

Impact of Repeated Doses of Subcutaneous Esketamine on Acute Dissociative Symptoms in Treatment-Resistant Depression
 and
and
Abstract
:1. Introduction
2. Results
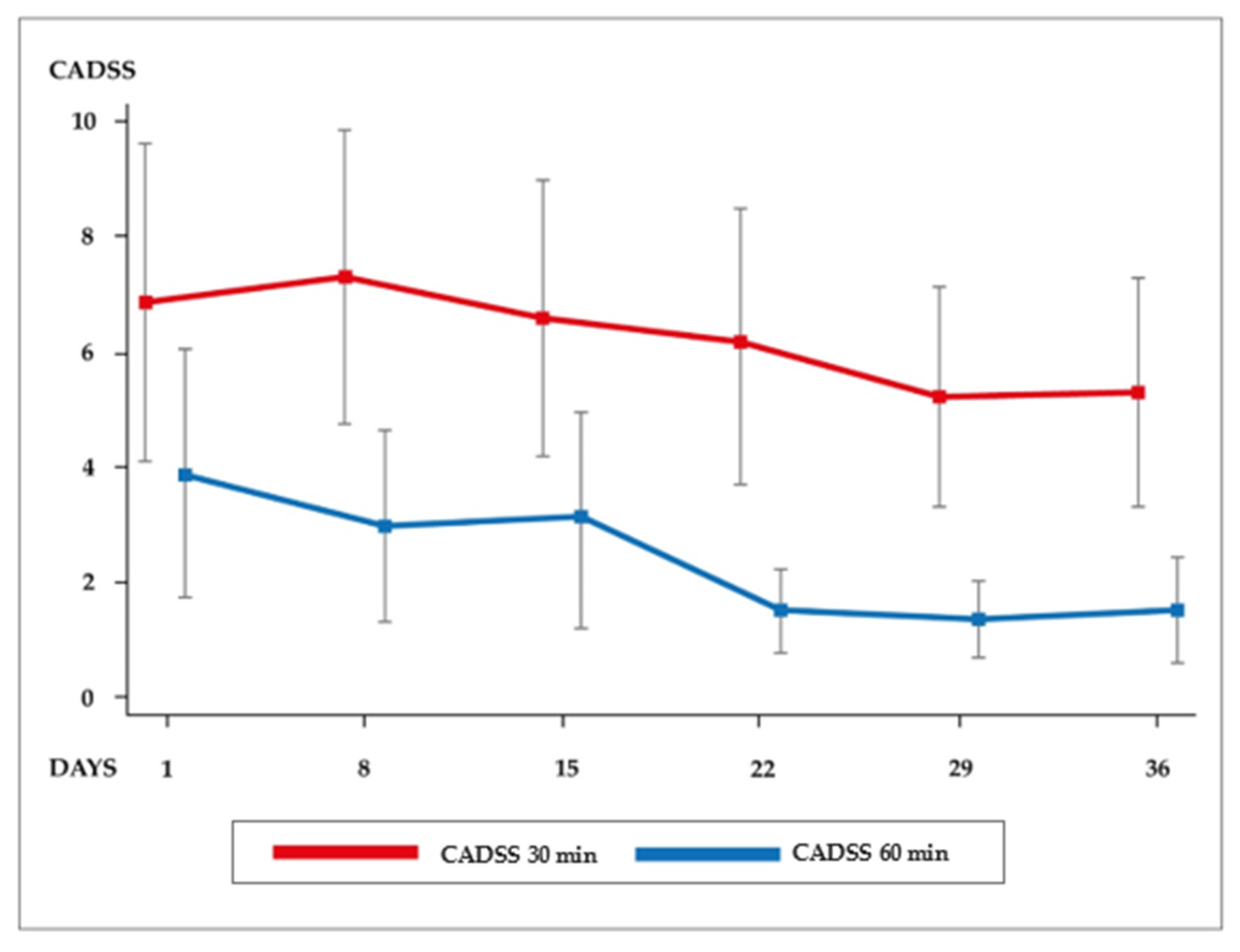
2.1. Dissociative Symptoms (CADSS Score) over Time
2.2. CADSS Scores over Time Adjusted by Dose
2.3. Mean CADSS Score over Time and Treatment Response
2.4. Mean CADSS Score over Time by Demographic and Clinical Characteristics
2.5. Mean CADSS Score over Time by Medication
3. Discussion
4. Materials and Methods
4.1. Procedures
4.2. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D.; Niederehe, G.; Thase, M.E.; Lavori, P.W.; Lebowitz, B.; et al. Acute and longer- term outcomes in depressed outpatients requiring one or several treatment steps: A STAR*D report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef] [PubMed]
- Berman, R.M.; Cappiello, A.; Anand, A.; Oren, D.A.; Heninger, G.R.; Charney, D.S.; Krystal, J.H. Antidepressant effects of ketamine in depressed patients. Biol. Psychiatry 2000, 47, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Canuso, C.M.; Singh, J.B.; Fedgchin, M.; Alphs, L.; Lane, R.; Lim, P.; Pinter, C.; Hough, D.; Sanacora, G.; Manji, H.; et al. Efficacy and safety of intranasal esketamine for the rapid reduction of symptoms of depression and suicidality in patients at imminent risk for suicide: Results of a double-blind, randomized, placebo-controlled study. Am. J. Psychiatry 2018, 175, 620–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daly, E.J.; Singh, J.B.; Fedgchin, M.; Cooper, K.; Lim, P.; Shelton, R.C.; Thase, M.E.; Winokur, A.; Van Nueten, L.; Manji, H.; et al. Efficacy and safety of intranasal esketamine adjunctive to oral antidepressant therapy in treatment-resistant depression: A randomized clinical trial. JAMA Psychiatry 2018, 75, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Daly, E.J.; Trivedi, M.H.; Janik, A.; Li, H.; Zhang, Y.; Li, X.; Lane, R.; Lim, P.; Duca, A.R.; Hough, D.; et al. Efficacy of esketamine nasal spray plus oral antidepressant treatment for relapse prevention in patients with treatment-resistant depression: A randomized clinical trial. JAMA Psychiatry 2019, 76, 893–903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doherty, T.; Wajs, E.; Melkote, R.; Miller, J.; Singh, J.B.; Weber, M.A. Cardiac safety of esketamine nasal spray in treatment-resistant depression: Results from the clinical development program. CNS Drugs 2020, 34, 299–310. [Google Scholar] [CrossRef] [Green Version]
- Popova, V.; Daly, E.J.; Trivedi, M.; Cooper, K.; Lane, R.; Lim, P.; Mazzucco, C.; Hough, D.; Thase, M.E.; Shelton, R.C.; et al. Efficacy and safety of flexibly dosed esketamine nasal spray combined with a newly initiated oral antidepressant in treatment-resistant depression: A randomized double-blind active-controlled study. Am. J. Psychiatry 2019, 176, 428–438. [Google Scholar] [CrossRef]
- Sleigh, J.; Harvey, M.; Voss, L.; Denny, B. Ketamine—More mechanisms of action than just NMDA blockade. Trends Anaesth. Crit. Care 2014, 4, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Short, B.; Fong, J.; Galvez, V.; Shelker, W.; Loo, C.K. Side-effects associated with ketamine use in depression: A systematic review. Lancet Psychiatry 2018, 5, 65–78. [Google Scholar] [CrossRef]
- Del Sant, L.C.; Sarin, L.M.; Magalhaes, E.J.M.; Lucchese, A.C.; Tuena, M.A.; Nakahira, C.; Fava, V.A.R.; Delfino, R.; Surjan, J.; Steiglich, M.S.; et al. Effects of subcutaneous esketamine on blood pressure and heart rate in treatment- resistant depression. J. Psychopharmacol. 2020, 34, 1155–1162. [Google Scholar] [CrossRef]
- Gálvez, V.; O’Keefe, E.; Cotiga, L.; Leyden, J.; Harper, S.; Glue, P.; Mitchell, P.B.; Somogyi, A.A.; DeLory, A.; Loo, C.K. Long-lasting effects of a single subcutaneous dose of ketamine for treating melancholic depression: A case report. Biol. Psychiatry 2014, 76, e1–e2. [Google Scholar] [CrossRef]
- George, D.; Gálvez, V.; Martin, D.; Kumar, D.; Leyden, J.; Hadzi-Pavlovic, D.; Harper, S.; Brodaty, H.; Glue, P.; Taylor, R.; et al. Pilot randomized controlled trial of titrated subcutaneous ketamine in older patients with treatment-resistant depression. Am. J. Geriatr. Psychiatry 2017, 25, 1199–1209. [Google Scholar] [CrossRef]
- Glue, P.; Medlicott, N.J.; Harland, S.; Neehoff, S.; Anderson-Fahey, B.; Le Nedelec, M.; Gray, A.; McNaughton, N. Ketamine’s dose-related effects on anxiety symptoms in patients with treatment refractory anxiety disorders. J. Psychopharmacol. 2017, 31, 1302–1305. [Google Scholar] [CrossRef]
- Loo, C.K.; Gálvez, V.; O’Keefe, E.; Mitchell, P.B.; Hadzi-Pavlovic, D.; Leyden, J.; Harper, S.; Somogyi, A.A.; Lai, R.; Weickert, C.S.; et al. Placebo-controlled pilot trial testing dose titration and intravenous, intramuscular and subcutaneous routes for ketamine in depression. Acta Psychiatr. Scand. 2016, 134, 48–56. [Google Scholar] [CrossRef]
- Correia-Melo, F.S.; Leal, G.C.; Vieira, F.; Jesus-Nunes, A.P.; Mello, R.P.; Magnavita, G.; Caliman-Fontes, A.T.; Echegaray, M.V.; Bandeira, I.D.; Silva, S.S.; et al. Efficacy and safety of adjunctive therapy using esketamine or racemic ketamine for adult treatment-resistant depression: A randomized, double-blind, non-inferiority study. J. Affect. Disord. 2020, 264, 527–534. [Google Scholar] [CrossRef]
- Singh, J.B.; Fedgchin, M.; Daly, E.; Xi, L.; Melman, C.; De Bruecker, G.; Tadic, A.; Sienaert, P.; Wiegand, F.; Manji, H.; et al. Intravenous Esketamine in Adult Treatment-Resistant Depression: A Double-Blind, Double-Randomization, Placebo-Controlled Study. Biol. Psychiatry 2016, 80, 424–431. [Google Scholar] [CrossRef] [Green Version]
- Van Schalkwyk, G.I.; Wilkinson, S.T.; Davidson, L.; Silverman, W.K.; Sanacora, G. Acute psychoactive effects of intravenous ketamine during treatment of mood disorders: Analysis of the Clinician Administered Dissociative State Scale. J. Affect. Disord. 2018, 227, 11–16. [Google Scholar] [CrossRef]
- Fedgchin, M.; Trivedi, M.; Daly, E.J.; Melkote, R.; Lane, R.; Lim, P.; Vitagliano, D.; Blier, P.; Fava, M.; Liebowitz, M.; et al. Efficacy and Safety of Fixed-Dose Esketamine Nasal Spray Combined with a New Oral Antidepressant in Treatment-Resistant Depression: Results of a Randomized, Double-Blind, Active-Controlled Study (TRANSFORM-1). Int. J. Neuropsychopharmacol. 2019, 22, 616–630. [Google Scholar] [CrossRef] [Green Version]
- Fava, M.; Freeman, M.P.; Flynn, M.; Judge, H.; Hoeppner, B.B.; Cusin, C.; Ionescu, D.F.; Mathew, S.J.; Chang, L.C.; Iosifescu, D.V.; et al. Double-blind, placebo-controlled, dose-ranging trial of intravenous ketamine as adjunctive therapy in treatment-resistant depression (TRD). Mol. Psychiatry 2020, 25, 1592–1603. [Google Scholar] [CrossRef]
- Rodrigues, N.B.; McIntyre, R.S.; Lipsitz, O.; Lee, Y.; Cha, D.S.; Shekotikhina, M.; Vinberg, M.; Gill, H.; Subramaniapillai, M.; Kratiuk, K.; et al. A simplified 6-Item clinician administered dissociative symptom scale (CADSS-6) for monitoring dissociative effects of sub-anesthetic ketamine infusions. J. Affect. Disord. 2021, 282, 160–164. [Google Scholar] [CrossRef]
- Luckenbaugh, D.A.; Niciu, M.J.; Ionescu, D.F.; Nolan, N.M.; Richards, E.M.; Brutsche, N.E.; Guevara, S.; Zarate, C.A. Do the dissociative side effects of ketamine mediate its antidepressant effects? J. Affect. Disord. 2014, 159, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niciu, M.J.; Shovestul, B.J.; Jaso, B.A.; Farmer, C.; Luckenbaugh, D.A.; Brutsche, N.E.; Park, L.T.; Ballard, E.D.; Zarate, C.A. Features of dissociation differentially predict antidepressant response to ketamine in treatment-resistant depression. J. Affect. Disord. 2018, 232, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Acevedo-Diaz, E.E.; Cavanaugh, G.W.; Greenstein, D.; Kraus, C.; Kadriu, B.; Zarate, C.A.; Park, L.T. Comprehensive assessment of side effects associated with a single dose of ketamine in treatment-resistant depression. J. Affect. Disord. 2020, 263, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Derntl, B.; Hornung, J.; Sen, Z.D.; Colic, L.; Li, M.; Walter, M. Interaction of Sex and Age on the Dissociative Effects of Ketamine Action in Young Healthy Participants. Front. Neurosci. 2019, 13, 616. [Google Scholar] [CrossRef]
- Lucchese, A.C.; Sarin, L.M.; Magalhães, E.J.M.; Del Sant, L.C.; Puertas, C.B.; A Tuena, M.; Nakahira, C.; Fava, V.A.; Delfino, R.; Surjan, J.; et al. Repeated subcutaneous esketamine for treatment-resistant depression: Impact of the degree of treatment resistance and anxiety comorbidity. J. Psychopharmacol. 2021, 35, 142–149. [Google Scholar] [CrossRef]
- Bremner, J.D.; Krystal, J.H.; Putnam, F.W.; Southwick, S.M.; Marmar, C.; Charney, D.S.; Mazure, C.M. Measurement of dissociative states with the Clinician-Administered Dissociative States Scale (CADSS). J. Trauma Stress 1998, 11, 125–136. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Variables | Clinical Variables | Current Pharmacotherapies | |||
|---|---|---|---|---|---|
| Variables | N/Mean (%/SD) | Variables | N/Mean (%/SD) | Variables | N (%) |
| Age (years) | 40.31 (12.67) | Diagnosis | Adjunctive Treatment | 64 (91.42) | |
| Gender (female) | 45 (64.30) | MDD BD | 39 (55.71) 31 (44.29) | Antidepressants | 48 (68.57) |
| Education (college graduate) | 41 (55.57) | Severity | Antipsychotics | 41 (58.57) | |
| Occupational status (employed) | 16 (22.86) | Baseline MADRS | 33.6 (6.32) | Lithium | 30 (42.85) |
| Maudslay * | 11.09 (2.03) | Anticonvulsants | 37 (52.85) | ||
| Anxiety Disorder | 31 (44.29) | Benzodiazepines | 26 (37.14) | ||
| BMI | 29.1 (7.5) | ||||
| Clinical Comorbidity | 57 (81.42) | ||||
| Obesity | 24 (34.29) | ||||
| Hypertension | 12 (17.14) | ||||
| 30 min | 60 min | |||
|---|---|---|---|---|
| Coefficient (CI 95%) | p | Coefficient (CI 95%) | p | |
| Day 1 | 0.483 | 0.006 | ||
| Day 8 | 0.01 (−2.56–2.58) | 0.994 | −1.62 (−3.46–0.22) | 0.084 |
| Day 15 | −1.08 (−4.28–2.11) | 0.507 | −2.21 (−4.45–0.03) | 0.053 |
| Day 22 | −1.62 (−5.03–1.80) | 0.354 | −4.01 (−6.39–−1.63) | 0.001 a |
| Day 29 | −2.59 (−6.08–0.89) | 0.145 | −4.26 (−6.69–−1.84) | 0.001 a |
| Day 36 | −2.52 (−6.06–1.02) | 0.164 | −4.10 (−6.56–−1.63) | 0.001 a |
| Dose | 2.29 (−4.40–8.98) | 0.502 | 4.38 (−0.10–8.86) | 0.055 |
| Constant | 5.74 (1.63–9.85) | 0.006 | 1.65 (−1.04–4.34) | 0.230 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Del Sant, L.C.; Sarin, L.M.; Lucchese, A.C.; Magalhães, E.J.M.; Tuena, M.A.; Nakahira, C.; Del Porto, J.A.; De Lacerda, A.L.T.; Mari, J.d.J. Impact of Repeated Doses of Subcutaneous Esketamine on Acute Dissociative Symptoms in Treatment-Resistant Depression. Pharmaceuticals 2023, 16, 31. https://doi.org/10.3390/ph16010031
Del Sant LC, Sarin LM, Lucchese AC, Magalhães EJM, Tuena MA, Nakahira C, Del Porto JA, De Lacerda ALT, Mari JdJ. Impact of Repeated Doses of Subcutaneous Esketamine on Acute Dissociative Symptoms in Treatment-Resistant Depression. Pharmaceuticals. 2023; 16(1):31. https://doi.org/10.3390/ph16010031
Chicago/Turabian StyleDel Sant, Lorena Catarina, Luciana Maria Sarin, Ana Cecília Lucchese, Eduardo Jorge Muniz Magalhães, Marco Aurélio Tuena, Carolina Nakahira, José Alberto Del Porto, Acioly Luiz Tavares De Lacerda, and Jair de Jesus Mari. 2023. "Impact of Repeated Doses of Subcutaneous Esketamine on Acute Dissociative Symptoms in Treatment-Resistant Depression" Pharmaceuticals 16, no. 1: 31. https://doi.org/10.3390/ph16010031