


Postsurgical Analysis of Gait, Radiological, and Functional Outcomes in Children with Developmental Dysplasia of the Hip

 , ,
, ,  , and
, and
Abstract
:1. Introduction
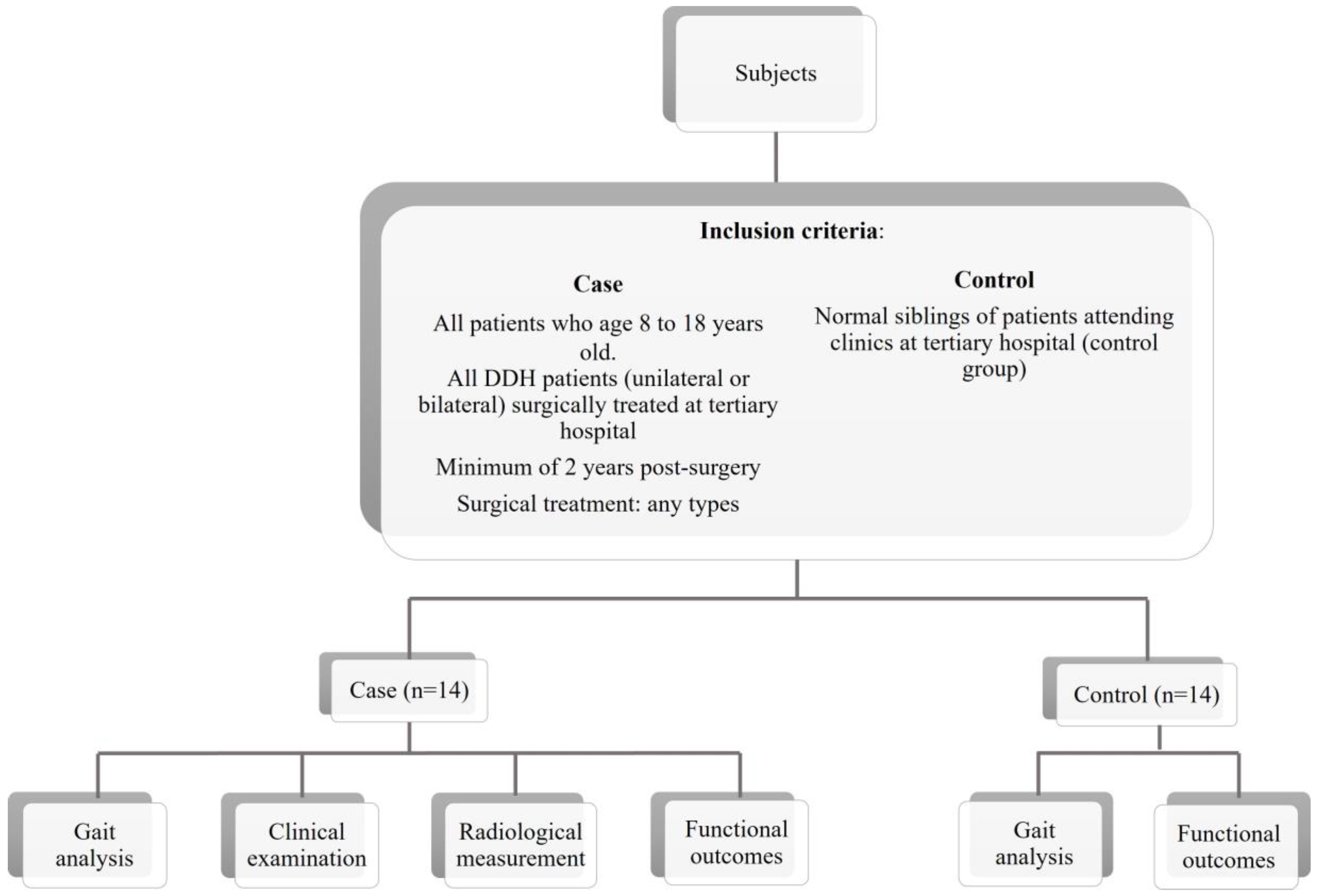
2. Materials and Methods
3. Results
3.1. Patient Demographics
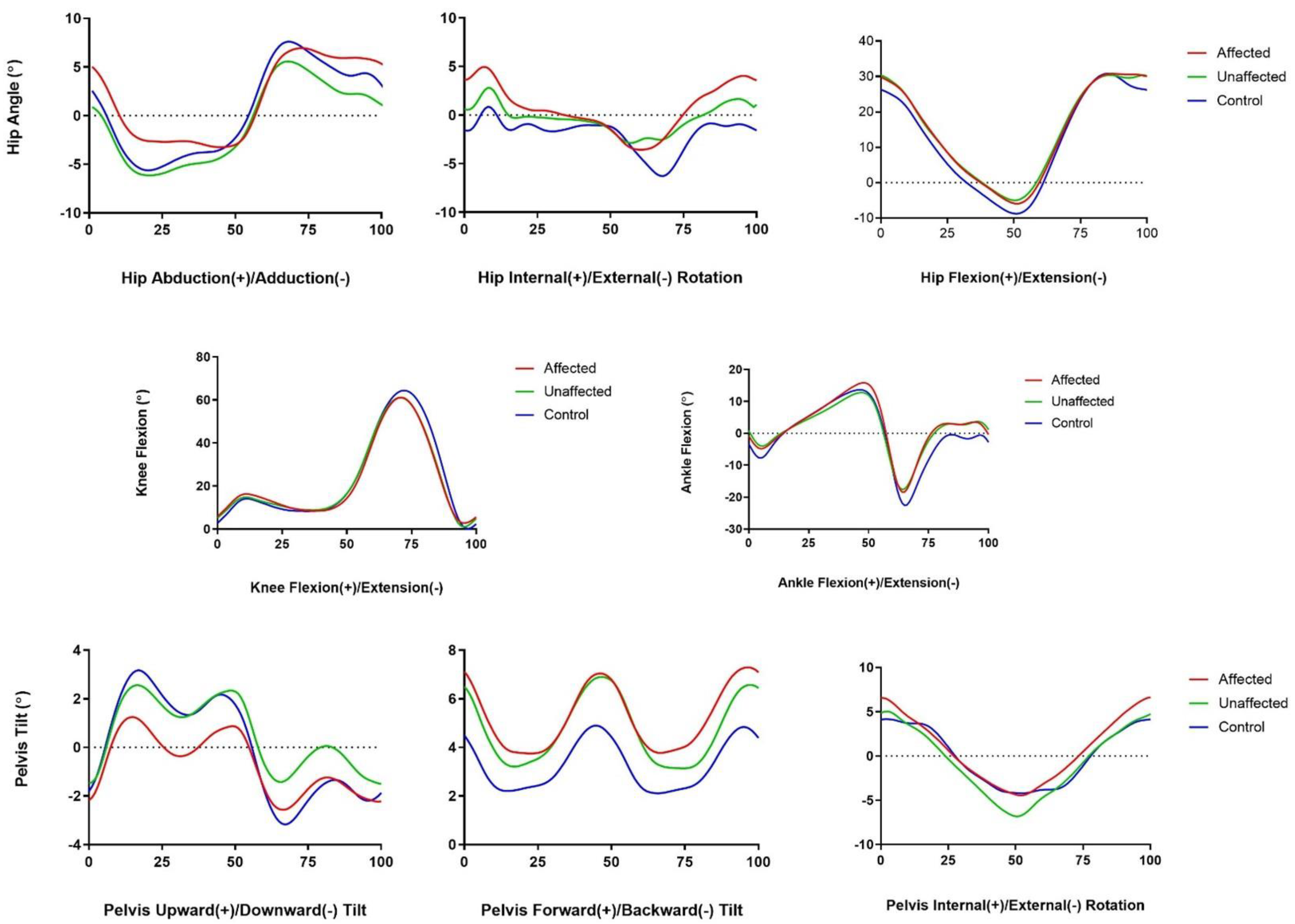
3.2. Gait Outcome
3.3. Radiological Outcomes
3.4. Functional Outcomes
3.5. Risk Factors Associations with Outcome in Children with DDH
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chang, C.-F.; Wang, T.-M.; Wang, J.-H.; Huang, S.-C.; Lu, T.-W. Residual gait deviations in adolescents treated during infancy for unilateral developmental dysplasia of the hip using Pemberton’s osteotomy. Gait Posture 2012, 35, 561–566. [Google Scholar] [CrossRef]
- Al-Essa, R.S.; Aljahdali, F.H.; Alkhilaiwi, R.M.; Philip, W.; Jawadi, A.H.; Khoshhal, K. Diagnosis and treatment of developmental dysplasia of the hip: A current practice of paediatric orthopaedic surgeons. J. Orthop. Surg. 2017, 2, 2309499017717197. [Google Scholar] [CrossRef] [Green Version]
- Pollet, V.; Percy, V.; Prior, H.J. Relative risk and incidence for developmental dysplasia of the hip. J. Pediatr. 2017, 181, 202–207. [Google Scholar] [CrossRef]
- Zamborsky, R.; Kokavec, M.; Harsanyi, S.; Attia, D.; Danisovic, L. Developmental dysplasia of hip: Perspectives in genetic screening. Med. Sci. 2019, 7, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadat-Ali, M. Developmental Dysplasia of the Hip (DDH) in Saudi Arabia: Time to Wake up. A Systematic Review (1980–2018). Open J. Epidemiol. 2020, 10, 125. [Google Scholar] [CrossRef] [Green Version]
- Vasilcova, V. Pilot study: Effect of developmental dysplasia of the hip on the gait and feet posture. Stud. Sport. 2022, 16, 134–142. [Google Scholar] [CrossRef]
- Storer, S.K.; Skaggs, D.L. Developmental dysplasia of the hip. Am. Fam. Physician 2006, 74, 1310–1316. [Google Scholar]
- Bjerkreim, I.; Arseth, P.H.; Palmen, K. Congenital dislocation of the hip in Norway late diagnosis CDH in the years 1970 to 1974. Acta Pædiatrica 1978, 67, 329–332. [Google Scholar] [CrossRef]
- Haasbeek, J.F.; Wright, J.G.; Hedden, D.M. Is there a difference between the epidemiologic characteristics of hip dislocation diagnosed early and late? Can. J. Surg. 1995, 38, 437–448. [Google Scholar] [PubMed]
- Wilkinson, J.A. A post-natal survey for congenital displacement of the hip. J. Bone Jt. Surg. Br. Vol. 1972, 54, 40–49. [Google Scholar] [CrossRef]
- Jain, R.K.; Patel, S. Developmental dysplasia of hip—An overview. Int. J. Orthop. Sci. 2017, 3, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Loder, R.T.C.; Shafer, C. The demographics of developmental hip dysplasia in the Midwestern United States (Indiana). J. Child. Orthop. 2015, 9, 93–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pirker, W.; Katzenschlager, R. Gait disorders in adults and the elderly. Wien. Klin. Wochenschr. 2017, 129, 81–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ur Razaq, M.N.; Younas, M.; Awan, A.S.; Waqas, M.; Alam, M.I.; Khan, I.U. Risk factors leading to developmental complications after open reduction in developmental dysplasia of hip. J. Ayub Med. Coll. Abbottabad 2016, 28, 26–28. [Google Scholar]
- Lee, W.C.; Chen, T.Y.; Hung, L.W.; Wang, T.-M.; Chang, C.-H.; Lu, T.-W. Increased Loading Rates During Gait Correlate with Morphology of Unaffected Hip in Juveniles with Treated Developmental Hip Dysplasia. Front. Bioeng. Biotechnol. 2021, 9, 704266. [Google Scholar] [CrossRef] [PubMed]
- Czubak, J.; Kowalik, K.; Kawalec, A.; Kwiatkowska, M. Dega pelvic osteotomy: Indications, results and complications. J. Child. Orthop. 2018, 12, 342–348. [Google Scholar] [CrossRef]
- Arshad, L.; Areeful Haque, M.; Bukhari, S.N.A.; Jantan, I. An overview of structure-Activity relationship studies of curcumin analogs as antioxidant and anti-inflammatory agents. Future Med. Chem. 2017, 9, 605–626. [Google Scholar] [CrossRef]
- Roposch, A.; Liu, L.Q.; Offiah, A.C.; Wedge, J.H. Functional outcomes in children with osteonecrosis secondary to treatment of developmental dysplasia of the hip. J. Bone Joint. Surg. Am. 2011, 93, e145. [Google Scholar] [CrossRef]
- Agostiniani, R.; Atti, G.; Bonforte, S.; Casini, C.; Cirillo, M.; De Pellegrin, M.; Di Bello, D.; Esposito, F.; Galla, A.; Brunenghi, G.M.; et al. Recommendations for early diagnosis of Developmental Dysplasia of the Hip (DDH): Working group intersociety consensus document. Ital. J. Pediatr. 2020, 46, 150. [Google Scholar] [CrossRef]
- Wang, C.W.; Wang, T.M.; Wu, K.W.; Huang, S.-C.; Kuo, K.N. The comparative, long-term effect of the Salter osteotomy and Pemberton acetabuloplasty on pelvic height, scoliosis and functional outcome. Bone Jt. J. 2016, 98, 1145–1150. [Google Scholar] [CrossRef]
- Nie, Y.; Ning, N.; Pei, F.; Shen, B.; Zhou, Z.; Li, Z. Gait kinematic deviations in patients with developmental dysplasia of the hip treated with total hip arthroplasty. Orthopedics 2017, 40, e425–e431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saqib, M.; Salman, M.; Hayat, S.; Khan, M.A.; Ullah, S. Developmental Dysplasia of The Hip In Older Children; Prospects Of Functional And Radiological Outcome Following A Single Stage Triple Procedure. J. Ayub Med. Coll. Abbottabad 2019, 31, 427–431. [Google Scholar] [PubMed]
- Gahramanov, A.; İnanıcı, F.; Çağlar, Ö.; Aksoy, C.; Tokgözoğlu, A.M.; Güner, S.; Baki, A.; Atilla, B. Functional results in periacetabular osteotomy: Is it possible to obtain a normal gait after the surgery? Hip Int. 2017, 27, 449–454. [Google Scholar] [CrossRef]
- Nishimura, M.; Takahira, N.; Fukushima, K.; Yamamoto, T.; Moriya, M.; Uchiyama, K. Early gait analysis after curved periacetabular osteotomy for acetabular dysplasia. Orthop. Res. Rev. 2015, 25, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Jamil, K.; Saharuddin, R.; Abd Rasid, A.F.; Rashid, A.H.A.; Ibrahim, S. Outcome of open reduction alone or with concomitant bony procedures for developmental dysplasia of the hip (DDH). Children 2022, 9, 1213. [Google Scholar] [CrossRef]
- Vasilcova, V.; AlHarthi, M.; Jawadi, A.H.; Zvonař, M. The Use of Visual Analysis for Gait and Foot Posture in Children with Developmental Dysplasia of the Hip. Diagnostics 2023, 13, 973. [Google Scholar] [CrossRef]
- Omeroğlu, H.; Yavuzer, G.; Biçimoğlu, A.; Ağuş, H.; Tümer, Y. No detectable major changes in gait analysis after soft tissue release in DDH. Clin. Orthop. Relat. Res. 2008, 466, 856–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karaismailoglu, B.; Erdogan, F.; Kaynak, G. High Hip Center Reduces the Dynamic Hip Range of Motion and Increases the Hip Load: A Gait Analysis Study in Hip Arthroplasty Patients With Unilateral Developmental Dysplasia. J. Arthroplast. 2019, 34, 1267–1272.e1. [Google Scholar] [CrossRef]
- Passmore, E.; Pandy, M.G.; Graham, H.K.; Sangeux, M. Measuring Femoral Torsion In Vivo Using Freehand 3-D Ultrasound Imaging. Ultrasound Med. Biol. 2016, 42, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Passmore, E.; Sangeux, M. Defining the medial-lateral axis of an anatomical femur coordinate system using freehand 3D ultrasound imaging. Gait Posture 2016, 45, 211–216. [Google Scholar] [CrossRef]
- Fjerstad, B.M.; Hammer, R.L.; Hammer, A.M.; Connolly, G.; Lomond, K.V.; O’connor, P. Comparison of Two Static Stretching Procedures on Hip Adductor Flexibility and Strength. Int. J. Exerc. Sci. 2018, 11, 1074–1085. [Google Scholar]
- Kolk, S.; Fluit, R.; Luijten, J.; Heesterbeek, P.J.; Geurts, A.C.; Verdonschot, N.; Weerdesteyn, V. Gait and lower limb muscle strength in women after triple innominate osteotomy. BMC Musculoskelet. Disord. 2015, 16, 68. [Google Scholar] [CrossRef] [Green Version]
- Leijendekkers, R.A.; Marra, M.A.; Kolk, S.; Van Bon, G.; Schreurs, B.W.; Weerdesteyn, V.; Verdonschot, N. Gait symmetry and hip strength in women with developmental dysplasia following hip arthroplasty compared to healthy subjects: A cross-sectional study. PLoS ONE 2018, 13, e0193487. [Google Scholar] [CrossRef] [Green Version]
- Wadsworth, J.B.; Smidt, G.L.; Johnston, R.C. Gait characteristics of subjects with hip disease. Phys. Ther. 1972, 52, 829–839. [Google Scholar] [CrossRef] [PubMed]
- Kothari, A.; Grammatopoulos, G.; Hopewell, S.; Theologis, T. How Does Bony Surgery Affect Results of Anterior Open Reduction in Walking-age Children With Developmental Hip Dysplasia? Clin. Orthop. Relat. Res. 2016, 474, 1199–1208. [Google Scholar] [CrossRef] [Green Version]
- Castañeda, P.; Masrouha, K.Z.; Ruiz, C.V.; Moscona-Mishy, L. Outcomes following open reduction for late-presenting developmental dysplasia of the hip. J. Child. Orthop. 2018, 12, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Hu, W.; Xun, F.; Lin, X.; Li, J.; Yuan, Z.; Liu, Y.; Canavese, F.; Xu, H. Risk factors associated with unsatisfactory hip function in children with late-diagnosed developmental dislocation of the hip treated by open reduction. Orthop. Traumatol. Surg. Res. 2020, 106, 1373–1381. [Google Scholar] [CrossRef] [PubMed]
- Eamsobhana, P.; Saisamorn, K.; Sisuchinthara, T.; Jittivilai, T.; Keawpornsawan, K. The Factor Causing Poor Results in Late Developmental Dysplasia of the Hip (DDH). J. Med. Assoc. Thai. 2015, 98 (Suppl. S8), S32–S37. [Google Scholar] [PubMed]
- Chen, Q.; Deng, Y.; Fang, B. Outcome of one-stage surgical treatment of developmental dysplasia of the hip in children from 1.5 to 6 years old. A retrospective study. Acta Orthop. Belg. 2015, 81, 375–383. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients with DDH (n = 14) | Controls (n = 14) | p-Value | |
|---|---|---|---|
| Age at follow up | 12.00 ± 2.83 | 12.79 ± 2.16 | 0.416 |
| 8 years old and younger | 2 (14.3%) | 0 (0%) | |
| 9–11 years old | 4 (28.6%) | 4 (28.6%) | |
| 12–14 years old | 6 (42.9%) | 7 (50%) | |
| 15 years old and older | 2 (14.3%) | 3 (21.4%) | |
| Height | 1.43 ± 0.11 | 1.46 ± 0.07 | 0.440 |
| Weight | 51.02 ± 18.52 | 40.86 ± 11.28 | 0.091 |
| Sex | |||
| Male | 3 (21.4%) | 3 (21.4%) | |
| Female | 11 (78.6%) | 11 (78.6%) | |
| Type of surgery | |||
| Open reduction | 7 (50%) | ||
| Femoral osteotomy | 1 (7.1%) | ||
| Pelvic osteotomy | 5 (35.7%) | ||
| Combined osteotomy | 1 (7.1%) | ||
| Age during surgery | 33.36 ± 27.89 | ||
| 24 months old and younger | 6 (42.8%) | ||
| 24–36 months old | 4 (28.6%) | ||
| 37–48 months old | 2 (14.3%) | ||
| 49 months old and older | 2 (14.3%) | ||
| Affected hip side | |||
| Right | 4 (28.6%) | ||
| Left | 10 (64.3%) | ||
| Bilateral | 1 (7.1%) |
| Measurement | Mean Value among Children with DDH | Mean Value among Control Children | Affected vs. Control | Affected vs. Unaffected | |
|---|---|---|---|---|---|
| Affected | Unaffected | p-Value | p-Value | ||
| Swing phase duration (s) | 0.49 ± 0.06 | 0.49 ± 0.07 | 0.43 ± 0.02 | <0.001 ** | 0.877 |
| Swing phase per gait cycle (%) | 44.62 ± 4.80 | 43.88 ± 4.86 | 40.49 ± 1.45 | <0.001 ** | 0.687 |
| Stance phase per gait cycle (%) | 51.97 ± 14.98 | 56.11 ± 4.93 | 59.48 ± 1.46 | 0.011 * | 0.351 |
| Single support phase duration (s) | 0.49 ± 0.07 | 0.49 ± 0.06 | 0.43 ± 0.02 | <0.001 ** | 0.785 |
| Single support per gait cycle (%) | 44.77 ± 5.20 | 43.67 ± 4.31 | 40.48 ± 1.44 | <0.001 ** | 0.550 |
| Double support phase duration (s) | 0.07 ± 0.04 | 0.08 ± 0.05 | 0.10 ± 0.02 | 0.001 * | 0.608 |
| Double support per gait cycle (%) | 6.20 ± 3.68 | 6.89 ± 3.93 | 9.50 ± 1.50 | <0.001 ** | 0.636 |
| Loading response duration (s) | 0.07 ± 0.04 | 0.08 ± 0.05 | 0.10 ± 0.02 | 0.001 * | 0.608 |
| Loading response per gait cycle (%) | 6.20 ± 3.68 | 6.89 ± 3.93 | 9.59 ± 1.63 | <0.001 ** | 0.636 |
| Midstance duration (s) | 0.24 ± 0.06 | 0.23 ± 0.04 | 0.20 ± 0.02 | 0.002 * | 0.579 |
| Midstance per gait cycle (%) | 22.08 ± 5.47 | 21.02 ± 3.35 | 18.80 ± 2.65 | 0.011 * | 0.550 |
| Preswing duration (s) | 0.07 ± 0.05 | 0.08 ± 0.04 | 0.10 ± 0.02 | 0.002 * | 0.756 |
| Outcomes | Gender | Type of Surgery | Age during Surgery | Height | Weight |
|---|---|---|---|---|---|
| Gait Outcome | |||||
| Min Pelvic Tilt (Backward) | 0.022 * | <0.001 ** | <0.001 ** | <0.001 ** | <0.001 ** |
| Max Pelvic Tilt (Forward) | 0.032 * | 0.001 * | <0.001 ** | <0.001 ** | <0.001 ** |
| Gait Cycle Duration | 0.014 * | 0.004 * | <0.001 ** | <0.001 ** | <0.001 ** |
| Step Duration | 0.100 | 0.179 | 0.049 * | 0.014 * | 0.031 * |
| Stance Phase Duration | 0.270 | 0.099 | 0.021 * | 0.100 | 0.050 |
| Radiological Outcome | |||||
| Bucholz and Olden Classification | 0.236 | <0.001 ** | <0.001 ** | 0.020 * | <0.001 ** |
| Severin Classification | 0.712 | 0.003 * | 0.001 * | 0.039 * | 0.001 * |
| Functional Outcome | |||||
| CHOHES Pain | 0.443 | 0.146 | 0.009 * | 0.545 | 0.009 * |
| CHOHES Function | 0.372 | 0.003 * | 0.001 * | 0.010 * | 0.001 * |
| CHOHES Physical Examination | 0.037 * | <0.001 ** | <0.001 ** | 0.001 * | <0.001 ** |
| Total CHOHES Score | 0.007 * | <0.001 ** | <0.001 ** | <0.001 ** | <0.001 ** |
| Outcomes | Age during Surgery OR (CI; p-Value) | Height OR (CI; p-Value) | Weight OR (CI; p-Value) | Femoral Osteotomy OR (CI; p-Value) | Combined Osteotomy OR (CI; p-Value) |
|---|---|---|---|---|---|
| Min Pelvic Tilt (Back) | −5.37 (−1.85–−1.54; 0.023 *) | ||||
| Max Pelvic Tilt (Forward) | −5.25 (−2.02–−0.25; 0.014 *) | ||||
| Gait Cycle Duration | −2.00 (−2.97–−0.86; 0.001 *) | 7.43 (0.03–0.06; <0.001 *) | −0.95 (−0.29–−0.13; <0.001 *) | ||
| Stance Phase Duration | 0.42 (0.00–0.00; 0.028 *) | ||||
| Severin Classification | 0.68 (0.54–2.12; 0.002 *) | 0.49 (0.27–2.18; 0.015 *) | |||
| CHOHES Function | −1.06 (−0.13–−0.03; 0.004 *) | −3.55 (−0.81–0.01; 0.045 *) | |||
| CHOHES PE | −0.75 (−0.07–−0.00; 0.028 *) | −3.23 (−0.43–−0.03; 0.029 *) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aslam, F.; Jamil, K.; Htwe, O.; Yuliawiratman, B.S.; Natarajan, E.; Elamvazuthi, I.; Naicker, A.S. Postsurgical Analysis of Gait, Radiological, and Functional Outcomes in Children with Developmental Dysplasia of the Hip. Sensors 2023, 23, 3386. https://doi.org/10.3390/s23073386
Aslam F, Jamil K, Htwe O, Yuliawiratman BS, Natarajan E, Elamvazuthi I, Naicker AS. Postsurgical Analysis of Gait, Radiological, and Functional Outcomes in Children with Developmental Dysplasia of the Hip. Sensors. 2023; 23(7):3386. https://doi.org/10.3390/s23073386
Chicago/Turabian StyleAslam, Firdaus, Kamal Jamil, Ohnmar Htwe, Brenda Saria Yuliawiratman, Elango Natarajan, Irraivan Elamvazuthi, and Amaramalar Selvi Naicker. 2023. "Postsurgical Analysis of Gait, Radiological, and Functional Outcomes in Children with Developmental Dysplasia of the Hip" Sensors 23, no. 7: 3386. https://doi.org/10.3390/s23073386