


The Analytical and Clinical Validity of the pfSTEP Digital Biomarker of the Susceptibility/Risk of Declining Physical Function in Community-Dwelling Older Adults
 , , ,
, , ,  and
and
Abstract
:1. Introduction
- Selecting a verified wrist-worn measurement system, formed by the GENEActiv accelerometer [49] and its accompanying open-source step counting algorithm.
- Establishing its analytical validity by measuring the level of concurrent agreement between the GENEActiv wrist system and the activPAL thigh system when worn simultaneously in a sample of older adults.
- Establishing its clinical validity by measuring the prospective association between repeated measures of daily stepping volume and rate with physical function measured via the Short Physical Performance Battery (SPPB) score [50] in a sample of older adults. The SPPB score is a clinically based measure of physical function associated with all-cause mortality, hospitalisation, future functional decline, and long-term disability [51,52]. Furthermore, the SPPB score is a predictor of frailty phenotypes and geriatric syndromes in community-dwelling older people [53].
2. Materials and Methods
2.1. Verification
2.2. Analytical Validity
2.2.1. Data Source
2.2.2. Processing of Raw Accelerometer Data
2.2.3. Data Quality and Aggregation
2.3. Clinical Validity
2.3.1. Data Source
2.3.2. Processing of Raw Accelerometer Data
2.3.3. Data Quality and Aggregation of Stepping Metrics
2.4. Statistical Analysis
2.4.1. Analytical Validity
2.4.2. Clinical Validity
- Model 1: ‘Total steps’ only.
- Model 2: ‘Faster-paced walking steps’ only.
- Model 3: ‘Faster-paced walking steps’ and ‘Slower-paced steps’.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall N = 651 | Male N = 217 | Female N = 434 | |
|---|---|---|---|
| Age at recruitment 1 | 77 (7) | 77 (7) | 77 (7) |
| Baseline physical function (SPPB) 1 | 8.47 (1.52) | 8.60 (1.48) | 8.40 (1.55) |
| IMD quintile 2 | |||
| 1/5 (Most deprived) | 69 (11%) | 24 (11%) | 45 (10%) |
| 2/5 | 130 (20%) | 46 (21%) | 84 (19%) |
| 3/5 | 130 (20%) | 46 (21%) | 84 (19%) |
| 4/5 | 136 (21%) | 42 (19%) | 94 (22%) |
| 5/5 (Least deprived) | 186 (29%) | 59 (27%) | 127 (29%) |
| Highest education 2 | |||
| Some/All secondary | 291 (45%) | 91 (42%) | 200 (46%) |
| Some college | 171 (26%) | 58 (27%) | 113 (26%) |
| All college/Degree | 189 (29%) | 68 (31%) | 121 (28%) |
| Comorbidity 2 | |||
| None | 549 (84%) | 182 (84%) | 367 (85%) |
| One or more | 102 (16%) | 35 (16%) | 67 (15%) |
| SF-36 General Health Score 2 | |||
| Very good/Excellent | 99 (15%) | 28 (13%) | 71 (16%) |
| Good | 310 (48%) | 109 (50%) | 201 (46%) |
| Fair/Poor | 242 (37%) | 80 (37%) | 162 (37%) |
| Allocation 2 | |||
| Control | 300 (46%) | 98 (45%) | 202 (47%) |
| Intervention | 351 (54%) | 119 (55%) | 232 (53%) |
| Site 2 | |||
| Bristol/Bath | 278 (43%) | 89 (41%) | 189 (44%) |
| Birmingham | 152 (23%) | 58 (27%) | 94 (22%) |
| Exeter | 221 (34%) | 70 (32%) | 151 (35%) |
2.5. Biomarker Description
3. Results
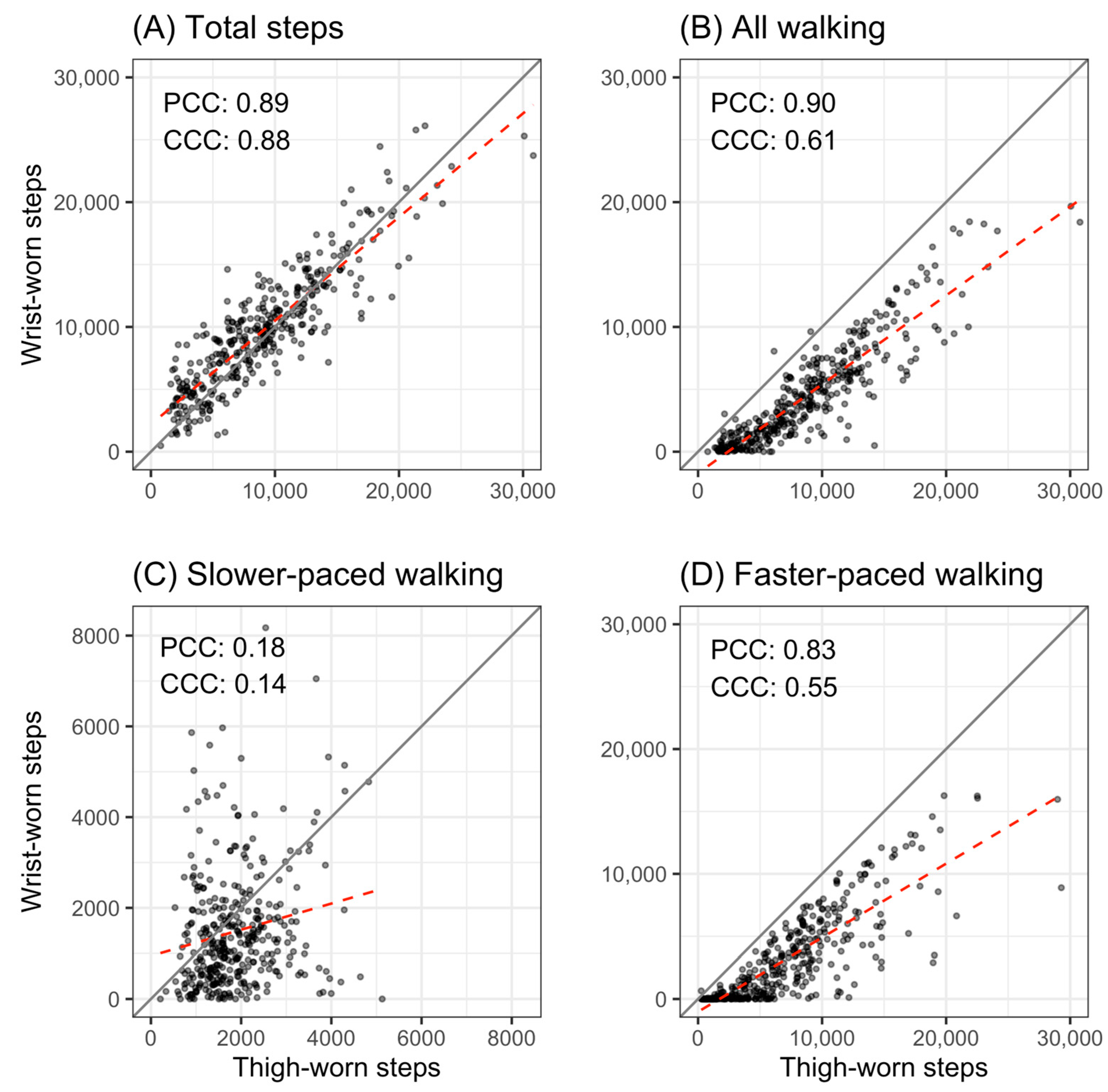
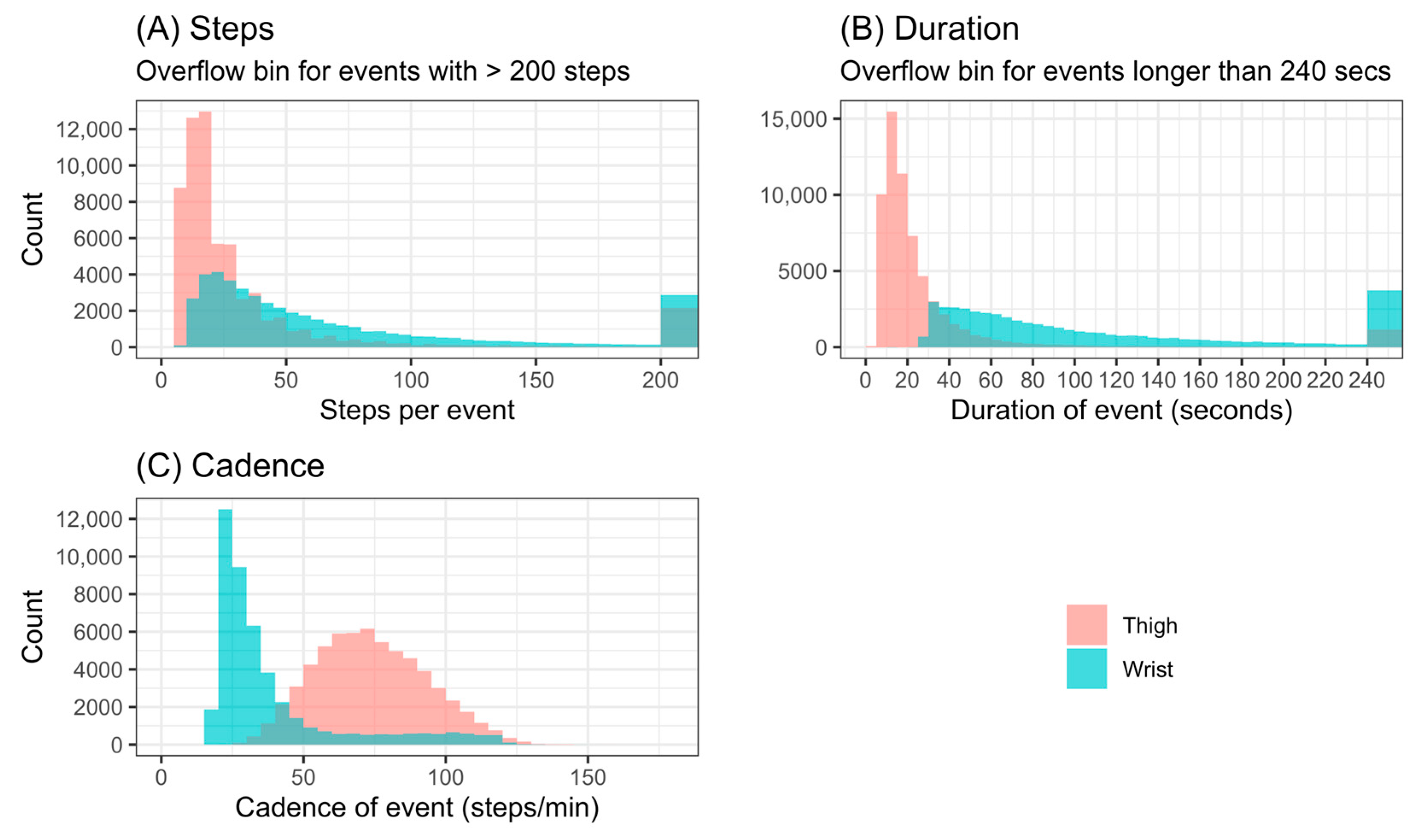
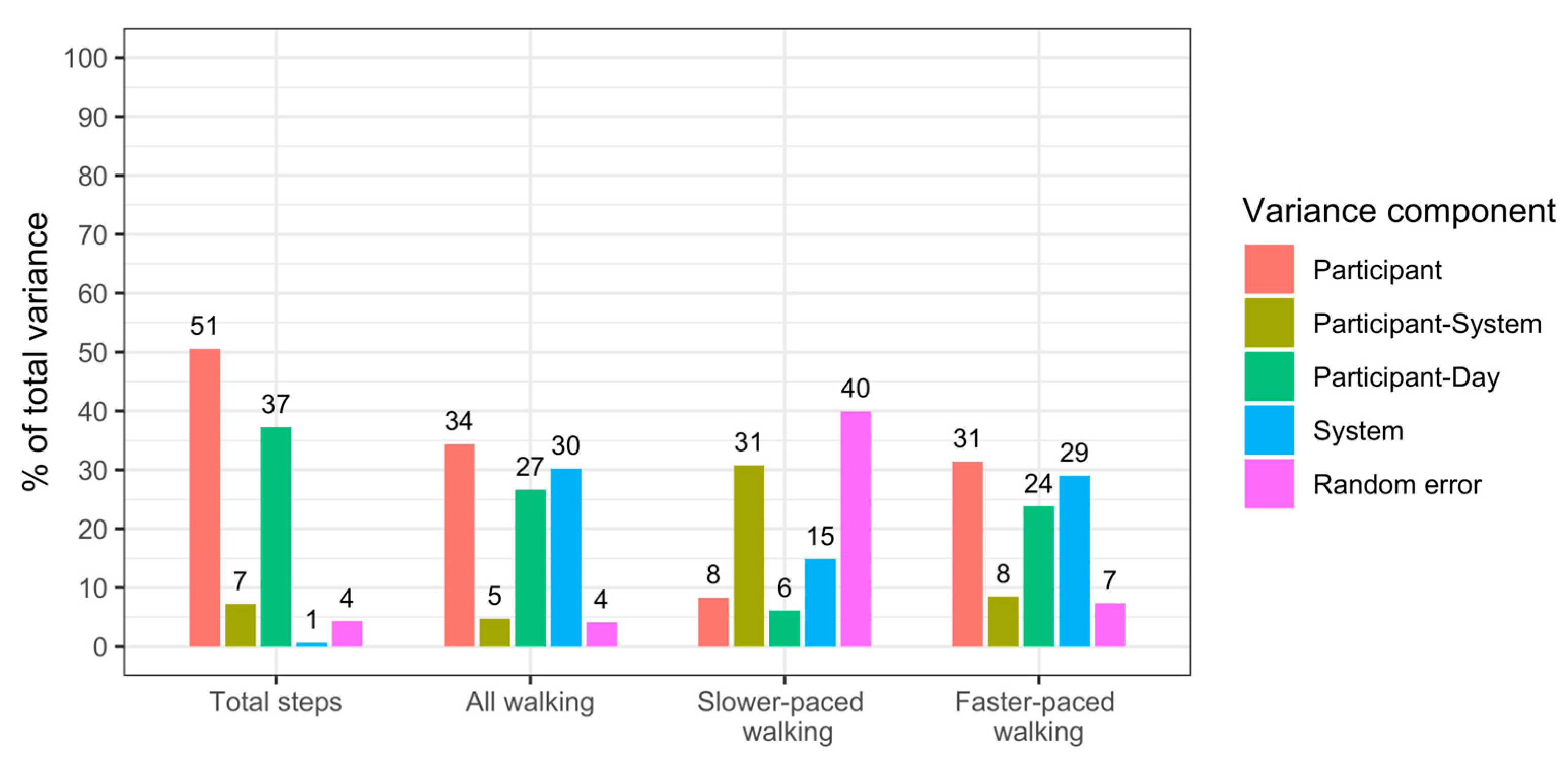
3.1. Analytical Validity
3.2. Clinical Validity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A




Appendix B
| Model 1b Total Steps Only | Model 2b Faster-Paced Walking Steps Only | Model 3b Faster-Paced Walking and Slower-Paced Steps | |
|---|---|---|---|
| Total steps (20–175 steps/min) | |||
| Baseline | 0.05 (0.00–0.09) * | N/A | N/A |
| 6 Months | 0.08 (0.03–0.13) ** | N/A | N/A |
| 12 Months | 0.13 (0.07–0.18) *** | N/A | N/A |
| 24 Months | 0.22 (0.16–0.27) *** | N/A | N/A |
| Faster-paced walking steps (63–175 steps/min) | |||
| Baseline | N/A | 0.10 (−0.05–0.25) | 0.06 (−0.10–0.23) |
| 6 Months | N/A | 0.28 (0.11–0.45) ** | 0.24 (0.05–0.43) * |
| 12 Months | N/A | 0.44 (0.26–0.62) *** | 0.36 (0.16–0.56) *** |
| 24 Months | N/A | 0.72 (0.53–0.91) *** | 0.54 (0.33–0.75) *** |
| Slower-paced steps (20–62 steps/min) | |||
| Baseline | N/A | N/A | 0.04 (−0.02–0.10) |
| 6 Months | N/A | N/A | 0.04 (−0.04–0.11) |
| 12 Months | N/A | N/A | 0.07 (−0.01–0.14) |
| 24 Months | N/A | N/A | 0.14 (0.07–0.21) *** |
| Goodness-of-fit | |||
| AIC | 8788 | 8799 | 8776 |
| Log-likelihood | −4375 | −4381 | −4365 |
| Model 1c Total Steps Only | Model 2c Faster-Paced Walking Steps Only | Model 3c Faster-Paced Walking and Slower-Paced Steps | |
|---|---|---|---|
| Total steps (20–175 steps/min) | |||
| Baseline | 0.04 (−0.02–0.10) | N/A | N/A |
| 6 Months | 0.12 (0.05–0.19) *** | N/A | N/A |
| 12 Months | 0.17 (0.10–0.24) *** | N/A | N/A |
| 24 Months | 0.29 (0.21–0.36) *** | N/A | N/A |
| Faster-paced walking steps (63–175 steps/min) | |||
| Baseline | N/A | 0.09 (−0.11–0.29) | 0.06 (−0.17–0.28) |
| 6 Months | N/A | 0.43 (0.20–0.65) *** | 0.36 (0.10–0.61) ** |
| 12 Months | N/A | 0.65 (0.40–0.89) *** | 0.55 (0.27–0.82) *** |
| 24 Months | N/A | 1.01 (0.74–1.29) *** | 0.79 (0.49–1.09) *** |
| Slower-paced steps (20–62 steps/min) | |||
| Baseline | N/A | N/A | 0.03 (−0.05–0.12) |
| 6 Months | N/A | N/A | 0.06 (−0.03–0.15) |
| 12 Months | N/A | N/A | 0.08 (−0.02–0.17) |
| 24 Months | N/A | N/A | 0.17 (0.07–0.27) ** |
| Goodness-of-fit | |||
| AIC | 8573 | 8570 | 8557 |
| Log-likelihood | −4249 | −4247 | −4236 |
| Model 1d Total Steps Only | Model 2d Faster-Paced Walking Steps Only | Model 3d Faster-Paced Walking and Slower-Paced Steps | |
|---|---|---|---|
| Total steps (20–175 steps/min) | |||
| Baseline | 0.04 (−0.03–0.10) | N/A | N/A |
| 6 Months | 0.00 (−0.07–0.16) | N/A | N/A |
| 12 Months | 0.08 (0.00–0.16) * | N/A | N/A |
| 24 Months | 0.19 (0.11–0.27) *** | N/A | N/A |
| Faster-paced walking steps (63–175 steps/min) | |||
| Baseline | N/A | 0.08 (−0.13–0.29) | 0.05 (−0.19–0.29) |
| 6 Months | N/A | 0.09 (−0.17–0.35) | 0.13 (−0.16–0.42) |
| 12 Months | N/A | 0.36 (0.06–0.67) * | 0.32 (−0.01–0.66) |
| 24 Months | N/A | 0.57 (0.30–0.84) *** | 0.45 (0.16–0.74) ** |
| Slower-paced steps (20–62 steps/min) | |||
| Baseline | N/A | N/A | 0.03 (−0.05–0.12) |
| 6 Months | N/A | N/A | −0.03 (−0.13–0.07) |
| 12 Months | N/A | N/A | 0.03 (−0.08–0.14) |
| 24 Months | N/A | N/A | 0.13 (0.03–0.23) * |
| Goodness-of-fit | |||
| AIC | 4026 | 4032 | 4027 |
| Log-likelihood | −1989 | −1992 | −1986 |
| Model 1e Total Steps Only | Model 2e Faster-Paced Walking Steps Only | Model 3e Faster-Paced Walking and Slower-Paced Steps | |
|---|---|---|---|
| Total steps (20–175 steps/min) | |||
| Baseline | 0.04 (−0.03–0.10) | N/A | N/A |
| 6 Months | 0.13 (0.06–0.20) *** | N/A | N/A |
| 12 Months | 0.15 (0.08–0.22) *** | N/A | N/A |
| 24 Months | 0.22 (0.15–0.30) *** | N/A | N/A |
| Faster-paced walking steps (63–175 steps/min) | |||
| Baseline | N/A | 0.09 (−0.11–0.30) | 0.07 (−0.16–0.30) |
| 6 Months | N/A | 0.37 (0.14–0.59) ** | 0.25 (0.00–0.51) * |
| 12 Months | N/A | 0.45 (0.23–0.69) *** | 0.35 (0.09–0.60) ** |
| 24 Months | N/A | 0.82 (0.55–1.09) *** | 0.62 (0.31–0.92) *** |
| Slower-paced steps (20–62 steps/min) | |||
| Baseline | N/A | N/A | 0.02 (−0.06–0.11) |
| 6 Months | N/A | N/A | 0.10 (0.00–0.20) * |
| 12 Months | N/A | N/A | 0.09 (−0.01–0.19) |
| 24 Months | N/A | N/A | 0.14 (0.03–0.24) * |
| Goodness-of-fit | |||
| AIC | 4744 | 4749 | 4740 |
| Log-likelihood | −2348 | −2351 | −2342 |
References
- Hall, K.S.; Hyde, E.T.; Bassett, D.R.; Carlson, S.A.; Carnethon, M.R.; Ekelund, U.; Evenson, K.R.; Galuska, D.A.; Kraus, W.E.; Lee, I.-M.; et al. Systematic Review of the Prospective Association of Daily Step Counts with Risk of Mortality, Cardiovascular Disease, and Dysglycemia. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 78. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Camhi, S.M.; Leonardi, C.; Johnson, W.D.; Katzmarzyk, P.T.; Earnest, C.P.; Church, T.S. Patterns of Adult Stepping Cadence in the 2005–2006 NHANES. Prev. Med. 2011, 53, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Granat, M.H. Event-Based Analysis of Free-Living Behaviour. Physiol. Meas. 2012, 33, 1785–1800. [Google Scholar] [CrossRef] [PubMed]
- Granat, M.; Clarke, C.; Holdsworth, R.; Stansfield, B.; Dall, P. Quantifying the Cadence of Free-Living Walking Using Event-Based Analysis. Gait Posture 2015, 42, 85–90. [Google Scholar] [CrossRef]
- Stansfield, B.; Hajarnis, M.; Sudarshan, R. Characteristics of Very Slow Stepping in Healthy Adults and Validity of the ActivPAL3TM Activity Monitor in Detecting These Steps. Med. Eng. Phys. 2015, 37, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Kraus, W.E.; Janz, K.F.; Powell, K.E.; Campbell, W.W.; Jakicic, J.M.; Troiano, R.P.; Sprow, K.; Torres, A.; Piercy, K.L. Daily Step Counts for Measuring Physical Activity Exposure and Its Relation to Health. Med. Sci. Sports Exerc. 2019, 51, 1206–1212. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.-M.; Shiroma, E.J.; Kamada, M.; Bassett, D.R.; Matthews, C.E.; Buring, J.E. Association of Step Volume and Intensity with All-Cause Mortality in Older Women. JAMA Intern. Med. 2019, 179, 1105. [Google Scholar] [CrossRef]
- Saint-Maurice, P.F.; Troiano, R.P.; Bassett, D.R.; Graubard, B.I.; Carlson, S.A.; Shiroma, E.J.; Fulton, J.E.; Matthews, C.E. Association of Daily Step Count and Step Intensity with Mortality among US Adults. JAMA 2020, 323, 1151. [Google Scholar] [CrossRef]
- Paluch, A.E.; Bajpai, S.; Bassett, D.R.; Carnethon, M.R.; Ekelund, U.; Evenson, K.R.; Galuska, D.A.; Jefferis, B.J.; Kraus, W.E.; Lee, I.-M.; et al. Daily Steps and All-Cause Mortality: A Meta-Analysis of 15 International Cohorts. Lancet Public Health 2022, 7, e219–e228. [Google Scholar] [CrossRef]
- Master, H.; Annis, J.; Huang, S.; Beckman, J.A.; Ratsimbazafy, F.; Marginean, K.; Carroll, R.; Natarajan, K.; Harrell, F.E.; Roden, D.M.; et al. Association of Step Counts over Time with the Risk of Chronic Disease in the All of Us Research Program. Nat. Med. 2022, 28, 2301–2308. [Google Scholar] [CrossRef]
- Paluch, A.E.; Bajpai, S.; Ballin, M.; Bassett, D.R.; Buford, T.W.; Carnethon, M.R.; Chernofsky, A.; Dooley, E.E.; Ekelund, U.; Evenson, K.R.; et al. Prospective Association of Daily Steps with Cardiovascular Disease: A Harmonized Meta-Analysis. Circulation 2023, 147, 122–131. [Google Scholar] [CrossRef]
- Mañas, A.; del Pozo Cruz, B.; Ekelund, U.; Losa Reyna, J.; Rodríguez Gómez, I.; Carnicero Carreño, J.A.; Rodríguez Mañas, L.; García García, F.J.; Ara, I. Association of Accelerometer-Derived Step Volume and Intensity with Hospitalizations and Mortality in Older Adults: A Prospective Cohort Study. J. Sport Health Sci. 2022, 11, 578–585. [Google Scholar] [CrossRef] [PubMed]
- del Pozo Cruz, B.; Ahmadi, M.N.; Lee, I.-M.; Stamatakis, E. Prospective Associations of Daily Step Counts and Intensity With Cancer and Cardiovascular Disease Incidence and Mortality and All-Cause Mortality. JAMA Intern. Med. 2022, 182, 1139. [Google Scholar] [CrossRef] [PubMed]
- Sumner, J.; Uijtdewilligen, L.; Yee, A.C.H.; Xian, S.N.H.; Barreira, T.V.; Sloan, R.A.; Van Dam, R.M.; Müller-Riemenschneider, F. Volume and Intensity of Stepping Activity and Cardiometabolic Risk Factors in a Multi-Ethnic Asian Population. Int. J. Environ. Res. Public. Health 2020, 17, 863. [Google Scholar] [CrossRef]
- del Pozo Cruz, B.; Ahmadi, M.; Naismith, S.L.; Stamatakis, E. Association of Daily Step Count and Intensity With Incident Dementia in 78 430 Adults Living in the UK. JAMA Neurol. 2022, 79, 1059. [Google Scholar] [CrossRef]
- Garduno, A.C.; LaCroix, A.Z.; LaMonte, M.J.; Dunstan, D.W.; Evenson, K.R.; Wang, G.; Di, C.; Schumacher, B.T.; Bellettiere, J. Associations of Daily Steps and Step Intensity with Incident Diabetes in a Prospective Cohort Study of Older Women: The OPACH Study. Diabetes Care 2022, 45, 339–347. [Google Scholar] [CrossRef]
- Cuthbertson, C.C.; Moore, C.C.; Sotres-Alvarez, D.; Heiss, G.; Isasi, C.R.; Mossavar-Rahmani, Y.; Carlson, J.A.; Gallo, L.C.; Llabre, M.M.; Garcia-Bedoya, O.L.; et al. Associations of Steps per Day and Step Intensity with the Risk of Diabetes: The Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Int. J. Behav. Nutr. Phys. Act. 2022, 19, 46. [Google Scholar] [CrossRef] [PubMed]
- Paluch, A.E.; Gabriel, K.P.; Fulton, J.E.; Lewis, C.E.; Schreiner, P.J.; Sternfeld, B.; Sidney, S.; Siddique, J.; Whitaker, K.M.; Carnethon, M.R. Steps per Day and All-Cause Mortality in Middle-Aged Adults in the Coronary Artery Risk Development in Young Adults Study. JAMA Netw. Open 2021, 4, e2124516. [Google Scholar] [CrossRef] [PubMed]
- Welk, G.J.; Mcclain, J.; Ainsworth, B.E. Protocols for Evaluating Equivalency of Accelerometry-Based Activity Monitors. Med. Sci. Sports Exerc. 2012, 44, S39–S49. [Google Scholar] [CrossRef]
- Ellingson, L.D.; Hibbing, P.R.; Welk, G.J.; Dailey, D.; Rakel, B.A.; Crofford, L.J.; Sluka, K.A.; Frey-Law, L.A. Choice of Processing Method for Wrist-Worn Accelerometers Influences Interpretation of Free-Living Physical Activity Data in a Clinical Sample. J. Meas. Phys. Behav. 2019, 2, 228–236. [Google Scholar] [CrossRef]
- Logan, G.R.M.; Duncan, S.; Harris, N.K.; Hinckson, E.A.; Schofield, G. Adolescent Physical Activity Levels: Discrepancies with Accelerometer Data Analysis. J. Sports Sci. 2016, 34, 2047–2053. [Google Scholar] [CrossRef] [PubMed]
- Rosenberger, M.E.; Haskell, W.L.; Albinali, F.; Mota, S.; Nawyn, J.; Intille, S. Estimating Activity and Sedentary Behavior from an Accelerometer on the Hip or Wrist. Med. Sci. Sports Exerc. 2013, 45, 964–975. [Google Scholar] [CrossRef] [PubMed]
- Kamada, M.; Shiroma, E.J.; Harris, T.B.; Lee, I.-M. Comparison of Physical Activity Assessed Using Hip- and Wrist-Worn Accelerometers. Gait Posture 2016, 44, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Cooke, A.B.; Daskalopoulou, S.S.; Dasgupta, K. The Impact of Accelerometer Wear Location on the Relationship between Step Counts and Arterial Stiffness in Adults Treated for Hypertension and Diabetes. J. Sci. Med. Sport 2018, 21, 398–403. [Google Scholar] [CrossRef] [PubMed]
- John, D.; Morton, A.; Arguello, D.; Lyden, K.; Bassett, D. “What Is a Step?” Differences in How a Step Is Detected among Three Popular Activity Monitors That Have Impacted Physical Activity Research. Sensors 2018, 18, 1206. [Google Scholar] [CrossRef] [PubMed]
- Mandigout, S.; Lacroix, J.; Perrochon, A.; Svoboda, Z.; Aubourg, T.; Vuillerme, N. Comparison of Step Count Assessed Using Wrist- and Hip-Worn Actigraph GT3X in Free-Living Conditions in Young and Older Adults. Front. Med. 2019, 6, 252. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Toth, L.P.; Hibbing, P.R.; Springer, C.M.; Kaplan, A.S.; Feyerabend, M.D.; Crouter, S.E.; Bassett, D.R. Dominant vs. Non-Dominant Wrist Placement of Activity Monitors: Impact on Steps per Day. J. Meas. Phys. Behav. 2019, 2, 118–123. [Google Scholar] [CrossRef]
- Maylor, B.D.; Edwardson, C.L.; Dempsey, P.C.; Patterson, M.R.; Plekhanova, T.; Yates, T.; Rowlands, A.V. Stepping towards More Intuitive Physical Activity Metrics with Wrist-Worn Accelerometry: Validity of an Open-Source Step-Count Algorithm. Sensors 2022, 22, 9984. [Google Scholar] [CrossRef]
- Lee, K.-Y.; Macfarlane, D.J.; Cerin, E. Comparison of Three Models of Actigraph Accelerometers during Free Living and Controlled Laboratory Conditions. Eur. J. Sport Sci. 2013, 13, 332–339. [Google Scholar] [CrossRef]
- Sellers, C.; Dall, P.; Grant, M.; Stansfield, B. Validity and Reliability of the ActivPAL3 for Measuring Posture and Stepping in Adults and Young People. Gait Posture 2016, 43, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Bourke, A.K.; Ihlen, E.A.F.; Helbostad, J.L. Validation of the ActivPAL3 in Free-Living and Laboratory Scenarios for the Measurement of Physical Activity, Stepping, and Transitions in Older Adults. J. Meas. Phys. Behav. 2019, 2, 58–65. [Google Scholar] [CrossRef]
- Feito, Y.; Garner, H.R.; Bassett, D.R. Evaluation of ActiGraph’s Low-Frequency Filter in Laboratory and Free-Living Environments. Med. Sci. Sports Exerc. 2015, 47, 211–217. [Google Scholar] [CrossRef]
- Takayanagi, N.; Sudo, M.; Yamashiro, Y.; Lee, S.; Kobayashi, Y.; Niki, Y.; Shimada, H. Relationship between Daily and In-Laboratory Gait Speed among Healthy Community-Dwelling Older Adults. Sci. Rep. 2019, 9, 3496. [Google Scholar] [CrossRef] [PubMed]
- Dall, P.M.; Mccrorie, P.R.W.; Granat, M.H.; Stansfield, B.W. Step Accumulation per Minute Epoch Is Not the Same as Cadence for Free-Living Adults. Med. Sci. Sports Exerc. 2013, 45, 1995–2001. [Google Scholar] [CrossRef]
- Dillon, C.B.; Fitzgerald, A.P.; Kearney, P.M.; Perry, I.J.; Rennie, K.L.; Kozarski, R.; Phillips, C.M. Number of Days Required to Estimate Habitual Activity Using Wrist-Worn GENEActiv Accelerometer: A Cross-Sectional Study. PLoS ONE 2016, 11, e0109913. [Google Scholar] [CrossRef]
- Meyer, B.M.; Depetrillo, P.; Franco, J.; Donahue, N.; Fox, S.R.; O’Leary, A.; Loftness, B.C.; Gurchiek, R.D.; Buckley, M.; Solomon, A.J.; et al. How Much Data Is Enough? A Reliable Methodology to Examine Long-Term Wearable Data Acquisition in Gait and Postural Sway. Sensors 2022, 22, 6982. [Google Scholar] [CrossRef] [PubMed]
- Troiano, R.P.; McClain, J.J.; Brychta, R.J.; Chen, K.Y. Evolution of Accelerometer Methods for Physical Activity Research. Br. J. Sports Med. 2014, 48, 1019–1023. [Google Scholar] [CrossRef]
- Scott, J.J.; Rowlands, A.V.; Cliff, D.P.; Morgan, P.J.; Plotnikoff, R.C.; Lubans, D.R. Comparability and Feasibility of Wrist- and Hip-Worn Accelerometers in Free-Living Adolescents. J. Sci. Med. Sport 2017, 20, 1101–1106. [Google Scholar] [CrossRef] [PubMed]
- McLellan, G.; Arthur, R.; Buchan, D.S. Wear Compliance, Sedentary Behaviour and Activity in Free-Living Children from Hip-and Wrist-Mounted ActiGraph GT3X+ Accelerometers. J. Sports Sci. 2018, 36, 2424–2430. [Google Scholar] [CrossRef]
- Goldsack, J.C.; Coravos, A.; Bakker, J.P.; Bent, B.; Dowling, A.V.; Fitzer-Attas, C.; Godfrey, A.; Godino, J.G.; Gujar, N.; Izmailova, E.; et al. Verification, Analytical Validation, and Clinical Validation (V3): The Foundation of Determining Fit-for-Purpose for Biometric Monitoring Technologies (BioMeTs). Npj Digit. Med. 2020, 3, 55. [Google Scholar] [CrossRef]
- Soltani, A.; Paraschiv-Ionescu, A.; Dejnabadi, H.; Marques-Vidal, P.; Aminian, K. Real-World Gait Bout Detection Using a Wrist Sensor: An Unsupervised Real-Life Validation. IEEE Access 2020, 8, 102883–102896. [Google Scholar] [CrossRef]
- McDevitt, B.; Moore, L.; Akhtar, N.; Connolly, J.; Doherty, R.; Scott, W. Validity of a Novel Research-Grade Physical Activity and Sleep Monitor for Continuous Remote Patient Monitoring. Sensors 2021, 21, 2034. [Google Scholar] [CrossRef]
- Chan, L.L.Y.; Choi, T.C.M.; Lord, S.R.; Brodie, M.A. Development and Large-Scale Validation of the Watch Walk Wrist-Worn Digital Gait Biomarkers. Sci. Rep. 2022, 12, 16211. [Google Scholar] [CrossRef] [PubMed]
- Femiano, R.; Werner, C.; Wilhelm, M.; Eser, P. Validation of Open-Source Step-Counting Algorithms for Wrist-Worn Tri-Axial Accelerometers in Cardiovascular Patients. Gait Posture 2022, 92, 206–211. [Google Scholar] [CrossRef]
- Mora-Gonzalez, J.; Gould, Z.R.; Moore, C.C.; Aguiar, E.J.; Ducharme, S.W.; Schuna, J.M.; Barreira, T.V.; Staudenmayer, J.; McAvoy, C.R.; Boikova, M.; et al. A Catalog of Validity Indices for Step Counting Wearable Technologies during Treadmill Walking: The CADENCE-Adults Study. Int. J. Behav. Nutr. Phys. Act. 2022, 19, 117. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, A.V.; Maylor, B.; Dawkins, N.P.; Dempsey, P.C.; Edwardson, C.L.; Soczawa-Stronczyk, A.A.; Bocian, M.; Patterson, M.R.; Yates, T. Stepping up with GGIR: Validity of Step Cadence Derived from Wrist-Worn Research-Grade Accelerometers Using the Verisense Step Count Algorithm. J. Sports Sci. 2022, 40, 2182–2190. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Barreira, T.V.; Schuna, J.M. Comparison of Step Outputs for Waist and Wrist Accelerometer Attachment Sites. Med. Sci. Sports Exerc. 2015, 47, 839–842. [Google Scholar] [CrossRef]
- Nuss, K.J.; Hulett, N.A.; Erickson, A.; Burton, E.; Carr, K.; Mooney, L.; Anderson, J.; Comstock, A.; Schlemer, E.J.; Archambault, L.J.; et al. Comparison of Energy Expenditure and Step Count Measured by ActiGraph Accelerometers Among Dominant and Nondominant Wrist and Hip Sites. J. Meas. Phys. Behav. 2020, 3, 315–322. [Google Scholar] [CrossRef]
- Activinsights Ltd., GENEActiv Accelerometer. Available online: https://activinsights.com/technology/geneactiv/ (accessed on 3 April 2023).
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A Short Physical Performance Battery Assessing Lower Extremity Function: Association With Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Gawel, J.; Vengrow, D.; Collins, J.; Brown, S.; Buchanan, A.; Cook, C. The Short Physical Performance Battery as a Predictor for Long Term Disability or Institutionalization in the Community Dwelling Population Aged 65 Years Old or Older. Phys. Ther. Rev. 2012, 17, 37–44. [Google Scholar] [CrossRef]
- Pavasini, R.; Guralnik, J.; Brown, J.C.; di Bari, M.; Cesari, M.; Landi, F.; Vaes, B.; Legrand, D.; Verghese, J.; Wang, C.; et al. Short Physical Performance Battery and All-Cause Mortality: Systematic Review and Meta-Analysis. BMC Med. 2016, 14, 215. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; López Sáez De Asteasu, M.; Morley, J.E.; Cano-Gutierrez, C.A.; Izquierdo, M. Performance of the Short Physical Performance Battery in Identifying the Frailty Phenotype and Predicting Geriatric Syndromes in Community-Dwelling Elderly. J. Nutr. Health Aging 2021, 25, 209–217. [Google Scholar] [CrossRef]
- FDA-NIH Biomarker Working Group. BEST (Biomarkers, EndpointS, and Other Tools) Resource; Food and Drug Administration (US): Silver Spring MD, USA, 2016.
- Esliger, D.W.; Rowlands, A.V.; Hurst, T.L.; Catt, M.; Murray, P.; Eston, R.G. Validation of the GENEA Accelerometer. Med. Sci. Sports Exerc. 2011, 43, 1085–1093. [Google Scholar] [CrossRef] [PubMed]
- PAL Technologies Ltd., ActivPAL Accelerometer and PALbatch Desktop Software for Processing of Raw Acceleration Data, Software Version 8.11.1.63. Available online: https://www.palt.com/ (accessed on 3 April 2023).
- Ryan, C.G. The Validity and Reliability of a Novel Activity Monitor as a Measure of Walking. Br. J. Sports Med. 2006, 40, 779–784. [Google Scholar] [CrossRef] [PubMed]
- van Hees, V.T.; Fang, Z.; Langford, J.; Assah, F.; Mohammad, A.; da Silva, I.C.M.; Trenell, M.I.; White, T.; Wareham, N.J.; Brage, S. Autocalibration of Accelerometer Data for Free-Living Physical Activity Assessment Using Local Gravity and Temperature: An Evaluation on Four Continents. J. Appl. Physiol. 2014, 117, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Fang, Z.; Langford, J.; Sweetland, C. GENEAread R Package for Reading Binary Files, Version 2.0.9. Available online: https://cran.r-project.org/web/packages/GENEAread/index.html (accessed on 3 April 2023).
- Campbell, C.; Gott, A.; Langford, J.; Sweetland, C. GENEAclassify R Package for the Segmentation and Classification of Accelerometer Data, Version 1.5.2. Available online: https://cran.r-project.org/web/packages/GENEAclassify/index.html (accessed on 3 April 2023).
- Migueles, J.H.; Rowlands, A.V.; Huber, F.; Sabia, S.; van Hees, V.T. GGIR: A Research Community–Driven Open Source R Package for Generating Physical Activity and Sleep Outcomes From Multi-Day Raw Accelerometer Data. J. Meas. Phys. Behav. 2019, 2, 188–196. [Google Scholar] [CrossRef]
- R Core Team R: A Language and Environment for Statistical Computing, Version 4.1.3. Available online: https://www.R-project.org/ (accessed on 3 April 2023).
- Toth, L.P.; Park, S.; Pittman, W.L.; Sarisaltik, D.; Hibbing, P.R.; Morton, A.L.; Springer, C.M.; Crouter, S.E.; Bassett, D.R. Effects of Brief Intermittent Walking Bouts on Step Count Accuracy of Wearable Devices. J. Meas. Phys. Behav. 2019, 2, 13–21. [Google Scholar] [CrossRef]
- Stathi, A.; Withall, J.; Greaves, C.J.; Thompson, J.L.; Taylor, G.; Medina-Lara, A.; Green, C.; Bilzon, J.; Gray, S.; Johansen-Berg, H.; et al. A Community-Based Physical Activity Intervention to Prevent Mobility-Related Disability for Retired Older People (REtirement in ACTion (REACT)): Study Protocol for a Randomised Controlled Trial. Trials 2018, 19, 228. [Google Scholar] [CrossRef]
- Withall, J.; Greaves, C.J.; Thompson, J.L.; de Koning, J.L.; Bollen, J.C.; Moorlock, S.J.; Fox, K.R.; Western, M.J.; Snowsill, T.; Medina-Lara, A.; et al. The Tribulations of Trials: Lessons Learnt Recruiting 777 Older Adults Into REtirement in ACTion (REACT), a Trial of a Community, Group-Based Active Aging Intervention Targeting Mobility Disability. J. Gerontol. Ser. A 2020, 75, 2387–2395. [Google Scholar] [CrossRef]
- Herrmann, S.D.; Barreira, T.V.; Kang, M.; Ainsworth, B.E. Impact of Accelerometer Wear Time on Physical Activity Data: A NHANES Semisimulation Data Approach. Br. J. Sports Med. 2014, 48, 278–282. [Google Scholar] [CrossRef]
- Lin, L.I.-K. A Concordance Correlation Coefficient to Evaluate Reproducibility. Biometrics 1989, 45, 255. [Google Scholar] [CrossRef]
- Carrasco, J.L.; King, T.S.; Chinchilli, V.M. The Concordance Correlation Coefficient for Repeated Measures Estimated by Variance Components. J. Biopharm. Stat. 2009, 19, 90–105. [Google Scholar] [CrossRef] [PubMed]
- Carrasco, J.L.; Martinez, J.P. Cccrm: Concordance Correlation Coefficient for Repeated (and Non-Repeated) Measures, Version 2.0.3. Available online: https://cran.r-project.org/web/packages/cccrm/index.html (accessed on 3 April 2023).
- StataCorp LLC, Stata SE-Standard Edition, Version 17.0 Revision 15 November 2022. Available online: http://www.stata.com (accessed on 3 April 2023).
- Altman, D.G. Practical Statistics for Medical Research; Chapman & Hall/CRC: Boca Raton, FL, USA, 1999; ISBN 978-1-00-022881-6. [Google Scholar]
- Stathi, A.; Greaves, C.J.; Thompson, J.L.; Withall, J.; Ladlow, P.; Taylor, G.; Medina-Lara, A.; Snowsill, T.; Gray, S.; Green, C.; et al. Effect of a Physical Activity and Behaviour Maintenance Programme on Functional Mobility Decline in Older Adults: The REACT (Retirement in Action) Randomised Controlled Trial. Lancet Public Health 2022, 7, e316–e326. [Google Scholar] [CrossRef] [PubMed]
- Zihajehzadeh, S.; Park, E.J. Regression Model-Based Walking Speed Estimation Using Wrist-Worn Inertial Sensor. PLoS ONE 2016, 11, e0165211. [Google Scholar] [CrossRef] [PubMed]
- Fasel, B.; Duc, C.; Dadashi, F.; Bardyn, F.; Savary, M.; Farine, P.-A.; Aminian, K. A Wrist Sensor and Algorithm to Determine Instantaneous Walking Cadence and Speed in Daily Life Walking. Med. Biol. Eng. Comput. 2017, 55, 1773–1785. [Google Scholar] [CrossRef]
- Soltani, A.; Dejnabadi, H.; Savary, M.; Aminian, K. Real-World Gait Speed Estimation Using Wrist Sensor: A Personalized Approach. IEEE J. Biomed. Health Inform. 2020, 24, 658–668. [Google Scholar] [CrossRef]
- Luu, L.; Pillai, A.; Lea, H.; Buendia, R.; Khan, F.M.; Dennis, G. Accurate Step Count with Generalized and Personalized Deep Learning on Accelerometer Data. Sensors 2022, 22, 3989. [Google Scholar] [CrossRef]
- Ermes, M.; Parkka, J.; Mantyjarvi, J.; Korhonen, I. Detection of Daily Activities and Sports With Wearable Sensors in Controlled and Uncontrolled Conditions. IEEE Trans. Inf. Technol. Biomed. 2008, 12, 20–26. [Google Scholar] [CrossRef]
- Gyllensten, I.C.; Bonomi, A.G. Identifying Types of Physical Activity With a Single Accelerometer: Evaluating Laboratory-Trained Algorithms in Daily Life. IEEE Trans. Biomed. Eng. 2011, 58, 2656–2663. [Google Scholar] [CrossRef]
- Rutjes, A.; Reitsma, J.; Coomarasamy, A.; Khan, K.; Bossuyt, P. Evaluation of Diagnostic Tests When There Is No Gold Standard. A Review of Methods. Health Technol. Assess. 2007, 11, iii, ix-51. [Google Scholar] [CrossRef]
- Kuo, P.-L.; Urbanek, J.K.; Schrack, J.A. Age-Related Bias in Total Step Count Recorded by Wearable Devices. JAMA Intern. Med. 2019, 179, 1602. [Google Scholar] [CrossRef]
- Chaudhry, U.A.R.; Wahlich, C.; Fortescue, R.; Cook, D.G.; Knightly, R.; Harris, T. The Effects of Step-Count Monitoring Interventions on Physical Activity: Systematic Review and Meta-Analysis of Community-Based Randomised Controlled Trials in Adults. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 129. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.; Bandeen-Roche, K.; Bhasin, S.A.R.; Eremenco, S.; Landi, F.; Muscedere, J.; Perera, S.; Reginster, J.-Y.; Woodhouse, L.; Vellas, B. Clinically meaningful change for physical performance: Perspectives of the icfsr task force. J. Frailty Aging 2019, 9, 9–13. [Google Scholar] [CrossRef]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful Change and Responsiveness in Common Physical Performance Measures in Older Adults: MEANINGFUL CHANGE AND PERFORMANCE. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef]
- Kwon, S.; Perera, S.; Pahor, M.; Katula, J.A.; King, A.C.; Groessl, E.J.; Studenski, S.A. What Is a Meaningful Change in Physical Performance? Findings from a Clinical Trial in Older Adults (the LIFE-P Study). J. Nutr. Health Aging 2009, 13, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Stansfield, B.; Clarke, C.; Dall, P.; Godwin, J.; Holdsworth, R.; Granat, M. True Cadence and Step Accumulation Are Not Equivalent: The Effect of Intermittent Claudication on Free-Living Cadence. Gait Posture 2015, 41, 414–419. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.W.; Johns, J.A.; Frayne, R.J.; Kimmerly, D.S. Comparison of Habitual Stepping Cadence Analysis Methods: Relationship with Step Counts. Gait Posture 2022, 92, 328–332. [Google Scholar] [CrossRef]
- Hillel, I.; Gazit, E.; Nieuwboer, A.; Avanzino, L.; Rochester, L.; Cereatti, A.; Croce, U.D.; Rikkert, M.O.; Bloem, B.R.; Pelosin, E.; et al. Is Every-Day Walking in Older Adults More Analogous to Dual-Task Walking or to Usual Walking? Elucidating the Gaps between Gait Performance in the Lab and during 24/7 Monitoring. Eur. Rev. Aging Phys. Act. 2019, 16, 6. [Google Scholar] [CrossRef]


| Thigh-Worn 1 | Wrist-Worn 1 | |
|---|---|---|
| Total steps | 20–175 | 20–175 |
| Non-walking steps | 20–44 | 20–44 |
| Slower-paced steps | 20–74 | 20–76 |
| Walking steps | 45–175 | 45–175 |
| Slower-paced walking steps | 45–74 | 45–76 |
| Faster-paced walking steps | 75–175 | 77–175 |
| Baseline N = 608 | 6 Months N = 565 | 12 Months N = 544 | 24 Months N = 504 | |
|---|---|---|---|---|
| Total steps (20–175 steps/min) | 5815 (3186; 100) | 5569 (3256; 100) | 5250 (3017; 100) | 4871 (3039; 100) |
| Non-walking steps (20–44 steps/min) | 4342 (2371; 75) | 4147 (2386; 74) | 3965 (2259; 76) | 3776 (2353; 78) |
| Slower-paced steps (20–62 steps/min) | 4923 (2640; 85) | 4702 (2676, 84) | 4470 (2490; 86) | 4215 (2570, 87) |
| Slower-paced walking steps (45–62 steps/min) | 581 (530; 10) | 555 (544; 10) | 505 (484; 10) | 439 (459; 9) |
| Faster-paced walking steps (63–175 steps/min) | 892 (938; 15) | 867 (996; 16) | 780 (915; 15) | 656 (857; 13) |
| Mean (SD; % of total). | ||||
| Model 1 Total Steps Only | Model 2 Faster-Paced Walking Steps Only | Model 3 Faster-Paced Walking and Slower-Paced Steps | |
|---|---|---|---|
| Total steps (20–175 steps/min) | |||
| Baseline | 0.04 (−0.01–0.08) | N/A | N/A |
| 6 Months | 0.07 (0.02–0.12) ** | N/A | N/A |
| 12 Months | 0.12 (0.07–0.17) *** | N/A | N/A |
| 24 Months | 0.21 (0.15–0.26) *** | N/A | N/A |
| Faster-paced walking steps (63–175 steps/min) | |||
| Baseline | N/A | 0.08 (−0.07–0.23) | 0.05 (−0.12–0.13) |
| 6 Months | N/A | 0.27 (0.10–0.44) ** | 0.22 (0.03–0.41) * |
| 12 Months | N/A | 0.43 (0.25–0.60) *** | 0.35 (0.15–0.55) ** |
| 24 Months | N/A | 0.69 (0.50–0.88) *** | 0.53 (0.32–0.74) *** |
| Slower-paced steps (20–62 steps/min) | |||
| Baseline | N/A | N/A | 0.03 (−0.03–0.10) |
| 6 Months | N/A | N/A | 0.04 (−0.03–0.10) |
| 12 Months | N/A | N/A | 0.06 (−0.01–0.13) |
| 24 Months | N/A | N/A | 0.13 (0.06–0.20) *** |
| Goodness-of-fit | |||
| AIC | 8759 | 8767 | 8749 |
| Log-likelihood | −4352 | −4356 | −4342 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schoenfelder, A.; Metcalf, B.; Langford, J.; Stathi, A.; Western, M.J.; Hillsdon, M. The Analytical and Clinical Validity of the pfSTEP Digital Biomarker of the Susceptibility/Risk of Declining Physical Function in Community-Dwelling Older Adults. Sensors 2023, 23, 5122. https://doi.org/10.3390/s23115122
Schoenfelder A, Metcalf B, Langford J, Stathi A, Western MJ, Hillsdon M. The Analytical and Clinical Validity of the pfSTEP Digital Biomarker of the Susceptibility/Risk of Declining Physical Function in Community-Dwelling Older Adults. Sensors. 2023; 23(11):5122. https://doi.org/10.3390/s23115122
Chicago/Turabian StyleSchoenfelder, Alexander, Brad Metcalf, Joss Langford, Afroditi Stathi, Max J. Western, and Melvyn Hillsdon. 2023. "The Analytical and Clinical Validity of the pfSTEP Digital Biomarker of the Susceptibility/Risk of Declining Physical Function in Community-Dwelling Older Adults" Sensors 23, no. 11: 5122. https://doi.org/10.3390/s23115122