
A Pharmacometric Model to Predict Chemotherapy-Induced Myelosuppression and Associated Risk Factors in Non-Small Cell Lung Cancer


Abstract
:1. Introduction
2. Methods
2.1. Data
2.2. Model Development
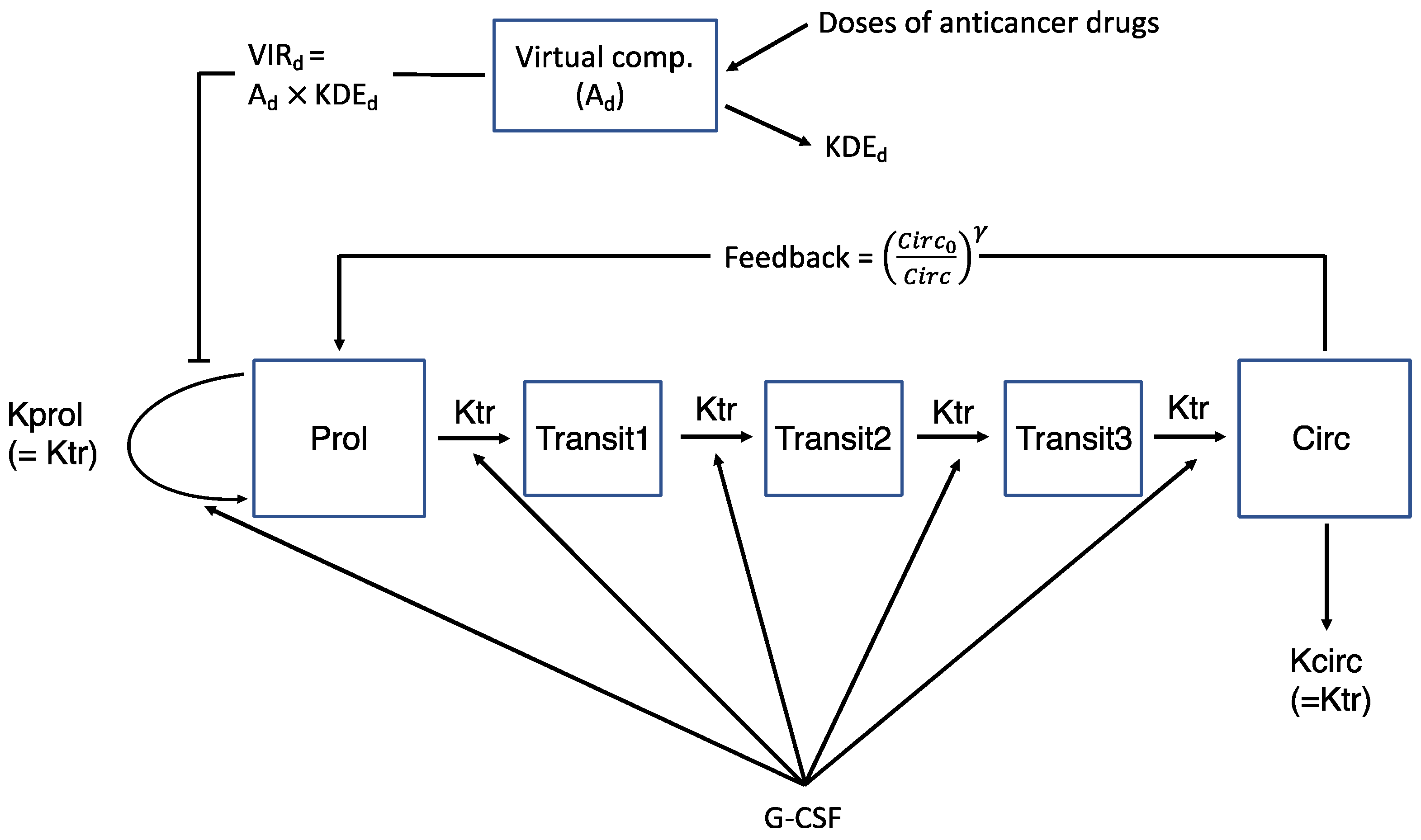
2.2.1. Semi-Mechanistic Myelosuppression Model
2.2.2. Kinetic-Pharmacodynamic (K-PD) Drug Model
2.2.3. Drug Effect of Combination Chemotherapy
2.2.4. G-CSF Effect
2.3. Covariate Modeling
2.4. Statistical Model
2.5. Model Evaluation
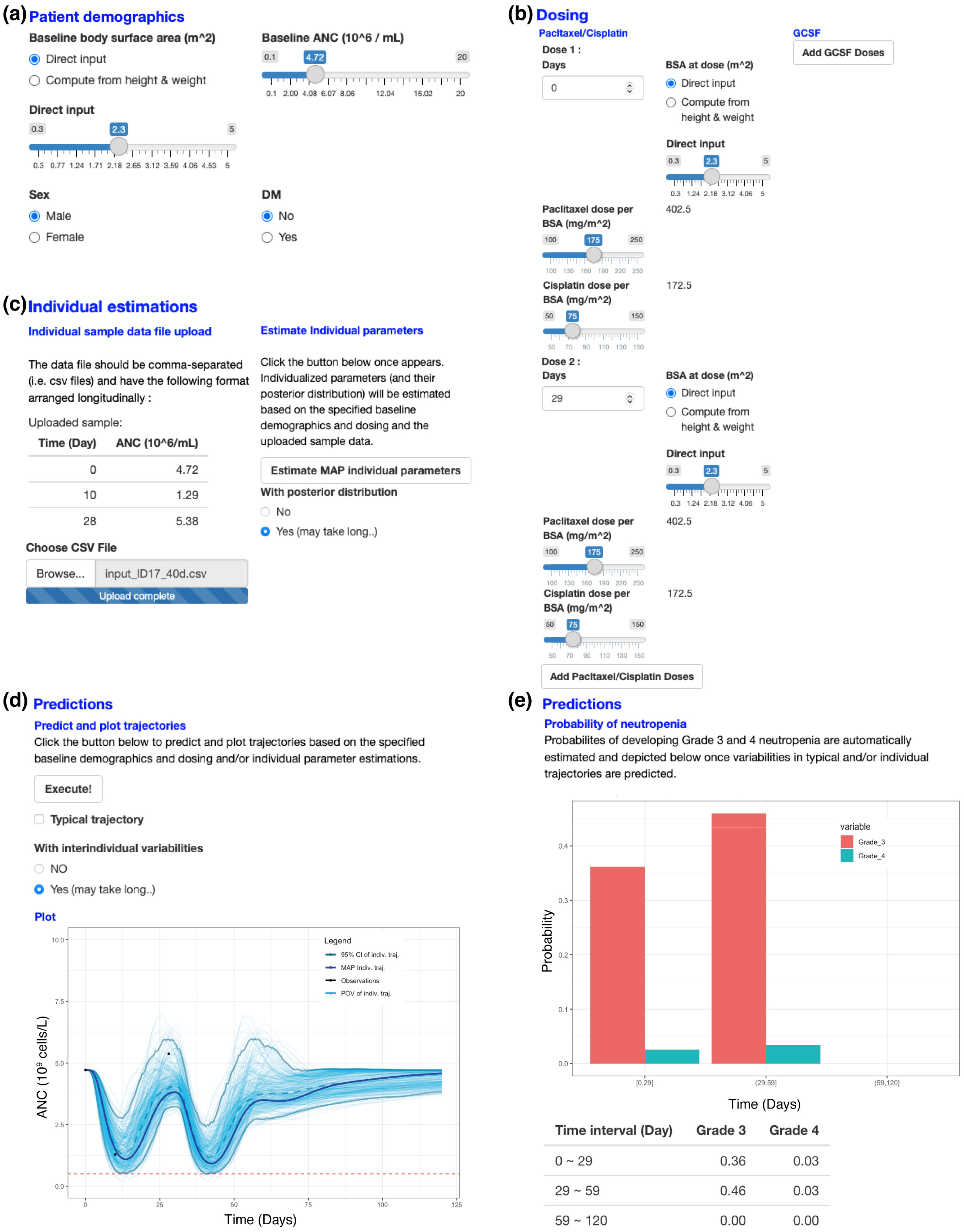
2.6. A Web Application for a New Patient’s ANC Prediction
2.7. Software
3. Results
3.1. Data
3.2. Basic Model for Drug Effect
3.3. Basic Model for Drug and G-CSF Effects
3.4. Covariate Modeling
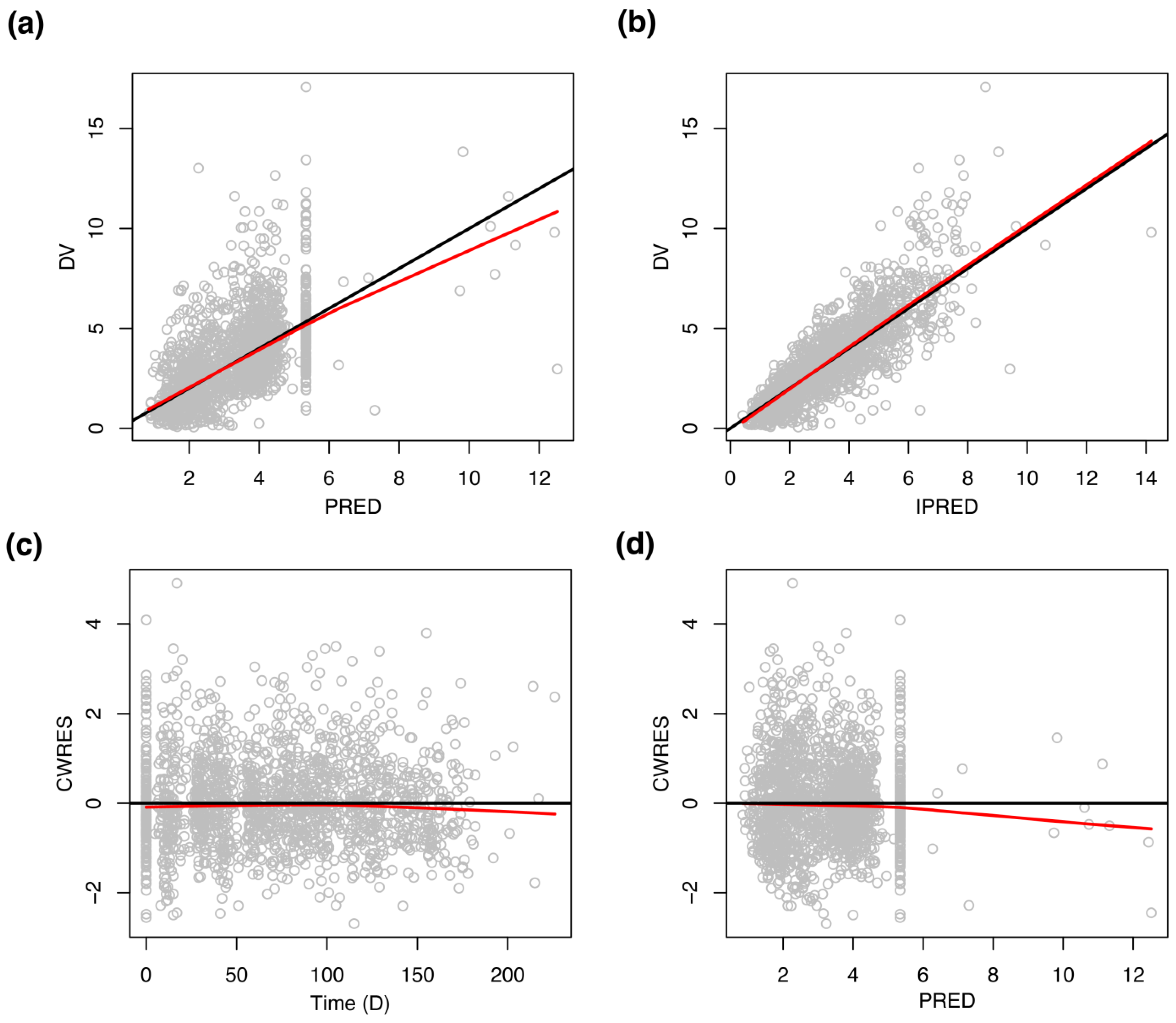
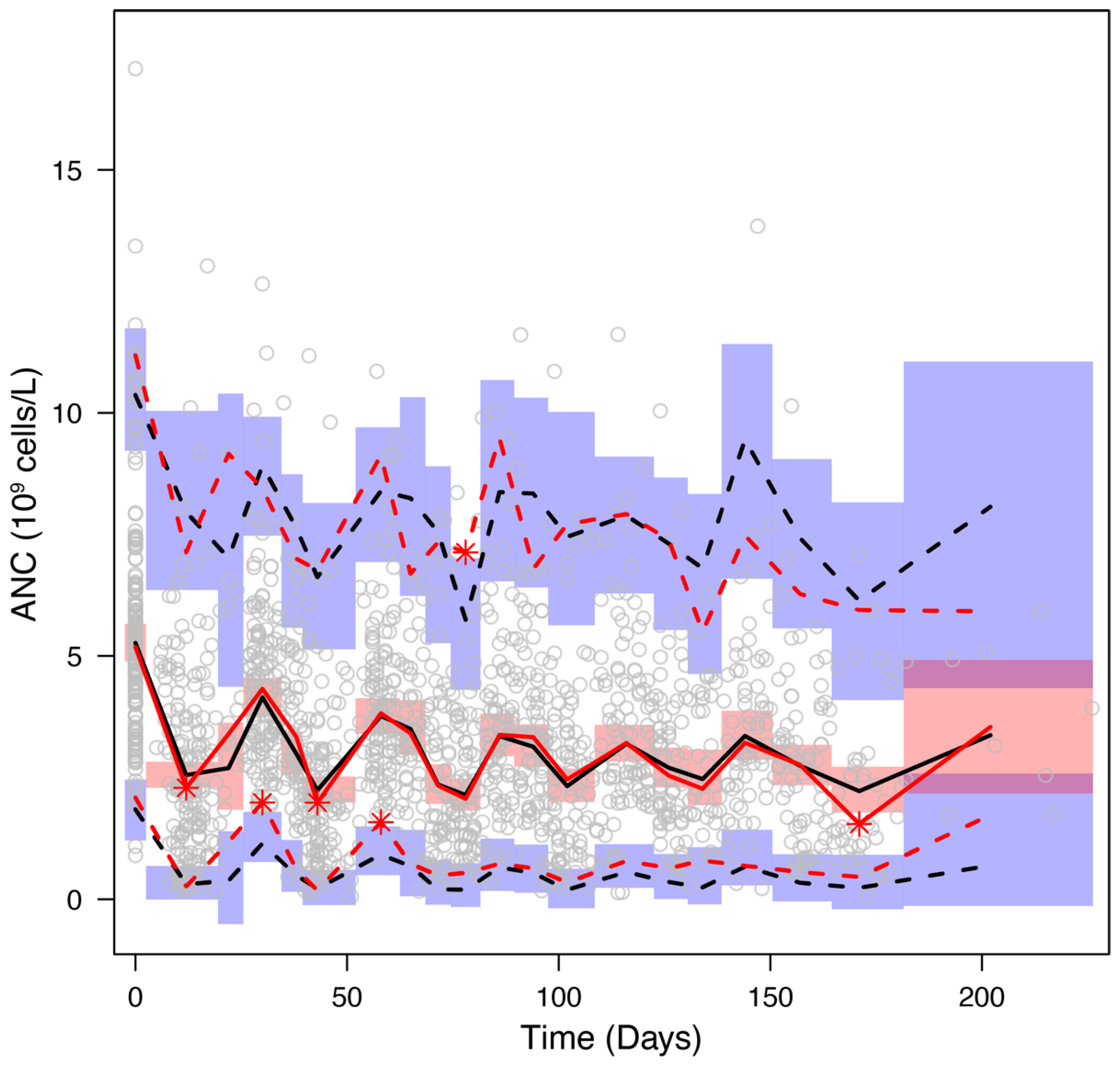
3.5. Model Evaluation
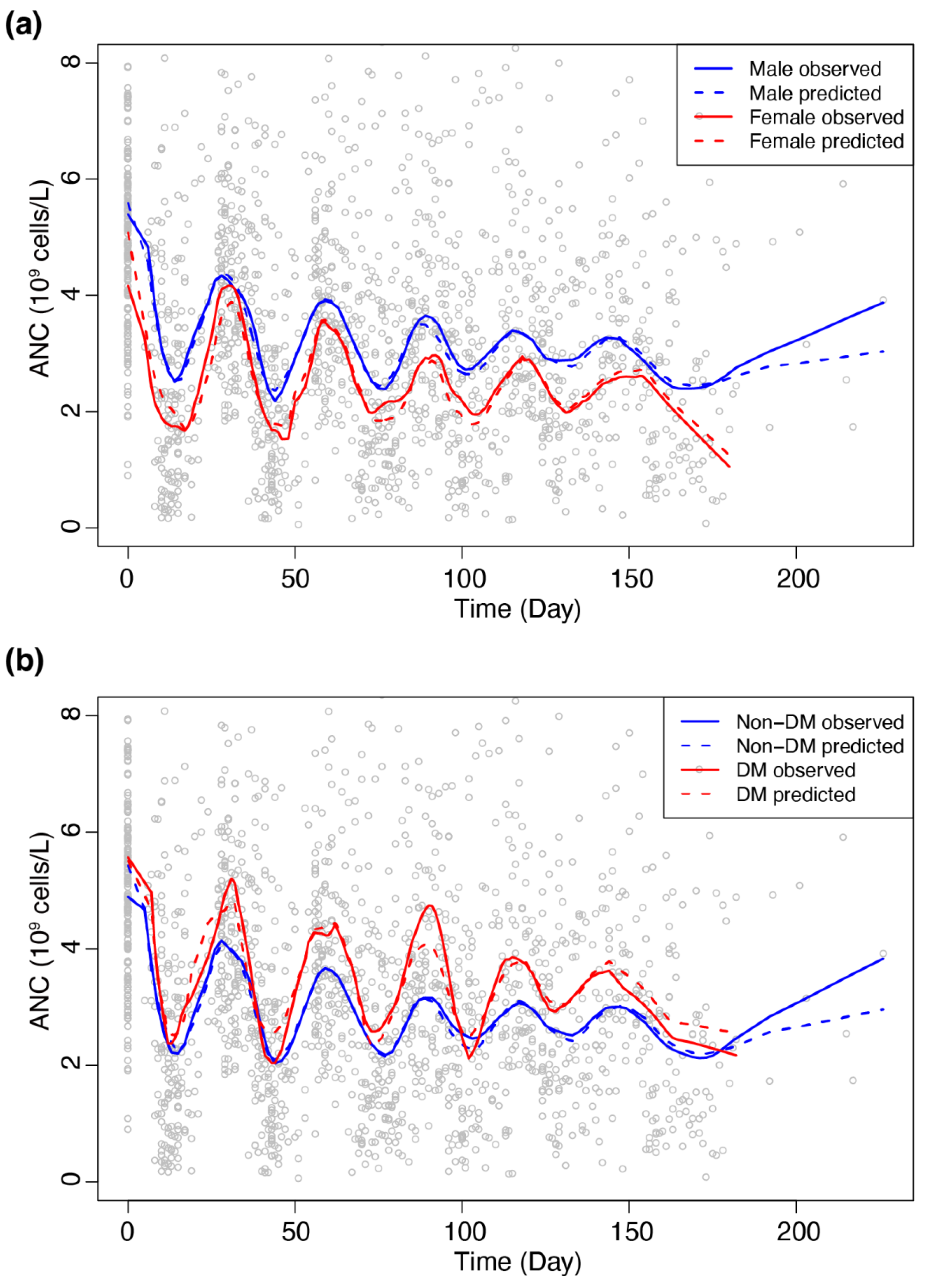
3.6. Sub-Group Analyses
3.7. A Web Application for a New Patient’s ANC Prediction
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- US Department of Health and Human Services, National Institutes of Health, National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) v5.0. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 21 January 2022).
- Friberg, L.E.; Henningsson, A.; Maas, H.; Nguyen, L.; Karlsson, M.O. Model of Chemotherapy-Induced Myelosuppression With Parameter Consistency Across Drugs. J. Clin. Oncol. 2002, 20, 4713–4721. [Google Scholar] [CrossRef] [PubMed]
- Henrich, A.; Joerger, M.; Kraff, S.; Jaehde, U.; Huisinga, W.; Kloft, C.; Parra-Guillen, Z.P. Semimechanistic Bone Marrow Exhaustion Pharmacokinetic/Pharmacodynamic Model for Chemotherapy-Induced Cumulative Neutropenia. J. Pharmacol. Exp. Ther. 2017, 362, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Krzyzanski, W.; Wiczling, P.; Lowe, P.; Pigeolet, E.; Fink, M.; Berghout, A.; Balser, S. Population Modeling of Filgrastim PK-PD in Healthy Adults Following Intravenous and Subcutaneous Administrations. J. Clin. Pharmacol. 2010, 50, 101S–112S. [Google Scholar] [CrossRef] [PubMed]
- Ramon-Lopez, A.; Nalda-Molina, R.; Valenzuela, B.; Perez-Ruixo, J.J. Semi-Mechanistic Model for Neutropenia after High Dose of Chemotherapy in Breast Cancer Patients. Pharm. Res. 2009, 26, 1952–1962. [Google Scholar] [CrossRef] [PubMed]
- Keizer, R.J.; ter Heine, R.; Frymoyer, A.; Lesko, L.J.; Mangat, R.; Goswami, S. Model-Informed Precision Dosing at the Bedside: Scientific Challenges and Opportunities. CPT Pharmacomet. Syst. Pharmacol. 2018, 7, 785–787. [Google Scholar] [CrossRef] [PubMed]
- Jacqmin, P.; Snoeck, E.; van Schaick, E.A.; Gieschke, R.; Pillai, P.; Steimer, J.-L.; Girard, P. Modelling Response Time Profiles in the Absence of Drug Concentrations: Definition and Performance Evaluation of the K–PD Model. J. Pharmacokinet. Pharmacodyn. 2007, 34, 57–85. [Google Scholar] [CrossRef] [PubMed]
- Cockcroft, D.W.; Gault, M.H. Prediction of Creatinine Clearance from Serum Creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Kallner, A.; Ayling, P.A.; Khatami, Z. Does EGFR Improve the Diagnostic Capability of S-Creatinine Concentration Results? A Retrospective Population Based Study. Int. J. Med. Sci. 2008, 5, 9–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twomey, P.J.; Reynolds, T.M. The MDRD Formula and Validation. QJM 2006, 99, 804–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minto, C.F.; Schnider, T.W.; Short, T.G.; Gregg, K.M.; Gentilini, A.; Shafer, S.L. Response Surface Model for Anesthetic Drug Interactions. Anesthesiology 2000, 92, 1603–1616. [Google Scholar] [CrossRef] [PubMed]
- Sandström, M.; Lindman, H.; Nygren, P.; Johansson, M.; Bergh, J.; Karlsson, M.O. Population Analysis of the Pharmacokinetics and the Haematological Toxicity of the Fluorouracil-Epirubicin-Cyclophosphamide Regimen in Breast Cancer Patients. Cancer Chemother. Pharmacol. 2006, 58, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Maier, C.; Hartung, N.; Wiljes, J.; Kloft, C.; Huisinga, W. Bayesian Data Assimilation to Support Informed Decision Making in Individualized Chemotherapy. CPT Pharmacomet. Syst. Pharmacol. 2020, 9, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Lindbom, L.; Pihlgren, P.; Jonsson, E.N.; Jonsson, N. PsN-Toolkit—A Collection of Computer Intensive Statistical Methods for Non-Linear Mixed Effect Modeling Using NONMEM. Comput. Methods Programs Biomed. 2005, 79, 241–257. [Google Scholar] [CrossRef] [PubMed]
- Lindbom, L.; Ribbing, J.; Jonsson, E.N. Perl-Speaks-NONMEM (PsN)—A Perl Module for NONMEM Related Programming. Comput. Methods Programs Biomed. 2004, 75, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Soto, E.; Banfield, C.; Gupta, P.; Peterson, M.C. Kinetic-Pharmacodynamic Model of Platelet Time Course in Patients With Moderate-to-Severe Atopic Dermatitis Treated With Oral Janus Kinase 1 Inhibitor Abrocitinib. CPT Pharmacomet. Syst. Pharmacol. 2020, 9, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Crawford, J.; Glaspy, J.A.; Stoller, R.G.; Tomita, D.K.; Vincent, M.E.; McGuire, B.W.; Ozer, H. Final Results of a Placebo-Controlled Study of Filgrastim in Small-Cell Lung Cancer: Exploration of Risk Factors for Febrile Neutropenia. Support. Cancer Ther. 2005, 3, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Alenzi, E.O.; Kelley, G.A. The Association of Hyperglycemia and Diabetes Mellitus and the Risk of Chemotherapy-Induced Neutropenia among Cancer Patients: A Systematic Review with Meta-Analysis. J. Diabetes Complicat. 2017, 31, 267–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferraro, F.; Lymperi, S.; Méndez-Ferrer, S.; Saez, B.; Spencer, J.A.; Yeap, B.Y.; Masselli, E.; Graiani, G.; Prezioso, L.; Rizzini, E.L.; et al. Diabetes impairs hematopoietic stem cell mobilization through alteration of niche function. Sci. Transl. Med. 2011, 3, 104ra101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadini, G.P.; Albiero, M.; Vigili de Kreutzenberg, S.; Boscaro, E.; Cappellari, R.; Marescotti, M.; Poncina, N.; Agostini, C.; Avogaro, A. Diabetes Impairs Stem Cell and Proangiogenic Cell Mobilization in Humans. Diabetes Care 2013, 36, 943–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Herbst, R.S.; Boshoff, C. Toward Personalized Treatment Approaches for Non-Small-Cell Lung Cancer. Nat. Med. 2021, 27, 1345–1356. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network None-Small Cell Lung Cancer (Version 1.2022). Available online: https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf (accessed on 21 January 2022).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (a) Continuous Variables | ||
|---|---|---|
| Variable | Mean (±SD) | Median (Min, Max) |
| Baseline ANC (106 cells/L) | 5521 (±2328) | 5183 (901, 17,080) |
| White blood cell count (109 cells/L) | 8.25 (±2.58) | 7.93 (2.14, 20.63) |
| Height (cm) | 164.3 (±8.6) | 165.0 (140.0, 186.0) |
| Body weight (kg) | 63.5 (±11.3) | 63.1 (38.0, 107.0) |
| Body surface area (m2) | 1.70 (±0.18) | 1.70 (1.24, 2.30) |
| ALT (IU/L) | 21.0 (±16.2) | 16 (6, 126) |
| AST (IU/L) | 21.4 (±12.8) | 18.0 (8.0, 112.0) |
| Creatinine (mg/dL) | 0.86 (±0.19) | 0.83 (0.43, 1.82) |
| Total bilirubin | 0.51 (±0.21) | 0.50 (0.10, 1.40) |
| CLcr (mL/min) | 81.0 (±23.6) | 75.7 (36.8, 153.6) |
| eGFR (mL/min/1.73 m2) | 86.2 (±13.3) | 90.0 (55.0, 130.6) |
| Age (years) | 61.0 (±9.2) | 62.0 (38.0, 82.0) |
| Primary tumor size (cm) (n = 145) | 4.7 (±2.3) | 4.3 (0.9, 17.0) |
| (b) Categorical Variables | ||
| Variable | n (%) | |
| Sex (male/female) | 127 (73.4)/46 (26.6) | |
| Hypertension (no/yes) | 88 (50.9)/85 (49.1) | |
| Diabetes mellitus (no/yes) | 141 (81.5)/32 (18.5) | |
| Tuberculosis (no/yes) | 152 (87.9)/21 (12.1) | |
| ECOG (0/1) | 149 (86.1)/24 (13.9) | |
| Smoker (Non/Current/Ex) | 51 (29.5)/72 (41.6)/50 (28.9) | |
| Stage (IIIB/IV) | 43 (24.9)/130 (75.1) | |
| Histology (Ad/Sq/Un) | 119 (68.8)/50 (28.9)/4 (2.3) | |
| Overall response (PR/SD/PD) | 45 (26.0)/55 (31.8)/73 (42.2) | |
| Treated cycles (2/3/4/5/6) | 8 (4.6)/37 (21.4)/27 (15.6)/12 (6.9)/89 (51.5) | |
| G-CSF treatment (no/yes) | 136 (78.6)/37 (21.4) | |
| Parameters | Estimate | RSE% | Bootstrap Median | 95% CI | Bootstrap RSE% |
|---|---|---|---|---|---|
| Circ0 (109 cells/L) | 5.34 | 2.8 | 5.34 | 5.10–5.60 | 2.8 |
| MTT (D) | 4.64 | 3.3 | 4.69 | 4.44–5.08 | 4.2 |
| γ | 0.188 | 6.4 | 0.193 | 0.173–0.214 | 6.6 |
| IR50 (mg/D) | : 88.9 | 7.8 | 86.6 | 74.0–104.3 | 10.9 |
| : −0.334 | 16.4 | −0.323 | −0.433 to −0.222 | 19.9 | |
| : 0.485 | 31.5 | 0.483 | 0.222–0.770 | 35.2 | |
| KDEp (/D) | 0.0326 | 13.2 | 0.0343 | 0.0240–0.0497 | 22.6 |
| KDEc (/D) | 0.188 | 24.5 | 0.176 | 0.122–0.353 | 40.9 |
| 3.50 | 8.7 | 3.48 | 2.26–4.69 | 19.8 | |
| 0.217 | 8.5 | 0.226 | 0.163–0.291 | 16.2 | |
| IIV of Circ0 (CV%) | 23.0 | 11.4 | 23.1 | 20.5–25.8 | 6.8 |
| IIV of MTT (CV%) | 16.2 | 16.3 | 15.7 | 12.3–18.7 | 13.6 |
| IIV of IR50 (CV%) | 23.3 | 24.5 | 24.0 | 12.4–34.3 | 28.2 |
| IIV of KDEp (CV%) | 95.6 | 13.8 | 88.7 | 58.4–110.9 | 19.1 |
| IIV of KDEc (CV%) | 92.0 | 24.1 | 93.1 | 70.5–113.5 | 14.8 |
| Residual Variability | Estimate | RSE% | Bootstrap Median | 95% CI | |
| σprop (CV(%)) | 30.0 | 3.9 | 29.3 | 26.2–32.8 | 6.6 |
| σadditive (109 cells/L) | 0.527 | 8.5 | 0.535 | 0.384–0.663 | 15.5 |
| Non-DM Patients (n = 141) | DM Patients (n = 32) | p-Value | |
|---|---|---|---|
| Continuous factors | |||
| Age (years) | 60.2 (±9.5) | 64.5 (±6.7) | 0.004 |
| Height (cm) | 164.1 (±8.8) | 165.3 (±7.7) | 0.418 |
| Body weight (kg) | 62.5 (±11.1) | 68.1 (±11.2) | 0.011 |
| Body surface area (m2) | 1.68 (±0.18) | 1.76 (±0.16) | 0.016 |
| ALT (IU/L) | 20.1 (±14.5) | 25.0 (±22.1) | 0.133 |
| AST (IU/L) | 21.1 (±11.2) | 22.7 (±18.3) | 0.726 |
| Creatinine (mg/dL) | 0.84 (±0.18) | 0.93 (±0.23) | 0.036 |
| Total bilirubin | 0.50 (±0.20) | 0.52 (±0.22) | 0.872 |
| CLcr (mL/min) | 81.8 (±23.9) | 77.7 (±22.3) | 0.513 |
| eGFR (mL/min/1.73 m2) | 87.0 (±13.6) | 82.7 (±11.3) | 0.056 |
| Categorical factors | |||
| Female sex | 40 (28.4%) | 6 (18.8%) | 0.375 |
| Hypertension | 64 (45.4%) | 21 (65.6%) | 0.050 |
| Tuberculosis | 15 (10.6%) | 6 (18.8%) | 0.231 |
| ECOG | >0.999 | ||
| 0 | 121 (85.8%) | 28 (87.5%) | |
| 1 | 20 (14.2%) | 4 (12.5%) | |
| Smoker | 0.338 | ||
| Non | 45 (31.9%) | 6 (18.8%) | |
| Current | 57 (40.4%) | 15 (46.9%) | |
| Ex | 39 (27.7%) | 11 (34.4%) | |
| Stage | >0.999 | ||
| IIIB | 35 (24.8%) | 8 (25.0%) | |
| IV | 106 (75.2%) | 24 (75.0%) | |
| Histology | 0.926 | ||
| Adenocarcinoma | 97 (68.8%) | 22 (68.8%) | |
| Squamous cell cancer | 40 (28.4%) | 10 (31.2%) | |
| Unspecfied | 4 (2.84%) | 0 (0%) | |
| Overall response | 0.447 | ||
| PR | 34 (24.1%) | 11 (34.4%) | |
| SD | 45 (31.9%) | 10 (31.2%) | |
| PD | 62 (44.0%) | 11 (34.4%) | |
| Treated cycles | 0.980 | ||
| 2 | 7 (5.0%) | 1 (3.1%) | |
| 3 | 31 (22.0%) | 6 (18.8%) | |
| 4 | 21 (14.9%) | 6 (18.8%) | |
| 5 | 10 (7.1%) | 2 (6.3%) | |
| 6 | 72 (51.1%) | 17 (53.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, K.; Kim, Y.; Son, M.; Chae, D.; Park, K. A Pharmacometric Model to Predict Chemotherapy-Induced Myelosuppression and Associated Risk Factors in Non-Small Cell Lung Cancer. Pharmaceutics 2022, 14, 914. https://doi.org/10.3390/pharmaceutics14050914
Park K, Kim Y, Son M, Chae D, Park K. A Pharmacometric Model to Predict Chemotherapy-Induced Myelosuppression and Associated Risk Factors in Non-Small Cell Lung Cancer. Pharmaceutics. 2022; 14(5):914. https://doi.org/10.3390/pharmaceutics14050914
Chicago/Turabian StylePark, Kyemyung, Yukyung Kim, Mijeong Son, Dongwoo Chae, and Kyungsoo Park. 2022. "A Pharmacometric Model to Predict Chemotherapy-Induced Myelosuppression and Associated Risk Factors in Non-Small Cell Lung Cancer" Pharmaceutics 14, no. 5: 914. https://doi.org/10.3390/pharmaceutics14050914