
Automatic Identification of Ultrasound Images of the Tibial Nerve in Different Ankle Positions Using Deep Learning
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
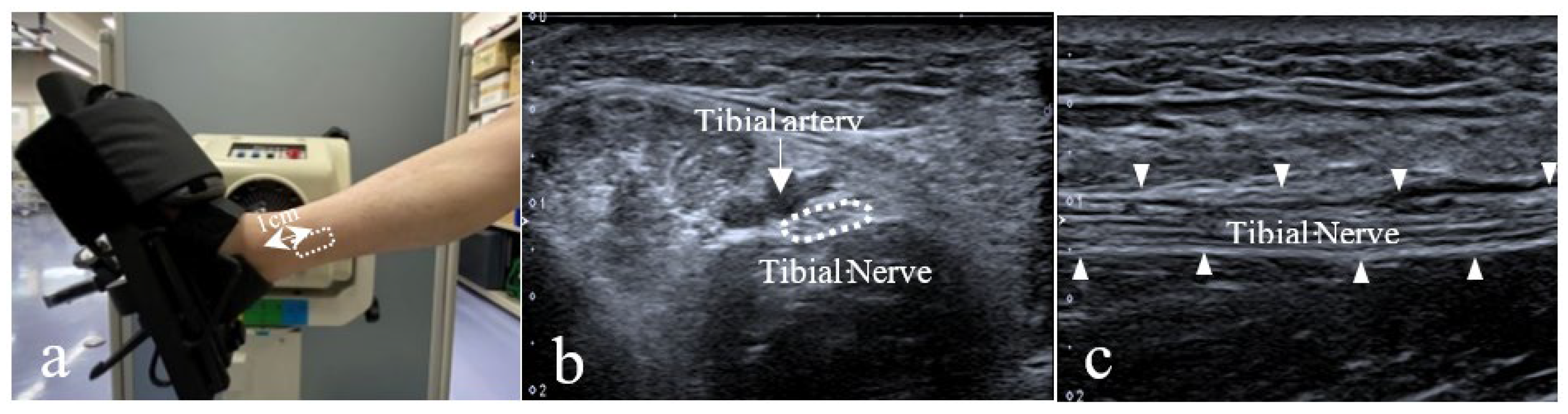
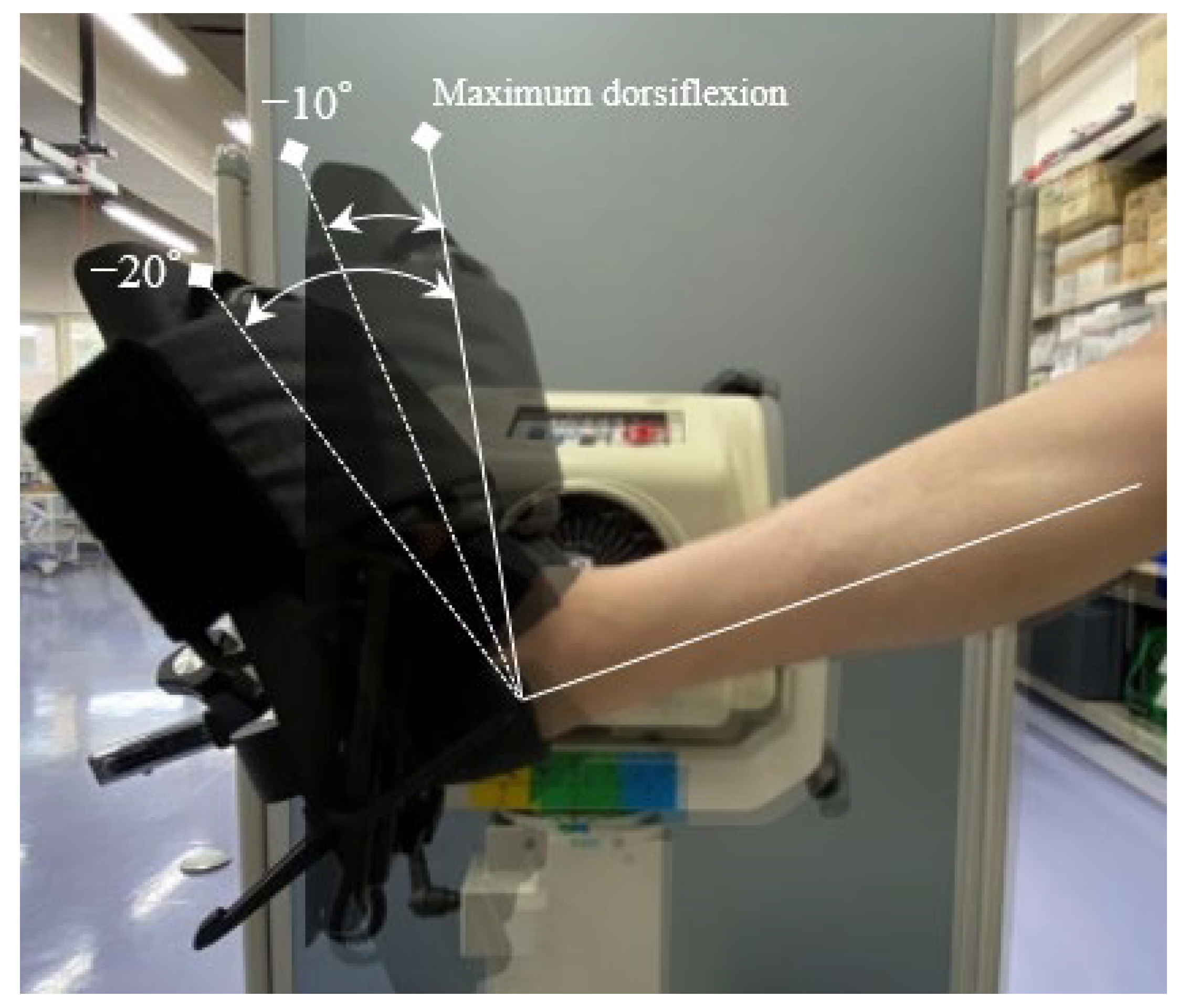
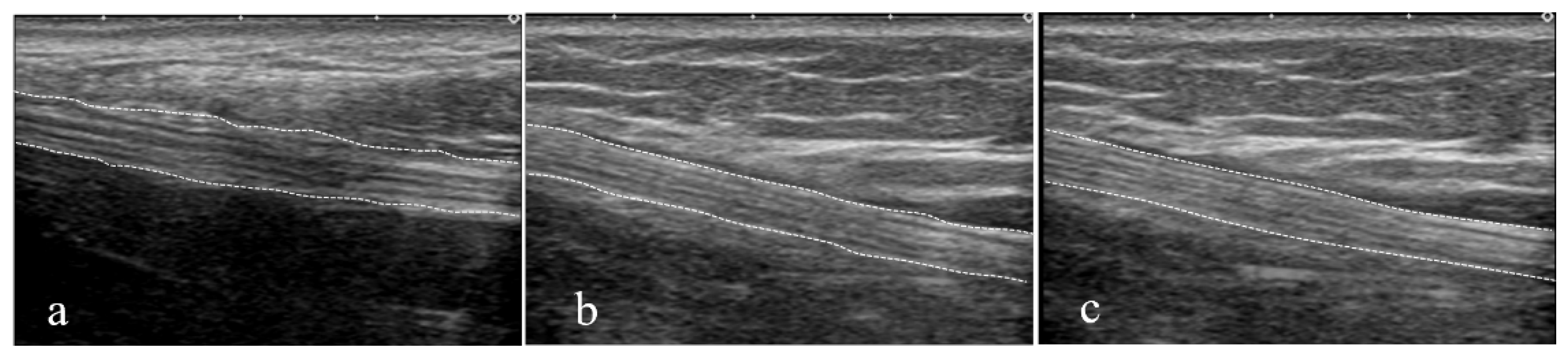
2.2. Ultrasound Image Capturing Method
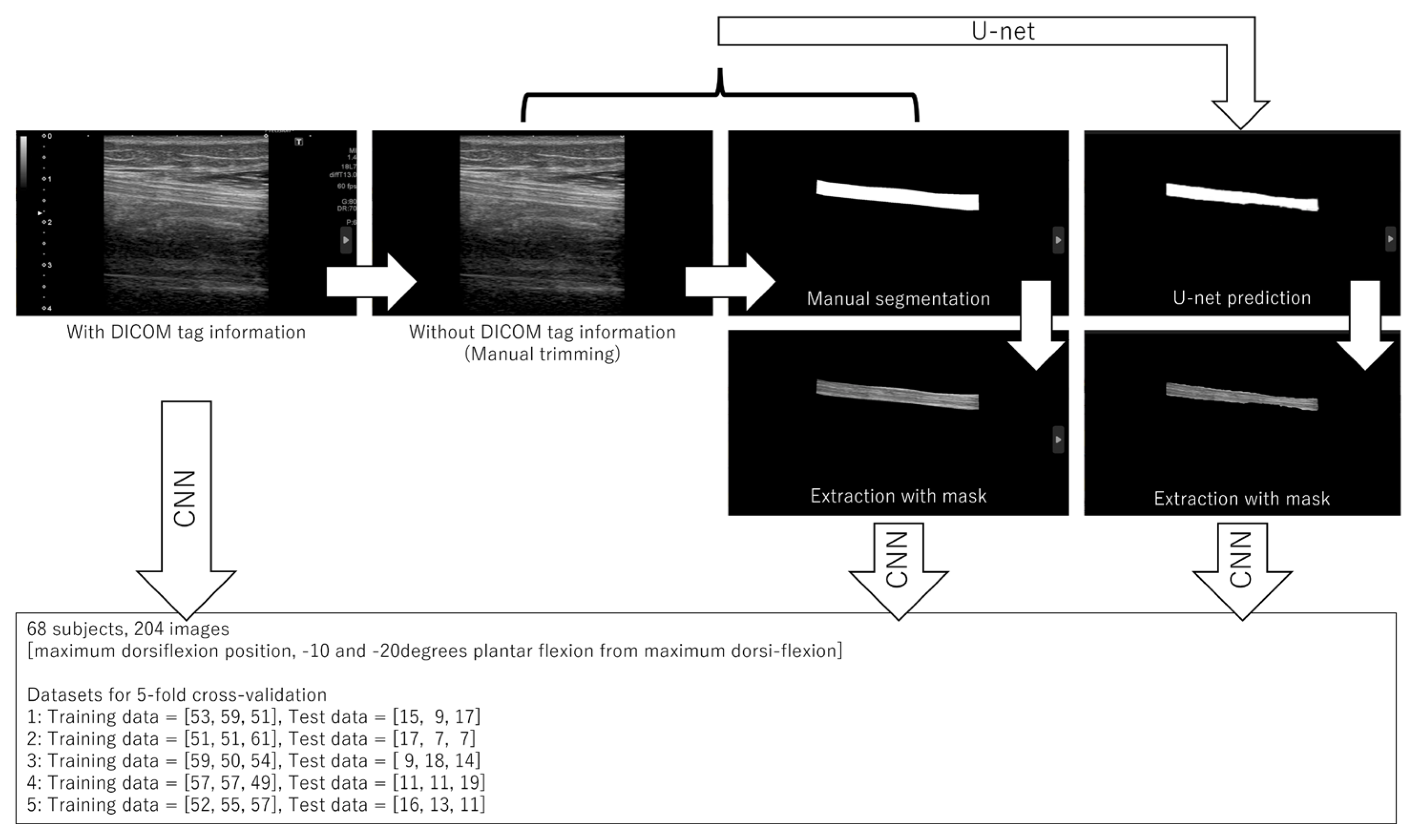
2.3. Manual Segmentation
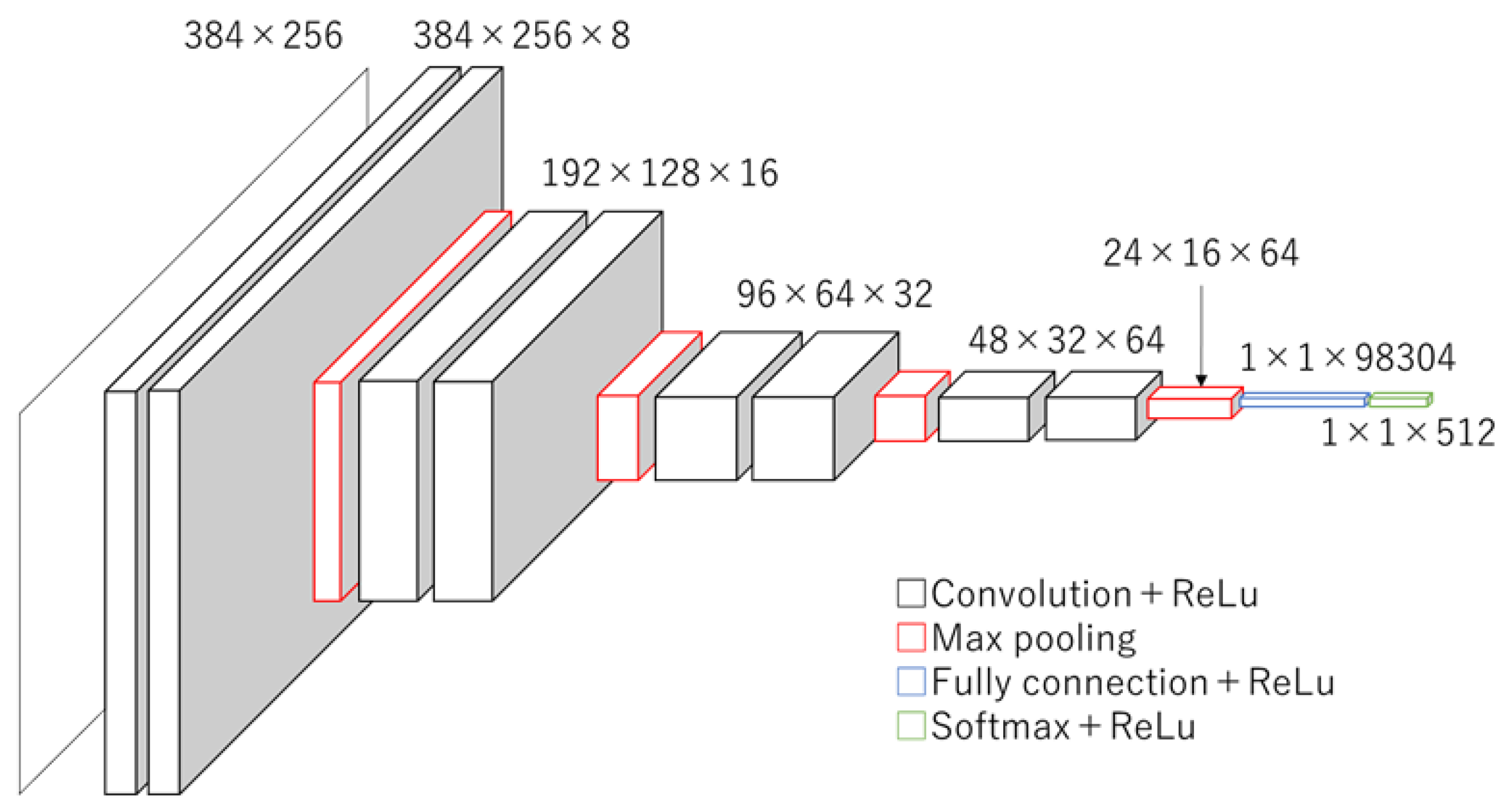
2.4. Convolutional Neural Network (CNN)
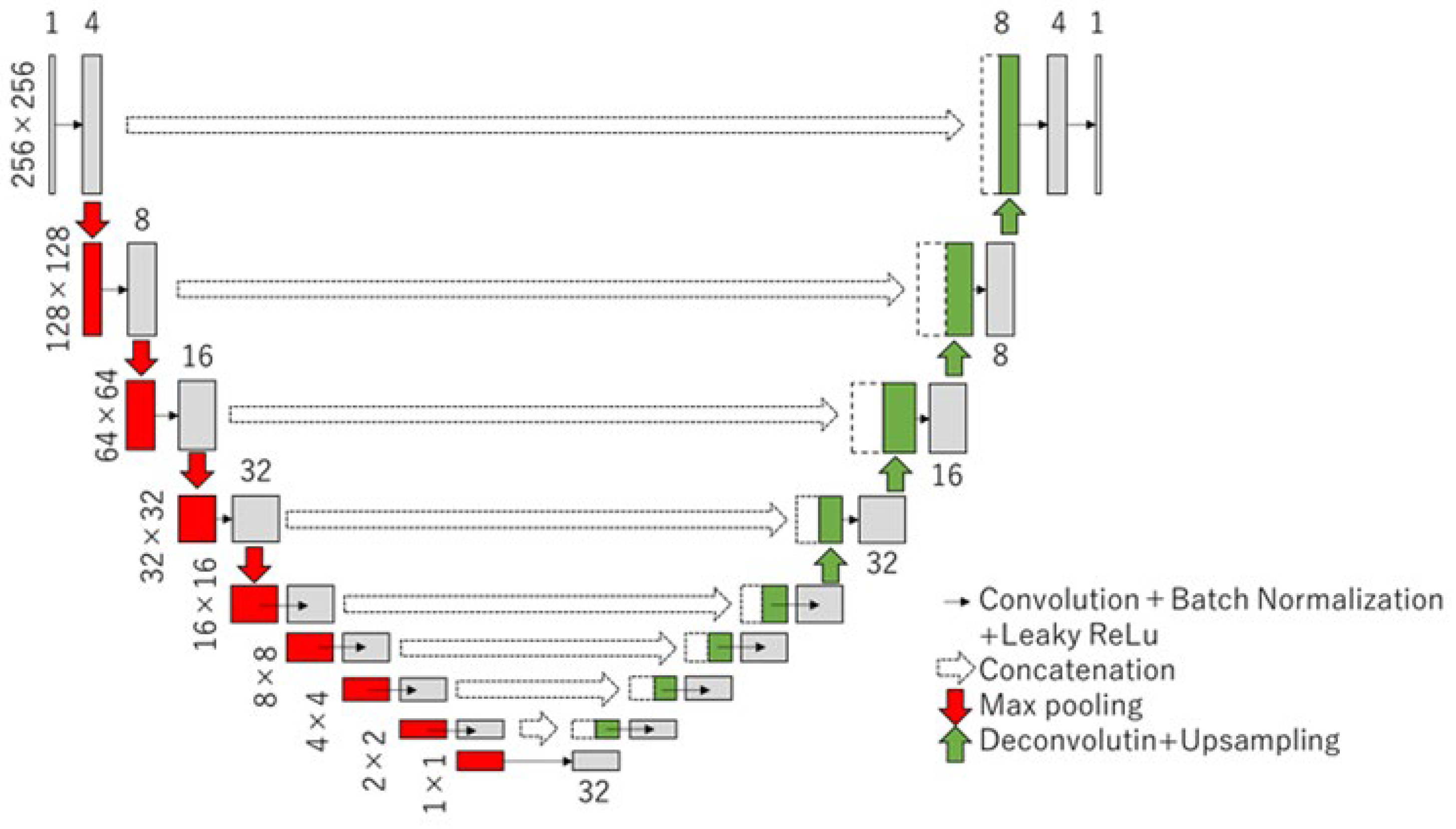
2.5. U-Net
2.6. Validation
3. Results
3.1. Segmentation
3.2. Classification
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moretti, E.; da Silva, I.B.; Boaviagem, A.; Barbosa, L.; de Lima, A.M.J.; Lemos, A. ‘Posterior Tibial Nerve’ or “Tibial Nerve”? Improving the Reporting in Health Papers. Neurourol. Urodyn. 2020, 39, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Mulherin, D.; Price, M. Efficacy of Tibial Nerve Block, Local Steroid Injection or Both in the Treatment of Plantar Heel Pain Syndrome. Foot 2009, 19, 98–100. [Google Scholar] [CrossRef] [PubMed]
- Dyck, P.J.; Overland, C.J.; Low, P.A.; Litchy, W.J.; Davies, J.L.; Dyck, P.J.; O’Brien, P.C.; Cl vs. NPhys Trial Investigators; Albers, J.W.; Andersen, H.; et al. Signs and Symptoms versus Nerve Conduction Studies to Diagnose Diabetic Sensorimotor Polyneuropathy: Cl vs. NPhys Trial. Muscle Nerve 2010, 42, 157–164. [Google Scholar] [CrossRef]
- Turns, M. The Diabetic Foot: An Overview of Assessment and Complications. Br. J. Nurs. 2011, 20 (Suppl. S8), S19–S25. [Google Scholar] [CrossRef]
- Çolak, A.; Kutlay, M.; Pekkafali, Z.; Saraçoglu, M.; Demircan, N.; Simşek, H.; Akin, O.N.; Kibici, K. Use of Sonography in Carpal Tunnel Syndrome Surgery. A Prospective Study. Neurol. Med. Chir. 2007, 47, 109–115. [Google Scholar] [CrossRef]
- Kerasnoudis, A.; Tsivgoulis, G. Nerve Ultrasound in Peripheral Neuropathies: A Review. J. Neuroimaging 2015, 25, 528–538. [Google Scholar] [CrossRef]
- Aslan, M.; Aslan, A.; Emeksiz, H.C.; Candan, F.; Erdemli, S.; Tombul, T.; Gunaydın, G.D.; Kabaalioğlu, A. Assessment of Peripheral Nerves with Shear Wave Elastography in Type 1 Diabetic Adolescents without Diabetic Peripheral Neuropathy. J. Ultrasound Med. 2019, 38, 1583–1596. [Google Scholar] [CrossRef]
- He, Y.; Xiang, X.; Zhu, B.H.; Qiu, L. Shear Wave Elastography Evaluation of the Median and Tibial Nerve in Diabetic Peripheral Neuropathy. Quant. Imaging Med. Surg. 2019, 9, 273–282. [Google Scholar] [CrossRef]
- Liu, S.; Wang, Y.; Yang, X.; Lei, B.; Liu, L.; Li, S.X.; Ni, D.; Wang, T. Deep Learning in Medical Ultrasound Analysis: A Review. Engineering 2019, 5, 261–275. [Google Scholar] [CrossRef]
- Fantino, O.; Bouysset, M.; Pialat, J.B. Can the axial cross-sectional area of the tibial nerve be used to diagnose tarsal tunnel syndrome? An ultrasonography study. Orthop. Traumatol. Surg. Res. 2021, 107, 102630. [Google Scholar] [CrossRef]
- Carroll, M.; Yau, J.; Rome, K.; Hing, W. Measurement of Tibial Nerve Excursion during Ankle Joint Dorsiflexion in a Weight-Bearing Position with Ultrasound Imaging. J. Foot Ankle Res. 2012, 5, 5. [Google Scholar] [CrossRef] [PubMed]
- Kawanishi, K.; Nariyama, Y.; Anegawa, K.; Tsutsumi, M.; Kudo, S. Changes in Tibial Nerve Stiffness during Ankle Dorsiflexion According to In-Vivo Analysis with Shear Wave Elastography. Medicine 2022, 101, e29840. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, F.; Kakimoto, A.; Ota, N.; Ito, S.; Nishizawa, S. Automated segmentation of 2D low-dose CT images of the psoas-major muscle using deep convolutional neural networks. Radiol. Phys. Technol. 2019, 12, 210–215. [Google Scholar] [CrossRef] [PubMed]
- An, S.; Zhou, X.; Zhu, H.; Zhou, F.; Wu, Y.; Yang, T.; Liu, X.; Zhang, Y.; Jiao, Z.; He, Y. Simultaneous Segmentation of Four Cardiac Chambers in Fetal Echocardiography. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Mexico City, Mexico, 1–5 November 2021; pp. 3122–3126. [Google Scholar] [CrossRef]
- Haak, A.; Vegas-Sánchez-Ferrero, G.; Mulder, H.W.; Ren, B.; Kirişli, H.A.; Metz, C.; van Burken, G.; van Stralen, M.; Pluim, J.P.; van der Steen, A.F.; et al. Segmentation of Multiple Heart Cavities in 3-D Transesophageal Ultrasound Images. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2015, 62, 1179–1189. [Google Scholar] [CrossRef] [PubMed]
- Lei, Y.; Fu, Y.; Roper, J.; Higgins, K.; Bradley, J.D.; Curran, W.J.; Liu, T.; Yang, X. Echocardiographic Image Multi-Structure Segmentation Using Cardiac-SegNet. Med. Phys. 2021, 48, 2426–2437. [Google Scholar] [CrossRef] [PubMed]
- Belasso, C.J.; Behboodi, B.; Benali, H.; Boily, M.; Rivaz, H.; Fortin, M. LUMINOUS Database: Lumbar Multifidus Muscle Segmentation from Ultrasound Images. BMC Musculoskelet. Disord. 2020, 21, 703. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, A.R.; Drukker, K.; Giger, M.L. Breast Image Feature Learning with Adaptive Deconvolutional Networks. SPIE Proc. 2012, 8315, 831506. [Google Scholar] [CrossRef]
- Guo, L.; Wang, D.; Xu, H.; Qian, Y.; Wang, C.; Zheng, X.; Zhang, Q.; Shi, J. CEUS-Based Classification of Liver Tumors with Deep Canonical Correlation Analysis and Multi-kernel Learning. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Republic of Korea, 11–15 July 2017; pp. 1748–1751. [Google Scholar] [CrossRef]
- Ma, J.; Wu, F.; Zhu, J.; Xu, D.; Kong, D. A Pre-trained Convolutional Neural Network Based Method for Thyroid Nodule Diagnosis. Ultrasonics 2017, 73, 221–230. [Google Scholar] [CrossRef]
- Wu, L.; Cheng, J.Z.; Li, S.; Lei, B.; Wang, T.; Ni, D. FUIQA: Fetal Ultrasound Image Quality Assessment with Deep Convolutional Networks. IEEE Trans. Cybern. 2017, 47, 1336–1349. [Google Scholar] [CrossRef]
- Alshami, A.M.; Babri, A.S.; Souvlis, T.; Coppieters, M.W. Strain in the Tibial and Plantar Nerves with Foot and Ankle Movements and the Influence of Adjacent Joint Positions. J. Appl. Biomech. 2008, 24, 368–376. [Google Scholar] [CrossRef]
- Coppieters, M.W.; Alshami, A.M.; Babri, A.S.; Souvlis, T.; Kippers, V.; Hodges, P.W. Strain and Excursion of the Sciatic, Tibial, and Plantar Nerves during a Modified Straight Leg Raising Test. J. Orthop. Res. 2006, 24, 1883–1889. [Google Scholar] [CrossRef] [PubMed]
- Sunderland, S.S. The Anatomy and Physiology of Nerve Injury. Muscle Nerve 1990, 13, 771–784. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class | Set 1 | Set 2 | Set 3 | Set 4 | Set 5 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Training | Test | Training | Test | Training | Test | Training | Test | Training | Test | |
| Md −20 | 53 | 15 | 51 | 17 | 59 | 9 | 57 | 11 | 52 | 16 |
| Md −10 | 59 | 9 | 51 | 17 | 50 | 18 | 57 | 11 | 55 | 13 |
| Md | 51 | 17 | 61 | 7 | 54 | 14 | 49 | 19 | 57 | 11 |
| Intersection over Union | Cross-Sectional Area Ratio | |
|---|---|---|
| 1 | 0.81 | 1 |
| 2 | 0.79 | 0.99 |
| 3 | 0.80 | 0.94 |
| 4 | 0.81 | 1 |
| 5 | 0.82 | 0.98 |
| Accuracy Average | 0.81 | 0.98 |
| Raw Data | Manual Segmentation | Full Auto Segmentation | ||||
|---|---|---|---|---|---|---|
| Accuracy | F-Value | Accuracy | F-Value | Accuracy | F-Value | |
| 1 | 0.37 | - | 0.98 | 0.98 | 0.83 | 0.82 |
| 2 | 0.59 | - | 0.95 | 0.95 | 0.80 | 0.79 |
| 3 | 0.22 | - | 0.83 | 0.83 | 0.66 | 0.67 |
| 4 | 0.27 | - | 0.93 | 0.93 | 0.80 | 0.81 |
| 5 | 0.73 | - | 0.93 | 0.93 | 0.75 | 0.73 |
| Average | 0.44 | - | 0.92 | 0.92 | 0.77 | 0.76 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawanishi, K.; Kakimoto, A.; Anegawa, K.; Tsutsumi, M.; Yamaguchi, I.; Kudo, S. Automatic Identification of Ultrasound Images of the Tibial Nerve in Different Ankle Positions Using Deep Learning. Sensors 2023, 23, 4855. https://doi.org/10.3390/s23104855
Kawanishi K, Kakimoto A, Anegawa K, Tsutsumi M, Yamaguchi I, Kudo S. Automatic Identification of Ultrasound Images of the Tibial Nerve in Different Ankle Positions Using Deep Learning. Sensors. 2023; 23(10):4855. https://doi.org/10.3390/s23104855
Chicago/Turabian StyleKawanishi, Kengo, Akihiro Kakimoto, Keisuke Anegawa, Masahiro Tsutsumi, Isao Yamaguchi, and Shintarou Kudo. 2023. "Automatic Identification of Ultrasound Images of the Tibial Nerve in Different Ankle Positions Using Deep Learning" Sensors 23, no. 10: 4855. https://doi.org/10.3390/s23104855