2.1. Participants and Data Collection
The study is based on data collected with wearable PPG devices during two scientific expeditions of the HIGHCARE projects (
www.highcareprojects.eu accessed on 6 April 2022). The experiments of the expeditions, both conducted in agreement with the principles of the Declaration of Helsinki, allow us to investigate distinct aspects related to the feasibility of HRV analysis by PPG during sleep. The HIGHCARE-ALPS 2010 expedition provides us with data on a relatively large group of participants (
n= 21, see details below) sojourning at a high altitude on Mt. Rosa, in the Italian Alps. These data allow us to quantify the discrepancies between PPG-derived and ECG-derived measures of sleep HRV in human models that simulate sleep-related breathing disorders with a broad range of severity. By contrast, the HIGHCARE-HIMALAYA expedition provides us with data from a small group of professional mountaineers (
n = 5) who attempted to climb the Mt. Everest summit. We also considered this small group of participants for two reasons. First, nighttime sleep recordings at such high altitudes are extremely rare and the data in five participants measured twice while sleeping in tents at very high camps provide precious information for understanding the feasibility of sleep studies by wearable PPG devices even in extreme high-mountain environments. Second, although the sample size is too small for obtaining solid statistical conclusions on the effects of high altitude on sleep HRV, it nevertheless may qualitatively describe whether the alterations quantified by PPG and ECG are comparable and consistent with each other. Details on the two expeditions follow.
Mt. Rosa expedition (EudraCT No. 2010-019986-27). In the summer of 2010, 41 volunteers of the Italian Alps expedition ascended in about 28 h from Milan to the Margherita Hut (4554 m a.s.l. on Mt. Rosa, Italian Alps), where they spent five days participating in a randomized study on the efficacy of acetazolamide vs. placebo as a treatment against symptoms of acute mountain sickness [
18]. Acetazolamide is expected to modify the chemoreflex response to hypobaric hypoxia. Details on the recruitment, drug and placebo administration, and general characteristics of the whole group of participants are reported in the
supplemental document. All participants underwent polysomnography starting on the evening of the third day of their stay. Twenty-one of them (11 males and 10 females, age between 24.4 and 42.7 years, body mass index between 17.2 and 27.1 kg/m
2, 12 taking acetazolamide and 9 a placebo) were instrumented with a wearable monitoring system called Maglietta Interattiva Computerizzata (MagIC). MagIC included two woven ECG electrodes (sampled at 200 Hz and 12 bit), a textile plethysmograph for measuring respiratory movements of the thorax (50 Hz, 12 bit), and a triaxial accelerometer (50 Hz, 12 bit), and it was connected to a Nonin Xpod
® device (Nonin Medical, Inc., Plymouth, MN, USA), which used red and infrared LEDs to record oxygen saturation (3 Hz, 8 bit) and a finger plethysmogram (75 Hz, 8 bit) [
19]. The recording lasted about 10 h and covered the whole period of night-time sleep.
Mt. Everest expedition (EudraCT No. 2008-000540-14). Among the participants of the Himalayan expedition, we considered five male alpine guides (age between 29 and 54 years, body mass index between 21.1 and 24.2 kg/m
2) who attempted to reach the summit of Mt. Everest while being monitored during the night by the MagIC device (details on the recruitment, drug and placebo administration, and general characteristics of the whole group of participants are reported in the
supplemental document). None of these five participants was taking any drugs or non-pharmacological interventions against mountain sickness. They performed the first nighttime recording in Milan (at a height of 120 m, approximately at sea level) wearing the MagIC system with the finger PPG device (see Mt. Rosa expedition section). After flight transportation to the village of Namche Bazar and a six-day trek, the five mountaineers reached the Mt. Everest base camp (5400 m) for a 12-day acclimation before moving to Camp 1 at 6000 m a.s.l. Here they performed a second nighttime recording with MagIC, sleeping within a tent. Due to adverse weather conditions, only four of the five mountaineers reached Camp 2 at 6800 m a.s.l., where they performed the third nighttime recording in the tent before returning to the base camp, giving up climbing to the summit. All of the recordings lasted about 10 h and covered the whole nighttime sleep.
2.2. Pre-Elaboration
The thoracic movements by the triaxial accelerometer and the textile thoracic band provided information on the respiratory efforts and the PPG identified episodes of oxygen desaturation. These pieces of information were processed together automatically by the Somnologica software (Medcare Flaga, Reykjavik, Iceland) that calculated the apnea-hypopnea index accordingly to the current guidelines [
20]. The evaluation of the apnea-hypopnea index with the MagIC device was previously validated vs. a standard cardiorespiratory monitor [
17].
To derive the tachograms for HRV analysis, the PPG signal was resampled at 200 Hz after linear interpolation to have the same sampling rate as the ECG. A segment of at least one-hour duration during sleep was visually selected looking for stable periods of the triaxial accelerometers in lying position. Premature beats and artifacts were identified visually on the selected ECG and PPG segments separately and removed. The percentage of removed signal over the total duration of the selected segment was calculated separately for each ECG and PPG signal.
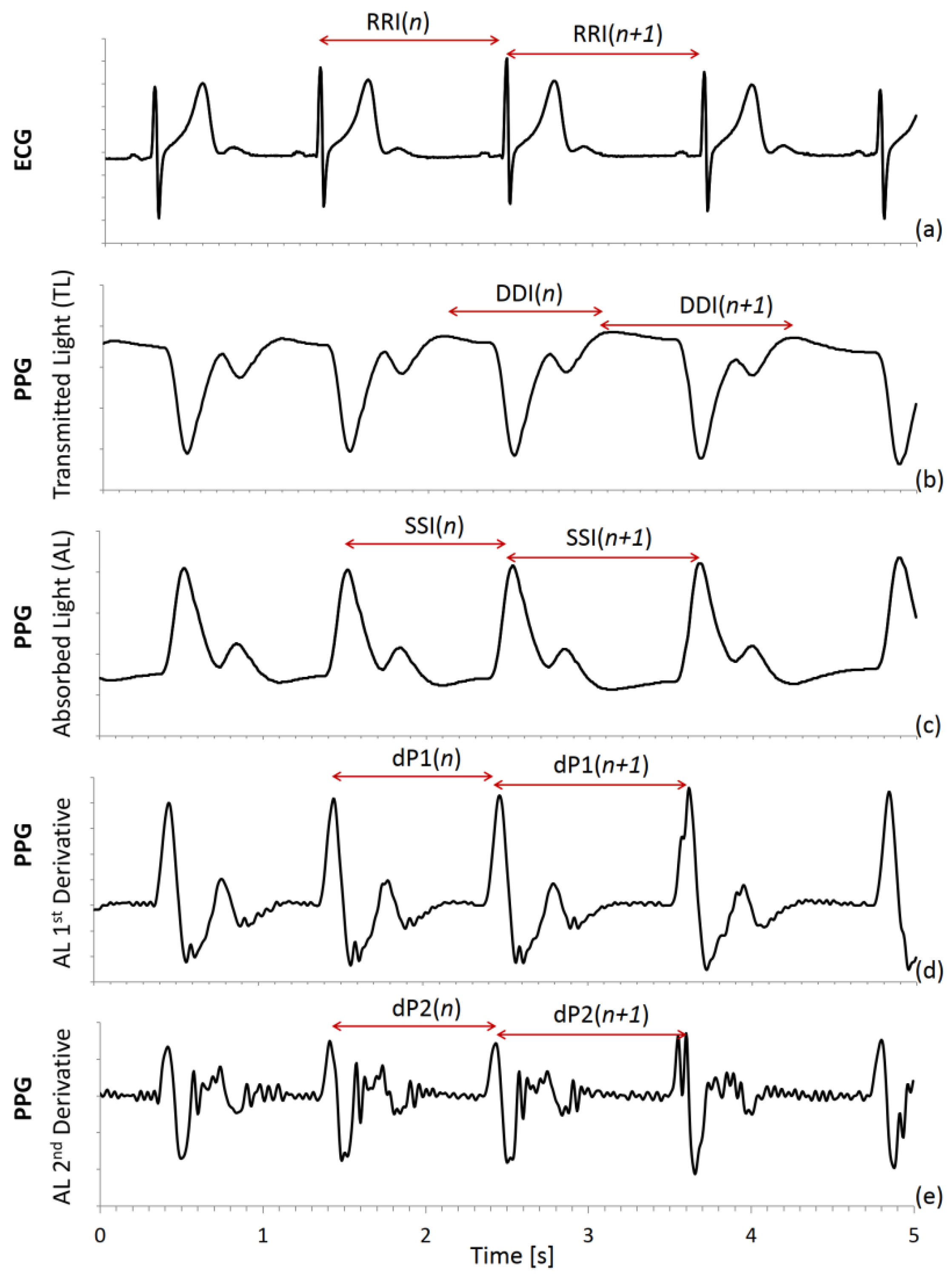
A derivative-and-threshold algorithm was applied to the ECG to identify the R peak, with parabolic interpolation to refine the R wave fiducial point [
4], and the R–R intervals (RRI) were calculated beat by beat (
Figure 1a). As to the photoplethysmogram, a similar derivative-and-threshold algorithm was applied to the photodetector signal, which measures the intensity of the transmitted light (TL) from the LED through the finger. A beat-to-beat series was extracted as the intervals between the maxima (DDI) in the diastolic phase of the heartbeat (
Figure 1b). The negative of light intensity (
Figure 1c) is proportional to the fraction of absorbed light (AL) by the finger tissues and a second series was obtained as the intervals between AL maxima, which occur in the systolic phase of the beat (SSI). Furthermore, we calculated the first (
Figure 1d) and second (
Figure 1e) derivatives of AL. Since the derivative operator amplifies the high-frequency noise, the calculus was performed after low-pass filtering (fourth-order zero-phase Butterworth filter with 25 Hz cut-off frequency). Then we identified the intervals between maxima of the first (dP1) and second (dP2) derivative.
SSI, which is the peak-to-peak interval, is a commonly used PPG tachogram because it is defined similarly to RRI. DDI has been also proposed to measure the distance between consecutive feet of the pulse waves and is also called valley-to-valley or foot-to-foot interval [
15,
21,
22]. The dP2 fiducial point is intended to identify the foot of the wave more precisely as the instant when the blood volume starts to rise after the heart contraction. The dP1 point is where the pulse wave upstroke is most rapid.
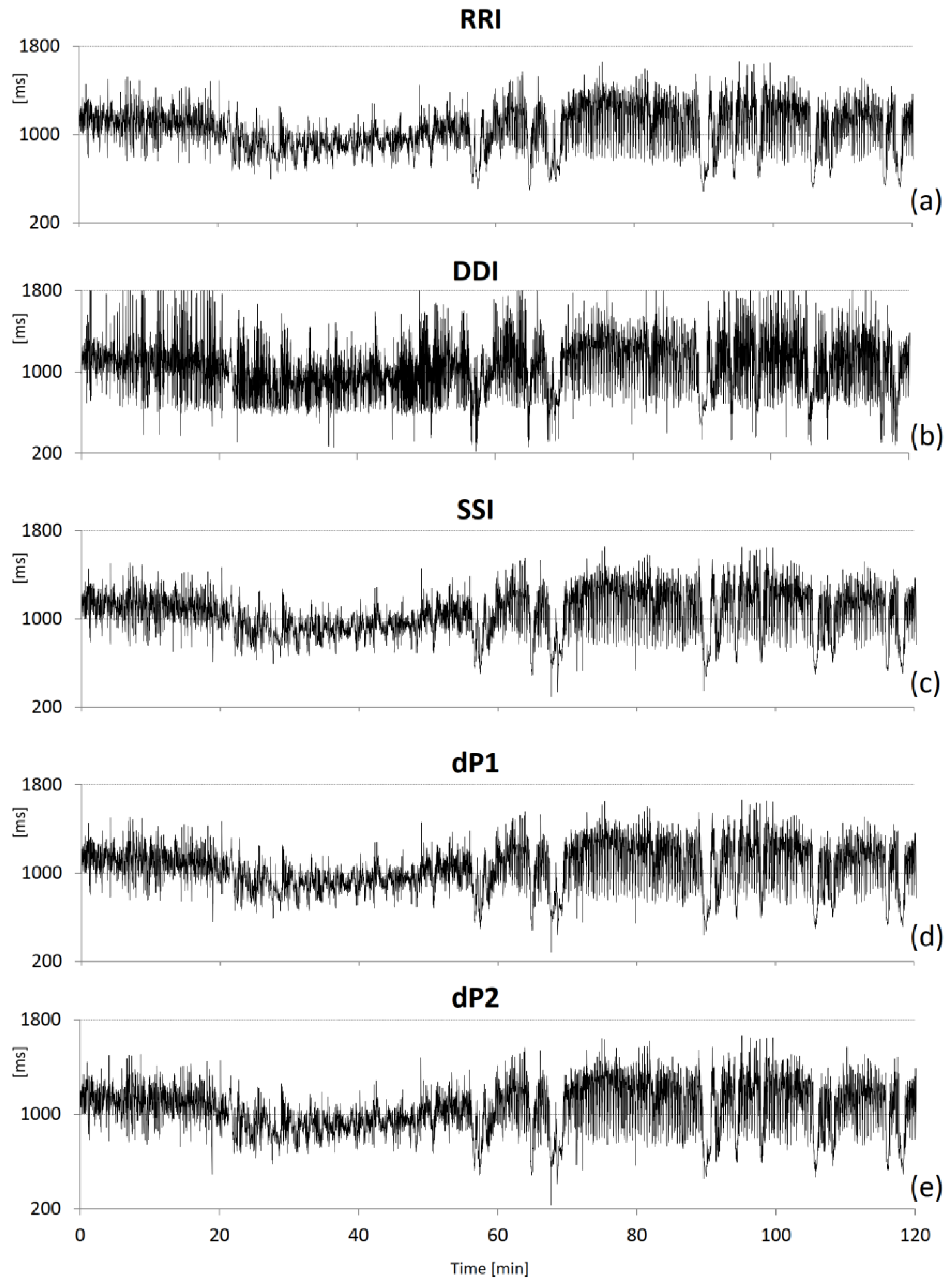
Figure 2 shows an example of the beat-to-beat intervals derived from the ECG and PPG.
2.3. HRV Analysis
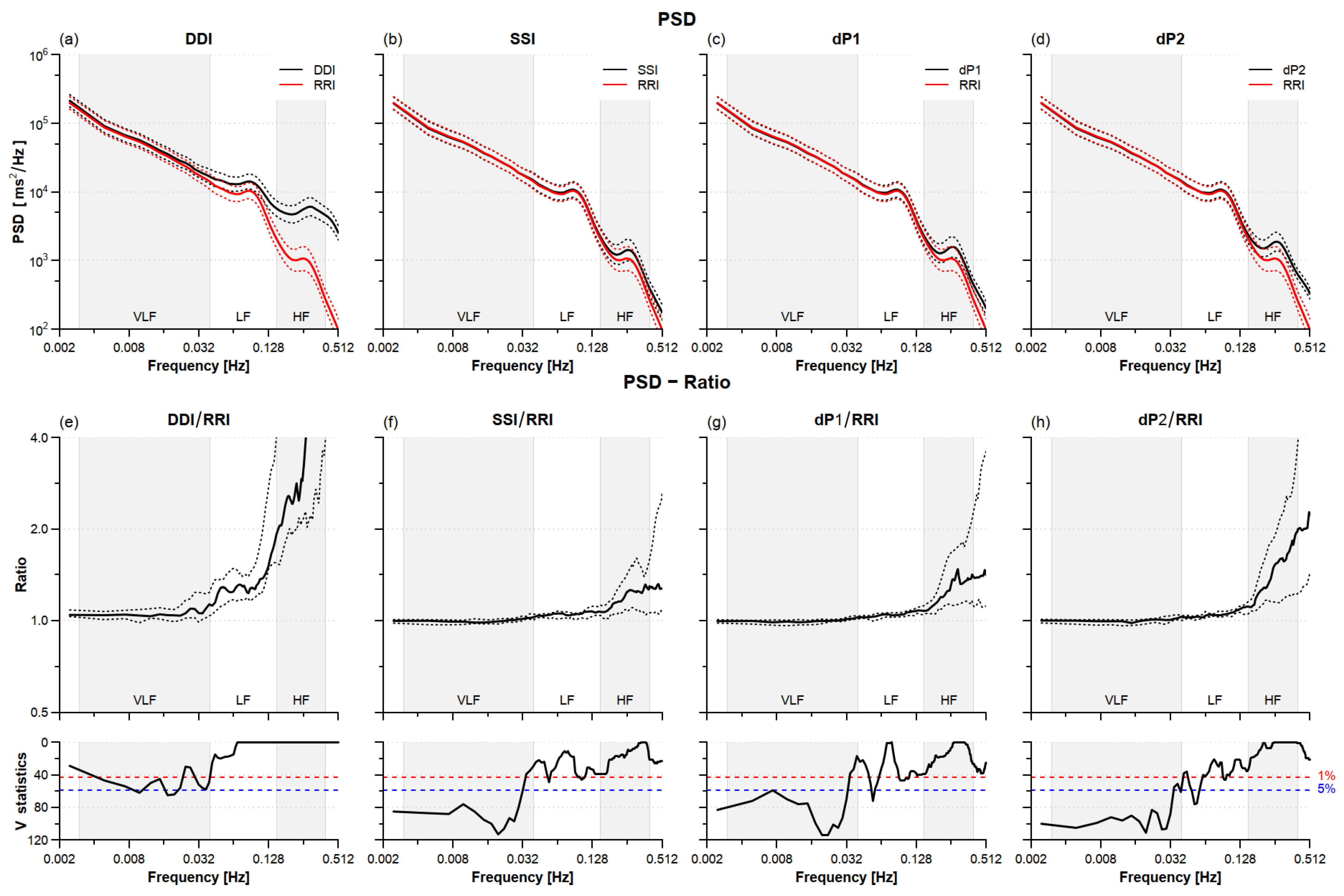
Beat-by-beat series were interpolated evenly at 5 Hz before spectral analysis. Power spectra were estimated by the Welch periodogram with 90% overlapped and linearly detrended Hann windows of 300 s length. The spectra were further broadband smoothed with a moving average whose order increased with the spectral frequency as in [
23] and integrated over the very-low-frequency (VLF, between 0.003 and 0.04 Hz), low-frequency (LF, between 0.04 and 0.15 Hz), and high-frequency (HF, between 0.15 and 0.4 Hz) bands [
4]. Discrepancies between PPG- and ECG-derived power spectra were quantified by the ratio between the spectrum of each PPG-derived tachogram (DDI, SSI, dP1, and dP2) and the RRI spectrum.
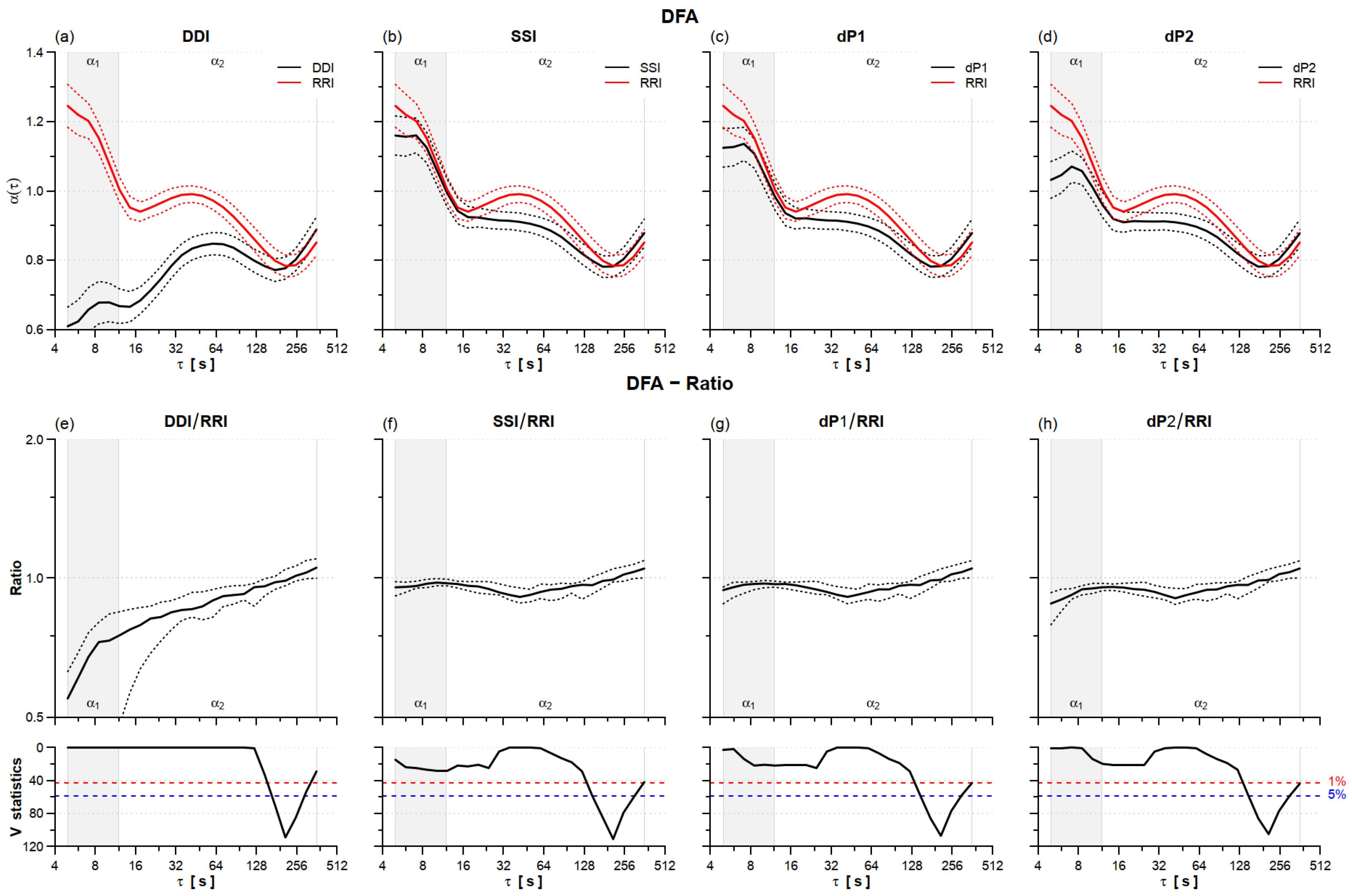
HRV complexity was quantified by self-similarity and entropy. The multiscale spectrum of self-similarity coefficients α(τ) was estimated as in [
24] with the detrended fluctuation analysis code provided in [
25]. The approach originally introduced in [
24] consists in calculating the self-similarity scale coefficients as a continuous function of the temporal scale τ, in seconds, from the scale coefficients α
B(
n) evaluated on the “beat domain” as the local slope of the detrended fluctuation function log F(
n) vs. log (
n) [
26]. This is done by mapping the scale units from the number of beats,
n, to time τ, in seconds, with the transformation τ =
n × μ
IBI, with μ
IBI the mean inter-beat-interval of the series, in seconds. Short- and long-term coefficients, α
1 and α
2, respectively, were similarly calculated considering temporal scales and not scales defined on the beat domain. This was done averaging α(τ) over the scales 5 ≤ τ ≤ 12 s to calculate α
1, and over 12 < τ ≤ 360 s to calculate α
2. Discrepancies between PPG- and ECG-derived self-similarity spectra were quantified by the ratio between α(τ) of each PPG tachogram (DDI, SSI, dP1, and dP2) and α(τ) of RRI.
The sample entropy, SampEn, was estimated setting the tolerance
r equal to 15% of the standard deviation of the series [
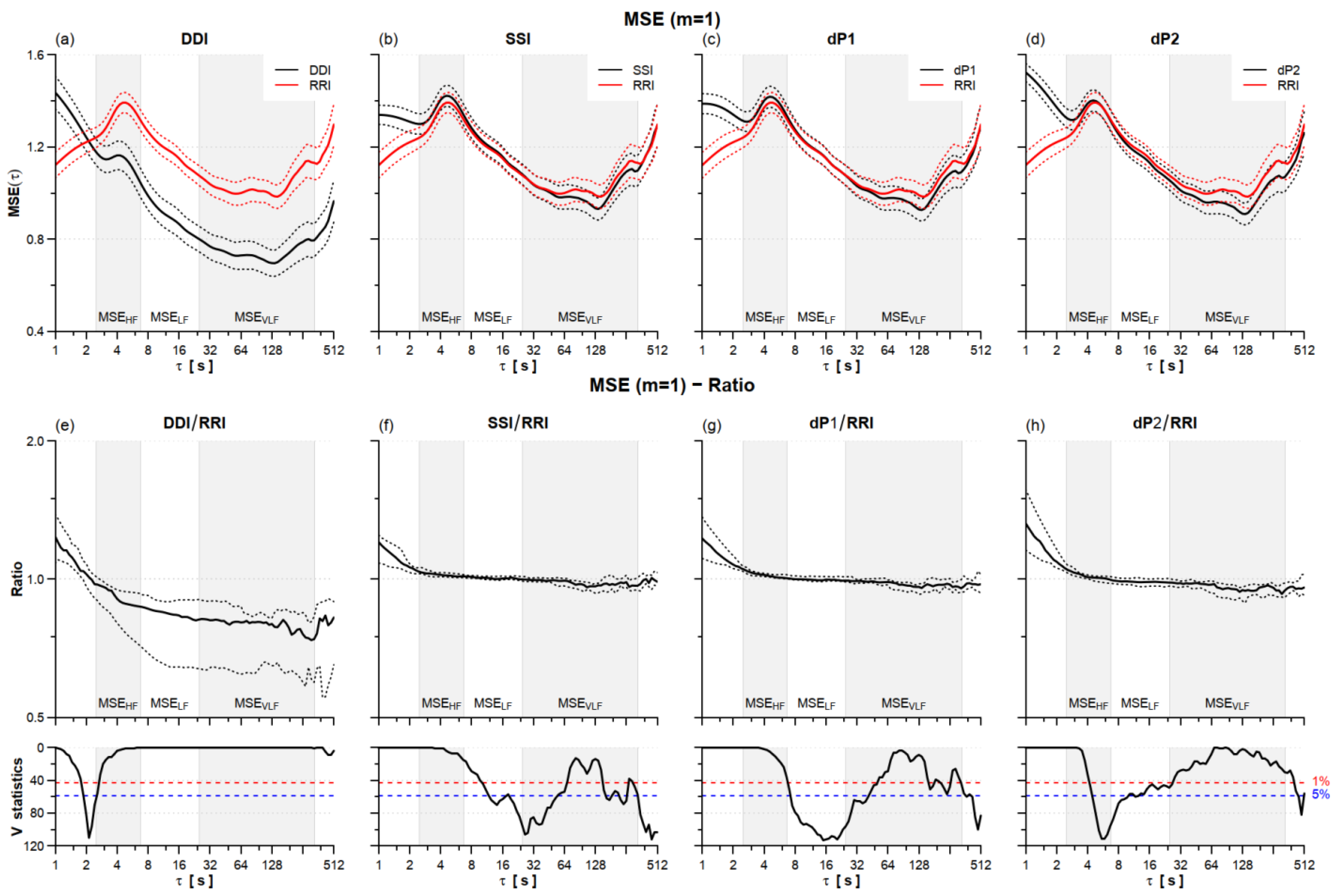
27]. The multiscale entropy, i.e., SampEn as a function of the time scale τ in seconds, MSE(τ), was calculated for
m = 1 and with a fixed tolerance
r = 15% of the standard deviation [
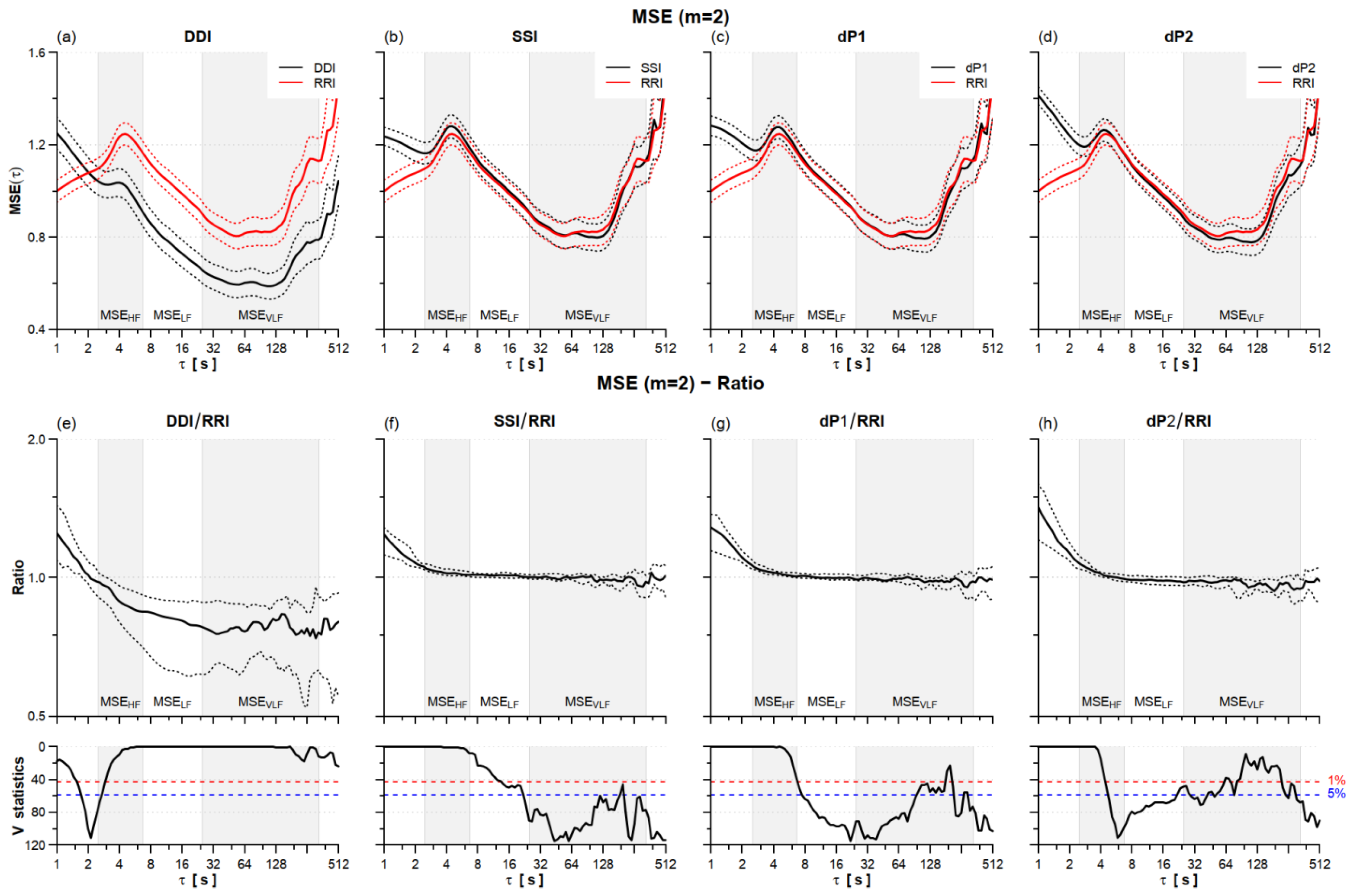
28]. Most of the literature on HRV evaluated SampEn with embedding dimension
m = 2 following the original proposal in [
27], but recently we showed that
m = 1 provides the same type of information on the cardiovascular irregularity with more stable estimates [
29]. Thus, this work shows the entropy estimates with
m = 1 and interested readers will find the results for
m = 2 in
Appendix A.
We extracted three entropy indexes, MSEHF, MSELF, and MSEVLF, averaging MSE(τ) over the scales corresponding to the HF (2.5 ≤ τ < 6.7 s), LF (6.7 ≤ τ < 25 s), and VLF (25 ≤ τ < 333 s) bands. Discrepancies between PPG- and ECG-derived multiscale entropies were quantified by the ratio between the MSE(τ) of each PPG tachogram (DDI, SSI, dP1, and dP2) and the MSE(τ) of RRI.


 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




