Wristbands Containing Accelerometers for Objective Arm Swing Analysis in Patients with Parkinson’s Disease

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
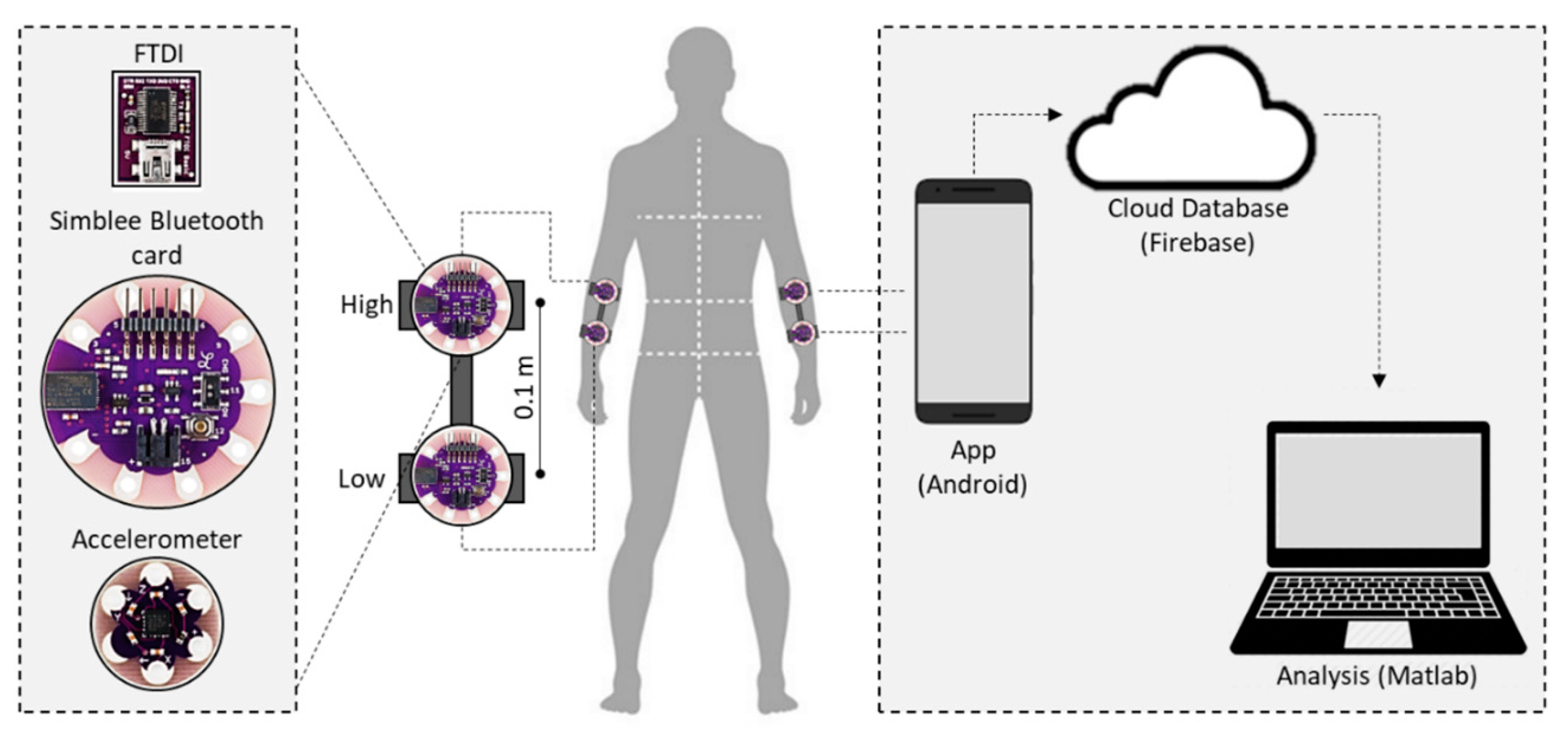
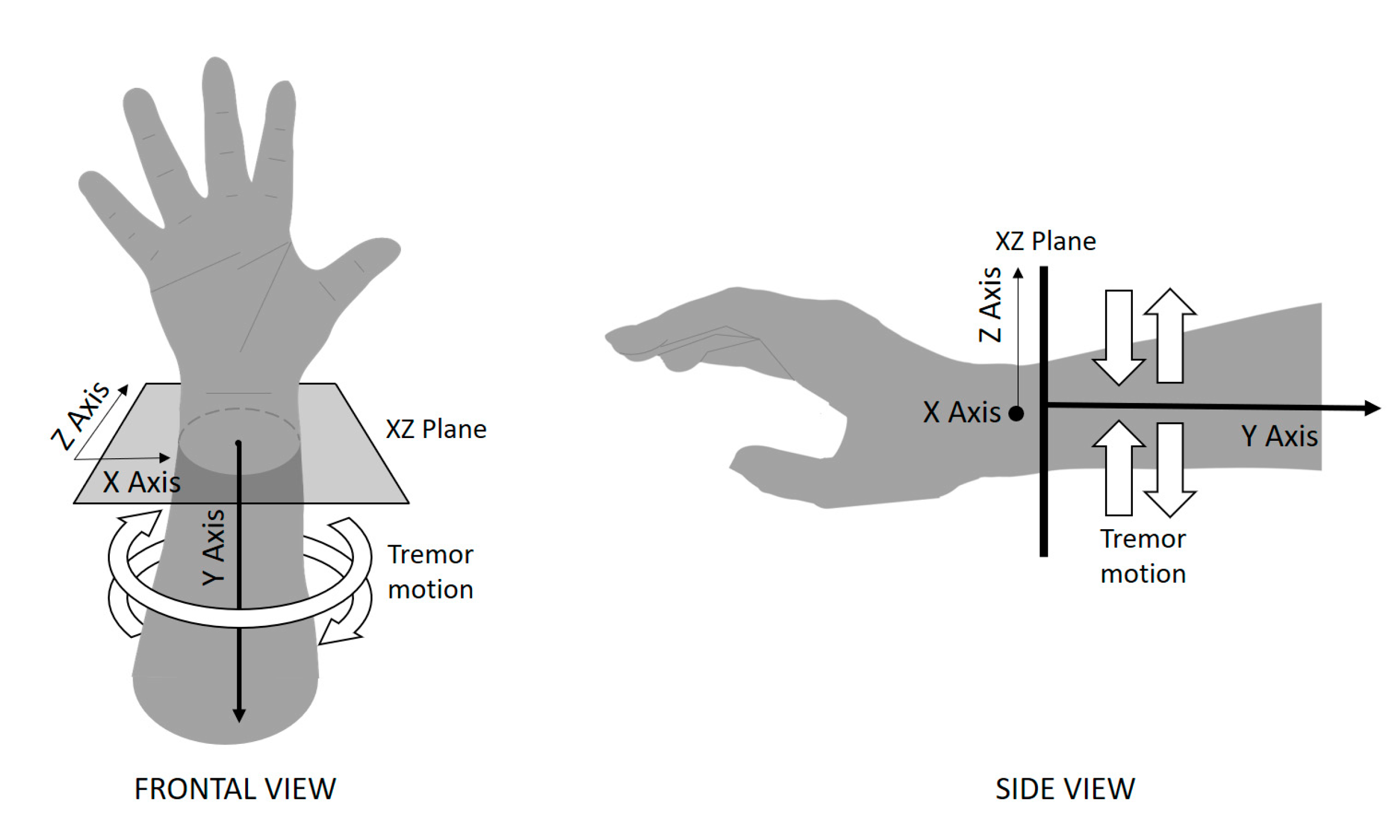
2.2. Measurement System
2.3. Experimental Setup
2.4. Feature Extraction Techniques
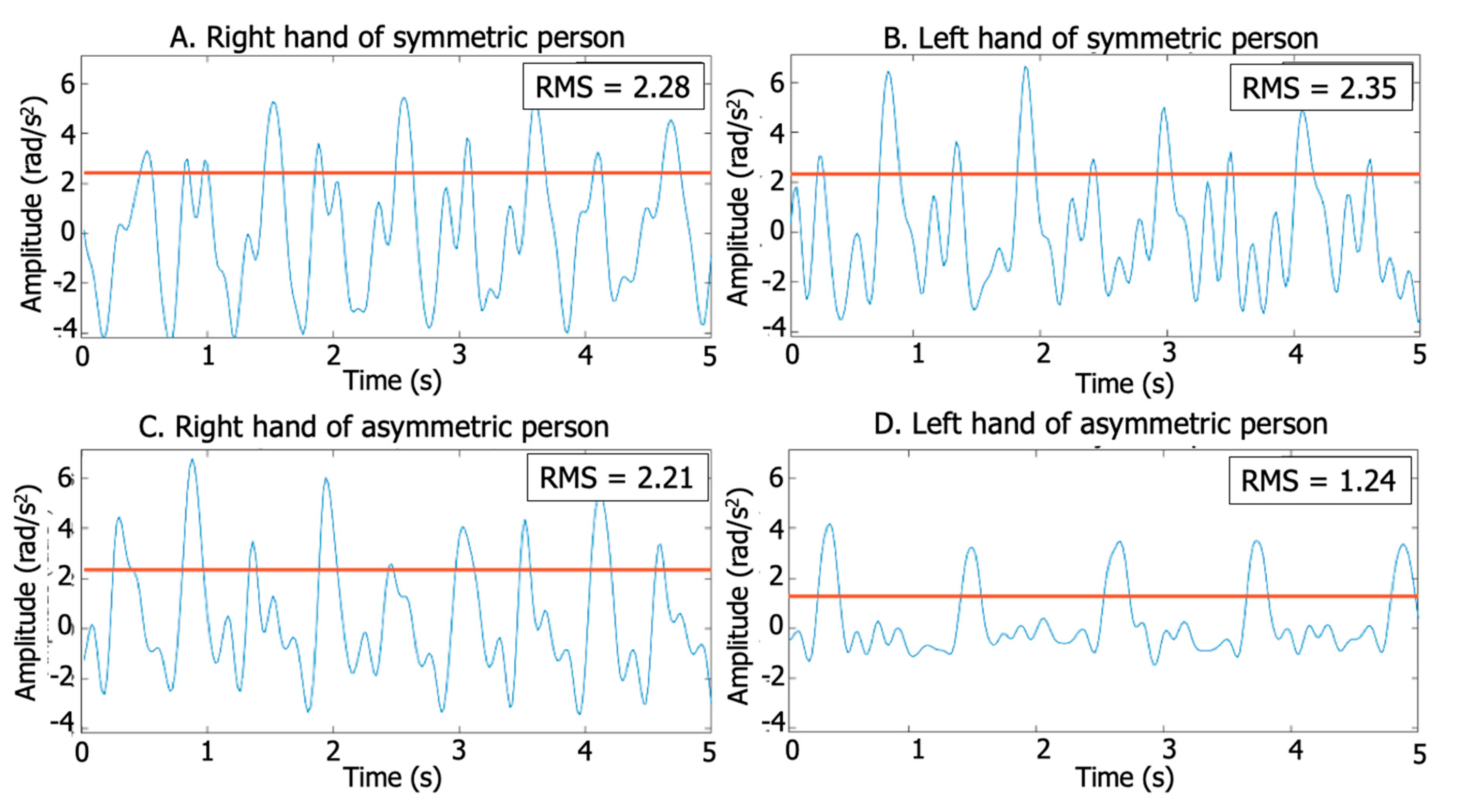
2.4.1. Root Mean Square (RMS) and RMS Asymmetry Calculations
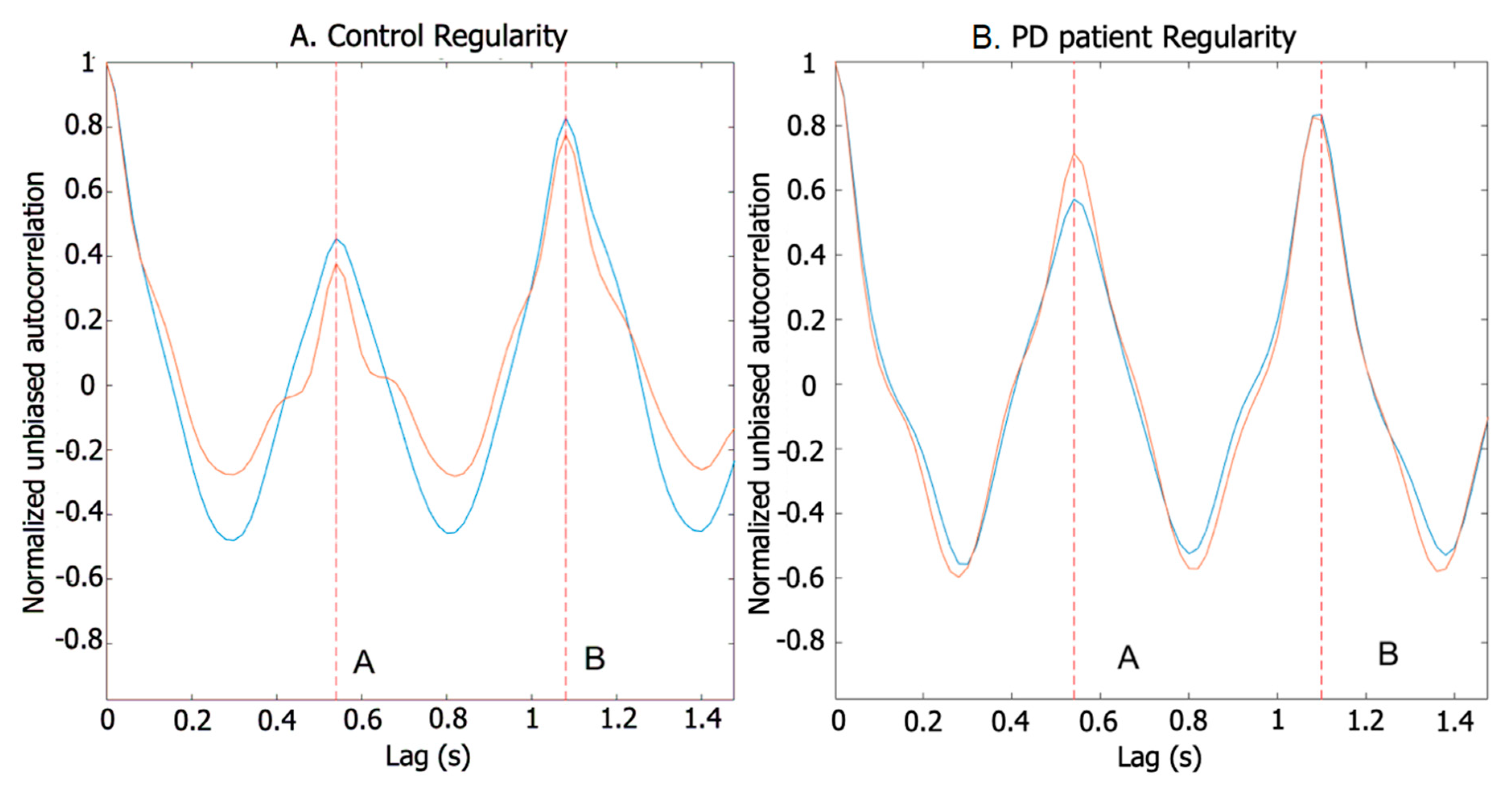
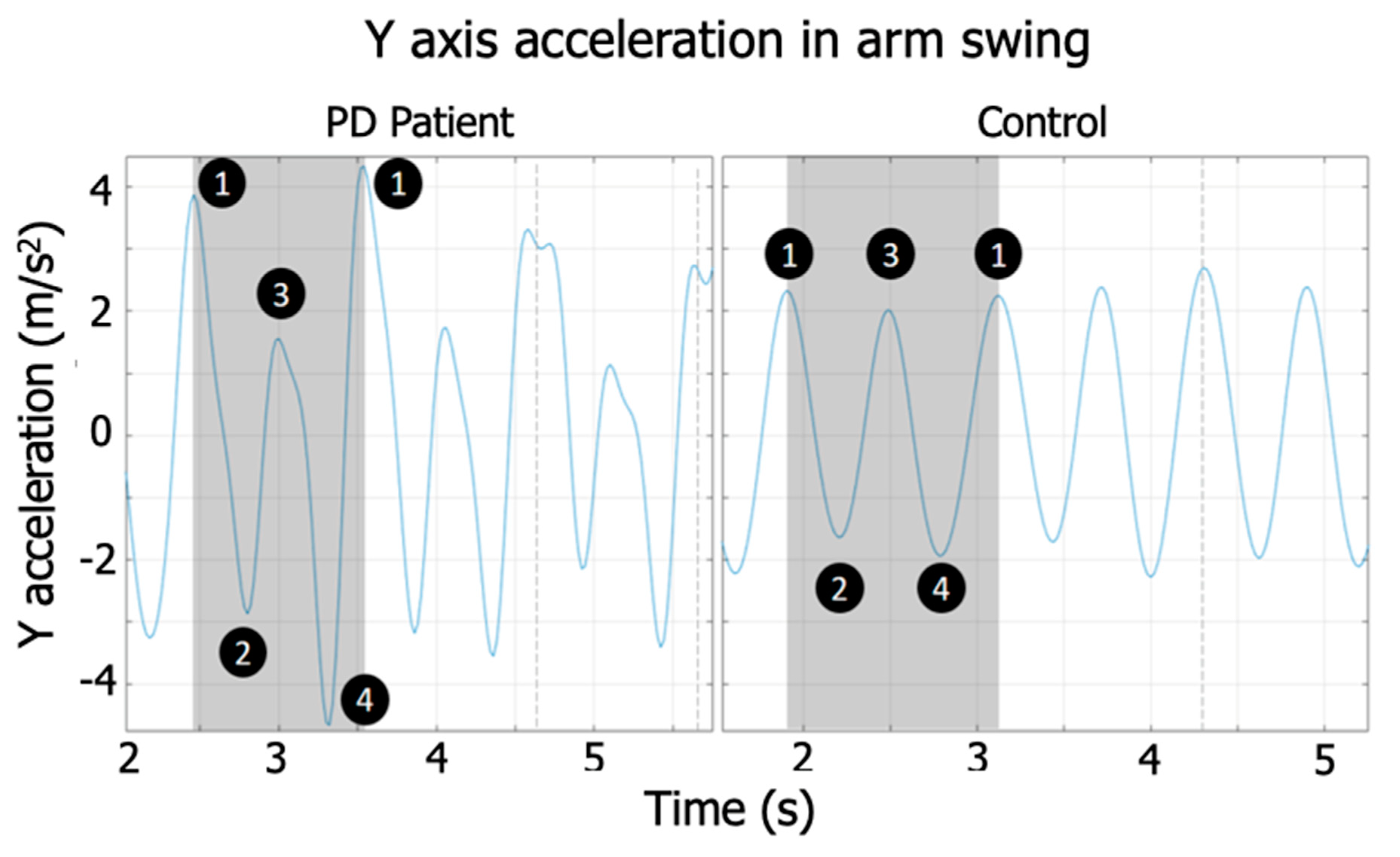
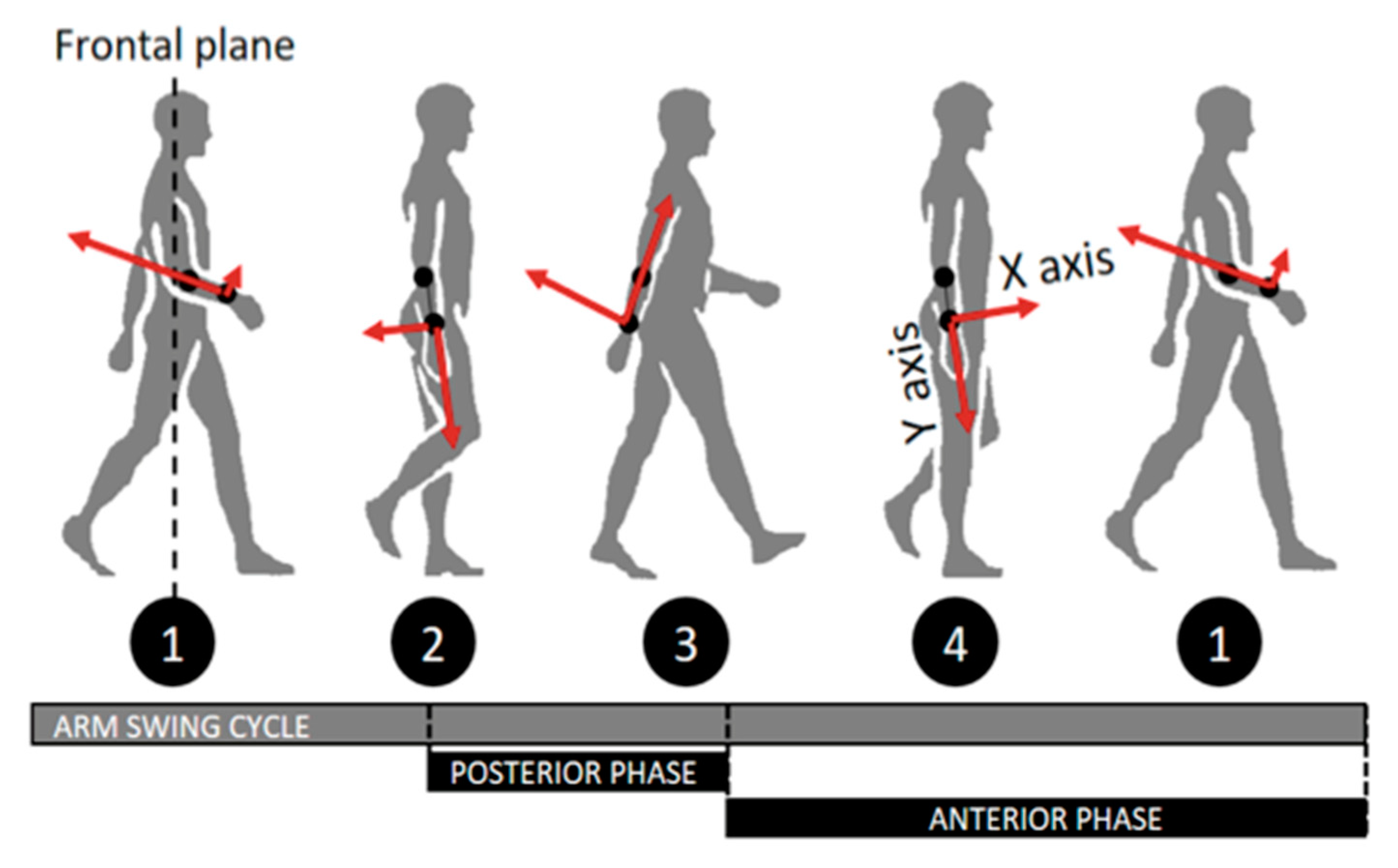
2.4.2. Arm Swing Cycle Regularity and Arm Swing Posterior–Anterior Phase Regularity
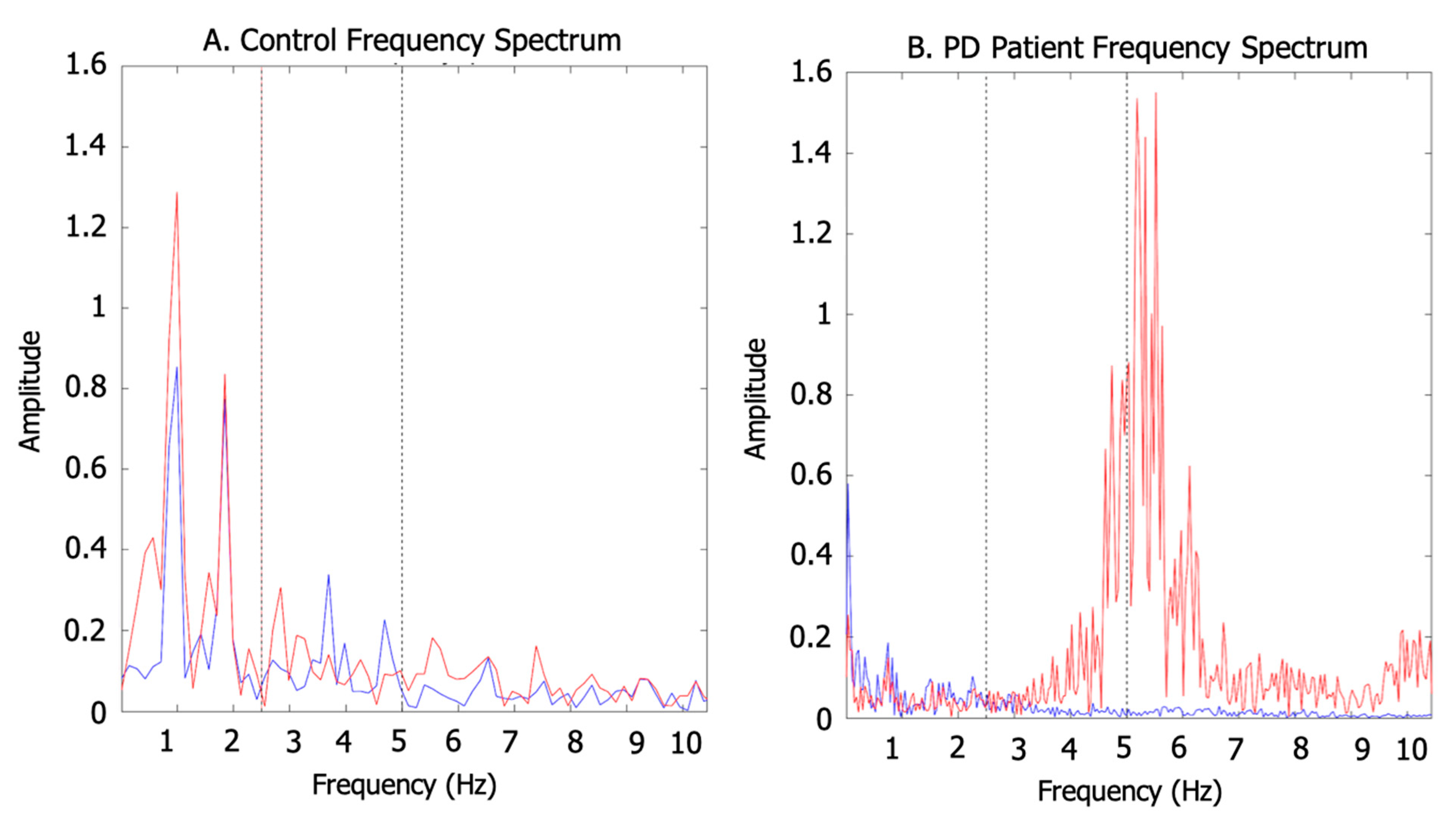
2.4.3. Arm Swing Energy Distribution
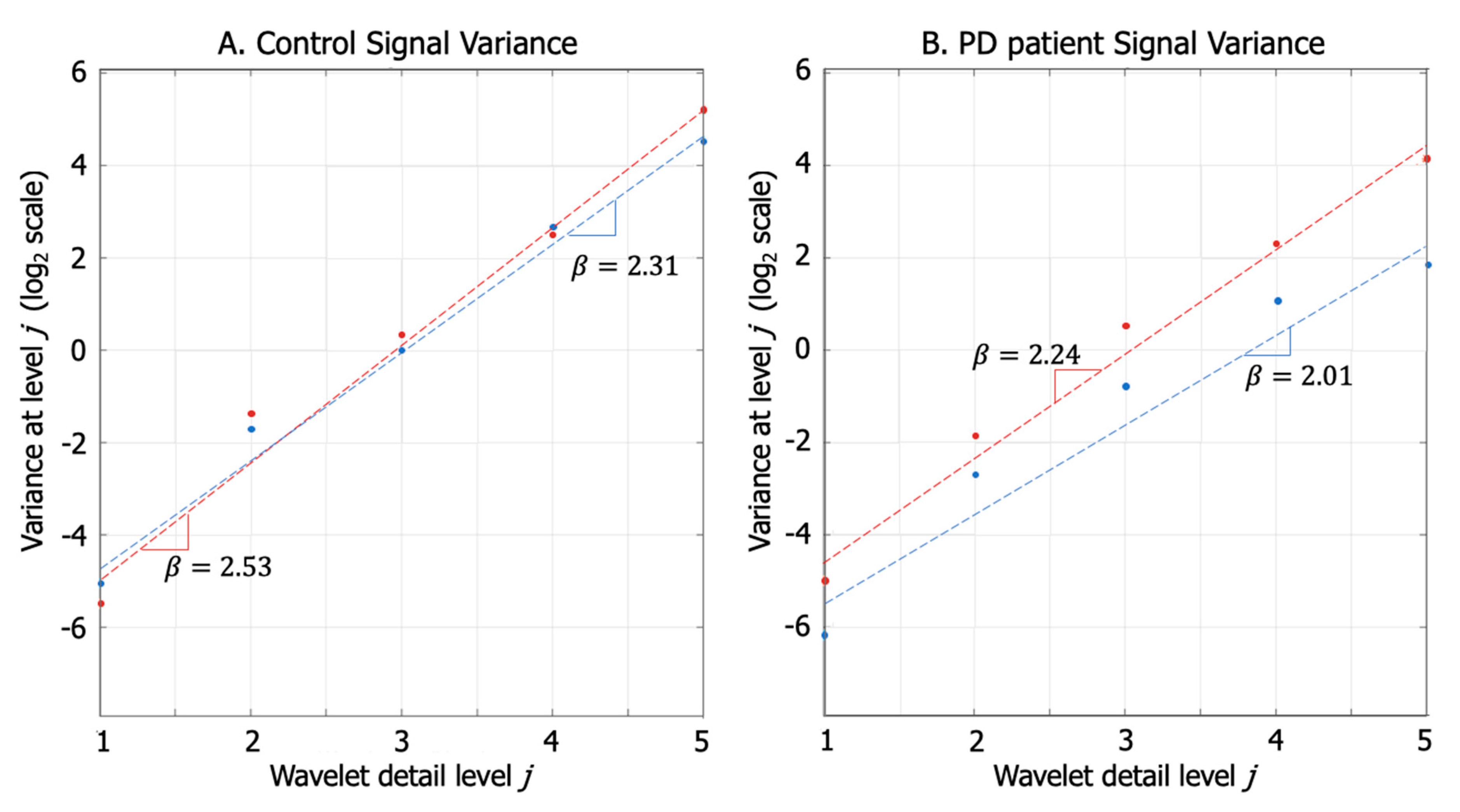
2.4.4. Fractal Dimension of Arm Swing Signals
2.5. Clinical Evaluation
2.6. Statistical Analysis
3. Results
4. Discussion
Advantages, Limitations, and Future Work
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mhyre, T.R.; Boyd, J.T.; Hamill, R.W.; Maguire-Zeiss, K.A. Parkinson’s Disease. In Protein Aggregation and Fibrillogenesis in Cerebral and Systemic Amyloid Disease; Harris, J.R., Ed.; Springer: Dordrecht, The Netherlands, 2012; Volume 65, pp. 389–455. ISBN 978-94-007-5415-7. Available online: http://www.springerlink.com/index/10.1007/978-94-007-5416-4_16 (accessed on 20 May 2020).
- Maetzler, W.; Hausdorff, J.M. Motor signs in the prodromal phase of Parkinson’s disease. Mov. Disord. 2012, 27, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.I.I.K.; van Wegen, E.E.H.; de Goede, C.J.T.; Jones, D.; Rochester, L.; Hetherington, V.; Nieuwboer, A.; Willems, A.M.; Kwakkel, G. Measuring gait and gait-related activities in Parkinson’s patients own home environment: A reliability, responsiveness and feasibility study. Parkinsonism Relat. Disord. 2005, 11, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Mitoma, H.; Yoneyama, M. Quantitative Analysis of Motor Status in Parkinson’s Disease Using Wearable Devices: From Methodological Considerations to Problems in Clinical Applications. Parkinson’s Dis. 2017, 2017, 6139716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpinella, I.; Crenna, P.; Calabrese, E.; Rabuffetti, M.; Mazzoleni, P.; Nemni, R.; Ferrarin, M. Locomotor Function in the Early Stage of Parkinson’s Disease. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Roggendorf, J.; Chen, S.; Baudrexel, S.; van de Loo, S.; Seifried, C.; Hilker, R. Arm swing asymmetry in Parkinson’s disease measured with ultrasound based motion analysis during treadmill gait. Gait Posture 2012, 35, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Caramia, C.; Torricelli, D.; Schmid, M.; Munoz-Gonzalez, A.; Gonzalez-Vargas, J.; Grandas, F.; Pons, J.L. IMU-Based Classification of Parkinson’s Disease From Gait: A Sensitivity Analysis on Sensor Location and Feature Selection. IEEE J. Biomed. Health Inf. 2018, 22, 1765–1774. [Google Scholar] [CrossRef]
- Dranca, L.; de Mendarozketa, L.D.A.R.; Gppoñi, A.; Illarramendi, A.; Gomez, I.N.; Alvarado, M.D.; Rodríguez-Oroz, M.C. Using Kinect to classify Parkinson’s disease stages related to severity of gait impairment. BMC Bioinform. 2018, 19, 471. Available online: https://bmcbioinformatics.biomedcentral.com/articles/10.1186/s12859-018-2488-4 (accessed on 20 May 2020). [CrossRef]
- Harris, T.J.; Owen, C.G.; Victor, C.R.; Adams, R.; Ekelund, U.; Cook, D.G. A comparison of questionnaire, accelerometer, and pedometer: Measures in older people. Med. Sci. Sports Exerc. 2009, 41, 1392–1402. [Google Scholar] [CrossRef]
- Esliger, D.W.; Probert, A.; Gorber, S.C.; Bryan, S.; Laviolette, M.; Tremblay, M.S. Validity of the Actical Accelerometer Step-Count Function. Med. Sci. Sports Exerc. 2007, 39, 1200–1204. [Google Scholar] [CrossRef]
- Brajdic, A.; Harle, R. Walk detection and step counting on unconstrained smartphones. In The 2013 ACM International Joint Conference on Pervasive and Ubiquitous Computing-Ubicomp ’13; ACM Press: Zurich, Switzerland, 2013; p. 225. Available online: http://dl.acm.org/citation.cfm?doid=2493432.2493449 (accessed on 19 December 2019).
- Dalton, A.; Khalil, H.; Busse, M.; Rosser, A.; van Deursen, R.; ÓLaighin, G. Analysis of gait and balance through a single triaxial accelerometer in presymptomatic and symptomatic Huntington’s disease. Gait Posture 2013, 37, 49–54. [Google Scholar] [CrossRef]
- Liu, K.; Liu, T.; Shibata, K.; Inoue, Y.; Zheng, R. Novel approach to ambulatory assessment of human segmental orientation on a wearable sensor system. J. Biomech. 2009, 42, 2747–2752. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Mahoney, J.M.; Lewis, M.M.; Du, G.; Piazza, S.J.; Cusumano, J.P. Both coordination and symmetry of arm swing are reduced in Parkinson’s disease. Gait Posture 2012, 35, 373–377. [Google Scholar] [CrossRef] [Green Version]
- Erdem, N.S.; Ersoy, C.; Tunca, C. Gait analysis using smartwatches. In Proceedings of the 2019 IEEE 30th International Symposium on Personal, Indoor and Mobile Radio Communications (PIMRC Workshops), Istanbul, Turkey, 8–11 September 2019; pp. 1–6. [Google Scholar]
- Gurchiek, R.D.; Garabed, C.P.; McGinnis, R.S. Gait Event Detection using a Thigh-Worn Accelerometer. Gait Posture 2020, 80, 214–216. [Google Scholar] [CrossRef] [PubMed]
- Schneider, B.; Banerjee, T.; Grover, F.; Riley, M. Comparison of gait speeds from wearable camera and accelerometer in structured and semi-structured environments. Healthc. Technol. Lett. 2020, 7, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Leirós-Rodríguez, R.; Romo-Pérez, V.; García-Soidán, J.L.; Soto-Rodríguez, A. Identification of Body Balance Deterioration of Gait in Women Using Accelerometers. Sustainability 2020, 12, 1222. [Google Scholar] [CrossRef] [Green Version]
- Rastegari, E.; Azizian, S.; Ali, H. Machine learning and similarity network approaches to support automatic classification of parkinson’s diseases using accelerometer-based gait analysis. In Proceedings of the 52nd Hawaii International Conference on System Sciences, Grand Wailea, Maui, HI, USA, 8–11 January 2019. [Google Scholar]
- Choi, S.-I.; Moon, J.; Park, H.-C.; Choi, S.T. User identification from gait analysis using multi-modal sensors in smart insole. Sensors 2019, 19, 3785. [Google Scholar] [CrossRef] [Green Version]
- Patel, M.; Pavic, A.; Goodwin, V.A. Wearable inertial sensors to measure gait and posture characteristic differences in older adult fallers and non-fallers: A scoping review. Gait Posture 2020, 76, 110–121. [Google Scholar] [CrossRef]
- Petraglia, F.; Scarcella, L.; Pedrazzi, G.; Brancato, L.; Puers, R.; Costantino, C. Inertial sensors versus standard systems in gait analysis: A systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2019, 55, 265–280. [Google Scholar] [CrossRef]
- Narayanan, A.; Desai, F.; Stewart, T.; Duncan, S.; Mackay, L. Application of Raw Accelerometer Data and Machine-Learning Techniques to Characterize Human Movement Behavior: A Systematic Scoping Review. J. Phys. Act. Health 2020, 17, 360–383. [Google Scholar] [CrossRef]
- Preece, S.J.; Goulermas, J.Y.; Kenney, L.P.J.; Howard, D. A Comparison of Feature Extraction Methods for the Classification of Dynamic Activities from Accelerometer Data. IEEE Trans. Biomed. Eng. 2009, 56, 871–879. [Google Scholar] [CrossRef]
- Yang, C.-C.; Hsu, Y.-L.; Shih, K.-S.; Lu, J.-M. Real-Time Gait Cycle Parameter Recognition Using a Wearable Accelerometry System. Sensors 2011, 11, 7314–7326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moe-Nilssen, R.; Helbostad, J.L. Estimation of gait cycle characteristics by trunk accelerometry. J. Biomech. 2004, 37, 121–126. [Google Scholar] [CrossRef]
- Sekine, M.; Tamura, T.; Akay, M.; Fujimoto, T.; Togawa, T.; Fukui, Y. Discrimination of walking patterns using wavelet-based fractal analysis. IEEE Trans. Neural Syst. Rehabil. Eng. 2002, 10, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Lewek, M.D.; Poole, R.; Johnson, J.; Halawa, O.; Huang, X. Arm swing magnitude and asymmetry during gait in the early stages of Parkinson’s disease. Gait Posture 2010, 31, 256–260. [Google Scholar] [CrossRef] [Green Version]
- Kwon, K.-Y.; Kim, M.; Lee, S.-M.; Kang, S.H.; Lee, H.M.; Koh, S.-B. Is reduced arm and leg swing in Parkinson’s disease associated with rigidity or bradykinesia? J. Neurol. Sci. 2014, 341, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Bryant, M.S.; Rintala, D.H.; Hou, J.G.; Charness, A.L.; Fernandez, A.L.; Collins, R.L.; Baker, J.; Lai, E.C.; Protas, E.J. Gait variability in Parkinson’s disease: Influence of walking speed and dopaminergic treatment. Neurol. Res. 2011, 33, 959–964. [Google Scholar] [CrossRef]
- Rennie, L.; Löfgren, N.; Moe-Nilssen, R.; Opheim, A.; Dietrichs, E.; Franzén, E. The reliability of gait variability measures for individuals with Parkinson’s disease and healthy older adults—The effect of gait speed. Gait Posture 2018, 62, 505–509. [Google Scholar] [CrossRef]
- Sugiarto, T.; Lin, Y.; Chang, C.; Hsu, W. Gait analysis based on an inertial measurement unit sensor: Validation of spatiotemporal parameters calculation in healthy young and older adults. In Proceedings of the 2017 IEEE/SICE International Symposium on System Integration (SII), Taipei, Taiwan, 11–14 December 2017; pp. 517–522. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Control Median (IQR) | Patient Median (IQR) | p-Value U-Test | Effect Size d Cohen ** |
|---|---|---|---|---|
| RMS LAS 1 | 5.249 (1.052) | 4.289 (2.163) | <0.05 * | 0.375 |
| RMS MAS 1 | 4.641 (1.511) | 3.493 (2.012) | <0.05 * | 0.934 |
| ASA of RMS 1 | 8.877 (7.849) | 16.385 (14.506) | <0.05 * | 0.927 |
| Posterior–anterior phase regularity LAS 2 | 0.512 (0.288) | 0.562 (0.148) | <0.05 * | 0.378 |
| Posterior–anterior phase regularity MAS 2 | 0.544 (0.241) | 0.629 (0.258) | <0.05 * | 0.324 |
| Arm swing cycle regularity LAS 2 | 0.696 (0.113) | 0.705 (0.137) | 0.142 | 0.250 |
| Arm swing cycle regularity MAS 2 | 0.731 (0.119) | 0.713 (0.115) | 0.359 | 0.041 |
| Low Energy LAS 3 | 5.393 (2.214) | 4.890 (1.882) | 0.156 | 0.351 |
| Mid Energy LAS 3 | 2.907 (1.628) | 2.758 (0.769) | 0.213 | 0.093 |
| High Energy LAS 3 | 5.702 (2.242) | 6.502 (2.045) | <0.05 * | 0.562 |
| Total Energy LAS 3 | 14.543 (6.108) | 14.794 (3.658) | 0.276 | 0.057 |
| Low Energy MAS 3 | 5.321 (1.878) | 4.664 (1.393) | 0.073 | 0.459 |
| Mid Energy MAS 3 | 2.974 (1.655) | 2.595 (0.473) | 0.127 | 0.224 |
| High Energy MAS 3 | 5.786 (2.240) | 7.090 (2.528) | <0.05 * | 0.814 |
| Total Energy MAS 3 | 14.408 (5.825) | 14.600 (3.580) | 0.210 | 0.102 |
| Dx LAS 4 | 1.446 (0.230) | 1.564 (0.288) | <0.05 * | 0.521 |
| Dx MAS 4 | 1.432 (0.243) | 1.607 (0.297) | <0.05 * | 1.196 |
| Dy LAS 4 | 1.529 (0.171) | 1.499 (0.329) | 0.271 | 0.042 |
| Dy MAS 4 | 1.506 (0.215) | 1.523 (0.302) | 0.094 | 0.163 |
| Dz LAS 4 | 1.291 (0.248) | 1.402 (0.210) | <0.05 * | 0.516 |
| Dz MAS 4 | 1.281 (0.179) | 1.459 (0.266) | <0.05 * | 1.153 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rincón, D.; Valderrama, J.; González, M.C.; Muñoz, B.; Orozco, J.; Montilla, L.; Castaño, Y.; Navarro, A. Wristbands Containing Accelerometers for Objective Arm Swing Analysis in Patients with Parkinson’s Disease. Sensors 2020, 20, 4339. https://doi.org/10.3390/s20154339
Rincón D, Valderrama J, González MC, Muñoz B, Orozco J, Montilla L, Castaño Y, Navarro A. Wristbands Containing Accelerometers for Objective Arm Swing Analysis in Patients with Parkinson’s Disease. Sensors. 2020; 20(15):4339. https://doi.org/10.3390/s20154339
Chicago/Turabian StyleRincón, Domiciano, Jaime Valderrama, Maria Camila González, Beatriz Muñoz, Jorge Orozco, Linda Montilla, Yor Castaño, and Andrés Navarro. 2020. "Wristbands Containing Accelerometers for Objective Arm Swing Analysis in Patients with Parkinson’s Disease" Sensors 20, no. 15: 4339. https://doi.org/10.3390/s20154339