
Diagnosis of Osteoarthritis at an Early Stage via Infrared Spectroscopy Combined Chemometrics in Human Serum: A Pilot Study
 , and
, and
Abstract
:1. Introduction
2. Methodology
2.1. Ethical Approval
2.2. Sample Size Calculation
2.3. Participants
2.4. Serum Collection
2.5. ATR-FTIR Spectral Acquisition
2.6. Chemometrics
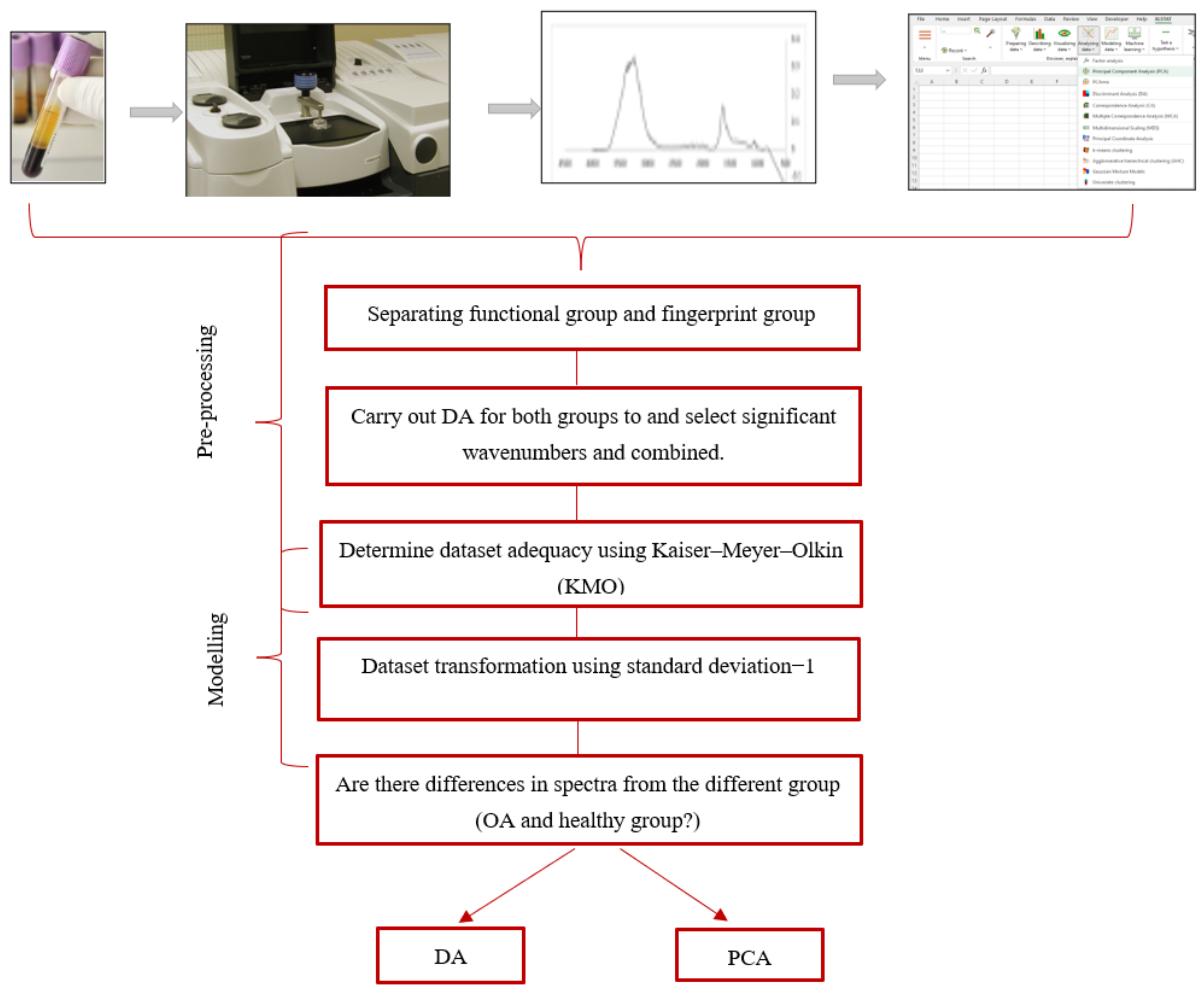
2.6.1. Data Pre-Processing
2.6.2. Kaiser-Meyer-Olkin Test
2.6.3. Dataset Transformation
2.6.4. Discriminant Analysis (DA)
2.6.5. Dataset Exploratory by PCA
3. Results and Discussion
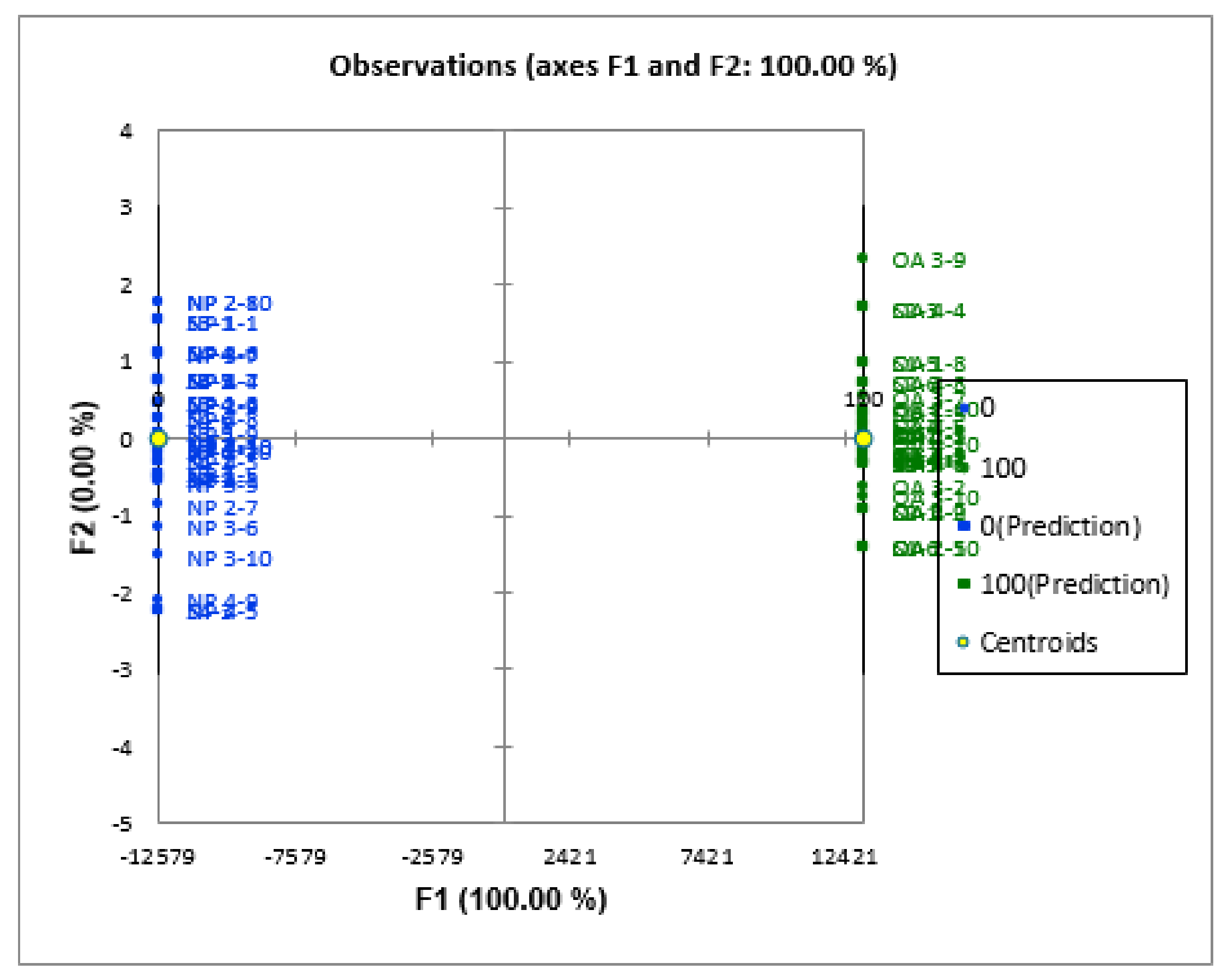
3.1. Validation and Verification of the DA Model between OA and Healthy Serum Samples
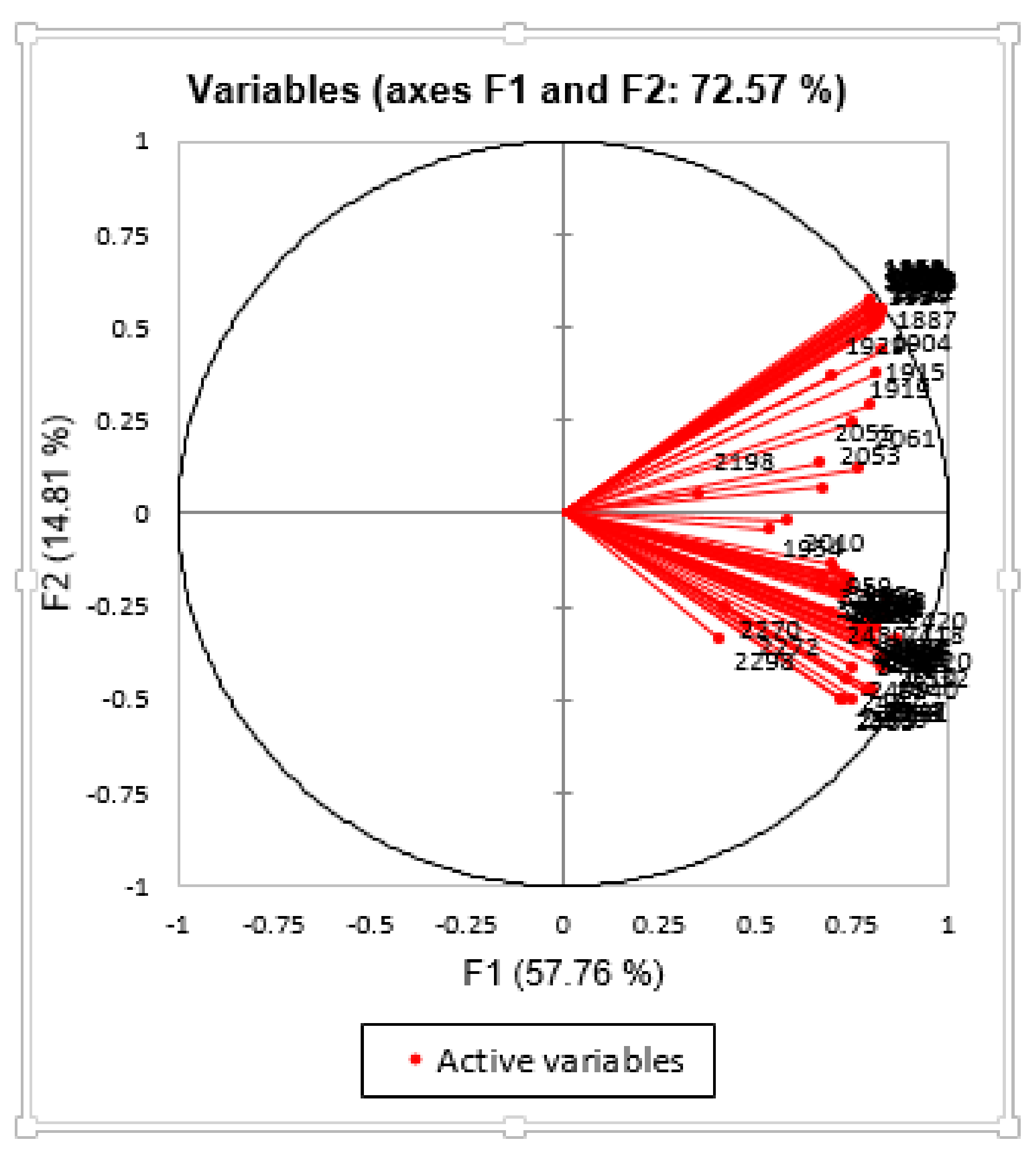
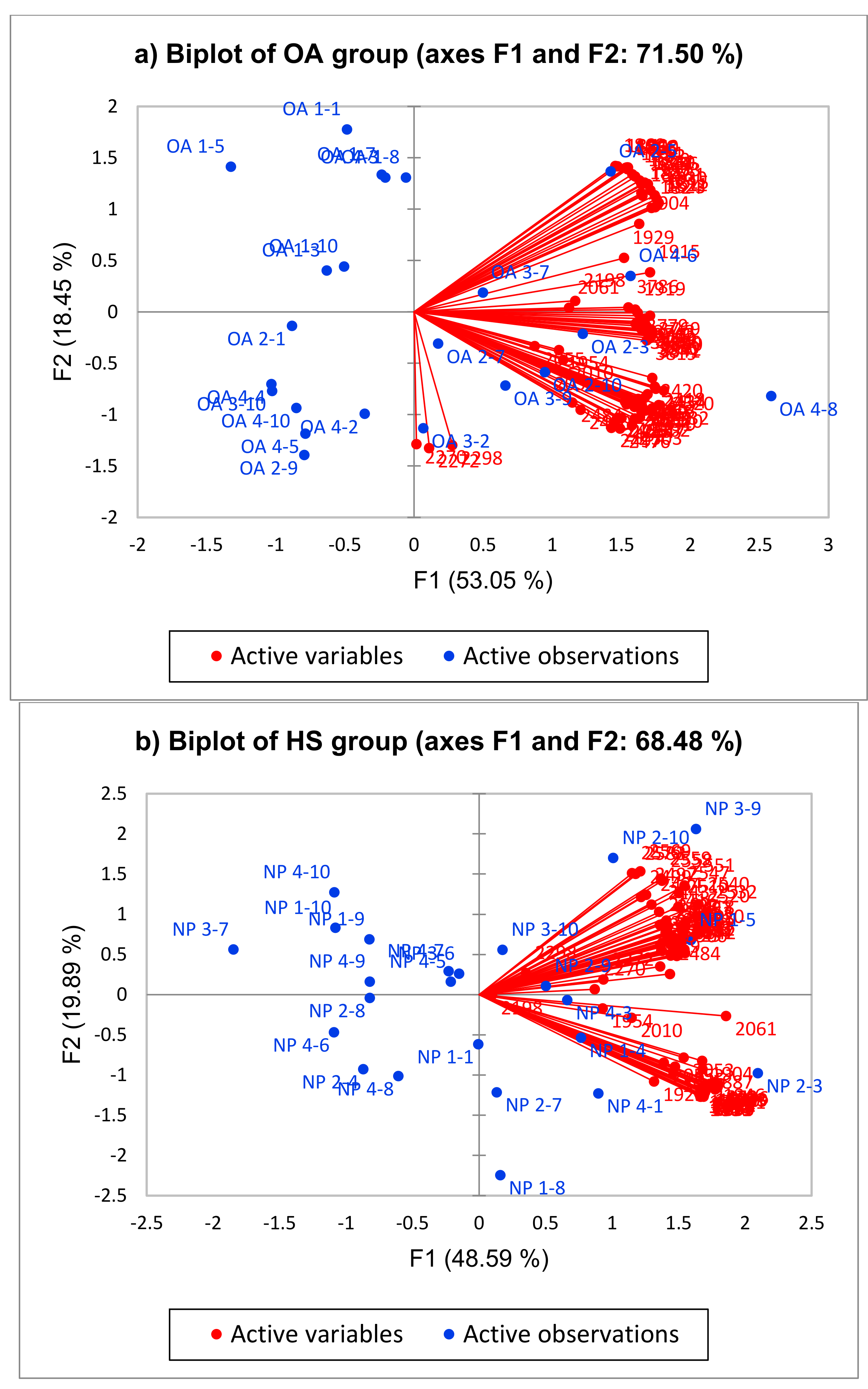
3.2. Apportionment of Wavenumber Contributing to OA in Serum
4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hsu, H.; Siwiec, R.M. Knee Osteoarthritis; StatPearls Publishing: Treasure Island, FL, USA, 2018. [Google Scholar]
- Migliorini, F.; Pintore, A.; Torsiello, E.; Oliva, F.; Spiezia, F.; Maffulli, N. Intensive Physical Activity Increases the Risk of Knee and Hip Arthroplasty: A Systematic Review. Sport. Med. Arthrosc. Rev. 2022, 30, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Hulshof, C.T.J.; Pega, F.; Neupane, S.; Colosio, C.; Daams, J.G.; Kc, P.; Kuijer, P.P.F.M.; Mandic-Rajcevic, S.; Masci, F.; van der Molen, H.F. The effect of occupational exposure to ergonomic risk factors on osteoarthritis of hip or knee and selected other musculoskeletal diseases: A systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury. Environ. Int. 2021, 150, 106349. [Google Scholar] [PubMed]
- Hunter, D.J.; March, L.; Chew, M. Osteoarthritis in 2020 and beyond: A Lancet Commission. Lancet 2020, 396, 1711–1712. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Li, Z.; Alexander, P.G.; Ocasio-Nieves, B.D.; Yocum, L.; Lin, H.; Tuan, R.S. Pathogenesis of osteoarthritis: Risk factors, regulatory pathways in chondrocytes, and experimental models. Biology 2020, 9, 194. [Google Scholar] [CrossRef]
- Rim, Y.A.; Nam, Y.; Ju, J.H. The role of chondrocyte hypertrophy and senescence in osteoarthritis initiation and progression. Int. J. Mol. Sci. 2020, 21, 2358. [Google Scholar] [CrossRef] [Green Version]
- Jiménez, G.; Cobo-Molinos, J.; Antich, C.; López-Ruiz, E. Osteoarthritis: Trauma vs disease. In Osteochondral Tissue Engineering; Springer: Berlin/Heidelberg, Germany, 2018; pp. 63–83. [Google Scholar]
- Bolduc, J.A.; Collins, J.A.; Loeser, R.F. Reactive oxygen species, aging and articular cartilage homeostasis. Free Radic. Biol. Med. 2019, 132, 73–82. [Google Scholar] [CrossRef]
- Thomas, A.C.; Hubbard-Turner, T.; Wikstrom, E.A.; Palmieri-Smith, R.M. Epidemiology of posttraumatic osteoarthritis. J. Athl. Train. 2017, 52, 491–496. [Google Scholar] [CrossRef] [Green Version]
- Brahim, A.; Jennane, R.; Riad, R.; Janvier, T.; Khedher, L.; Toumi, H.; Lespessailles, E. A decision support tool for early detection of knee OsteoArthritis using X-ray imaging and machine learning: Data from the OsteoArthritis Initiative. Comput. Med. Imaging Graph. 2019, 73, 11–18. [Google Scholar] [CrossRef]
- Hayashi, D.; Roemer, F.W.; Guermazi, A. Imaging of Osteoarthritis by Conventional Radiography, MR Imaging, PET–Computed Tomography, and PET–MR Imaging. PET Clin. 2019, 14, 17–29. [Google Scholar] [CrossRef]
- Yeğin, T.; Altan, L.; Aksoy, M.K. The effect of therapeutic ultrasound on pain and physical function in patients with knee osteoarthritis. Ultrasound Med. Biol. 2017, 43, 187–194. [Google Scholar] [CrossRef]
- Sulaiman, S.Z.S.; Tan, W.M.; Radzi, R.; Shafie, I.N.F.; Ajat, M.; Mansor, R.; Mohamed, S.; Ng, A.M.H.; Lau, S.F. Comparison of bone and articular cartilage changes in osteoarthritis: A micro-computed tomography and histological study of surgically and chemically induced osteoarthritic rabbit models. J. Orthop. Surg. Res. 2021, 16, 663. [Google Scholar] [CrossRef]
- Karpiński, R. Knee joint osteoarthritis diagnosis based on selected acoustic signal discriminants using machine learning. Appl. Comput. Sci. 2022, 18, 71–85. [Google Scholar] [CrossRef]
- Qiu, X.; Liu, Z.; Zhuang, M.; Cheng, D.; Zhu, C.; Zhang, X. Fusion of cnn1 and cnn2-based magnetic resonance image diagnosis of knee meniscus injury and a comparative analysis with computed tomography. Comput. Methods Programs Biomed. 2021, 211, 106297. [Google Scholar] [CrossRef]
- Zhang, W.; Robertson, W.B.; Zhao, J.; Chen, W.; Xu, J. Emerging trend in the pharmacotherapy of osteoarthritis. Front. Endocrinol. 2019, 10, 431. [Google Scholar] [CrossRef]
- Krakowski, P.; Nogalski, A.; Jurkiewicz, A.; Karpiński, R.; Maciejewski, R.; Jonak, J. Comparison of diagnostic accuracy of physical examination and MRI in the most common knee injuries. Appl. Sci. 2019, 9, 4102. [Google Scholar] [CrossRef] [Green Version]
- Chong, T.; Don, D.W.; Kao, M.C.; Wong, D.; Mitra, R. The value of physical examination in the diagnosis of hip osteoarthritis. J. Back Musculoskelet. Rehabil. 2013, 26, 397–400. [Google Scholar] [CrossRef]
- Maheu, E.; Bannuru, R.R.; Herrero-Beaumont, G.; Allali, F.; Bard, H.; Migliore, A. Why we should definitely include intra-articular hyaluronic acid as a therapeutic option in the management of knee osteoarthritis: Results of an extensive critical literature review. Semin. Arthritis Rheum. 2019, 48, 563–572. [Google Scholar] [CrossRef]
- Zhang, H.; Cai, D.; Bai, X. Macrophages regulate the progression of osteoarthritis. Osteoarthr. Cartil. 2020, 28, 555–561. [Google Scholar] [CrossRef]
- Anderson, J.R.; Chokesuwattanaskul, S.; Phelan, M.M.; Welting, T.J.; Lian, L.Y.; Peffers, M.J.; Wright, H.L. 1H NMR metabolomics identifies underlying inflammatory pathology in osteoarthritis and rheumatoid arthritis synovial joints. J. Proteome Res. 2018, 17, 3780–3790. [Google Scholar] [CrossRef] [Green Version]
- Shi, X.; Wu, P.; Jie, L.; Zhang, L.; Mao, J.; Yin, S. Integrated Serum Metabolomics and Network Pharmacology to Reveal the Interventional Effects of Quzhi Decoction against Osteoarthritis Pain. Int. J. Anal. Chem. 2022, 2022, 9116175. [Google Scholar] [CrossRef]
- Leal, L.B.; Nogueira, M.S.; Canevari, R.A.; Carvalho, L.F.C.S. Vibration spectroscopy and body biofluids: Literature review for clinical applications. Photodiagnosis Photodyn. Ther. 2018, 24, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Balan, V.; Mihai, C.T.; Cojocaru, F.D.; Uritu, C.M.; Dodi, G.; Botezat, D.; Gardikiotis, I. Vibrational spectroscopy fingerprinting in medicine: From molecular to clinical practice. Materials 2019, 12, 2884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamwal, R.; Kumari, S.; Sharma, S.; Kelly, S.; Cannavan, A.; Singh, D.K. Recent trends in the use of FTIR spectroscopy integrated with chemometrics for the detection of edible oil adulteration. Vib. Spectrosc. 2021, 113, 103222. [Google Scholar] [CrossRef]
- Virtanen, V.; Tafintseva, V.; Shaikh, R.; Nippolainen, E.; Haas, J.; Afara, I.O.; Töyräs, J.; Kröger, H.; Solheim, J.; Zimmermann, B.; et al. Infrared spectroscopy is suitable for objective assessment of articular cartilage health. Osteoarthr. Cartil. Open 2022, 4, 100250. [Google Scholar] [CrossRef]
- Enders, A.A.; North, N.M.; Fensore, C.M.; Velez-Alvarez, J.; Allen, H.C. Confidential Manuscript: Functional group identification for FTIR spectra using image-based machine learning models. Anal. Chem. 2021, 93, 9711–9718. [Google Scholar] [CrossRef]
- Feng, A.L.; Wesely, N.C.; Hoehle, L.P.; Phillips, K.M.; Yamasaki, A.; Campbell, A.P.; Gregorio, L.L.; Killeen, T.E.; Caradonna, D.S.; Meier, J.C.; et al. A validated model for the 22-item Sino-Nasal Outcome Test subdomain structure in chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2017, 7, 1140–1148. [Google Scholar] [CrossRef]
- Ismail, A.M.; Sani, M.S.A.; Azid, A.; Zaki, N.N.M.; Arshad, S.; Tukiran, N.A.; Abidin, S.A.S.Z.; Samsudin, M.S.; Ismail, A. Food forensics on gelatine source via ultra-high-performance liquid chromatography diode-array detector and principal component analysis. SN Appl. Sci. 2021, 3, 79. [Google Scholar] [CrossRef]
- Sani, M.S.A.; Ismail, A.M.; Azid, A.; Samsudin, M.S. Establishing forensic food models for authentication and quantification of porcine adulterant in gelatine and marshmallow. Food Control 2021, 130, 108350. [Google Scholar] [CrossRef]
- Liang, D.; Xu, W.; Bai, X. An end-to-end transformer model for crowd localisation. arXiv 2022, arXiv:2202.13065. [Google Scholar]
- Santiago, D.D.B.; Barbosa, H.A.; Correia Filho, W.L.F.; Oliveira-Júnior, J.F.D. Interactions of Environmental Variables and Water Use Efficiency in the Matopiba Region via Multivariate Analysis. Sustainability 2022, 14, 8758. [Google Scholar] [CrossRef]
- Morais, C.L.; Lima, K.M.; Singh, M.; Martin, F.L. Tutorial: Multivariate classification for vibrational spectroscopy in biological samples. Nat. Protoc. 2020, 15, 2143–2162. [Google Scholar] [CrossRef] [PubMed]
- Talari, A.C.S.; Movasaghi, Z.; Rehman, S.; Rehman, I.U. Raman spectroscopy of biological tissues. Appl. Spectrosc. Rev. 2015, 50, 46–111. [Google Scholar] [CrossRef]
- Yu, K.; Wang, G.; Cai, W.; Wu, D.; Wei, X.; Zhang, K.; Liu, R.; Sun, Q.; Wang, Z. Identification of antemortem, perimortem and postmortem fractures by FTIR spectroscopy based on a rabbit tibial fracture model. Spectrochim. Acta Part A: Mol. Biomol. Spectrosc. 2020, 239, 118535. [Google Scholar] [CrossRef]
- Westad, F.; Marini, F. Validation of chemometric models–a tutorial. Anal. Chim. Acta 2015, 893, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Van Oudenaarde, K.; Jobke, B.; Oostveen, A.C.M.; Marijnissen, A.C.A.; Wolterbeek, R.; Wesseling, J.; Bierma-Zeinstra, S.M.A.; Bloem, H.L.; Reijnierse, M.; Kloppenburg, M. Predictive value of MRI features for development of radiographic osteoarthritis in a cohort of participants with pre-radiographic knee osteoarthritis—The CHECK study. Rheumatology 2016, 56, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Guermazi, A.; Burstein, D.; Conaghan, P.; Eckstein, F.; Le Graverand-Gastineau, M.P.H.; Keen, H.; Roemer, F.W. Imaging in osteoarthritis. Rheum. Dis. Clin. North Am. 2008, 34, 645–687. [Google Scholar] [CrossRef]
- Attur, M.; Krasnokutsky-Samuels, S.; Samuels, J.; Abramson, S.B. Prognostic biomarkers in osteoarthritis. Curr. Opin. Rheumatol. 2013, 25, 136. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.Y.; Li, J.Q.; Liu, H.G.; Wang, Y.Z. Attenuated total reflection-Fourier transform infrared spectroscopy (ATR-FTIR) combined with chemometrics methods for the classification of Lingzhi species. Molecules 2019, 24, 2210. [Google Scholar] [CrossRef] [Green Version]
- Lotz, M.; Martel-Pelletier, J.; Christiansen, C.; Brandi, M.L.; Bruyère, O.; Chapurlat, R.; Collette, J.; Cooper, C.; Giacovelli, G.; Kanis, J.A.; et al. Republished: Value of biomarkers in osteoarthritis: Current status and perspectives. Postgrad. Med. J. 2014, 90, 171–178. [Google Scholar] [CrossRef] [Green Version]
- Hoch, J.M.; Mattacola, C.G.; McKeon, J.M.; Howard, J.S.; Lattermann, C. Serum cartilage oligomeric matrix protein (sCOMP) is elevated in patients with knee osteoarthritis: A systematic review and meta-analysis. Osteoarthr. Cartil. 2011, 19, 1396–1404. [Google Scholar] [CrossRef] [Green Version]
- Heard, B.J.; Rosvold, J.M.; Fritzler, M.J.; El-Gabalawy, H.; Wiley, J.P.; Krawetz, R.J. Blood serum to diagnose osteoarthritis–biomarkers and machine learning. Osteoarthr. Cartil. 2014, 22, S64. [Google Scholar] [CrossRef]
- Reedy, J.; Lerman, J.L.; Krebs-Smith, S.M.; Kirkpatrick, S.I.; Pannucci, T.E.; Wilson, M.M.; Subar, A.F.; Kahle, L.L.; Tooze, J.A. Evaluation of the healthy eating index-2015. J. Acad. Nutr. Diet. 2018, 118, 1622–1633. [Google Scholar] [CrossRef] [PubMed]
- Elkorashey, R.M. Utilising chemometric techniques to evaluate water quality spatial and temporal variation. A case study: Bahr El-Baqar drain—Egypt. Environ. Technol. Innov. 2022, 26, 102332. [Google Scholar] [CrossRef]
- Alberto-Silva, C.; Malheiros, F.B.M.; Querobino, S.M. Fourier-transformed infrared spectroscopy, physicochemical and biochemical properties of chondroitin sulfate and glucosamine as supporting information on quality control of raw materials. Future J. Pharm. Sci. 2020, 6, 98. [Google Scholar] [CrossRef]
- Talari, A.C.S.; Martinez, M.A.G.; Movasaghi, Z.; Rehman, S.; Rehman, I.U. Advances in Fourier transform infrared (FTIR) spectroscopy of biological tissues. Appl. Spectrosc. Rev. 2017, 52, 456–506. [Google Scholar] [CrossRef]
- Mononen, M.E.; Tanska, P.; Isaksson, H.; Korhonen, R.K. New algorithm for simulation of proteoglycan loss and collagen degeneration in the knee joint: Data from the osteoarthritis initiative. J. Orthop. Res. 2018, 36, 1673–1683. [Google Scholar] [CrossRef]
- Loh, K.W.; Shaz, N.; Singh, S.; Raman, M.M.; Raghavendran, H.R.B.; Kamarul, T. Cytokine release by human bone marrow stromal cells isolated from osteoarthritic and diabetic osteoarthritic patients in vitro. J. Basic Clin. Physiol. Pharmacol. 2021. [Google Scholar] [CrossRef]
- Stockwell, B.R.; Angeli, J.P.F.; Bayir, H.; Bush, A.I.; Conrad, M.; Dixon, S.J.; Fulda, S.; Gascón, S.; Hatzios, S.K.; Kagan, V.E. Ferroptosis: A regulated cell death nexus linking metabolism, redox biology, and disease. Cell 2017, 171, 273–285. [Google Scholar] [CrossRef] [Green Version]
- Xu, Y.; Qian, S.Y. Anti-cancer activities of ω-6 polyunsaturated fatty acids. Biomed. J. 2014, 37, 112. [Google Scholar]
- Caruso, I. Use of 6-halo-4-quinolone Compounds and Pharmaceutical Compositions Thereof for the Preparation of a Medicament for the Therapeutical Application in Rheumatoid Arthritis. EP0361177A2. Available online: https://patents.google.com/patent/EP0361177A2/en (accessed on 29 August 1988).
- Brighty, K.E.; Gootz, T.D. Chemistry and mechanism of action of the quinolone antibacterials. In The Quinolones; Academic Press: Cambridge, MA, USA, 1990; pp. 33–97. [Google Scholar]
- Abdel-Aziz, H.A.; Eldehna, W.M.; Fares, M.; Al-Rashood, S.T.A.; Abdel-Aziz, M.M.; Soliman, D.H. Synthesis, biological evaluation and 2D-QSAR study of halophenyl bis-hydrazones as antimicrobial and antitubercular agents. Int. J. Mol. Sci. 2015, 16, 8719–8743. [Google Scholar] [CrossRef] [Green Version]
- Oinas, J.; Rieppo, L.; Finnilä, M.A.J.; Valkealahti, M.; Lehenkari, P.; Saarakkala, S. Imaging of osteoarthritic human articular cartilage using fourier transform infrared microspectroscopy combined with multivariate and univariate analysis. Sci. Rep. 2016, 6, 30008. [Google Scholar] [CrossRef] [Green Version]
- Unal, M.; Akkus, O. Shortwave-infrared Raman spectroscopic classification of water fractions in articular cartilage ex vivo. J. Biomed. Opt. 2018, 23, 015008. [Google Scholar] [CrossRef]
- Yavorskyy, A.; Hernandez-Santana, A.; McCarthy, G.; McMahon, G. Detection of calcium phosphate crystals in the joint fluid of patients with osteoarthritis–analytical approaches and challenges. Analyst 2008, 133, 302–318. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Control Group (Non-OA) | Inclusion Experimental Group (OA Group) | Exclusion Control and Experimental Group |
|---|---|---|
|
|
|
| Kaiser-Mayer Measure of Sampling Adequacy: |
|---|
| KMO: 0.820 |
| Discriminating Model (DM) | Ranking of Significant of Functional Group (cm−1) Contributed to Discriminating Model (p < 0.01) | Dataset | Correct Classification (100%) |
|---|---|---|---|
| OAHS: Osteoarthritis & healthy serum | 3960, 3880, 3860, 3850, 3842, 3841, 3819, 3816, 3814, 3786, 3779, 3769, 3743, 3742, 3729, 2583, 2579, 2569, 2559, 2558, 2551, 2547, 2540, 2532, 2520, 2510, 2503, 2502, 2499, 2497, 2487, 2484, 2480, 2476, 2459, 2458, 2455, 2453, 2443, 2439, 2437, 2434, 2420, 2418, 2416, 2298, 2272, 2270, 2198, 2061, 2055, 2053, 2010, 1954, 1929, 1919, 1915, 1904, 1887, 1870, 1869, 1866, 1865, 1860, 1858, 1856, 1854, 1852, 1850, 1846, 1843, 1841, 1839, 1836, 1833, 1831, 1830, 1824, 1823, 1821, 1815, 959 | Training dataset | |
| 0% | 100% | ||
| 100% | 100% | ||
| Total | 100% | ||
| Cross-validation dataset | |||
| 0% | 79.17% | ||
| 100% | 69.57% | ||
| Total | 74.47% | ||
| Testing dataset | |||
| 0% | 100% | ||
| 100% | 100% | ||
| Total | 100% | ||
| Verification dataset | |||
| 0% | 100% | ||
| 100% | 100% | ||
| Total | 100% |
| Peak | Frequency Range (cm−1) | Functional Group | Compound Class | Description | References |
|---|---|---|---|---|---|
| 1 | 3248 | O-H Stretching | Carboxylic Acid | Carboxylic Acid Indicates Fatty Acids Level | [46] |
| 2 | 1000 | C-O Stretching | Alcohol | Associated With The Changes In The Proteoglycan Contents | [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47] |
| 3 | 635 | C-Ci Stretching | Halo Compound | Due To The Presence Of Ring Deformation Of Phenyl Compounds. | [34] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aziz, A.A.; Selvaratnam, V.; Fikri, Y.F.B.A.; Sani, M.S.A.; Kamarul, T. Diagnosis of Osteoarthritis at an Early Stage via Infrared Spectroscopy Combined Chemometrics in Human Serum: A Pilot Study. Processes 2023, 11, 404. https://doi.org/10.3390/pr11020404
Aziz AA, Selvaratnam V, Fikri YFBA, Sani MSA, Kamarul T. Diagnosis of Osteoarthritis at an Early Stage via Infrared Spectroscopy Combined Chemometrics in Human Serum: A Pilot Study. Processes. 2023; 11(2):404. https://doi.org/10.3390/pr11020404
Chicago/Turabian StyleAziz, Atiqah Ab, Veenesh Selvaratnam, Yasmin Fadzlin Binti Ahmad Fikri, Muhamad Shirwan Abdullah Sani, and Tunku Kamarul. 2023. "Diagnosis of Osteoarthritis at an Early Stage via Infrared Spectroscopy Combined Chemometrics in Human Serum: A Pilot Study" Processes 11, no. 2: 404. https://doi.org/10.3390/pr11020404