
Classification of Blood Volume Decompensation State via Machine Learning Analysis of Multi-Modal Wearable-Compatible Physiological Signals

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Data
2.2. Data Processing and Feature Extraction
- (1)
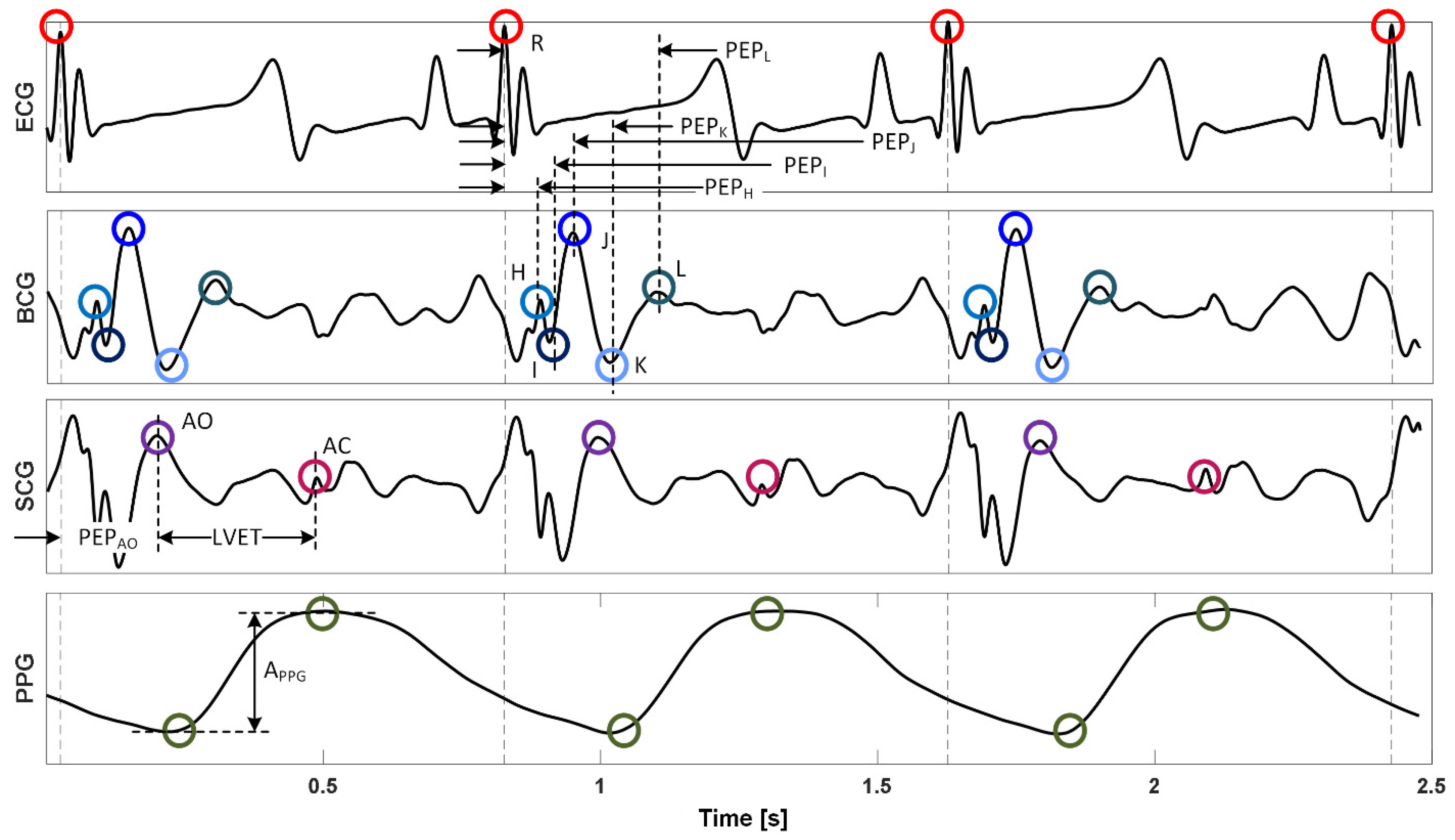
- Heart rate and heart rate variability based on three different methods [31] were calculated, including (i) time-domain method HRVT, (ii) Poincare method HRVP, and (iii) frequency-domain method HRVF. These constituted 4 features (HRVT, HRVP, HRVF, and heart rate).
- (2)
- Cardiac timing intervals including pre-ejection period (PEP, as the time interval between the R wave in the ECG and (i) the AO [32] point in the SCG as well as (ii) the H, I, J, K, and L waves in the BCG; thus 6 in total) and left ventricular ejection time (LVET, as the time interval between the AO point and the AC point [32] in the SCG) as well as their ratios (PEP/LVET; 6 based on 6 PEPs) were calculated. These constituted 13 features.
- (3)
- PPG amplitude (APPG, as the vertical difference between the diastolic trough and systolic peak) was calculated as a measure of peripheral vasoconstriction/vasodilation. This constituted one feature.
- (4)
- Various time intervals and amplitudes based on the fiducial points in the BCG were calculated: H, I, J, K, and L wave amplitudes, a total of 10 wave-to-wave time intervals and amplitudes (H-I, I-J, J-K, I-K, and K-L), and the variability associated with all these time intervals and amplitudes (as the standard deviation of the 100 causal beats preceding the cardiac beat of interest) were calculated (except the I-K interval and amplitude since I-K amplitude showed a very large coefficient of variation). These constituted 28 features.
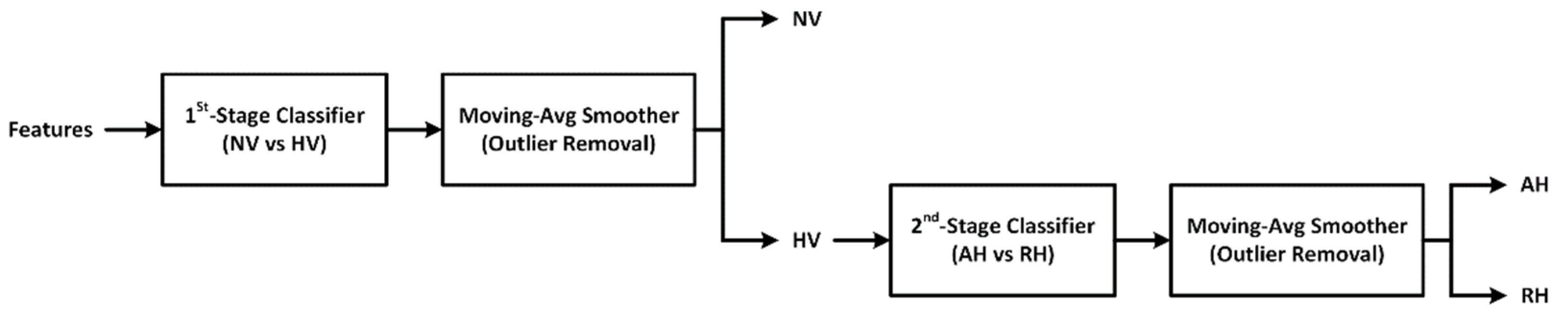
2.3. Classification of Blood Volume Decompensation State
2.3.1. ML-Based Blood Volume Decompensation State Classifier: Development
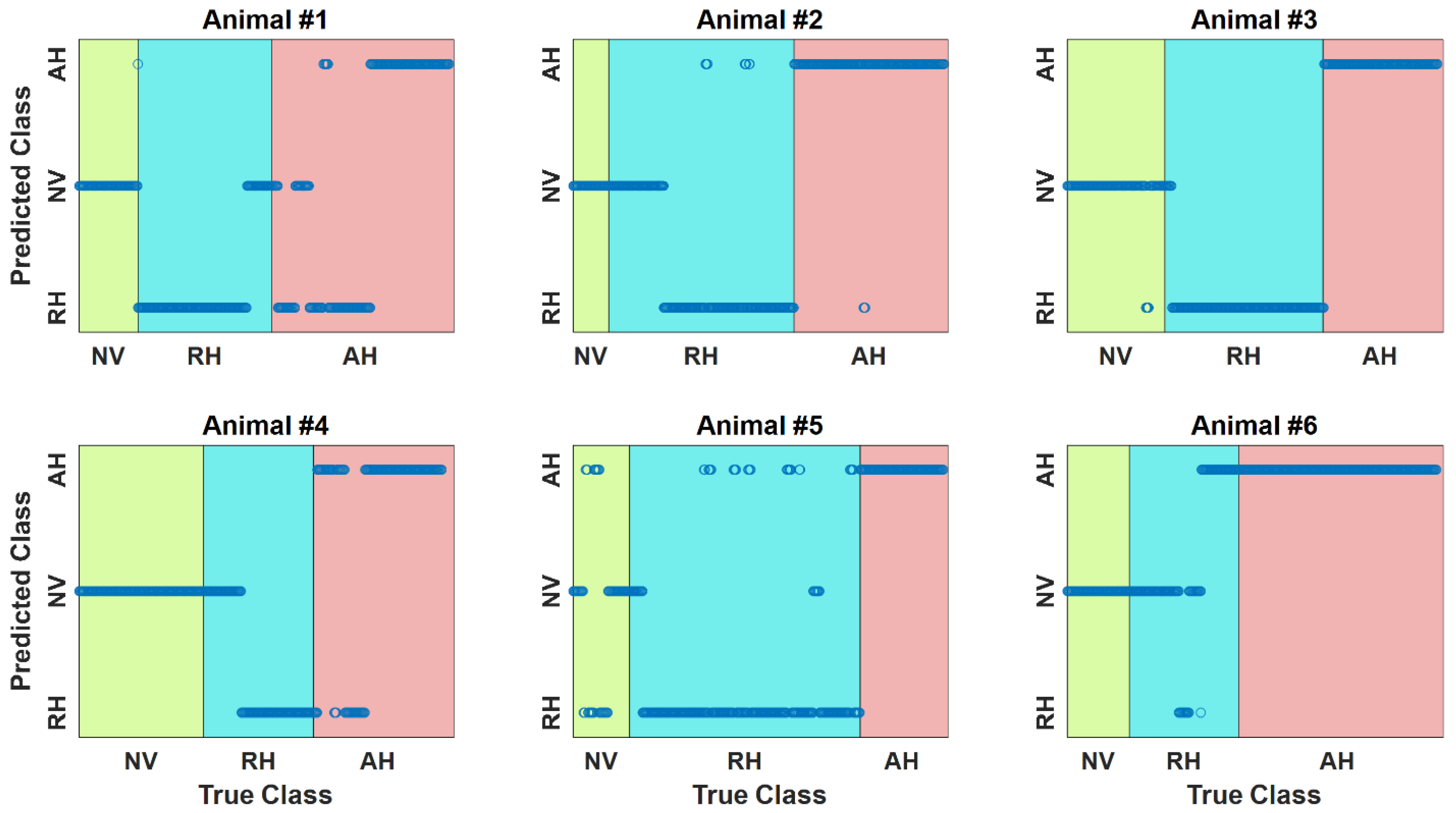
2.3.2. ML-Based Blood Volume Decompensation State Classifier: Evaluation
3. Results
4. Discussion
4.1. Blood Volume Decompensation State Classification Performance
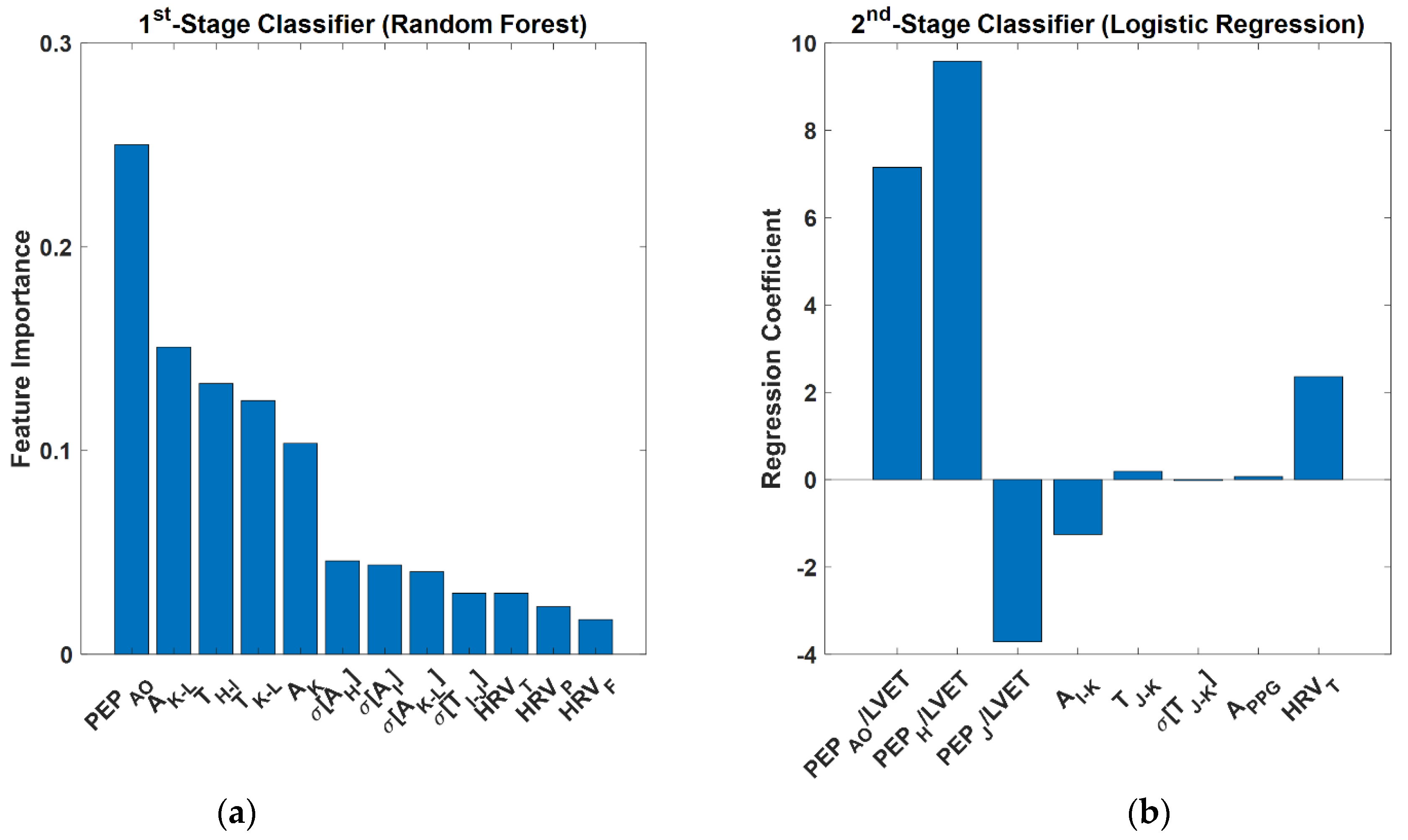
4.2. Feature Importance and Interpretation
4.3. Study Limitations and Future Opportunities
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Airapetian, N.; Maizel, J.; Slama, M. Diagnosis of Central Hypovolemia in a Spontaneously Breathing Patient. In Intensive Care Medicine; Vincent, J.L., Ed.; Springer: New York, NY, USA, 2007. [Google Scholar]
- Gitz Holler, J.; Jensen, H.K.; Henriksen, D.P.; Rasmussen, L.M.; Mikkelsen, S.; Pedersen, C.; Lassen, A.T. Etiology of Shock in the Emergency Department: A 12-Year Population-Based Cohort Study. Shock 2019, 51, 60–67. [Google Scholar] [CrossRef] [PubMed]
- McGee, S.; Abernethy, W.B.; Simel, D.L. Is This Patient Hypovolemic? J. Am. Med. Assoc. 1999, 281, 1022–1029. [Google Scholar] [CrossRef] [PubMed]
- Sinert, R.; Spektor, M. Clinical Assessment of Hypovolemia. Ann. Emerg. Med. 2005, 45, 327–329. [Google Scholar]
- Warden, G.D. Burn Shock Resuscitation. World J. Surg. 1992, 16, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Sigmann, P. Review: Physical Signs Are Not Useful for Detecting Non-Blood-Loss Hypovolemia. ACP J. Club 1999, 131, 48. [Google Scholar]
- Husain, F.A.; Martin, M.J.; Mullenix, P.S.; Steele, S.R.; Elliott, D.C. Serum Lactate and Base Deficit as Predictors of Mortality and Morbidity. Am. J. Surg. 2003, 185, 485–491. [Google Scholar] [CrossRef]
- Bendjelid, K.; Romand, J.A. Fluid Responsiveness in Mechanically Ventilated Patients: A Review of Indices Used in Intensive Care. Intensive Care Am. J. Surg. Med. 2003, 29, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, J.G.; Mahon, S.; Tromberg, B.J.; Ryan, K.L.; Convertino, V.A.; Rickards, C.A.; Osann, K.; Brenner, M. Tissue Hemoglobin Monitoring of Progressive Central Hypovolemia in Humans using Broadband Diffuse Optical Spectroscopy. J. Biomed. Opt. 2008, 13, 064027. [Google Scholar] [CrossRef] [Green Version]
- Gyang, E.; Shieh, L.; Forsey, L.; Maggio, P. A Nurse-Driven Screening Tool for the Early Identification of Sepsis in an Intermediate Care Unit Setting. J. Hosp. Med. 2015, 10, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.I.; Park, S. Sepsis: Early Recog nition and Optimized Treatment. Tuberc. Respir. Dis. 2019, 82, 6–14. [Google Scholar] [CrossRef]
- Calvert, J.S.; Price, D.A.; Chettipally, U.K.; Barton, C.W.; Feldman, M.D.; Hoffman, J.L.; Jay, M.; Das, R. A Computational Approach to Early Sepsis Detection. Comput. Biol. Med. 2016, 74, 69–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szabó, V.; Halász, G.; Gondos, T. Detecting Hypovolemia in Postoperative Patients using a Discrete Fourier Transform. Comput. Biol. Med. 2015, 59, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Lefevre, R.J.; Balzer, C.; Baudenbacher, F.J.; Riess, M.L.; Hernandez, A.; Eagle, S.S. Venous Waveform Analysis Correlates with Echocardiography in Detecting Hypovolemia in a Rat Hemorrhage Model. Semin. Cardiothorac. Vasc. Anesth. 2021, 25, 11–18. [Google Scholar] [CrossRef]
- Convertino, V.A.; Grudic, G.; Mulligan, J.; Moulton, S. Estimation of Individual-Specific Progression to Impending Cardiovascular Instability using Arterial Waveforms. J. Appl. Physiol. 2013, 115, 1196–1202. [Google Scholar] [CrossRef] [PubMed]
- Van der Ster, B.J.P.; Westerhof, B.E.; Stok, W.J.; van Lieshout, J.J. Detecting Central Hypovolemia in Simulated Hypovolemic Shock by Automated Feature Extraction with Principal Component Analysis. Physiol. Rep. 2018, 6, e13895. [Google Scholar] [CrossRef] [Green Version]
- Reljin, N.; Zimmer, G.; Malyuta, Y.; Shelley, K.; Mendelson, Y.; Blehar, D.J.; Darling, C.E.; Chon, K.H. Using Support Vector Machines on Photoplethysmographic Signals to Discriminate between Hypovolemia and Euvolemia. PLoS ONE 2018, 13, e0195087. [Google Scholar] [CrossRef] [Green Version]
- Bedoya, A.D.; Futoma, J.; Clement, M.E.; Corey, K.; Brajer, N.; Lin, A.; Simons, M.G.; Gao, M.; Nichols, M.; Balu, S.; et al. Machine Learning for Early Detection of Sepsis: An Internal and Temporal Validation Study. JAMIA Open 2020, 3, 252–260. [Google Scholar] [CrossRef]
- Reyna, M.A.; Josef, C.S.; Jeter, R.; Shashikumar, S.P.; Westover, M.B.; Nemati, S.; Clifford, G.D.; Sharma, A. Early Prediction of Sepsis from Clinical Data: The PhysioNet/Computing in Cardiology Challenge 2019. Crit. Care Med. 2020, 48, 210–217. [Google Scholar] [CrossRef] [Green Version]
- Goh, K.H.; Wang, L.; Yeow, A.Y.K.; Poh, H.; Li, K.; Yeow, J.J.L.; Tan, G.Y.H. Artificial Intelligence in Sepsis Early Prediction and Diagnosis using Unstructured Data in Healthcare. Nat. Commun. 2021, 12, 711. [Google Scholar] [CrossRef]
- Zöllei, É.; Bertalan, V.; Németh, A.; Csábi, P.; László, I.; Kaszaki, J.; Rudas, L. Non-Invasive Detection of Hypovolemia or Fluid Responsiveness in Spontaneously Breathing Subjects. BMC Anesthesiol. 2013, 13, 40. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Guo, F.; Kaffashi, F.; Jacono, F.J.; DeGeorgia, M.; Loparo, K.A. INSMA: An integrated system for multimodal data acquisition and analysis in the intensive care unit. J. Biomed. Inform. 2020, 106, 103434. [Google Scholar] [CrossRef] [PubMed]
- Klum, M.; Urban, M.; Tigges, T.; Pielmus, A.-G.; Feldheiser, A.; Schmitt, T.; Orglmeister, R. Wearable Cardiorespiratory Monitoring Employing a Multimodal Digital Patch Stethoscope: Estimation of ECG, PEP, LVET and Respiration Using a 55 mm Single-Lead ECG and Phonocardiogram. Sensors 2020, 20, 2033. [Google Scholar] [CrossRef] [Green Version]
- Zia, J.; Kimball, J.; Rolfes, C.; Hahn, J.-O.; Inan, O.T. Enabling the Assessment of Trauma-Induced Hemorrhage via Smart Wearable Systems. Sci. Adv. 2020, 6, eabb1708. [Google Scholar] [CrossRef] [PubMed]
- Kimball, J.P.; Zia, J.S.; An, S.; Rolfes, C.; Hahn, J.O.; Sawka, M.; Inan, O.T. Unifying the Estimation of Blood Volume Decompensation Status in a Porcine Model of Relative and Absolute Hypovolemia via Wearable Sensing. IEEE J. Biomed. Health Inform. 2021, 25, 3351–3360. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.; Ganti, V.G.; Heller, J.A.; Abdallah, C.A.; Etemadi, M.; Inan, O.T. Enabling Continuous Wearable Reflectance Pulse Oximetry at the Sternum. Biosensors 2021, 11, 521. [Google Scholar] [CrossRef]
- Ganti, V.G.; Carek, A.M.; Nevius, B.N.; Heller, J.A.; Etemadi, M.; Inan, O.T. Wearable Cuff-Less Blood Pressure Estimation at Home via Pulse Transit Time. IEEE J Biomed. Health Inform 2020, 25, 1926–1937. [Google Scholar] [CrossRef]
- Mukkamala, R.; Hahn, J.O.; Inan, O.T.; Mestha, L.K.; Kim, C.S.; Töreyin, H.; Kyal, S. Toward Ubiquitous Blood Pressure Monitoring via Pulse Transit Time: Theory and Practice. IEEE. Trans. Biomed. Eng. 2015, 62, 1879–1901. [Google Scholar] [CrossRef] [Green Version]
- Shandhi, M.M.H.; Semiz, B.; Hersek, S.; Goller, N.; Ayazi, F.; Inan, O.T. Performance Analysis of Gyroscope and Accelerometer Sensors for Seismocardiography-Based Wearable Pre-Ejection Period Estimation. IEEE J. Biomed. Health Inform. 2019, 23, 2365–2374. [Google Scholar] [CrossRef]
- Yousefian, P.; Shin, S.; Mousavi, A.S.; Tivay, A.; Kim, C.; Mukkamala, R.; Jang, D.-G.; Ko, B.H.; Lee, J.; Kwon, U.-K.; et al. Pulse Transit Time-Pulse Wave Analysis Fusion Based on Wearable Wrist Ballistocardiogram for Cuff-Less Blood Pressure Trend Tracking. IEEE Access 2020, 8, 138077–138087. [Google Scholar] [CrossRef]
- Acharya, U.R.; Joseph, K.P.; Kannathal, N.; Lim, C.M.; Suri, J.S. Heart Rate Variability: A Review. Med. Biol. Eng. Comput. 2006, 44, 1031–1051. [Google Scholar] [CrossRef]
- Inan, O.T.; Migeotte, P.F.; Park, K.S.; Etemadi, M.; Tavakolian, K.; Casanella, R.; Zanetti, J.; Tank, J.; Funtova, I.; Prisk, G.K.; et al. Ballistocardiography and Seismocardiography: A Review of Recent Advances. IEEE J. Biomed. Health Inform. 2015, 19, 1414–1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohavi, R.; John, G.H. The Wrapper Approach. In Feature Extraction, Construction and Selection; Liu, H., Motoda, H., Eds.; Spinger: Boston, MA, USA, 1998; pp. 33–50. [Google Scholar] [CrossRef]
- Bergstra, J.; Bengio, Y. Random Search for Hyper-Parameter Optimization. J. Mach. Learn. Res. 2012, 13, 281–305. [Google Scholar]
- Kim, C.-S.; Ober, S.L.; McMurtry, M.S.; Finegan, B.A.; Inan, O.T.; Mukkamala, R.; Hahn, J.-O. Ballistocardiogram: Mechanism and Potential for Unobtrusive Cardiovascular Health Monitoring. Sci. Rep. 2016, 6, 31297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yousefian, P.; Shin, S.; Mousavi, A.S.; Kim, C.-S.; Finegan, B.; McMurtry, M.S.; Mukkamala, R.; Jang, D.-G.; Kwon, U.; Kim, Y.H.; et al. Physiological Association between Limb Ballistocardiogram and Arterial Blood Pressure Waveforms: A Mathematical Model-Based Analysis. Sci. Rep. 2019, 9, 5146. [Google Scholar] [CrossRef] [Green Version]
- Yao, Y.; Shin, S.; Mousavi, A.; Kim, C.S.; Xu, L.; Mukkamala, R.; Hahn, J.O. Unobtrusive Estimation of Cardiovascular Parameters with Limb Ballistocardiography. Sensors 2019, 19, 2922. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.S.; Levinson, G.E.; Schwartz, C.J.; Etringer, P. Systolic Time Intervals as Measures of the Contractile State of the Left Ventricular Myocardium in Man. Circulation 1972, 46, 559–571. [Google Scholar] [CrossRef] [Green Version]
- Garrard, C.L.; Weissler, A.M.; Dodge, H.T. The Relationship of Alterations in Systolic Time Intervals to Ejection Fraction in Patients with Cardiac Disease. Circulation 1970, 42, 455–462. [Google Scholar] [CrossRef] [Green Version]
- Middleton, P.M.; Chan, G.S.H.; O’Lone, E.; Steel, E.; Carroll, R.; Celler, B.G.; Lovell, N.H. Changes in Left Ventricular Ejection Time and Pulse Transit Time Derived from Finger Photoplethysmogram and Electrocardiogram During Moderate Haemorrhage. Clin. Physiol. Funct. Imaging 2009, 29, 163–169. [Google Scholar] [CrossRef]
- Grum, D.F.; Dauchot, P.J. Systolic Time Intervals; List, W., Gravenstein, J.S., Spodick, D.H., Eds.; Springer: Berlin/Heidelberg, Germany, 1980; pp. 218–222. [Google Scholar] [CrossRef]
- Hinojosa-Laborde, C.; Rickards, C.A.; Ryan, K.L.; Convertino, V.A. Heart Rate Variability During Simulated Hemorrhage with Lower Body Negative Pressure in High and Low Tolerant Subjects. Front. Physiol. 2011, 2, 85. [Google Scholar] [CrossRef] [Green Version]
- Cooke, W.H.; Convertino, V.A. Heart Rate Variability and Spontaneous Baroreflex Sequences: Implications for Autonomic Monitoring During Hemorrhage. J. Trauma Acute Care Surg. 2005, 58, 798–805. [Google Scholar] [CrossRef]
- Salomão, E.; Otsuki, D.A.; Correa, A.L.; Fantoni, D.T.; Dos Santos, F.; Irigoyen, M.C.; Auler, J.O.C. Heart Rate Variability Analysis in an Experimental Model of Hemorrhagic Shock and Resuscitation in Pigs. PLoS ONE 2015, 10, e0134387. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Tejuja, A.; Newman, K.D.; Zarychanski, R.; Seely, A.J.E. Clinical Review: A Review and Analysis of Heart Rate Variability and the Diagnosis and Prognosis of Infection. Crit. Care 2009, 13, 232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wee, B.Y.H.; Lee, J.H.; Mok, Y.H.; Chong, S.-L. A Narrative Review of Heart Rate and Variability in Sepsis. Ann. Transl. Med. 2020, 8, 768. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Mousavi, A.; Lyle, S.; Jang, E.; Yousefian, P.; Mukkamala, R.; Jang, D.G.; Kim, Y.H.; Hahn, J.O. Posture-Dependent Variability in Wrist Ballistocardiogram-Photoplethysmogram Pulse Transit Time: Implication to Cuff-Less Blood Pressure Tracking. IEEE. Trans. Biomed. Eng. 2022, 69, 347–355. [Google Scholar] [CrossRef]
- Yao, Y.; Ghasemi, Z.; Shandhi, M.M.H.; Ashouri, H.; Xu, L.; Mukkamala, R.; Inan, O.T.; Hahn, J.O. Mitigation of Instrument-Dependent Variability in Ballistocardiogram Morphology: Case Study on Force Plate and Customized Weighing Scale. IEEE J. Biomed. Health Inform. 2020, 24, 69–78. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (a) Logistic Regression | ||||
| Animal | Accuracy | Precision | Recall | F1 Score |
| 1 | 0.77 | 0.94 | 0.78 | 0.85 |
| 2 | 0.93 | 0.93 | 1.00 | 0.96 |
| 3 | 0.64 | 1.00 | 0.52 | 0.68 |
| 4 | 0.74 | 0.71 | 1.00 | 0.83 |
| 5 | 0.79 | 0.97 | 0.77 | 0.86 |
| 6 | 0.83 | 0.97 | 0.82 | 0.89 |
| Aggregated | 0.78 ± 0.09 | 0.92 ± 0.10 | 0.81 ± 0.16 | 0.85 ± 0.08 |
| (b) Random Forest | ||||
| Animal | Accuracy | Precision | Recall | F1 Score |
| 1 | 0.88 | 1.00 | 0.86 | 0.92 |
| 2 | 0.85 | 1.00 | 0.84 | 0.91 |
| 3 | 0.97 | 0.99 | 0.97 | 0.98 |
| 4 | 0.93 | 1.00 | 0.89 | 0.94 |
| 5 | 0.89 | 0.92 | 0.96 | 0.94 |
| 6 | 0.84 | 1.00 | 0.81 | 0.89 |
| Aggregated | 0.89 ± 0.04 | 0.98 ± 0.03 | 0.89 ± 0.06 | 0.93 ± 0.03 |
| (c) Support Vector Machine | ||||
| Animal | Accuracy | Precision | Recall | F1 Score |
| 1 | 0.80 | 1.00 | 0.76 | 0.86 |
| 2 | 0.88 | 1.00 | 0.86 | 0.93 |
| 3 | 0.78 | 0.86 | 0.83 | 0.85 |
| 4 | 0.86 | 1.00 | 0.79 | 0.88 |
| 5 | 0.96 | 0.98 | 0.97 | 0.97 |
| 6 | 0.73 | 1.00 | 0.67 | 0.80 |
| Aggregated | 0.83 ± 0.07 | 0.97 ± 0.05 | 0.81 ± 0.09 | 0.88 ± 0.05 |
| (a) Logistic Regression | ||||
| Animal | Accuracy | Precision | Recall | F1 Score |
| 1 | 0.69 | 1.00 | 0.47 | 0.64 |
| 2 | 0.98 | 0.96 | 0.99 | 0.97 |
| 3 | 0.99 | 1.00 | 0.99 | 0.99 |
| 4 | 0.89 | 1.00 | 0.80 | 0.89 |
| 5 | 0.93 | 0.79 | 0.99 | 0.88 |
| 6 | 0.86 | 0.82 | 1.00 | 0.90 |
| Aggregated | 0.89 ± 0.10 | 0.93 ± 0.09 | 0.87 ± 0.19 | 0.88 ± 0.11 |
| (b) Random Forest | ||||
| Animal | Accuracy | Precision | Recall | F1 Score |
| 1 | 0.52 | 0.55 | 0.89 | 0.68 |
| 2 | 0.98 | 0.99 | 0.96 | 0.98 |
| 3 | 0.98 | 0.95 | 0.99 | 0.97 |
| 4 | 0.95 | 1.00 | 0.92 | 0.96 |
| 5 | 0.99 | 1.00 | 0.99 | 0.99 |
| 6 | 0.85 | 0.93 | 0.84 | 0.88 |
| Aggregated | 0.88 ± 0.16 | 0.90 ± 0.16 | 0.93 ± 0.05 | 0.91 ± 0.10 |
| (c) Support Vector Machine | ||||
| Animal | Accuracy | Precision | Recall | F1 Score |
| 1 | 0.49 | 0.53 | 0.83 | 0.66 |
| 2 | 0.99 | 0.97 | 1.00 | 0.99 |
| 3 | 0.92 | 0.85 | 0.99 | 0.91 |
| 4 | 0.86 | 1.00 | 0.75 | 0.85 |
| 5 | 0.99 | 1.00 | 0.99 | 0.99 |
| 6 | 0.77 | 0.97 | 0.66 | 0.78 |
| Aggregated | 0.84 ± 0.17 | 0.89 ± 0.17 | 0.87 ± 0.13 | 0.86 ± 0.11 |
| Animal | Accuracy | Precision | Recall | F1 Macro Score |
|---|---|---|---|---|
| 1 | 0.68 | 0.70 | 0.77 | 0.68 |
| 2 | 0.83 | 0.78 | 0.88 | 0.78 |
| 3 | 0.97 | 0.96 | 0.97 | 0.97 |
| 4 | 0.82 | 0.85 | 0.84 | 0.81 |
| 5 | 0.83 | 0.79 | 0.76 | 0.77 |
| 6 | 0.73 | 0.58 | 0.66 | 0.59 |
| Aggregated | 0.81 ± 0.09 | 0.78 ± 0.11 | 0.81 ± 0.09 | 0.77 ± 0.11 |
| NV (ML) | HV-RH (ML) | HV-AH (ML) | |
|---|---|---|---|
| NV | 13,205 (15.8%) | 913 (1.0%) | 385 (0.4%) |
| HV-RH | 7595 (9.1%) | 27,319 (32.6%) | 3965 (4.7%) |
| HV-AH | 950 (1.1%) | 2345 (2.8%) | 27,005 (32.2%) |
| Final Classifier | No SCG | No BCG | Vital Signs | |
|---|---|---|---|---|
| Accuracy | 0.81 ± 0.09 | 0.77 ± 0.08 | 0.69 ± 0.21 | 0.47 ± 0.12 † |
| F1 Macro | 0.77 ± 0.11 | 0.75 ± 0.09 | 0.68 ± 0.21 | 0.41 ± 0.17 † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chalumuri, Y.R.; Kimball, J.P.; Mousavi, A.; Zia, J.S.; Rolfes, C.; Parreira, J.D.; Inan, O.T.; Hahn, J.-O. Classification of Blood Volume Decompensation State via Machine Learning Analysis of Multi-Modal Wearable-Compatible Physiological Signals. Sensors 2022, 22, 1336. https://doi.org/10.3390/s22041336
Chalumuri YR, Kimball JP, Mousavi A, Zia JS, Rolfes C, Parreira JD, Inan OT, Hahn J-O. Classification of Blood Volume Decompensation State via Machine Learning Analysis of Multi-Modal Wearable-Compatible Physiological Signals. Sensors. 2022; 22(4):1336. https://doi.org/10.3390/s22041336
Chicago/Turabian StyleChalumuri, Yekanth Ram, Jacob P. Kimball, Azin Mousavi, Jonathan S. Zia, Christopher Rolfes, Jesse D. Parreira, Omer T. Inan, and Jin-Oh Hahn. 2022. "Classification of Blood Volume Decompensation State via Machine Learning Analysis of Multi-Modal Wearable-Compatible Physiological Signals" Sensors 22, no. 4: 1336. https://doi.org/10.3390/s22041336