 | 33.25 | Normosmia | 25–50% |
| C07 | 6.75 | 12 | 8 | 26.75 | Hyposmia | 0–5% |
| C21 | 9.75 | 9 | 13 | 31.75 | Normosmia | 10–25% |
| C22 | 1.75 | 11 | 4 | 16.75 | Hyposmia | 0–5% |
| C23 | 11.25 | 12 | 10 | 33.25 | Normosmia | 25–50% |
| C24 | 5.5 | 11 | 8 | 24.5 | Hyposmia | 0–5% |
| C25 | 13.5 | 12 | 14 | 39.5 | Normosmia | 90% |
| C26 | 9 | 12 | 4 | 25 | Hyposmia | 0–5% |
| C27 | 4.5 | 9 | 12 | 25.5 | Hyposmia | 5–10% |
| C28 | 10.5 | 11 | 8 | 29.5 | Hyposmia | 5–10% |
| C29 | 12.5 | 9 | 7 | 28.5 | Hyposmia | 0–5% |
| C30 | 6.5 | 12 | 10 | 28.5 | Hyposmia | 10–25% |
| C31 | 7.5 | 11 | 7 | 25.5 | Hyposmia | 0–5% |
| C32 | 3.5 | 13 | 8 | 24.5 | Hyposmia | 0–5% |
| C33 | 9.25 | 13 | 9 | 31.25 | Hyposmia | 10–25% |
| C34 | 4.25 | 9 | 9 | 22.25 | Hyposmia | 0–5% |
| C35 | 9.25 | 11 | 10 | 30.25 | Hyposmia | 5–10% |
| C36 | 1.5 | 7 | 7 | 15.5 | Anosmia | 0–5% |
| C37 | 6 | 12 | 10 | 28 | Hyposmia | 0–5% |
| C38 | 3.25 | 4 | 7 | 14.25 | Anosmia | 0–5% |
| Point 1 [V/m] | Point 2 [V/m] | Point 3 [V/m] | Maximum [V/m] | |
|---|---|---|---|---|
| Model 1 | 0.0982 | 0.1302 | 0.0848 | 0.1827 |
| Model 2 | 0.0993 | 0.1324 | 0.0915 | 0.206 |
| Model 3 | 0.0585 | 0.0704 | 0.0458 | 0.0939 |
| Model 4 | 0.0387 | 0.0537 | 0.0389 | 0.0855 |
| Model 5 | 0.0777 | 0.1043 | 0.0722 | 0.1821 |
| Stim Subject | C22 | C28 | C30 | C31 | C33 | C35 | C36 | C38 |
| Age | 52 | 40 | 54 | 29 | 46 | 34 | 28 | 42 |
| Gender | M | F | M | M | F | M | F | F |
| Time Olfactory Tests | 128 | 77 | 63 | 95 | 90 | 34 | 52 | 28 |
| Time Stimulation—Test | 6 | 14 | 4 | 1 | 6 | 1 | 3 | 14 |
| THR Initial | 1.75 | 10.5 | 6.5 | 7.5 | 9.25 | 9.25 | 1.5 | 3.25 |
| THR Final | 2.5 | 10.25 | 8.25 | 1 | 8 | 9.5 | 1 | 1 |
| THR Difference | 0.75 | −0.25 | 1.75 | −6.5 | −1.25 | 0.25 | −0.5 | −2.25 |
| DR Initial | 11 | 11 | 12 | 11 | 13 | 11 | 7 | 4 |
| DR Final | 12 | 6 | 13 | 13 | 14 | 9 | 9 | 9 |
| DR Difference | 1 | −5 | 1 | 2 | 1 | −2 | 2 | 5 |
| ID Initial | 4 | 8 | 10 | 7 | 9 | 10 | 7 | 7 |
| ID Final | 10 | 8 | 8 | 7 | 4 | 11 | 8 | 6 |
| ID Difference | 6 | 0 | −2 | 0 | −5 | 1 | 1 | −1 |
| TDI Initial | 16.75 | 29.5 | 28.5 | 25.5 | 31.25 | 30.25 | 15.5 | 14.25 |
| TDI Final | 24.5 | 24.25 | 29.25 | 21 | 26 | 29.5 | 18 | 16 |
| TDI Difference | 7.75 | −5.25 | 0.75 | −4.5 | −5.25 | −0.75 | 2.5 | 2.25 |
| Sham Subject | C21 | C23 | C27 | C29 | C32 | C34 | C37 | |
| Age | 23 | 25 | 53 | 37 | 53 | 55 | 30 | |
| Gender | F | M | F | M | M | F | M | |
| Time Olfactory Tests | 116 | 89 | 132 | 82 | 62 | 91 | 23 | |
| Time Stimulation—Test | 7 | 4 | 8 | 11 | 6 | 7 | 6 | |
| THR Initial | 9.75 | 11.25 | 4.5 | 12.5 | 3.5 | 4.25 | 6 | |
| THR Final | 10.25 | 10.5 | 1 | 10.25 | 3 | 6.75 | 10 | |
| THR Difference | 0.5 | −0.75 | −3.5 | −2.25 | −0.5 | 2.5 | 4 | |
| DR Initial | 9 | 12 | 9 | 9 | 13 | 9 | 12 | |
| DR Final | 15 | 6 | 6 | 12 | 11 | 10 | 13 | |
| DR Difference | 6 | −6 | −3 | 3 | −2 | 1 | 1 | |
| ID Initial | 13 | 10 | 12 | 7 | 8 | 9 | 10 | |
| ID Final | 12 | 13 | 11 | 8 | 7 | 8 | 10 | |
| ID Difference | −1 | 3 | −1 | 1 | −1 | −1 | 0 | |
| TDI Initial | 31.75 | 33.25 | 25.5 | 28.5 | 24.5 | 22.25 | 28 | |
| TDI Final | 37.25 | 29.5 | 18 | 30.25 | 21 | 24.75 | 33 | |
| TDI Difference | 5.5 | −3.75 | −7.5 | 1.75 | −3.5 | 2.5 | 5 |
| THR | ||||||
| Sum of Squares | df | Mean Squares | F | p-value | ||
| Group stimulation | 107.05 | 2 | 53.52 | 4.27 | 0.0258 | 0.18 |
| Olfactory assessment | 3.13 | 1 | 3.13 | 0.25 | 0.6218 | −0.03 |
| Group stimulation × Olfactory assessment | 2.05 | 2 | 1.03 | 0.08 | 0.9215 | −0.07 |
| Residual | 300.51 | 24 | 12.52 | |||
| DR | ||||||
| Sum of Squares | df | Mean Squares | F | -value | ||
| Group stimulation | 50.12 | 2 | 25.06 | 4.17 | 0.0279 | 0.18 |
| Olfactory assessment | 6.19 | 1 | 6.19 | 1.03 | 0.3202 | 0.001 |
| Group stimulation × Olfactory assessment | 11.75 | 2 | 5.88 | 0.98 | 0.3908 | −0.002 |
| Residual | 144.26 | 24 | 6.01 | |||
| ID | ||||||
| Sum of Squares | df | Mean Squares | F | -value | ||
| Group stimulation | 32.9 | 2 | 16.45 | 3.4 | 0.0502 | 0.14 |
| Olfactory assessment | 0.15 | 1 | 0.15 | 0.03 | 0.8598 | −0.03 |
| Group stimulation × Olfactory assessment | 0.22 | 2 | 0.11 | 0.02 | 0.9779 | −0.07 |
| Residual | 116.21 | 24 | 4.84 | |||
| TDI | ||||||
| Sum of Squares | df | Mean Squares | F | -value | ||
| Group stimulation | 421.68 | 2 | 210.84 | 8.9 | 0.0013 | 0.35 |
| Olfactory assessment | 0.11 | 1 | 0.11 | 0 | 0.9469 | −0.04 |
| Group stimulation × Olfactory assessment | 6.49 | 2 | 3.24 | 0.14 | 0.8727 | −0.06 |
| Residual | 568.64 | 24 | 23.69 | |||
| Stim—Anosmia | Stim—Hyposmia | Stim | Sham—Anosmia | Sham—Hyposmia | Sham | |
|---|---|---|---|---|---|---|
| THR Initial | - | |||||
| DR Initial | - | |||||
| ID Initial | - | |||||
| TDI Initial | - | |||||
| THR Final | - | |||||
| DR Final | - | |||||
| ID Final | - | |||||
| TDI Final | - | |||||
| Anosmia | Hyposmia | Total | ||||
| THR Initial | ||||||
| DR Initial | ||||||
| ID Initial | ||||||
| TDI Initial | ||||||
| THR Final | ||||||
| DR Final | ||||||
| ID Final | ||||||
| TDI Final |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gracia, D.I.; Ortiz, M.; Candela, T.; Iáñez, E.; Sánchez, R.M.; Díaz, C.; Azorín, J.M. Design and Evaluation of a Potential Non-Invasive Neurostimulation Strategy for Treating Persistent Anosmia in Post-COVID-19 Patients. Sensors 2023, 23, 5880. https://doi.org/10.3390/s23135880
Gracia DI, Ortiz M, Candela T, Iáñez E, Sánchez RM, Díaz C, Azorín JM. Design and Evaluation of a Potential Non-Invasive Neurostimulation Strategy for Treating Persistent Anosmia in Post-COVID-19 Patients. Sensors. 2023; 23(13):5880. https://doi.org/10.3390/s23135880
Chicago/Turabian StyleGracia, Desirée I., Mario Ortiz, Tatiana Candela, Eduardo Iáñez, Rosa M. Sánchez, Carmina Díaz, and José M. Azorín. 2023. "Design and Evaluation of a Potential Non-Invasive Neurostimulation Strategy for Treating Persistent Anosmia in Post-COVID-19 Patients" Sensors 23, no. 13: 5880. https://doi.org/10.3390/s23135880