

The Impact of Sex on the Response to Proton Pump Inhibitor Treatment


1
Department of Internal Medicine, Haraldsplass Diaconal Hospital, 5009 Bergen, Norway
2
Department of Gastroenterology, Haukeland University Hospital, 5009 Bergen, Norway
3
Department of Gastroenterology, Landspitali University Hospital, 101 Reykjavik, Iceland
4
Faculty of Medicine, University of Iceland, 101 Reykjavik, Iceland
*
Author to whom correspondence should be addressed.
Pharmaceuticals 2023, 16(12), 1722; https://doi.org/10.3390/ph16121722
Submission received: 8 November 2023
/
Revised: 5 December 2023
/
Accepted: 7 December 2023
/
Published: 12 December 2023
(This article belongs to the Special Issue Sex Differences in Pharmaceutical Practice)
Abstract
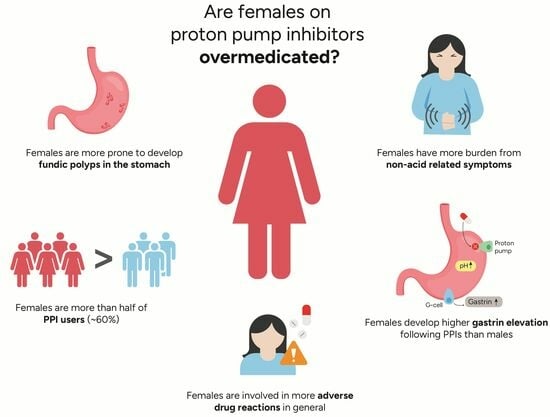
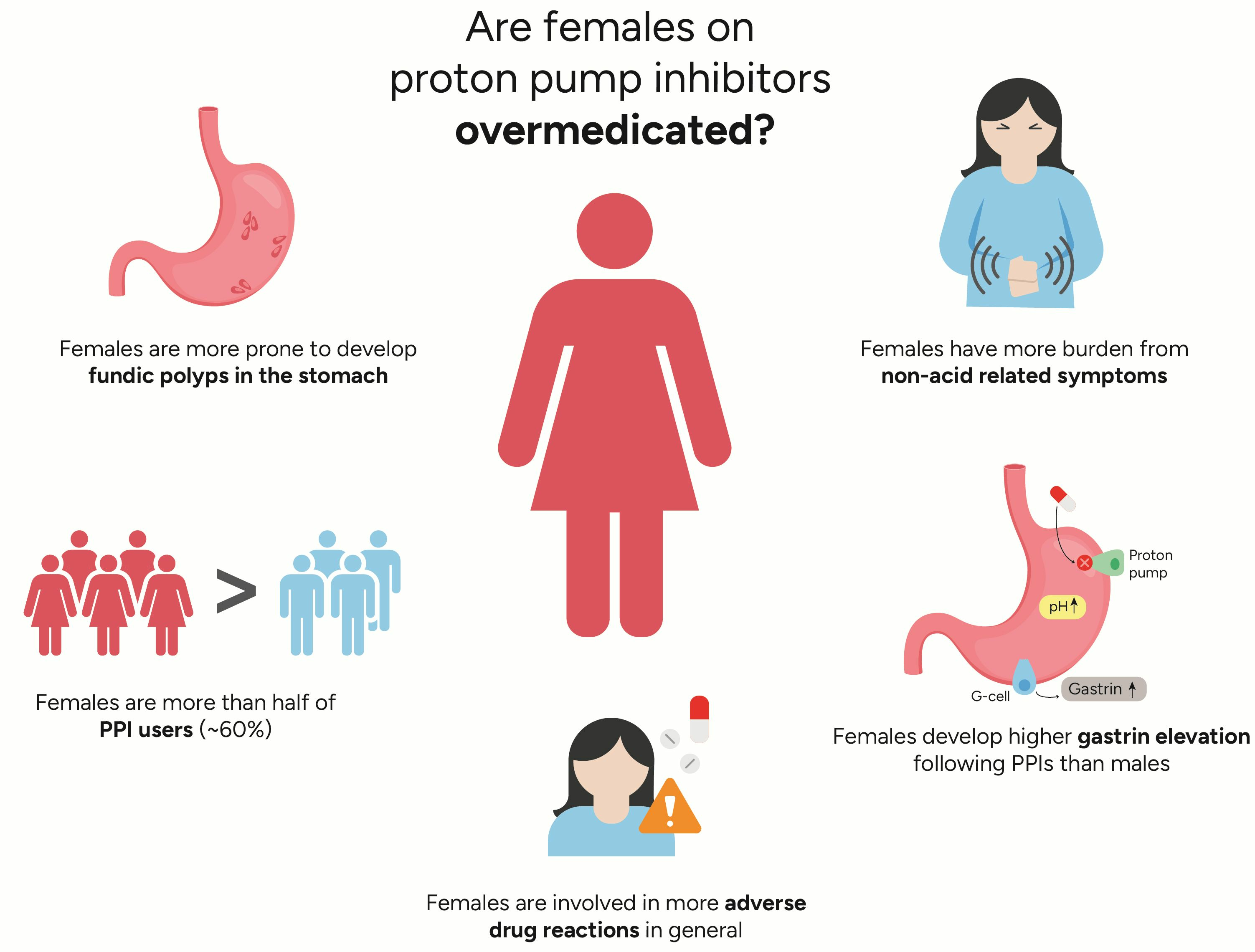
:Proton pump inhibitor (PPI) treatment is responsible for substantial gastrin elevation secondary to reduced intragastric acidity. Due to the increasing global prevalence of PPI users, concerns have been raised about the clinical significance of continuous gastrin elevation and its potential long-term side effects. Hypergastrinemia secondary to PPIs has trophic effects on gastric mucosa, leading to enterochromaffin-like cell hyperplasia and gastric (fundic) polyp formation, and it is believed to provoke acid rebound following PPI withdrawal that induces PPI overutilization. Previous studies have found higher gastrin release following PPI therapy in females compared with males, and sex differences have also been demonstrated in pharmacokinetic parameters and dose requirements for acid reflux. It is conceivable that females might be at increased risk of PPI overuse, because they often receive higher milligram-per-kilogram doses. The prevalence of PPI use is more common among females, and the female sex is a risk factor for adverse drug reactions. This non-systematic review outlines the current knowledge of the impact of biological sex on the response to PPIs. The aim is to highlight the female sex as a potential risk factor that could be a step toward precision medicine and should be considered in future research on the response to PPI treatment.
1. Introduction
A recent literature review showed that compared with males, females were involved in more adverse drug reaction (ADR) reports [1]. Studies on specific types of drugs illustrating this sex difference and the underlying pathophysiology are important. Proton pump inhibitors (PPIs) are by far the most used acid-suppressive drugs and constitute the first-choice treatment for gastric acid-related disorders [2]. The major adequate indications for their use are treatment of gastro-esophageal reflux disease, peptic ulcers, eradication of Helicobacter pylori infection in combination with antibiotics, and ulcer prophylaxis for patients on non-steroidal anti-inflammatory or antiplatelet drugs [3]. Since their introduction in clinical practice over 30 years ago, their therapeutic success has been accompanied by a dramatic rise in the prevalence of PPI users [4]. PPIs are currently among the most prescribed of all drugs, and the rate of PPI use continues to increase. Similar to other drugs, PPIs have some side effects, and there is considerable concern regarding their long-term safety. One of these long-standing concerns is PPI-induced gastrin elevation secondary to hypoacidity. Profound acid inhibition by PPIs leads to gastrin elevation. Gastrin is a growth hormone, and concerns have been raised regarding its potent trophic effects: gastric polyp formation and potential progression to dysplasia following long-term acid suppression [5]. PPI-induced gastrin elevation is also believed to play a role in rebound hyperacidity when PPIs are discontinued [6,7,8,9]. This could induce dyspeptic symptoms that might result in the resumption of PPI therapy. This rebound acid hypersecretion (RAHS) is believed to result from gastrin’s hypertrophic effects on enterochromaffin-like (ECL) cells in the stomach [8,9]. RAHS leads to increased acid production after therapy is discontinued, which might partly explain the increasing prevalence of overall PPI use [6,7]. PPIs are generally well tolerated and considered safe drugs, which might also play a role in the overutilization and inappropriate long-term use of the drugs [10,11]. Therefore, using the lowest effective dose for the shortest possible time has been the mainstream method employed to promote long-term safety. Careful consideration by prescribers of the appropriate indication, as well as the dose and duration of treatment, is necessary in the determination of the benefit–harm balance of PPI therapy. Only a few studies have aimed to investigate the impact of sex on PPI treatment, and some of the findings on sex differences indicate that compared with males, females might be more sensitive to PPIs’ inhibitory effects on acid secretion and induced gastrin release [12,13]. Gender difference may also exist in PPI indications, symptom perception, and other pre-treatment factors not related to acid regurgitation that affect the PPI response [14,15,16]. One of these factors is PPI metabolism and pharmacogenetics [17]. A review of 12 pharmacokinetic studies from 2001 suggested a sex-related difference in the pharmacokinetic parameters, where the area under the curve (AUC) and maximum concentrations (Cmax) values were approximately 30% higher in females than in males after a single dose [18]. The practitioner’s consideration of sex and gender as a possible factor contributing to PPI treatment response is not a mainstream approach but might be appropriate. This review is based on a non-systematic search in PubMed and the authors’ own clinical experience and research, and the aim is to highlight a few reasons why considering the female sex as a risk factor could be an appropriate step toward precision medicine that would probably benefit individualized treatment. In this review, the term sex refers to the biological and physiological characteristics, and gender refers to the socioeconomic or cultural distinctions and roles associated with being male or female [19].
2. Association between Female Sex and Increased Gastrin Release Following PPIs
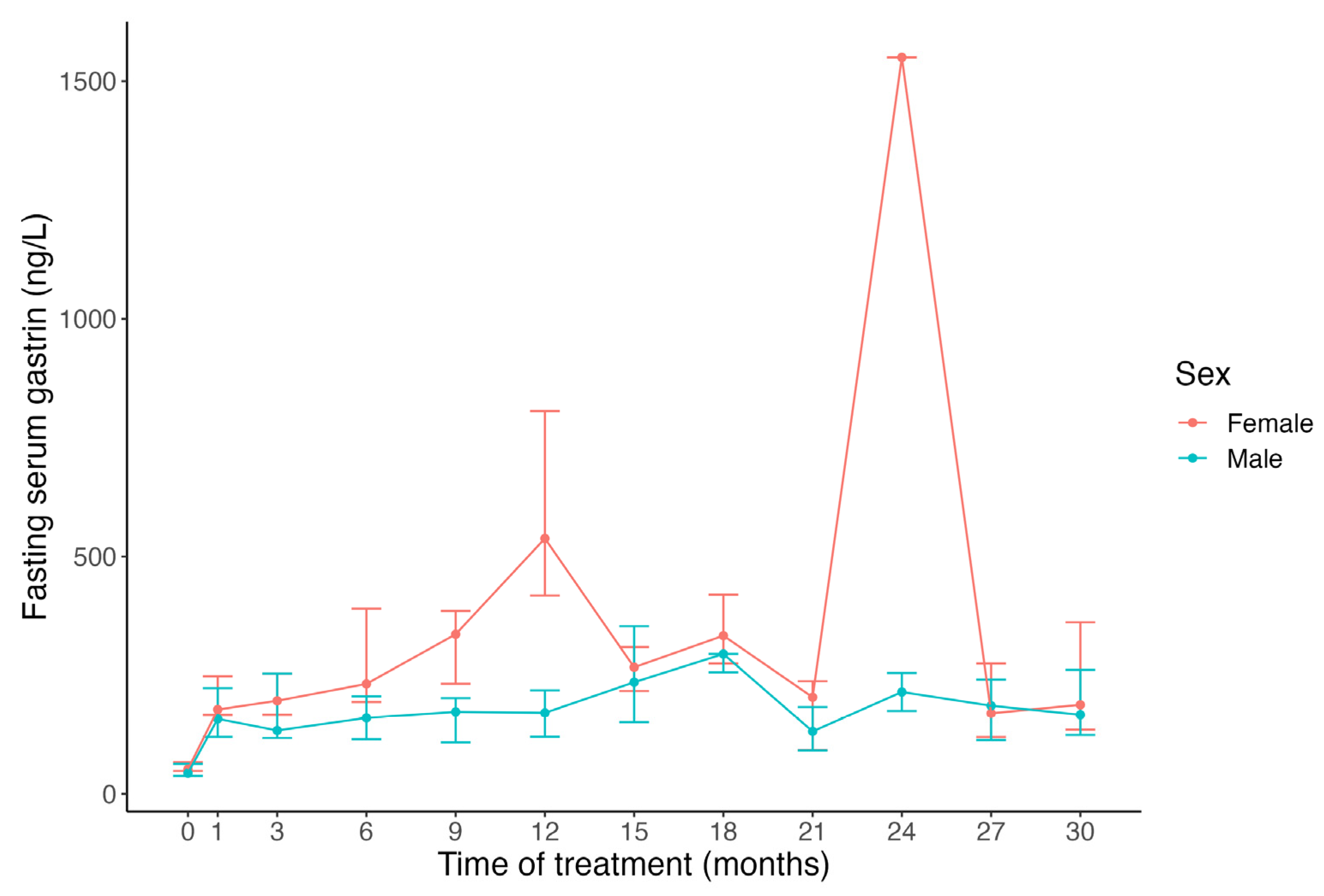
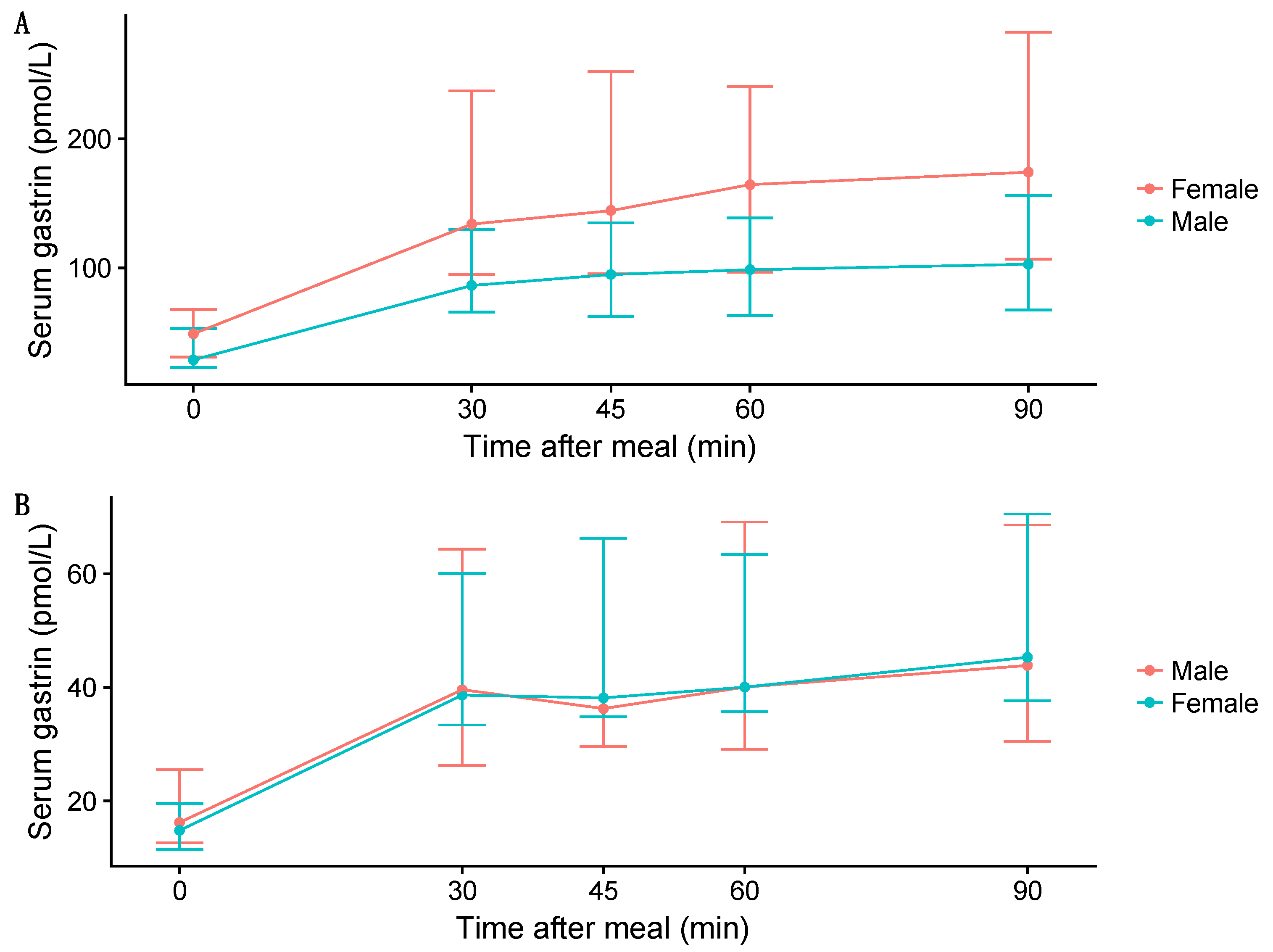
It is widely accepted that all individuals undergoing PPI treatment develop varying degrees of gastrin elevation [20,21]. Currently, there is limited information on which individuals are likely to develop significant hypergastrinemia, defined as gastrin levels above the upper limit of the reference range for fasting blood gastrin. Serum gastrin levels during PPI treatment have been positively correlated with basal gastrin levels prior to PPI treatment [22,23]. This suggests an individual effect, beyond PPI and acid inhibition itself, that likely contributes to enhanced gastrin levels. Demographics that have been associated with higher gastrin levels include H. pylori infection [24], atrophic gastritis [25], age [26], and sex [20,21]. Shortly after the introduction of PPIs in the late 1980s, it was reported that females were more likely to develop higher gastrin levels early in the course of omeprazole treatment, reaching statistically significant differences at 18 and 21 months (Figure 1) [22]. Since the turn of the 21st century, many researchers have studied PPIs’ long-term effect on gastrin, mainly on the fasting serum gastrin values, but only a limited number of these studies have included sex-disaggregated data [27,28]. A significant sex difference was reported again in 2014, with higher basal and meal-stimulated serum gastrin levels among females than males on long-term PPI therapy for gastroesophageal reflux disease (GERD), whereas such sex difference was not observed in healthy controls who were not on PPIs (Figure 2) [28].
Previous studies that examined sex difference in gastrin response among healthy subjects and patients showed conflicting results, while suggesting a sex-related difference in gastrin release. The results of 11 studies with published sex-disaggregated data on gastrin release and/or gastrin elevation in healthy volunteers and patients on PPIs are listed in Table 1. Interestingly, if sex difference was found, gastrin levels were higher in females than in males. Despite the sex difference among healthy subjects, as reported in the literature throughout the 20th century, sex difference is rarely documented in papers about PPI-induced gastrin elevation. Sex difference in gastrin release among PPI users is still incompletely defined, with a limited number of studies examining sex-related differences. Likewise, most of the studies listed in Table 1 measured fasting serum gastrin levels, whereas only a few studies evaluated meal-stimulated gastrin concentrations and the area under the meal-stimulated gastrin curve, which are better indicators of hypergastrinemia [30,31]. A single fasting gastrin measurement might underestimate the hormone production, because gastrin levels are at their lowest point during overnight fasting. Daily fluctuations in gastrin levels continue in patients on PPIs—but to a higher degree [32]. High degrees of intra- and inter-individual variations in serum gastrin levels were observed in previous studies, supporting the argument that repeated sampling of gastrin levels on different days or meal-stimulated measurements might provide better estimates of chronic gastrin elevation [27,28,31]. The reason for the observed sex difference in gastrin response induced by PPI therapy remains unclear. Table 2 presents a list of possible factors that could contribute to sex-related differences in gastrin release in healthy subjects and gastrin elevation secondary to PPI therapy.
3. Role of Sex in Metabolism of PPIs
PPIs undergo low rates of first-pass hepatic metabolism, and the oral bioavailability of PPIs is high. Additionally, the rate of protein binding is >95% and independent of sex [18,47]. PPIs are metabolized in the liver by cytochrome P450 (CYP) enzymes, known to show marked inter-individual and inter-ethnic variations. CYP2C19 and CYP3A4 are the two enzymes mainly involved in the metabolism of PPIs [18,45]. All PPIs, except rabeprazole, rely significantly on CYP2C19 for their clearance [48]. Sex difference in the expression and activity of CYP2C19 and CYP3A4 has been reported [46,49,50,51,52]. Generally, PPIs have similar efficacy, although they have some differences regarding their pharmacokinetics and pharmacodynamics. PPI effectiveness can also vary, depending on each PPI’s affinity to the CYP2C19 enzyme.
A review of 12 pharmacokinetic studies suggested a sex difference in two pharmacokinetic parameters [18]. The area under the curve (AUC) and maximum concentration (Cmax) values were approximately 30% higher in females than in males after a single dose, with less difference during repeated administration of esomeprazole 40 mg during fasting conditions [18]. This might be due to the differences in CYP2C19 and CYP3A4 expression between the two sexes. It was previously shown that females had higher CYP3A4 activity than males, whereas CYP2C19 activity was lower in females [50]. In a large population study involving Dutch Caucasians, CYP2C19 activity was 40% greater in males than in females [51]. Other possible explanations might be differences in body weight (higher in males than in females) or volume of distribution (Vd), with females having a higher percentage of body fat than males [46]. A study in Iran found that females on omeprazole had higher weight-normalized Vd and clearance (Cl) [45]. The authors suggested that these sex differences might be explained by sex differences in metabolism and body fat percentage, respectively [45]. However, another study in Iceland on the pharmacokinetics of esomeprazole in healthy males and females found no sex difference in the pharmacokinetic parameters after a single dose or repeated doses for five days [38].
The pharmacokinetic parameters may also greatly differ by the CYP2C19 genotype, including extensive metabolizers (EMs), intermediate metabolizers (IMs), and poor metabolizers (PMs), and this can cause considerable inter-individual and -ethnic variation in the PPI metabolism [17]. PPIs are rapidly eliminated from systemic circulation in individuals with the EM genotype, resulting in markedly lower plasma PPI concentrations than those observed in individuals with the PM genotype [47]. The genotype may therefore influence the PPI response, with risk of under-treatment (partial symptom response or non-response) among EMs and risk of over-treatment among PMs (adverse events, unnecessary expense) [17]. In one of the studies that reported hypergastrinemia more frequently in females on long-term PPI use, CYP2C19 polymorphisms were also assessed, but no significant difference in median gastrin levels was found dependent on CYP2C19 gene polymorphisms (EM vs. IM vs. PM) [20]. It remains unclear whether the pharmacokinetics of PPIs play a role in the previously described sex difference in secondary gastrin response (other possible factors are listed in Table 2).
4. Is There a Need for Sex-Specific PPI Dosage?
The female sex and PPI dosage seem to perform an important function in the development of hypergastrinemia during PPI treatment [21]. Several studies have found higher gastrin levels in patients on higher PPI doses [21,53,54,55]. The elevated serum gastrin levels observed in patients exposed to higher PPI doses (in milligrams per day) are likely the effect of gastric acid inhibition. Gastrin elevation is correlated with the degree of acid inhibition by PPIs, measured by the fasting intragastric pH level [56,57]. It is known that females have smaller stomachs and parietal cell masses than males [39,40], and it is conceivable that the PPI doses used in females are higher than necessary to inhibit acid secretion in order to obtain symptomatic relief. In other words, compared with males, females might be more sensitive to PPIs’ inhibitory effects on acid secretion and induced gastrin release. A randomized clinical trial found that female gastroesophageal reflux disease (GERD) patients on long-term PPIs were three times more likely than males to tolerate a 50% reduction in their prior doses over an 8-week period [12]. The female sex was the only independent predictor of a successful step-down, though with only a modest odds ratio (OR: 1.3 [95% CI: 1.01–1.6]). In another step-down study, male patients were less likely to be candidates for a step-down because of the worse control of their GERD symptoms despite twice-daily PPI use initially [13]. This sex difference also did not reach statistical significance; female patients who did not retain heartburn control after the therapy switch had an OR of 0.499 (95% CI: 0.178–1.396) [13]. The reason why the sex difference did not reach statistical significance in these two studies might be the relatively small sample sizes of the step-down groups, with 50 (25 females) and 142 (80 females) participants, respectively [12,13]. To date, a limited number of deprescribing studies have provided information on the differences between the sexes (Table 3) [12,13,58,59]. Female participants were also underrepresented in previous step-down research, accounting for <5% of the total study population in a couple of studies [60,61]. However, the above-mentioned sex-specific findings on PPI dose requirements suggest that females need lower PPI doses than males do to obtain relief from acid-related symptoms.
5. Overuse or Overmedication of PPIs among Females
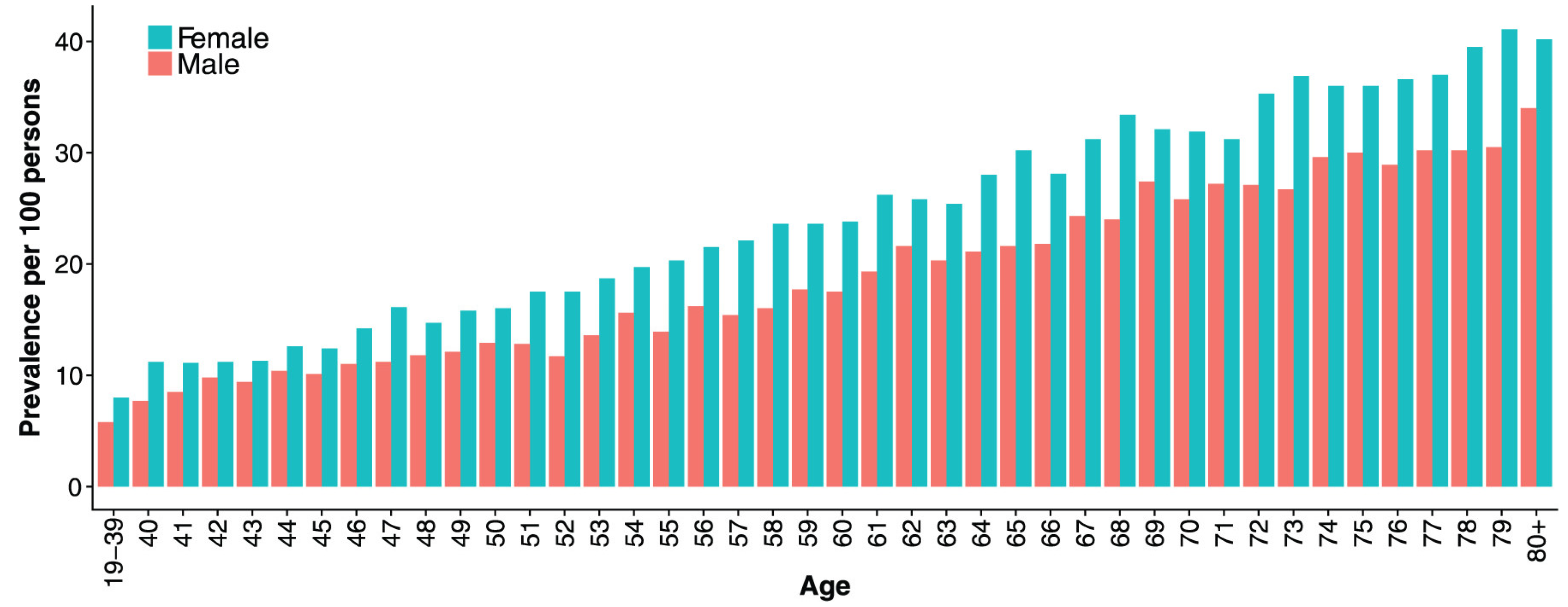
In recent years, concerns have been raised about the increasing prevalence of patients on long-term PPI therapy. Although the incidence of new therapy with PPIs remains stable, the prevalence of PPI therapy continues to rise [4,62,63]. Some studies have shown that females generally use PPIs more often than males [4,62,64,65]. In a recent systematic review that described global PPI use patterns by demographics, females comprised 56% of PPI users in the general population; 60 of the 65 studies included in the analysis provided sex information [66]. The same review reported that nearly two-thirds of the users were on high doses (≥defined daily dose (DDD)) [66]. Similar to almost all types of drugs, PPI dosage has not been sex-specific, but females often receive higher milligram/kilogram doses than males. A nationwide drug utilization study from Iceland that described the outpatient PPI use among the entire adult population found that in addition to the rising prevalence of PPI use across time, the prevalence increased with higher age and was higher among females than males in all age groups (Figure 3) [62]. In addition, long-term PPI use (over 1 year) was highest among the elderly population, and they are also generally at greater risk for polypharmacy and adverse drug reactions because of the metabolic changes associated with ageing [62,67].
Serum gastrin was found to be an independent predictor of PPI requirement in a study on the discontinuation of PPIs after long-term treatment [58]. Studies on RAHS in patients after their long-term PPI therapy are largely lacking. RAHS is believed to contribute to difficulties in the discontinuation of treatment and in acid rebound, which might explain—at least partly—the increase in long-term users without an adequate indication of needing PPIs [68]. Concerns have been raised about this physical dependence on PPIs and its potential complications and economic consequences [69]. It has also been hypothesized that the increase in reflux disease incidence over recent decades may be due to the worsening of reflux symptoms caused by RAHS; in other words, PPI therapy for reflux symptoms might be worsening the disease itself [9]. It is conceivable that although females might need lower doses of PPIs to control their acid-related symptoms, they might be more at risk of RAHS due to elevated gastrin levels, which in turn might contribute to their higher prevalence of PPI use. However, this needs to be investigated in clinical studies.
In post-hoc analysis, partial PPI treatment response is more common in non-erosive reflux disease (NERD) than in reflux esophagitis [70] and has been associated with the female gender [14]. Since NERD is more common in females, this might explain the gender difference in PPI response, because NERD is less often caused by acidic reflux [16,70]. Among 580 GERD patients who responded partially to PPIs, a history of reflux esophagitis was significantly higher in males than in females (24% vs. 11%) [14]. In the same analysis, females had significantly more burdens from extra-esophageal symptoms, abdominal pain, indigestion, and constipation [14]. The prevalence of anxiety, depression, and use of antidepressants was also significantly higher among females than males [14]. The authors suggested that these comorbidities increased symptom burden in females and might contribute to their partial PPI response [14]. Another post-hoc analysis showed that females with GERD were more likely to need dose escalation because of inadequate symptom control [71]. Of the 99 patients (33 females) who needed dose escalation, one-third could return to the lower dosage over the coming years, but those patients’ characteristics were not mentioned [71]. In a multicenter prospective observational study, which included 182 Japanese patients with symptomatic GERD (62 females (34%)), a multiple regression analysis found the following pre-treatment factors to be associated with residual symptom rate: milder GERD symptoms, absence of esophagitis, severer epigastric pain/ burning symptoms, lower BMI, and severer depression [15].
PPIs are widely prescribed today, not only for acid-related disorders but frequently also for a variety of upper gastrointestinal (GI) conditions not necessarily related to acid, partly due to a lack of other therapeutic modalities for upper GI symptoms, often minor symptoms with unidentifiable causes (dyspepsia). PPIs are beneficial to those who have appropriate indications but obviously not to those who have inappropriate indications. With the increase in long-term PPI use in patients with inappropriate indications, the risks of long-term PPI use must be weighed against the benefits. Inappropriate PPI use has not been associated with any gender, but it has been associated with older age, non-steroidal anti-inflammatory and anti-platelet drugs [72], and polypharmacy in elderly patients [73].
As pointed out, the prevalence of global PPI use in the general population has been shown to be more common among females [66]. Among others, heartburn, regurgitation, and extra-esophageal symptoms have been more frequently reported by women than by men, suggesting that sex and gender play a role in symptom perception [16]. Research on lower PPI response among females also suggests that comorbid anxiety and depression may contribute to the increased symptom burden in females [14]. PPIs are also widely used by pregnant and breastfeeding women, since GERD is one of the most common medical complaints during pregnancy [74]. In contrast, males seem to have a higher prevalence of pathologic acid-related diseases, such as reflux esophagitis, Barrett’s esophagus (BE), and esophageal adenocarcinoma (EAC), that require continuous maintenance therapy with PPIs [16]. Differential sensitivity with augmented symptoms in females might have diagnostic and therapeutic influences. Therefore, it is important to consider other comorbidities and symptoms not associated with acid that may contribute to the increased symptom burden in females before attempting dose escalation in PPI partial responders or non-responders (Table 4).
6. Side Effects of Secondary Gastrin Elevation
Although PPIs are generally safe, their extensive and increasingly long-term use has led to concerns about the safety of long-term PPI treatment. Although the clinical significance of elevated fasting gastrin levels has not been fully determined, they have a well-documented association with both ECL hyperplasia and increased risk of gastric polyps in humans, especially fundic gland polyps (FGPs) [5,75]. FGPs are the most common gastric polyps arising within fundic gland mucosa in the fundus and body of the stomach [76]. They are known to be associated with PPI use and are generally considered benign [76]. A recent Chinese study on the characteristics of 186 gastric polyps found significantly more polyps in females than in males (with a ratio of 2.4:1), of whom 78% of the total study population were long-term PPI users (>5 years) [77]. In a population of 1005 patients, of whom 441 received acid-suppressive therapy, a multivariate analysis found the female sex to be associated with the prevalence of FGPs and multiple white elevated lesions in gastric mucosa [78]. Although gastrin was not measured in that study, the authors suggested that higher gastrin levels among females might influence the prevalence of multiple white elevated lesions, as well as FGPs [78]. Despite the low rate of dysplasia or carcinoma in FGPs, a summary of 11 cases found that the majority of them involved middle-aged women (65.7%), most of whom were receiving PPI therapy [79]. A theoretical link between gastrin elevation and gastric cancer was previously proposed [80]. Several large cohort studies suggest that PPI use is associated with an increased risk of gastric intestinal metaplasia and gastric cancer with duration and dose-dependent association [81,82]. However, most of these are retrospective observational studies hampered by important methodological weaknesses, and causal relationship has been difficult to demonstrate [81,82]. Although the reported risk is only possible, and the precise underlying mechanism is unclear, the increasing prevalence of PPIs worldwide remains a matter of concern.
7. Other Side Effects of PPIs
Gastrin elevation is only one of many concerns that have been raised parallel to the increase in long-term PPI use with or without appropriate indications [66,83]. The putative adverse effects of long-term PPI therapy are mainly obtained from observational studies in various patient populations with many unmeasured variables [84]. Some have been related to the PPI-induced hypochlorhydria, which has been associated with increased risk for infections (Clostridium difficile infection and pneumonia) and malabsorption of micronutrients (magnesium, calcium, and vitamin B12 deficiencies) [83,84]. Others are idiosyncratic, and the precise molecular mechanism of how they occur is often unclear. These include, for example, increased risk of bone fractures, kidney disease, cardiac disease, and dementia [83,84]. These associations, just like the above-mentioned cancer risk, should be interpreted with caution owing to the lack of high-quality studies exploring these relationships. Pharmacokinetic (PK) interactions are also important when PPIs are prescribed with other drugs, since PPIs competitively inhibit certain CYP enzymes (e.g., CYP2C19) to varying degrees [84].
A recent literature review showed that compared with males, females were involved in more ADR reports [1]. This might be due to gender-related factors, such as females’ higher tendency to report their health conditions compared with that of males. A cross-sectional study of 66,102 subjects who reported ADRs (while taking PPIs) to the Food and Drug Administration (FDA) database between 1997 and 2012 found that more females indicated one or more ADR (57.3%) [85]. Several gender differences in the adverse reactions to PPIs have been reported. A recent study in China demonstrated that women were more likely to develop the PPI-related syndrome of inappropriate antidiuretic secretion (SIADH) [86]. However, the risk of PPI-associated hypomagnesemia was higher in males and in the elderly population [85].
Many of the side effects associated with long-term PPI therapy have been shown to be dose-related [87]. In a recent placebo-controlled study, women on PPI therapy were three times more likely than men on PPI therapy to decrease their PPI doses by half [12]. If the majority of female patients on PPI therapy tend to be overmedicated and could reduce their PPI use, this could lead to major economic benefits for the healthcare system and potentially decrease the risk of side effects associated with long-term PPI use. As pointed out, the female sex has been shown to be a risk factor for clinically relevant ADRs [1,46].
8. Limitations
Our review includes some limitations that need to be addressed. First, this is a non-systematic review. Second, our hypothesis that females might be more sensitive to the inhibitory effect of PPIs is derived from own clinical research. Third, we did not conduct any statistical comparison between included studies. Therefore, we cannot exclude the possibility of selection bias, which may lead to biased conclusions and potentially overestimation of the plausible impact of sex on the response to PPI therapy.
9. Summary and Future Directions
Biological sex and sociocultural gender both seem to contribute to differences in PPI treatment indication, response, and potential outcomes. Secondary gastrin elevation seems to be a dose-dependent response to acid inhibition by PPI therapy, but there are also individual effects underlying the intra- and inter-individual variations in the observed serum gastrin levels following PPI treatment. The role of sex in gastrin elevation has not received much attention, and the inclusion of sex as a variable in studies on gastrin levels in patients on PPIs is often lacking. However, when sex-disaggregated data are presented, it seems that the female sex is a risk factor for gastrin elevation following PPI therapy. Further studies are needed to increase the understanding of the sex difference in gastrin elevation induced by PPIs, and it is still unclear whether this is a clinically important difference.
There is a constantly growing concern about the worldwide overuse of PPIs, especially their long-term use and potential adverse events. According to recent studies, females currently comprise more than half of PPI users and are involved in more ADRs in general. It is still unknown whether females are more sensitive to the inhibitory effect of PPIs, but gastrin is believed to play a role in the RAHS phenomenon after PPI withdrawal, which might maintain the need for further PPI use. The long-term consequences of continuous gastrin elevation remain unknown, but efforts should be made to examine the role of gastrin elevation in the overutilization of PPIs. Gastrin also exerts trophic effects on the GI tract mucosa; therefore, females might be at increased risk of developing morphological changes, such as FGPs in the gastric mucosa.
Gender and sex differences in PPI indications and sensitivity might have diagnostic and therapeutic influences. PPIs are now used for a variety of indications in a highly heterogeneous human population, making it difficult to generalize the findings from one study to another. Many studies are also aimed at symptomatology, and to a lesser extent, at physiology, thus putting little emphasis on the functions of PPIs in gastric acid inhibition and secondary gastrin elevation. However, it is conceivable that females might be at risk of PPI overuse, not only because they often receive higher milligram-per-kilogram doses, but they are also more likely than males to have burdens from non-acid-related symptoms. Such information is important to elucidate in the future. If the majority of female patients on long-term PPI therapy are able to step down or step off their PPI use, this could lead to major economic benefits for healthcare systems in many countries and potentially decrease the risks of side effects associated with long-term PPI use.
10. Conclusions
This review examined the literature related to the impact of female sex on the response to PPI therapy. Recent studies indicate that females on PPIs have increased gastrin release, which might contribute to differences in PPI treatment indication, response, and potential outcomes. Given the extensive use of PPI therapy, it seems prudent to address the potential issue of PPI overmedication of females, who could potentially benefit from receiving lower dosages of PPIs than those administered to males. The cornerstone of pharmacological therapy is to use the lowest effective dose to treat symptoms, and this is of course true for PPI therapy. Further studies are needed to increase the understanding of the sex difference in gastrin elevation induced by PPIs, and it is still unclear whether this is a clinically important difference. Also, the inclusion of sex- and gender-based analyses of PPI indication, response, and outcomes should be emphasized in future research.
Author Contributions
Conceptualization, H.H. and E.S.B.; writing—original draft preparation, H.H.; writing—review and editing, E.S.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Data sharing is not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Brabete, A.C.; Greaves, L.; Maximos, M.; Huber, E.; Li, A.; Le, M.L. A Sex- and Gender-Based Analysis of Adverse Drug Reactions: A Scoping Review of Pharmacovigilance Databases. Pharmaceuticals 2022, 15, 298. [Google Scholar] [CrossRef] [PubMed]
- Targownik, L.E.; Fisher, D.A.; Saini, S.D. AGA Clinical Practice Update on De-Prescribing of Proton Pump Inhibitors: Expert Review. Gastroenterology 2022, 162, 1334–1342. [Google Scholar] [CrossRef] [PubMed]
- Savarino, V.; Marabotto, E.; Zentilin, P.; Furnari, M.; Bodini, G.; De Maria, C.; Pellegatta, G.; Coppo, C.; Savarino, E. Proton pump inhibitors: Use and misuse in the clinical setting. Expert. Rev. Clin. Pharmacol. 2018, 11, 1123–1134. [Google Scholar] [CrossRef] [PubMed]
- Torres-Bondia, F.; de Batlle, J.; Galvan, L.; Buti, M.; Barbe, F.; Pinol-Ripoll, G. Evolution of the consumption trend of proton pump inhibitors in the Lleida Health Region between 2002 and 2015. BMC Public Health 2022, 22, 818. [Google Scholar] [CrossRef] [PubMed]
- Tran-Duy, A.; Spaetgens, B.; Hoes, A.W.; de Wit, N.J.; Stehouwer, C.D. Use of Proton Pump Inhibitors and Risks of Fundic Gland Polyps and Gastric Cancer: Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2016, 14, 1706–1719.e5. [Google Scholar] [CrossRef]
- Niklasson, A.; Lindstrom, L.; Simren, M.; Lindberg, G.; Bjornsson, E. Dyspeptic symptom development after discontinuation of a proton pump inhibitor: A double-blind placebo-controlled trial. Am. J. Gastroenterol. 2010, 105, 1531–1537. [Google Scholar] [CrossRef]
- Reimer, C.; Sondergaard, B.; Hilsted, L.; Bytzer, P. Proton-pump inhibitor therapy induces acid-related symptoms in healthy volunteers after withdrawal of therapy. Gastroenterology 2009, 137, 80–87.e1. [Google Scholar] [CrossRef]
- Cui, G.; Waldum, H.L. Physiological and clinical significance of enterochromaffin-like cell activation in the regulation of gastric acid secretion. World J. Gastroenterol. 2007, 13, 493–496. [Google Scholar] [CrossRef]
- Waldum, H.L.; Qvigstad, G.; Fossmark, R.; Kleveland, P.M.; Sandvik, A.K. Rebound acid hypersecretion from a physiological, pathophysiological and clinical viewpoint. Scand. J. Gastroenterol. 2010, 45, 389–394. [Google Scholar] [CrossRef]
- Ahrens, D.; Chenot, J.F.; Behrens, G.; Grimmsmann, T.; Kochen, M.M. Appropriateness of treatment recommendations for PPI in hospital discharge letters. Eur. J. Clin. Pharmacol. 2010, 66, 1265–1271. [Google Scholar] [CrossRef]
- Heidelbaugh, J.J.; Goldberg, K.L.; Inadomi, J.M. Overutilization of proton pump inhibitors: A review of cost-effectiveness and risk [corrected]. Am. J. Gastroenterol. 2009, 104 (Suppl. S2), S27–S32. [Google Scholar] [CrossRef] [PubMed]
- Helgadottir, H.; Metz, D.C.; Lund, S.H.; Gizurarson, S.; Jacobsen, E.I.; Asgeirsdottir, G.A.; Yngadottir, Y.; Bjornsson, E.S. Study of Gender Differences in Proton Pump Inhibitor Dose Requirements for GERD: A Double-Blind Randomized Trial. J. Clin. Gastroenterol. 2017, 51, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Fass, R.; Inadomi, J.; Han, C.; Mody, R.; O’Neil, J.; Perez, M.C. Maintenance of heartburn relief after step-down from twice-daily proton pump inhibitor to once-daily dexlansoprazole modified release. Clin. Gastroenterol. Hepatol. 2012, 10, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Vakil, N.; Niklasson, A.; Denison, H.; Ryden, A. Gender differences in symptoms in partial responders to proton pump inhibitors for gastro-oesophageal reflux disease. United Eur. Gastroenterol. J. 2015, 3, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Matsuhashi, N.; Kudo, M.; Yoshida, N.; Murakami, K.; Kato, M.; Sanuki, T.; Oshio, A.; Joh, T.; Higuchi, K.; Haruma, K.; et al. Factors affecting response to proton pump inhibitor therapy in patients with gastroesophageal reflux disease: A multicenter prospective observational study. J. Gastroenterol. 2015, 50, 1173–1183. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Kim, N.; Kim, G.H. Sex and Gender Differences in Gastroesophageal Reflux Disease. J. Neurogastroenterol. Motil. 2016, 22, 575–588. [Google Scholar] [CrossRef] [PubMed]
- Dickson, E.J.; Stuart, R.C. Genetics of response to proton pump inhibitor therapy: Clinical implications. Am. J. Pharmacogenom. 2003, 3, 303–315. [Google Scholar] [CrossRef]
- Andersson, T.; Hassan-Alin, M.; Hasselgren, G.; Rohss, K.; Weidolf, L. Pharmacokinetic studies with esomeprazole, the (S)-isomer of omeprazole. Clin. Pharmacokinet. 2001, 40, 411–426. [Google Scholar] [CrossRef]
- Mauvais-Jarvis, F.; Bairey Merz, N.; Barnes, P.J.; Brinton, R.D.; Carrero, J.J.; DeMeo, D.L.; De Vries, G.J.; Epperson, C.N.; Govindan, R.; Klein, S.L.; et al. Sex and gender: Modifiers of health, disease, and medicine. Lancet 2020, 396, 565–582. [Google Scholar] [CrossRef]
- Shiotani, A.; Katsumata, R.; Gouda, K.; Fukushima, S.; Nakato, R.; Murao, T.; Ishii, M.; Fujita, M.; Matsumoto, H.; Sakakibara, T. Hypergastrinemia in Long-Term Use of Proton Pump Inhibitors. Digestion 2018, 97, 154–162. [Google Scholar] [CrossRef]
- Helgadottir, H.; Lund, S.H.; Gizurarson, S.; Metz, D.C.; Bjornsson, E.S. Predictors of Gastrin Elevation Following Proton Pump Inhibitor Therapy. J. Clin. Gastroenterol. 2020, 54, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Jansen, J.B.; Klinkenberg-Knol, E.C.; Meuwissen, S.G.; De Bruijne, J.W.; Festen, H.P.; Snel, P.; Luckers, A.E.; Biemond, I.; Lamers, C.B. Effect of long-term treatment with omeprazole on serum gastrin and serum group A and C pepsinogens in patients with reflux esophagitis. Gastroenterology 1990, 99, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Koop, H.; Klein, M.; Arnold, R. Serum gastrin levels during long-term omeprazole treatment. Aliment. Pharmacol. Ther. 1990, 4, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Sokic-Milutinovic, A.; Todorovic, V.; Milosavljevic, T.; Micev, M.; Drndarevic, N.; Mitrovic, O. Gastrin and antral G cells in course of Helicobacter pylori eradication: Six months follow up study. World J. Gastroenterol. 2005, 11, 4140–4147. [Google Scholar] [CrossRef]
- Veysey-Smith, R.; Moore, A.R.; Murugesan, S.V.; Tiszlavicz, L.; Dockray, G.J.; Varro, A.; Pritchard, D.M. Effects of Proton Pump Inhibitor Therapy, H. pylori Infection and Gastric Preneoplastic Pathology on Fasting Serum Gastrin Concentrations. Front. Endocrinol. 2021, 12, 741887. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.S.; Varro, A.; Lightdale, C.J.; Lertkowit, N.; Slack, K.N.; Fingerhood, M.L.; Tsai, W.Y.; Wang, T.C.; Abrams, J.A. Elevated serum gastrin is associated with a history of advanced neoplasia in Barrett’s esophagus. Am. J. Gastroenterol. 2010, 105, 1039–1045. [Google Scholar] [CrossRef] [PubMed]
- Brunner, G.; Athmann, C.; Schneider, A. Long-term, open-label trial: Safety and efficacy of continuous maintenance treatment with pantoprazole for up to 15 years in severe acid-peptic disease. Aliment. Pharmacol. Ther. 2012, 36, 37–47. [Google Scholar] [CrossRef]
- Helgadottir, H.; Metz, D.C.; Yang, Y.X.; Rhim, A.D.; Bjornsson, E.S. The effects of long-term therapy with proton pump inhibitors on meal stimulated gastrin. Dig. Liver Dis. 2014, 46, 125–130. [Google Scholar] [CrossRef]
- Helgadottir, H. Proton Pump Inhibitors. Acid Rebound, Development and Predictors of Gastrin Elevation and Dosage Based in Gender. Ph.D. Thesis, University of Iceland, Reykjavík, Iceland, 2019. [Google Scholar]
- Korman, M.G.; Hansky, J.; Strickland, R.G. Progressive increase in the functional G cell mass with age in atrophic gastritis. Gut 1973, 14, 549–551. [Google Scholar] [CrossRef]
- Waldum, H.L.; Arnestad, J.S.; Brenna, E.; Eide, I.; Syversen, U.; Sandvik, A.K. Marked increase in gastric acid secretory capacity after omeprazole treatment. Gut 1996, 39, 649–653. [Google Scholar] [CrossRef]
- Prewett, E.J.; Smith, J.T.; Nwokolo, C.U.; Sawyerr, A.M.; Pounder, R.E. Twenty-four hour intragastric acidity and plasma gastrin concentration profiles in female and male subjects. Clin. Sci. 1991, 80, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Gedde-Dahl, D. Radioimmunoassay of gastrin. Fasting serum levels in humans with normal and high gastric acid secreation. Scand. J. Gastroenterol. 1974, 9, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Archimandritis, A.; Alegakis, G.; Theodoropoulos, G.; Kalos, A.; Drivas, G.; Melissinos, K. Serum gastrin concentrations in healthy males and females of various ages. Acta Hepato-Gastroenterol. 1979, 26, 58–63. [Google Scholar]
- Feldman, M.; Richardson, C.T.; Walsh, J.H. Sex-related differences in gastrin release and parietal cell sensitivity to gastrin in healthy human beings. J. Clin. Investig. 1983, 71, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Mossi, S.; Meyer-Wyss, B.; Renner, E.L.; Merki, H.S.; Gamboni, G.; Beglinger, C. Influence of Helicobacter pylori, sex, and age on serum gastrin and pepsinogen concentrations in subjects without symptoms and patients with duodenal ulcers. Gut 1993, 34, 752–756. [Google Scholar] [CrossRef] [PubMed]
- Camilo, S.M.; Almeida, E.C.; Miranzi, B.A.; Silva, J.C.; Nomelini, R.S.; Etchebehere, R.M. Endoscopic and histopathologic gastric changes in chronic users of proton-pump inhibitors. Arq. Gastroenterol. 2015, 52, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Helgadottir, H.; Lund, S.H.; Gizurarson, S.; Waldum, H.; Bjornsson, E.S. Pharmacokinetics of single and repeated oral doses of esomeprazole and gastrin elevation in healthy males and females. Scand. J. Gastroenterol. 2021, 56, 128–136. [Google Scholar] [CrossRef]
- Card, W.I.; Marks, I.N. The relationship between the acid output of the stomach following “maximal” histamine stimulation and the parietal cell mass. Clin. Sci. 1960, 19, 147–163. [Google Scholar]
- Cox, A.J. Stomach size and its relation to chronic peptic ulcer. AMA Arch. Pathol. 1952, 54, 407–422. [Google Scholar]
- Leblanc, V.; Begin, C.; Corneau, L.; Dodin, S.; Lemieux, S. Gender differences in dietary intakes: What is the contribution of motivational variables? J. Hum. Nutr. Diet. 2015, 28, 37–46. [Google Scholar] [CrossRef]
- Sadik, R.; Abrahamsson, H.; Stotzer, P.O. Gender differences in gut transit shown with a newly developed radiological procedure. Scand. J. Gastroenterol. 2003, 38, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Graff, J.; Brinch, K.; Madsen, J.L. Gastrointestinal mean transit times in young and middle-aged healthy subjects. Clin. Physiol. 2001, 21, 253–259. [Google Scholar] [CrossRef]
- Slagter, S.N.; van Waateringe, R.P.; van Beek, A.P.; van der Klauw, M.M.; Wolffenbuttel, B.H.R.; van Vliet-Ostaptchouk, J.V. Sex, BMI and age differences in metabolic syndrome: The Dutch Lifelines Cohort Study. Endocr. Connect. 2017, 6, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Ala, S.; Zanad, F.; Shiran, M.R. Population pharmacokinetics of omeprazole in a random Iranian population. Caspian J. Intern. Med. 2013, 4, 712–716. [Google Scholar] [PubMed]
- Anderson, G.D. Sex and racial differences in pharmacological response: Where is the evidence? Pharmacogenetics, pharmacokinetics, and pharmacodynamics. J. Womens Health 2005, 14, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Hagymasi, K.; Mullner, K.; Herszenyi, L.; Tulassay, Z. Update on the pharmacogenomics of proton pump inhibitors. Pharmacogenomics 2011, 12, 873–888. [Google Scholar] [CrossRef] [PubMed]
- McColl, K.E.; Kennerley, P. Proton pump inhibitors--differences emerge in hepatic metabolism. Dig. Liver Dis. 2002, 34, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Hunt, C.M.; Westerkam, W.R.; Stave, G.M. Effect of age and gender on the activity of human hepatic CYP3A. Biochem. Pharmacol. 1992, 44, 275–283. [Google Scholar] [CrossRef]
- Harris, R.Z.; Benet, L.Z.; Schwartz, J.B. Gender effects in pharmacokinetics and pharmacodynamics. Drugs 1995, 50, 222–239. [Google Scholar] [CrossRef]
- Tamminga, W.J.; Wemer, J.; Oosterhuis, B.; Weiling, J.; Wilffert, B.; de Leij, L.F.; de Zeeuw, R.A.; Jonkman, J.H. CYP2D6 and CYP2C19 activity in a large population of Dutch healthy volunteers: Indications for oral contraceptive-related gender differences. Eur. J. Clin. Pharmacol. 1999, 55, 177–184. [Google Scholar] [CrossRef]
- Wolbold, R.; Klein, K.; Burk, O.; Nussler, A.K.; Neuhaus, P.; Eichelbaum, M.; Schwab, M.; Zanger, U.M. Sex is a major determinant of CYP3A4 expression in human liver. Hepatology 2003, 38, 978–988. [Google Scholar] [CrossRef] [PubMed]
- Pregun, I.; Herszenyi, L.; Juhasz, M.; Miheller, P.; Hritz, I.; Patocs, A.; Racz, K.; Tulassay, Z. Effect of proton-pump inhibitor therapy on serum chromogranin a level. Digestion 2011, 84, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Sharma, B.K.; Walt, R.P.; Pounder, R.E.; Gomes, M.D.; Wood, E.C.; Logan, L.H. Optimal dose of oral omeprazole for maximal 24 hour decrease of intragastric acidity. Gut 1984, 25, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Ligumsky, M.; Lysy, J.; Siguencia, G.; Friedlander, Y. Effect of long-term, continuous versus alternate-day omeprazole therapy on serum gastrin in patients treated for reflux esophagitis. J. Clin. Gastroenterol. 2001, 33, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Sanduleanu, S.; Stridsberg, M.; Jonkers, D.; Hameeteman, W.; Biemond, I.; Lundqvist, G.; Lamers, C.; Stockbrugger, R.W. Serum gastrin and chromogranin A during medium- and long-term acid suppressive therapy: A case-control study. Aliment. Pharmacol. Ther. 1999, 13, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Bonapace, E.S.; Fisher, R.S.; Parkman, H.P. Does fasting serum gastrin predict gastric acid suppression in patients on proton-pump inhibitors? Dig. Dis. Sci. 2000, 45, 34–39. [Google Scholar] [CrossRef]
- Bjornsson, E.; Abrahamsson, H.; Simren, M.; Mattsson, N.; Jensen, C.; Agerforz, P.; Kilander, A. Discontinuation of proton pump inhibitors in patients on long-term therapy: A double-blind, placebo-controlled trial. Aliment. Pharmacol. Ther. 2006, 24, 945–954. [Google Scholar] [CrossRef]
- Hendricks, E.; Ajmeri, A.N.; Singh, M.M.; Mongalo, M.; Goebel, L.J. A Randomized Open-Label Study of Two Methods of Proton Pump Inhibitors Discontinuation. Cureus 2021, 13, e15022. [Google Scholar] [CrossRef]
- Inadomi, J.M.; McIntyre, L.; Bernard, L.; Fendrick, A.M. Step-down from multiple- to single-dose proton pump inhibitors (PPIs): A prospective study of patients with heartburn or acid regurgitation completely relieved with PPIs. Am. J. Gastroenterol. 2003, 98, 1940–1944. [Google Scholar] [CrossRef]
- Cote, G.A.; Ferreira, M.R.; Rozenberg-Ben-Dror, K.; Howden, C.W. Programme of stepping down from twice daily proton pump inhibitor therapy for symptomatic gastro-oesophageal reflux disease associated with a formulary change at a VA medical center. Aliment. Pharmacol. Ther. 2007, 25, 709–714. [Google Scholar] [CrossRef]
- Halfdanarson, O.O.; Pottegard, A.; Bjornsson, E.S.; Lund, S.H.; Ogmundsdottir, M.H.; Steingrimsson, E.; Ogmundsdottir, H.M.; Zoega, H. Proton-pump inhibitors among adults: A nationwide drug-utilization study. Therap. Adv. Gastroenterol. 2018, 11, 1756284818777943. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, V.; Tzadok, R.; Chodick, G.; Kariv, R. Proton pump inhibitors long term use-trends and patterns over 15 years of a large health maintenance organization. Pharmacoepidemiol. Drug Saf. 2021, 30, 1576–1587. [Google Scholar] [CrossRef] [PubMed]
- Othman, F.; Card, T.R.; Crooks, C.J. Proton pump inhibitor prescribing patterns in the UK: A primary care database study. Pharmacoepidemiol. Drug Saf. 2016, 25, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Pottegard, A.; Broe, A.; Hallas, J.; de Muckadell, O.B.; Lassen, A.T.; Lodrup, A.B. Use of proton-pump inhibitors among adults: A Danish nationwide drug utilization study. Therap. Adv. Gastroenterol. 2016, 9, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Shanika, L.G.T.; Reynolds, A.; Pattison, S.; Braund, R. Proton pump inhibitor use: Systematic review of global trends and practices. Eur. J. Clin. Pharmacol. 2023, 79, 1159–1172. [Google Scholar] [CrossRef]
- Maes, M.L.; Fixen, D.R.; Linnebur, S.A. Adverse effects of proton-pump inhibitor use in older adults: A review of the evidence. Ther. Adv. Drug Saf. 2017, 8, 273–297. [Google Scholar] [CrossRef]
- McColl, K.E.; Gillen, D. Evidence that proton-pump inhibitor therapy induces the symptoms it is used to treat. Gastroenterology 2009, 137, 20–22. [Google Scholar] [CrossRef]
- Moayyedi, P.; Mason, J. Clinical and economic consequences of dyspepsia in the community. Gut 2002, 50 (Suppl. S4), iv10–iv12. [Google Scholar] [CrossRef]
- Bytzer, P.; van Zanten, S.V.; Mattsson, H.; Wernersson, B. Partial symptom-response to proton pump inhibitors in patients with non-erosive reflux disease or reflux oesophagitis—A post hoc analysis of 5796 patients. Aliment. Pharmacol. Ther. 2012, 36, 635–643. [Google Scholar] [CrossRef]
- Lundell, L.; Hatlebakk, J.; Galmiche, J.P.; Attwood, S.E.; Ell, C.; Fiocca, R.; Persson, T.; Nagy, P.; Eklund, S.; Lind, T. Long-term effect on symptoms and quality of life of maintenance therapy with esomeprazole 20 mg daily: A post hoc analysis of the LOTUS trial. Curr. Med. Res. Opin. 2015, 31, 65–73. [Google Scholar] [CrossRef]
- Koggel, L.M.; Lantinga, M.A.; Buchner, F.L.; Drenth, J.P.H.; Frankema, J.S.; Heeregrave, E.J.; Heringa, M.; Numans, M.E.; Siersema, P.D. Predictors for inappropriate proton pump inhibitor use: Observational study in primary care. Br. J. Gen. Pract. 2022, 72, e899–e906. [Google Scholar] [CrossRef] [PubMed]
- Voukelatou, P.; Vrettos, I.; Emmanouilidou, G.; Dodos, K.; Skotsimara, G.; Kontogeorgou, D.; Kalliakmanis, A. Predictors of Inappropriate Proton Pump Inhibitors Use in Elderly Patients. Curr. Gerontol. Geriatr. Res. 2019, 2019, 7591045. [Google Scholar] [CrossRef] [PubMed]
- Ali, R.A.R.; Hassan, J.; Egan, L.J. Review of recent evidence on the management of heartburn in pregnant and breastfeeding women. BMC Gastroenterol. 2022, 22, 219. [Google Scholar] [CrossRef] [PubMed]
- Waldum, H.L.; Hauso, O.; Brenna, E.; Qvigstad, G.; Fossmark, R. Does long-term profound inhibition of gastric acid secretion increase the risk of ECL cell-derived tumors in man? Scand. J. Gastroenterol. 2016, 51, 767–773. [Google Scholar] [CrossRef]
- Freeman, H.J. Proton pump inhibitors and an emerging epidemic of gastric fundic gland polyposis. World J. Gastroenterol. 2008, 14, 1318–1320. [Google Scholar] [CrossRef]
- Gao, W.; Huang, Y.; Lu, S.; Li, C. The clinicopathological characteristics of gastric polyps and the relationship between fundic gland polyps, Helicobacter pylori infection, and proton pump inhibitors. Ann. Palliat. Med. 2021, 10, 2108–2114. [Google Scholar] [CrossRef] [PubMed]
- Shinozaki, S.; Osawa, H.; Hayashi, Y.; Sakamoto, H.; Miura, Y.; Lefor, A.K.; Yamamoto, H. Changes in gastric morphology during long-term use of vonoprazan compared to proton pump inhibitors. Singapore Med. J. 2022, 63, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Sano, W.; Inoue, F.; Hirata, D.; Iwatate, M.; Hattori, S.; Fujita, M.; Sano, Y. Sporadic fundic gland polyps with dysplasia or carcinoma: Clinical and endoscopic characteristics. World J. Gastrointest. Oncol. 2021, 13, 662–672. [Google Scholar] [CrossRef]
- Murphy, G.; Abnet, C.C.; Choo-Wosoba, H.; Vogtmann, E.; Weinstein, S.J.; Taylor, P.R.; Mannisto, S.; Albanes, D.; Dawsey, S.M.; Rehfeld, J.F.; et al. Serum gastrin and cholecystokinin are associated with subsequent development of gastric cancer in a prospective cohort of Finnish smokers. Int. J. Epidemiol. 2017, 46, 914–923. [Google Scholar] [CrossRef]
- Abrahami, D.; McDonald, E.G.; Schnitzer, M.E.; Barkun, A.N.; Suissa, S.; Azoulay, L. Proton pump inhibitors and risk of gastric cancer: Population-based cohort study. Gut 2022, 71, 16–24. [Google Scholar] [CrossRef]
- Snir, Y.; Leibovitzh, H.; Leibovici-Weissman, Y.; Vilkin, A.; Cohen, A.D.; Shochat, T.; Niv, Y.; Dotan, I.; Feldhamer, I.; Boltin, D.; et al. Dose-dependent association of proton pump inhibitors use with gastric intestinal metaplasia among Helicobacter pylori-positive patients. United Eur. Gastroenterol. J. 2021, 9, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.M.; Poly, T.N.; Walther, B.A.; Dubey, N.K.; Anggraini Ningrum, D.N.; Shabbir, S.A.; Jack Li, Y.C. Adverse outcomes of long-term use of proton pump inhibitors: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2018, 30, 1395–1405. [Google Scholar] [CrossRef] [PubMed]
- Jaynes, M.; Kumar, A.B. The risks of long-term use of proton pump inhibitors: A critical review. Ther. Adv. Drug Saf. 2019, 10, 2042098618809927. [Google Scholar] [CrossRef] [PubMed]
- Luk, C.P.; Parsons, R.; Lee, Y.P.; Hughes, J.D. Proton pump inhibitor-associated hypomagnesemia: What do FDA data tell us? Ann. Pharmacother. 2013, 47, 773–780. [Google Scholar] [CrossRef]
- Wang, M.; Zhang, L.; Jia, M.; Wang, J.; Shen, Z.; Wang, S.; Zhang, X.; Xu, J.; Zheng, Z.; Lv, X.; et al. Syndrome of inappropriate antidiuretic hormone secretion is associated with different proton pump inhibitor use: A pharmacovigilance study. BMC Nephrol. 2022, 23, 191. [Google Scholar] [CrossRef]
- Yang, Y.X.; Metz, D.C. Safety of proton pump inhibitor exposure. Gastroenterology 2010, 139, 1115–1127. [Google Scholar] [CrossRef]
Figure 1.
Median fasting serum gastrin levels in reflux esophagitis patients before treatment (0 months) and during omeprazole maintenance treatment. The graph is based on data from non-antrectomized patients (n = 29 (14 females)) [22]. Gastrin levels were higher in females (red line) than males (blue line). The error bars show the 25th and the 75th interquartile range [22]. Reprinted/adapted with permission from Ref. [22].
Figure 1.
Median fasting serum gastrin levels in reflux esophagitis patients before treatment (0 months) and during omeprazole maintenance treatment. The graph is based on data from non-antrectomized patients (n = 29 (14 females)) [22]. Gastrin levels were higher in females (red line) than males (blue line). The error bars show the 25th and the 75th interquartile range [22]. Reprinted/adapted with permission from Ref. [22].

Figure 2.
Median fasting (time = 0) and postprandial serum gastrin levels in patients with gastroesophageal reflux disease on long-term (over 2 years) proton pump inhibitor therapy (A) and controls not taking proton pump inhibitors (B). The graph is based on data from 100 patients (44 females) and 50 healthy controls (25 females) [28,29]. The error bars show the 25th and the 75th interquartile range. Female patients (red line) had significantly higher gastrin levels than males (blue line) pre- and postprandial, whereas such differences were not found in the control group (males in red, females in blue) [28]. Reprinted/adapted with permission from Ref. [28].
Figure 2.
Median fasting (time = 0) and postprandial serum gastrin levels in patients with gastroesophageal reflux disease on long-term (over 2 years) proton pump inhibitor therapy (A) and controls not taking proton pump inhibitors (B). The graph is based on data from 100 patients (44 females) and 50 healthy controls (25 females) [28,29]. The error bars show the 25th and the 75th interquartile range. Female patients (red line) had significantly higher gastrin levels than males (blue line) pre- and postprandial, whereas such differences were not found in the control group (males in red, females in blue) [28]. Reprinted/adapted with permission from Ref. [28].

Figure 3.
Sex- and sage-specific prevalence of proton pump inhibitor use among adults in Iceland in 2015. Reprinted with permission from Ref. [62]. 2018, copyright SAGE Publications.
Figure 3.
Sex- and sage-specific prevalence of proton pump inhibitor use among adults in Iceland in 2015. Reprinted with permission from Ref. [62]. 2018, copyright SAGE Publications.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Overview of studies that examined sex differences in gastrin release and/or gastrin elevation in healthy volunteers or patients receiving or not receiving PPI therapy.
Table 1.
Overview of studies that examined sex differences in gastrin release and/or gastrin elevation in healthy volunteers or patients receiving or not receiving PPI therapy.
| Author, Year | N (M/F) | Subjects | Sex Difference | Baseline Gastrin (M vs. F) | Comments |
|---|---|---|---|---|---|
| Gedde-Dahl, 1974 [33] | 298 (180/118) | Patients | No | 67 (45) vs. 65 (40) (mean (SD)) | Patients with different diseases undergoing pentagastrin test |
| Archimandritis et al., 1979 [34] | 80 (43/37) | Healthy volunteers | No | 54 (3) vs. 56.5 (3) pg/cc (mean (SEM)) | No gender difference found 10 and 40 min after a meal |
| Feldman et al., 1983 [35] | 41 (26/15) | Healthy volunteers | Yes | - | Females had higher basal and meal-stimulated gastrin levels, with average rises of 19 (2) vs. 53 (10) pg/mL (p < 0.001). |
| Prewett et al., 1991 [32] | 131 (96/35) | Healthy volunteers | Yes | 185 vs. 407 | Gastrin values are 24 h integrated plasma gastrin concentrations (pmol⋅h⋅L−1). |
| Mossi et al., 1993 [36] | 62 (30/32) | Healthy volunteers, H. pylori (-) | No | 73 (5) vs. 74 (5) pg/mL (mean (SEM)) | No association between sex or age and baseline gastrin levels |
| Jansen et al., 1990 [22] | 32 (18/14) | EE patients | No | Baseline (p = NS) | At all-time intervals, females had higher fasting gastrin levels than males. Eight patients reached gastrin levels > 6 times the upper limit of normal range during follow-up (5 females). |
| on PPIs | Yes | 18 months (p < 0.01) | |||
| Yes | 21 months (p < 0.05) | ||||
| Wang et al., 2010 [26] | 95 (67/28) | BE and GERD patients on chronic PPIs | No | 65 vs. 80 pM (mean) 40 vs. 47 pM (median) | No association between sex or age and baseline gastrin levels |
| Camilo et al., 2015 [37] | 81 (13/68) | Chronic PPI users | - | - | Females were the only patients with gastrin levels > 115 pg/mL. |
| Shiotani et al., 2018 [20] | 199 (143/56) | CV patients on PPIs, prophylaxis with aspirin | Yes | 214 vs. 357 pg/mL | The F gender was associated with hypergastrinemia in a multiple logistic regression analysis, adjusted also for PPI use (vs. H2RAs and controls) and corpus atrophy. |
| Helgadottir et al., 2020 [21] | 157 (79/78) | GERD patients on long-term PPIs | Yes | 60 (42–90) vs. 92 (53–118) pg/mL (median (IQR)) | Gastrin elevation was significantly associated with the F sex and PPI dosage. |
| Helgadottir et al., 2021 [38] | 29 (14/15) | Healthy volunteers on short-term PPIs | Yes | Day 0 (12 vs. 7 pM) | Females had significantly higher baseline gastrin levels than males, but there was no significant difference between the sexes at the end of treatment (day 5). |
| No | Day 5 (15 vs. 15 pM) |
Acronyms and abbreviations: BE = Barrett’s esophagus, CV = cardiovascular, EE = erosive esophagitis, F = female, GERD = gastroesophageal reflux disease, H2RAs = histamine type-2 receptor antagonists, IQR = interquartile range, M = male, NS = non-significant, PPI = proton pump inhibitor, SD = standard deviation, SEM = standard error of the mean.
Table 2.
Possible factors that could contribute to gender-related differences in gastrin release in healthy subjects and gastrin elevation secondary to PPI therapy.
Table 2.
Possible factors that could contribute to gender-related differences in gastrin release in healthy subjects and gastrin elevation secondary to PPI therapy.
| Females have a lower number of parietal cells [39]. |
| Females are less sensitive to gastrin effects on parietal cells [35]. |
| Smaller stomachs of females, with more postprandial distension [40] |
| Gender differences in dietary intakes, lower energy density in females than in males [41] |
| Gender differences in gastric emptying, with slower gastric emptying in females [42,43] |
| Gender difference in body mass index (BMI) [44] |
| Sex hormones (unlikely, as no fluctuations in gastrin release throughout one menstrual cycle were observed in six females) [35] |
| Difference in metabolism of PPIs [45,46] |
Table 3.
Overview of previous studies that have examined PPI deprescribing.
| Author, Year | N (M/F) | Subjects | Type of Study | Sex Variable Mentioned | Type of PPI Deprescribing | Predictors and Other Comments |
|---|---|---|---|---|---|---|
| Inadomi et al., 2003 [60] | 117 (112/5) | Patients with heartburn or acid regurgitatio | Prospective study | No | Step-down from multiple- to single-dose | Only the duration of PPI use before study predicted successful step-down (OR 0.66). |
| Bjornsson et al., 2006 [58] | 96 (44/52) | Patients without history of PUD or EE | Double-blind, placebo-controlled trial | No | Step-off | GERD as PPI indication (OR 8.050) and serum gastrin (OR 1.018) predicted the need for reinstitution of PPIs after discontinuation. |
| Cote et al., 2007 [61] | 223 | GERD patients | Retrospective study | Very few females (~1%) | Step-down from BID to SID | Dose reduction was more successful in those without EE. |
| Fass et al., 2012 [13] | 142 (62/80) | Symptomatic GERD patients | Single-blind trial | Yes | Step-down from BID to SID modified release PPI | No predictor was significant (age, sex, BMI, and baseline symptom scores). But OR for females not remaining well controlled was 0.499, NS. |
| Helgadottir et al., 2017 [12] | 100 (51/49) | EE patients | Double-blind randomized trial | Yes | 50% dose reduction | Successful step-down was predicted only by female sex with OR 1.3 (p = 0.048). Baseline fasting s-gastrin was NS (p = 0.49). |
| Hendricks et al., 2021 [59] | 33 (19/15) | Patients with a clinical diagnosis of GERD | Randomized open-label trial | Yes | Step-off | Sex was not associated with resuming PPIs. H2RA use was associated with successful discontinuation of PPIs with HR 0.21 (p = 0.002). |
Acronyms and abbreviations: BID = bis in die/twice a day, BMI = body mass index, EE = erosive esophagitis, F = female, GERD = gastroesophageal reflux disease, H2RAs = histamine type-2 receptor antagonists, HR = hazard ratio, M = male, NS = non-significant, OR = odds ratio, PPI = proton pump inhibitor, PUD = peptic ulcer disease, SID = semel in die/once a day.
Table 4.
The potential role of sex and gender on PPI overuse or overmedication.
| Sex | Diagnosis | PPI Overmedication? |
|---|---|---|
| Female > Male | Non-erosive reflux disease Heartburn or regurgitation Extra-esophageal symptoms Comorbid anxiety or depression | Females at risk for overmedication because of partial symptom response and unnecessary PPI dose escalation for symptoms that are not related to acid reflux |
| Male > Female | Reflux esophagitis Barrett’s esophagus Esophageal adenocarcinoma | Females at risk for overmedication because they might be more sensitive to PPIs than males and could remain symptom control on lower PPI doses |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Helgadottir, H.; Björnsson, E.S. The Impact of Sex on the Response to Proton Pump Inhibitor Treatment. Pharmaceuticals 2023, 16, 1722. https://doi.org/10.3390/ph16121722
AMA Style
Helgadottir H, Björnsson ES. The Impact of Sex on the Response to Proton Pump Inhibitor Treatment. Pharmaceuticals. 2023; 16(12):1722. https://doi.org/10.3390/ph16121722
Chicago/Turabian StyleHelgadottir, Holmfridur, and Einar S. Björnsson. 2023. "The Impact of Sex on the Response to Proton Pump Inhibitor Treatment" Pharmaceuticals 16, no. 12: 1722. https://doi.org/10.3390/ph16121722
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.