
Development, Feasibility, Impact and Acceptability of a Community Pharmacy-Based Diabetes Care Plan in a Low–Middle-Income Country

Abstract
:1. Introduction
2. Materials and Methods
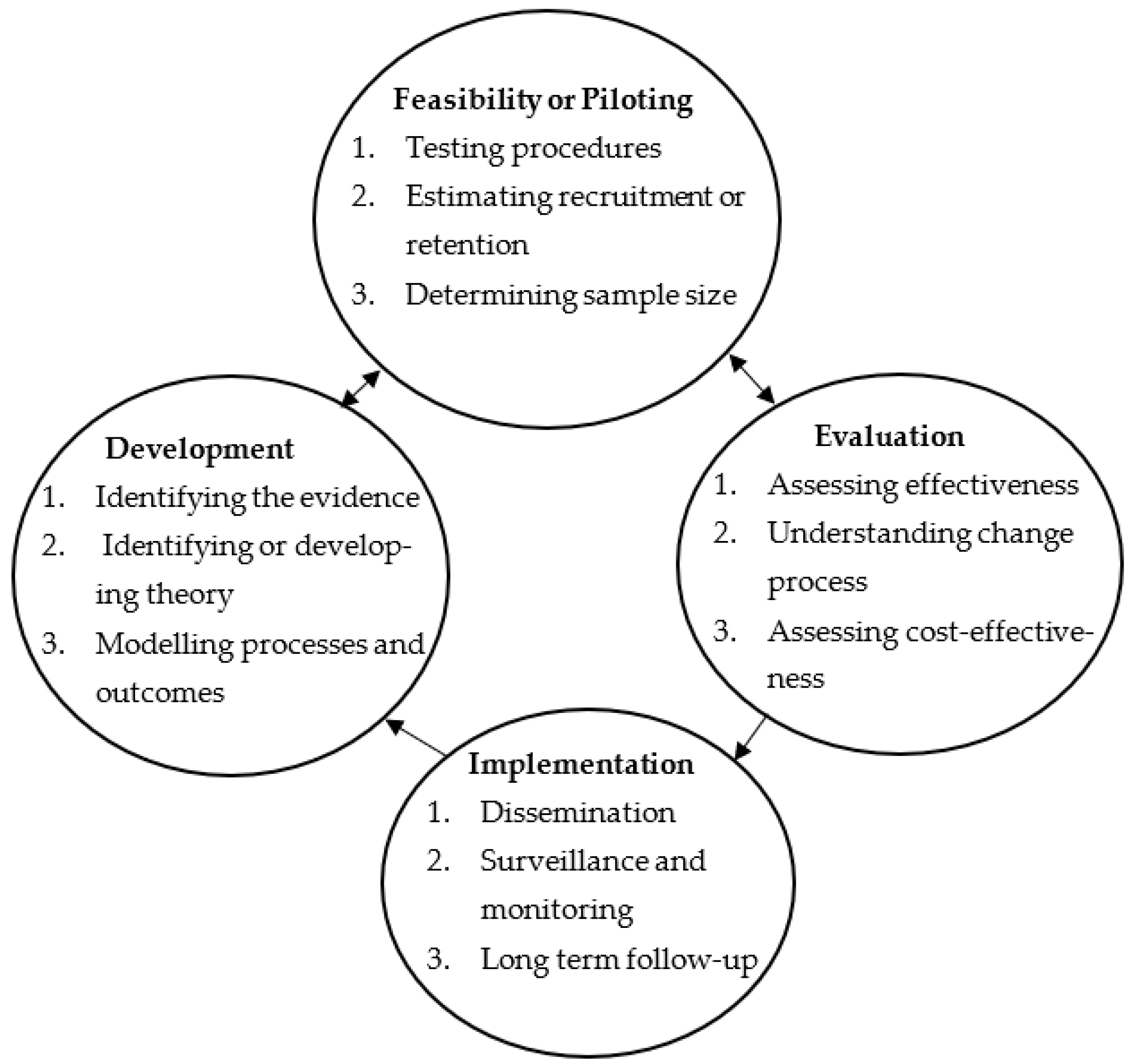
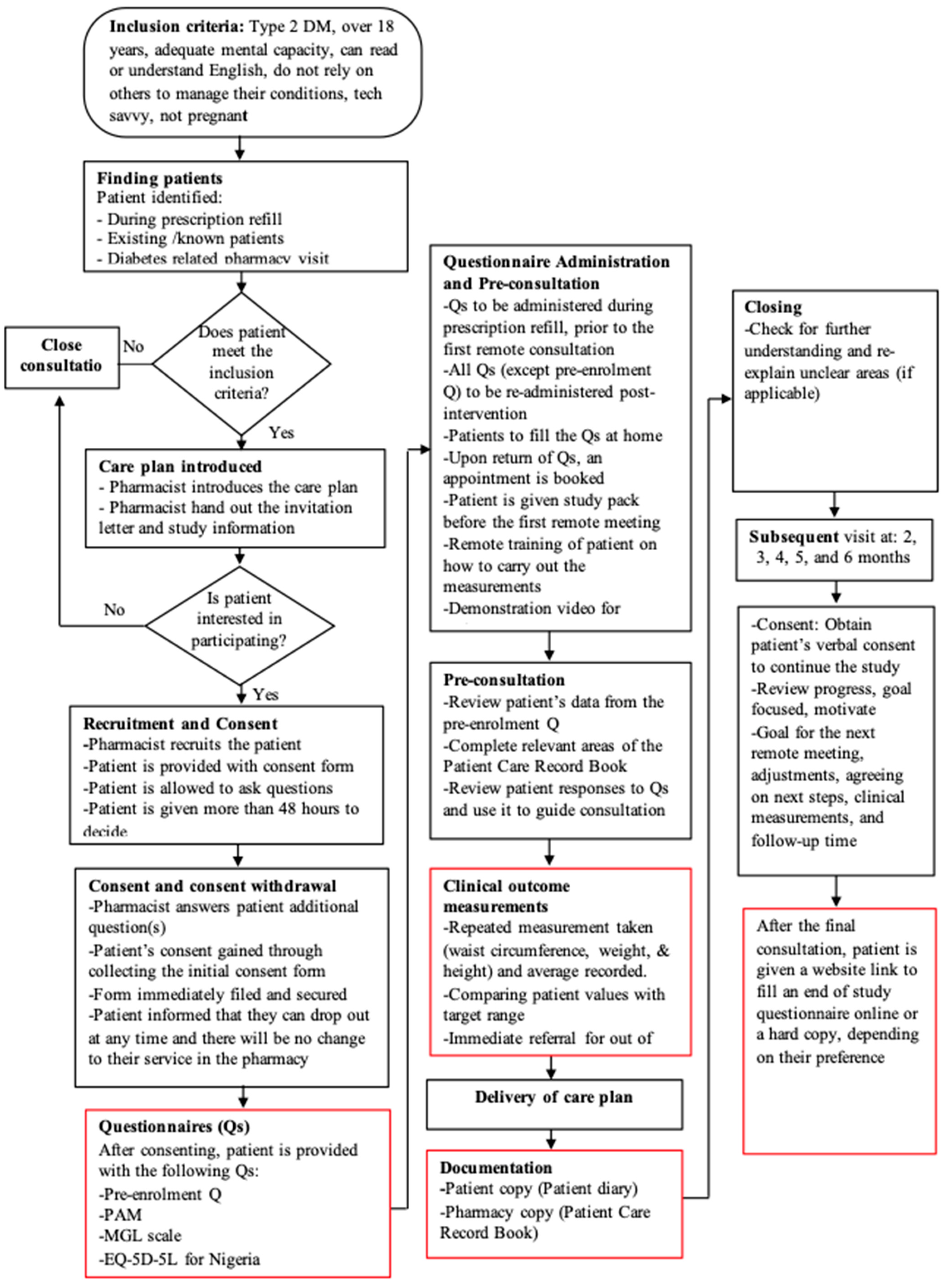
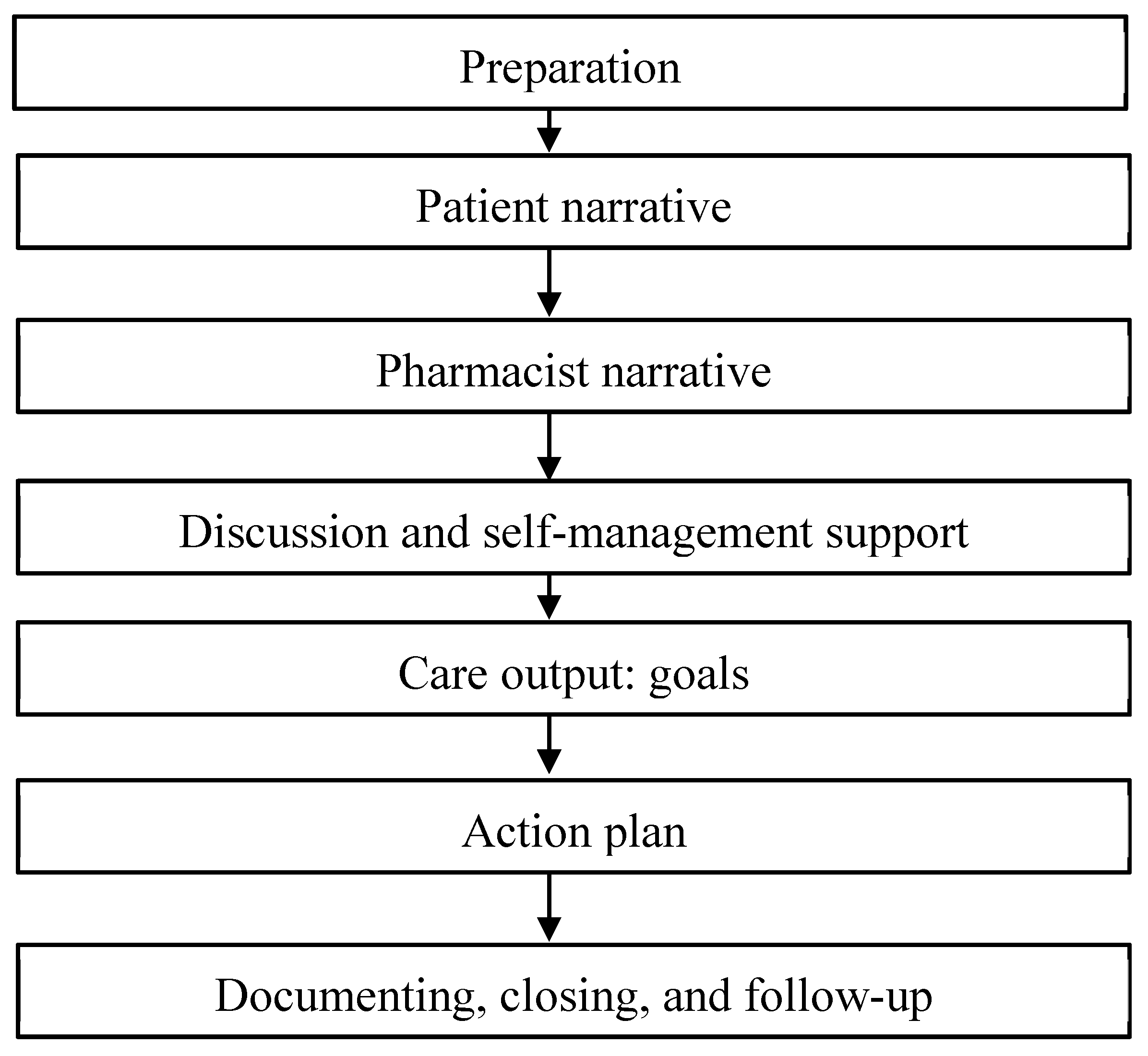
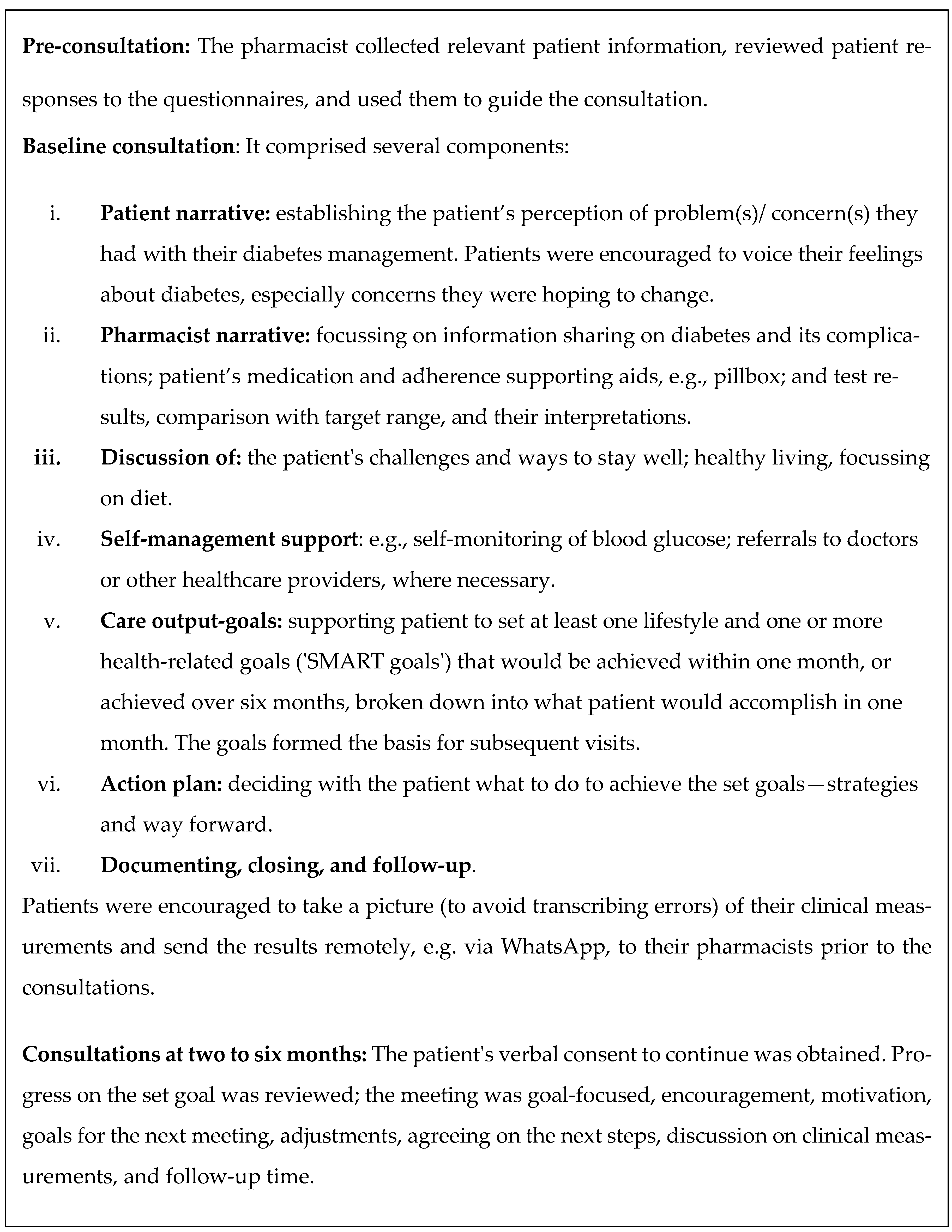
2.1. Intervention Development and Implementation
2.2. Feasibility
2.3. Data Collection Methods for Intervention Evaluation
2.4. Data Sharing and Analysis
3. Results
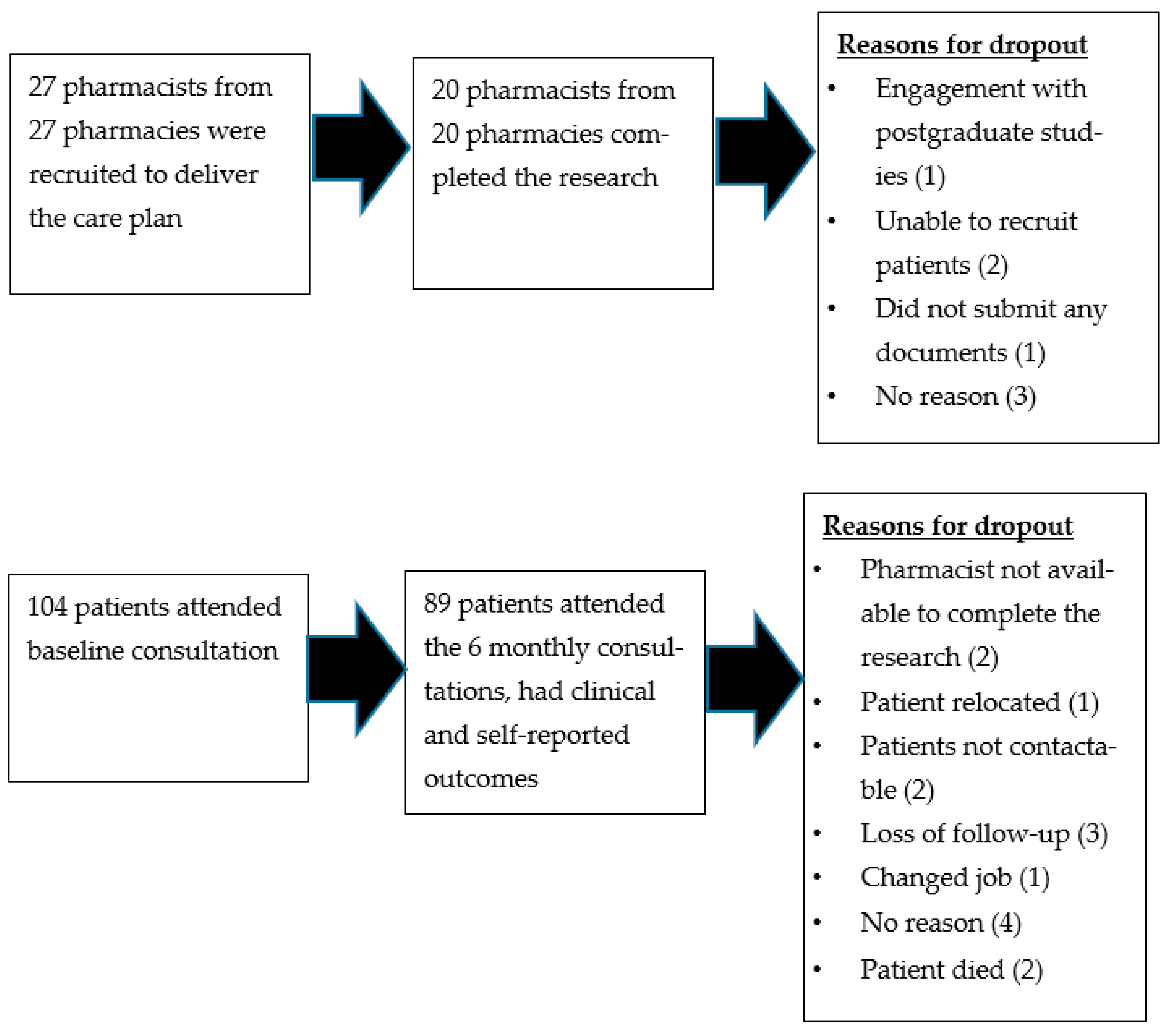
3.1. Recruitment and Response Rates
3.2. Characteristics of Enrolled Patients
3.3. Interviewees’ Socio-Demographic Details
3.4. Self-Reported and Clinical Outcome Measures
3.5. Acceptability and Usefulness of the Diabetes Care Plan
3.5.1. Interviews
“I joined the research because I am passionate about patient care. People living with diabetes need special care; some believe that having diabetes is a life sentence. I will acquire more knowledge and still help to debunk that myth about diabetes.”Pharmacist 7
“I recommend this service to everyone because it is not all the time that one would want to go to the hospital. […] It’s always good to have a professional that one can talk to, maybe about fear or anxiety or whatever. It helps a lot and is comforting. I am always looking forward to the end of month discussion with the pharmacist because it was beneficial. Reviewing my measurements and goals together and discussing my health has been comforting.”Patient 11
“Personally, maybe it’s just for me personally, but timing is a big issue and getting a hold of the participants. Sometimes you plan your time schedule, and they have their own schedule as well, and sometimes they don’t just fall into your plan. And a lot of times, I don’t know if it’s because it’s calls… remote meetings, but they seem to always want it out of hours.”Pharmacist 5
“That (remote consultation) was also a very good one because as much as for us in the pharmacy here, yes, we had some of our clients that were walk-in clients, but we had some geriatric clients also who can’t... don’t come as often as possible. So, the remote consultations came in very handy. So, we were able to communicate with them as much as possible…”Pharmacist 2
“Yea, it is the first of its kind, at least to the best of my knowledge within this community. You know, picking up your phone and consulting with a diabetic patient. They were very happy about that, and it is something that one should consider because we are used to this physical consultation, but suddenly, there is this pandemic, and it has made everyone get used to doing some things virtual.”Pharmacist 10
“This programme has impacted me, and I now know that having diabetes is not a life sentence. It has also given me some skills and has helped to improve my confidence in managing my diabetes. Confidence is very important because sometimes, having diabetes can lead to feeling inferior. I don’t struggle with the inferiority anymore. That confidence is there. I am grateful to the pharmacist and the research team.”Patient 01
“… I allow them to set their goals, to decide their goals by themselves. I would have explained to them where they are, what they can do to get to where they are supposed to be and the consequences of their decisions. I also educate them on how complications can develop. I let them know that the ability to get to where they want is in their own hands, and they are to decide for themselves. More of discussion and putting the ball in their court. Then I follow-up”Pharmacist 9
3.5.2. Post-Study Questionnaire (PSQ)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association Professional Practice Committee. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2022. Diabetes Care 2021, 45 (Suppl. 1), S17–S38. [Google Scholar]
- Bellou, V.; Belbasis, L.; Tzoulaki, I.; Evangelou, E. Risk Factors for Type 2 Diabetes Mellitus: An Exposure-Wide Umbrella Review of Meta-Analyses. PLoS ONE 2018, 13, e0194127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, B.; Gulanick, M.; Lamendola, C. Risk Factors Type 2 Diabetes Mellitus. J. Cardiovasc. Nurs. 2002, 16, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Wing, R.R.; Goldstein, M.G.; Acton, K.J.; Birch, L.L.; Jakicic, J.M.; Sallis, J.F.; Smith-West, D.; Jeffery, R.W.; Surwit, R.S. Behavioral Science Research in Diabetes: Lifestyle Changes Related to Obesity, Eating Behavior, and Physical Activity. Diabetes Care 2001, 24, 117–123. [Google Scholar] [CrossRef] [Green Version]
- Fasanmade, O.A.; Dagogo-Jack, S. Diabetes Care in Nigeria. Ann. Glob. Health 2016, 81, 821–829. [Google Scholar] [CrossRef]
- Adeloye, D.; Ige, J.O.; Aderemi, A.V.; Adeleye, N.; Amoo, E.O.; Auta, A.; Oni, G. Estimating the Prevalence, Hospitalisation and Mortality from Type 2 Diabetes Mellitus in Nigeria: A Systematic Review and Meta-Analysis. BMJ Open 2017, 7, e015424. [Google Scholar] [CrossRef]
- The World Bank. Open Data. 2022. Available online: https://data.worldbank.org/indicator (accessed on 9 December 2022).
- Guariguata, L.; Guariguata, L.; Whiting, D.R.; Hambleton, I.; Beagley, J.; Linnenkamp, U.; Shaw, J.E. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res. Clin. Pract. 2014, 103, 137–149. [Google Scholar] [CrossRef]
- World Health Organization. Preventing Chronic Diseases: A Vital Investment; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Anderson, B.; Funnel, M.M. The Art of Empowerment: Stories and Strategies for Diabetes Educators; American Diabetes Association: Alexandria, VA, USA, 2005. [Google Scholar]
- Coulter, A.; Roberts, S.; Dixon, A. Delivering Better Services for People with Long-Term Conditions: Building the House of Care; The King’s Fund: London, UK, 2013; pp. 1–28. [Google Scholar]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach: Update to a Position Statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2014, 38, 140–149. [Google Scholar] [CrossRef] [Green Version]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of Hyperglycemia in Type 2 Diabetes: A Patient-Centered Approach: Position Statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2012, 35, 1364–1379. [Google Scholar] [CrossRef] [Green Version]
- El-Shirbiny, D. Person-Centred Care. In Tackling Causes and Consequences of Health Inequalities; CRC Press: Boca Raton, FL, USA, 2020; pp. 147–152. [Google Scholar]
- Coulter, A.; Entwistle, V.A.; Eccles, A.; Ryan, S.; Shepperd, S.; Perera, R. Personalised care planning for adults with chronic or long-term health conditions. Cochrane Database Syst. Rev. 2015, 2015, CD010523. [Google Scholar] [CrossRef] [Green Version]
- Schafheutle, E.I. Personalised chronic care planning shows limited but promising effects on physical and psychological health and self-management capabilities. BMJ Evid. Based Med. 2015, 20, 172. [Google Scholar] [CrossRef] [PubMed]
- Mikkola, I.; Hagnas, M.; Hartsenko, J.; Kaila, M.; Winell, K. A Personalized Care Plan Is Positively Associated With Better Clinical Outcomes in the Care of Patients With Type 2 Diabetes: A Cross-Sectional Real-Life Study. Can. J. Diabetes 2020, 44, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Glenn, L.E.; Nichols, M.; Enriquez, M.; Jenkins, C. Impact of a Community-based Approach to Patient Engagement in Rural, Low-income Adults with Type 2 Diabetes. Public Health Nurs. 2020, 37, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Sacks, R.M.; Greene, J.; Hibbard, J.; Overton, V.; Parrotta, C.D. Does Patient Activation Predict the Course of Type 2 Diabetes? A Longitudinal Study. Patient Educ. Couns. 2017, 100, 1268–1275. [Google Scholar] [CrossRef]
- Hibbard, J.; Gilburt, H. Supporting People to Manage their Health: An Introduction to Patient Activation; The King’s Fund: London, UK, 2014; pp. 1–54. [Google Scholar]
- Hibbard, J.H.; Mahoney, E.R.; Stockard, J.; Tusler, M. Development and testing of a short form of the patient activation measure. Health Serv. Res. 2005, 40, 1918–1930. [Google Scholar] [CrossRef] [Green Version]
- Al Hamarneh, Y.N.; Hemmelgarn, B.R.; Hassan, I.; Jones, C.A.; Tsuyuki, R.T. The Effectiveness of Pharmacist Interventions on Cardiovascular Risk in Adult Patients with Type 2 Diabetes: The Multicentre Randomized Controlled RxEACH Trial. Can. J. Diabetes 2017, 41, 580–586. [Google Scholar] [CrossRef]
- Hendrie, D.; Miller, T.R.; Woodman, R.J.; Hoti, K.; Hughes, J. Cost-effectiveness of Reducing Glycaemic Episodes Through Community Pharmacy Management of Patients with Type 2 Diabetes Mellitus. J. Prim. Prev. 2014, 35, 439–449. [Google Scholar] [CrossRef]
- Mansell, K.; Blackburn, D.; Taylor, J.; Jiricka, K. Pharmacists Providing Education to Help Optimize Frequency of Self-monitoring of Blood Blucose in Non-insulin Dependent Type 2 Diabetes Mellitus. Can. J. Diabetes 2012, 36, 332–336. [Google Scholar] [CrossRef]
- Mehuys, E.; Van Bortel, L.; De Bolle, L.; Van Tongelen, I.; Annemans, L.; Remon, J.P.; Giri, M. Effectiveness of a Community Pharmacist Intervention in Diabetes Care: A Randomized Controlled trial. J. Clin. Pharm. Ther. 2011, 36, 602–613. [Google Scholar] [CrossRef]
- Twigg, M.J.; Bhattacharya, D.; Desborough, J.A.; Wright, D. A drop-in Clinic for Patients with Poorly-Controlled Diabetes: A Community Pharmacy Feasibility Study. Int. J. Clin. Pharm. 2015, 37, 395–402. [Google Scholar] [CrossRef]
- Seston, E.M.; Magola, E.; Bower, P.; Chen, L.-C.; Jacobs, S.; Lewis, P.J.; Steinke, D.; Willis, S.C.; Schafheutle, E.I. Supporting Patients with Long-term Conditions in the Community: Evaluation of the Greater Manchester Community Pharmacy Care Plan Service. Health Soc. Care Community 2020, 28, 1671–1687. [Google Scholar] [CrossRef] [PubMed]
- Twigg, M.J.; Wright, D.; Barton, G.; Kirkdale, C.L.; Thornley, T. The Pharmacy Care Plan Service: Evaluation and Estimate of Cost-effectiveness. Res. Soc. Adm. Pharm. 2019, 15, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Drake, E.S.; Harris, D.K.; Marciniak, M.W. Community Pharmacist–led Intervention to Identify Persons with Diabetes not on Statin Therapy. J. Am. Pharm. Assoc. 2018, 58 (Suppl. 4), S125–S130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Regina, R.; Pandolfi, D.; Stabile, N.; Beloni, L.; Glisenti, F.; Griggio, P.; La Regina, M.; La Regina, G. A New Case Manager for Diabetic Patients: A Pilot Observational Study of the Role of Community Pharmacists and Pharmacy Services in the Case Management of Diabetic Patients. Pharmacy 2020, 8, 193. [Google Scholar] [CrossRef]
- Ali, M.; Schifano, F.; Robinson, P.; Phillips, G.; Doherty, L.; Melnick, P.; Laming, L.; Sinclair, A.; Dhillon, S. Impact of community pharmacy diabetes monitoring and education programme on diabetes management: A randomized controlled study. Diabet. Med. 2012, 29, e326–e333. [Google Scholar] [CrossRef] [PubMed]
- Kjeldsen, L.J.; Bjerrum, L.; Dam, P.; Larsen, B.O.; Rossing, C.; Søndergaard, B.; Herborg, H. Safe and Effective Use of Medicines for Patients with Type 2 diabetes–a randomized controlled Trial of Two Interventions Delivered by Local Pharmacies. Res. Soc. Adm. Pharm. 2015, 11, 47–62. [Google Scholar] [CrossRef] [PubMed]
- Krass, I.; Armour, C.L.; Mitchell, B.; Brillant, M.; Dienaar, R.; Hughes, J.; Lau, P.; Peterson, G.; Stewart, K.; Taylor, S.; et al. The Pharmacy Diabetes Care Program: Assessment of a Community Pharmacy Diabetes Service Model in Australia. Diabet. Med. 2007, 24, 677–683. [Google Scholar] [CrossRef]
- Cahyaningsih, I.; Lambert, M.; Ochi, T.; Li, F.; Li, X.; Denig, P.; Taxis, K. Community Pharmacist-led Interventions in Patients with Type 2 Diabetes in Low-Income and Middle-Income Countries: A Scoping Review. Res. Soc. Adm. Pharm. 2023. [Google Scholar] [CrossRef]
- Li, H.; Zheng, S.; Liu, F.; Liu, W.; Zhao, R. Fighting against COVID-19: Innovative Strategies for Clinical Pharmacists. Res. Soc. Adm. Pharm. 2021, 17, 1813–1818. [Google Scholar] [CrossRef]
- Merks, P.; Jakubowska, M.; Drelich, E.; Świeczkowski, D.; Bogusz, J.; Bilmin, K.; Sola, K.F.; May, A.; Majchrowska, A.; Koziol, M.; et al. The legal Extension of the Role of Pharmacists in Light of the COVID-19 Global Pandemic. Res. Soc. Adm. Pharm. 2021, 17, 1807–1812. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and Evaluating Complex Interventions: The New Medical Research Council Guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, P.; Petticrew, M. Developing and Evaluating Complex Interventions: Reflections on the 2008 MRC guidance. Int. J. Nurs. Stud. 2013, 50, 585–587. [Google Scholar] [CrossRef] [PubMed]
- Al Hamarneh, Y.N.; Charrois, T.; Lewanczuk, R.; Tsuyuki, R.T. Pharmacist Intervention for Glycaemic Control in the Community (the RxING study). BMJ Open 2013, 3, e003154. [Google Scholar] [CrossRef] [Green Version]
- Krass, I.; Mitchell, B.; Song, Y.J.C.; Stewart, K.; Peterson, G.; Hughes, J.; Smith, L.; White, L.; Armour, C. Diabetes Medication Assistance Service Stage 1: Impact and sustainability of glycaemic and lipids control in patients with Type 2 diabetes. Diabet. Med. 2011, 28, 987. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, B.; Armour, C.; Lee, M.; Song, Y.J.; Stewart, K.; Peterson, G.; Hughes, J.; Smith, L.; Krass, I. Diabetes Medication Assistance Service: The Pharmacist’s Role in Supporting Patient Self-Management of Type 2 Diabetes (T2DM) in Australia. Patient Educ. Couns. 2011, 83, 288–294. [Google Scholar] [CrossRef] [Green Version]
- Redding, D.; Hutchinson, S. Person-Centred Care in 2017–Evidence from Service Users; National Voices: London, UK, 2017. [Google Scholar]
- Miller, E. Person-Centred Care Literature Review; Healthcare Improvement Scotland: Edinburgh, UK, 2021. [Google Scholar]
- Bennett, H.D.; Coleman, E.A.; Parry, C.; Bodenheimer, T.; Chen, E.H. Health Coaching for Patients with Chronic Illness. Fam. Pract. Manag. 2010, 17, 24. [Google Scholar]
- Coulter, A.; Oldham, J.M. Person-centred care: What is it and how do we get there? Future Hosp. J. 2016, 3, 114–116. [Google Scholar] [CrossRef]
- Pharmacy Council of Nigeria. About Pharmacy Council of Nigeria. 2023. Available online: https://www.pcn.gov.ng/ (accessed on 9 February 2023).
- Twigg, M.J.; Wright, D.; Kirkdale, C.L.; Desborough, J.A.; Thornley, T. The UK Pharmacy Care Plan Service: Description, Recruitment and Initial Views on a New Community Pharmacy Intervention. PLoS ONE 2017, 12, e0174500. [Google Scholar] [CrossRef] [Green Version]
- Morisky, D.E.; Green, L.W.; Levine, D.M. Concurrent and Predictive Validity of a self-Reported measure of medication adherence. Med. Care 1986, 24, 67–74. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and Preliminary Testing of the New Five-Level Version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Insignia Health. Patient Activation Measure (PAM) Survey. 2021. Available online: http://www.insigniahealth.com/products/pam-survey (accessed on 9 December 2022).
- Group, T.E. EuroQol-A New Facility for The Measurement of Health-Related Quality of Life. Health Policy 1990, 16, 199–208. [Google Scholar]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Xu, M.; Fralick, D.; Zheng, J.Z.; Wang, B.; Changyong, F.E.N.G. The Differences and Similarities Between Two-Sample T-Test and Paired T-Test. Shanghai Arch. Psychiatry 2017, 29, 184. [Google Scholar]
- Garrett, D.G.; Bluml, B.M. Patient Self-Management Program for Diabetes: First-Year Clinical, Humanistic, and Economic Outcomes. J. Am. Pharm. Assoc. 2005, 45, 130–137. [Google Scholar] [CrossRef] [Green Version]
- Shiyanbola, O.O.; Maurer, M.; Schwerer, L.; Sarkarati, N.; Wen, M.J.; Salihu, E.Y.; Nordin, J.; Xiong, P.; Egbujor, U.M.; Williams, S.D. A Culturally Tailored Diabetes Self-Management Intervention Incorporating Race-Congruent Peer Support to Address Beliefs, Medication Adherence and Diabetes Control in African Americans: A Pilot Feasibility Study. Patient Prefer. Adherence 2022, 16, 2893–2912. [Google Scholar] [CrossRef] [PubMed]
- Shiyanbola, O.O.; Ward, E.C.; Brown, C.M. Utilizing the Common Sense Model to Explore African Americans’ Perception Of Type 2 Diabetes: A Qualitative Study. PLoS ONE 2018, 13, e0207692. [Google Scholar] [CrossRef] [Green Version]
- Fatehi, F.l.; Menon, A.; Bird, D. Diabetes care in the digital era: A synoptic overview. Curr. Diabetes Rep. 2018, 18, 1–8. [Google Scholar] [CrossRef]
- McGrail, K.M.; Ahuja, M.A.; Leaver, C.A. Virtual visits and patient-centered care: Results of a patient survey and observational study. J. Med. Internet Res. 2017, 19, e177. [Google Scholar] [CrossRef] [Green Version]
- Scottish, G. Scotland’s Digital Health and Care Strategy: Enabling, Connecting and Empowering; Government of Scotland: Edinburgh, UK, 2018.
- Gavidia, M. Telehealth during COVID-19: How Hospitals, Healthcare Providers are Optimizing Virtual Care. Am. J. Manag. Care 2020. [Google Scholar]
- Severino, R.; Director, O.C.R. Notification of Enforcement Discretion for Telehealth Remote Communications during the COVID-19 Nationwide Public Health Emergency; US Department of Health & Human Services: Washington, DC, USA, 2020.
- Kovačević, M.; Ćulafić, M.; Vezmar Kovačević, S.; Borjanić, S.; Keleč, B.; Miljković, B.; Amidžić, R. Telepharmacy service experience during the COVID-19 pandemic in the Republic of Srpska, Bosnia and Herzegovina. Health Soc. Care Community 2022, 30, e1639–e1650. [Google Scholar] [CrossRef]
- Car, J.; Koh, G.C.H.; Foong, P.S.; Wang, C.J. Video Consultations in Primary And Specialist Care During the COVID-19 Pandemic and Beyond. BMJ 2020, 371, m3945. [Google Scholar] [CrossRef]
- Austin, Z.; Martin, J.C.; Gregory, P.A. Pharmacy practice in times of civil crisis: The experience of SARS and “the blackout” in Ontario, Canada. Res. Soc. Adm. Pharm. 2007, 3, 320–335. [Google Scholar] [CrossRef] [PubMed]
- Chin, T.W.; Chant, C.; Tanzini, R.; Wells, J. Severe Acute Respiratory Syndrome (SARS): The Pharmacist’s Role. J. Hum. Pharmacol. Drug Ther. 2004, 24, 705–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullen, E.; Smith, G.H.; Irwin, A.N.; Angeles, M. Pandemic H1n1 Influenza Virus: Academy Perspectives on Pharmacy’s Critical Role in Treatment, Prev. Am. Pharm. Assoc. 2009, 49, 728. [Google Scholar] [CrossRef] [PubMed]
- World Bank. A Better Future for All Nigerians: Nigeria Poverty Assessment 2022; World Bank: Washington, DC, USA, 2022. [Google Scholar]
- Cranor, C.W.; Bunting, B.A.; Christensen, D.B. The Asheville Project: Long-term clinical and economic outcomes of a community pharmacy diabetes care program. J. Am. Pharm. Assoc. 2003, 43, 173–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcome | Measurement Process | Time of Measurement | Statistical Analysis |
|---|---|---|---|
| Plasma glucose | Measured with Accucheck Instant® glucometer handed to patients | All consultations | Mean values (and standard deviations) were calculated and comparisons between baseline and study completion were conducted using paired t-test. |
| Weight and height | Measured in pharmacy (if patients do not know) | Height once, weight all consultations | Comparison of mean score at baseline and study completion using paired t-test |
| Waist circumference | Measured by patients using the provided waist measuring tape | All consultations | Comparison of mean score at baseline and study completion using paired t-test |
| Patient activation | PAM-13 [50]: Responses were converted to a scale of 0–100 scale & categorised into 1 of 4 activation levels. | Baseline and on study completion | Paired t-test compared the mean PAM score. |
| Medicine adherence | MGL scale [48]: Respondents answered ‘yes’ or ‘no’ to four negative worded questions—one point score for each positive response and 0 point for a “NO” answer. | Baseline and on study completion | Simple proportion. |
| Quality of life | EQ-5D-5L, EQ-VAS [51]. Five statements in EQ-5D-5L. EQVAS records patient’s self-rated health on a vertical visual analogue scale (0–100), endpoints labelled ‘best imaginable health state’ & ‘worst imaginable health state.’ | Baseline and on study completion | Comparison of mean score at baseline and study completion using paired t test. |
| Variable | Frequency (%) |
|---|---|
| Mean age (SD) | 57 (10) |
| Age category (years) | |
| 30–39 | 3 (3) |
| 40–49 | 15 (17) |
| 50–59 | 41 (46) |
| 60–69 | 17 (19) |
| 70–79 | 12 (13) |
| 80–89 | 1 (1) |
| Duration of diabetes (years) | |
| Less than 5 | 45 (51) |
| 6–10 | 9 (10) |
| 11–15 | 16(18) |
| 16–20 | 5 (6) |
| ≥21 | 14 (16) |
| Other medical conditions | |
| None | 37 (42) |
| Hypertension | 42 (47) |
| COPD/Asthma | 1 (1) |
| Hypertension + Other | 6 (7) |
| Others | 3 (3) |
| Other providers (apart from doctor) involved in patient’s diabetes care? | |
| Yes | 64 (72) |
| No | 25 (28) |
| Pharmacy where diabetes medication was purchased | |
| Hospital Pharmacy | 8 (9) |
| Community Pharmacy | 72 (81) |
| Hospital + Community Pharmacy | 9 (10) |
| Description of pharmacy use | |
| Visit the same pharmacy all the time | 39 (44) |
| Visit variety of pharmacies but one most frequently | 45 (51) |
| Visit variety of pharmacies but none more frequently | 2 (2) |
| Not applicable | 3 (3) |
| Outcome | Population (Baseline, End of Study) | Baseline Mean (SD) | End of Study Mean (SD) | Mean Difference (CI) | p Value |
|---|---|---|---|---|---|
| EQ-VAS score | 89 | 76.0 (13) | 83.0 (12) | 7.3 (9.9, 4.7) | <0.001 |
| PAM Score | 89 | 64.1 (16) | 69.2 ( 18) | 5.1 ( 9.1, 1.2) | 0.0116 |
| BMI (kg/m2) | 89 | 29.4 (4.9) | 28.8 (4.5) | −0.6 (−0.9, −0.3) | <0.001 |
| Waist circumference (cm) | 89 | 99.0 (11.5) | 96.7 (9.8) | −2.3 (−3.4, −1.1) | <0.001 |
| Fasting plasma glucose (mmol/L) | 61 | 7.0 (2.3) | 6.1 (1.3) | −0.9 (−1.4, −0.4) | <0.001 |
| Phys. Activity (mins/week) | 82 | 95.3 (49.6) | 114.8 (47.0) | 19.5 (11.5, 27.5) | <0.001 |
| Outcome | Baseline (n = 89) | End of Study (n = 89) | Statistical Test | p Value |
|---|---|---|---|---|
| High adherence n (%) | 22 (25) | 45 (51) | n/a | n/a |
| Medium adherence n (%) | 51 (57) | 34 (38) | n/a | n/a |
| Low adherence n (%) | 16 (18) | 10 (11) | n/a | n/a |
| Adherence assessment | n/a | n/a | Fisher’s exact | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikolaba, F.S.A.; Schafheutle, E.I.; Steinke, D. Development, Feasibility, Impact and Acceptability of a Community Pharmacy-Based Diabetes Care Plan in a Low–Middle-Income Country. Pharmacy 2023, 11, 109. https://doi.org/10.3390/pharmacy11040109
Ikolaba FSA, Schafheutle EI, Steinke D. Development, Feasibility, Impact and Acceptability of a Community Pharmacy-Based Diabetes Care Plan in a Low–Middle-Income Country. Pharmacy. 2023; 11(4):109. https://doi.org/10.3390/pharmacy11040109
Chicago/Turabian StyleIkolaba, Fatima S. Abdulhakeem, Ellen I. Schafheutle, and Douglas Steinke. 2023. "Development, Feasibility, Impact and Acceptability of a Community Pharmacy-Based Diabetes Care Plan in a Low–Middle-Income Country" Pharmacy 11, no. 4: 109. https://doi.org/10.3390/pharmacy11040109