
Smartphone App-Based Interventions to Support Smoking Cessation in Smokers with Mental Health Conditions: A Systematic Review

1
The National Institute for Health Innovation, School of Population Health, The University of Auckland, Auckland 1023, New Zealand
2
School of Population Health, The University of Auckland, Auckland 1023, New Zealand
*
Author to whom correspondence should be addressed.
Psych 2023, 5(4), 1077-1100; https://doi.org/10.3390/psych5040072
Submission received: 29 July 2023
/
Revised: 12 September 2023
/
Accepted: 19 September 2023
/
Published: 8 October 2023
(This article belongs to the Section Neuropsychology, Mental Health and Brain Disorders)
Abstract
:Background—Despite global efforts to control tobacco use, smoking remains a leading cause of preventable diseases, mortality, and disparities, especially among individuals with mental health conditions. Smartphone apps have emerged as cost-effective tools to aid smokers in quitting; however, their evidence-based foundation remains understudied. This research conducted two searches to identify relevant apps: one through the scientific literature and the other from app stores. Methods—The study sought apps designed to assist smokers with mental health conditions in quitting. Searches were conducted in the scientific literature and major app stores. The apps found were evaluated for their basis in theory, features, and claimed effectiveness. Usage and rating scores were compared. Results—Among 23 apps found from app store search, only 10 (43%) were evidence-based and none had explicit reference to theory, while all apps identified in the literature were developed by applying theory. However, app store apps had significantly higher user numbers and ratings than those identified in the literature (mean rating 4.7 out of 5.0). Conclusion—Smokers with mental health conditions have limited support from currently available smoking cessation apps. Apps identified in the scientific literature lack sufficient use and longevity. Sustained support beyond research projects is crucial for enabling theoretically informed evidence-based apps to be available for people with mental health conditions, as is greater collaboration between developers and researchers to create apps that engage with end-user design.
1. Introduction
Tobacco smoking is a leading cause of preventable death in the world [1]. Although millions of smokers receive advice from their healthcare providers each year for quitting smoking, and over half of them attempt to quit, the success rate is low [2]. Without any support, the success rate from a quit attempt is about 5% to 7% [3], but it can be raised to over 20% with behavioural intervention even without pharmacotherapy [4,5]. Unfortunately, 85% of tobacco users in the world have no access to cessation support [6].
Mental health conditions and smoking are strongly correlated; people with mental health conditions are far more likely to smoke tobacco than those without mental health conditions, and smoking amplifies the negative impacts of their medication and physical co-morbidities on their mental wellbeing [7,8,9,10]. Nevertheless, there is good evidence that smokers with mental health issues are just as interested in and able to quit smoking as others, even more so when support is provided [7,8,9,10]. For this reason, people with mental illness and other addictions often carry a greater burden of disease due to smoking. Poor lung health, smoking, and poor mental health co-occur: 50% of Chronic Obstructive Pulmonary Disease (COPD) patients have depressive symptoms, and over one in five COPD patients experience anxiety [7,11,12]. Smokers are more likely to develop depressive symptoms than non-smokers [10]. Smokers with mental health issues are also more likely to (1) keep on smoking; (2) consume more tobacco products; (3) die on average 10 to 20 years earlier; and (4) need higher doses of antipsychotic medicines and antidepressants [10]. Smoking also increases socioeconomic and ethnic disparities [7,10,11]. However, by quitting smoking, people may experience a reduction in anxiety, depression, and stress levels; improvements in quality of life and mood; and decreases in use of mental health medicines [7,10,11].
The most recent Cochrane Review found moderate-certainty evidence, limited by inconsistency, that mobile smoking cessation (text message-based) interventions were more effective than minimal smoking cessation support (risk ratio “RR” = 1.54, 95% CI = 1.19 to 2.00; 13 studies, 14,133 participants) [13]. There was also moderate-certainty evidence, limited by imprecision, that text messaging added to other smoking cessation interventions was more effective than the other smoking cessation interventions alone (RR = 1.59, 95% CI = 1.09 to 2.33; four studies, 997 participants) [13]. Compared to traditional in-person interventions, mobile smoking cessation interventions have been shown to improve user engagement with a cessation programme by expanding communication through real-time messaging with support networks, and by reducing barriers to access, such as cost, location, or timing conflicts [14,15,16].
However, text-based programmes have limited functionality, whereas smartphone apps offer more interactive and customisable tools to support smokers throughout the multi-stage process of quitting smoking, such as tools for self-monitoring, progress tracking, urges overcoming, daily reminders, and social support [17]. A growing number of apps purporting to be effective at helping smokers quit are available for downloading [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66].
In recent years, apps have been developed to support individuals with mental health issues to quit smoking [45,47,67]. Research suggests that smoking cessation apps can engage smokers with mental health issues, [27] including those who are not already receiving nor seeking professional help [47], may promote smoking cessation or reduction of tobacco consumption [67], and improve mental health status [45]. With the proliferation of smartphones, mobile health tools are uniquely positioned to reach and influence the smoking populations that need both smoking cessation and mental health support [68]. However, there has been little assessment of the quality of content, engagement, and reach of apps that are underpinned by research or theory, compared with apps commonly used in the marketplace [45,58,59,60,61,62,63,64,65,66,67] that purport to assist smokers with mental health issues to quit [69,70].
The aim of this review was to identify all available apps designed to support smoking cessation of smokers with mental health conditions, identify apps developed from theory and/or empirical scientific evidence, and apps without such a basis, available from app stores and to determine and compare the usage, user ratings, and availability of such apps.
2. Methods
We assessed the app market from two distinct viewpoints: firstly, that of health professionals; and secondly, that of consumers, specifically smokers with mental health conditions. Health professionals typically consult scientific literature, whereas consumers, often without access to such literature, tend to rely on app store recommendations when choosing healthcare apps. This dual approach necessitated our exploration of apps in two ways: firstly, by beginning with the literature and then locating the identified apps in the app stores; and secondly, by directly starting from the app stores.
In alignment with established systematic review practices [69,70,71,72,73], we adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) model [74]. Whilst numerous smoking cessation apps incorporate evidence-based behaviour change strategies, many have not been featured in published research articles. We prioritised apps that have been recognised and recommended by the scientific community, focusing on published research articles as evidence of their scientific support. We identified and assessed apps designed to help smokers with mental health issues quit smoking through a four-step process.
2.1. Identify the Scientific Literature
We performed a literature search of EMBASE, MEDLINE, APA PsycInfo, PubMed, Scopus, ACM Digital Library, and IEEE Xplore on 30 September 2020. A second round of the literature search was conducted on 23 July 2023. The gap is based on two reasons: (1) we aimed for a comprehensive capture of all pertinent studies, especially given the swift evolution and introduction of new apps in the market, and (2) the dynamic nature of the app market and the continuous release of new research articles led us to believe that a more extended gap would yield a richer and more current dataset for our review. Table 1 shows the search terms used in different fields of the study. Because search engines differ between databases, search strategies were adapted to each database. Appendix A shows the search strategies used in the different databases. Only peer-reviewed articles on the topic of smoking cessation apps for smokers with mental health conditions that were published in English before the search date were included for the review.
A data extraction sheet based on the review of mobile phone-based interventions for smoking cessation published in the Cochrane Database of Systematic Reviews [14] was developed to collect data from the identified articles. The data extraction sheet was adapted by adding a field on the impact of the intervention on the mental health statuses of users. One review author (JChe) from the team extracted the data, and the other authors (CB, JC, SM, TS) checked the data. Disagreements were resolved by consensus. Information included: (1) information about the study (including country and year of the study’s implementation); (2) characteristics of the app (including the name of the app, underpinning theories, app development methods, functions, and target users); and (3) evaluation of the app (including the assessment method, interventions, participants, duration, types of measure, findings, bias, and limitations).
No gold standard exists against which to evaluate a smoking cessation app for smokers with mental health conditions. A meta-analysis of study findings was, therefore, not possible. Hence, the identified literature was analysed by identifying the availability, validity, user experience, and effectiveness of current smoking cessation apps for mental health smokers. Analysis of the features of current apps, their potential for improvement, and the feasibility of evaluation to validate these apps’ effectiveness and acceptability was also included.
We assessed risk of bias and obtained methodological details using a standardised form applied by a Cochrane Review on mobile smoking cessation interventions [14]. Different types of bias were assessed across studies including: (1) selection bias—whether study participants are representative to the target population; (2) performance bias and detection bias—whether any types of blinding were performed; (3) attrition bias—incomplete outcome or loss of follow-up; and (4) other bias—specified as small sample size, short follow-up, and confounding factors. Each type of bias was rated for each study by JChe with one of the following three risk levels: “high risk”; “low risk”; and “unclear”. The results of the rating were reviewed by other authors (CB, JC, SM, TS) and agreement was reached between authors.
2.2. Identify the Literature-Based Apps from App Stores
Each app identified in the scientific literature during phase 1 was searched for in each of the following online app stores: the Apple App Store and the Google Play Store. Apps with the same name and developer of those listed in the literature were considered a match. Functions of smoking cessation apps were classified based on the taxonomy created by the National Tobacco Cessation Collaboration (NTCC) [75] and its updated version of the classification method developed by Abroms et al. [71].
2.3. Identify Market-Based Smoking Cessation Apps from App Stores
We searched the two main online app stores (Apple App Store and the Google Play Store) in January 2021 using the following terms: mental health smoking, mental health, and quit smoking. Each search term was searched separately and all three were used for each of the two stores, totaling six separate searches. The top five apps returned per search were documented for each store. Apps not relevant to the support of smoking cessation or improving of users’ mental health status were removed.
2.4. Identify Market-Based Apps Developed from Theory or Empirical Evidence
The top five apps per search term were opened and reviewed regarding their developers, theories, development methods, smoking cessation features, mental health features, target users, categories, charges (pay for download or free), download rate, and user rating. The description (both in app stores and in the “About” section of the apps) of the apps was reviewed to determine if the reviewed apps were developed based on theories. An app with explicit theory or theoretical functions or components mentioned in its description was considered as theory-based. Apps that had been tested in a methodologically robust way were considered as based on empirical evidence. Only the top five apps were chosen to best represent real search behaviours of focusing on the top apps of search results, which is unlikely to include all apps available for the given health concerns [76,77]. An app list was created by one review author (JChe) and shared with the other review authors (CB, JC, SM, and TS). All authors reviewed and analysed apps independently and discussed the key findings of the analysis.
3. Results
3.1. Literature Search Results
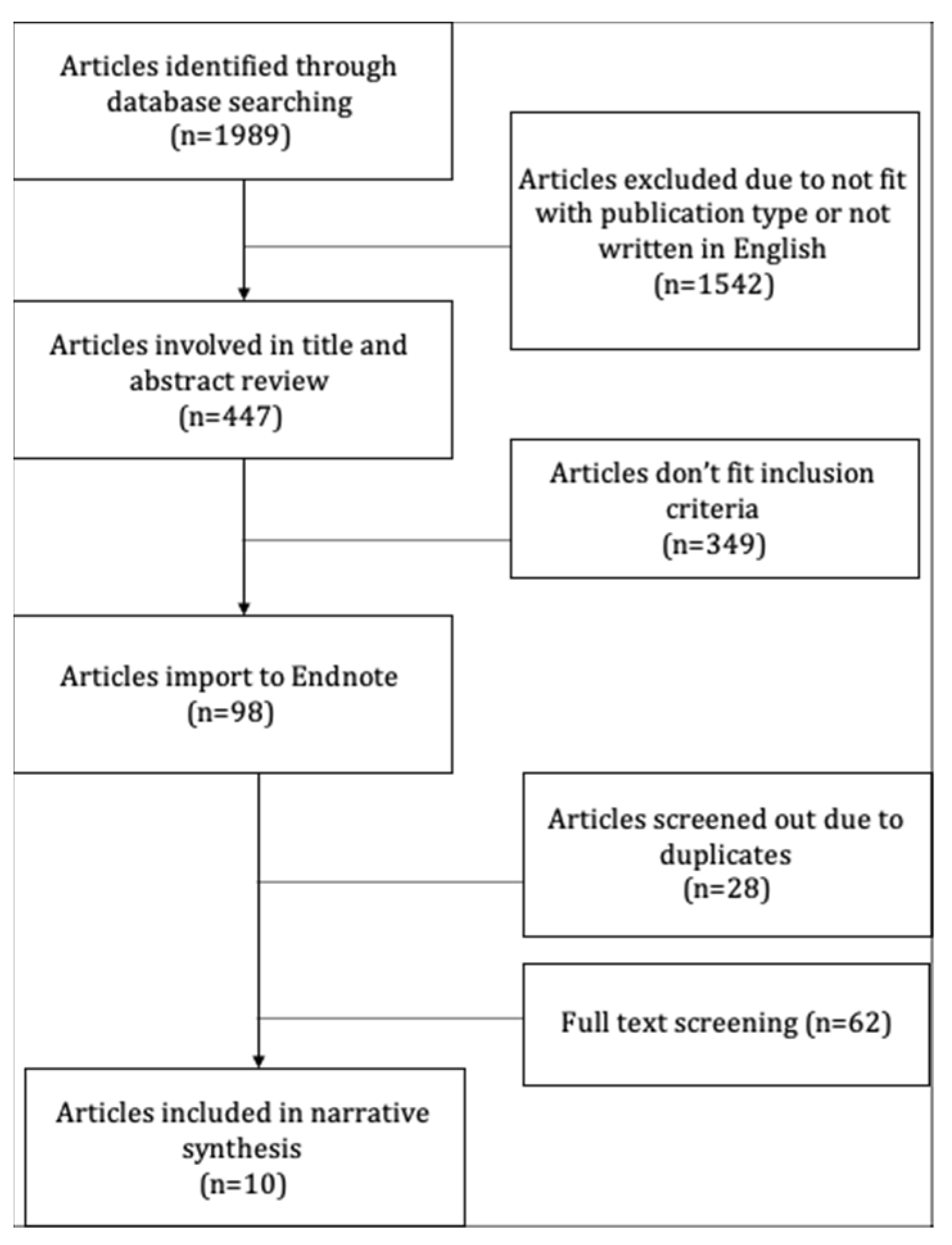
The search of listed databases provided a total of 1989 articles. After adjusting publication types and written languages, 447 articles remained. Of these, 349 articles were discarded because after reviewing the abstracts, these articles did not meet the inclusion criteria. The review article inclusion criteria include: (1) studies that focus on smartphone app-based interventions for smoking cessation; (2) research articles that specifically target smokers with mental health conditions; (3) studies published in English or Chinese; (4) peer-reviewed articles published between January 2010 and July 2023, and (5) articles that provide clear outcomes related to the efficacy or effectiveness of the app interventions. By the end of the title and abstract review, 98 articles were imported into the Endnote reference management system, where 28 duplicate articles were identified and excluded.
The full text of the remaining articles was examined In detail. Two additional articles were identified by the search conducted on 23 July 2023. Sixty-one studies did not meet the inclusion criteria as described, leaving only ten studies in the systematic literature review. No additional studies were identified by checking the references of located, relevant papers and searching for studies that have been cited by included studies. No unpublished studies were obtained. The flow diagram of articles selection is shown in Figure 1. Appendix A summarises the details of the reviewed studies.
All ten reviewed articles were published in English. Two of these articles reported pilot randomised controlled trials (RCTs), four reported qualitative studies, two reported pilot trials, one reported a full RCT, one reported a development study, and one reported a mixed-method study. The duration of studies ranged from three days to six months. The studies involved a total of only 160 participants. The main inclusion criteria entailed adults (18 years or older), smokers (smoke one or more cigarettes or using other types of tobacco products on a daily basis), with mental health issues (10 out of 160 studied participants were not diagnosed with psychotic disorders) and using a smartphone. The studied intervention in the reviewed articles is a smoking cessation app for smokers with mental health issues.
The primary outcome of six reviewed studies was smoking status of participants. Smoking status was measured in different ways, including self-reported smoking abstinence and biochemical verification of smoking abstinence with different follow-up. Four studies reported smoking abstinence with biochemical verification [45,67,78,79]. The duration of abstinence ranged from 7-day to 30-day. Secondary outcomes of reviewed studies included adherence, user experience, participant mental health status, acceptability, and feasibility of the intervention.
Six studies concluded that smoking cessation apps support smokers with mental health conditions to quit smoking [29,45,67,78,80,81]. However, none of these studies had conclusive findings on the effectiveness of smoking cessation apps. User experience of smoking cessation apps varied across different studies [25,29,45,47,67,81]. The majority indicated smoking cessation apps achieved positive user experience, while one study stated that the smoking cessation app scored five points below industry standard (65.5 out of 100) on the user experience measuring scale [25]. The same study found that some features of smoking cessation app are redundant and rarely used [25]. Eight studies measured participants’ adherence to intervention activities. Most of these studies reported a high compliance level of participants to intervention [25,45,47,67,78], while one reported low compliance [81]. Only one study measured participants’ mental health status [45]. This study indicated that the use of smoking cessation app led to a significant decrease in depressive symptoms among app users [45].
Due to the diversity of study designs, participants, interventions, and outcome measures, and a high risk of bias (Appendix B), a meta-analysis of these studies was not appropriate [82].
Four studies had a high risk of selection bias—specific population groups (e.g., mental health smokers from high socioeconomic status) were invited to take part in these studies, leading to a lack of generalisability of the study results [25,47,67,83]. All reviewed trials had a high risk of performance bias because blinding was not performed by researchers or trial participants in any of these trials [29,45,67,78,79]. The majority of reviewed studies had small sample sizes and failed to detect a statistically significant smoking cessation outcome [29,45,67,78,79]. All studies had a short to medium length of follow-up. Two studies had a six-month follow-up, while the other studies had less than a three-month follow-up. The reviewed studies could not detect the long-term impacts of smoking cessation apps on smokers with mental health conditions. Two reviewed studies have no post-treatment assessment to the control group, which made it impossible to identify the size of the effect of the evaluated interventions [45,79].
3.2. Apps Identified from the Literature Search
Five smoking cessation apps for smokers with mental health conditions were identified from the reviewed studies. Details of these apps (both from the literatures and app store search) are summarised in Appendix C. All were built based on theories and clinical guidelines. Six had their development methods and processes discussed in the reviewed articles. Seven focused on smokers with mental health conditions while one targeted all smokers. Two apps include functions for both smoking cessation and mental health management, but six had only functions for smoking cessation. Four apps include the keyword “quit” in their name.
Three were unavailable in both the Apple and the Google App store, one was only available at no cost in the Apple app store, while four were available (free of charge) in both Apple and Google App stores. Four apps have their download rates available in the Google App store. The user rating scores are available for five literature-based apps. The app named Actify! has a user rating score of 1.5 out of 5.0 in the Apple App store, but it was only rated by four users. The app quitSTART was rated as 4.5 out of 5.0 (No. of reviewers = 1500) in the Apple App store and rated as 3.4 out of 5.0 (No. of reviewers = 276) in the Google App store.
3.3. Smoking Cessation Apps in App Stores
Appendix D summarises the details of the top listed apps identified from the app store search. The Apple App store search returned 13 apps and the Google App store returned ten apps (some apps exist more than once when searching by different keywords). Three apps (Wysa: Mental Health Support, MindDoc: Depression & Anxiety, and Smoke Free—Stop Smoking Now) existed multiple times in both app stores and for different keywords. Some keywords, such as “mental health” (n = 5), “smok*” (n = 8), and “quit” (n = 8) are common in the names of the apps.
By entering “mental health smoking” into the Google App store, two of the top five returned apps focused on mental health conditions and three on smoking cessation. The most commonly seen smoking cessation functions are Calculator (n = 3) and Gamification (n = 3). By entering “mental health” into the same app store, the top five apps all focus on supporting mental health management. The most common functions of these apps are Mood tracking (n = 4), Mental health practice (n = 4), and Diary (n = 3). By entering “quit smoking” into the app store, four of the top five returned apps are focusing on supporting users to quit smoking, and one is focusing on both supporting smoking cessation and mental health management. The most common functions among these apps are Calendar (n = 4), Gamification (n = 3), and Information (n = 3).
Eleven out of the 13 apps from the Apple App store require in-app purchases, which means some functions of the app are not available to users unless users pay for using. The price of these features ranged from $1.69 to $159.99 NZD (approx. $1.21 to $114.81 USD). All download rates were for apps in the Apple App store. Ten apps have their user rating scores available in the Apple App store. The average user rating score of these ten apps is 4.7 out of 5.0 (ranged from 4.5 to 5.0 out of 5.0). The average number of reviewers is 606 (ranged from 5 to 3100 reviewers).
All apps identified from the Google App store require in-app purchases. The price of these features ranged from NZD $1.69 to $239.99 (approx. $1.21 to $172.22 USD). Six of these apps were downloaded over 1,000,000 times, two were downloaded over 500,000 times, one was downloaded over 100,000 times and one was downloaded over 1000 times. The average user rating score of these apps is 4.7 out of 5.0 (ranged from 4.5 to 4.8 out of 5.0). The average number of reviewers is 41,109 (ranged from 94 to 100,413 reviewers).
3.4. Apps from the App Stores Developed Based on Theories
Six apps from Apple App Store were developed by following theories to help their users. Two of these apps post their development methods in the app store page. Four identified apps from the Google App Store use theory-based approaches to support their users. One shows its development method in the app store page. Seven apps from the Apple App Store were developed to target smokers, five were designed to support the general population who want to maintain good mental health, and one was developed to support construction workers. Nine of these apps are categorised as Health and Fitness apps, three as Lifestyle apps, and one as a Medical app. Five identified apps from the Google App Store are targeting smokers while the other five are targeting the general population. Eight of them are categorised as Health and Fitness apps, and two as Medical apps. Most apps (n = 21 out of 23) from app stores have either functions for supporting smoking cessation or managing mental health status.
4. Discussion
This systematic review aimed to identify smoking cessation apps for smokers with mental health conditions. A search of studies from seven databases identified only ten studies, 75% of which provide some supportive evidence of positive impacts of smoking cessation apps on helping smokers with mental health conditions to quit smoking. Most of the reviewed articles were small pilot studies. It was impossible to conduct a meaningful meta-analysis with such heterogeneous measures [82]. Nevertheless, the narrative synthesis of evidence about mHealth app-based interventions for smoking cessation enables researchers to make several observations, as follows.
4.1. Findings from Reviewed Studies
Based on the reviewed studies, there are no standard methods to develop or evaluate smoking cessation apps for smokers with mental health conditions. In general, the sample sizes of current studies are small. Most reviewed studies were unable to detect statistically significant results.
The effectiveness of supporting smoking cessation and user experience are the two most common outcome measures of the reviewed studies. Most studies indicated that smoking cessation apps had some positive impacts on supporting smokers with mental health conditions to quit smoking. In contrast, two studies show that smoking cessation apps may weaken the effectiveness of another smoking cessation programme when used together [29,79]. Other literature reviews [70] on smoking cessation apps and app content analysis [72,73,84,85,86,87,88,89,90,91,92] also draw the same conclusion: that the evidence for the effectiveness of smoking cessation apps in helping smokers to quit smoking is limited.
User satisfaction and perceived effectiveness were used to reflect the user experience of apps. Most reviewed studies found that participants perceived smoking cessation apps as a helpful tool to support smoking cessation. Two studies indicate that smoking cessation apps have an average user satisfaction. For instance, the study conducted by Vilardaga et al. found that the app “QuitPal” was five points below the industry standard based on the rating given by the study participants on the system usability scale (SUS) [25]. As mentioned by some smoking cessation app studies and reviews, limited evidence is available about the factors that increase a smoking cessation app’s user experience. Some potential positive factors may include providing multi-media information (e.g., audio, video) to users and being built by following theories [20,23,28,42,49,50,88].
Although all studies targeted smokers with mental health conditions, only one study measured the mental health status of the participants. In Heffner’s study, a significant decrease in Patient Health Questionnaire (PHQ) score was found in participants who used the smoking cessation app to achieve smoking abstinence (mean change in PHQ–9 scores were −4.5, 95% CI −7.7 to −1.3; p = 0.01) [45]. However, the mechanism between quitting smoking and improving mental health status was not explained. The reason why mental health status was not included as an outcome measurement by most of the reviewed studies is not made clear, but what is clear is that mental health status improvement should be an essential parameter to include in studies, given the strong correlation between tobacco use and mental health conditions [7,8,9,10].
4.2. Findings from App Review
Overall, 31 apps were discussed in this review (eight reviewed literature-based apps, and twenty-three apps identified from the Apple and Google App stores). Key words, such as “mental health”, “smok*”, and “quit” are very common in apps from app stores than apps introduced in the reviewed studies. This may be the reason why the literature-based apps were difficult to find in app stores (three out of eight apps were unavailable). Instead of typing the names of the research-based apps, these apps were out of the top 50 searching results when typing terms, such as “mental health smoking”, “mental health”, and “quit smoking”. It is very unlikely for smartphone users to download an app that requires too many scrolls or swipes [76,77]. It will be worthwhile for researchers who are developing smoking cessation apps for smokers with mental health smokers to understand the logic of app stores for exhibiting apps in response to search. One technique is the use of the hyphen between the app name and the aims of the app. For example, the apps’ names like “What’s Up?—A Mental Health App”, “Stop Smoking—EasyQuit free”, and “Flamy—quit smoking & become a non-smoker” make them easy to navigate when typing the correct keywords.
All literature-based apps use approaches developed based on theories to support smoking cessation and mental health management. In comparison, less than half of the apps searched from app stores apply theory-based approaches. The finding of lack of theory-based approaches in health-related commercial apps is similar to other studies on health-related apps targeting other conditions [93,94]. The application of theory-based approaches to support smoking cessation and mental health management should be used as a marketing highlight to promote the literature-based apps or other research-based apps. Supportive evidence has been found from an existing smoking cessation app analysis. Cheng et al. found that a smoking cessation app’s theories and guideline adherence level is positively related to its rating in app stores [88]. Abroms et al. also found that a smoking cessation app’s user experience rating is positively associated with its score on the application of theory and guideline-based approaches [71]. Although there are some exceptions, the application of theory-based approaches secures the safety, rigour, and potentially, the effectiveness of the apps.
Two literature-based apps have both smoking cessation and mental health management functions, while two apps searched from the app stores have functions from both categories. However, the functions of app store-searched apps are relatively easier compared to the literature-based apps. For instance, the app named “Construction Industry Helpline” has both smoking cessation and mental health-related functions, but the smoking cessation approach it uses is just providing smoking harm information to users. This situation is less common among research-based apps. For example, the app called “Stay Quit Coach” introduced by reviewed studies has multiple functions related to both smoking cessation and mental health management [29,47,81]. As introduced, smoking and mental health conditions are two strongly connected health conditions [7,8,9,10]. It is important to understand the mechanism between how these two factors affect one another before designing an appropriate smoking cessation app for smokers with mental health conditions.
The majority of apps searched from app stores only provide free trial versions for their users. The cost of these apps is varied. It shows the business potentials of smoking cessation and/or mental health management apps, but also reflects the potential cost for maintaining these products. Although the download rate is unavailable for apps from Apple App Store, the identified apps from the Google App Store provide some information about how popular these apps are. Based on the ten identified apps from the Google App Store, six of them were downloaded over 1 million times. The massive difference in download rates reflects a vast difference between the literature-based and commercial apps to reach their target users. Commercial apps also achieve higher user rating scores and are more likely to be rated by their users than the literature-based apps. They provide some excellent examples for researchers about designing and developing an attractive and engaging app. Collaboration between research teams and commercial companies or applying app design standards from commercial companies can be a method to improve the attractiveness and engagement of research-based apps [95,96].
4.3. Limitations
There are a number of limitations in this systematic review. First, there was an inconsistency of interventions and study settings, making a meta-analysis inappropriate [13]. Without a meta-analysis, no conclusive statements can be made about the impacts of smoking cessation apps on supporting smokers with mental health conditions. More standardised approaches to the research design and evaluation would enable greater comparability between studies. Second, the quality of studies varied widely. Six trials had a small sample size (n < 50 participants) and failed to detect statistically significant results. Most studies had a short follow-up (<3 months) and were unable to measure long-term impacts. Only one study measured changes in participants’ mental health status. Studies with larger sample sizes, longer follow-up, and measures of a range of impacts are needed. A third limitation of this study is the limited number of apps included in our analysis (n = 31, eight based on reviewed literature and 23 from app stores). Commercial apps were the top five apps in the two major app stores but there are hundreds of apps available in both app stores that were not reviewed.
5. Conclusions
In this systematic review, we meticulously examined the current literature on smoking cessation apps tailored for smokers with mental health conditions. Our findings underscore a notable gap: there is limited evidence to conclusively determine the efficacy of these apps in assisting individuals with mental health challenges to quit smoking. While the impact of these apps on users’ mental health remains largely uncharted, it is evident that apps grounded in research are generally perceived as effective by their users, often employing theory-driven strategies.
However, a stark contrast emerges when comparing research-based apps with their commercial counterparts. The former, despite their evidence-based foundations, often fall short in terms of user engagement and appeal. Enhancing the marketability of research-based apps is crucial. Adopting effective naming conventions and aligning with industry design standards can significantly elevate their appeal.
Moving forward, there is a compelling case for the creation of smoking cessation apps for this demographic, drawing from both scientific evidence (including established theories and pertinent clinical guidelines) and the best practices observed in popular commercial apps. Future research, particularly randomised controlled trials, should aspire for more robust methodologies, encompassing larger participant cohorts, extended monitoring durations, and a broader spectrum of outcome metrics.
Author Contributions
Conceptualization, C.B. and J.C. (Jinsong Chen); methodology, C.B. and J.C. (Jinsong Chen); literature search, J.C. (Jinsong Chen); formal analysis, C.B., J.C. (Joanna Chu), S.M. and J.C. (Jinsong Chen); writing—original draft preparation, J.C. (Jinsong Chen); writing—review and editing, C.B., J.C. (Joanna Chu), S.M., J.C. (Jinsong Chen) and T.S.; visualization, J.C. (Jinsong Chen); supervision, C.B.; project administration, J.C. (Jinsong Chen). All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by The Ember Korowai Takitini, grant number 20201214.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Acknowledgments
We would like to acknowledge our study funder The Ember Korowai Takitini for providing us with an opportunity to work on such an interesting and meaningful topic.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A

{kind=link}
Table A1.
Details of the Reviewed Studies.
| Source | Study Design Participant | Interventions and Follow-Up | Outcomes and Measures |
|---|---|---|---|
| Hertzberg et al., 2013 [78] | Pilot RCT Smokers with PTSD (n = 22) | Intervention: mCM (app) and two smoking cessation counselling sessions, nicotine replacement, and bupropion (n = 11) Control: non-app conditions (n = 11) | Adherence: Compliance with trial activities Smoking status: CO-verified 7-day PPA at 4-week and 3-month follow-up |
| Vilardaga et al., 2016 [25] | Qualitative study Individuals with a history of serious mental illness (n = 5) | Day 1: introduced participants to QuitPal (app) with a brief hands-on demonstration and explained its functions Day 2–3: participants field-tested QuitPal and interacted with the app to gain a more in-depth user experience | Adherence: App usage logs User experience: Interview and SUS questionnaire |
| Hicks et al., 2017 [29] | Pilot RCT Smokers with PTSD (n = 11) | Intervention: QUIT4EVER, an intervention combining mobile contingency management smoking cessation counselling and medications, and the SCQ app (n = 5) Control: a contact control condition that was identical to QUIT4EVER except SCQ app was not included (n = 6) | Smoking status: Self-reported prolonged smoking abstinence User experience: Perceived effectiveness on a Likert scale questionnaire |
| Minami et al., 2018 [67] | Pilot trial Smokers with psychiatric disorders (have a depressive disorder or bipolar disorder) (n = 8) | A smartphone intervention app that prompts participants to practice mindfulness (listening to an audio recording on the smartphone five times per day), complete EMA reports five times per day, and submit CO videos twice per day Follow-up: Three months | Adherence: Compliance with trial activities Smoking status: CO-verified 7-day PPA at 2-, 4-week, and 3-month post-quit follow-ups, and Cigarettes use reduction. User experience: Satisfaction to the programme questionnaire |
| Heffner et al., 2019 [45] | Pilot trial Daily smokers with mild to moderate depressive symptoms (n = 16) | Smokefree TXT along with Actify! (app) to provide cessation content that had not yet been built into the app for this pilot testing Follow-up: Six weeks | Adherence: Number of log-ins per participants and reported usability challenges Mental health status: Depressive symptoms measured by the PHQ Smoking status: CO-verified, 7-day and 30-day PPA at 6-week follow-up User experience: Interview |
| Herbst et al., 2019 [47] | Qualitative study | Use of the SQC app | Adherence: Retention User experience: Comfort levels with mobile technology (baseline measure)—the PMPIQ-P and Interview |
| US military veterans with PTSD who smoked at least five cigarettes per day for 15 of the past 30 days and stated an interested in cessation (n = 20) | Follow-up: Three months | ||
| Klein et al., 2019 [80] | Qualitative study | Intervention: view prototype of the Kick.it app | Acceptability: Explored participants’ smoking-related experiences and perceptions of social support for smoking cessation Feasibility: Participants’ perceptions of the feasibility, utility, and acceptability of the app features for SMI populations |
| Smokers with severe mental illness (SMI) (n = 12) | Follow-up: Two consecutive semi-structured in-depth interviews (Stage 1 = 1 h, Stage 2 = 1.5 h) | ||
| Wilson et al., 2019 [81] | Qualitative study | The intervention included mobile contingency management (i.e., financial compensation for confirmed abstinence from smoking), pharmacotherapy for smoking cessation, cognitive–behavioural counselling sessions, and the use of SQC app for relapse prevention | Adherence: Compliance with treatment Smoking status: Self-reported smoking abstinence User experience: Interview Perception of usefulness |
| Smokers with schizophrenia, schizoaffective, or psychotic disorders) two cohorts (Cohort 1 n = 5, Cohort 2 n = 8, total n = 13) | Follow-up: Three months | ||
| Alyssa et al., 2020 [79] | RCT | Intervention: mobile CM (i.e., monetary compensation for bio-verification of abstinence through using a phone app), CBT, and pharmacotherapy for smoking cessation (n = 21) | Acceptability: A questionnaire assessing eight self-reported items Feasibility: A questionnaire that was completed by the therapist about the participant Knowledge of treatment: A tailored questionnaire Smoking status: Self-reported prolonged abstinence, Bio-verified (including saliva and CO verification) prolonged abstinence at 6-month follow-up, 7-day, and 30-day self-reported PPA |
| Smokers with diagnosed mental health illness (n = 34) | Control: ITC, which contained all components except the CM (n = 13) Follow-up: Six months | ||
| Gowarty et al., 2021 [83] | Mixed-method (descriptive statistics and analysis of app utilisation data and semi-structured interview) | Intervention: QuitGuide and quitSTART. Participants were randomly assigned to one of the two apps. | Adherence: backend app usage data Acceptability: perceptions of the acceptability assessed using a modified version of the Acceptability of Intervention Measure (AIM) User experience: assessed using the System Usability Scale (SUS) |
| Daily smokers (n = 17, and 7 of them were diagnosed with psychotic disorders) | Follow-up: The follow-up period lasted for 2 weeks, during which participants were instructed to use their assigned app independently. |
SUS: System Usability Scale; PPA: Point Prevalence Abstinence; PHQ: Patient Health Questionnaire; PTSD: Post-Traumatic Stress Disorder; PMPIQ-P: Perceptions of Mobile Phone Interventions Questionnaire–Patient (version); EMA: Ecological Momentary Assessment; CO: Carbon Monoxide; CBT: Cognitive Behavioural Therapy; ITC: Intensive Treatment Comparison.
Appendix B
Table A2.
Risk of bias of the reviewed studies.
| Source | Selection Bias | Performance Bias | Attrition Bias | Other Bias |
|---|---|---|---|---|
| Hertzberg et al., 2013 [78] | Low | High | Low |
|
| Vilardaga et al., 2016 [25] | High | NA | Low |
|
| Hicks et al., 2017 [29] | Low | High | Low |
|
| Minami et al., 2018 [67] | High | High | Low |
|
| Heffner et al., 2019 [45] | High | High | Low |
|
| Herbst et al., 2019 [47] | High | NA | Low |
|
| Klein et al., 2019 [80] | Low | High | NA | NA |
| Wilson et al., 2019 [81] | Low | NA | High |
|
| Alyssa et al., 2020 [79] | Low | High | Low |
|
| Gowarty et al., 2021 [83] | High | High | Low |
|
Appendix C
Table A3.
Details of apps identified from the reviewed studies.
| Source | App Names | Grounding Theories | Development Methods | Target Users | Smoking Cessation Features | Mental Health Features | No. of Downloads App Store Rating (n= No. of User Rated) | Cost in NZD | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | Other | ||||||||
| Vilardaga et al., 2016 [25] | QuitPal (Apple and Google) | USPHSCPG | Iterative development | Smokers | ✓ | ✓ | ✓ | ✓ | ✓ | 1. Social support 2. Contact to Quitline | NA | NA | NA | ||
| Minami, et al., 2018 [67] | NA | CM and EMA | NA | Smokers with psychiatric disorders | ✓ | Bio-verification on quitting data | 1. Mental health practice 2. Prompt to complete EMA reports | NA | NA | ||||||
| Heffner et al., 2019 [45] | Actify! (Apple) | BAT-D and BATS | User-centred design process including competitive analysis, focus groups, and usability testing of low- and high-fidelity prototypes | Smokers with depressive symptoms | ✓ | ✓ | Quitting plan | NA | Download rate unavailable User rating: Apple-1.5/5.0 (n = 4) | Free | |||||
| Hicks et al., 2017 [29] | Stay Quit Coach (SQC) (Apple and Google) | CBT and USPHSCPG | The app is part of the integrated care (IC) treatment protocol, which consists of combined behavioural and pharmacotherapy treatment | Smokers with PTSD | ✓ | ✓ | 1. Quitting plan 2. Contact to Quitline | 1. Mental health practice (reduce anxiety sensitivity and hyperarousal) 2. Help users to cope with negative emotions | Download rate: Apple-unavailable; Google-10,000+ User rating: Apple-3.5/5.0 (n = 2); Google-4.0/5.0 (n = 21) | Free | |||||
| Herbst et al., 2019 [47] | |||||||||||||||
| Wilson et al., 2019 [81] | |||||||||||||||
| Klein et al., 2019 [80] | Kick.it (Apple and Google) | IM and TDF | The development method for the Kick.it was co-design, which involved consumer involvement and collaboration in the tailoring of the app | Individuals with SMI who are seeking to quit smoking | ✓ | ✓ | NA | NA | Download rate: Apple-unavailable; Google-10,000+ User rating: Apple-3.8/5.0 (n = 9); Google-NA Renamed as “No Butts” | Free | |||||
| Hertzberg et al., 2013 [78] | mCM (Apple) | CM | - | Smokers with PTSD | 1. Bio-verification on quitting data 2. Compensation to quitting behaviours | NA | NA | NA | |||||||
| Alyssa et al., 2020 [79] | |||||||||||||||
| Gowarty et al., 2021 [83] | QuitGuide | BCTs and CPGs | Mixed usability reviews | Young adults with SMI who were current smokers | ✓ | ✓ | ✓ | NA | NA | Download rate: Apple-unavailable; Google-50,000+ User rating: Apple-4.2/5.0 (n = 17); Google-NA | Free | ||||
| quitSTART | BCTs and CPGs | Mixed usability reviews | ✓ | ✓ | ✓ | NA | NA | Download rate: Apple-unavailable; Google-50,000+ User rating: Apple-4.5/5.0 (n = 1500); Google-3.4/5.0 (n = 276) | Free | ||||||
USPHCPG—US Public Health Service’s Clinical Practice Guideline for Treating Tobacco Use and Dependence; EMA—Ecological momentary assessment; CM—Contingency management; BAT-D—Behavioural Activation Treatment for Depression; BATS—Behavioural Activation Treatment for Smoking; CBT—Cognitive Behaviour Therapy; IM—Intervention Mapping; TDF—Theoretical Domains Framework; PTSD—Posttraumatic Stress Disorder; BCTs—Behaviour Change Theories; CPGs—Clinical Practice Guidelines; 1—Calculator; 2—Calendar; 3—Gamification; 4—Hypnosis; 5—Information; 6—Lung Health Tester; 7—Rationing.
Appendix D
Table A4.
Details of apps found from the Apple and Google App Stores.
| App Names | Developer Grounding Theories Development Methods | Target Users Category | Smoking Cessation Features | Mental Health Features | No. of Downloads App Store Rating (n= No. of User Rated) | Cost in NZD $ | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | Other | ||||||
| Apple App Store—“Mental health smoking”. | |||||||||||||
| LIFEGIFT HERE4U | LifeGift Pte. Ltd. NA NA | Smokers Health and fitness | ✓ | Download rate: NA User Rating: NA | $1.69 (in-app purchase) | ||||||||
| Construction Industry Helpline | Construction Industry Solutions Limited NA NA | Construction worker with any of the four areas of need: mental, physical, financial and social health Lifestyle | ✓ | 1. An assessment tool to evaluate conditions 2. Self-help tools to cope with conditions | Download rate: NA User Rating: NA | NA | |||||||
| Smoke Free—Stop Smoking Now | Smoke Free, Inc. UK Transtheoretical model of behaviour change NA | People who are trying to quit smoking Health and fitness | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | Quit Planning Community Chat | 1. Mood tracker | Download rate: NA User Rating: 4.7/5.0 (n = 1700) | $1.99 per week or $5.99 per month (in-app purchase) |
| Apple App Store—“Mental health”. | |||||||||||||
| Daylio Journal | Relaxio s.r.o. NA Principles: help users being mindful, identify the influence of new hobby, easy-to-use | Everyone Lifestyle | 1. Calendar 2. Diary 3. Mood tracking 4. Prompt goals setting (include mood and health behaviours) | NA 4.7 out of 5.0 (n = 452) | $4.99 to $39.99 (in-app purchase, depending on the package) | ||||||||
| Morning!—A 5 Minute Journal | Adriana Padilla NA NA | Everyone Lifestyle | 1. Calendar 2. Daily quotes 3. Diary 4. Mood tracking 5. Reminders | NA 4.9 out of 5.0 (n = 12) | $9.99 (in-app purchase) | ||||||||
| Wysa: Mental Health Support | Touchkin CBT, DBT, Yoga and meditation NA | Everyone Health and Fitness | 1. Chatbot communication supports 2. Contact to therapists 3. Self-help tools to cope with conditions | NA 4.7 out of 5.0 (n = 34) | $8.49 to $119.99 (in-app purchase, depending on package) | ||||||||
| MindDoc: Depression & Anxiety | MindDoc Health GmbH NA Developed with psychotherapists and scientists | Everyone Medical | 1. Information 2. Mental health practice (course) 3. Mood tracking | NA 4.7 out of 5.0 (n = 281) | $7.49 to $76.99 (in-app purchase, depending on the package) | ||||||||
| Stoic. Mental health journal | Maciej Lobodzinski Stoicism NA | Everyone Health and Fitness | 1. Calendar 2. Diary 3. Daily quotes | NA 4.7 out of 5.0 (n = 93) | $10.99 to $159.99 (in-app purchase, depending on the package) | ||||||||
| Apple App Store—“Quit smoking”. | |||||||||||||
| Quit smoking | Dennis Ebbinghaus NA NA | Smokers Health and Fitness | ✓ | ✓ | ✓ | ✓ | 1. Craving supports 2. Goal setting | NA 4.5 out of 5.0 (n = 28) | $1.99 to $46.99 (in-app purchase, depending on the package) | ||||
| Smoke-Free—Stop Smoking Now | David Crane 30+ proven quit smoking techniques and the most reliable quitting methods science NA | Smokers Health and Fitness | ✓ | ✓ | ✓ | ✓ | Goal setting | NA 4.7 out of 5.0 (n = 1125) | $1.69 to $49.99 (in-app purchase, depend on package) | ||||
| My QuitBuddy | Australian National Preventive Health Agency NA NA | Smokers Health and Fitness | ✓ | ✓ | Social support | NA 5.0 out of 5.0 (n = 22) | NA | ||||||
| Quit Genius—quit smoking | Digital Therapeutics Ltd. CBT NA | Smokers Health and Fitness | ✓ | 1. Reminders 2. Quitting exercise | NA 4.5 out of 5.0 (n = 3100) | $10.99 to $149.99 (in-app purchase, depend on package) | |||||||
| Kwit—Quit smoking and vaping | KWIT CBT NA | Smokers Health and Fitness | ✓ | ✓ | ✓ | Motivational messages | NA 4.6 out of 5.0 (n = 5) | $2.49 to $89.99 (in-app purchase, depend on package) | |||||
| Google App Store—“Mental Health Smoking” | |||||||||||||
| Quit Tracker: Stop Smoking | despDev NA NA | Smokers Health and Fitness | ✓ | ✓ | ✓ | 1,000,000+ 4.7 out of 5.0 (n = 100,413) | $3.99 (in app purchase) | ||||||
| Smoke Free, stop smoking now and quit for good | David Crane 30+ proven quit smoking techniques and the most reliable quitting methods science NA | Smokers Health and Fitness | ✓ | ✓ | ✓ | ✓ | Goal setting | 1,000,000+ 4.8 out of 5.0 (n = 52,631) | $1.69 to $47.99 (in-app purchase, depend on package) | ||||
| Guided Mental Health Journal—Iona Mind | Iona Mind—Mental Health Support CBT and performance psychology NA | Everyone Health and Fitness | 1. Diary 2. Information (CBT) 3. Mood tracking 4. Mental health practice 5. Goal setting | 1000+ 4.8 out of 5.0 (n = 94) | $7.99 to $89.99 (in-app purchase, depending on the package) | ||||||||
| Stop Smoking—EasyQuit free | Mario Herzberg (Hanna) NA NA | Smoker Health and Fitness | ✓ | ✓ | ✓ | ✓ | Quitting plan | 1,000,000+ 4.8 out of 5.0 (n = 78,056) | $7.99 to $89.99 (in-app purchase, depend on package) | ||||
| Wysa: stress, depression & anxiety therapy chatbot | Touchkin CBT, DBT, Yoga and meditation NA | Everyone Health and Fitness | 1. Chatbot communication supports 2. Contact to therapists 3. Self-help tools to cope with conditions | 1,000,000+ 4.8 out of 5.0 (n = 72,643) | $2.49 to $239.99 (in-app purchase, depend on package) | ||||||||
| Google App Store—“Mental health”. | |||||||||||||
| Guided Mental Health Journal—Iona Mind | |||||||||||||
| Wysa: stress, depression & anxiety therapy chatbot | |||||||||||||
| Mind journal: anxiety relief & mental health diary | Bazimo CBT NA | Everyone Health and Fitness | 1. Diary 2. Mood tracking 3. Mental health practice | 100,000+ 4.8 out of 5.0 (n = 4873) | $12.99 to $32.99 (in-app purchase, depend on package) | ||||||||
| What’s Up?—A Mental Health App | Jackson Tempra CBT and ACT NA | Everyone Health and Fitness | 1. Behaviour tracking (habit) 2. Diary 3. Gamification 4. Mental health practice 5. Mood tracking 6. Daily quotes | 500,000+ 4.8 out of 5.0 (n = 3354) | $1.34 to $5.62 (in-app purchase, depend on package) | ||||||||
| MindDoc: Depression & Anxiety | MindDoc Health GmbH NA Developed with psychotherapists and scientists | Everyone Medical | 1. Information 2. Mental health practice (course) 3. Mood tracking | 1,000,000+ 4.5 out of 5.0 (n = 35,355) | $8.49 to $129.99 (in-app purchase, depend on package) | ||||||||
| Google App Store—“Quit smoking” | |||||||||||||
| Quit Tracker: Stop Smoking | ✓ | ✓ | ✓ | ||||||||||
| Smoke Free, stop smoking now and quit for good | ✓ | ✓ | ✓ | ✓ | Goal setting | ||||||||
| Stop Smoking—EasyQuit free | ✓ | ✓ | ✓ | ✓ | Quitting plan | ||||||||
| Flamy—quit smoking & become a non-smoker | Offlinefirst NA NA | Smoker Health and Fitness | ✓ | ✓ | 1. Social support 2. Craving supports | 500,000+ 4.8 out of 5.0 (n = 10,815) | $0.99 to $13.99 (in-app purchase, depend on package) | ||||||
| QuitNow! | Fewlaps NA NA | Smoker Medical | ✓ | ✓ | Quitting plan | Mental health practice | 1,000,000+ 4.6 out of 5.0 (n = 52,860) | $6.99 (in-app purchase) | |||||
CBT—Cognitive Behaviour Therapy; DBT—Dialectical Behaviour Therapy; 1—Calculator; 2—Calendar; 3—Gamification; 4—Hypnosis; 5—Information; 6—Lung Health Tester; 7—Rationing.
References
- World Health Organization. WHO Report on the Global Tobacco Epidemic 2019: Offer Help to Quit Tobacco Use; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Shiffman, S.; Brockwell, S.E.; Pillitteri, J.L.; Gitchell, J.G. Use of Smoking-Cessation Treatments in the United States. Am. J. Prev. Med. 2008, 34, 102–111. [Google Scholar] [CrossRef]
- Zhang, M.; Wang, L.-M.; Li, Y.-C.; Li, X.-Y.; Jiang, Y.; Hu, N.; Xiao, L.; Li, Q.; Yang, Y.; Yang, G.-H. Cross-sectional survey on smoking and smoking cessation behaviors among Chinese adults in 2010. Zhonghua Yu Fang Yi Xue Za Zhi 2012, 46, 404–408. [Google Scholar] [PubMed]
- Khan, N.; Anderson, J.R.; Du, J.; Tinker, D.; Bachyrycz, A.M.; Namdar, R. Smoking Cessation and Its Predictors: Results from a Community-Based Pharmacy Tobacco Cessation Program in New Mexico. Ann. Pharmacother. 2012, 46, 1198–1204. [Google Scholar] [CrossRef]
- Chen, J.; Ho, E.; Jiang, Y.; Whittaker, R.; Yang, T.; Bullen, C. Mobile Social Network–Based Smoking Cessation Intervention for Chinese Male Smokers: Pilot Randomized Controlled Trial. JMIR mHealth uHealth 2020, 8, e17522. [Google Scholar] [CrossRef]
- World Health Organization. Mobile Health for Tobacco Cessation (mTobaccoCessation). 2015. Available online: https://www.who.int/publications/i/item/978924154981-3 (accessed on 1 May 2023).
- Cafarella, P.A.; Effing, T.W.; Usmani, Z.-A.; Frith, P.A. Treatments for anxiety and depression in patients with chronic obstructive pulmonary disease: A literature review. Respirology 2012, 17, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.R.; Patel, A.R.; Singh, S.; Singh, S.; Khawaja, I. Global Initiative for Chronic Obstructive Lung Disease: The Changes Made. Cureus 2019, 11, e4985. [Google Scholar] [CrossRef]
- Cantor, L.; Jacobson, R. COPD: How to manage comorbid depression and anxiety. J. Fam. Pract. 2003, 2, 11. [Google Scholar]
- National Health Service. Stopping Smoking is Good for Your Mental Health. 2018. Available online: https://www.nhs.uk/live-well/quit-smoking/stopping-smoking-mental-health-benefits/ (accessed on 1 May 2023).
- Yohannes, A.M.; Alexopoulos, G.S. Depression and anxiety in patients with COPD. Eur. Respir. Rev. 2014, 23, 345–349. [Google Scholar] [CrossRef]
- Tselebis, A.; Pachi, A.; Ilias, I.; Kosmas, E.; Bratis, D.; Moussas, G.; Tzanakis, N. Strategies to improve anxiety and depression in patients with COPD: A mental health perspective. Neuropsychiatr. Dis. Treat. 2016, 12, 297–328. [Google Scholar] [CrossRef]
- Whittaker, R.; McRobbie, H.; Bullen, C.; Rodgers, A.; Gu, Y.; Dobson, R. Mobile phone text messaging and app-based interventions for smoking cessation. Cochrane Database Syst. Rev. 2019, 2019, CD006611. [Google Scholar]
- Keoleian, V.; Polcin, D.; Galloway, G.P. Text Messaging for Addiction: A Review. J. Psychoact. Drugs 2015, 47, 158–176. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.K.; Cole-Lewis, H.; Bernhardt, J.M. Mobile Text Messaging for Health: A Systematic Review of Reviews. Annu. Rev. Public Health 2015, 36, 393–415. [Google Scholar] [CrossRef]
- Jamison, J.; Naughton, F.; Gilbert, H.; Sutton, S. Delivering Smoking Cessation Support by Mobile Phone Text Message: What Information do Smokers Want? A Focus Group Study. J. Appl. Biobehav. Res. 2013, 18, 1–23. [Google Scholar] [CrossRef]
- Schwartz, R.P.; Gryczynski, J.; Mitchell, S.G.; Gonzales, A.; Moseley, A.; Peterson, T.R.; Ondersma, S.J.; O’Grady, K.E. Computerized versus in-person brief intervention for drug misuse: A randomized clinical trial. Addiction 2014, 109, 1091–1098. [Google Scholar] [CrossRef]
- BinDhim, N.F.; McGeechan, K.; Trevena, L. Assessing the effect of an interactive decision-aid smartphone smoking cessation application (app) on quit rates: A double-blind automated randomised control trial protocol. BMJ Open 2014, 4, e005371. [Google Scholar] [CrossRef] [PubMed]
- Bricker, J.B.; Mull, K.E.; Kientz, J.A.; Vilardaga, R.; Mercer, L.D.; Akioka, K.J.; Heffner, J.L. Randomized, controlled pilot trial of a smartphone app for smoking cessation using acceptance and commitment therapy. Drug Alcohol Depend. 2014, 143, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Buller, D.B.; Borland, R.; Bettinghaus, E.P.; Shane, J.H.; Zimmerman, D.E.; Comello, M.L.G.; Porter, J.H.; Wang, J.; Wang, Y.; Wei, C.; et al. Randomized Trial of a Smartphone Mobile Application Compared to Text Messaging to Support Smoking Cessation. Telemed. e-Health 2014, 20, 206–214. [Google Scholar] [CrossRef]
- Ploderer, B.; Smith, W.; Pearce, J.; Borland, R. A Mobile App Offering Distractions and Tips to Cope with Cigarette Craving: A Qualitative Study. JMIR mHealth uHealth 2014, 2, e23. [Google Scholar] [CrossRef]
- Ubhi, H.K.; Michie, S.; Kotz, D.; Wong, W.C.; West, R. A Mobile App to Aid Smoking Cessation: Preliminary Evaluation of SmokeFree28. J. Med. Internet Res. 2015, 17, e17. [Google Scholar] [CrossRef]
- McClure, J.B.; Anderson, M.L.; Bradley, K.; An, L.C.; Catz, S.L. Evaluating an Adaptive and Interactive mHealth Smoking Cessation and Medication Adherence Program: A Randomized Pilot Feasibility Study. JMIR mHealth uHealth 2016, 4, e94. [Google Scholar] [CrossRef]
- Naughton, F.; Hopewell, S.; Lathia, N.; Schalbroeck, R.; Brown, C.; Mascolo, C.; McEwen, A.; Sutton, S. A Context-Sensing Mobile Phone App (Q Sense) for Smoking Cessation: A Mixed-Methods Study. JMIR mHealth uHealth 2016, 4, e106. [Google Scholar] [CrossRef]
- Vilardaga, R.; Rizo, J.; Kientz, J.A.; McDonell, M.G.; Ries, R.K.; Sobel, K. User Experience Evaluation of a Smoking Cessation App in People with Serious Mental Illness. Nicotine Tob. Res. 2016, 18, 1032–1038. [Google Scholar] [CrossRef]
- Bricker, J.B.; Copeland, W.; Mull, K.E.; Zeng, E.Y.; Watson, N.L.; Akioka, K.J.; Heffner, J.L. Single-arm trial of the second version of an acceptance & commitment therapy smartphone application for smoking cessation. Drug Alcohol Depend. 2017, 170, 37–42. [Google Scholar]
- Gordon, J.S.; Armin, J.S.; Cunningham, J.K.; Muramoto, M.L.; Christiansen, S.M.; Jacobs, T.A. Lessons learned in the development and evaluation of RxCoach™, an mHealth app to increase tobacco cessation medication adherence. Patient Educ. Couns. 2017, 100, 720–727. [Google Scholar] [CrossRef]
- Hassandra, M.; Lintunen, T.; Hagger, M.S.; Heikkinen, R.; Vanhala, M.; Kettunen, T. An mHealth App for Supporting Quitters to Manage Cigarette Cravings with Short Bouts of Physical Activity: A Randomized Pilot Feasibility and Acceptability Study. JMIR mHealth uHealth 2017, 5, e74. [Google Scholar] [CrossRef]
- Hicks, T.A.; Thomas, S.P.; Wilson, S.M.; Calhoun, P.S.; Kuhn, E.R.; Beckham, J.C. A Preliminary Investigation of a Relapse Prevention Mobile Application to Maintain Smoking Abstinence Among Individuals with Posttraumatic Stress Disorder. J. Dual Diagn. 2016, 13, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Iacoviello, B.M.; Steinerman, J.R.; Klein, D.B.; Silver, T.L.; Berger, A.G.; Luo, S.X.; Schork, N.J. Clickotine, A Personalized Smartphone App for Smoking Cessation: Initial Evaluation. JMIR mHealth uHealth 2017, 5, e56. [Google Scholar] [CrossRef]
- Pechmann, C.; Delucchi, K.; Lakon, C.M.; Prochaska, J.J. Randomised controlled trial evaluation of Tweet2Quit: A social network quit-smoking intervention. Tob. Control 2017, 26, 188–194. [Google Scholar] [CrossRef]
- Regmi, K.; Kassim, N.; Ahmad, N.H.; Tuah, N.A. Assessment of content, quality and compliance of the STaR mobile application for smoking cessation. Tob. Prev. Cessat. 2017, 3, 120. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Starkey, N.J.; Sargisson, R.J. Using SmartQuit®, an Acceptance and Commitment Therapy Smartphone application, to reduce smoking intake. Digit. Health 2017, 3, 2055207617729535. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Tombor, I.; Shahab, L.; West, R. Usability testing of a smoking cessation smartphone application (‘SmokeFree Baby’): A think-aloud study with pregnant smokers. Digit. Health 2017, 3, 2055207617704273. [Google Scholar] [CrossRef] [PubMed]
- BinDhim, N.F.; McGeechan, K.; Trevena, L. Smartphone Smoking Cessation Application (SSC App) trial: A multicountry double-blind automated randomised controlled trial of a smoking cessation decision-aid ‘app’. BMJ Open 2018, 8, e017105. [Google Scholar] [CrossRef] [PubMed]
- Crane, D.; Ubhi, H.K.; Brown, J.; West, R. Relative effectiveness of a full versus reduced version of the ‘Smoke Free’ mobile application for smoking cessation: An exploratory randomised controlled trial. F1000Research 2019, 7, 1524. [Google Scholar] [CrossRef] [PubMed]
- Dar, R. Effect of Real-Time Monitoring and Notification of Smoking Episodes on Smoking Reduction: A Pilot Study of a Novel Smoking Cessation App. Nicotine Tob. Res. 2018, 20, 1515–1518. [Google Scholar] [CrossRef] [PubMed]
- Garrison, K.A.; Pal, P.; O’malley, S.S.; Pittman, B.P.; Gueorguieva, R.; Rojiani, R.; Scheinost, D.; Dallery, J.; Brewer, J.A. Craving to Quit: A Randomized Controlled Trial of Smartphone App–Based Mindfulness Training for Smoking Cessation. Nicotine Tob. Res. 2018, 22, 324–331. [Google Scholar] [CrossRef] [PubMed]
- McClure, E.A.; Tomko, R.L.; Carpenter, M.J.; Treiber, F.A.; Gray, K.M. Acceptability and compliance with a remote monitoring system to track smoking and abstinence among young smokers. Am. J. Drug Alcohol Abus. 2018, 44, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Patrick, H.; Fujii, C.A.; Glaser, D.B.; Utley, D.S.; Marler, J.D. A Comprehensive Digital Program for Smoking Cessation: Assessing Feasibility in a Single-Group Cohort Study. JMIR mHealth uHealth 2018, 6, e11708. [Google Scholar] [CrossRef]
- Schick, R.S.; Kelsey, T.W.; Marston, J.; Samson, K.; Humphris, G.W. MapMySmoke: Feasibility of a new quit cigarette smoking mobile phone application using integrated geo-positioning technology, and motivational messaging within a primary care setting. Pilot Feasibility Stud. 2018, 4, 19. [Google Scholar] [CrossRef]
- Shuter, J.; Kim, R.S.; An, L.C.; Abroms, L.C. Feasibility of a Smartphone-Based Tobacco Treatment for HIV-Infected Smokers. Nicotine Tob. Res. 2018, 22, 398–407. [Google Scholar] [CrossRef]
- Tan, N.C.; Mohtar, Z.B.M.; Koh, E.Y.L.; Sankari, U.; Tay, D.H.C.; Yu, S.; Tan, W.B.W. An exhaled carbon monoxide self-monitoring device linked to social media to support smoking cessation: A proof of concept pilot study. Proc. Singap. Healthc. 2018, 27, 187–192. [Google Scholar] [CrossRef]
- Tudor-Sfetea, C.; Rabee, R.; Najim, M.; Amin, N.; Chadha, M.; Jain, M.; Karia, K.; Kothari, V.; Patel, T.; Suseeharan, M.; et al. Evaluation of Two Mobile Health Apps in the Context of Smoking Cessation: Qualitative Study of Cognitive Behavioral Therapy (CBT) Versus Non-CBT-Based Digital Solutions. JMIR mHealth uHealth 2018, 6, e98. [Google Scholar] [CrossRef]
- Heffner, J.L.; Watson, N.L.; Serfozo, E.; Mull, K.E.; MacPherson, L.; Gasser, M.; Bricker, J.B. A Behavioral Activation Mobile Health App for Smokers with Depression: Development and Pilot Evaluation in a Single-Arm Trial. JMIR Form. Res. 2019, 3, e13728. [Google Scholar] [CrossRef]
- Herbec, A.; Brown, J.; Shahab, L.; West, R.; Raupach, T. Pragmatic randomised trial of a smartphone app (NRT2Quit) to improve effectiveness of nicotine replacement therapy in a quit attempt by improving medication adherence: Results of a prematurely terminated study. Trials 2019, 20, 547. [Google Scholar] [CrossRef] [PubMed]
- Herbst, E.; McCaslin, S.E.; Daryani, S.H.; Laird, K.T.; Hopkins, L.B.; Pennington, D.; Kuhn, E. A Qualitative Examination of Stay Quit Coach, A Mobile Application for Veteran Smokers with Posttraumatic Stress Disorder. Nicotine Tob. Res. 2019, 22, 560–569. [Google Scholar] [CrossRef]
- Hoeppner, B.B.; Hoeppner, S.S.; Carlon, H.A.; Perez, G.K.; Helmuth, E.; Kahler, C.W.; Kelly, J.F. Leveraging Positive Psychology to Support Smoking Cessation in Nondaily Smokers Using a Smartphone App: Feasibility and Acceptability Study. JMIR mHealth uHealth 2019, 7, e13436. [Google Scholar] [CrossRef] [PubMed]
- Krebs, P.; Burkhalter, J.; Fiske, J.; Snow, H.; Schofield, E.; Iocolano, M.; Borderud, S.; Ostroff, J.S. The QuitIT Coping Skills Game for Promoting Tobacco Cessation Among Smokers Diagnosed with Cancer: Pilot Randomized Controlled Trial. JMIR mHealth uHealth 2019, 7, e10071. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, N.; Elf, J.L.; Chon, S.; Golub, J.E. COach2Quit: A Pilot Randomized Controlled Trial of a Personal Carbon Monoxide Monitor for Smoking Cessation. Nicotine Tob. Res. 2019, 21, 1573–1577. [Google Scholar] [CrossRef] [PubMed]
- Luna-Perejon, F.; Malwade, S.; Styliadis, C.; Civit, J.; Cascado-Caballero, D.; Konstantinidis, E.; Abdul, S.S.; Bamidis, P.D.; Civit, A.; Li, Y.-C. Evaluation of user satisfaction and usability of a mobile app for smoking cessation. Comput. Methods Programs Biomed. 2019, 182, 105042. [Google Scholar]
- Marler, J.D.; Fujii, C.A.; Utley, D.S.; Tesfamariam, L.J.; Galanko, J.A.; Patrick, H. Initial Assessment of a Comprehensive Digital Smoking Cessation Program That Incorporates a Mobile App, Breath Sensor, and Coaching: Cohort Study. JMIR mHealth uHealth 2019, 7, e12609. [Google Scholar] [CrossRef]
- Masaki, K.; Tateno, H.; Kameyama, N.; Morino, E.; Watanabe, R.; Sekine, K.; Ono, T.; Satake, K.; Suzuki, S.; Nomura, A.; et al. Impact of a Novel Smartphone App (CureApp Smoking Cessation) on Nicotine Dependence: Prospective Single-Arm Interventional Pilot Study. JMIR mHealth uHealth 2019, 7, e12694. [Google Scholar] [CrossRef]
- O’connor, M.; Whelan, R.; Bricker, J.; McHugh, L. Randomized Controlled Trial of a Smartphone Application as an Adjunct to Acceptance and Commitment Therapy for Smoking Cessation. Behav. Ther. 2019, 51, 162–177. [Google Scholar] [CrossRef]
- Pbert, L.; Druker, S.; Crawford, S.; Frisard, C.; Trivedi, M.; Osganian, S.K.; Brewer, J. Feasibility of a Smartphone App with Mindfulness Training for Adolescent Smoking Cessation: Craving to Quit (C2Q)-Teen. Mindfulness 2019, 11, 720–733. [Google Scholar] [CrossRef]
- Peiris, D.; Wright, L.; News, M.; Rogers, K.; Redfern, J.; Chow, C.; Thomas, D. A Smartphone App to Assist Smoking Cessation Among Aboriginal Australians: Findings from a Pilot Randomized Controlled Trial. JMIR mHealth uHealth 2019, 7, e12745. [Google Scholar] [CrossRef] [PubMed]
- Schlam, T.R.; Baker, T.B. Playing Around with Quitting Smoking: A Randomized Pilot Trial of Mobile Games as a Craving Response Strategy. Games Health J. 2020, 9, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Sridharan, V.; Shoda, Y.; Heffner, J.; Bricker, J. A Pilot Randomized Controlled Trial of a Web-Based Growth Mindset Intervention to Enhance the Effec-tiveness of a Smartphone App for Smoking Cessation. JMIR mHealth uHealth 2019, 7, e14602. [Google Scholar] [CrossRef]
- Tombor, I.; Beard, E.; Brown, J.; Shahab, L.; Michie, S.; West, R. Randomized factorial experiment of components of the SmokeFree Baby smartphone application to aid smoking cessation in pregnancy. Transl. Behav. Med. 2018, 9, 583–593. [Google Scholar] [CrossRef]
- Bricker, J.B.; Watson, N.L.; Heffner, J.L.; Sullivan, B.; Mull, K.; Kwon, D.; Westmaas, J.L.; Ostroff, J. A Smartphone App Designed to Help Cancer Patients Stop Smoking: Results from a Pilot Randomized Trial on Feasibility, Acceptability, and Effectiveness. JMIR Form. Res. 2020, 4, e16652. [Google Scholar] [CrossRef]
- Bricker, J.B.; Watson, N.L.; Mull, K.E.; Sullivan, B.M.; Heffner, J.L. Efficacy of Smartphone Applications for Smoking Cessation: A Randomized Clinical Trial. JAMA Intern Med. 2020, 180, 1472–1480. [Google Scholar] [CrossRef]
- Goldenhersch, E.; Thrul, J.; Ungaretti, J.; Rosencovich, N.; Waitman, C.; Ceberio, M.R. Virtual Reality Smartphone-Based Intervention for Smoking Cessation: Pilot Randomized Controlled Trial on Initial Clinical Efficacy and Adherence. J. Med. Internet Res. 2020, 22, e17571. [Google Scholar] [CrossRef] [PubMed]
- Hébert, E.T.; Ra, C.K.; Alexander, A.C.; Helt, A.; Moisiuc, R.; Kendzor, D.E.; Vidrine, D.J.; Funk-Lawler, R.K.; Businelle, M.S. A Mobile Just-in-Time Adaptive Intervention for Smoking Cessation: Pilot Randomized Controlled Trial. J. Med. Internet Res. 2020, 22, e16907. [Google Scholar] [CrossRef]
- Masaki, K.; Tateno, H.; Nomura, A.; Muto, T.; Suzuki, S.; Satake, K.; Hida, E.; Fukunaga, K. A randomized controlled trial of a smoking cessation smartphone application with a carbon monoxide checker. npj Digit. Med. 2020, 3, 35. [Google Scholar] [CrossRef]
- Pallejà-Millán, M.; Rey-Reñones, C.; Uriarte, M.L.B.; Granado-Font, E.; Basora, J.; Flores-Mateo, G.; Duch, J. Evaluation of the Tobbstop Mobile App for Smoking Cessation: Cluster Randomized Controlled Clinical Trial. JMIR mHealth uHealth 2020, 8, e15951. [Google Scholar] [CrossRef] [PubMed]
- Webb, J.; Peerbux, S.; Smittenaar, P.; Siddiqui, S.; Sherwani, Y.; Ahmed, M.; MacRae, H.; Puri, H.; Bhalla, S.; Majeed, A. Preliminary Outcomes of a Digital Therapeutic Intervention for Smoking Cessation in Adult Smokers: Randomized Controlled Trial. JMIR Ment. Health 2020, 7, e22833. [Google Scholar] [CrossRef] [PubMed]
- Minami, H.; Brinkman, H.R.; Nahvi, S.; Arnsten, J.H.; Rivera-Mindt, M.; Wetter, D.W.; Bloom, E.L.; Price, L.H.; Vieira, C.; Donnelly, R.; et al. Rationale, design and pilot feasibility results of a smartphone-assisted, mindfulness-based intervention for smokers with mood disorders: Project mSMART MIND. Contemp. Clin. Trials 2018, 66, 36–44. [Google Scholar] [CrossRef] [PubMed]
- BinDhim, N.F.; McGeechan, K.; Trevena, L. Who Uses Smoking Cessation Apps? A Feasibility Study Across Three Countries via Smartphones. JMIR mHealth uHealth 2014, 2, e4. [Google Scholar] [CrossRef]
- Chu, K.-H.; Matheny, S.J.; Escobar-Viera, C.G.; Wessel, C.; Notier, A.E.; Davis, E.M. Smartphone health apps for tobacco Cessation: A systematic review. Addict. Behav. 2021, 112, 106616. [Google Scholar] [CrossRef]
- Haskins, B.L.; Lesperance, D.; Gibbons, P.; Boudreaux, E.D. A systematic review of smartphone applications for smoking cessation. Transl. Behav. Med. 2017, 7, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Abroms, L.C.; Westmaas, J.L.; Bontemps-Jones, J.; Ramani, R.; Mellerson, J. A Content Analysis of Popular Smartphone Apps for Smoking Cessation. Am. J. Prev. Med. 2013, 45, 732–736. [Google Scholar] [CrossRef]
- Choi, J.; Noh, G.-Y.; Park, D.-J. Smoking Cessation Apps for Smartphones: Content Analysis with the Self-Determination Theory. J. Med. Internet Res. 2014, 16, e44. [Google Scholar] [CrossRef]
- Watson, A.M.; Alber, J.M.; Barnett, T.E.; Mercado, R.; Bernhardt, J.M. Content Analysis of Anti-Tobacco Videogames: Characteristics, Content, and Qualities. Games Health J. 2016, 5, 216–223. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- National Tobacco Cessation Collaborative. Quit Smoking Apps on the iPhone. 2008 2018/01. Available online: http://www.tobacco-cessation.org/news/news_dec08.htm#spotlight (accessed on 1 May 2023).
- Jakob, N. Search: Visible and Simple. 2001. Available online: https://www.nngroup.com/articles/search-visible-and-simple/ (accessed on 1 May 2023).
- Jakob, N. Scrolling and Attention. 2010. Available online: https://www.nngroup.com/articles/scrolling-and-attention/ (accessed on 1 May 2023).
- Hertzberg, J.S.; Carpenter, V.L.; Kirby, A.C.; Calhoun, P.S.; Moore, S.D.; Dennis, M.F.; Dennis, P.A.; Dedert, E.A.; Beckham, J.C. Mobile Contingency Management as an Adjunctive Smoking Cessation Treatment for Smokers with Posttraumatic Stress Disorder. Nicotine Tob. Res. 2013, 15, 1934–1938. [Google Scholar] [CrossRef] [PubMed]
- Medenblik, A.M.; Mann, A.M.; Beaver, T.A.; Dedert, E.A.; Wilson, S.M.; Calhoun, P.S.; Beckham, J.C. Treatment Outcomes of a Multi-Component Mobile Health Smoking Cessation Pilot Intervention for People with Schizophrenia. J. Dual Diagn. 2020, 16, 420–428. [Google Scholar] [CrossRef]
- Klein, P.; Lawn, S.; Tsourtos, G.; Van Agteren, J. Tailoring of a Smartphone Smoking Cessation App (Kick.it) for Serious Mental Illness Populations: Qualitative Study. JMIR Hum. Factors 2019, 6, e14023. [Google Scholar] [CrossRef]
- Wilson, S.M.; Thompson, A.C.; Currence, E.D.; Thomas, S.P.; Dedert, E.A.; Kirby, A.C.; Elbogen, E.B.; Moore, S.D.; Calhoun, P.S.; Beckham, J.C. Patient-Informed Treatment Development of Behavioral Smoking Cessation for People with Schizophrenia. Behav. Ther. 2019, 50, 395–409. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G.; Cochrane Statistical Methods Group. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019; pp. 241–284. [Google Scholar]
- Gowarty, M.A.; Longacre, M.R.; Vilardaga, R.; Kung, N.J.; Maher, A.E.; Brunette, M.F. Usability and Acceptability of Two Smartphone Apps for Smoking Cessation Among Young Adults with Serious Mental Illness: Mixed Methods Study. JMIR Ment. Health 2021, 8, e26873. [Google Scholar] [CrossRef]
- Bennett, M.E.; Toffey, K.; Dickerson, F.; Himelhoch, S.; Katsafanas, E.; Savage, C.L. A Review of Android Apps for Smoking Cessation. J. Smok. Cessat. 2014, 10, 106–115. [Google Scholar] [CrossRef]
- Heffner, J.L.; Vilardaga, R.; Mercer, L.D.; Kientz, J.A.; Bricker, J.B. Feature-level analysis of a novel smartphone application for smoking cessation. Am. J. Drug Alcohol Abus. 2015, 41, 68–73. [Google Scholar] [CrossRef]
- Ubhi, H.K.; Kotz, D.; Michie, S.; van Schayck, O.C.; Sheard, D.; Selladurai, A.; West, R. Comparative analysis of smoking cessation smartphone applications available in 2012 versus 2014. Addict. Behav. 2016, 58, 175–181. [Google Scholar] [CrossRef]
- Ubhi, H.K.; Michie, S.; Kotz, D.; van Schayck, O.C.P.; Selladurai, A.; West, R. Characterising smoking cessation smartphone applications in terms of behaviour change techniques, engagement and ease-of-use features. Transl. Behav. Med. 2016, 6, 410–417. [Google Scholar] [CrossRef]
- Cheng, F.; Xu, J.; Su, C.; Fu, X.; Bricker, J. Content Analysis of Smartphone Apps for Smoking Cessation in China: Empirical Study. JMIR mHealth uHealth 2017, 5, e93. [Google Scholar] [CrossRef] [PubMed]
- Ferron, J.C.; Brunette, M.F.; Geiger, P.; Marsch, L.A.; Adachi-Mejia, A.M.; Bartels, S.J. Mobile Phone Apps for Smoking Cessation: Quality and Usability Among Smokers with Psychosis. JMIR Hum. Factors 2017, 4, e7. [Google Scholar] [CrossRef] [PubMed]
- Thornton, L.; Quinn, C.; Birrell, L.; Guillaumier, A.; Shaw, B.; Forbes, E.; Deady, M.; Kay-Lambkin, F. Free smoking cessation mobile apps available in Australia: A quality review and content analysis. Aust. N. Z. J. Public Health 2017, 41, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Regmi, D.; Tobutt, C.; Shaban, S. Quality and use of free smoking cessation apps for smartphones. Int. J. Technol. Assess. Health Care 2018, 34, 476–480. [Google Scholar] [CrossRef]
- Robinson, C.D.; Seaman, E.L.; Grenen, E.; Montgomery, L.; Yockey, R.A.; Coa, K.; Prutzman, Y.; Augustson, E. A content analysis of smartphone apps for adolescent smoking cessation. Transl. Behav. Med. 2018, 10, 302–309. [Google Scholar] [CrossRef]
- Conroy, D.E.; Yang, C.H.; Maher, J.P. Behavior change techniques in top-ranked mobile apps for physical activity. Am. J. Prev. Med. 2014, 46, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Cowan, L.T.; Van Wagenen, S.A.; Brown, B.A.; Hedin, R.J.; Seino-Stephan, Y.; Hall, P.C.; West, J.H. Apps of steel: Are exercise apps providing consumers with realistic expectations?: A content analysis of exercise apps for presence of behavior change theory. Health Educ. Behav. 2013, 40, 133–139. [Google Scholar] [CrossRef]
- Tencent. WeChat Mini-Programme Design Guideline; Tencent: Shenzhen, China, 2019; Available online: https://developers.weixin.qq.com/miniprogram/en/design/#Provide-Clear-Processes (accessed on 1 May 2023).
- Google Inc. Google Material User Interface Design Guideline; Google Inc.: Mountain View, CA, USA, 2021; Available online: https://developers.google.com/assistant/interactivecanvas/design (accessed on 1 May 2023).
Figure 1.
Flow Diagram of Study Selection.

Table 1.
Search terms used.
| Fields | Terms |
|---|---|
| Smoking | Smoking OR “smoking cessation” OR “quit smoking” OR “stop smoking” OR cigarette OR “cigarette cessation” OR tobacco OR “tobacco cessation”. |
| Smartphone | Smartphone OR “mobile phone” OR phone OR iPhone OR iOS OR Android OR “smartphone” OR “cell phone”. |
| App | App* OR application OR “mobile app*” OR “mobile software” OR “mobile program*” OR “smartphone app*” OR “smartphone software” OR “smartphone program*”. |
| Mental Health | Anxiety OR depression OR stress OR emotion* OR mental OR “mental health” OR “mental health wellbeing” OR “mental disorder*” OR “mental illness*” OR “psychiatric disorder*”. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chen, J.; Chu, J.; Marsh, S.; Shi, T.; Bullen, C. Smartphone App-Based Interventions to Support Smoking Cessation in Smokers with Mental Health Conditions: A Systematic Review. Psych 2023, 5, 1077-1100. https://doi.org/10.3390/psych5040072
AMA Style
Chen J, Chu J, Marsh S, Shi T, Bullen C. Smartphone App-Based Interventions to Support Smoking Cessation in Smokers with Mental Health Conditions: A Systematic Review. Psych. 2023; 5(4):1077-1100. https://doi.org/10.3390/psych5040072
Chicago/Turabian StyleChen, Jinsong, Joanna Chu, Samantha Marsh, Tianyi Shi, and Chris Bullen. 2023. "Smartphone App-Based Interventions to Support Smoking Cessation in Smokers with Mental Health Conditions: A Systematic Review" Psych 5, no. 4: 1077-1100. https://doi.org/10.3390/psych5040072