
Understanding the Influence of Socioeconomic Variables on Medicinal Plant Knowledge in the Peruvian Andes


1
Instituto de Investigación para el Desarrollo Sustentable de Ceja de Selva, Universidad Nacional Toribio Rodríguez de Mendoza de Amazonas, Chachapoyas 01001, Peru
2
Departamento de Biología, Área de Botánica, Universidad Autónoma de Madrid, Calle Darwin 2, ES–28049 Madrid, Spain
3
Centro de Investigación en Biodiversidad y Cambio Global (CIBC-UAM), Universidad Autónoma de Madrid, Calle Darwin 2, ES–28049 Madrid, Spain
*
Author to whom correspondence should be addressed.
Plants 2022, 11(20), 2681; https://doi.org/10.3390/plants11202681
Submission received: 18 July 2022
/
Revised: 27 September 2022
/
Accepted: 3 October 2022
/
Published: 12 October 2022
(This article belongs to the Section Plant Ecology)
Abstract
:In this study, we analyze the impact of 18 socioeconomic factors at individual, family, and locality levels to understand their influence on medicinal plant knowledge (MPK) in four provinces and 12 localities of the northern Andes of Peru. We interviewed 50 participants per locality (totaling 600 people) from lowlands and highlands ecoregions. The participants were balanced in terms of generations and gender. We performed multivariate statistical analyses—generalized linear mixed models (GLMMs) and nonmetric multidimensional scaling (NMDS) ordinations—that showed the influence of each socioeconomic variable on the medicinal plant knowledge of people in the different sites. At the individual level, we found that most participants with higher MPK were women, elders, people with lower levels of education and job qualifications, non-migrants, and participants who have lived for a long period in the same region. At the family level, we found that participants living in low economic conditions with few material goods, including their means of transport, tools possession, access to technology, farm size, number of farm animals, and house quality, had higher MPK. At the locality level, we found that people living in more isolated areas with scarce regional services, such as access to paved roads, hospitals, big markets, tourist development, and chlorination of drinking water, had higher MPK. In short, people with less access to modern services and with low economic resources are the main depositaries of MPK. Policy makers and decision makers should consider the significance of MPK in alleviating health problems and diseases in Andean regions, especially for people with rural livelihoods. This local botanical knowledge of medicinal plants should be preserved in the area as a great natural heritage for humanity.
1. Introduction
Socioeconomic and cultural changes have different implications for the medicinal plant knowledge (MPK) of distinct human populations, at both the global and local scales. MPK is particularly significant in developing countries that conserve traditions more prominently and depend on natural resources [1,2]. In recent decades, the socioeconomic framework has changed rapidly during the lifetimes of people in developing countries [3]. Usually, when the socioeconomic situation has improved at both personal and regional levels, it has been accompanied by the loss of MPK and cultural identity for local people [4,5].
One way to analyze these socioeconomic and cultural changes is through ethnobotanical studies, which provide good models for understanding patterns of change across societies, focusing on the use of plants by people who clearly depend on their socioeconomic and cultural situations [6,7,8]. In this sense, medicinal plants have a special relevance for economies and for the conservation of culture, as they help in maintaining health, providing basic sustenance for people’s livelihoods, and reflecting their traditions, at costs that are cheaper than those of allopathic medicine [9,10].
Socioeconomic variables can be classified into three different levels for a human group living in a rural environment: an individual level, a family level, and a locality level [11]. All three of these three levels have been reported to influence MPK.
At the individual level, many earlier studies documented that women and older age groups are the most important custodians of MPK [12,13]. In addition, there are other variables that influence MPK at this level, such as higher levels of education, which seem to displace the traditional culture, knowledge, and skills of younger people [14], and personal occupations, as people in highly specialized jobs demonstrate a low level of MPK [15,16]. The migratory status and time-of-residence of people in a particular area are also related to MPK, which is more common among residents who were born and lived in the same region for a long time [17,18].
At the family level, distinct variables have also been used to analyze different forms of economic wealth in relation to MPK, such as means of transport, access to technological services, and ownership of tools, cattle, and farmland. In all these situations, having more possessions is related to lower MPK [19]. If a family home is in good condition, this can be related to the family’s greater economic ability to repair any damage to the home; such families tend to have lower MPK [20].
At the locality level, low access to regional services, such as paved roads, hospitals, and big markets, results in the isolation of a locality, enhancing the preservation of their MPK [21,22]. In contrast, the implementation of water treatment with chlorination for human consumption reduces the incidence of diarrheal diseases and other infectious diseases transmitted by water [23], which may be related to a low transmission of MPK from the elder people to younger people. Likewise, tourist attractions provide direct economic benefits for local inhabitants, which may be an advantage for economic development but a disadvantage for maintaining traditional knowledge [24].
In Peru, some studies have focused on the maintenance of MPK at the personal level [25,26,27,28], but to the best of our knowledge, this is the first study that analyzes the relationships between the socioeconomic situation of people at individual, family, and locality levels and their usage of medicinal plants. The aim of this paper is to combine a study that integrates the largest number of socioeconomic factors, gathered from hundreds of participants living in different Andean ecoregions, with their MPK obtained over the course of their lives, using a stratified interview methodology with the collaboration of local mestizo inhabitants.
Specifically, in this study we analyzed the impact of socioeconomic factors on the use of medicinal plants for rural populations in the Peruvian Andes. Our first hypothesis, related to the influence of socioeconomic factors at the individual level, was that people with higher educational levels, specialized jobs, shorter residence times, and migrant status will have lower MPK. Our second hypothesis, related to the impact of socioeconomic variables at the family level, was that people with greater financial resources, in the form of modern means of transport and tools, access to technological services, possession of livestock, and farm size, will know less about medicinal plants and their uses. Our third hypothesis, at the locality level, was that people living in localities that are close to tourist attractions, paved roads, hospitals, big markets, and treated water services will have lower MPK.
2. Results
2.1. The Influence of Socioeconomic Factors on MPK
Overall, localities in the highlands had higher numbers of medicinal plants and reported greater usage of medicinal plants, compared with localities in the lowlands, particularly in the province of Chachapoyas (Table 1). In relation to the age of participants and family size, the results showed a positive relationship with MPK in all highlands and lowlands, although the significance of this relationship differed between them.
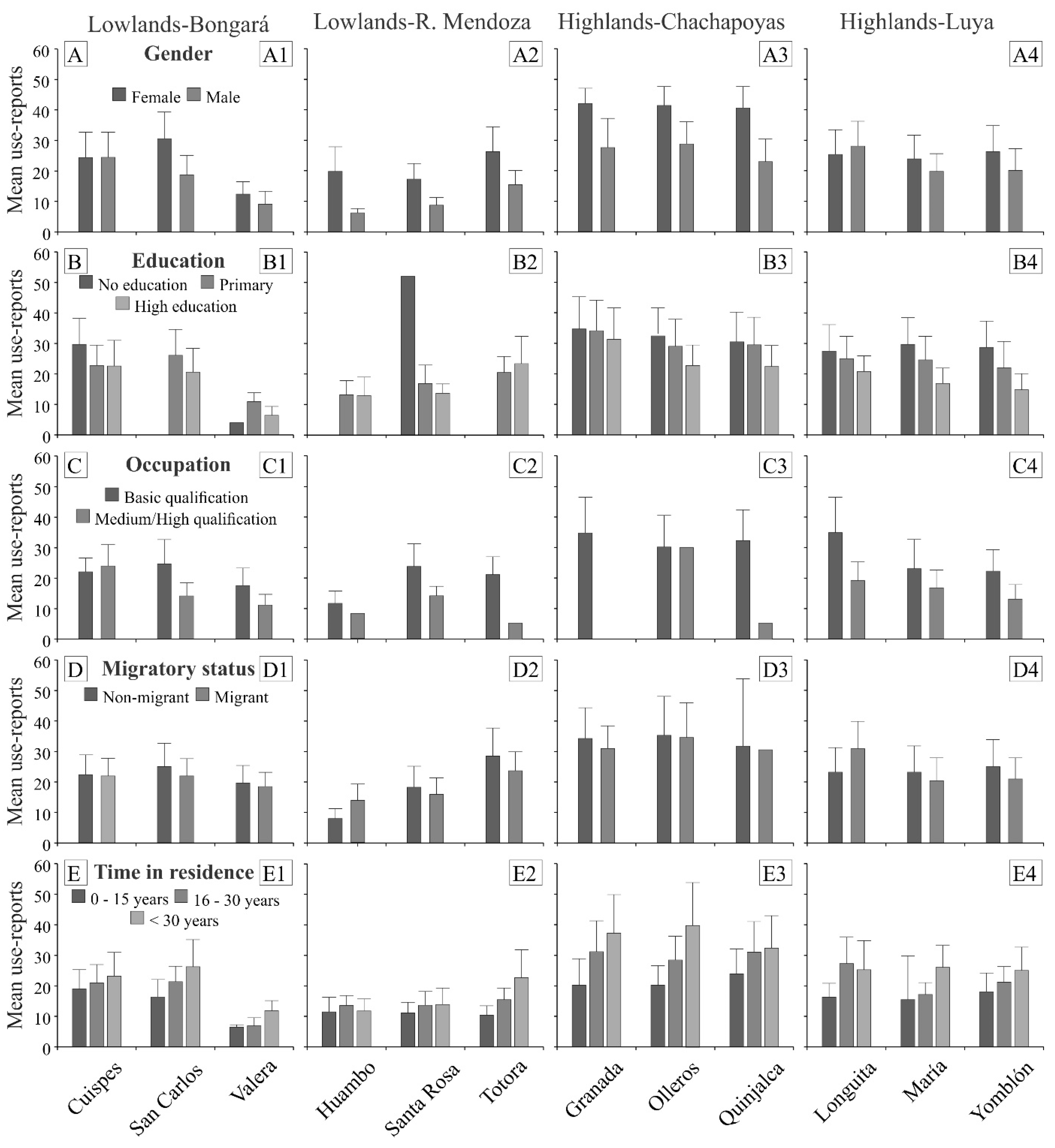
At the individual level, the results for the different socioeconomic factors were as follows (Figure 1, Table S1): (1) Women had MPK in higher numbers than men in the four provinces, although in the locality of Longuita the results were reversed (Figure 1A); (2) Overall, education had a negative effect on MPK, indicating that MPK decreased as formal education increased in all localities, with the exceptions of Valera and Totora (Figure 1B); (3) People with specialized jobs demonstrated lower MPK than people with basic occupations, with the exception of Cuispes (Figure 1C); (4) Non-migrants had MPK in higher numbers than migrants, with the exceptions of Huambo and Longuita (Figure 1D); and (5) Participants who had been living in an area for longer periods had higher MPK, with the exceptions of Huambo and Longuita (Figure 1E).
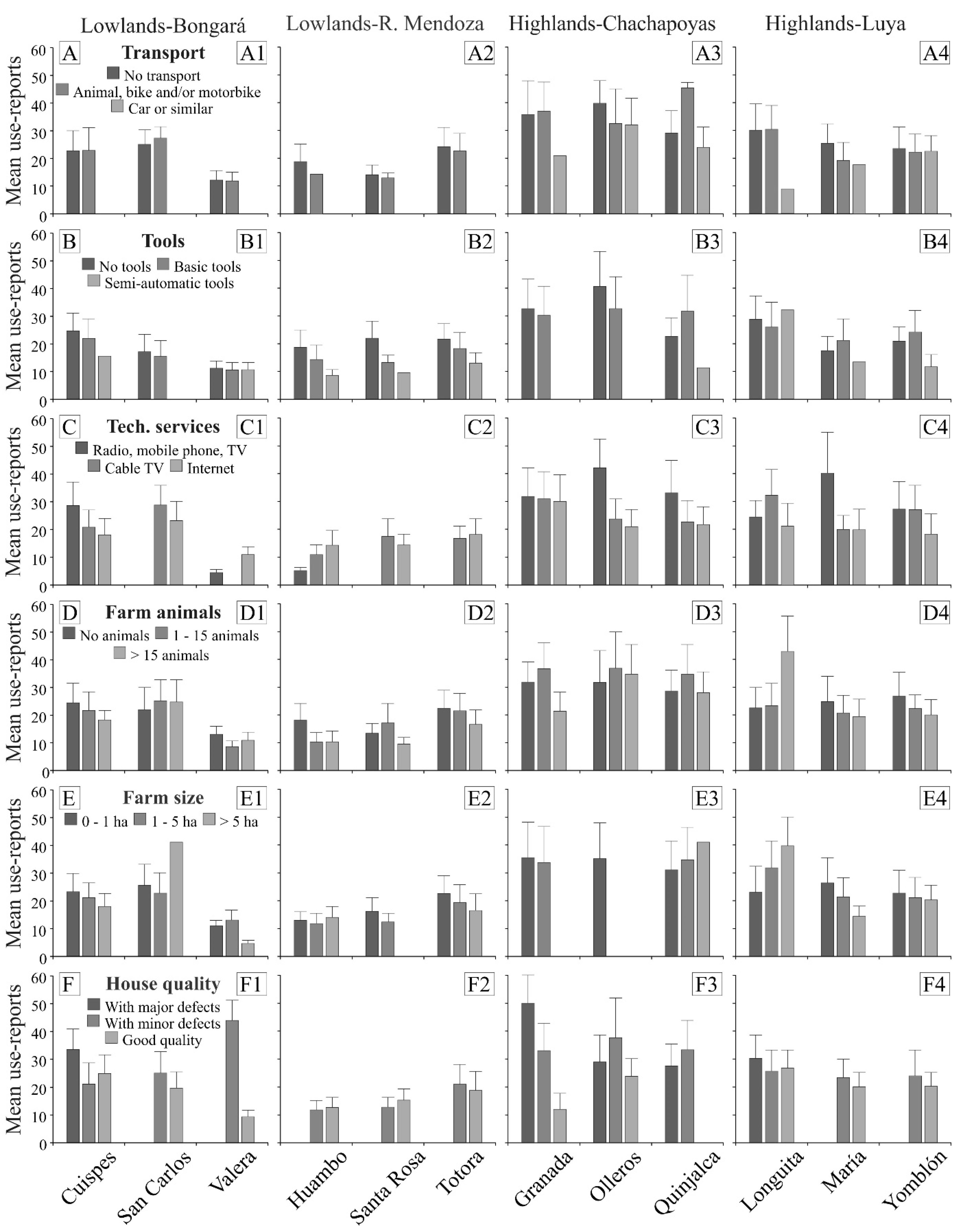
At the family level, we found the following results (Figure 2, Table S1): (1) Participants that possessed no transport or basic transports demonstrated higher MPK than participants with motor vehicles (Figure 2A); (2) Participants who did not possess any tools, or just basic tools, had higher MPK than participants with semi-automatic tools, with the exception of Longuita (Figure 2B); (3) People in localities of the lowlands, with lower MPK, had access to cable TV or the Internet, with the exception of Cuispes, while people in localities of the highlands, with higher MPK, had no access to technology, with the exception of Longuita (Figure 2C); (4) Participants who did not possess farm animals. or possessed a low number of them, had higher MPK than participants who used farm animals for trade, with the exceptions of Santa Rosa and Longuita (Figure 2D); (5) Families with a farm size of less than five hectares had higher MPK, with the exception of San Carlos and Huambo in the lowlands and Quinjalca and Longuita in the highlands (Figure 2E); (6) Families whose houses had major defects had higher MPK than those with good quality houses, with the exception of Cuispes, Huambo, and Santa Rosa in the lowlands (Figure 2F).
At the locality level, we found that participants living in localities without access to paved roads, hospitals, big markets, and tourist attractions showed higher MPK than participants living in localities with access to these services (Table 2). In addition, people from localities that had no chlorination system for drinking water had higher MPK than people from localities that had this service.
2.2. Mixed-Model Effects of Socioeconomic Factors on MPK
We found that nine of the 18 socioeconomic factors showed a significant association with MPK in 11 of the 12 localities, with the exception of María (highlands), and those 11 localities showed significant associations with one to three socioeconomic factors (Table 3). At the individual level, the associations were as follows: (1) Gender had a statistically significant negative association in three localities of the lowlands (San Carlos, Valera, and Totora) and in one locality of the highlands (Quinjalca); (2) Education had a statistically significant negative influence on MPK in three localities of the lowlands (San Carlos, Santa Rosa, and Totora) and in one locality of the highlands (Yomblón); (3) Occupation had a negative association with MPK in two localities of the lowlands (San Carlos and Santa Rosa); (4) Migration had a statistically significant negative relationship with MPK only in Longuita; (5) Time-in-residence showed significant associations with MPK in two localities of the highlands (Longuita and Yomblón).
At the family level, the associations were as follows: (1) Family size had a statistically significant positive association in three localities of the highlands (Granada, Olleros, and Yomblón); (2) Transport showed statistically negative associations with the maintenance of MPK only in Totora; (3) The possession of tools had a negative association with MPK in two localities of the highlands (Granada and Olleros) and two localities of the lowlands (Cuispes and Valera); and (4) Access to technological services showed negative significant associations in the lowlands (Huambo and Santa Rosa) and in the highlands (Granada).
2.3. Relationship between Socioeconomic Factors and Medicinal Categories
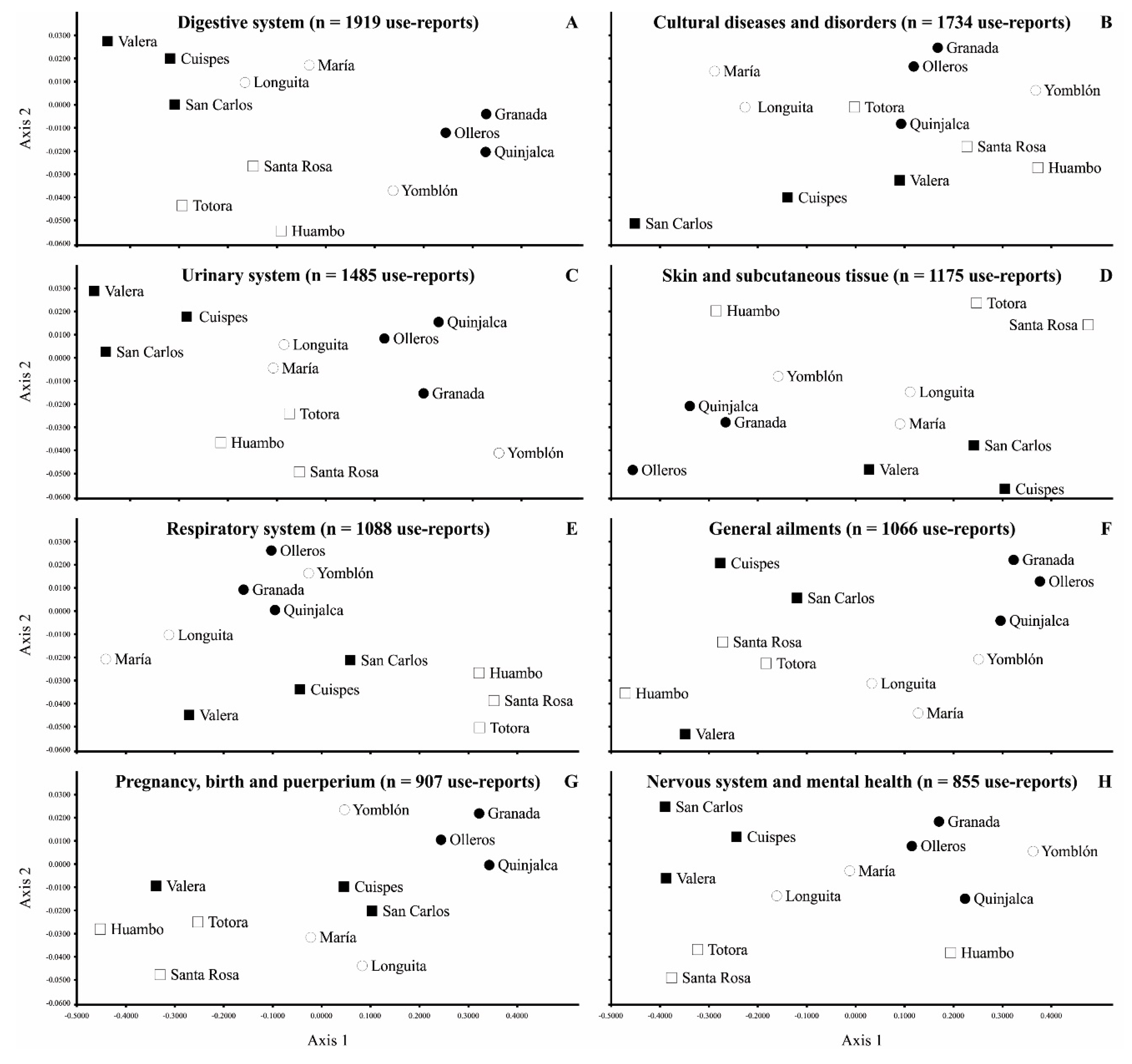
Overall, localities in both the highlands and the lowlands tended to be grouped into different medicinal categories. In the highlands, the three localities of the Chachapoyas province showed a clear group in each of the different medicinal categories. Within the localities of the Luya province (highlands), Yomblón tended to be closer to the localities of the Chachapoyas province, while Longuita and María were grouped across all the medicinal categories. In the lowlands, the three localities of the Rodríguez de Mendoza province were grouped for most of the categories (Figure 3A,C,E–G), but Huambo was clearly separated in the categories of s”Skin and subcutaneous tissue” and ”Nervous system and mental health” (Figure 3D,H, respectively). Finally, the localities of the Bongará province were grouped for most of the medicinal categories (Figure 3A–E,H), but Valera showed a distinct pattern for the categories of “General ailments and unspecific symptoms” and ”Pregnancy, birth and puerperium” (Figure 3F,G, respectively).
3. Discussion
3.1. Influence of Socioeconomic Factors on MPK at the Individual Level
The results for the socioeconomic factors at the personal level supported our first hypothesis: higher educational levels, higher job qualifications, shorter residence times in a region, and non-migrant status were negatively related to the maintenance of MPK. These findings can be explained on the basis that conventional education currently removes young people from their natural environment and, consequently, reduces their opportunity to learn traditional knowledge from their predecessors [29,30]. Education has a close relationship with future occupation, because achieving a higher level of education is related to having a specialized job; such jobs are usually found in cities with a certain concentration of businesses and/or public institutions and, therefore, city people tend to have lower traditional knowledge [31,32]. Migratory status showed a negative relationship with MPK, consistent with the commonly reported phenomenon that migration and globalization are related to the loss of MPK [33]. Time-in-residence showed a pattern similar to that of migratory status, indicating that longer residence times for people in a region generate more direct contact with their environment and, therefore, time-in-residence is related to higher MPK [1,34], although some other studies have found an opposite pattern [18,35].
Generally, women had higher MPK than men, consistent with most earlier studies in the Andes, based on their role in taking care of children and elders [13,36]. Overall, elders showed greatest MPK, as they had the opportunity to accumulate traditional knowledge in earlier times, as many other papers have previously documented [28,37].
3.2. Influence of Socioeconomic Factors on MPK at the Family Level
Our second hypothesis was also supported. We established that the possession of material goods (modern means of transport and tools, access to technological services, possession of livestock, and farm size) is related to lower MPK, and our results support that conclusion in most localities. The possession of assets depends on the availability of economic resources to obtain them, and their use in close relation to agricultural and livestock practices may be focused on trade; consequently, such usage may require more technical tools, better means of transport, and access to technological services [38,39]. This hypothesis was also related to the number of children per family who had a positive association with the maintenance of MPK in both ecoregions. Families with a larger number of members tend to have lower economic possibilities and more economic difficulties in accessing health services, as previously reported in other studies [40,41]. In general, families living in houses that needed some repair showed higher MPK than families living in houses of good quality, which again reflects their respective economic resources (Corroto, personal observations).
3.3. Influence of Socioeconomic Factors on MPK at the Locality Level
Our results support our third hypothesis, confirming that participants living in localities close to tourist attractions, paved roads, hospitals, big markets, and water chlorination showed a lower MPK. Highlands localities had fewer regional services than lowlands localities, and this isolation provided an advantage for the conservation of medicinal traditional knowledge [22,42,43]. In contrast, the lowlands localities are characterized by better levels of regional economic development, such as paved roads, commercial urban centers, and health services, which are related to a lower maintenance of MPK [44,45]. In addition, localities close to hospitals tend to place their trust in allopathic medicine, unlike those distant localities that still trust in traditional medical healers, as is the case with people from the highlands in our study [46,47]. The localities closer to tourist attractions have medical centers and posts, which are related to the progressive abandonment of traditional medicine [48]. Finally, all localities in the lowlands, unlike some localities in the highlands, have a chlorinated water supply for human consumption, which is an indicator of progress in developing countries. as its implementation reduces health problems [49]; therefore, the people in the localities of Chachapoyas, which have no water chlorination systems, showed higher MPK.
3.4. Similarities of Socioeconomic Factors across Localities and Medicinal Categories
Based on socioeconomic factors, the different ecoregions and localities showed a relatively similar pattern of spatial ordination for the different medicinal categories. The separation into two groups of the highlands localities was related to their differential socioeconomic factors. For most medicinal categories, the three localities of the Chachapoyas province were grouped together with the locality of Yomblón (in the Luya province), because they share geographical isolation and limited access to regional services, including paved roads. Their isolation and limited access to contemporary health care favor the preservation of traditional medical practices that are similar, as reflected in the different medicinal categories [50]. In the case of lowlands, the localities were mainly grouped within the same province, with two exceptions in terms of divergent medicinal categories: Valera (in the Bongará province), which is closer to the localities of the Rodríguez de Mendoza province. and Huambo (in the Rodríguez de Mendoza province), which is closer to the localities of the Chachapoyas province. These localities were grouped together because they have analogous socioeconomic factors and geographical situations within their regional context. Finally, one of the factors that most affected the maintenance of MPK was probably proximity to a hospital, which may explain that the localities of the Rodríguez de Mendoza province suffered a greater loss of MPK, as has been recorded in other studies [51].
4. Materials and Methods
4.1. Study Area
Our research was carried out in high tropical montane regions (highlands) and low tropical montane regions (lowlands) of the northeastern Peruvian Andes, in the Amazonas Department (Figure 4). These classifications were based on the descriptions of the Peruvian ecological regions proposed by León et al. [52]. In each ecoregion, we studied two provinces (Chachapoyas and Luya in the highlands, Bongará and Rodríguez de Mendoza in the lowlands) and three localities per province, all of which were inhabited by mestizo people. Six of the 12 localities were established between 2500 m and 3500 m in the highlands (Granada, Olleros, and Quinjalca in Chachapoyas; Longuita, María, and Yomblón in Luya), while the six other localities were located between 1500 m and 2500 m in the lowlands (Cuispes, San Carlos, and Valera in Bongará; Huambo, Santa Rosa, and Totora in Rodríguez de Mendoza). In both ecoregions, there is a seasonal climate that alternates with a wet season between November and May, and a dry season for the remaining months of the year, with an average annual rainfall of 780 mm and average temperatures of 14 °C, which are somewhat lower in the highlands, compared with the lowlands (900 mm and 19 °C, respectively) [53].
The selection of the localities was based on different geographical characteristics and socioeconomic development. In general terms, the populations of the lowlands have more economic resources and better infrastructures than the populations of the highlands (Table 4). The localities of the Rodríguez de Mendoza province (lowlands) are the only ones that have a productive coffee monoculture and intensive livestock, while the three other provinces have subsistence agriculture (Bongará) or more diverse productive agriculture (highlands). There are touristic attractions in both Bongará (lowlands) and Luya (highlands), with the exception of Yomblón. Localities in the Rodríguez de Mendoza and Luya provinces have paved roads (except for Yomblón). The only localities with a hospital are in Rodríguez de Mendoza. The localities of the Chachapoyas province are the only ones with no access to big markets or water chlorination. The lowlands localities have a higher population density than the highlands localities; Chachapoyas, by far, is the province with the lowest population [30].
4.2. Data Collection
A total of 600 semi-structured interviews (50 per locality) were carried out to gather information on medicinal plants. We divided participants into five age groups (18–30, 31–40, 41–50, 51–60, and >60 years old), balancing the participants between men and women (see [55] for further details). We conducted closed interviews with all of the participants to gather socioeconomic information related to 18 variables, classified into three levels: an individual level, a family level, and a locality level (Table 5). At the individual level, we included gender, age, education, occupation, migratory status, and time-of-residence in the region. At the family level, we studied family size, means of transport, possession of tools, access to technological services, number of farm animals, farm size, and house quality. At the locality level, we analyzed the proximity to paved roads, hospitals, big markets, tourist attractions, and water treatment for human consumption.
The identification of plant specimens was carried out in the Herbarium Truxillense (HUT), and a voucher containing all of the collected information was deposited in this institution. The scientific names followed the plant list [56] and the taxonomic classification at the family level followed the angiosperm phylogeny group [57].
4.3. Data Analysis
All of the reported medicinal indications were classified into 19 use categories, following international standards [58], with added modifications based on the cultural, ritual, or magical diseases proposed by [59,60].
We classified the 18 socioeconomic factors into three types of variables: nominal (gender and locality); ordinal (education, occupation, migration status, time-in-residence, transport, tools, access to technological services, farm animals, farm size, house quality, proximity to paved roads, proximity to hospitals, proximity to big markets, proximity to places of tourist interest, and water quality); and continuous (age and family size) (Table 5).
Two ethnobotanical indicators were analyzed: (1) reports on the usage of medicinal plants use, which were the sum of all medicinal uses reported by one participant for all of the species known, and (2) useful medicinal plant species, which corresponded to the sum of all of the documented species by each participant. We defined “medicinal use” as the use of a plant part of a species that is associated with a medicinal category for a particular disease or ailment [40]. We found strong correlations between the two ethnobotanical indicators for all localities (highlands r = 0.66–0.84; lowlands r = 0.62–0.82) and, therefore, we decided to use only the reports on medicinal plants usage as the dependent variable in all of the the subsequent analyses.
To analyze MPK related to the 18 socioeconomic variables studied in the 12 localities, we first used multivariate analysis of variance (MANOVA) analyses with the full dataset and its corresponding post hoc Tukey test for the 16 categorical variables and Pearson correlations for the two continuous variables (Table 5). After these analyses, we selected the socioeconomic variables for use in the analyses that followed. We excluded categorical variables that had significant differences based on their different levels, and also excluded continuous variables with p < 0.05.
To assess the variations in traditional knowledge in the 12 studied localities of the Andean lowlands and highlands, we carried out generalized linear mixed models with negative binominal distribution to analyze the effects of the socioeconomic variables on MPK, using the reports on medicinal plants usage. We implemented models for each of the three different socioeconomic levels: an individual level, a family level, and a locality level. The dependent variable was the number of reports on medicinal plants usage, and the independent variables with a fixed effect were the socioeconomic factors that were selected in each region, based on the initial descriptive analysis. Regions were established as random factors for the categorical variable locality. The one-level random-intercept model that we constructed was based on the following formula:
where Yij is the independent variable, ƴ00 is the common intercept, β and τ are the respective coefficients of the continuous variables Xi and categorical X´i, r0j has a normal distribution with median 0, standard deviation σL represents the variability of the 12 localities, and eij is the error or residual for each of the interviewees.
To visualize whether the provinces and localities were spatially grouped according to socioeconomic levels, we performed nonmetric multidimensional scaling (NMDS) analyses with all socioeconomic variables for the eight most-cited medicinal categories (>800 reports of usage). To calculate the (dis-)similarities between the localities, we used Euclidean distances and we implemented analyses for the first two axes that were subsequently plotted in Figure 3A–H. All of the analyses were performed with Infostat Analytical Software for Windows [61].
5. Conclusions
Socioeconomic factors have a strong influence in the maintenance of medicinal plant knowledge (MPK) along the northern Peruvian Andes. Our research showed that people with higher MPK have lower levels of education and unspecialized jobs, and that they have been living in the same region for a long period of time. Such people usually have large families, low economic wealth, and few material goods, and they live in localities that are relatively isolated, with scarce regional services. In short, people with less access to modern services and with low economic resources are the main carriers of MPK. This conclusion can probably be generalized to other developing countries, in similar Andean regions, for all types of traditional knowledge. Politicians and decision makers who are concerned with social and conservation issues, at both national and international levels, should consider the significance of MPK when implementing poverty alleviation programs, in order to improve people’s livelihoods. In addition, this magnificent traditional knowledge must be documented for humankind before it vanishes forever.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/plants11202681/s1, Table S1: Number of participants interviewed for each socioeconomic variable in 12 localities of northern Peruvian Andes.
Author Contributions
Conceptualization, F.C., O.A.G.T. and M.J.M.; formal analysis, F.C. and M.J.M.; investigation, F.C., O.A.G.T. and M.J.M.; methodology, M.J.M.; resources, O.A.G.T.; supervision, O.A.G.T.; validation, M.J.M.; writing—review and editing, F.C. and M.J.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Universidad Nacional Toribio Rodríguez de Mendoza and Universidad Autónoma de Madrid. M.J. Macía received support from the Spanish Ministry of Economy and Competitiveness [grant number CGL2016-75414-p].
Institutional Review Board Statement
The study was carried out according to the Convention on Biological Diversity, taking into account the Bonn guidelines and the Nagoya Protocol [62,63]. A written permit for the approval of the study was required by the local authorities of Chachapoyas and by the Regional Government of the Amazonas Department. Informed consent was provided by each participant, indicating that (1) they could stop the interview at any time, and (2) the data processing would be anonymous. The ethics committee of the Autonomous University of Madrid approved this statement (CEI 73-1327 to M.J. Macía).
Informed Consent Statement
Informed consent was obtained from all the authorities of the municipalities involved in the study and oral consent from all 600 participants.
Data Availability Statement
The data presented in this study are available in this article and its supplementary material.
Acknowledgments
We are deeply thankful to the 600 participants who shared their time and knowledge with us and to the political and communal representatives that permitted the study. Special thanks to Damaris Leiva Tafur, Jhesibel Chavez Ortiz, and Jesús Rascón Barrios for their invaluable assistance in data collection in the field, and to Elgar Barboza for his help in the preparation of Figure 4.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Almeida, C.F.C.B.R.; Ramos, M.A.; Amorim, E.L.C.; Albuquerque, U.P. A comparison of knowledge about medicinal plants for three rural communities in the semi-arid region of northeast of Brazil. J. Ethnopharmacol. 2010, 127, 674–684. [Google Scholar] [CrossRef]
- Mafimisebi, T.E.; Oguntade, A.E.; Fajemisin, A.N.; Aiyelari, O.P. Local knowledge and socio-economic determinants of traditional medicines’ utilization in livestock health management in Southwest Nigeria. J. Ethnobiol. Ethnomed. 2012, 8, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albuquerque, U.P.; Nascimento, A.L.B.; Soldati, G.T.; Feitosa, I.S.; Campos, J.L.A.; Hurrell, J.A.; Hanazaki, N.; Medeiros, P.M.D.; Silva, R.R.V.D.; Ludwinsky, R.H.; et al. Ten important questions/issues for ethnobotanical research. Acta Bot. Brasilica 2019, 33, 376–385. [Google Scholar] [CrossRef]
- Botha, J.; Witkowski, E.T.F.; Shackleton, C.M. Market profiles and trade in medicinal plants in the Lowveld, South Africa. Env. Conserv. 2004, 31, 38–46. [Google Scholar] [CrossRef] [Green Version]
- Mathez-Stiefel, S.L.; Brandt, R.; Lachmuth, S.; Rist, S. Are the young less knowledgeable? Local knowledge of natural remedies and its transformations in the Andean Highlands. Hum. Ecol. 2012, 40, 909–930. [Google Scholar] [CrossRef] [Green Version]
- Phillips, O.; Gentry, A.H.; Reynel, C.; Wilkin, P.; Gálvez-Durand, B.C. Quantitative ethnobotany and Amazonian conservation. Conserv. Biol. 1994, 8, 225–248. [Google Scholar] [CrossRef]
- Reyes-Garcia, V.; McDade, T.; Vadez, V.; Huanca, T.; Leonard, W.R.; Tanner, S.; Godoy, R. Non-market returns to traditional human capital: Nutritional status and traditional knowledge in a native Amazonian society. J. Dev. Stud. 2008, 44, 217–232. [Google Scholar] [CrossRef]
- Bussmann, R.W.; Sharon, D.; Lopez, A. Blending traditional and Western medicine: Medicinal plant use among patients at Clinica Anticona in El Porvenir, Peru. Ethnobot. Res. Appl. 2007, 5, 185–199. [Google Scholar] [CrossRef] [Green Version]
- Macía, M.J.; García, E.; Vidaurre, P.J. An ethnobotanical survey of medicinal plants commercialized in the markets of La Paz and El Alto, Bolivia. J. Ethnopharmacol. 2005, 97, 337–350. [Google Scholar] [CrossRef] [PubMed]
- Pardo-de-Santayana, M.; Macía, M.J. Biodiversity: The benefits of traditional knowledge. Nature 2015, 518, 487–488. [Google Scholar] [CrossRef] [PubMed]
- Salpeteur, M.; Patel, H.H.; Molina, J.L.; Balbo, A.L.; Rubio-Campillo, X.; Reyes-García, V.; Madella, M. Comigrants and friends: Informal networks and the transmission of traditional ecological knowledge among seminomadic pastoralists of Gujarat, India. Ecol. Soc. 2016, 21, 20. [Google Scholar] [CrossRef] [Green Version]
- Voeks, R.A. Are women reservoirs of traditional plant knowledge? Gender, ethnobotany and globalization in northeast Brazil. Singap. J. Trop. Geogr. 2007, 28, 7–20. [Google Scholar] [CrossRef]
- Mathez-Stiefel, S.L.; Vandebroek, I. Distribution and transmission of medicinal plant knowledge in the Andean highlands: A case study from Peru and Bolivia. Evid. Based Complement. Altern. Med. 2012, 2012, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes-García, V.; Guèze, M.; Luz, A.C.; Paneque-Gálvez, J.; Macía, M.J.; Orta-Martínez, M.; Pino, J.; Rubio-Campillo, X. Evidence of traditional knowledge loss among a contemporary indigenous society. Evol. Hum. Behav. 2013, 34, 249–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muthu, C.; Ayyanar, M.; Raja, N.; Ignacimuthu, S. Medicinal plants used by traditional healers in Kancheepuram District of Tamil Nadu, India. J. Ethnobiol. Ethnomed. 2006, 2, 43. [Google Scholar] [CrossRef] [Green Version]
- Corroto, F.; Rascón, J.; Barboza, E.; Macía, M.J. Medicinal plants for rich people vs. Medicinal plants for poor people: A case study from the Peruvian andes. Plants 2021, 10, 1634. [Google Scholar] [CrossRef] [PubMed]
- Pirker, H.; Haselmair, R.; Kuhn, E.; Schunko, C.; Vogl, C.R. Transformation of traditional knowledge of medicinal plants: The case of Tyroleans (Austria) who migrated to Australia, Brazil and Peru. J. Ethnobiol. Ethnomed. 2012, 8, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abreu, D.B.O.; Santoro, F.R.; Albuquerque, U.P.; Ladio, A.H.; Medeiros, P.M. Medicinal plant knowledge in a context of cultural pluralism: A case study in Northeastern Brazil. J. Ethnopharmacol. 2015, 175, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Kunwar, R.M.; Bussmann, R.W. Ethnobotany in the Nepal Himalaya. J. Ethnobiol. Ethnomed. 2008, 4, 24. [Google Scholar] [CrossRef] [Green Version]
- Benz, B.F.; Cevallos, J.; Santana, F.; Rosales, J.; Graf, S. Losing knowledge about plant use in the Sierra de Manantlan biosphere reserve Mexico Econ. Botany 2000, 54, 183–191. [Google Scholar] [CrossRef]
- Rai, P.K.; Lalramnghinglova, H. Ethnomedicinal plant resources of Mizoram, India: Implication of traditional knowledge in health care system. Ethnobot. Leafl. 2010, 14, 274–305. [Google Scholar]
- Vandebroek, I. The dual intracultural and intercultural relationship between medicinal plant knowledge and consensus. Econ. Bot. 2010, 64, 303–317. [Google Scholar] [CrossRef]
- World Health Organization. Progress on Drinking Water, Sanitation and Hygiene: 2017 Update and SDG Baselines; World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF): Geneva, Switzerland, 2017. [Google Scholar]
- Wearing, S.; McDonald, M. The development of community-based tourism: Re-thinking the relationship between tour operators and development agents as intermediaries in rural and isolated area communities. J. Sustain. Tour. 2002, 10, 191–206. [Google Scholar] [CrossRef]
- De la Cruz, H.; Vilcapoma, G.; Zevallos, P.A. Ethnobotanical study of medicinal plants used by the Andean people of Canta, Lima, Peru. J. Ethnopharmacol. 2007, 111, 284–294. [Google Scholar] [CrossRef]
- Monigatti, M.; Bussmann, R.W.; Weckerle, C.S. Medicinal plant use in two Andean communities located at different altitudes in the Bolívar Province, Peru. J. Ethnopharmacol. 2013, 145, 450–464. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, M.; Malpartida, S.B.; Santiago, H.B.; Jullian, V.; Bourdy, G. Hot and cold: Medicinal plant uses in Quechua speaking communities in the high Andes (Callejón de Huaylas, Ancash, Perú). J. Ethnopharmacol. 2014, 155, 1093–1117. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Biset, J.; Campos de la Cruz, J.; Epiquién Rivera, M.A.; Canigueral, S. A first survey on the medicinal plants of the Chazuta valley (Peruvian Amazon). J. Ethnopharmacol. 2009, 122, 333–362. [Google Scholar] [CrossRef]
- Sylvester, O.; Segura, A.G.; Davidson-Hunt, I.J. Wild food harvesting and access by household and generation in the Talamanca Bribri Indigenous Territory, Costa Rica. Hum. Ecol. 2016, 44, 449–461. [Google Scholar] [CrossRef]
- Arruda, H.L.S.; Santos, J.F.O.; Albuquerque, U.P.; Ramos, M.A. Influence of Socioeconomic Factors on the Knowledge and Consumption of Firewood in the Atlantic Forest of Northeast Brazil. Econ. Bot. 2019, 73, 1–12. [Google Scholar] [CrossRef]
- Case, R.J.; Pauli, G.F.; Soejarto, D.D. Factors in maintaining indigenous knowledge among ethnic communities of Manus Island. Econ. Bot. 2005, 59, 356–365. [Google Scholar] [CrossRef]
- McMillen, H. Ethnobotanical knowledge transmission and evolution: The case of medicinal markets in Tanga, Tanzania. Econ. Bot. 2012, 66, 121–131. [Google Scholar] [CrossRef]
- Vandebroek, I.; Balick, M.J. Globalization and loss of plant knowledge: Challenging the paradigm. PLoS ONE 2012, 7, e37643. [Google Scholar] [CrossRef] [PubMed]
- Miguéis, G.S.; Da Silva, R.H.; Júnior, G.A.D.; Guarim-Neto, G. Plants used by the rural community of Bananal, Mato Grosso, Brazil: Aspects of popular knowledge. PLoS ONE 2019, 14, e0210488. [Google Scholar] [CrossRef] [PubMed]
- Byg, A.; Balslev, H. Diversity and use of palms in Zahamena, eastern Madagascar. Biodivers. Conserv. 2001, 10, 951–970. [Google Scholar] [CrossRef]
- Singhal, R. Medicinal plants and primary health care: The role of gender. J. Health Manag. 2005, 7, 277–293. [Google Scholar] [CrossRef]
- Signorini, M.A.; Piredda, M.; Bruschi, P. Plants and traditional knowledge: An ethnobotanical investigation on Monte Ortobene (Nuoro, Sardinia). J. Ethnobiol. Ethnomed. 2009, 5, 6. [Google Scholar] [CrossRef] [Green Version]
- Nolan, J.M.; Robbins, M.C. Cultural conservation of medicinal plant use in the Ozarks. Hum. Organ. 1999, 58, 67–72. [Google Scholar] [CrossRef]
- Menendez-Baceta, G.; Pardo-de-Santayana, M.; Aceituno-Mata, L.; Tardío, J.; Reyes-García, V. Trends in wild food plants uses in Gorbeialdea (Basque Country). Appetite 2017, 112, 9–16. [Google Scholar] [CrossRef]
- Paniagua-Zambrana, N.; Cámara-Leret, R.; Bussmann, R.; Macía, M.J. The influence of socioeconomic factors on traditional knowledge: A cross scale comparison of palm use in northwestern South America. Ecol. Soc. 2014, 19, 9. [Google Scholar] [CrossRef] [Green Version]
- Andriamparany, J.N.; Brinkmann, K.; Jeannoda, V.; Buerkert, A. Effects of socio-economic household characteristics on traditional knowledge and usage of wild yams and medicinal plants in the Mahafaly region of south-western Madagascar. J. Ethnobiol. Ethnomed. 2014, 10, 82. [Google Scholar] [CrossRef] [Green Version]
- Mauro, F.; Hardison, P.D. Traditional knowledge of indigenous and local communities: International debate and policy initiatives. Ecol. Appl. 2000, 10, 1263–1269. [Google Scholar] [CrossRef]
- Toda, M.; Salgado, E.L.R.; Masuda, M. Assessing medicinal plants as the linkage between healthcare, livelihood and biodiversity: A case study from native villages surrounding a second-tier city in the central Peruvian Amazon. Tropics 2016, 25, 53–65. [Google Scholar] [CrossRef]
- Bellia, G.; Pieroni, A. Isolated, but transnational: The glocal nature of Waldensian ethnobotany, Western Alps, NW Italy. J. Ethnobiol. Ethnomed. 2015, 11, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leatherman, T.L.; Carey, J.W.; Thomas, R.B. Socioeconomic change and patterns of growth in the Andes. Amer. J. Phys. Anthr. 1995, 97, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Vandebroek, I.; Calewaert, J.B.; Sanca, S.; Semo, L.; Van Damme, P.; Van Puyvelde, L.; De Kimpe, N. Use of medicinal plants and pharmaceuticals by indigenous communities in the Bolivian Andes and Amazon. Bull. World Health Organ. 2004, 82, 243–250. [Google Scholar]
- Sandlos, J.; Keeling, A. Aboriginal communities, traditional knowledge, and the environmental legacies of extractive development in Canada. Extr. Ind. Soc. 2015, 3, 278–287. [Google Scholar] [CrossRef]
- Johnston, A. Indigenous peoples and ecotourism: Bringing indigenous knowledge and rights into the sustainability equation. Tour. Recreat. Res. 2000, 25, 89–96. [Google Scholar] [CrossRef]
- Cotruvo, J.A. WHO Guidelines for Drinking Water Quality: First Addendum to the Fourth Edition. J. Am. Water Work. Assoc. 2017, 109, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Pieroni, A.; Quave, C. Traditional pharmacopoeias and medicines among Albanians and Italians in southern Italy: A comparison. J. Ethnopharmacol. 2005, 101, 258–270. [Google Scholar] [CrossRef]
- Eyssartier, C.; Ladio, A.H.; Lozada, M. Cultural transmission of traditional knowledge in two populations of north-western Patagonia. J. Ethnobiol. Ethnomed. 2008, 4, 25. [Google Scholar] [CrossRef] [Green Version]
- León, B.; Pitman, N.; Roque, J. Introducción a las plantas endémicas del Perú. Rev. Per. Bio. 2006, 13, 9–22. [Google Scholar] [CrossRef] [Green Version]
- SENAMHI (Servicio Nacional de Meteorología e Hidrología). Reporte mensual de Meteorología y Climatología. 2019. Lima, Peru. Available online: https://www.senamhi.gob.pe/?p=descarga-datos-hidrometeorologicos/>/ (accessed on 6 March 2019).
- INEI (Instituto Nacional de Estadística e Informática). Síntesis Estadística 2015. Boletín Especial, N° 18, Septiembre, 2015. Lima: INEI. Available online: https://www.inei.gob.pe/estadisticas/indice-tematico/poblacion-y-vivienda/ (accessed on 10 March 2019).
- Corroto, F.; Torres, O.A.G.; Macía, M.J. Different patterns in medicinal plant use along an elevational gradient in northern Peruvian Andes. J. Ethnopharmacol. 2019, 239, 111924. [Google Scholar] [CrossRef]
- The Plant List: A Working List of All Known Plant Species. 2018. Available online: http://www.theplantlist.org (accessed on 4 December 2018).
- Chase, M.W.; Christenhusz, M.J.M.; Fay, M.F.; Judd, W.S. An update of the Angiosperm Phylogeny Group classification for the orders and families of flowering plants: APG IV. Bot. J. Linn. Soc. 2016, 181, 1–20. [Google Scholar] [CrossRef] [Green Version]
- WONCA. ICPC-2-R: International Classification of Primary Care, 2nd ed.; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Macía, M.J.; Armesilla, P.J.; Cámara-Leret, R.; Paniagua-Zambrana, N.; Villalba, S.; Balslev, H.; Pardo-de-Santayana, M. Palm uses in northwestern South America: A quantitative review. Bot. Rev. 2011, 77, 462–570. [Google Scholar] [CrossRef]
- Gruca, M.; Cámara-Leret, R.; Macía, M.J.; Balslev, H. New categories for traditional medicine in the Economic Botany Data Collection Standard. J. Ethnopharmacol. 2014, 155, 1388–1392. [Google Scholar] [CrossRef]
- Di Rienzo, J.A.; Casanoves, F.; Balzarini, M.G.; Gonzalez, L.; Tablada, M.; Robledo, C.W. InfoStat version 2011. Grupo InfoStat, FCA. 2011. Universidad Nacional de Córdoba, Argentina. Available online: http://www.infostat.com.ar (accessed on 5 November 2018).
- SCBD (Secretariat of the Convention on Biological Diversity). Nagoya Protocol on Access to Genetic Resources and the Fair and Equitable Sharing of Benefits Arising from Their Utilization to the Convention on Biological Diversity; Secretariat of the Convention on Biological Diversity: Montreal, QC, Canada, 2011; pp. 1–15. Available online: https://www.cbd.int/abs/doc/protocol/nagoya-protocol-en.pdf (accessed on 23 March 2020).
- SCBD (Secretariat of the Convention on Biological Diversity). Bonn Guidelines on Access to Genetic Resources and Fair and Equitable Sharing of the Benefits Arising Out of Their Utilization; Secretariat of the Convention on Biological Diversity: Montreal, QC, Canada, 2002; pp. 1–26. Available online: https://www.cbd.int/doc/publications/cbd-bonn-gdls-en.pdf (accessed on 22 March 2020).
Figure 1.
Relationship between socioeconomic factors at the individual level and MPK, measured as the mean of reports of medicinal usage gathered in 12 localities of the northern Peruvian Andes.
Figure 1.
Relationship between socioeconomic factors at the individual level and MPK, measured as the mean of reports of medicinal usage gathered in 12 localities of the northern Peruvian Andes.

Figure 2.
Relationship between socioeconomic factors at the family level and MPK, measured as the mean of reports of medicinal usage gathered from participants in 12 localities of the northern Peruvian Andes.
Figure 2.
Relationship between socioeconomic factors at the family level and MPK, measured as the mean of reports of medicinal usage gathered from participants in 12 localities of the northern Peruvian Andes.

Figure 3.
Nonmetric multidimensional scaling (NMDS) ordination showing the similarity of the 18 socioeconomic factors influencing MPK (means of reports of medicinal usage) for the eight most cited medicinal categories in 12 localities of the northern Peruvian Andes. Symbols indicate the different provinces, as follow: Lowlands: Bongará (■) and Rodríguez de Mendoza (□). Highlands: Chachapoyas (●) and Luya (○).
Figure 3.
Nonmetric multidimensional scaling (NMDS) ordination showing the similarity of the 18 socioeconomic factors influencing MPK (means of reports of medicinal usage) for the eight most cited medicinal categories in 12 localities of the northern Peruvian Andes. Symbols indicate the different provinces, as follow: Lowlands: Bongará (■) and Rodríguez de Mendoza (□). Highlands: Chachapoyas (●) and Luya (○).

Figure 4.
Map of the study area in the northern Peruvian Andes, showing the two ecoregions (highlands and lowlands), the four provinces, and the 12 localities where information about medicinal plants uses and socioeconomic factors was obtained via 600 interviews.
Figure 4.
Map of the study area in the northern Peruvian Andes, showing the two ecoregions (highlands and lowlands), the four provinces, and the 12 localities where information about medicinal plants uses and socioeconomic factors was obtained via 600 interviews.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Mean (± standard deviation) values of the number of medicinal plant species and the reported usage of medicinal plants, based on information gathered from participants and mean Pearson correlation statistics for two socioeconomic variables and MPK (based on the reported uses). We carried out 600 interviews in 12 localities of the Peruvian Andes.
Table 1.
Mean (± standard deviation) values of the number of medicinal plant species and the reported usage of medicinal plants, based on information gathered from participants and mean Pearson correlation statistics for two socioeconomic variables and MPK (based on the reported uses). We carried out 600 interviews in 12 localities of the Peruvian Andes.
| Ecoregion—Province | Locality | # Medicinal Species | # Medicinal Plant Usage | Age | Family Size |
|---|---|---|---|---|---|
| Lowlands—Bongará | Cuispes | 19.4 ± 6.4 | 22.2 ± 7.1 | 0.08 | 0.14 |
| San Carlos | 22.0 ± 5.8 | 24.6 ± 7.9 | 0.17 | 0.03 | |
| Valera | 9.6 ± 3.6 | 10.8 ± 4.5 | 0.14 | 0.28 | |
| Lowlands—R. Mendoza | Huambo | 10.6 ± 3.9 | 12.3 ± 4.1 | 0.24 | 0.04 |
| Santa Rosa | 13.1 ± 4.0 | 13.8 ± 4.2 | 0.15 | 0.19 | |
| Totora | 18.5 ± 4.4 | 20.8 ± 5.2 | 0.09 | 0.14 | |
| Highlands—Chachapoyas | Granada | 26.9 ± 7.8 | 34.8 ± 8.9 | 0.23 | 0.28 |
| Olleros | 27.2 ± 7.3 | 35.1 ± 7.8 | 0.29 | 0.09 | |
| Quinjalca | 26.8 ± 7.5 | 31.8 ± 7.6 | 0.06 | 0.11 | |
| Highlands—Luya | Longuita | 22.4 ± 6.6 | 26.2 ± 7.1 | 0.12 | 0.13 |
| María | 19.0 ± 5.9 | 22.3 ± 6.6 | 0.12 | 0.25 | |
| Yomblón | 20.1 ± 6.0 | 23.1 ± 6.8 | 0.19 | 0.18 |
Table 2.
Relationship between socioeconomic factors at the locality level and MPK, measured as mean (± standard deviation) of reports of medicinal usage gathered from participants in 12 localities of the northern Peruvian Andes. The impact of the distinct socioeconomic factors per locality was classified at three levels (high, medium, and low), depending on the proximity to the analyzed factor and the availability of chlorinated water.
Table 2.
Relationship between socioeconomic factors at the locality level and MPK, measured as mean (± standard deviation) of reports of medicinal usage gathered from participants in 12 localities of the northern Peruvian Andes. The impact of the distinct socioeconomic factors per locality was classified at three levels (high, medium, and low), depending on the proximity to the analyzed factor and the availability of chlorinated water.
| Attributes | High | Medium | Low |
|---|---|---|---|
| Proximity of tourist attractions | 19.7 ± 6.4 | 23.4 ± 7.2 | 30.1 ± 8.4 |
| Proximity to paved roads | 19.1 ± 6.7 | 19.2 ± 6.4 | 31.2 ± 8.2 |
| Proximity to hospitals | 15.6 ± 5.4 | 21.2 ± 6.8 | 31.2 ± 8.2 |
| Proximity to big markets | 17.4 ± 5.6 | 24.2 ± 7.5 | 31.2 ± 8.2 |
| Chlorination of drinking water | 18.9 ± 6.1 | – | 29.1 ± 8.0 |
Table 3.
Mixed-model effects of the number of reports of medicinal use and coefficients of the socioeconomic factors evaluated in 12 localities of northern Peruvian Andes. Levels of significance: * p < 0.05; ** p < 0.01; nd: no data.
Table 3.
Mixed-model effects of the number of reports of medicinal use and coefficients of the socioeconomic factors evaluated in 12 localities of northern Peruvian Andes. Levels of significance: * p < 0.05; ** p < 0.01; nd: no data.
| Attributes | Lowlands—Bongará | Lowlands—Mendoza | Highlands—Chachapoyas | Highlands—Luya | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cuispes | San Carlos | Valera | Huambo | Santa Rosa | Totora | Granada | Olleros | Quinjalca | Longuita | María | Yomblón | |
| Intercept | 45.462 | 24.553 | 35.234 ** | 11.791 | 23.797 | 34.316 * | 37.979 | 24.263 | 11.641 | 19.558 | 42.486 | 23.159 |
| Women | 1.245 | 3.244 ** | 2.506 * | 0.821 | 1.109 | 2.068 * | 1.110 | 1.080 | 2.471 * | 0.809 | 0.908 | 0.859 |
| Education | 1.077 | −3.618 * | 0.714 | −1.752 | −4.291 ** | −2.662 * | −0.580 | 0.490 | 0.520 | −1.532 | −0.400 | −3.246 * |
| Occupation | 1.012 | −4.783 ** | −1.527 | 0.206 | −4.935 ** | −1.672 | nd | 0.919 | −0.353 | −1.992 | −0.506 | 0.065 |
| Migratory status | −0.373 | −0.348 | −0.161 | 0.508 | 0.422 | 0.534 | −0.161 | −1.029 | −0.015 | −3.347 * | −1.656 | −0.107 |
| Time-in-residence | 0.927 | 0.791 | 0.734 | 0.839 | 0.248 | 1.449 | 0.811 | 1.599 | −0.143 | 2.471 * | 1.711 | 2.124 * |
| Family size | 0.697 | 0.409 | 0.218 | 0.703 | 1.405 | 0.616 | 2.072 * | 2.782 * | 0.979 | 1.405 | 0.779 | 3.271 * |
| Transport | 0.863 | 0.919 | −0.969 | −0.389 | −0.835 | −2.138 * | 0.753 | −0.536 | 0.767 | −1.596 | −0.901 | −1.528 |
| Tools | −3.927 * | −1.207 | −4.768 * | −0.361 | −0.738 | −0.424 | −4.284 * | −8.122 ** | 0.326 | 0.951 | 1.298 | −0.966 |
| Technologic access | −0.406 | −0.073 | −1.589 | −1.771 * | −2.741 ** | 0.053 | −2.195 * | −0.252 | −1.055 | 0.857 | −0.238 | −0.548 |
| Locality | 8.682 | 5.466 | 6.022 | 4.440 | 8.212 | 6.799 | 6.245 | 3.599 | 2.421 | 3.328 | 7.056 | 5.592 |
| Interviewed residuals | 6.324 | 3.026 | 4.073 | 1.893 | 5.889 | 3.802 | 3.935 | 1.447 | 0.971 | 1.722 | 4.800 | 3.232 |
Table 4.
Socioeconomic characteristics of the two studied ecoregions in the tropical montane areas of the northern Peruvian Andes. The population data were obtained from the Instituto Nacional de Estadística e Informática (INEI) [54] and referred to the number of inhabitants per province.
Table 4.
Socioeconomic characteristics of the two studied ecoregions in the tropical montane areas of the northern Peruvian Andes. The population data were obtained from the Instituto Nacional de Estadística e Informática (INEI) [54] and referred to the number of inhabitants per province.
| Attributes | Bongará (Lowlands) | R. Mendoza (Lowlands) | Chachapoyas (Highlands) | Luya (Highlands) |
|---|---|---|---|---|
| Agriculture | Subsistence agriculture (corn, fruit trees, and pasture) | Predominance of productive coffee | Predominance of productive Andean tubers, corn, and pasture | Predominance of productive Andean tubers, corn, and pasture |
| Livestock | Extensive subsistence cattle | Intensive bovine cattle and swine | Extensive subsistence cattle | Extensive subsistence cattle |
| Fisheries | Small-scale trout farms | Fishing in rivers | Small-scale trout farms | Small-scale trout farms |
| Tourist attractions | Yes | No | No | Yes |
| Paved roads | No | Yes | No | Yes |
| Hospitals | No | Yes | No | No |
| Big markets | Yes | Yes | No | Yes |
| Water chlorination | Yes | Yes | No | Yes |
| Population | 2588 | 3277 | 1034 | 1991 |
Table 5.
Description of the 18 socioeconomic variables for which data were obtained from 600 interviews in 12 localities of the northern Peruvian Andes.
Table 5.
Description of the 18 socioeconomic variables for which data were obtained from 600 interviews in 12 localities of the northern Peruvian Andes.
| Independent Variable Name | Variable Scale | Variable Type | Variable Classification |
|---|---|---|---|
| Gender | Individual | Nominal | (0) Men; (1) Women |
| Age (years) | Individual | Continuous | Between 18 and 91 |
| Education | Individual | Ordinal | (0) No education; (1) Primary education; (2) High education |
| Occupation | Individual | Ordinal | (0) Basic qualification; (1) Medium/High qualifiation |
| Migratory status | Individual | Ordinal | (0) Non-migrant; (1) Migrant |
| Time-in-residence | Individual | Ordinal | (0) Between 0–15 years; (1) Between 16–30 years; (2) More than 30 years |
| Family size | Familiar | Continuous | Between 0–11 children |
| Means of transport | Familiar | Ordinal | (0) No transport; (1) Animal and bicycle; (2) Motorbike, car, or similar |
| Tools | Familiar | Ordinal | (0) No tools; (1) Basic tools; (2) Semi-automatic tools |
| Technological services | Familiar | Ordinal | (0) Radio, mobile phone, TV; (1) Cable TV; (2) Internet |
| Farm animals | Familiar | Ordinal | (0) No animals; (1) 1–15 animals; (2) >15 animals |
| Farm size | Familiar | Ordinal | (0) 0–1 ha; (1) 1–5 ha; (2) >5 ha |
| House quality | Familiar | Ordinal | (0) Some defects; (1) Good quality, no defects |
| Proximity to tourist attractions | Locality | Ordinal | (0) Less than 1 h; (1) 1–2 h; (2) More than 2 h |
| Proximity to paved roads | Locality | Ordinal | (0) Less than 1 h; (1) 1–2 h; (2) More than 2 h |
| Proximity to hospitals | Locality | Ordinal | (0) Less than 1 h; (1) 1–2 h; (2) More than 2 h |
| Proximity to big markets | Locality | Ordinal | (0) Less than 1 h; (1) 1–2 h; (2) More than 2 h |
| Water quality | Locality | Ordinal | (0) Drinking water with a chlorination system; (1) Unguarded, without a chlorination system |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Corroto, F.; Gamarra Torres, O.A.; Macía, M.J. Understanding the Influence of Socioeconomic Variables on Medicinal Plant Knowledge in the Peruvian Andes. Plants 2022, 11, 2681. https://doi.org/10.3390/plants11202681
AMA Style
Corroto F, Gamarra Torres OA, Macía MJ. Understanding the Influence of Socioeconomic Variables on Medicinal Plant Knowledge in the Peruvian Andes. Plants. 2022; 11(20):2681. https://doi.org/10.3390/plants11202681
Chicago/Turabian StyleCorroto, Fernando, Oscar Andrés Gamarra Torres, and Manuel J. Macía. 2022. "Understanding the Influence of Socioeconomic Variables on Medicinal Plant Knowledge in the Peruvian Andes" Plants 11, no. 20: 2681. https://doi.org/10.3390/plants11202681
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.