
The Impact of Metformin on the Development of Hypothyroidism and Cardiotoxicity Induced by Cyclophosphamide, Methotrexate, and Fluorouracil in Rats

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
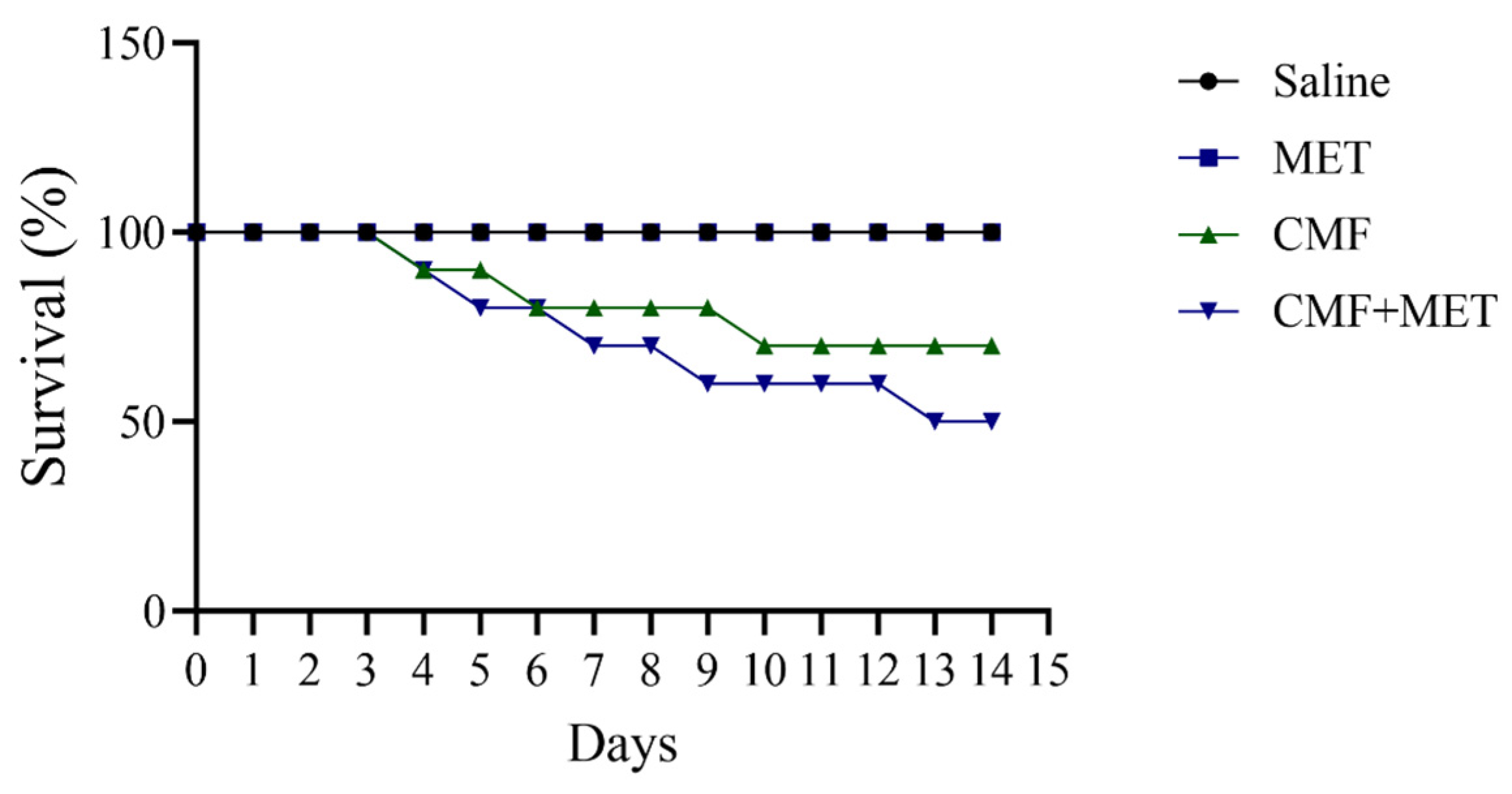
2.1. Effect of CMF and MET on Mortality
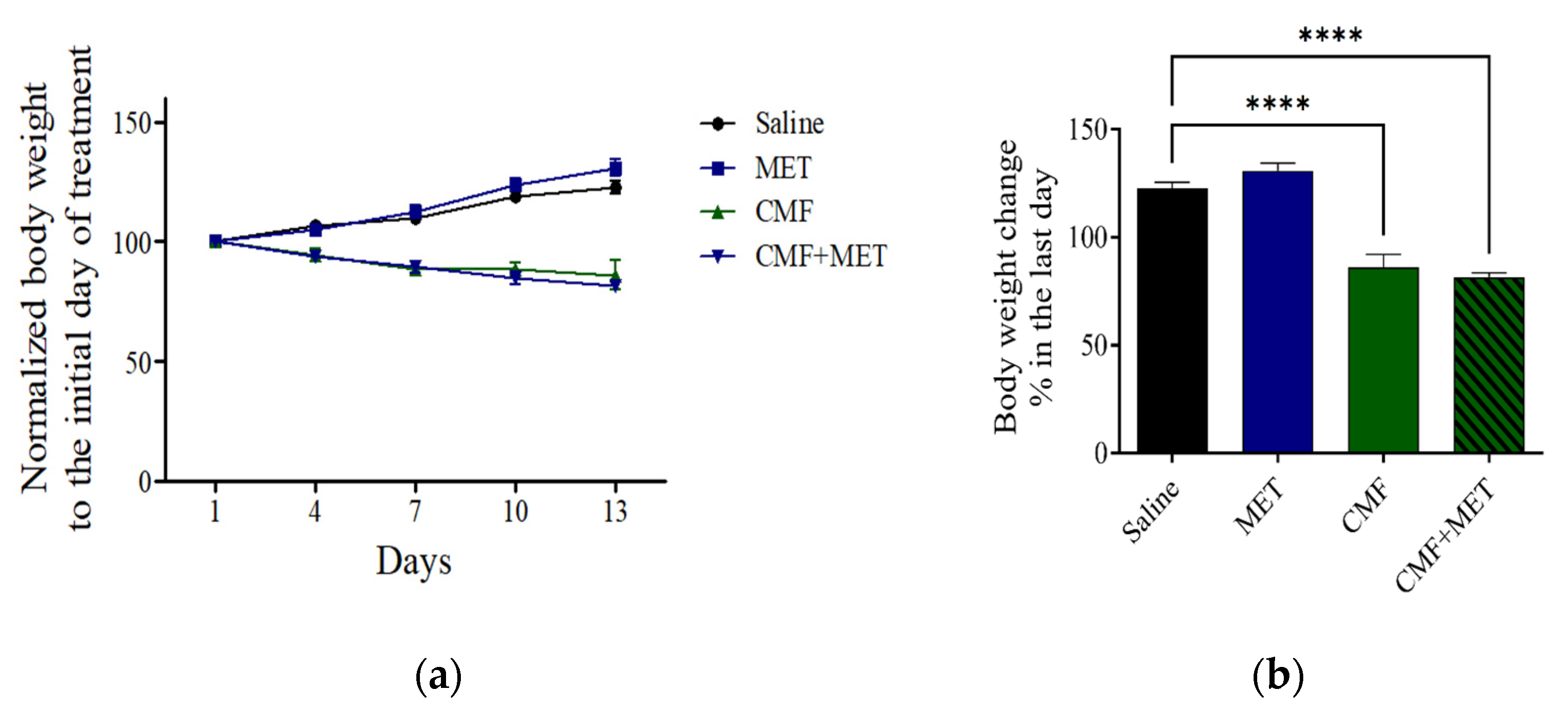
2.2. Effect of CMF and MET on the Body Weight
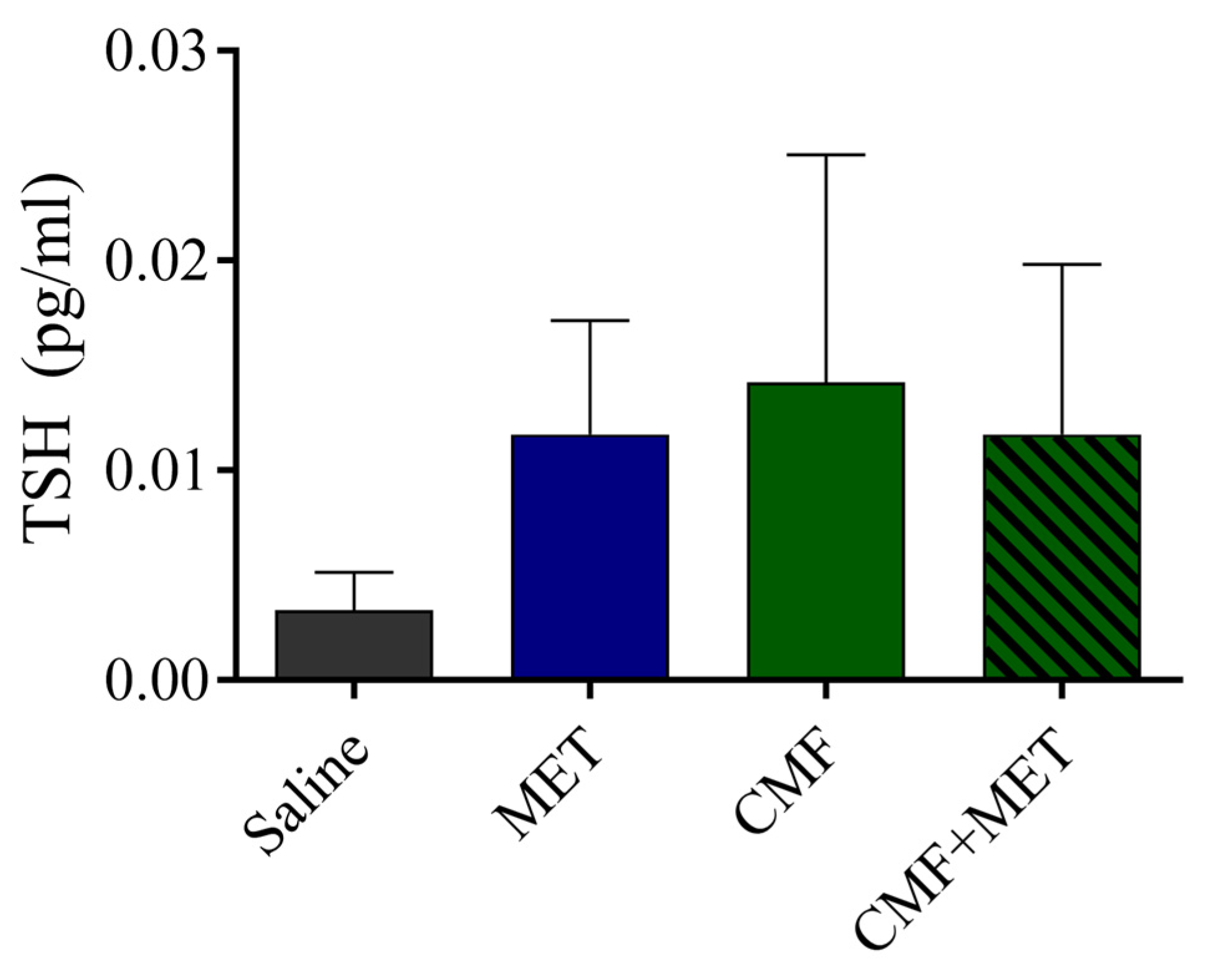
2.3. The TSH Levels Were Unaffected by CMF or MET
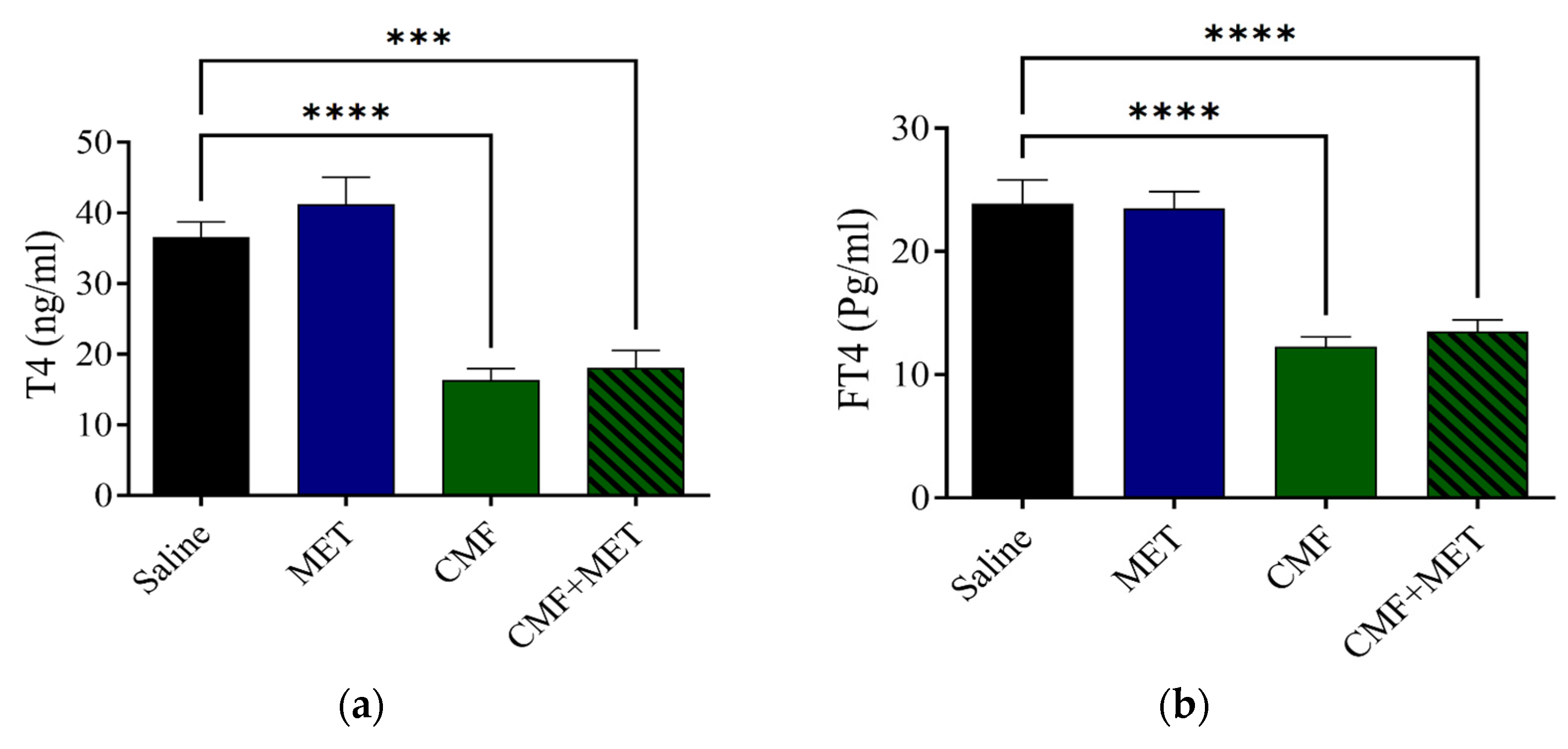
2.4. MET Did Not Reduce CMF Toxic Effects on T4 and FT4 Levels
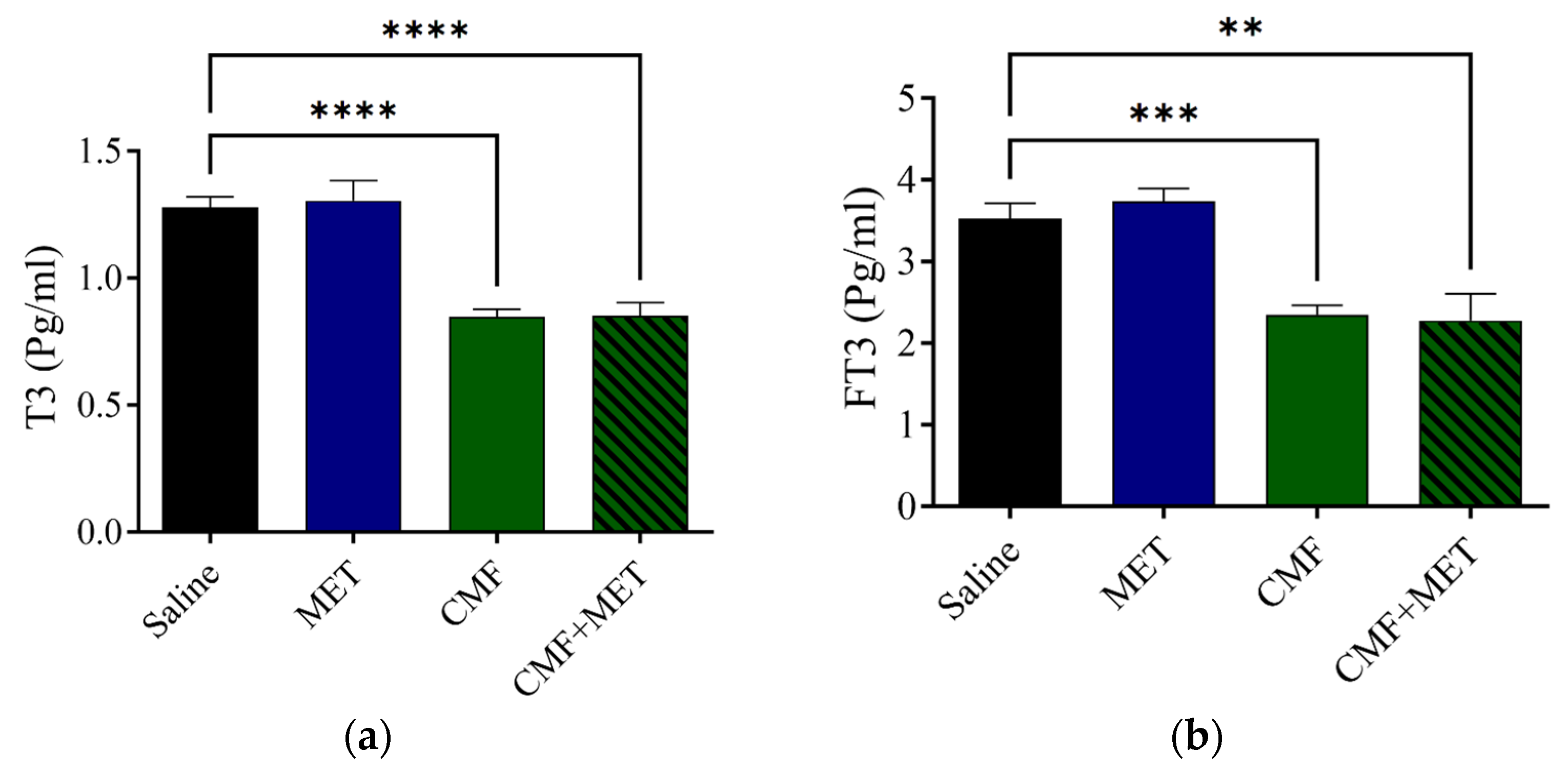
2.5. MET Did Not Improve CMF Toxic Effects on T3 and FT3 Levels
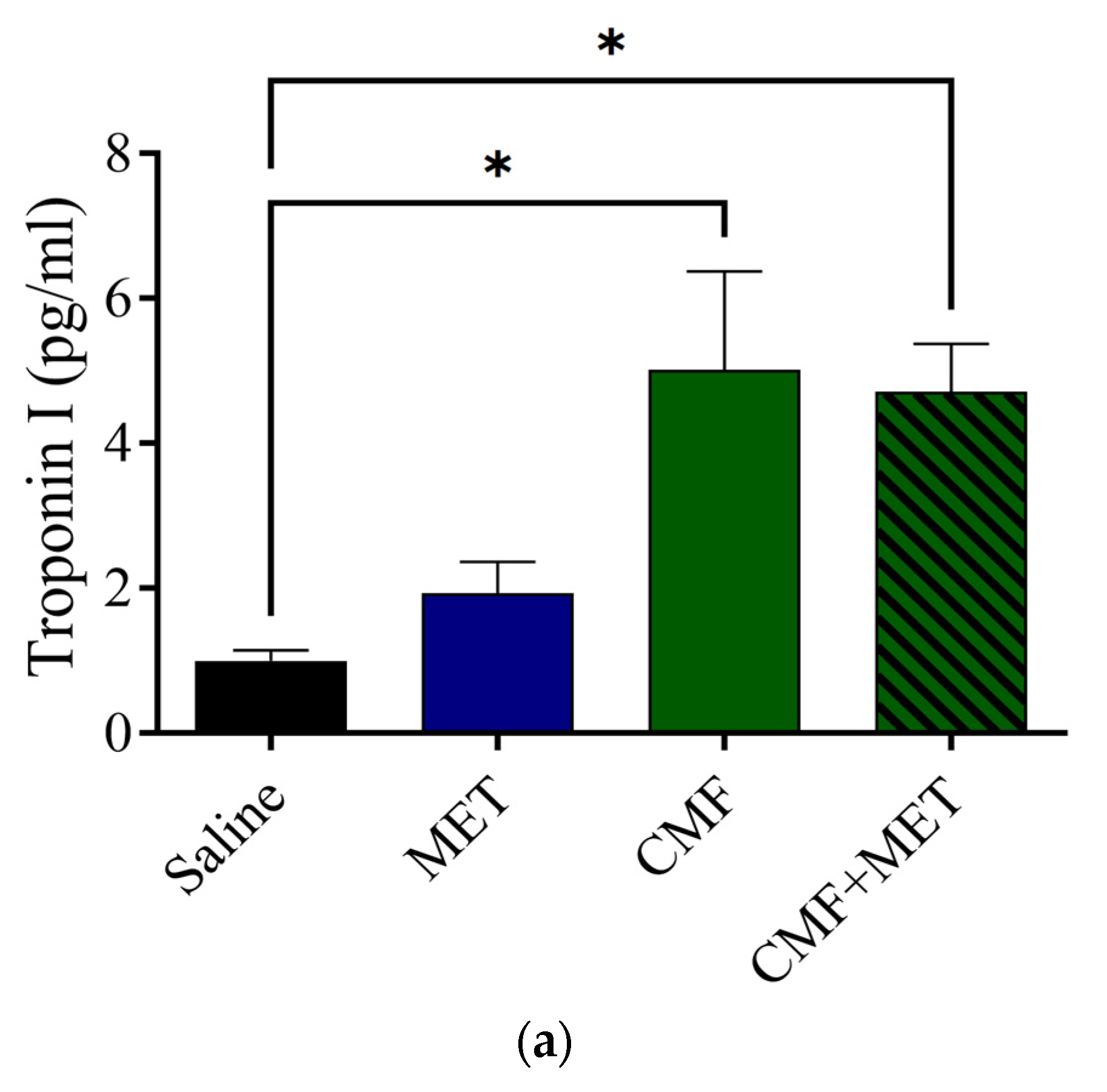
2.6. Effect of CMF and MET on Troponin I, CK, and CK-MB Levels
3. Discussion
4. Materials and Methods
4.1. Study Area
4.2. Drugs
4.3. Experimental Design
4.4. Electrochemiluminescence Immunoassays
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alhowail, A.H.; Almogbel, Y.S.; Abdellatif, A.A.H.; Aldubayan, M.A.; Chigurupati, S.; Nemala, R.A. Effects of CMF and MET on glutamate and dopamine levels in the brain, and their impact on cognitive function. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 2353–2362. [Google Scholar] [CrossRef] [PubMed]
- Tacar, O.; Sriamornsak, P.; Dass, C.R. Doxorubicin: An update on anticancer molecular action, toxicity and novel drug delivery systems. J. Pharm. Pharmacol. 2013, 65, 157–170. [Google Scholar] [CrossRef] [PubMed]
- Alotayk, L.I.; Aldubayan, M.A.; Alenezi, S.K.; Anwar, M.J.; Alhowail, A.H. Comparative evaluation of doxorubicin, cyclophosphamide, 5-fluorouracil, and cisplatin on cognitive dysfunction in rats: Delineating the role of inflammation of hippocampal neurons and hypothyroidism. Biomed. Pharmacother. 2023, 165, 115245. [Google Scholar] [CrossRef] [PubMed]
- Małyszko, J.; Kozłowska, K.; Kozłowski, L.; Małyszko, J. Nephrotoxicity of anticancer treatment. Nephrol. Dial. Transplant. 2016, 32, 924–936. [Google Scholar] [CrossRef]
- Briones, T.L.; Woods, J. Chemotherapy-induced cognitive impairment is associated with decreases in cell proliferation and histone modifications. BMC Neurosci. 2011, 12, 124. [Google Scholar] [CrossRef]
- Park, J.H.; Im, S.-A.; Byun, J.M.; Kim, K.H.; Kim, J.-S.; Choi, I.S.; Kim, H.-J.; Lee, K.-H.; Kim, T.-Y.; Han, S.-W.; et al. Cyclophosphamide, Methotrexate, and 5-Fluorouracil as Palliative Treatment for Heavily Pretreated Patients with Metastatic Breast Cancer: A Multicenter Retrospective Analysis. J. Breast Cancer 2017, 20, 347–355. [Google Scholar] [CrossRef]
- Gourzones, C.; Bret, C.; Moreaux, J. Treatment May Be Harmful: Mechanisms/Prediction/Prevention of Drug-Induced DNA Damage and Repair in Multiple Myeloma. Front. Genet. 2019, 10, 861. [Google Scholar] [CrossRef]
- Koźmiński, P.; Halik, P.K.; Chesori, R.; Gniazdowska, E. Overview of Dual-Acting Drug Methotrexate in Different Neurological Diseases, Autoimmune Pathologies and Cancers. Int. J. Mol. Sci. 2020, 21, 3483. [Google Scholar] [CrossRef]
- Stegmann, K.M.; Dickmanns, A.; Gerber, S.; Nikolova, V.; Klemke, L.; Manzini, V.; Schlösser, D.; Bierwirth, C.; Freund, J.; Sitte, M.; et al. The folate antagonist methotrexate diminishes replication of the coronavirus SARS-CoV-2 and enhances the antiviral efficacy of remdesivir in cell culture models. Virus Res. 2021, 302, 198469. [Google Scholar] [CrossRef]
- Whittle, S.L. Folate supplementation and methotrexate treatment in rheumatoid arthritis: A review. Rheumatology 2003, 43, 267–271. [Google Scholar] [CrossRef]
- Matuszyk, J. MALAT1-miRNAs network regulate thymidylate synthase and affect 5FU-based chemotherapy. Mol. Med. 2022, 28, 89. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Kim, J.-S.; Song, M.-S.; Kim, S.-H.; Kang, S.S.; Bae, C.-S.; Kim, J.-C.; Wang, H.; Shin, T.; Moon, C. Cyclophosphamide impairs hippocampus-dependent learning and memory in adult mice: Possible involvement of hippocampal neurogenesis in chemotherapy-induced memory deficits. Neurobiol. Learn. Mem. 2010, 93, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.E.; Trujillo, M.; McElroy, T.; Groves, T.; Alexander, T.; Kiffer, F.; Allen, A.R. Early Effects of Cyclophosphamide, Methotrexate, and 5-Fluorouracil on Neuronal Morphology and Hippocampal-Dependent Behavior in a Murine Model. Toxicol. Sci. 2020, 173, 156–170. [Google Scholar] [CrossRef] [PubMed]
- Dhesi, S.; Chu, M.P.; Blevins, G.; Paterson, I.; Larratt, L.; Oudit, G.Y.; Kim, D.H. Cyclophosphamide-Induced Cardiomyopathy. J. Investig. Med. High Impact Case Rep. 2013, 1. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.B.; Fink, A.; Levis, S.; Xu, P.; Tamura, R.; Krischer, J. Thyroid function in the etiology of fatigue in breast cancer. Oncotarget 2018, 9, 25723–25737. [Google Scholar] [CrossRef]
- Roelfsema, F.; Veldhuis, J.D. Thyrotropin Secretion Patterns in Health and Disease. Endocr. Rev. 2013, 34, 619–657. [Google Scholar] [CrossRef]
- Brent, G.A. Mechanisms of thyroid hormone action. J. Clin. Investig. 2012, 122, 3035–3043. [Google Scholar] [CrossRef]
- Mullur, R.; Liu, Y.-Y.; Brent, G.A. Thyroid Hormone Regulation of Metabolism. Physiol. Rev. 2014, 94, 355–382. [Google Scholar] [CrossRef]
- Mendoza, A.; Hollenberg, A.N. New insights into thyroid hormone action. Pharmacol. Ther. 2017, 173, 135–145. [Google Scholar] [CrossRef]
- Liu, Y.-C.; Yeh, C.-T.; Lin, K.-H. Molecular Functions of Thyroid Hormone Signaling in Regulation of Cancer Progression and Anti-Apoptosis. Int. J. Mol. Sci. 2019, 20, 4986. [Google Scholar] [CrossRef]
- Schroeder, A.C.; Privalsky, M.L. Thyroid Hormones, T3 and T4, in the Brain. Front. Endocrinol. 2014, 5, 40. [Google Scholar] [CrossRef] [PubMed]
- Chi, H.-C.; Tsai, C.-Y.; Tsai, M.-M.; Yeh, C.-T.; Lin, K.-H. Molecular functions and clinical impact of thyroid hormone-triggered autophagy in liver-related diseases. J. Biomed. Sci. 2019, 26, 24. [Google Scholar] [CrossRef] [PubMed]
- Fauquier, T.; Romero, E.; Picou, F.; Chatonnet, F.; Nguyen, X.-N.; Quignodon, L.; Flamant, F. Severe impairment of cerebellum development in mice expressing a dominant-negative mutation inactivating thyroid hormone receptor alpha1 isoform. Dev. Biol. 2011, 356, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Samuels, M.H. Psychiatric and cognitive manifestations of hypothyroidism. Curr. Opin. Endocrinol. Diabetes Obes. 2014, 21, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Göbel, A.; Göttlich, M.; Heldmann, M.; Georges, R.; Nieberding, R.; Rogge, B.; Sartorius, A.; Brabant, G.; Münte, T.F. Experimentally induced subclinical hypothyroidism causes decreased functional connectivity of the cuneus: A resting state fMRI study. Psychoneuroendocrinology 2019, 102, 158–163. [Google Scholar] [CrossRef]
- Levy, M.J.; Koulouri, O.; Gurnell, M. How to interpret thyroid function tests. Clin. Med. 2013, 13, 282–286. [Google Scholar] [CrossRef]
- Mladěnka, P.; Applová, L.; Patočka, J.; Costa, V.M.; Remiao, F.; Pourová, J.; Mladěnka, A.; Karlíčková, J.; Jahodář, L.; Vopršalová, M.; et al. Comprehensive review of cardiovascular toxicity of drugs and related agents. Med. Res. Rev. 2018, 38, 1332–1403. [Google Scholar] [CrossRef] [PubMed]
- Al-Hussaniy, H.A.; Alburghaif, A.H.; Alkhafaje, Z.; Al-Zobaidy, M.A.-H.J.; Alkuraishy, H.M.; Mostafa-Hedeab, G.; Azam, F.; Al-Samydai, A.M.; Al-Tameemi, Z.S.; Naji, M.A. Chemotherapy-induced cardiotoxicity: A new perspective on the role of Digoxin, ATG7 activators, Resveratrol, and herbal drugs. J. Med. Life 2023, 16, 491–500. [Google Scholar] [CrossRef]
- Lazar, L.; Csapo, M. Chemotherapy-Induced Cardiotoxicity: Pathophysiology and Prevention. Med. Pharm. Rep. 2014, 87, 135–142. [Google Scholar] [CrossRef]
- Chatterjee, K.; Zhang, J.; Honbo, N.; Karliner, J.S. Doxorubicin Cardiomyopathy. Cardiology 2010, 115, 155–162. [Google Scholar] [CrossRef]
- Volkova, M.; Russell, R. Anthracycline Cardiotoxicity: Prevalence, Pathogenesis and Treatment. Curr. Cardiol. Rev. 2012, 7, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Vriens, B.E.P.J.; Aarts, M.J.B.; de Vries, B.; van Gastel, S.M.; Wals, J.; Smilde, T.J.; van Warmerdam, L.J.C.; de Boer, M.; van Spronsen, D.J.; Borm, G.F.; et al. Doxorubicin/cyclophosphamide with concurrent versus sequential docetaxel as neoadjuvant treatment in patients with breast cancer. Eur. J. Cancer 2013, 49, 3102–3110. [Google Scholar] [CrossRef] [PubMed]
- Mancilla, T.R.; Iskra, B.; Aune, G.J. Doxorubicin-Induced Cardiomyopathy in Children. Compr. Physiol. 2019, 9, 905–931. [Google Scholar] [PubMed]
- Armenian, S.H.; Lacchetti, C.; Barac, A.; Carver, J.; Constine, L.S.; Denduluri, N.; Dent, S.; Douglas, P.S.; Durand, J.-B.; Ewer, M.; et al. Prevention and Monitoring of Cardiac Dysfunction in Survivors of Adult Cancers: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2017, 35, 893–911. [Google Scholar] [CrossRef] [PubMed]
- Babuin, L.; Jaffe, A.S. Troponin: The biomarker of choice for the detection of cardiac injury. Can. Med. Assoc. J. 2005, 173, 1191–1202. [Google Scholar] [CrossRef]
- Aydin, S.; Ugur, K.; Aydin, S.; Sahin, İ.; Yardim, M. Biomarkers in acute myocardial infarction: Current perspectives. Vasc. Health Risk Manag. 2019, 15, 1–10. [Google Scholar] [CrossRef]
- Zilinyi, R.; Czompa, A.; Czegledi, A.; Gajtko, A.; Pituk, D.; Lekli, I.; Tosaki, A. The Cardioprotective Effect of Metformin in Doxorubicin-Induced Cardiotoxicity: The Role of Autophagy. Molecules 2018, 23, 1184. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhou, F.; Guan, J.; Zhou, L.; Chen, B. Action Mechanism of Metformin and Its Application in Hematological Malignancy Treatments: A Review. Biomolecules 2023, 13, 250. [Google Scholar] [CrossRef]
- Argun, M.; Uzum, K.; Sonmez, M.F.; Ozyurt, A.; Karabulut, D.; Soyersarica, Z.; Cilenk, K.T.; Unalmis, S.; Pamukcu, O.; Baykan, A.; et al. Cardioprotective effect of metformin against doxorubicin cardiotoxicity in rats. Anadolu Kardiyol. Derg./Anatol. J. Cardiol. 2015, 16, 234. [Google Scholar] [CrossRef]
- Serageldin, M.A.; Kassem, A.B.; El-Kerm, Y.; Helmy, M.W.; El-Mas, M.M.; El-Bassiouny, N.A. The Effect of Metformin on Chemotherapy-Induced Toxicities in Non-diabetic Breast Cancer Patients: A Randomised Controlled Study. Drug Saf. 2023, 46, 587–599. [Google Scholar] [CrossRef]
- Harada, N. Effects of metformin on blood glucose levels and bodyweight mediated through intestinal effects. J. Diabetes Investig. 2020, 11, 1420–1421. [Google Scholar] [CrossRef] [PubMed]
- Rojas, L.B.A.; Gomes, M.B. Metformin: An old but still the best treatment for type 2 diabetes. Diabetol. Metab. Syndr. 2013, 5, 6. [Google Scholar] [CrossRef] [PubMed]
- Baker, C.; Retzik-Stahr, C.; Singh, V.; Plomondon, R.; Anderson, V.; Rasouli, N. Should metformin remain the first-line therapy for treatment of type 2 diabetes? Ther. Adv. Endocrinol. Metab. 2021, 12, 2042018820980225. [Google Scholar] [CrossRef] [PubMed]
- Genazzani, A.D.; Ricchieri, F.; Lanzoni, C. Use of Metformin in the Treatment of Polycystic Ovary Syndrome. Womens Health 2010, 6, 577–593. [Google Scholar] [CrossRef] [PubMed]
- Alhowail, A. Potential mechanisms of metformin-induced memory impairment. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 4757–4761. [Google Scholar] [CrossRef] [PubMed]
- Borchelt, D.R.; Zhou, W.; Kavelaars, A.; Heijnen, C.J. Metformin Prevents Cisplatin-Induced Cognitive Impairment and Brain Damage in Mice. PLoS ONE 2016, 11, e0151890. [Google Scholar] [CrossRef]
- Alhowail, A.; Almogbel, Y. Metformin administration increases the survival rate of doxorubicin-treated mice. Pharmazie 2019, 74, 737–739. [Google Scholar]
- Malaekeh-Nikouei, A.; Shokri-Naei, S.; Karbasforoushan, S.; Bahari, H.; Baradaran Rahimi, V.; Heidari, R.; Askari, V.R. Metformin beyond an anti-diabetic agent: A comprehensive and mechanistic review on its effects against natural and chemical toxins. Biomed. Pharmacother. 2023, 165, 115263. [Google Scholar] [CrossRef]
- Alhowail, A.H.; Almogbel, Y.S.; Abdellatif, A.A.H.; Alsalehi, N.F.; Alghenaim, F.A.; Aldubayan, M.A.; Felemban, S.G. CMF and MET treatment induce cognitive impairment through upregulation of IL-1alpha in rat brain. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 4385–4393. [Google Scholar] [CrossRef]
- Mani, V.; Arfeen, M.; Mohammed, H.A.; Elsisi, H.A.; Sajid, S.; Almogbel, Y.; Aldubayan, M.; Dhanasekaran, M.; Alhowail, A. Sukkari dates seed improves type-2 diabetes mellitus-induced memory impairment by reducing blood glucose levels and enhancing brain cholinergic transmission: In vivo and molecular modeling studies. Saudi Pharm. J. 2022, 30, 750–763. [Google Scholar] [CrossRef]
- Alhowail, A.H.; Almogbel, Y.S.; Abdellatif, A.A.H.; Aldubayan, M.A.; Almami, I.S. Elucidating the mechanism underlying cognitive dysfunction by investigating the effects of CMF and MET treatment on hippocampal neurons. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Mortezaee, K.; Ahmadi, A.; Haghi-Aminjan, H.; Khanlarkhani, N.; Salehi, E.; Shabani Nashtaei, M.; Farhood, B.; Najafi, M.; Sahebkar, A. Thyroid function following breast cancer chemotherapy: A systematic review. J. Cell. Biochem. 2019, 120, 12101–12107. [Google Scholar] [CrossRef]
- Huang, J.; Jin, L.; Ji, G.; Xing, L.; Xu, C.; Xiong, X.; Li, H.; Wu, K.; Ren, G.; Kong, L. Implication from thyroid function decreasing during chemotherapy in breast cancer patients: Chemosensitization role of triiodothyronine. BMC Cancer 2013, 13, 334. [Google Scholar] [CrossRef]
- Razvi, S.; Jabbar, A.; Pingitore, A.; Danzi, S.; Biondi, B.; Klein, I.; Peeters, R.; Zaman, A.; Iervasi, G. Thyroid Hormones and Cardiovascular Function and Diseases. J. Am. Coll. Cardiol. 2018, 71, 1781–1796. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, O.M.; El-Gareib, A.W.; El-bakry, A.M.; Abd El-Tawab, S.M.; Ahmed, R.G. Thyroid hormones states and brain development interactions. Int. J. Dev. Neurosci. 2007, 26, 147–209. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, R.A.; Alam, M.F.; Alshahrani, S.; Jali, A.M.; Qahl, A.M.; Khalid, M.; Muzafar, H.M.A.; Alhamami, H.N.; Anwer, T. Capsaicin Ameliorates the Cyclophosphamide-Induced Cardiotoxicity by Inhibiting Free Radicals Generation, Inflammatory Cytokines, and Apoptotic Pathway in Rats. Life 2023, 13, 786. [Google Scholar] [CrossRef]
- Dyhl-Polk, A.; Schou, M.; Vistisen, K.K.; Sillesen, A.-S.; Serup-Hansen, E.; Faber, J.; Klausen, T.W.; Bojesen, S.E.; Vaage-Nilsen, M.; Nielsen, D.L. Myocardial Ischemia Induced by 5-Fluorouracil: A Prospective Electrocardiographic and Cardiac Biomarker Study. Oncologist 2021, 26, e403–e413. [Google Scholar] [CrossRef]
- Refaie, M.M.M.; Abdel-Gaber, S.A.; Rahman, S.A.A.E.; Hafez, S.M.N.A.; Khalaf, H.M. Cardioprotective effects of bosentan in 5-fluorouracil-induced cardiotoxicity. Toxicology 2022, 465, 153042. [Google Scholar] [CrossRef]
- El Kiki, S.M.; Omran, M.M.; Mansour, H.H.; Hasan, H.F. Metformin and/or low dose radiation reduces cardiotoxicity and apoptosis induced by cyclophosphamide through SIRT-1/SOD and BAX/Bcl-2 pathways in rats. Mol. Biol. Rep. 2020, 47, 5115–5126. [Google Scholar] [CrossRef]
- Shiga, T.; Hiraide, M. Cardiotoxicities of 5-Fluorouracil and Other Fluoropyrimidines. Curr. Treat. Options Oncol. 2020, 21, 27. [Google Scholar] [CrossRef]
- Bakry, H.M.; Mansour, N.O.; ElKhodary, T.R.; Soliman, M.M. Efficacy of metformin in prevention of paclitaxel-induced peripheral neuropathy in breast cancer patients: A randomized controlled trial. Front. Pharmacol. 2023, 14, 1181312. [Google Scholar] [CrossRef] [PubMed]
- Kelleni, M.T.; Amin, E.F.; Abdelrahman, A.M. Effect of Metformin and Sitagliptin on Doxorubicin-Induced Cardiotoxicity in Rats: Impact of Oxidative Stress, Inflammation, and Apoptosis. J. Toxicol. 2015, 2015, 424813. [Google Scholar] [CrossRef] [PubMed]
- Ajzashokouhi, A.H.; Bostan, H.B.; Jomezadeh, V.; Hayes, A.W.; Karimi, G. A review on the cardioprotective mechanisms of metformin against doxorubicin. Hum. Exp. Toxicol. 2020, 39, 237–248. [Google Scholar] [CrossRef] [PubMed]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhowail, A.H.; Aldubayan, M.A. The Impact of Metformin on the Development of Hypothyroidism and Cardiotoxicity Induced by Cyclophosphamide, Methotrexate, and Fluorouracil in Rats. Pharmaceuticals 2023, 16, 1312. https://doi.org/10.3390/ph16091312
Alhowail AH, Aldubayan MA. The Impact of Metformin on the Development of Hypothyroidism and Cardiotoxicity Induced by Cyclophosphamide, Methotrexate, and Fluorouracil in Rats. Pharmaceuticals. 2023; 16(9):1312. https://doi.org/10.3390/ph16091312
Chicago/Turabian StyleAlhowail, Ahmad H., and Maha A. Aldubayan. 2023. "The Impact of Metformin on the Development of Hypothyroidism and Cardiotoxicity Induced by Cyclophosphamide, Methotrexate, and Fluorouracil in Rats" Pharmaceuticals 16, no. 9: 1312. https://doi.org/10.3390/ph16091312