
Single-Strain Probiotic Lactobacilli for the Treatment of Atopic Dermatitis in Children: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Eligibility Criteria
2.3. Data Extraction and Critical Assessment
2.4. Statistical Analysis
3. Results
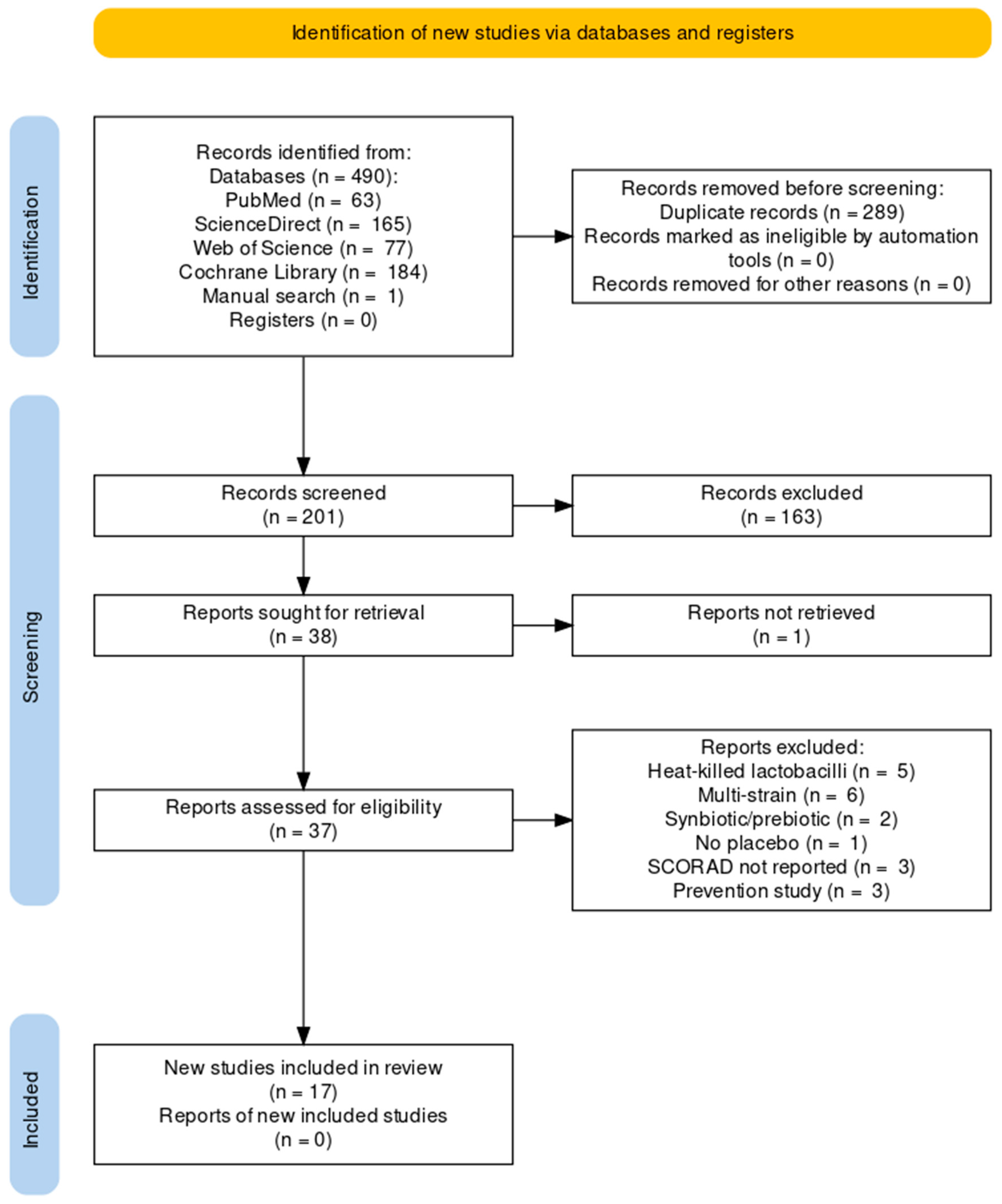
3.1. Study Selection
3.2. Characteristics of the Included Studies
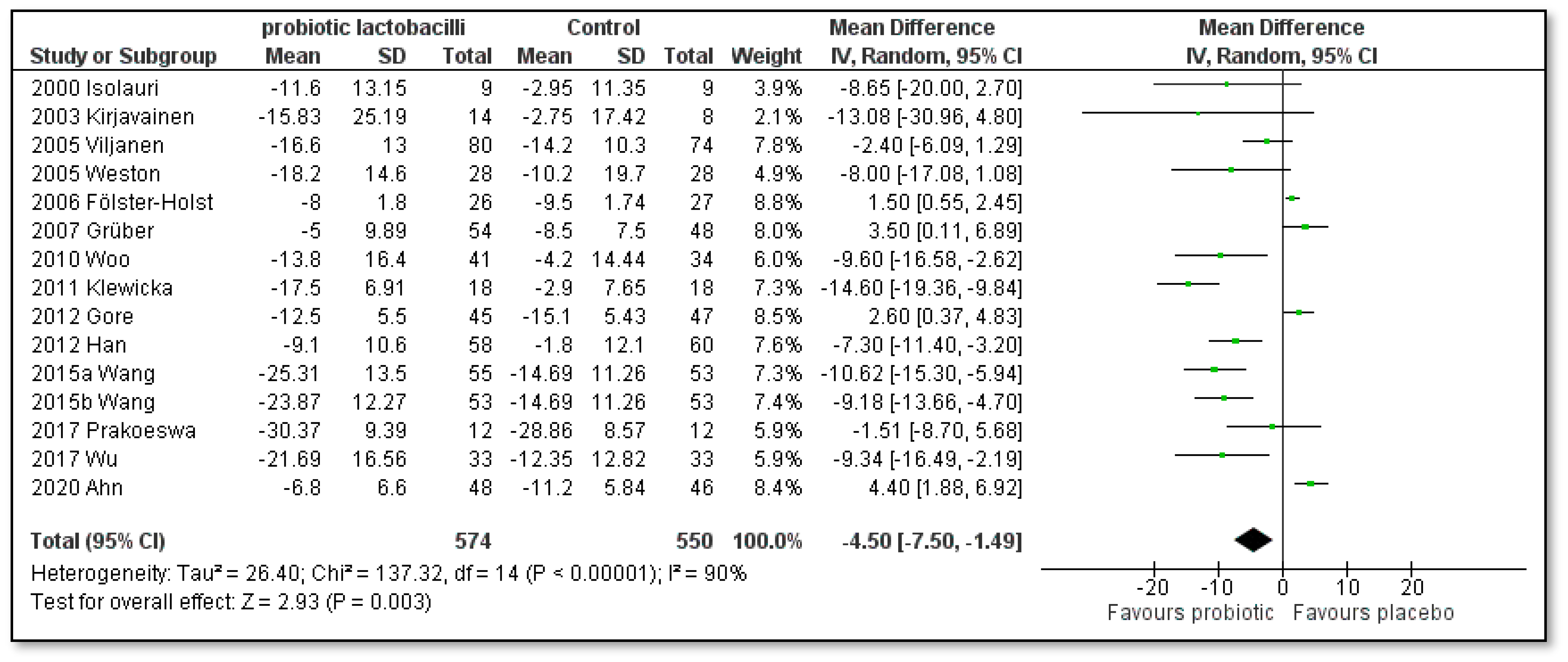
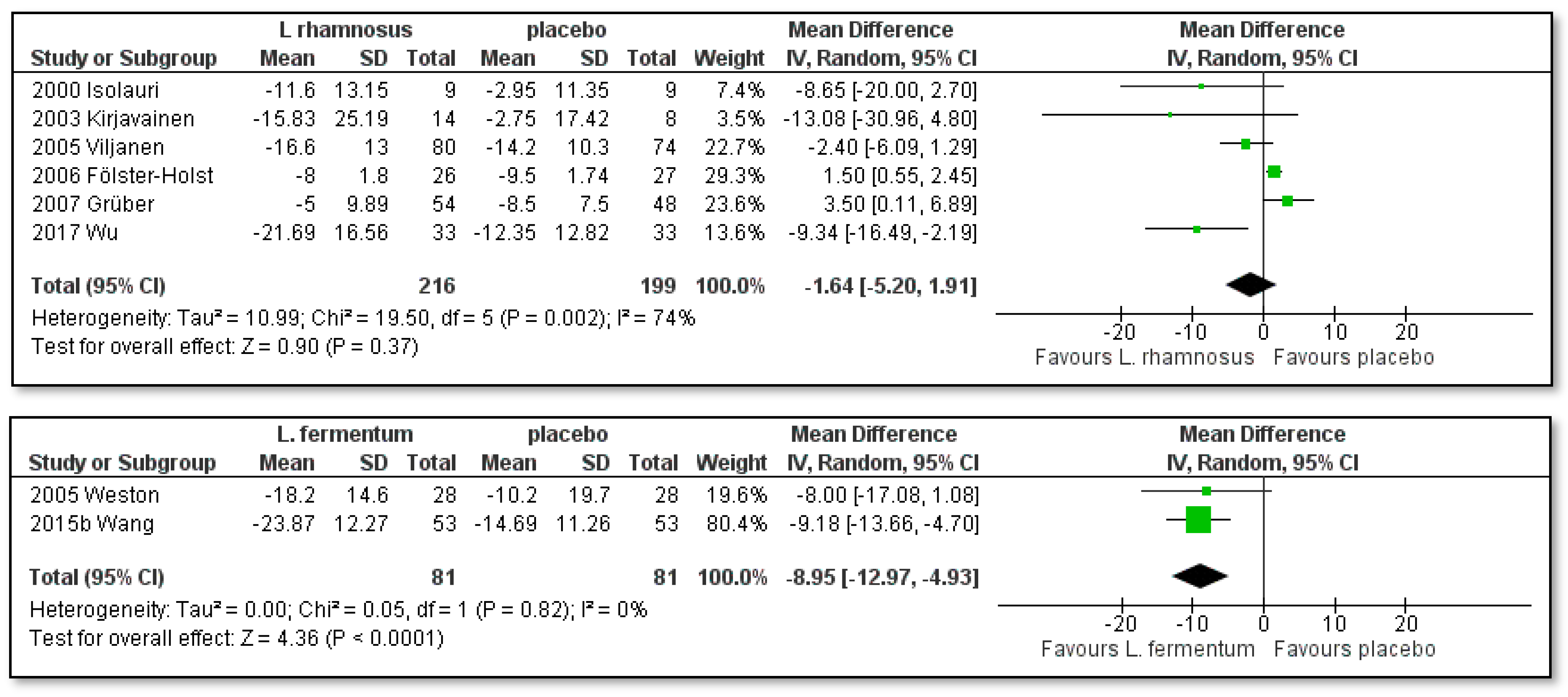
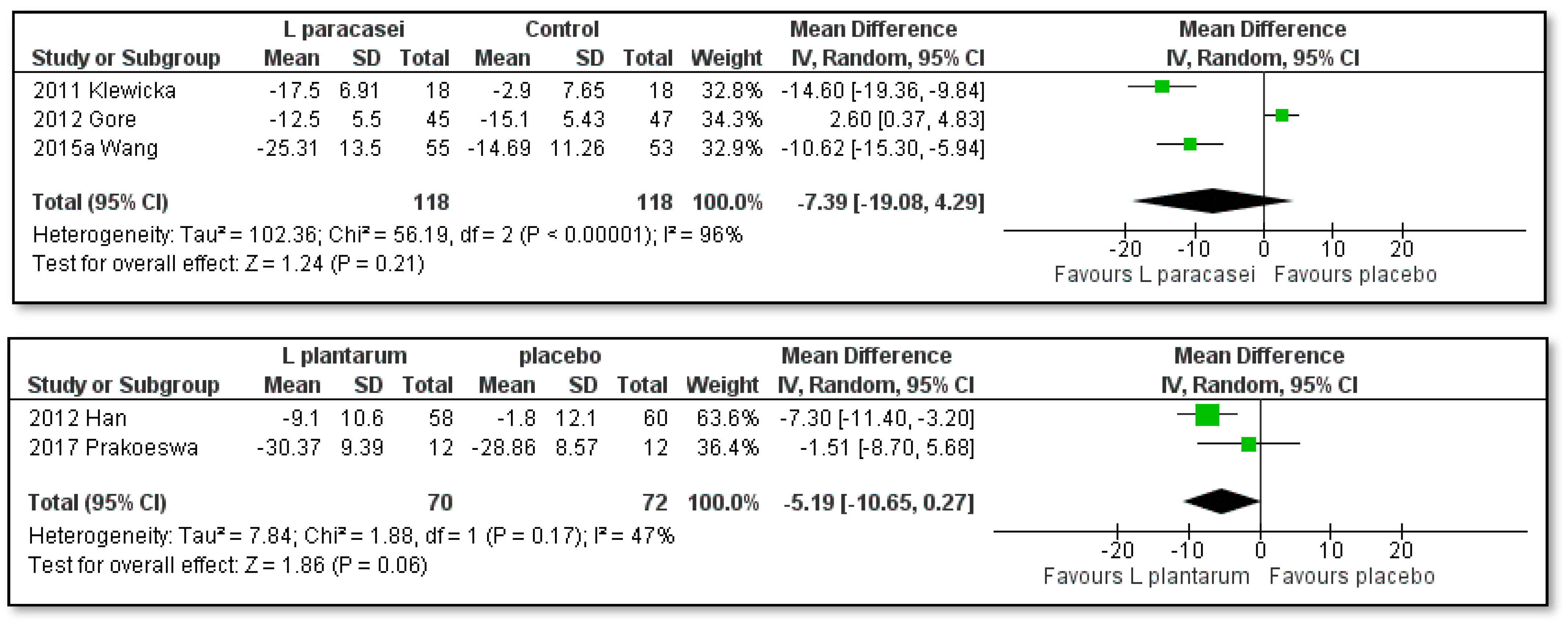
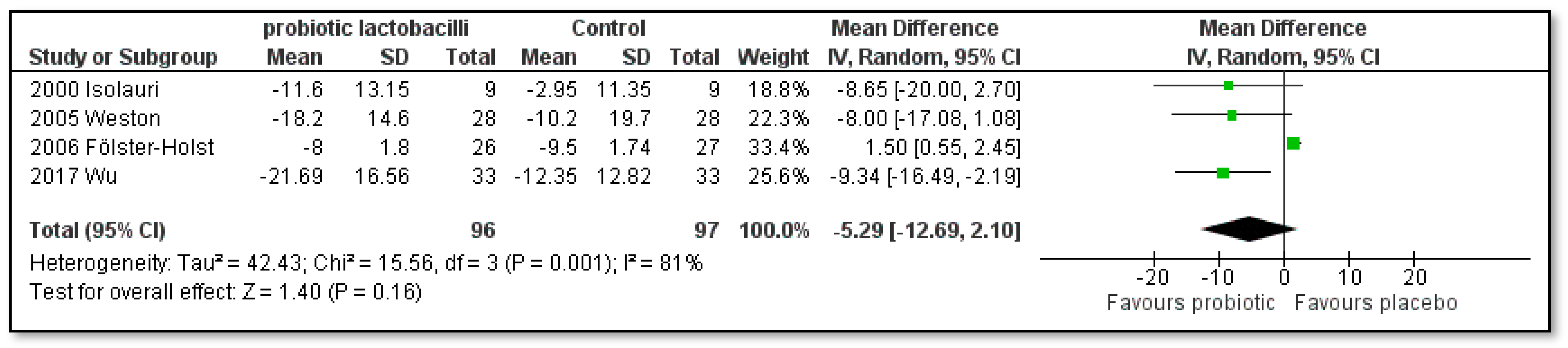
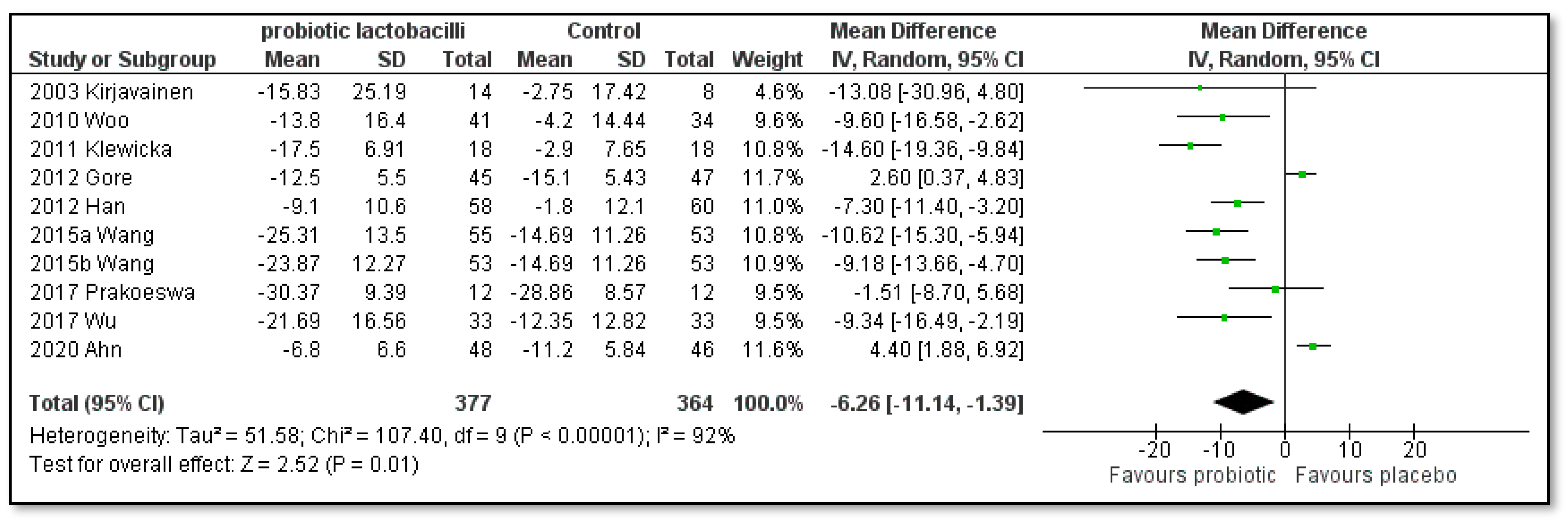
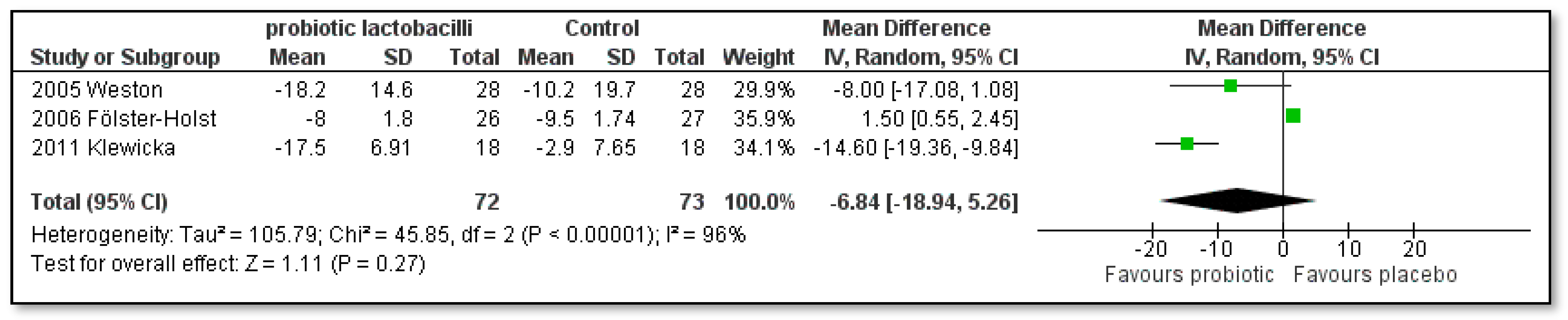
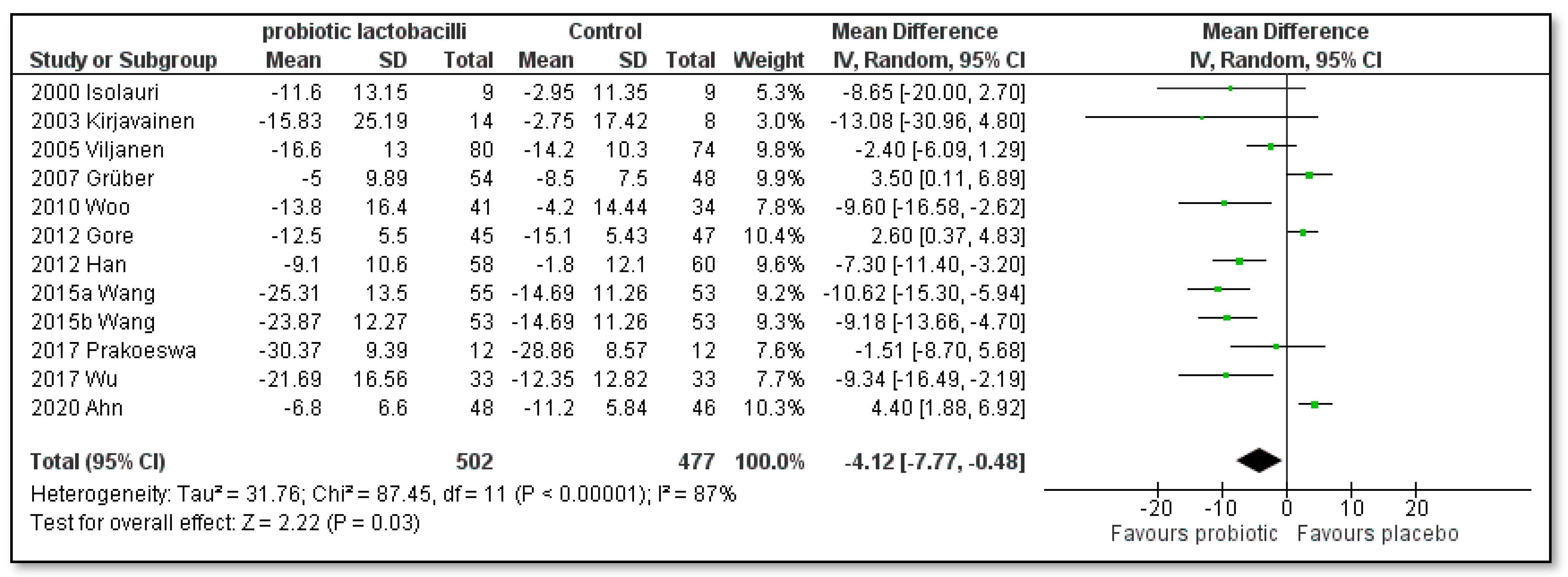
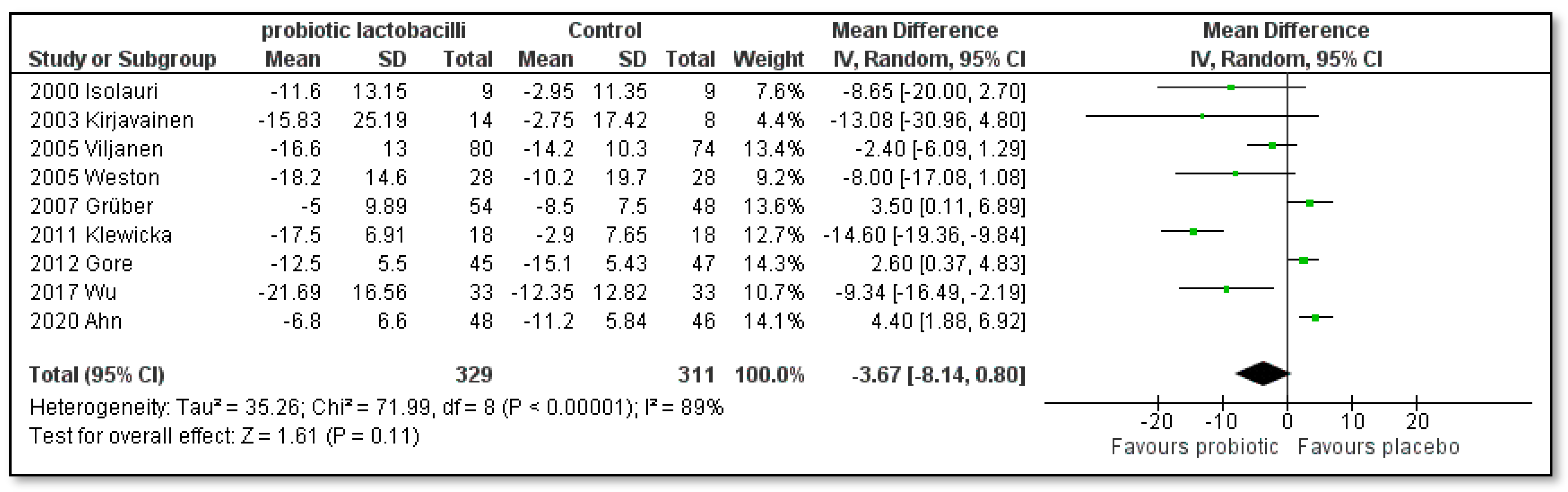
3.3. Meta-Analysis of the Effect of Single-Strain Probiotic Lactobacilli for the Treatment of Atopic Dermatitis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Powers, C.E.; McShane, D.B.; Gilligan, P.H.; Burkhart, C.N.; Morrell, D.S. Microbiome and pediatric atopic dermatitis. J. Dermatol. 2015, 42, 1137–1142. [Google Scholar] [CrossRef]
- Williams, H.C.; Burden-Teh, E. On the definition of dermatological disease. Part 2: Approaches for defining dermatological diseases. Clin. Exp. Dermatol. 2022, 47, 1812–1819. [Google Scholar] [CrossRef]
- Raimondo, A.; Lembo, S. Atopic Dermatitis: Epidemiology and Clinical Phenotypes. Dermatol. Pract. Concept. 2021, 11, e2021146. [Google Scholar] [CrossRef]
- Johnson, H.; Yu, J. Current and Emerging Therapies in Pediatric Atopic Dermatitis. Dermatol. Ther. 2022, 12, 2691–2703. [Google Scholar] [CrossRef] [PubMed]
- Oranje, A.P. Practical issues on interpretation of scoring atopic dermatitis: SCORAD Index, objective SCORAD, patient-oriented SCORAD and Three-Item Severity score. Curr. Probl. Dermatol. 2011, 41, 149–155. [Google Scholar] [CrossRef]
- Chopra, R.; Vakharia, P.P.; Sacotte, R.; Patel, N.; Immaneni, S.; White, T.; Kantor, R.; Hsu, D.Y.; Silverberg, J.I. Severity strata for Eczema Area and Severity Index (EASI), modified EASI, Scoring Atopic Dermatitis (SCORAD), objective SCORAD, Atopic Dermatitis Severity Index and body surface area in adolescents and adults with atopic dermatitis. Br. J. Dermatol. 2017, 177, 1316–1321. [Google Scholar] [CrossRef] [PubMed]
- Oranje, A.P.; Glazenburg, E.J.; Wolkerstorfer, A.; de Waard-van der Spek, F.B. Practical issues on interpretation of scoring atopic dermatitis: The SCORAD index, objective SCORAD and the three-item severity score. Br. J. Dermatol. 2007, 157, 645–648. [Google Scholar] [CrossRef] [PubMed]
- Shi, B.; Bangayan, N.J.; Curd, E.; Taylor, P.A.; Gallo, R.L.; Leung, D.Y.M.; Li, H. The skin microbiome is different in pediatric versus adult atopic dermatitis. J. Allergy Clin. Immunol. 2016, 138, 1233–1236. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Sicherer, S.H. Timing of food introduction and atopy prevention. Clin. Dermatol. 2017, 35, 398–405. [Google Scholar] [CrossRef]
- Arkwright, P.D.; Koplin, J.J. Impact of a Decade of Research into Atopic Dermatitis. J. Allergy Clin. Immunol. Pract. 2022, 11, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Wittouck, S.; Salvetti, E.; Franz, C.; Harris, H.M.B.; Mattarelli, P.; O’Toole, P.W.; Pot, B.; Vandamme, P.; Walter, J.; et al. A taxonomic note on the genus Lactobacillus: Description of 23 novel genera, emended description of the genus Lactobacillus Beijerinck 1901, and union of Lactobacillaceae and Leuconostocaceae. Int. J. Syst. Evol. Microbiol. 2020, 70, 2782–2858. [Google Scholar] [CrossRef] [PubMed]
- Fijan, S. Microorganisms with Claimed Probiotic Properties: An Overview of Recent Literature. Int. J. Environ. Res. Public Health 2014, 11, 4745–4767. [Google Scholar] [CrossRef] [PubMed]
- Fuchs-Tarlovsky, V.; Marquez-Barba, M.F.; Sriram, K. Probiotics in dermatologic practice. Nutrition 2016, 32, 289–295. [Google Scholar] [CrossRef]
- Ganji-Arjenaki, M.; Rafieian-Kopaei, M. Probiotics are a good choice in remission of inflammatory bowel diseases: A meta analysis and systematic review. J. Cell Physiol. 2018, 233, 2091–2103. [Google Scholar] [CrossRef]
- Holte, K.; Krag, A.; Gluud, L.L. Systematic review and meta-analysis of randomized trials on probiotics for hepatic encephalopathy. Hepatol Res. 2012, 42, 1008–1015. [Google Scholar] [CrossRef]
- Hungin, A.P.; Mulligan, C.; Pot, B.; Whorwell, P.; Agréus, L.; Fracasso, P.; Lionis, C.; Mendive, J.; Philippart de Foy, J.M.; Rubin, G.; et al. Systematic review: Probiotics in the management of lower gastrointestinal symptoms in clinical practice—An evidence-based international guide. Aliment Pharmacol. Ther. 2013, 38, 864–886. [Google Scholar] [CrossRef] [PubMed]
- Salem, I.; Ramser, A.; Isham, N.; Ghannoum, M.A. The Gut Microbiome as a Major Regulator of the Gut-Skin Axis. Front. Microbiol. 2018, 9, 1459. [Google Scholar] [CrossRef] [PubMed]
- Clarke, G.; Stilling, R.M.; Kennedy, P.J.; Stanton, C.; Cryan, J.F.; Dinan, T.G. Minireview: Gut Microbiota: The Neglected Endocrine Organ. Mol. Endocrinol. 2014, 28, 1221–1238. [Google Scholar] [CrossRef]
- Maldonado Galdeano, C.; Cazorla, S.I.; Lemme Dumit, J.M.; Vélez, E.; Perdigón, G. Beneficial Effects of Probiotic Consumption on the Immune System. Ann. Nutr. Metab. 2019, 74, 115–124. [Google Scholar] [CrossRef]
- Liu, Y.; Alookaran, J.J.; Rhoads, J.M. Probiotics in Autoimmune and Inflammatory Disorders. Nutrients 2018, 10, 1537. [Google Scholar] [CrossRef]
- Kerry, R.G.; Patra, J.K.; Gouda, S.; Park, Y.; Shin, H.S.; Das, G. Benefaction of probiotics for human health: A review. J. Food Drug Anal. 2018, 26, 927–939. [Google Scholar] [CrossRef]
- Zhu, G.; Zhao, J.; Zhang, H.; Chen, W.; Wang, G. Probiotics for Mild Cognitive Impairment and Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Foods 2021, 10, 1672. [Google Scholar] [CrossRef]
- Binda, S.; Hill, C.; Johansen, E.; Obis, D.; Pot, B.; Sanders, M.E.; Tremblay, A.; Ouwehand, A.C. Criteria to Qualify Microorganisms as "Probiotic" in Foods and Dietary Supplements. Front. Microbiol. 2020, 11, 1662. [Google Scholar] [CrossRef]
- Rautava, S.; Kalliomäki, M.; Isolauri, E. New therapeutic strategy for combating the increasing burden of allergic disease: Probiotics-A Nutrition, Allergy, Mucosal Immunology and Intestinal Microbiota (NAMI) Research Group report. J. Allergy Clin. Immunol. 2005, 116, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Anania, C.; Brindisi, G.; Martinelli, I.; Bonucci, E.; D’Orsi, M.; Ialongo, S.; Nyffenegger, A.; Raso, T.; Spatuzzo, M.; De Castro, G.; et al. Probiotics Function in Preventing Atopic Dermatitis in Children. Int. J. Mol. Sci. 2022, 23, 5409. [Google Scholar] [CrossRef]
- Liu, Y.; Du, X.; Zhai, S.; Tang, X.; Liu, C.; Li, W. Gut microbiota and atopic dermatitis in children: A scoping review. BMC Pediatr. 2022, 22, 323. [Google Scholar] [CrossRef] [PubMed]
- Boggio Marzet, C.; Burgos, F.; Del Compare, M.; Gerold, I.; Tabacco, O.; Vinderola, G. Approach to probiotics in pediatrics: The role of Lactobacillus rhamnosus GG. Arch. Argent Pediatr. 2022, 120, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Ni, B.; Liu, Z.; Liu, X.; Xie, W.; Wu, I.X.Y.; Li, X. The Role of Probiotics in the Prevention and Treatment of Atopic Dermatitis in Children: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials. Paediatr. Drugs 2020, 22, 535–549. [Google Scholar] [CrossRef]
- Sun, S.; Chang, G.; Zhang, L. The prevention effect of probiotics against eczema in children: An update systematic review and meta-analysis. J. Dermatol. Treat. 2022, 33, 1844–1854. [Google Scholar] [CrossRef]
- D’Elios, S.; Trambusti, I.; Verduci, E.; Ferrante, G.; Rosati, S.; Marseglia, G.L.; Drago, L.; Peroni, D.G. Probiotics in the prevention and treatment of atopic dermatitis. Pediatr. Allergy Immunol. 2020, 31 (Suppl. 26), 43–45. [Google Scholar] [CrossRef]
- Huang, R.; Ning, H.; Shen, M.; Li, J.; Zhang, J.; Chen, X. Probiotics for the Treatment of Atopic Dermatitis in Children: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Cell Infect. Microbiol. 2017, 7, 392. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; López-López, J.A.; Becker, B.J.; Davies, S.R.; Dawson, S.; Grimshaw, J.M.; McGuinness, L.A.; Moore, T.H.M.; Rehfuess, E.A.; Thomas, J.; et al. Synthesising quantitative evidence in systematic reviews of complex health interventions. BMJ Glob. Health 2019, 4, e000858. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef] [PubMed]
- Tufanaru, C.; Munn, Z.; Aromataris, E.; Campbell, J.; Hopp, L. Chapter 3: Systematic reviews of effectiveness. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI, University of Adelaide: Adelaide, Australia, 2020. [Google Scholar]
- Camp, S.; Legge, T. Simulation as a Tool for Clinical Remediation: An Integrative Review. Clin. Simul. Nurs. 2018, 16, 48–61. [Google Scholar] [CrossRef]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.2.0. 2017. Available online: https://training.cochrane.org/handbook (accessed on 3 November 2022).
- Cumpston, M.S.; McKenzie, J.E.; Welch, V.A.; Brennan, S.E. Strengthening systematic reviews in public health: Guidance in the Cochrane Handbook for Systematic Reviews of Interventions, 2nd edition. J. Public Health 2022, 44, e588–e592. [Google Scholar] [CrossRef] [PubMed]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Isolauri, E.; Arvola, T.; Sütas, Y.; Moilanen, E.; Salminen, S. Probiotics in the management of atopic eczema. Clin. Exp. Allergy 2000, 30, 1604–1610. [Google Scholar] [CrossRef]
- Kirjavainen, P.V.; Salminen, S.J.; Isolauri, E. Probiotic bacteria in the management of atopic disease: Underscoring the importance of viability. J. Pediatr. Gastroenterol. Nutr. 2003, 36, 223–227. [Google Scholar] [CrossRef]
- Viljanen, M.; Savilahti, E.; Haahtela, T.; Juntunen-Backman, K.; Korpela, R.; Poussa, T.; Tuure, T.; Kuitunen, M. Probiotics in the treatment of atopic eczema/dermatitis syndrome in infants: A double-blind placebo-controlled trial. Allergy 2005, 60, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Weston, S.; Halbert, A.; Richmond, P.; Prescott, S.L. Effects of probiotics on atopic dermatitis: A randomised controlled trial. Arch. Dis. Child 2005, 90, 892–897. [Google Scholar] [CrossRef]
- Brouwer, M.L.; Wolt-Plompen, S.A.; Dubois, A.E.; van der Heide, S.; Jansen, D.F.; Hoijer, M.A.; Kauffman, H.F.; Duiverman, E.J. No effects of probiotics on atopic dermatitis in infancy: A randomized placebo-controlled trial. Clin. Exp. Allergy 2006, 36, 899–906. [Google Scholar] [CrossRef] [PubMed]
- Fölster-Holst, R.; Müller, F.; Schnopp, N.; Abeck, D.; Kreiselmaier, I.; Lenz, T.; von Rüden, U.; Schrezenmeir, J.; Christophers, E.; Weichenthal, M. Prospective, randomized controlled trial on Lactobacillus rhamnosus in infants with moderate to severe atopic dermatitis. Br. J. Dermatol. 2006, 155, 1256–1261. [Google Scholar] [CrossRef] [PubMed]
- Grüber, C.; Wendt, M.; Sulser, C.; Lau, S.; Kulig, M.; Wahn, U.; Werfel, T.; Niggemann, B. Randomized, placebo-controlled trial of Lactobacillus rhamnosus GG as treatment of atopic dermatitis in infancy. Allergy 2007, 62, 1270–1276. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.I.; Kim, J.Y.; Lee, Y.J.; Kim, N.S.; Hahn, Y.S. Effect of Lactobacillus sakei supplementation in children with atopic eczema-dermatitis syndrome. Ann. Allergy Asthma Immunol. 2010, 104, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Klewicka, E.; Cukrowska, B.; Libudzisz, Z.; Slizewska, K.; Motyl, I. Changes in gut microbiota in children with atopic dermatitis administered the bacteria Lactobacillus casei DN--114001. Pol. J. Microbiol. 2011, 60, 329–333. [Google Scholar] [CrossRef]
- Gore, C.; Custovic, A.; Tannock, G.W.; Munro, K.; Kerry, G.; Johnson, K.; Peterson, C.; Morris, J.; Chaloner, C.; Murray, C.S.; et al. Treatment and secondary prevention effects of the probiotics Lactobacillus paracasei or Bifidobacterium lactis on early infant eczema: Randomized controlled trial with follow-up until age 3 years. Clin. Exp. Allergy 2012, 42, 112–122. [Google Scholar] [CrossRef]
- Han, Y.; Kim, B.; Ban, J.; Lee, J.; Kim, B.J.; Choi, B.S.; Hwang, S.; Ahn, K.; Kim, J. A randomized trial of Lactobacillus plantarum CJLP133 for the treatment of atopic dermatitis. Pediatr. Allergy Immunol. 2012, 23, 667–673. [Google Scholar] [CrossRef]
- Wang, I.J.; Wang, J.Y. Children with atopic dermatitis show clinical improvement after Lactobacillus exposure. Clin. Exp. Allergy 2015, 45, 779–787. [Google Scholar] [CrossRef]
- Prakoeswa, C.R.S.; Herwanto, N.; Prameswari, R.; Astari, L.; Sawitri, S.; Hidayati, A.N.; Indramaya, D.M.; Kusumowidagdo, E.R.; Surono, I.S. Lactobacillus plantarum IS-10506 supplementation reduced SCORAD in children with atopic dermatitis. Benef. Microbes 2017, 8, 833–840. [Google Scholar] [CrossRef]
- Wu, Y.J.; Wu, W.F.; Hung, C.W.; Ku, M.S.; Liao, P.F.; Sun, H.L.; Lu, K.H.; Sheu, J.N.; Lue, K.H. Evaluation of efficacy and safety of Lactobacillus rhamnosus in children aged 4-48 months with atopic dermatitis: An 8-week, double-blind, randomized, placebo-controlled study. J. Microbiol. Immunol. Infect. 2017, 50, 684–692. [Google Scholar] [CrossRef]
- Ahn, S.H.; Yoon, W.; Lee, S.Y.; Shin, H.S.; Lim, M.Y.; Nam, Y.D.; Yoo, Y. Effects of Lactobacillus pentosus in Children with Allergen-Sensitized Atopic Dermatitis. J. Korean Med. Sci. 2020, 35, e128. [Google Scholar] [CrossRef]
- Rather, I.A.; Kim, B.C.; Lew, L.C.; Cha, S.K.; Lee, J.H.; Nam, G.J.; Majumder, R.; Lim, J.; Lim, S.K.; Seo, Y.J.; et al. Oral Administration of Live and Dead Cells of Lactobacillus sakei proBio65 Alleviated Atopic Dermatitis in Children and Adolescents: A Randomized, Double-Blind, and Placebo-Controlled Study. Probiotics Antimicrob. Proteins 2021, 13, 315–326. [Google Scholar] [CrossRef]
- Carucci, L.; Nocerino, R.; Paparo, L.; De Filippis, F.; Coppola, S.; Giglio, V.; Cozzolino, T.; Valentino, V.; Sequino, G.; Bedogni, G.; et al. Therapeutic effects elicited by the probiotic Lacticaseibacillus rhamnosus GG in children with atopic dermatitis. The results of the ProPAD trial. Pediatr. Allergy Immunol. 2022, 33, e13836. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-O.; Ah, Y.-M.; Yu, Y.M.; Choi, K.H.; Shin, W.-G.; Lee, J.-Y. Effects of probiotics for the treatment of atopic dermatitis: A meta-analysis of randomized controlled trials. Ann. Allergy Asthma Immunol. 2014, 113, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Pessi, T.; Sütas, Y.; Hurme, M.; Isolauri, E. Interleukin-10 generation in atopic children following oral Lactobacillus rhamnosus GG. Clin. Exp. Allergy 2000, 30, 1804–1808. [Google Scholar] [CrossRef] [PubMed]
- Steiner, N.C.; Lorentz, A. Probiotic Potential of Lactobacillus Species in Allergic Rhinitis. Int. Arch. Allergy Immunol. 2021, 182, 807–818. [Google Scholar] [CrossRef]
- Bianchini, S.; Orabona, C.; Camilloni, B.; Berioli, M.G.; Argentiero, A.; Matino, D.; Alunno, A.; Albini, E.; Vacca, C.; Pallotta, M.T.; et al. Effects of probiotic administration on immune responses of children and adolescents with type 1 diabetes to a quadrivalent inactivated influenza vaccine. Hum. Vaccines Immunother. 2020, 16, 86–94. [Google Scholar] [CrossRef]
- Naghmouchi, K.; Belguesmia, Y.; Bendali, F.; Spano, G.; Seal, B.S.; Drider, D. Lactobacillus fermentum: A bacterial species with potential for food preservation and biomedical applications. Crit. Rev. Food Sci. Nutr. 2020, 60, 3387–3399. [Google Scholar] [CrossRef] [PubMed]
- Gupta, T.; Kaur, H.; Kapila, S.; Kapila, R. Lactobacillus fermentum (MTCC-5898) alleviates Escherichia coli-induced inflammatory responses in intestinal epithelial cells by modulating immune genes and NF-κB signalling. J. Appl. Microbiol. 2021, 131, 3008–3017. [Google Scholar] [CrossRef]
- Lee, C.S.; Kim, S.H. Anti-inflammatory and Anti-osteoporotic Potential of Lactobacillus plantarum A41 and L. fermentum SRK414 as Probiotics. Probiotics Antimicrob. Proteins 2020, 12, 623–634. [Google Scholar] [CrossRef] [PubMed]
- Viljanen, M.; Kuitunen, M.; Haahtela, T.; Juntunen-Backman, K.; Korpela, R.; Savilahti, E. Probiotic effects on faecal inflammatory markers and on faecal IgA in food allergic atopic eczema/dermatitis syndrome infants. Pediatr. Allergy Immunol. 2005, 16, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Viljanen, M.; Pohjavuori, E.; Haahtela, T.; Korpela, R.; Kuitunen, M.; Sarnesto, A.; Vaarala, O.; Savilahti, E. Induction of inflammation as a possible mechanism of probiotic effect in atopic eczema-dermatitis syndrome. J. Allergy Clin. Immunol. 2005, 115, 1254–1259. [Google Scholar] [CrossRef] [PubMed]
- Wickens, K.; Black, P.N.; Stanley, T.V.; Mitchell, E.; Fitzharris, P.; Tannock, G.W.; Purdie, G.; Crane, J. A differential effect of 2 probiotics in the prevention of eczema and atopy: A double-blind, randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 2008, 122, 788–794. [Google Scholar] [CrossRef]
- Simpson, M.R.; Dotterud, C.K.; Storrø, O.; Johnsen, R.; Øien, T. Perinatal probiotic supplementation in the prevention of allergy related disease: 6 year follow up of a randomised controlled trial. BMC Dermatol. 2015, 15, 13. [Google Scholar] [CrossRef]
- Wickens, K.; Black, P.; Stanley, T.V.; Mitchell, E.; Barthow, C.; Fitzharris, P.; Purdie, G.; Crane, J. A protective effect of Lactobacillus rhamnosus HN001 against eczema in the first 2 years of life persists to age 4 years. Clin. Exp. Allergy 2012, 42, 1071–1079. [Google Scholar] [CrossRef]
- Rose, M.A.; Stieglitz, F.; Köksal, A.; Schubert, R.; Schulze, J.; Zielen, S. Efficacy of probiotic Lactobacillus GG on allergic sensitization and asthma in infants at risk. Clin. Exp. Allergy 2010, 40, 1398–1405. [Google Scholar] [CrossRef]
- Moro, G.; Arslanoglu, S.; Stahl, B.; Jelinek, J.; Wahn, U.; Boehm, G. A mixture of prebiotic oligosaccharides reduces the incidence of atopic dermatitis during the first six months of age. Arch. Dis. Child 2006, 91, 814–819. [Google Scholar] [CrossRef]
- Shafiei, A.; Moin, M.; Pourpak, Z.; Gharagozlou, M.; Aghamohamadi, A.; Sajedi, V.; Soheili, H.; Sotoodeh, S.; Movahedi, M. Synbiotics could not Reduce the Scoring of Childhood Atopic Dermatitis (SCORAD): A Randomized Double Blind Placebo-Controlled Trial. Iran. J. Allergy Asthma Immunol. 2011, 10, 21–28. [Google Scholar]
- Sharma, R.; Honda, S.; Mahajan, R.; De, D.; Sachdeva, N. Evaluating the Effect of Supplementation with Bacillus clausii on Therapeutic Outcomes in Atopic Eczema-Results of an Observer-Blinded Parallel-Group Randomized Controlled Study. Indian J. Dermatol. 2022, 67, 121–126. [Google Scholar] [CrossRef]
- Ivakhnenko, E.S.; Nian’kovskiĭ, S.L. Effect of probiotics on the dynamics of gastrointestinal symptoms of food allergy to cow’s milk protein in infants. Georgian Med. News 2013, 219, 46–52. [Google Scholar]
- van der Aa, L.B.; Lutter, R.; Heymans, H.S.; Smids, B.S.; Dekker, T.; van Aalderen, W.M.; Sillevis Smitt, J.H.; Knippels, L.M.; Garssen, J.; Nauta, A.J.; et al. No detectable beneficial systemic immunomodulatory effects of a specific synbiotic mixture in infants with atopic dermatitis. Clin. Exp. Allergy 2012, 42, 531–539. [Google Scholar] [CrossRef]
- Navarro-Lopez, V.; Ramirez-Bosca, A.; Ramon-Vidal, D.; Ruzafa-Costas, B.; Genoves-Martinez, S.; Chenoll-Cuadros, E.; Carrion-Gutierrez, M.; de la Parte, J.H.; Prieto-Merino, D.; Codoner-Cortes, F.M. Effect of Oral Administration of a Mixture of Probiotic Strains on SCORAD Index and Use of Topical Steroids in Young Patients With Moderate Atopic Dermatitis A Randomized Clinical Trial. JAMA Dermatol. 2018, 154, 37–43. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kwon, J.H.; Ahn, S.H.; Lee, S.I.; Han, Y.S.; Choi, Y.O.; Lee, S.Y.; Ahn, K.M.; Ji, G.E. Effect of probiotic mix (Bifidobacterium bifidum, Bifidobacterium lactis, Lactobacillus acidophilus) in the primary prevention of eczema: A double-blind, randomized, placebo-controlled trial. Pediatr. Allergy Immunol. 2010, 21, e386–e393. [Google Scholar] [CrossRef] [PubMed]
- Gerasimov, S.V.; Vasjuta, V.V.; Myhovych, O.O.; Bondarchuk, L.I. Probiotic supplement reduces atopic dermatitis in preschool children: A randomized, double-blind, placebo-controlled, clinical trial. Am. J. Clin. Dermatol. 2010, 11, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeldt, V.; Benfeldt, E.; Nielsen, S.D.; Michaelsen, K.F.; Jeppesen, D.L.; Valerius, N.H.; Paerregaard, A. Effect of probiotic Lactobacillus strains in children with atopic dermatitis. J. Allergy Clin. Immunol. 2003, 111, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Cukrowska, B.; Ceregra, A.; Maciorkowska, E.; Surowska, B.; Zegadło-Mylik, M.A.; Konopka, E.; Trojanowska, I.; Zakrzewska, M.; Bierła, J.B.; Zakrzewski, M.; et al. The Effectiveness of Probiotic Lactobacillus rhamnosus and Lactobacillus casei Strains in Children with Atopic Dermatitis and Cow’s Milk Protein Allergy: A Multicenter, Randomized, Double Blind, Placebo Controlled Study. Nutrients 2021, 13, 1169. [Google Scholar] [CrossRef]
- Farid, R.; Ahanchian, H.; Jabbari, F.; Moghiman, T. Effect of a New Synbiotic Mixture on Atopic Dermatitis in Children: A Randomized-Controlled Trial. Iran. J. Pediatr. 2011, 21, 225–230. [Google Scholar] [PubMed]
- D’Auria, E.; Panelli, S.; Lunardon, L.; Pajoro, M.; Paradiso, L.; Beretta, S.; Loretelli, C.; Tosi, D.; Perini, M.; Bedogni, G.; et al. Rice flour fermented with Lactobacillus paracasei CBA L74 in the treatment of atopic dermatitis in infants: A randomized, double- blind, placebo- controlled trial. Pharmacol. Res. 2021, 163, 105284. [Google Scholar] [CrossRef]
- Jeong, K.; Kim, M.; Jeon, S.A.; Kim, Y.H.; Lee, S. A randomized trial of Lactobacillus rhamnosus IDCC 3201 tyndallizate (RHT3201) for treating atopic dermatitis. Pediatr. Allergy Immunol. 2020, 31, 783–792. [Google Scholar] [CrossRef]
- Nakata, J.; Hirota, T.; Umemura, H.; Nakagawa, T.; Kando, N.; Futamura, M.; Nakamura, Y.; Ito, K. Additive effect of Lactobacillus acidophilus L-92 on children with atopic dermatitis concomitant with food allergy. Asia Pac. Allergy 2019, 9, e18. [Google Scholar] [CrossRef]
- Yan, D.C.; Hung, C.H.; Sy, L.B.; Lue, K.H.; Shih, I.H.; Yang, C.Y.; Chen, L.C.; Sun, H.L.; Lee, M.S.; Chambard, J.; et al. A Randomized, Double-Blind, Placebo-Controlled Trial Assessing the Oral Administration of a Heat-Treated Lactobacillus paracasei Supplement in Infants with Atopic Dermatitis Receiving Topical Corticosteroid Therapy. Skin Pharmacol. Physiol. 2019, 32, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Passeron, T.; Lacour, J.P.; Fontas, E.; Ortonne, J.P. Prebiotics and synbiotics: Two promising approaches for the treatment of atopic dermatitis in children above 2 years. Allergy 2006, 61, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Aldaghi, M.; Tehrani, H.; Karrabi, M.; Abadi, F.S.; Sahebkar, M. The effect of multi-strain synbiotic and vitamin D3 supplements on the severity of atopic dermatitis among infants under 1 year of age: A double-blind, randomized clinical trial study. J. Dermatol. Treat. 2022, 33, 812–817. [Google Scholar] [CrossRef] [PubMed]
- Rozé, J.C.; Barbarot, S.; Butel, M.J.; Kapel, N.; Waligora-Dupriet, A.J.; De Montgolfier, I.; Leblanc, M.; Godon, N.; Soulaines, P.; Darmaun, D.; et al. An α-lactalbumin-enriched and symbiotic-supplemented v. a standard infant formula: A multicentre, double-blind, randomised trial. Br. J. Nutr. 2012, 107, 1616–1622. [Google Scholar] [CrossRef]
- Wu, K.G.; Li, T.H.; Peng, H.J. Lactobacillus salivarius plus fructo-oligosaccharide is superior to fructo-oligosaccharide alone for treating children with moderate to severe atopic dermatitis: A double-blind, randomized, clinical trial of efficacy and safety. Br. J. Dermatol. 2012, 166, 129–136. [Google Scholar] [CrossRef]
- Zhao, M.; Shen, C.; Ma, L. Treatment efficacy of probiotics on atopic dermatitis, zooming in on infants: A systematic review and meta-analysis. Int. J. Dermatol. 2018, 57, 635–641. [Google Scholar] [CrossRef]
- Lambring, C.B.; Siraj, S.; Patel, K.; Sankpal, U.T.; Mathew, S.; Basha, R. Impact of the Microbiome on the Immune System. Crit. Rev. Immunol. 2019, 39, 313–328. [Google Scholar] [CrossRef]
- Eslami, M.; Bahar, A.; Keikha, M.; Karbalaei, M.; Kobyliak, N.M.; Yousefi, B. Probiotics function and modulation of the immune system in allergic diseases. Allergol. Immunopathol. 2020, 48, 771–788. [Google Scholar] [CrossRef]
- Fenner, J.; Silverberg, N.B. Oral supplements in atopic dermatitis. Clin. Dermatol. 2018, 36, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Boulos, S.; Yan, A.C. Current concepts in the prevention of atopic dermatitis. Clin. Dermatol. 2018, 36, 668–671. [Google Scholar] [CrossRef] [PubMed]
- Elghazaly, S.M.; Hamam, K.M.; Badawy, M.M.; Yakoub Agha, N.A.; Samy, A.; Abbas, A.M. Efficacy and safety of single dose of oral secnidazole 2 g in treatment of bacterial vaginosis: A systematic review and meta-analysis. Eur. J. Obstet Gynecol. Reprod. Biol. 2019, 238, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Yao, Z.; Chen, H.; Wang, X.; Zhang, Y.; Jian, M.; Hu, J.; Yu, B.; Jiang, L. Efficacy of the Short-Term versus Long-Term Administration of Antimicrobial Prophylaxis in Gastric Cancer Surgery: A Meta-Analysis of Randomized Controlled Trials. Surg. Infect. 2022, 23, 625–633. [Google Scholar] [CrossRef]
- Janjua, S.; Mathioudakis, A.G.; Fortescue, R.; Walker, R.A.E.; Sharif, S.; Threapleton, C.J.D.; Dias, S. Prophylactic antibiotics for adults with chronic obstructive pulmonary disease: A network meta-analysis. Cochrane Database Syst. Rev. 2021, 1, CD013198. [Google Scholar] [CrossRef]
- Ricci, G.; Cipriani, F.; Cuello-Garcia, C.A.; Brożek, J.L.; Fiocchi, A.; Pawankar, R.; Yepes-Nuñes, J.J.; Terraciano, L.; Gandhi, S.; Agarwal, A.; et al. A clinical reading on “World Allergy Organization-McMaster University Guidelines for Allergic Disease Prevention (GLAD-P): Probiotics”. World Allergy Organ. J. 2016, 9, 9. [Google Scholar] [CrossRef]
- Fiocchi, A.; Pawankar, R.; Cuello-Garcia, C.; Ahn, K.; Al-Hammadi, S.; Agarwal, A.; Beyer, K.; Burks, W.; Canonica, G.W.; Ebisawa, M.; et al. World Allergy Organization-McMaster University Guidelines for Allergic Disease Prevention (GLAD-P): Probiotics. World Allergy Organ. J. 2015, 8, 4. [Google Scholar] [CrossRef]
- Underwood, M.A. Should we treat every infant with a probiotic? Minerva. Pediatr. 2019, 71, 253–262. [Google Scholar] [CrossRef]
- Blauvelt, A.; de Bruin-Weller, M.; Gooderham, M.; Cather, J.C.; Weisman, J.; Pariser, D.; Simpson, E.L.; Papp, K.A.; Hong, H.C.; Rubel, D.; et al. Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): A 1-year, randomised, double-blinded, placebo-controlled, phase 3 trial. Lancet 2017, 389, 2287–2303. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Quality Index |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Isolauri 2000 [41] | unclear | unclear | YES | YES | YES | YES | YES | YES | unclear | YES | YES | YES | YES | Medium-high |
| Kirjavainen 2003 [42] | unclear | unclear | YES | YES | NO | YES | YES | YES | unclear | YES | YES | YES | YES | Medium-high |
| Viljanen 2005 [43] | YES | YES | YES | YES | YES | YES | YES | YES | unclear | YES | YES | YES | YES | Excellent |
| Weston et al., 2005 [44] | YES | YES | YES | YES | YES | YES | YES | YES | unclear | YES | YES | YES | YES | Excellent |
| Brouwer 2006 [45] | unclear | unclear | YES | YES | YES | YES | YES | YES | unclear | YES | YES | YES | YES | Medium-high |
| Fölster-Holst 2006 [46] | unclear | unclear | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | High |
| Grüber 2007 [47] | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | Excellent |
| Woo 2010 [48] | unclear | unclear | YES | YES | YES | YES | YES | YES | unclear | YES | YES | YES | YES | Medium-high |
| Klewicka 2011 [49] | unclear | YES | YES | YES | YES | YES | YES | YES | unclear | YES | YES | YES | YES | High |
| Gore 2012 [50] | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | Excellent |
| Han 2012 [51] | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | Excellent |
| Wang 2015 [52] | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | Excellent |
| Prakoeswa 2017 [53] | unclear | unclear | YES | YES | YES | YES | YES | YES | unclear | YES | YES | YES | YES | Medium-high |
| Wu 2017 [54] | unclear | unclear | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | High |
| Ahn 2020 [55] | unclear | YES | YES | YES | YES | YES | YES | YES | unclear | YES | YES | YES | YES | High |
| Rather 2021 [56] | YES | YES | YES | YES | YES | YES | YES | YES | unclear | YES | YES | YES | YES | Excellent |
| Carucci 2022 [57] | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | Excellent |
| Reference (First Author, Year) | Population That Completed Trial | Intervention of Single-Strain Probiotic Lactobacilli | Main Findings | |
|---|---|---|---|---|
| Probiotic/Dosage | Duration | |||
| Isolauri 2000 [41] | In this study, 27 patients, mean age 4.6 months, with atopic disease symptoms, divided into three equal groups. A total of 9 in two probiotic groups (Group 2: not lactobacilli) and 9 in the placebo group. | Lacticaseibacillus 1 rhamnosus GG (LGG), 3 × 108 cfu/g | 2 months | A statistically significant decrease in the SCORAD index was found in both probiotic groups compared to the placebo. Both probiotics also counteracted inflammatory responses compared to the placebo (CD4 levels were statistically significantly lower in the probiotic group compared to the placebo). |
| Kirjavainen 2003 [42] | In this study, 35 patients, mean age 5.5 months, with atopic disease symptoms, divided into three groups. A total of 14 in group one, 13 in group two (heat-killed LGG) and 8 in the placebo group. | Lacticaseibacillus rhamnosus GG, 1 × 109 cfu, qd | 7.5 weeks | The decrease in the SCORAD index within the viable LGG group tended to be greater than within the placebo group. The treatment with heat-inactivated LGG was associated with adverse gastrointestinal symptoms and diarrhea. |
| Viljanen 2005 [43] | In this study, 230 patients aged 1–12 months with atopic eczema–dermatitis syndrome, divided into three groups. A total of 80 in probiotic group 1, 76 in group 2 (multi-strain) and 74 in the placebo group. | Lacticaseibacillus rhamnosus GG, 5 × 109 cfu, qd | 4 weeks | No statistically significant effects of probiotic supplementation on mean SCORAD index reduction between groups were found. A statistically significant lower SCORAD index was observed in Ig-E sensitized infants after supplementation in the probiotic group compared to placebo. |
| Weston 2005 [44] | In this study, 56 patients aged 6–18 months with moderate to severe AD. A total of 26 in the probiotic group and 27 in the placebo group. | Limosilactobacillus 1 fermentum VRI-033 PCC, 1 × 109 cfu, bid | 8 weeks | A statistically significant lower SCORAD index was observed after supplementation in the probiotic group compared to the placebo. The reduction in the SCORAD index over time was significant in the probiotic group but not in the placebo group. |
| Brouwer 2006 [45] | In this study, 50 patients aged 1–5 months with AD, divided into three groups. A total of 33 in both single-strain probiotic lactobacilli groups (16 in group 1 and 17 in group 2) and 17 in the placebo group. | Lacticaseibacillus rhamnosus GG, 5 × 109 cfu/g | 3 months | There were no statistically significant effects of probiotic supplementation on SCORAD, sensitization, inflammatory parameters or cytokine production between groups. |
| Lacticaseibacillus rhamnosus, 5 × 109 cfu/g | ||||
| Fölster-Holst 2006 [46] | In this study, 42 patients aged 1–55 months with moderate to severe AD. A total of 21 in both the probiotic and placebo group. | Lacticaseibacillus rhamnosus GG, 1 × 1010 cfu, qd | 8 weeks | No significant differences were observed between the groups with respect to the SCORAD index. No significant differences were observed between the groups with respect to other clinical symptoms (pruritus, sleep loss), the use of topical corticosteroids and antihistamines or immunological parameters. |
| Grüber 2007 [47] | In this study, 102 patients aged 3–12 months with mild to moderate AD. A total of 54 in the probiotic group and 48 in the placebo group. | Lacticaseibacillus rhamnosus GG, 5 × 109 cfu, bid | 12 weeks | No significant differences were observed for the SCORAD index, use of rescue medicine or increase in mean total logarithmic serum immunoglobin E after supplementation in the probiotic group compared to placebo. When stratified for age, eczema severity or use of rescue medication, no statistically significant group differences in improvement were found. |
| Woo 2010 [48] | In this study, 75 patients aged 2–10 years with eczema–dermatitis syndrome. A total of 41 in the probiotic group and 43 in the placebo group. | Latilactobacillus 1 sakei KCTC 10755BP, 5 × 109 cfu, bid | 12 weeks | Statistically significant lower SCORAD index, mean disease activity, proportions of patients achieving improvement and serum chemokine levels were observed after supplementation in the probiotic group compared to placebo. |
| Klewicka 2011 [49] | In this study, 40 patients aged 6–18 months with medium to severe AD. A total of 18 in the probiotic group and 22 in the placebo group. | Lacticaseibacillus casei DN-114001, 1 × 109 cfu, qd | 3 months | A decrease in the SCORAD index was observed in the probiotic group. Supplementation with probiotics positively affected their gut microbiota. |
| Gore 2012 [50] | In this study, 133 patients aged 3–6 months with AD. A total of 43 in probiotic group I, 44 in probiotic group II (not lactobacilli) and 46 in the placebo group. | Lacticaseibacillus 1 paracasei CNCM I-2116, 1 × 1010 cfu, qd | 12 weeks | No significant differences were observed for the SCORAD index after supplementation in the probiotic group compared to the placebo. Results were similar when the analysis was controlled for allergen-sensitization or when only sensitized infants were analyzed. |
| Han 2012 [51] | In this study, 83 patients aged 1–13 years with AD. A total of 44 in the probiotic group and 39 in the placebo group. | Lactiplantibacillus 1 plantarum CJLP133, 5 × 109 cfu, bid | 12 weeks | Statistically significant mean changes in SCORAD index and lower SCORAD index, eosinophil counts, and logarithmic interferon-gamma and interleukin-4 were observed after supplementation in the probiotic group compared to placebo. |
| Wang 2015 [52] | In this study, 212 patients aged 1–18 years with AD and positive skin prick test, divided into 4 groups. A total of 159 in 3 probiotic groups with 55 in group 1 (single-strain), 53 in group 2 (single-strain), 51 in group 3 (both strains) and 53 in the placebo group. | Lacticaseibacillus paracasei GMNL-133 (Lp), 2 × 109 cfu, qd | 3 months | A statistically significant lower SCORAD index and interleukin-4 levels were observed after supplementation in all three probiotic groups compared to the placebo. |
| Limosilactobacillus fermentum GM090 (Lf), 2 × 109 cfu, qd | ||||
| Prakoeswa 2017 [53] | In this study, 22 patients aged 0–14 years with mild and moderate AD. A total of 12 in the probiotic group and 10 in the placebo group. | Lactiplantibacillus plantarum IS-10506, 1 × 1010 cfu, qd | 12 weeks | A statistically significant lower SCORAD index and levels of interleukin-4, interferon-gamma and interleukin-17 levels were observed after supplementation in the probiotic group compared to the placebo. The ratio of forkhead box P3 to interleukin-10 was significantly higher after supplementation in the probiotic group than in the placebo group. |
| Wu 2017 [54] | In this study, 62 patients aged 4–48 months with AD. A total of 30 in the probiotic group and 32 in the placebo group. | Lacticaseibacillus rhamnosus MP108, 1 capsule 2, qd | 8 weeks | A statistically significant lower SCORAD index was observed after supplementation in the probiotic group compared to the placebo. Mean changes from baseline declined in the probiotic and placebo groups, but no statistically significant differences were noted. |
| Ahn 2020 [55] | In this study, 82 patients aged 2–13 years with mild to moderate AD. A total of 41 in each group. | Lactiplantibacillus pentosus 3, 1 × 1010 cfu, bid | 12 weeks | No significant difference was found in the reduction in the SCORAD index after supplementation in the probiotic group compared to the placebo. However, a statistically significant reduction in the SCORAD index was observed in the subgroup of Immunoglobulin E-sensitized AD compared to placebo. |
| Rather 2021 [56] | In this study, 58 patients aged 3–18 years with mild to moderate AD divided into three groups. A total of 16 in the probiotic group, 22 in group II (received dead cells) and 20 in the placebo group. | Latilactobacillus sakei proBio65, 1010 cfu, qd | 12 weeks | A statistically significant lower SCORAD total index was observed after supplementation in the probiotic group and the group receiving non-viable cells compared to the placebo. Statistically significant increase in skin sebum in the probiotic group as well as in the group that received non-viable cells. |
| Carucci 2022 [57] | In this study, 91 patients aged 6–36 months with AD. A total of 46 in probiotic group A and 45 in the placebo group. | Lacticaseibacillus rhamnosus GG, 1010 cfu, qd | 12 weeks | A statistically significant higher rate of participants in the probiotic group after supplementation achieved the minimum clinically important difference in the SCORAD index compared to the placebo. The probiotic group also observed a beneficial modulation of the gut and skin microbiome. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fijan, S.; Kolč, N.; Hrašovec, M.; Jamtvedt, G.; Pogačar, M.Š.; Mičetić Turk, D.; Maver, U. Single-Strain Probiotic Lactobacilli for the Treatment of Atopic Dermatitis in Children: A Systematic Review and Meta-Analysis. Pharmaceutics 2023, 15, 1256. https://doi.org/10.3390/pharmaceutics15041256
Fijan S, Kolč N, Hrašovec M, Jamtvedt G, Pogačar MŠ, Mičetić Turk D, Maver U. Single-Strain Probiotic Lactobacilli for the Treatment of Atopic Dermatitis in Children: A Systematic Review and Meta-Analysis. Pharmaceutics. 2023; 15(4):1256. https://doi.org/10.3390/pharmaceutics15041256
Chicago/Turabian StyleFijan, Sabina, Nina Kolč, Metka Hrašovec, Gro Jamtvedt, Maja Šikić Pogačar, Dušanka Mičetić Turk, and Uroš Maver. 2023. "Single-Strain Probiotic Lactobacilli for the Treatment of Atopic Dermatitis in Children: A Systematic Review and Meta-Analysis" Pharmaceutics 15, no. 4: 1256. https://doi.org/10.3390/pharmaceutics15041256