
Ocular Manifestations of Flavivirus Infections
by
 ,
,
Sourour Meziou Zina
1,2,
Gautier Hoarau
1,
Marc Labetoulle
1,3,
Moncef Khairallah
2 and
Antoine Rousseau
1,3,* 1
Department of Ophthalmology, Bicêtre Hospital, Public Assistance, Hospitals of Paris, Reference Network for Rare Diseases in Ophthalmology (OPHTARA), 94270 Le Kremlin-Bicêtre, France
2
Department of Ophthalmology, Faculty of Medicine, University of Monastir, Monastir 5019, Tunisia
3
Center for Immunology of Viral, Auto-Immune, Hematological and Bacterial Diseases (IMVA-HB), Infectious Diseases Models for Innovative Therapies (IDMIT), French Alternative Energies and Atomic Commission (CEA), 92260 Fontenay-aux-Roses, France
*
Author to whom correspondence should be addressed.
Pathogens 2023, 12(12), 1457; https://doi.org/10.3390/pathogens12121457
Submission received: 25 October 2023
/
Revised: 4 December 2023
/
Accepted: 12 December 2023
/
Published: 15 December 2023
(This article belongs to the Special Issue Current Advances in Flavivirus and Other Arboviruses)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Flaviviruses are a group of positive-sense, single-stranded RNA viruses predominantly transmitted by arthropods (mainly mosquitoes) that cause severe endemic infections and epidemics on a global scale. They represent a major cause of systemic morbidity and death and are expanding worldwide. Among this group, dengue fever, the West Nile virus, yellow fever, Japanese Encephalitis, and, recently, the Zika virus have been linked to a spectrum of ocular manifestations. These manifestations encompass subconjunctival hemorrhages and conjunctivitis, anterior and posterior uveitis (inclusive of vitritis, chorioretinitis, and retinal vasculitis), maculopathy, retinal hemorrhages, and optic neuritis. Clinical diagnosis of these infectious diseases is primarily based on epidemiological data, history, systemic symptoms and signs, and the pattern of ocular involvement. Diagnosis confirmation relies on laboratory testing, including RT-PCR and serological testing. Ocular involvement typically follows a self-limited course but can result in irreversible visual impairment. Effective treatments of flavivirus infections are currently unavailable. Prevention remains the mainstay for arthropod vector and zoonotic disease control. Effective vaccines are available only for the yellow fever virus, dengue virus, and Japanese Encephalitis virus. This review comprehensively summarizes the current knowledge regarding the ophthalmic manifestations of the foremost flavivirus-associated human diseases.
1. Introduction
Flaviviruses constitute a group of 90 positive-sense, single-stranded RNA viruses, with 30 capable of causing severe disease in both humans and animals. This viral family is primarily transmitted by hematophagous arthropods, notably ticks and mosquitoes, resulting in widespread endemic infections and global epidemics [1,2]. Some members of the flavivirus family continue to pose a significant global threat, leading to systemic morbidity and an expanding worldwide mortality [3]. Flaviviral infections often manifest as either asymptomatic or non-specific febrile illnesses. However, severe and potentially fatal systemic complications, such as hemorrhagic fever and neurological involvement, can occur. In addition to systemic infections that entail hemorrhages, vascular leakage, encephalitis, microcephaly, and Guillain–Barre syndrome, certain specific flaviviruses, including dengue fever (DFV), West Nile virus (WNV), yellow fever virus (YFV), Japanese Encephalitis virus (JEV), and Zika virus, have recently been linked to uveitis and other ocular manifestations [4,5,6,7,8]. There are no specific antiviral therapies for flavivirus infections and treatment is essentially symptomatic [3,4,5,7]. This manuscript aims to provide an overview of the ophthalmic manifestations associated with the most significant flavivirus-related human diseases.
2. General Aspects
2.1. Virological Features
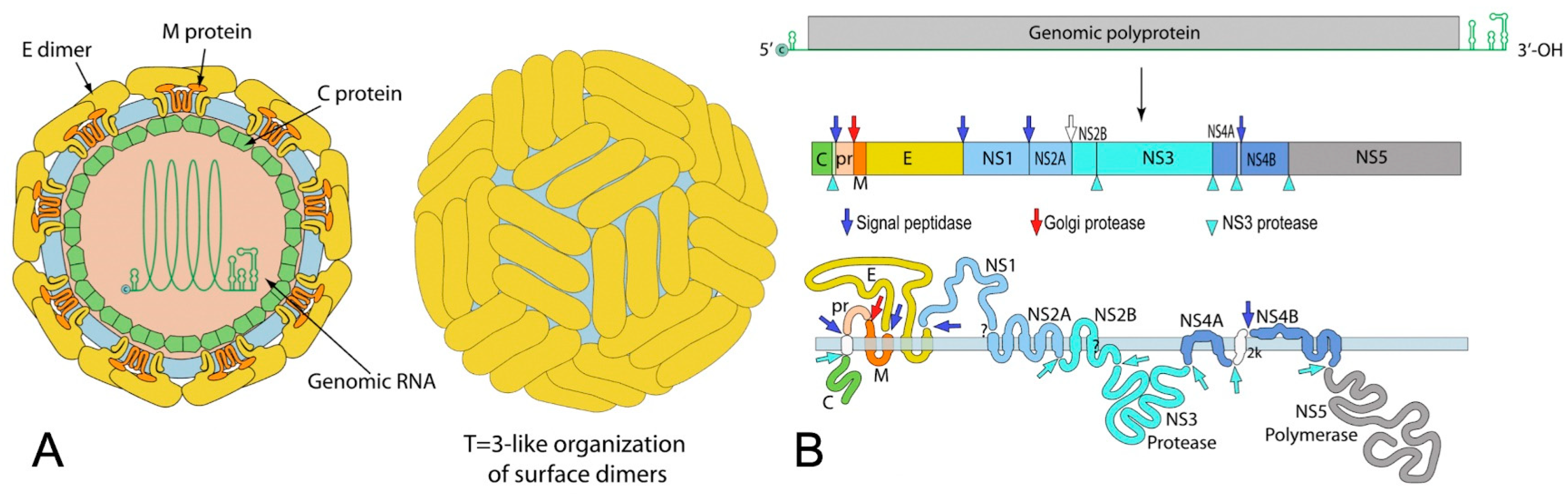
Flaviviruses are a family of enveloped viruses with a compact, positive-sense, single-stranded RNA genome of approximately 10.5 kb (Figure 1). This genome encodes three structural and seven non-structural proteins. These ten essential proteins serve crucial functions in virion assembly, cell receptor binding and entry, viral polyprotein processing, and viral replication. After entering the host via an infected vector, the virus infects macrophages, monocytes, and dendritic cells [9,10,11]. Flaviviruses enter cells through receptor-mediated endocytosis, binding with host endosomes in an acidic environment, leading to conformational changes in their envelope (E) glycoprotein [2]. These changes facilitate fusion of the host and viral membranes, releasing the nucleocapsid and viral RNA genome into the host cell’s cytoplasm. The polypeptide is then translated into the ten viral proteins, comprising three structural proteins (C, prM, and E protein) and seven non-structural proteins (NS1, NS2A, NS2B, NS3, NS4A, NS4B, and NS5) [1,2]. The non-structural proteins oversee viral genome replication, budding, and the hijacking of host cell machinery. Following translation, RNA-dependent RNA polymerase (RdRp), NS5, generates a negative strand from genomic RNA, serving as a template for the production of a new positive strand. In the rough Endoplasmic Reticulum (ER), viral proteins commence assembly, packaging viral RNA with C, E, and prM structural proteins. Viral particles are subsequently transported to the trans-Golgi network, where prM is cleaved into M. The mature virus is then released from the host into the extracellular space through exocytosis [2].
2.2. Transmission
Flaviviruses persist in an enzootic cycle, primarily involving mosquitoes as the main vectors and mammals and birds as the amplifying hosts, and are incidentally transmitted to humans [3]. While arthropod-borne transmission is predominant, alternative transmission routes have been documented. For instance, WNV can be transmitted among humans via blood transfusions and organ transplants, or from mother to newborn through transplacental transmission [13,14,15]. WNV can also be transmitted orally in hamsters, birds, and mice [16,17,18]. Some cases of human-to-human DENV transmissions via blood transfusions have been reported [19,20]. JEV and Zika virus can be transmitted transplacentally from an infected mother to the fetus in the first and second trimester [21,22]. Seminal transmission of JEV in pigs, resulting in embryo abortion, has been documented [23]. Similarly, ZIKV has been shown to persist in bodily fluids, suggesting a route of horizontal transmission [24].
2.3. Diagnosis
The diagnosis of flavivirus infections is typically carried out using conventional methods, including serology and molecular assays [25]. Reverse Transcription Polymerase Chain Reaction (RT-PCR) is commonly employed during the early stage of the disease, typically within the first week of infection. Serological testing, specifically Enzyme-Linked Immunosorbent Assays (ELISAs), is generally used during the acute phase to detect IgM antibodies and in the later stages to detect IgG antibodies. However, it is important to note that cross-reactivity is common among viruses in the Flaviviridae family, which can reduce the specificity of the diagnosis [25]. In this context, a specific technique of ELISA called “antibody capture ELISA”, also known as “sandwich ELISA”, has been developed to enhance the accuracy of the assay [26]. Moreover, the plaque reduction neutralization test (PRNT), often considered as a gold standard, is used to confirm equivocal results. The PRNT is highly specific among serological assays, showing minimal cross-reactivity, and is used to detect neutralizing antibodies [25]. Finally, cell culture procedures may be conducted at designated research facilities, aimed at isolating the viral strain. Handling of the isolated virus should take place in biosafety level 3 laboratories, especially in the case of JEV [25,27].
3. Ocular Complications of Flaviviruses
3.1. Dengue Fever (DF)
3.1.1. Epidemiology
Dengue virus comprises four distinct serotypes (DF-1 to DF-4), each lacking cross-immunity, thus allowing for multiple dengue fever infections in a given individual [28]. Transmission occurs via the bite of an infected female Aedes aegypti/albopictus mosquito. Aedes albopictus vectors tend to trigger slower outbreaks compared to the rapid epidemics associated with Aedes aegypti [29]. DF ranks as a significant arthropod-borne disease in tropical and subtropical regions, endemic in over 100 countries spanning America, Southeast Asia, the Western Pacific, Africa, and the Eastern Mediterranean [30]. The incidence of DF has surged 30-fold in recent decades, affecting an estimated 390 million people annually [5]. This has resulted in approximately 96 million symptomatic infections yearly, with two million cases of severe dengue and an annual death toll of 21,000 [31,32,33]. Manifesting in endemic–epidemic cycles within densely populated tropical urban areas, the majority of infections occur in children across Asia and young adults within the American tropics, though the impact extends to other continents [34].
3.1.2. Systemic Manifestations
Dengue fever occurs 3–14 days after a mosquito bite [28]. Infection can be asymptomatic, result in a non-specific febrile illness, or exhibit classic DF symptoms, including a sudden high fever, a severe headache, myalgias, arthralgias, nausea, vomiting, hepatomegaly, lymphopenia, and a maculopapular rash. Most DF cases resolve spontaneously. However, a minority of patients may progress to a life-threatening condition known as dengue hemorrhagic fever (or dengue shock syndrome), characterized by thrombocytopenia, hypotension, and the potential for multi-system organ failure [5].
3.1.3. Ocular Manifestations
The precise incidence of ocular manifestations during DF remains uncertain since most studies focus on cases seen by hospital specialists. Nevertheless, reported incidences range from 7.1% to 40.3%, likely reflecting varying disease severities and the diverse ocular assessments used in each study [35,36]. Ocular involvement in DF, typically bilateral, can result from thrombocytopenia, inflammation, and ischemic mechanisms [5,37]. These ocular manifestations can occur from days to months after the onset of fever.
- -
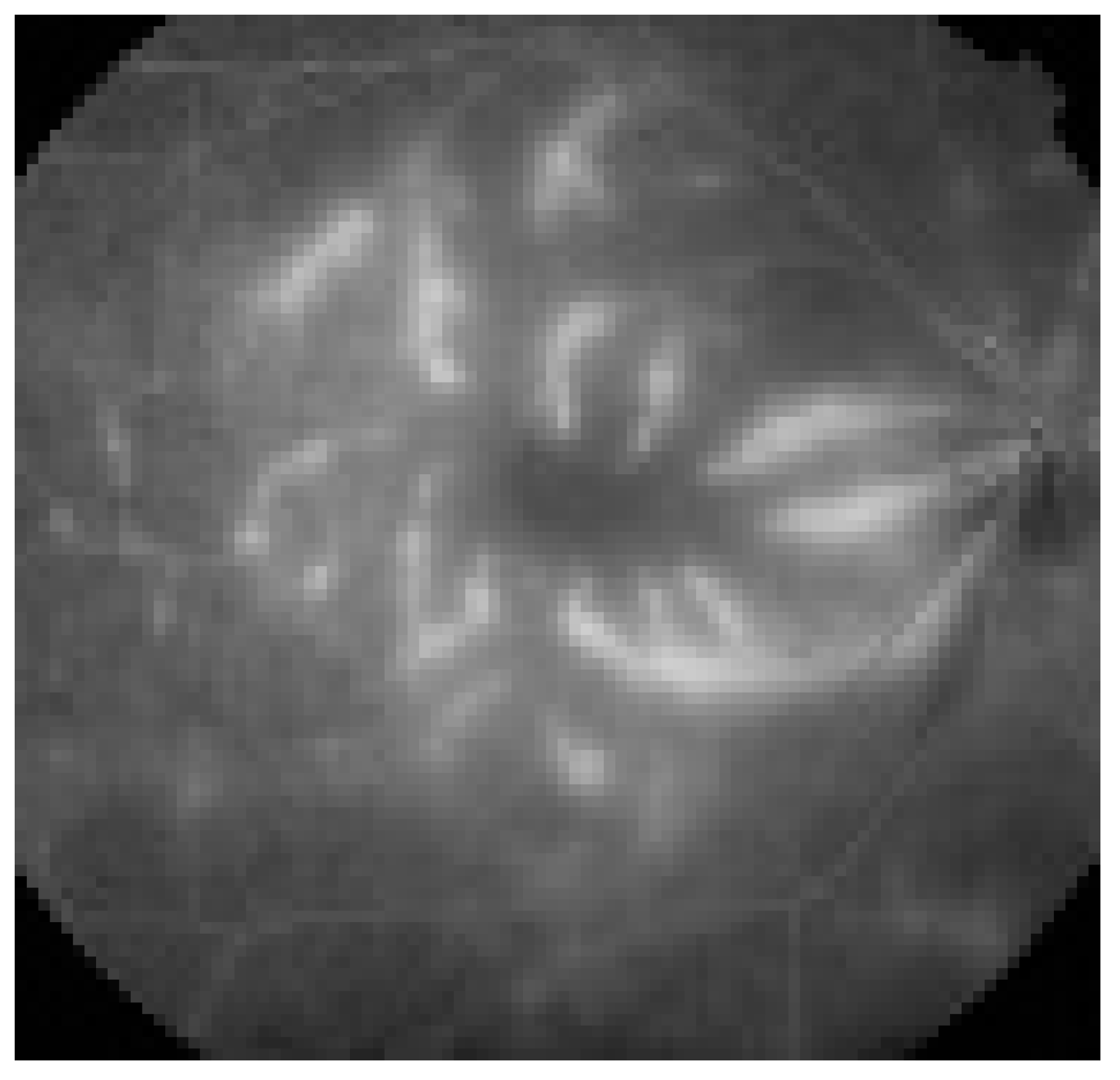
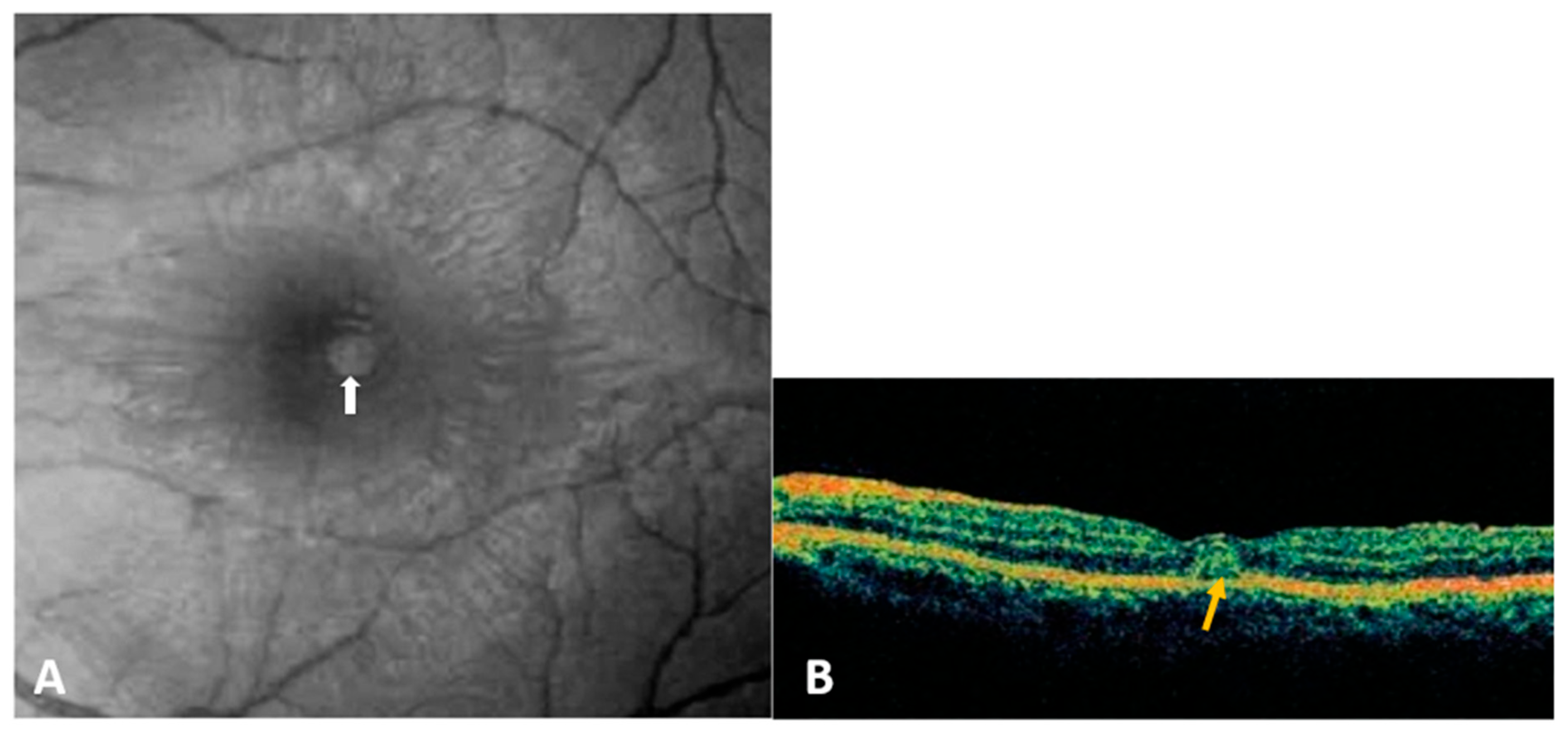
- Dengue-fever-associated maculopathy:DF-associated maculopathy, the most common ocular manifestation of acute DFV infection, is reported in 10% of hospitalized patients and is serotype-dependent [38,39]. Notably, one study linked maculopathy to serotype specificity, with a 10% incidence during DENV-1 epidemics but nothing during DENV-2 outbreaks [39]. Symptoms typically emerge 3–11 days after fever onset and improve over 2–4 weeks. Patients may present with sudden vision loss, central scotoma, or floaters. The lesions are typically asymmetric and often bilateral, primarily associated with intraretinal hemorrhages, manifesting as dots, blots, or flame-shaped hemorrhages. However, some patients remain asymptomatic, with lesions visible only through fluorescein or indocyanine green angiography (ICGA) [4,7,40,41]. Fluorescein angiography (FA) commonly reveals retinal vascular leakage (Figure 2) and occlusion, while ICGA identifies hypofluorescent spots corresponding to subretinal lesions and additional spots in areas without clinically evident dots [37]. OCT is valuable for detecting and monitoring dengue-induced inflammatory ischemic foveolitis and outer maculopathy, showing disruptions in outer retinal layers, conical foveal elevation, and focal thickening of the outer neurosensory retina RPE, aligning with round foveal yellowish lesions seen clinically (Figure 3). OCT is also instrumental in detecting and assessing associated serous retinal detachment (SRD) and macular edema. Teoh et al. used OCT to categorize patients into three groups: (1) diffuse retinal thickening, (2) cystoid macular edema, and (3) foveolitis. Their findings were correlated with visual acuity and prognosis [40]. DF-related foveolitis pertains to the yellow-orange central foveal lesion in patients with dengue maculopathy, visible on OCT as conical foveal elevation and focal outer neurosensory RPE thickening, often associated with prolonged scotomata persistence [40,42]. In dengue-related maculopathy, the prevalence of cystoid macular edema and foveolitis was evaluated to 24.6% and 33.7%, respectively [40]. More recently, OCT–angiography (OCTA) has revealed ischemia in the deep retinal capillary plexus [40,43].
- -
- Other posterior segment manifestations
Other posterior ocular features associated with DF include posterior uveitis and, less commonly, vascular occlusions, panuveitis, vitritis, retinal and vitreous hemorrhages, choroidal changes, and yellow sub-retinal spots [6,37,42,44,45]. A study of patients (eyes, n = 65) with ocular manifestations of DF reported a prevalence of retinal vasculitis in 23.1% of cases [40].
- -
- Anterior segment manifestations
In addition to the common subconjunctival hemorrhages observed in nearly half of the patients, reported anterior segment manifestations include anterior uveitis (7.7%) and, less frequently, shallow anterior chambers, acute angle-closure glaucoma due to ciliochoroidal effusion, superficial corneal punctate erosions, keratitis, and scleritis [7,36,42,46,47,48].
- -
- Other ocular manifestations
3.1.4. Diagnosis
DF diagnosis relies on the characteristic clinical presentation and is confirmed through laboratory tests, including dengue virus nonstructural protein 1 detection and IgM/IgG antibody analysis [6,46]. Real-time RT-PCR or NS1 antigen detection is used for confirmation within the first 5 days, while ELISA-based detection of anti-dengue IgM or seroconversion in paired acute and convalescent serum samples are the more common methods for confirmation after 5 days [28]. Reported sensitivities of RT-PCR vary widely in the medical literature, ranging from 48.4% to 98.2% depending on sample timing [51]. Sensitivity is higher during the acute phase, coinciding with viremia. Additionally, sensitivity tends to be higher in primary infections compared to secondary infections, indicating the influence of the immune response [52]. RNA detection in urine samples extends beyond the viremic period by up to 16 days, with an estimated sensitivity ranging between 50% and 80% [53].
3.1.5. Treatment and Prognosis
Treatment is essentially symptomatic [54]. In most cases, ocular manifestations resolve spontaneously with a favorable visual prognosis. However, severe cases have been treated with customized immunomodulatory therapies, including topical, periocular, oral, and intravenous steroids and immune globulins, with varying degrees of success depending on clinical presentation [41,55]. Various herbal remedies, such as Carica papaya, have been employed in treating DF [56]. A meta-analysis on Carica papaya indicated potential benefits in improving the platelet count during DF and reducing hospital stays, although the evidence quality was low [57]. The visual prognosis is good in most patients. However, permanent visual impairment may occur mainly due to retinal vasculitis, dengue maculopathy, or optic neuropathy [6].
Two live-attenuated tetravalent vaccines are currently available. Dengvaxia® (Sanofi Pasteur, Chimeric viruses YFV/DEN1-4) is administered in three doses spaced six months apart. Its use is reserved for populations in which the seroprevalence is over 70% in the age bracket for vaccination, due to the weak efficacy of the vaccine and the potential long-term risks of severe DF in vaccinated seronegative subjects. The efficacy rate over the initial 25 months was assessed as 60.3% [58]. Vaccination is not recommended for children under 9 years of age [59]. More recently, Qdenga® (Takeda, chimeric viruses DEN-2 PDK-53, DEN-1,-3,-4), administered in two doses with a 3-month interval, has received marketing authorization. The efficacy after two doses in children aged 4 to 16 years was assessed as 80.2% within 12 months [60]. At 18 months, the efficacy was lower, at 76.1% in immune recipients and 66.2% in non-immune recipients [61]. Vaccination can be performed in persons aged above 4, regardless of past dengue virus infection.
3.2. West Nile Virus (WNV) Infection
3.2.1. Epidemiology
The West Nile virus (WNV), a zoonotic disease within the Japanese encephalitis serocomplex of viruses [62], has five distinct phylogenetic lineages. Among these, lineage one, which is globally distributed, and lineage two, primarily found in Africa, are known to cause human disease [62,63]. WNV primarily resides in birds, with transmission to humans occurring via Culex mosquitoes. Bird–mosquito–human transmission accounts for the majority of human cases [62]. The virus was first isolated in Uganda in 1937 and has since spread to Europe, Australia, Asia, and, since 1999, the United States, Canada, Mexico, the Caribbean, and parts of Central and South America [64]. Recently, co-circulation with the Usutu virus, another neurotropic mosquito-borne flavivirus, has been observed in Europe, raising the potential for WNV to expand to regions previously only affected by Usutu virus and vice versa [65].
3.2.2. Systemic Manifestations
The incubation period for WNV infection ranges from 3 to 14 days and is most often followed in humans by an asymptomatic infection. Only approximately 25% of infected persons develop a self-limiting, non-specific viral illness, including fever, headaches, fatigue, nausea and vomiting, lymphadenopathy, and skin rashes, that typically lasts less than a week [62]. Severe neurologic manifestations may develop in less than 1% of cases including encephalitis, meningoencephalitis, acute flaccid paralysis, movement disorders, poliomyelitis-like syndrome, and Guillain–Barré Syndrome [63]. Asymmetric paralysis of acute onset and absence of reflexes without pain are characteristic of WNV [66]. Neuroinvasive disease is associated with high rates of morbidity and mortality, especially in patients with an advanced age or diabetes [66].
3.2.3. Ocular Manifestations
Multifocal chorioretinitis, typically bilateral, is the most common ocular manifestation of acute WNV infection, occurring in nearly 80% of patients with neurologic symptoms [67,68]. However, the reported rate of multifocal chorioretinitis varies widely in the literature, ranging from 14% to 79% [69]. There appears to be an increased prevalence of multifocal chorioretinitis associated with the presence of neurological manifestations. [70]. WNV-associated chorioretinitis often presents with minimal symptoms, such as floaters, a mild vision reduction, redness, ocular pain, visual field defects, or diplopia [4,7,67,71,72].
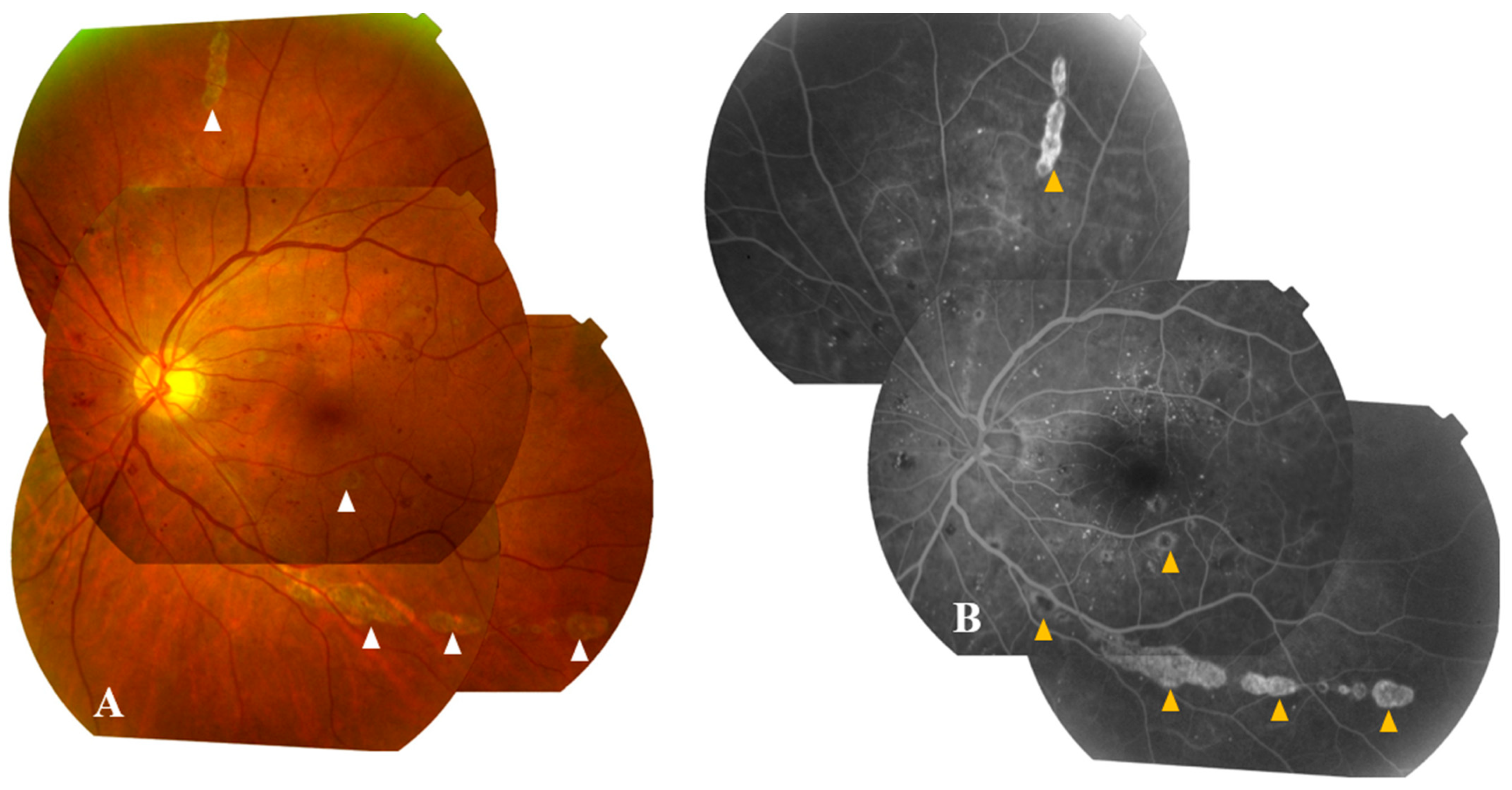
Active chorioretinal lesions are circular, deep, and yellowish on ophthalmoscopy, with early hypofluorescence and late staining on FA [67]. Inactive lesions appear round and atrophic, sometimes with central pigmentation, typically showing a “target-like appearance” on FA, featuring central hypofluorescence and peripheral hyperfluorescence (Figure 4) [67]. These lesions vary in number and size (ranging from 100 to 1500 µm in diameter), involving the midperiphery, possibly with posterior pole involvement [7,67]. They typically align radially in the nasal and peripheral fundus or follow a curvilinear pattern in the temporal posterior fundus, associated with the course of retinal nerve fibers [67,73].
OCT through lesions reveals their deep retinal location with focal disruption of the outer nuclear layer and retinal pigment epithelium (RPE) [74]. ICGA highlights well-defined hypofluorescent choroidal spots, often more numerous than clinically appreciated or seen on FA [75]. Chorioretinitis is more common in individuals over 50 and those with diabetes mellitus, with a significant proportion also displaying concurrent diabetic retinopathy.
Other manifestations have been described, including non-granulomatous anterior uveitis, retinal hemorrhages, focal or diffuse retinal vascular sheathing, vascular leakage, occlusive vasculitis, congenital chorioretinal scarring, zones of atrophy and mottling of the RPE, macular edema, optic neuritis, papilledema, and binocular diplopia related to sixth cranial nerve involvement [6,7,44,67,68,72,76,77]. Patients (n = 51 eyes) with intraocular inflammation tested positive for WNV-related vitritis (73%), papilledema (14%), intraretinal hemorrhages (43%), vasculitis (32%), and retinal occlusive vasculitis (16%) [71].
Noteworthy, OCTA allows for the detection and precise delineation of areas of retinal capillary nonperfusion in both the superficial and deep capillary plexuses in cases of associated occlusive retinal vasculitis [78].
3.2.4. Diagnosis
WNV infection is diagnosed primarily based on clinical features and confirmed through the detection of IgM antibodies in serum or cerebrospinal fluid [79]. However, serological tests may show cross-reactivity with other flaviviruses or yield false negative results [25]. Therefore, virus detection using RT-PCR is increasingly becoming the gold standard for WNV diagnosis [79]. During the viremic period, RT-PCR sensitivity was evaluated at 86.8% in whole-blood samples [80]. Detection rates were lower in serum, cerebrospinal fluid, plasma, and urine, respectively, at 26%, 16.6%, 20%, and 58.3% [80].
3.2.5. Treatment and Prognosis
Neurological manifestations are addressed through intensive supportive care. Ongoing clinical trials are exploring novel therapeutic strategies, including interferon alpha-2b, interferon beta, and high-titer intravenous immunoglobulin [81,82,83]. Potential in vitro antiviral compounds include Delphinidin and Epigallocatechin Gallate [84]. The primary approach to WNV infection control remains prevention, achieved by reducing mosquito populations (such as draining standing water and using larvicides) and implementing personal protection measures (such as repellents, window screens, and protective clothing) [62]. Four veterinary vaccines are approved for use in horses, requiring annual boosters [85]. Currently, there are no licensed human vaccines available. Only phase 2 clinical trials have been conducted [86]. A live attenuated chimeric vaccine (ChimeriVax WN02) elicited immunogenicity after a single dose. A predictive model indicated that effective WNV vaccination in areas with increased incidence could potentially reduce the annual morbidity of neuroinvasive diseases cases by 30% and deaths by 60% in the United States [87].
Specific ophthalmic treatments may be necessary to address intraocular inflammation or posterior segment complications. These treatments include topical steroids for anterior uveitis, peripheral retinal photocoagulation for neovascularization resulting from occlusive vasculitis, pars plana vitrectomy for non-clearing vitreous hemorrhage or tractional retinal detachment, and intravitreal injection of anti-vascular endothelial growth factor agents for choroidal neovascularization or associated macular edema in cases of chorioretinitis [88,89,90]. The benefit of systemic steroids is not evidence-based, but the positive role in recovery could justify their use in cases of severe posterior segment involvement. Ocular diseases associated with WNV infection usually have a self-limited course, and visual acuity returns to baseline in most patients [67]. However, persistent visual impairment can occur due to various factors, including chorioretinal scarring, choroidal neovascularization, vitreous hemorrhage, tractional retinal detachment, severe ischemic maculopathy, optic atrophy, and retrogeniculate damage [6,44,67,68,76,91,92].
3.3. Yellow Fever Virus
3.3.1. Epidemiology
Yellow fever virus (YFV) is primarily transmitted to humans through bites from infected Aedes aegypti and Aedes albopictus mosquitoes. It is maintained through sylvatic (jungle) transmission cycles involving mosquitoes and non-human primates, as well as mosquito–human transmission cycles in urban areas [93,94]. YFV is a re-emerging arboviral disease that can potentially be lethal, causing an estimated 30,000–60,000 fatalities annually in endemic regions across Africa, South, and Central America [95].
3.3.2. Systemic Manifestations
Yellow fever is characterized by rapid jaundice development and liver dysfunction, which are distinctive clinical features of the disease. Most YFV-infected individuals are either asymptomatic or experience an acute febrile phase lasting around 4 days, accompanied by symptoms like myalgia, headaches, back pain, nausea, and vomiting. This phase typically resolves within days. However, approximately 15–25% of patients progress to a severe toxic form of the disease, which includes symptoms such as viremia, fever, jaundice, prostration, hematemesis, hemorrhagic diathesis, and failure of the liver, kidneys, and myocardium. This severe form is associated with a 50% mortality rate [93].
3.3.3. Ocular Manifestations
In the initial phase of yellow fever, conjunctivitis is the most common ocular finding. However, scleral icterus often occurs during the toxic phase [4,7]. Some case reports have suggested additional ocular manifestations. In yellow fever patients, retinopathy may occur in 20% of cases [96], which includes retinal nerve fiber layer infarcts (55%), superficial hemorrhages (35%), and grayish deep lesions (30%). Silvana Vianello et al. documented two intensive care patients in Brazil who exhibited increased choroidal thickness bilaterally, with retinal vein congestion in one patient and a 360° mid-peripheral choroidal detachment with yellowish subretinal lesions in the other patient [97]. Another publication reported the case of a 53-year-old Brazilian patient with a YFV infection with a unilateral retinal edema, macular exudates, and hemorrhages during the convalescent stage, possibly due to an immune-mediated mechanism rather than direct viral invasion or infection of the ocular tissues [97].
3.3.4. Diagnosis
Diagnosis of YFV is based on PCR of blood or urine samples in the early stages, and ELISA or PRNT antibody detection in later stages [93,97]. Data regarding PCR sensitivities are scarce. A Brazilian study conducted after the last outbreak from 2016 to 2018 indicated detection rates of 8.9% in serum and 50% in blood samples during the viremic phase [98]. Urine sample sensitivity was evaluated as 25% [99]. The RNA recovery in urine samples could extend up to 69 days after symptom onset [99].
3.3.5. Treatment and Prognosis
The development of two live-attenuated YF vaccines in the 1930s and their wide deployment in the 1940s led to a significant decline in the disease. The historical 17 D strain is still used to produce the vaccine. A meta-analysis confirmed a high seroprotection rate after a single dose which lasted five to ten years after vaccination [100]. However, some ocular complications related to YFV vaccination have been reported, particularly when the live YFV vaccine is administered alongside other vaccines such as Hepatitis A/B, Neisseria Meningitidis, or Typhoid [7]. These complications vary and encompass anterior and intermediate uveitis, unilateral optic neuropathy, multifocal choroiditis, evanescent white dot syndrome, arteriolar occlusion, and conditions resembling Vogt–Koyanagi–Harada disease [4,101,102]. Other YF vaccine candidates are currently in development and have not yet been tested beyond phase 1 clinical trials [103].
There is currently no proven specific antiviral drug available, with a strong emphasis on prevention through public health measures and vaccination [104,105]. Ongoing clinical trials are investigating novel therapeutic strategies, including phase I human immunoglobulin anti-YFV [106]. A Brazilian randomized clinical trial is assessing the efficacy of the antiviral sofosbuvir, a nucleotide analogue inhibitor, that exhibits activity in vitro and in animal models [107]. Ribavirin has shown potential activity in vitro but requires high concentrations that are not achievable in human serum [108]. In cases of severe systemic disease, intensive supportive therapy is indicated. Ocular complications associated with YFV and its vaccine are most often self-limiting, with a favorable course with supportive care.
3.4. Zika Virus
3.4.1. Epidemiology
Zika virus is primarily transmitted by Aedes mosquitoes [109], but it can also be transmitted vertically during pregnancy [22], through sexual contact [110], and via contaminated blood transfusions [111]. The first human case was reported in Uganda, Africa, in 1952 [112], and subsequent epidemics have occurred globally since 2007, including in Micronesia, French Polynesia, and South America [109]. In 2016, a significant outbreak occurred in Brazil, affecting 1.6 million people, with 1950 cases of infection-related microcephaly in newborns [113]. The infection can pose a substantial burden, especially in infants with congenital Zika syndrome (CZS) and adult patients with Guillain–Barre syndrome.
3.4.2. Systemic Manifestations
In adults, Zika infection is asymptomatic in 80% of cases [114]. After an incubation of 3–12 days, infected patients experience nonspecific flu-like symptoms [109]. Neurological complications may occur, including encephalitis, myelitis, and Guillain–Barre syndrome [115]. Generally, the median time between the onset of the infectious disease and neurologic features varies between 5 and 12 days [116]. Intrauterine infection and maternal–fetal transmission can occur during pregnancy in patients with a Zika infection. In newborns, CZS is defined by a pattern of anomalies including microcephaly, brain abnormalities, osteoskeletal abnormalities (mainly arthrogryposis and club foot), neurosensorial defects, and ocular manifestations (see below) [117].
3.4.3. Ocular Manifestations
In the acute phase, reported ophthalmological signs include non-purulent conjunctivitis (40%) and retroorbital pain (40%) [8,118,119]. Mild non-granulomatous anterior uveitis may be present in approximately half of patients presenting with red eyes [118]. Less-frequent manifestations have been described. Acute maculopathy has been reported in a 64-year-old man. OCT showed a disruption of the outer retinal layer in the central macula [120]. Otherwise, bilateral posterior uveitis with chorioretinal lesions was described in a 26-year-old man [121]. OCT showed hyperreflective nodules in the outer retina, and indocyanine green angiography confirmed active choroidal lesions.
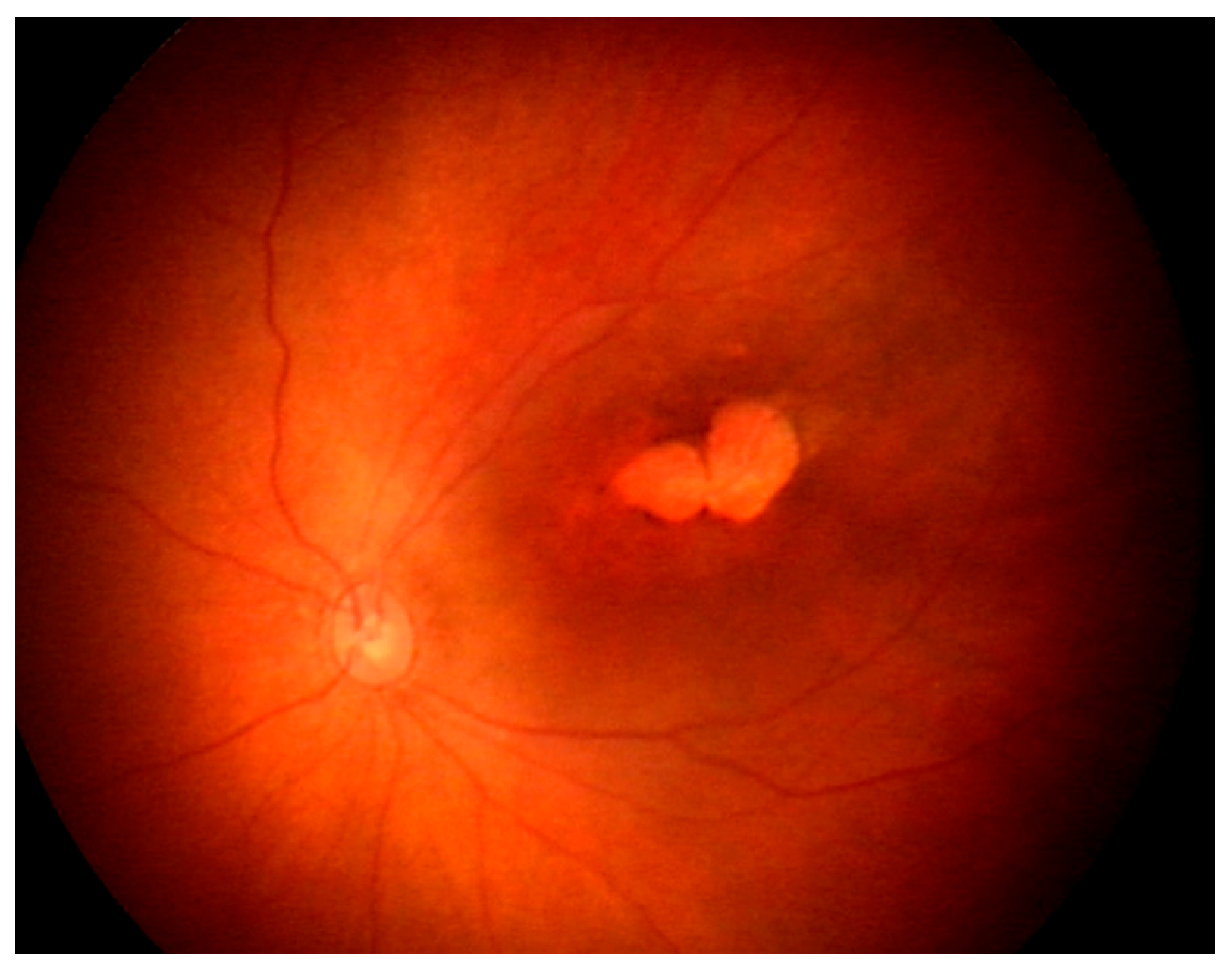
Ocular findings have been observed in 21.4–55% of CZS newborns [122]. Risk factors for ocular involvement in CZS include a smaller cephalic diameter at birth and infective symptoms during the first trimester of pregnancy [123]. However, ocular findings may occur in infants without microcephaly, suggesting that the absence of this feature does not preclude CZS screening. The most common ocular signs (85%) are macular and optic nerve abnormalities [124]. Posterior segment lesions include chorioretinal atrophy (Figure 5) and pigment mottling in the macular area [125,126]. Optical coherence tomography (OCT) of these lesions shows ellipsoid zone disruption (100%) and retinal and choroidal thinning (respectively, 89% and 78%) [127]. Retinal hemorrhages can also be observed on ocular fundus and are considered a screening criterion for CZS [128]. Anterior segment lesions include iris coloboma, corneal ectasia, lens subluxation, cataracts, and congenital glaucoma (12%) [129,130,131]. Neuroophthalmological lesions encompass strabismus, disc hypoplasia, increased cup-to-disc ratios, disc pallor, and horizontal nystagmus [125]. Histopathological studies on deceased fetuses have revealed pupillary membranes, immature anterior chamber angles, loss of pigment, retinal pigment epithelium thinning, choroidal thinning, and undifferentiated nuclear layers of the retina [132].
3.4.4. Diagnosis
A biological diagnosis can be obtained using various samples, including urine, amniotic fluid, serum, cerebrospinal fluid, semen, and tears, employing molecular biology techniques such as RT-PCR and serology methods like ELISAs [109,133]. Molecular diagnosis is typically carried out during the acute phase of the disease, approximately 3–5 days after incubation [133]. The rate of RNA detection in serum samples is low, ranging from 41% to 56% within 5 days of symptom onset [134,135,136], while in urine samples, it is higher, at around 95% [136]. Serial serum sampling between days 3 and 13 can detect an additional 25% of cases [134]. RNA detection in urine samples can remain positive for up to three weeks [137]. IgM antibodies can be detected in serum and cerebrospinal fluid samples within the first week of illness [138]. If IgM results are equivocal, confirmation can be obtained using a PRNT [133,138].
3.4.5. Treatment and Prognosis
No specific treatment is currently available. However, natural products isolated from medicinal herbs have demonstrated inhibition of ZIKV in vitro [139]. Only one in vivo animal model is available, reporting the anti-ZIKV activity of emetine [140].
Well-tolerated vaccine candidates have progressed through phase 1 or phase 2 development [141]. A completed phase 2/2B trial assessed a ZIKA DNA vaccine (VRC 5283) expressing prM-E structural genes. This vaccine was immunogenic in humans and generated cross-reactivity but did not produce cross-neutralizing antibodies against other flaviviruses, especially DENV [142]. Another ongoing phase 2 trial is evaluating a ZIKA mRNA vaccine (mRNA-1853) delivering modified prM-E mRNA [143]. However, the lack of current outbreaks hinders the advancement of clinical trials. Supportive care is recommended for adult patients experiencing inflammatory ocular manifestations. Corticosteroid eye drops can be employed to manage anterior uveitis [118].
The burden of Zika virus infection can be substantial, particularly in cases of congenital Zika syndrome (CZS). Ophthalmologists play a crucial role in early CZS assessment in newborns and the treatment of visual impairments and related ocular issues. Recommendations from the French High Council for Public Health [144] and the CDC [145] advise comprehensive ophthalmic screenings for all infants born from mothers infected during pregnancy, with the first examination before one month of age and a follow-up at one year. Public health campaigns should reinforce preventive measures, including the use of repellents to prevent mosquito bites and advising pregnant women in their first two trimesters to avoid traveling to disease-endemic areas [133].
3.5. Japanese Encephalitis Virus
3.5.1. Epidemiology
Japanese encephalitis (JE), caused by the JEV, is predominantly found in Asia and the Western Pacific, including Australia, where outbreaks have been reported recently [146]. Annually, an estimated 50,000 cases of JE are reported globally, resulting in approximately 15,000 deaths [147]. JE primarily occurs in rural areas and is transmitted through an enzootic cycle involving Culex mosquitoes and vertebrate hosts, including water birds and swine [148]. Vertical transmission has also been documented [21].
3.5.2. Systemic Manifestations
After an incubation period of 5 to 15 days [149], infected individuals develop flu-like symptoms with fever. Neurological complications, such as encephalitis, occur in only 1 out of 200–300 infected individuals [150]. During the encephalitic phase, various neurological symptoms may arise depending on the anatomical lesions. JEV infection can lead to a Parkinsonian syndrome or polio-like acute flaccid paralysis [151]. The case fatality rate is estimated to be as high as 30% among patients with neurological complications [152]. Survivors may experience a high burden of the disease, with 30–50% developing long-term sequelae [152].
3.5.3. Ocular Manifestations
Reports of ocular complications related to JEV are rare and likely underdiagnosed. One case occurred in a 53-year-old woman in 2006, who developed ischemic maculopathy during infection [153]. Fundus examination revealed a “white” macula and retinal hemorrhages, while FA showed non-perfusion areas of the macula. Another case was reported in 2020, involving a 45-year-old man who had visited Bali [154]. He experienced febrile confusion with dysphasia and bilateral conjunctival injection. Ophthalmological examination revealed moderate non-granulomatous anterior uveitis, and the ocular fundus showed bilateral vessel tortuosity and pale chorioretinal lesions, suggestive of chorioretinitis [154].
3.5.4. Diagnosis
Available diagnostic tests include serology (antibody capture ELISA) and RT-PCR, performed on serum and cerebrospinal fluid samples [27]. The gold standard for diagnosing JEV is IgM testing by ELISA in cerebrospinal fluid, with specific IgM detectable during the first week of illness [155]. Cross-reactions are common among flaviviruses, which is concerning in regions where both the dengue virus and JEV are present. The sensitivity of molecular diagnosis is low, at less than 25% in the acute phase [156,157]. Combining the two techniques can increase the sensitivity to 31% [158].
3.5.5. Treatment and Prognosis
JEV infection can lead to severe systemic disease, including neurological manifestations which can be managed with supportive care. Potential in vitro antiviral compounds include Baicalein, Curcumin, and Kaempferol [84]. Specific therapies are inadequate, with corticosteroids, ribavirin, minocycline, intravenous immunoglobulin, and interferon alpha-2a showing inefficacy [151]. However, vaccination has reduced the burden of JEV disease [159]. Currently available vaccines include cell-culture-derived live-attenuated; cell-culture-derived killed-inactivated; and cell-culture-derived live-attenuated chimeric vaccines [160]. The use of mouse-brain-derived killed-inactivated vaccines, which induced immune adverse events, has been discontinued [160]. Most vaccines are based on the SA14-14-2 strain, providing nearly complete protection with two doses for up to five years [151]. It is advisable, according to the CDC’s advisory committee on immunization practices, to recommend JEV vaccination for long-term travel to endemic regions, or for persons moving to an endemic country to live [149]. The JEV vaccine can also be considered in residents of rural areas in endemic locations. Indeed, implementation of vaccination programs reduced the incidence of JEV diseases in some countries [161]. The scarcity of reports on ocular manifestations hinders definitive conclusions about visual prognosis of JEV-related ocular issues. Nevertheless, cases of severe ischemic macular involvement indicate a potentially high burden of ocular complications [153].
3.6. Kyasanur Forest Disease Virus
3.6.1. Epidemiology
Kyasanur forest disease virus (KFDV) is a biosafety level 4 organism belonging to the tick-borne encephalitis serocomplex, causing a rare hemorrhagic fever disease currently limited to India [162]. First reported in 1957 in Kyasanur Forest, Karnataka, India [163], there have been about 500 annual cases in recent decades [164]. KFDV is transmitted to humans and animals through the bite of an infected hard tick (Hemaphysalis turturis/spinigera) or contact with an infected animal [165]. Variants of KFDV have been identified in patients with hemorrhagic fever in Saudi Arabia, referred to as Alkhurma hemorrhagic fever disease, sharing 97% homology with KFDV and suggesting a common ancestral origin [162].
3.6.2. Systemic Manifestations
KFD typically follows a biphasic course. After an incubation period of 2–7 days, patients experience an acute febrile phase characterized by flu-like symptoms and hemorrhagic manifestations, lasting up to two weeks [162]. In the convalescent phase, 10–20% of patients may experience severe hemorrhagic fever symptoms, including gastrointestinal bleeding and pneumonia, along with neurological complications resembling meningoencephalitis [162]. The estimated case fatality rate ranges from 3 to 10% [166].
3.6.3. Ocular Manifestations
Ocular manifestations are common in KFD, with rare historical studies reporting conjunctival congestion as the most frequent ocular sign (100%) [167]. Other ophthalmic features include hemorrhages in various ocular sites (conjunctiva (11%), vitreous humor (1%), retina (12%)), iritis (3%), keratitis (9%), and papilledema (1%) that may occur in encephalitic patients [167]. Lens opacification has been reported [168].
3.6.4. Diagnosis
Biological diagnosis can be performed from serum samples in the early stage (first two weeks) using RT-PCR [169]. Serology (antibody capture ELISA) can be used in the acute (IgM) and convalescent phases (IgG) [169]. Studies assessing the diagnostic performance of RT-PCR are limited. However, one study demonstrated a low detection rate of approximately 34.3% in serum samples [169].
3.6.5. Treatment and Prognosis
Specific therapies are deficient; notably, inefficacy was observed with interferon alpha-2a [170]. A vaccination strategy was developed in the 1990s using a formalin-inactivated tissue culture vaccine [171]. The vaccine’s efficacy is estimated at 83% after two doses. Annual administration of booster doses is recommended for five years after the last report of KFD cases in the area [172]. Currently, efforts are ongoing to optimize this vaccine by reducing the formalin concentration to mitigate side effects such as swelling and irritation, aiming to enhance vaccine acceptance [173]. Public health campaigns in affected areas promote the use of repellents to prevent tick bites [162]. Limited data are available on the visual outcomes of this rare disease, which mainly occurs in low-resource rural areas [162].
4. Conclusions
Flavivirus infections are on the rise due to various human activities, including climate change and deforestation, which promote vector-borne zoonotic diseases [174,175]. This emergence represents a potential public health issue, resulting in not only conditions that can be life-threatening but also those that can jeopardize vision. This was illustrated in recent Zika virus outbreaks that have resulted in substantial ocular morbidity [113]. In accordance with the information provided in this review, most cases of human flavivirus infections are linked to eye-related symptoms, which might be inaugural. Nevertheless, these symptoms can vary widely. On one hand, certain clinical features can be distinctive and indicative of the infection, such as the linear pattern of chorioretinitis seen in WNV cases. On the other hand, some viruses can cause non-specific symptoms, making diagnosis challenging. The screening for flavivirus infections should be tailored to the specific clinical context, taking into consideration epidemiological factors like current outbreaks and recent travel history. Additionally, a thorough ophthalmologic evaluation seems crucial if visual symptoms develop during the course of a flavivirus infection.
Author Contributions
Writing—original draft preparation, S.M.Z. and G.H.; Review and editing, A.R. and M.K.; Supervision, M.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ludwig, G.V.; Iacono-Connors, L.C. Insect-Transmitted Vertebrate Viruses: Flaviviridae. In Vitro Cell. Dev. Biol. Anim. 1993, 29, 296–309. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Garcia, M.-D.; Mazzon, M.; Jacobs, M.; Amara, A. Pathogenesis of Flavivirus Infections: Using and Abusing the Host Cell. Cell Host Microbe 2009, 5, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Pandit, P.S.; Doyle, M.M.; Smart, K.M.; Young, C.C.W.; Drape, G.W.; Johnson, C.K. Predicting Wildlife Reservoirs and Global Vulnerability to Zoonotic Flaviviruses. Nat. Commun. 2018, 9, 5425. [Google Scholar] [CrossRef] [PubMed]
- Merle, H.; Donnio, A.; Jean-Charles, A.; Guyomarch, J.; Hage, R.; Najioullah, F.; Césaire, R.; Cabié, A. Ocular Manifestations of Emerging Arboviruses: Dengue Fever, Chikungunya, Zika Virus, West Nile Virus, and Yellow Fever. J. Fr. Ophtalmol. 2018, 41, e235–e243. [Google Scholar] [CrossRef] [PubMed]
- Lucena-Neto, F.D.; Falcão, L.F.M.; Moraes, E.C.d.S.; David, J.P.F.; Vieira-Junior, A.d.S.; Silva, C.C.; de Sousa, J.R.; Duarte, M.I.S.; Vasconcelos, P.F.d.C.; Quaresma, J.A.S. Dengue Fever Ophthalmic Manifestations: A Review and Update. Rev. Med. Virol. 2023, 33, e2422. [Google Scholar] [CrossRef] [PubMed]
- Khairallah, M.; Mahendradas, P.; Curi, A.; Khochtali, S.; Cunningham, E.T. Emerging Viral Infections Causing Anterior Uveitis. Ocul. Immunol. Inflamm. 2019, 27, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, A.; Patel, R.; Goyal, S.; Rajaratnam, T.; Sharma, A.; Hossain, P. Ocular Manifestations of Emerging Viral Diseases. Eye 2021, 35, 1117–1139. [Google Scholar] [CrossRef] [PubMed]
- Benzekri, R.; Belfort, R.; Ventura, C.V.; de Paula Freitas, B.; Maia, M.; Leite, M.; Labetoulle, M.; Rousseau, A. Ocular manifestations of Zika virus: What we do and do not know. J. Fr. Ophtalmol. 2017, 40, 138–145. [Google Scholar] [CrossRef]
- Marianneau, P.; Steffan, A.M.; Royer, C.; Drouet, M.T.; Jaeck, D.; Kirn, A.; Deubel, V. Infection of Primary Cultures of Human Kupffer Cells by Dengue Virus: No Viral Progeny Synthesis, but Cytokine Production Is Evident. J. Virol. 1999, 73, 5201–5206. [Google Scholar] [CrossRef]
- Tassaneetrithep, B.; Burgess, T.H.; Granelli-Piperno, A.; Trumpfheller, C.; Finke, J.; Sun, W.; Eller, M.A.; Pattanapanyasat, K.; Sarasombath, S.; Birx, D.L.; et al. DC-SIGN (CD209) Mediates Dengue Virus Infection of Human Dendritic Cells. J. Exp. Med. 2003, 197, 823–829. [Google Scholar] [CrossRef]
- Krishnan, M.N.; Sukumaran, B.; Pal, U.; Agaisse, H.; Murray, J.L.; Hodge, T.W.; Fikrig, E. Rab 5 Is Required for the Cellular Entry of Dengue and West Nile Viruses. J. Virol. 2007, 81, 4881–4885. [Google Scholar] [CrossRef] [PubMed]
- Hulo, C.; de Castro, E.; Masson, P.; Bougueleret, L.; Bairoch, A.; Xenarios, I.; Le Mercier, P. ViralZone: A Knowledge Resource to Understand Virus Diversity. Nucleic Acids Res. 2011, 39, D576–D582. [Google Scholar] [CrossRef] [PubMed]
- Alpert, S.G.; Fergerson, J.; Noël, L.P. Intrauterine West Nile Virus: Ocular and Systemic Findings. Am. J. Ophthalmol. 2003, 136, 733–735. [Google Scholar] [CrossRef]
- Iwamoto, M.; Jernigan, D.B.; Guasch, A.; Trepka, M.J.; Blackmore, C.G.; Hellinger, W.C.; Pham, S.M.; Zaki, S.; Lanciotti, R.S.; Lance-Parker, S.E.; et al. Transmission of West Nile Virus from an Organ Donor to Four Transplant Recipients. N. Engl. J. Med. 2003, 348, 2196–2203. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Intrauterine West Nile Virus Infection—New York, 2002. MMWR Morb. Mortal. Wkly. Rep. 2002, 51, 1135–1136. [Google Scholar]
- Sbrana, E.; Tonry, J.H.; Xiao, S.-Y.; da Rosa, A.P.A.T.; Higgs, S.; Tesh, R.B. Oral Transmission of West Nile Virus in a Hamster Model. Am. J. Trop. Med. Hyg. 2005, 72, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Komar, N.; Langevin, S.; Hinten, S.; Nemeth, N.; Edwards, E.; Hettler, D.; Davis, B.; Bowen, R.; Bunning, M. Experimental Infection of North American Birds with the New York 1999 Strain of West Nile Virus. Emerg. Infect. Dis. 2003, 9, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Odelola, H.A.; Oduye, O.O. West Nile Virus Infection of Adult Mice by Oral Route. Arch. Virol. 1977, 54, 251–253. [Google Scholar] [CrossRef]
- Sabino, E.C.; Loureiro, P.; Lopes, M.E.; Capuani, L.; McClure, C.; Chowdhury, D.; Di-Lorenzo-Oliveira, C.; Oliveira, L.C.; Linnen, J.M.; Lee, T.-H.; et al. Transfusion-Transmitted Dengue and Associated Clinical Symptoms during the 2012 Epidemic in Brazil. J. Infect. Dis. 2016, 213, 694–702. [Google Scholar] [CrossRef]
- Slavov, S.N.; Cilião-Alves, D.C.; Gonzaga, F.A.C.; Moura, D.R.; de Moura, A.C.A.M.; de Noronha, L.A.G.; Cassemiro, É.M.; Pimentel, B.M.S.; Costa, F.J.Q.; da Silva, G.A.; et al. Dengue Seroprevalence among Asymptomatic Blood Donors during an Epidemic Outbreak in Central-West Brazil. PLoS ONE 2019, 14, e0213793. [Google Scholar] [CrossRef]
- Chaturvedi, U.C.; Mathur, A.; Chandra, A.; Das, S.K.; Tandon, H.O.; Singh, U.K. Transplacental Infection with Japanese Encephalitis Virus. J. Infect. Dis. 1980, 141, 712–715. [Google Scholar] [CrossRef] [PubMed]
- Oliveira Melo, A.S.; Malinger, G.; Ximenes, R.; Szejnfeld, P.O.; Alves Sampaio, S.; Bispo de Filippis, A.M. Zika Virus Intrauterine Infection Causes Fetal Brain Abnormality and Microcephaly: Tip of the Iceberg? Ultrasound Obstet. Gynecol. 2016, 47, 6–7. [Google Scholar] [CrossRef] [PubMed]
- Guérin, B.; Pozzi, N. Viruses in Boar Semen: Detection and Clinical as Well as Epidemiological Consequences Regarding Disease Transmission by Artificial Insemination. Theriogenology 2005, 63, 556–572. [Google Scholar] [CrossRef] [PubMed]
- Paz-Bailey, G.; Rosenberg, E.S.; Doyle, K.; Munoz-Jordan, J.; Santiago, G.A.; Klein, L.; Perez-Padilla, J.; Medina, F.A.; Waterman, S.H.; Gubern, C.G.; et al. Persistence of Zika Virus in Body Fluids—Final Report. N. Engl. J. Med. 2018, 379, 1234–1243. [Google Scholar] [CrossRef] [PubMed]
- Kuno, G. Serodiagnosis of Flaviviral Infections and Vaccinations in Humans. Adv. Virus Res. 2003, 61, 3–65. [Google Scholar] [CrossRef] [PubMed]
- Alhajj, M.; Zubair, M.; Farhana, A. Enzyme Linked Immunosorbent Assay. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Roberts, A.; Gandhi, S. Japanese Encephalitis Virus: A Review on Emerging Diagnostic Techniques. Front. Biosci. 2020, 25, 1875–1893. [Google Scholar] [CrossRef]
- Guzman, M.G.; Gubler, D.J.; Izquierdo, A.; Martinez, E.; Halstead, S.B. Dengue Infection. Nat. Rev. Dis. Primers 2016, 2, 16055. [Google Scholar] [CrossRef] [PubMed]
- Halstead, S.B. Dengue. Curr. Opin. Infect. Dis. 2002, 15, 471–476. [Google Scholar] [CrossRef]
- Murray, N.E.A.; Quam, M.B.; Wilder-Smith, A. Epidemiology of Dengue: Past, Present and Future Prospects. Clin. Epidemiol. 2013, 5, 299–309. [Google Scholar] [CrossRef]
- WHO. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control: New Edition; WHO Guidelines Approved by the Guidelines Review Committee; World Health Organization: Geneva, Switzerland, 2009; ISBN 978-92-4-154787-1. [Google Scholar]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The Global Distribution and Burden of Dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef]
- World Health Organization. Global Strategy for Dengue Prevention and Control 2012–2020; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Gubler, D.J. Dengue, Urbanization and Globalization: The Unholy Trinity of the 21(St) Century. Trop. Med. Health 2011, 39, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, H.K.; Bhai, S.; John, M.; Xavier, J. Ocular Manifestations of Dengue Fever in an East Indian Epidemic. Can. J. Ophthalmol. 2006, 41, 741–746. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Srinivasan, R.; Setia, S.; Soundravally, R.; Pandian, D.G. Uveitis Following Dengue Fever. Eye 2009, 23, 873–876. [Google Scholar] [CrossRef] [PubMed]
- Loh, B.-K.; Bacsal, K.; Chee, S.-P.; Cheng, B.C.-L.; Wong, D. Foveolitis Associated with Dengue Fever: A Case Series. Ophthalmologica 2008, 222, 317–320. [Google Scholar] [CrossRef]
- Su, D.H.-W.; Bacsal, K.; Chee, S.-P.; Flores, J.V.P.; Lim, W.-K.; Cheng, B.C.-L.; Jap, A.H.-E.; Dengue Maculopathy Study Group. Prevalence of Dengue Maculopathy in Patients Hospitalized for Dengue Fever. Ophthalmology 2007, 114, 1743–1747. [Google Scholar] [CrossRef]
- Chee, E.; Sims, J.L.; Jap, A.; Tan, B.H.; Oh, H.; Chee, S.-P. Comparison of Prevalence of Dengue Maculopathy during Two Epidemics with Differing Predominant Serotypes. Am. J. Ophthalmol. 2009, 148, 910–913. [Google Scholar] [CrossRef]
- Teoh, S.C.; Chee, C.K.; Laude, A.; Goh, K.Y.; Barkham, T.; Ang, B.S.; Eye Institute Dengue-related Ophthalmic Complications Workgroup. Optical Coherence Tomography Patterns as Predictors of Visual Outcome in Dengue-Related Maculopathy. Retina 2010, 30, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Bacsal, K.E.; Chee, S.-P.; Cheng, C.-L.; Flores, J.V.P. Dengue-Associated Maculopathy. Arch. Ophthalmol. 2007, 125, 501–510. [Google Scholar] [CrossRef]
- Yip, V.C.-H.; Sanjay, S.; Koh, Y.T. Ophthalmic Complications of Dengue Fever: A Systematic Review. Ophthalmol. Ther. 2012, 1, 2. [Google Scholar] [CrossRef]
- Agarwal, A.; Aggarwal, K.; Dogra, M.; Kumar, A.; Akella, M.; Katoch, D.; Bansal, R.; Singh, R.; Gupta, V.; OCTA Study Group. Dengue-Induced Inflammatory, Ischemic Foveolitis and Outer Maculopathy: A Swept-Source Imaging Evaluation. Ophthalmol. Retina 2019, 3, 170–177. [Google Scholar] [CrossRef]
- Khairallah, M.; Yahia, S.B.; Attia, S. Arthropod Vector-Borne Uveitis in the Developing World. Int. Ophthalmol. Clin. 2010, 50, 125–144. [Google Scholar] [CrossRef] [PubMed]
- Tabbara, K. Dengue Retinochoroiditis. Ann. Saudi Med. 2012, 32, 530–533. [Google Scholar] [CrossRef] [PubMed]
- Somkijrungroj, T.; Kongwattananon, W. Ocular Manifestations of Dengue. Curr. Opin. Ophthalmol. 2019, 30, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Dhoot, S.K. Bilateral Ciliochoroidal Effusion with Secondary Angle Closure and Myopic Shift in Dengue Fever. Ocul. Immunol. Inflamm. 2023, 31, 847–850. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.W.; Teoh, S.C. Dengue Eye Disease. Surv. Ophthalmol. 2015, 60, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Saranappa, S.B.S.; Sowbhagya, H.N. Panophthalmitis in Dengue Fever. Indian Pediatr. 2012, 49, 760. [Google Scholar] [CrossRef] [PubMed]
- Arya, D.; Das, S.; Shah, G.; Gandhi, A. Panophthalmitis Associated with Scleral Necrosis in Dengue Hemorrhagic Fever. Indian J. Ophthalmol. 2019, 67, 1775–1777. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.F.; Ooi, E.E. Diagnosis of Dengue: An Update. Expert Rev. Anti-Infect. Ther. 2012, 10, 895–907. [Google Scholar] [CrossRef]
- Teoh, B.-T.; Sam, S.-S.; Tan, K.-K.; Johari, J.; Abd-Jamil, J.; Hooi, P.-S.; AbuBakar, S. The Use of NS1 Rapid Diagnostic Test and qRT-PCR to Complement IgM ELISA for Improved Dengue Diagnosis from Single Specimen. Sci. Rep. 2016, 6, 27663. [Google Scholar] [CrossRef]
- Hirayama, T.; Mizuno, Y.; Takeshita, N.; Kotaki, A.; Tajima, S.; Omatsu, T.; Sano, K.; Kurane, I.; Takasaki, T. Detection of Dengue Virus Genome in Urine by Real-Time Reverse Transcriptase PCR: A Laboratory Diagnostic Method Useful after Disappearance of the Genome in Serum. J. Clin. Microbiol. 2012, 50, 2047–2052. [Google Scholar] [CrossRef]
- Kularatne, S.A.; Dalugama, C. Dengue Infection: Global Importance, Immunopathology and Management. Clin. Med. 2022, 22, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.-K.; Mathur, R.; Koh, A.; Yeoh, R.; Chee, S.-P. Ocular Manifestations of Dengue Fever. Ophthalmology 2004, 111, 2057–2064. [Google Scholar] [CrossRef] [PubMed]
- Saleh, M.S.M.; Kamisah, Y. Potential Medicinal Plants for the Treatment of Dengue Fever and Severe Acute Respiratory Syndrome-Coronavirus. Biomolecules 2020, 11, 42. [Google Scholar] [CrossRef] [PubMed]
- Rajapakse, S.; De Silva, N.L.; Weeratunga, P.; Rodrigo, C.; Sigera, C.; Fernando, S.D. Carica Papaya Extract in Dengue: A Systematic Review and Meta-Analysis. BMC Complement. Altern. Med. 2019, 19, 265. [Google Scholar] [CrossRef] [PubMed]
- Hadinegoro, S.R.; Arredondo-García, J.L.; Capeding, M.R.; Deseda, C.; Chotpitayasunondh, T.; Dietze, R.; Muhammad Ismail, H.I.H.; Reynales, H.; Limkittikul, K.; Rivera-Medina, D.M.; et al. Efficacy and Long-Term Safety of a Dengue Vaccine in Regions of Endemic Disease. N. Engl. J. Med. 2015, 373, 1195–1206. [Google Scholar] [CrossRef] [PubMed]
- Scherwitzl, I.; Mongkolsapaja, J.; Screaton, G. Recent Advances in Human Flavivirus Vaccines. Curr. Opin. Virol. 2017, 23, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Biswal, S.; Reynales, H.; Saez-Llorens, X.; Lopez, P.; Borja-Tabora, C.; Kosalaraksa, P.; Sirivichayakul, C.; Watanaveeradej, V.; Rivera, L.; Espinoza, F.; et al. Efficacy of a Tetravalent Dengue Vaccine in Healthy Children and Adolescents. N. Engl. J. Med. 2019, 381, 2009–2019. [Google Scholar] [CrossRef]
- Biswal, S.; Borja-Tabora, C.; Martinez Vargas, L.; Velásquez, H.; Theresa Alera, M.; Sierra, V.; Johana Rodriguez-Arenales, E.; Yu, D.; Wickramasinghe, V.P.; Duarte Moreira, E.; et al. Efficacy of a Tetravalent Dengue Vaccine in Healthy Children Aged 4-16 Years: A Randomised, Placebo-Controlled, Phase 3 Trial. Lancet 2020, 395, 1423–1433. [Google Scholar] [CrossRef]
- Petersen, L.R.; Brault, A.C.; Nasci, R.S. West Nile Virus: Review of the Literature. JAMA 2013, 310, 308–315. [Google Scholar] [CrossRef]
- Garg, S.; Jampol, L.M. Systemic and Intraocular Manifestations of West Nile Virus Infection. Surv. Ophthalmol. 2005, 50, 3–13. [Google Scholar] [CrossRef]
- Troupin, A.; Colpitts, T.M. Overview of West Nile Virus Transmission and Epidemiology. Methods Mol. Biol. 2016, 1435, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Zannoli, S.; Sambri, V. West Nile Virus and Usutu Virus Co-Circulation in Europe: Epidemiology and Implications. Microorganisms 2019, 7, 184. [Google Scholar] [CrossRef] [PubMed]
- Gyure, K.A. West Nile Virus Infections. J. Neuropathol. Exp. Neurol. 2009, 68, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Khairallah, M.; Ben Yahia, S.; Ladjimi, A.; Zeghidi, H.; Ben Romdhane, F.; Besbes, L.; Zaouali, S.; Messaoud, R. Chorioretinal Involvement in Patients with West Nile Virus Infection. Ophthalmology 2004, 111, 2065–2070. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.K.; Limstrom, S.A.; Tarasewicz, D.G.; Lin, S.G. Ocular Features of West Nile Virus Infection in North America: A Study of 14 Eyes. Ophthalmology 2006, 113, 1539–1546. [Google Scholar] [CrossRef] [PubMed]
- Winward, B.K.; Gottlieb, J.L.; Chang, J.S.; Bradbury, L.; Maganti, N.; Pathak, C.; Fowler, B.J. Ocular Findings Aid in Diagnosis of West Nile Virus. WMJ 2023, 122, 208–212. [Google Scholar] [PubMed]
- Abroug, F.; Ouanes-Besbes, L.; Letaief, M.; Ben Romdhane, F.; Khairallah, M.; Triki, H.; Bouzouiaia, N. A Cluster Study of Predictors of Severe West Nile Virus Infection. Mayo Clin. Proc. 2006, 81, 12–16. [Google Scholar] [CrossRef]
- Sivakumar, R.R.; Prajna, L.; Arya, L.K.; Muraly, P.; Shukla, J.; Saxena, D.; Parida, M. Molecular Diagnosis and Ocular Imaging of West Nile Virus Retinitis and Neuroretinitis. Ophthalmology 2013, 120, 1820–1826. [Google Scholar] [CrossRef]
- Dahal, U.; Mobarakai, N.; Sharma, D.; Pathak, B. West Nile Virus Infection and Diplopia: A Case Report and Review of Literature. Int. J. Gen. Med. 2013, 6, 369–373. [Google Scholar] [CrossRef]
- Khairallah, M.; Ben Yahia, S.; Attia, S.; Zaouali, S.; Ladjimi, A.; Messaoud, R. Linear Pattern of West Nile Virus-Associated Chorioretinitis Is Related to Retinal Nerve Fibres Organization. Eye 2007, 21, 952–955. [Google Scholar] [CrossRef]
- Learned, D.; Nudleman, E.; Robinson, J.; Chang, E.; Stec, L.; Faia, L.J.; Wolfe, J.; Williams, G.A. Multimodal Imaging of West Nile Virus Chorioretinitis. Retina 2014, 34, 2269–2274. [Google Scholar] [CrossRef] [PubMed]
- Khairallah, M.; Ben Yahia, S.; Attia, S.; Zaouali, S.; Jelliti, B.; Jenzri, S.; Ladjimi, A.; Messaoud, R. Indocyanine Green Angiographic Features in Multifocal Chorioretinitis Associated with West Nile Virus Infection. Retina 2006, 26, 358–359. [Google Scholar] [CrossRef] [PubMed]
- Khairallah, M.; Jelliti, B.; Jenzeri, S. Emergent Infectious Uveitis. Middle East Afr. J. Ophthalmol. 2009, 16, 225–238. [Google Scholar] [CrossRef] [PubMed]
- Khairallah, M.; Kahloun, R. Ocular Manifestations of Emerging Infectious Diseases. Curr. Opin. Ophthalmol. 2013, 24, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Khairallah, M.; Kahloun, R.; Gargouri, S.; Jelliti, B.; Sellami, D.; Ben Yahia, S.; Feki, J. Swept-Source Optical Coherence Tomography Angiography in West Nile Virus Chorioretinitis and Associated Occlusive Retinal Vasculitis. Ophthalmic. Surg. Lasers Imaging Retin. 2017, 48, 672–675. [Google Scholar] [CrossRef] [PubMed]
- Shukla, J.; Saxena, D.; Rathinam, S.; Lalitha, P.; Joseph, C.R.; Sharma, S.; Soni, M.; Rao, P.V.L.; Parida, M. Molecular Detection and Characterization of West Nile Virus Associated with Multifocal Retinitis in Patients from Southern India. Int. J. Infect. Dis. 2012, 16, e53–e59. [Google Scholar] [CrossRef] [PubMed]
- Lustig, Y.; Mannasse, B.; Koren, R.; Katz-Likvornik, S.; Hindiyeh, M.; Mandelboim, M.; Dovrat, S.; Sofer, D.; Mendelson, E. Superiority of West Nile Virus RNA Detection in Whole Blood for Diagnosis of Acute Infection. J. Clin. Microbiol. 2016, 54, 2294–2297. [Google Scholar] [CrossRef] [PubMed]
- Lazear, H.M.; Pinto, A.K.; Vogt, M.R.; Gale, M.; Diamond, M.S. Beta Interferon Controls West Nile Virus Infection and Pathogenesis in Mice. J. Virol. 2011, 85, 7186–7194. [Google Scholar] [CrossRef]
- Ben-Nathan, D.; Gershoni-Yahalom, O.; Samina, I.; Khinich, Y.; Nur, I.; Laub, O.; Gottreich, A.; Simanov, M.; Porgador, A.; Rager-Zisman, B.; et al. Using High Titer West Nile Intravenous Immunoglobulin from Selected Israeli Donors for Treatment of West Nile Virus Infection. BMC Infect. Dis. 2009, 9, 18. [Google Scholar] [CrossRef]
- Gorman, M.J.; Poddar, S.; Farzan, M.; Diamond, M.S. The Interferon-Stimulated Gene Ifitm3 Restricts West Nile Virus Infection and Pathogenesis. J. Virol. 2016, 90, 8212–8225. [Google Scholar] [CrossRef]
- Goh, V.S.L.; Mok, C.-K.; Chu, J.J.H. Antiviral Natural Products for Arbovirus Infections. Molecules 2020, 25, 2796. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, A.; Haigh, O.; Ksiaa, I.; Khairallah, M.; Labetoulle, M. Ocular Manifestations of West Nile Virus. Vaccines 2020, 8, 641. [Google Scholar] [CrossRef] [PubMed]
- Gould, C.V.; Staples, J.E.; Huang, C.Y.-H.; Brault, A.C.; Nett, R.J. Combating West Nile Virus Disease—Time to Revisit Vaccination. N. Engl. J. Med. 2023, 388, 1633–1636. [Google Scholar] [CrossRef] [PubMed]
- Curren, E.J.; Shankar, M.B.; Fischer, M.; Meltzer, M.I.; Erin Staples, J.; Gould, C.V. Cost-Effectiveness and Impact of a Targeted Age- and Incidence-Based West Nile Virus Vaccine Strategy. Clin. Infect. Dis. 2021, 73, 1565–1570. [Google Scholar] [CrossRef] [PubMed]
- Seth, R.K.; Stoessel, K.M.; Adelman, R.A. Choroidal Neovascularization Associated with West Nile Virus Chorioretinitis. Semin. Ophthalmol. 2007, 22, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Afshar, A.R.; Hariprasad, S.M.; Jampol, L.M.; Sheth, V.S. Use of Intravitreous Bevacizumab to Treat Macular Edema in West Nile Virus Chorioretinitis. Arch. Ophthalmol. 2012, 130, 396–398. [Google Scholar] [CrossRef] [PubMed]
- Sanz, G.; De Jesus Rodriguez, E.; Vila-Delgado, M.; Oliver, A.L. An Unusual Case of Unilateral Chorioretinitis and Blind Spot Enlargement Associated with Asymptomatic West Nile Virus Infection. Am. J. Ophthalmol. Case Rep. 2020, 18, 100723. [Google Scholar] [CrossRef]
- Khairallah, M.; Yahia, S.B.; Letaief, M.; Attia, S.; Kahloun, R.; Jelliti, B.; Zaouali, S.; Messaoud, R. A Prospective Evaluation of Factors Associated with Chorioretinitis in Patients with West Nile Virus Infection. Ocul. Immunol. Inflamm. 2007, 15, 435–439. [Google Scholar] [CrossRef]
- Khairallah, M.; Ben Yahia, S.; Attia, S.; Jelliti, B.; Zaouali, S.; Ladjimi, A. Severe Ischemic Maculopathy in a Patient with West Nile Virus Infection. Ophthalmic. Surg. Lasers Imaging 2006, 37, 240–242. [Google Scholar] [CrossRef]
- Monath, T.P. Yellow Fever: An Update. Lancet Infect. Dis. 2001, 1, 11–20. [Google Scholar] [CrossRef]
- Lucey, D.; Gostin, L.O. A Yellow Fever Epidemic: A New Global Health Emergency? JAMA 2016, 315, 2661–2662. [Google Scholar] [CrossRef] [PubMed]
- Douam, F.; Ploss, A. Yellow Fever Virus: Knowledge Gaps Impeding the Fight Against an Old Foe. Trends Microbiol. 2018, 26, 913–928. [Google Scholar] [CrossRef] [PubMed]
- Brandão-de-Resende, C.; Cunha, L.H.M.; Oliveira, S.L.; Pereira, L.S.; Oliveira, J.G.F.; Santos, T.A.; Vasconcelos-Santos, D.V. Characterization of Retinopathy Among Patients With Yellow Fever During 2 Outbreaks in Southeastern Brazil. JAMA Ophthalmol. 2019, 137, 996–1002. [Google Scholar] [CrossRef] [PubMed]
- Vianello, S.; Silva de Souza, G.; Maia, M.; Belfort, R.; de Oliveira Dias, J.R. Ocular Findings in Yellow Fever Infection. JAMA Ophthalmol. 2019, 137, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, A.L.N.; Barros, R.S.; Silva, S.P.; Rodrigues, D.S.G.; Cruz, A.C.R.; Dos Santos, F.B.; Vasconcelos, P.F.C.; Tesh, R.B.; Nunes, B.T.D.; Medeiros, D.B.A. The Usefulness of a Duplex RT-qPCR during the Recent Yellow Fever Brazilian Epidemic: Surveillance of Vaccine Adverse Events, Epizootics and Vectors. Pathogens 2021, 10, 693. [Google Scholar] [CrossRef] [PubMed]
- De Rezende, I.M.; Oliveira, G.F.G.; Costa, T.A.; Khan, A.; Pereira, L.S.; Santos, T.A.; Alves, P.A.; Calzavara-Silva, C.E.; Martins-Filho, O.A.; Teixeira-Carvalho, A.; et al. Yellow Fever Molecular Diagnosis Using Urine Specimens during Acute and Convalescent Phases of the Disease. J. Clin. Microbiol. 2022, 60, e00254-22. [Google Scholar] [CrossRef] [PubMed]
- Kling, K.; Domingo, C.; Bogdan, C.; Duffy, S.; Harder, T.; Howick, J.; Kleijnen, J.; McDermott, K.; Wichmann, O.; Wilder-Smith, A.; et al. Duration of Protection After Vaccination Against Yellow Fever: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2022, 75, 2266–2274. [Google Scholar] [CrossRef] [PubMed]
- Biancardi, A.L.; Moraes, H.V. de Anterior and Intermediate Uveitis Following Yellow Fever Vaccination with Fractional Dose: Case Reports. Ocul. Immunol. Inflamm. 2019, 27, 521–523. [Google Scholar] [CrossRef]
- Campos, W.R.; Cenachi, S.P.F.; Soares, M.S.; Gonçalves, P.F.; Vasconcelos-Santos, D.V. Vogt-Koyanagi-Harada-like Disease Following Yellow Fever Vaccination. Ocul. Immunol. Inflamm. 2021, 29, 124–127. [Google Scholar] [CrossRef]
- Hansen, C.A.; Barrett, A.D.T. The Present and Future of Yellow Fever Vaccines. Pharmaceuticals 2021, 14, 891. [Google Scholar] [CrossRef]
- Vannice, K.; Wilder-Smith, A.; Hombach, J. Fractional-Dose Yellow Fever Vaccination—Advancing the Evidence Base. N. Engl. J. Med. 2018, 379, 603–605. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Child Health and Human Development. Yellow Fever Vaccine. In Drugs and Lactation Database (LactMed®); National Institute of Child Health and Human Development: Bethesda, MD, USA, 2006. [Google Scholar]
- Low, J.G.; Ng, J.H.J.; Ong, E.Z.; Kalimuddin, S.; Wijaya, L.; Chan, Y.F.Z.; Ng, D.H.L.; Tan, H.-C.; Baglody, A.; Chionh, Y.-H.; et al. Phase 1 Trial of a Therapeutic Anti-Yellow Fever Virus Human Antibody. N. Engl. J. Med. 2020, 383, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo-Mello, C.; Casadio, L.V.B.; Avelino-Silva, V.I.; Yeh-Li, H.; Sztajnbok, J.; Joelsons, D.; Antonio, M.B.; Pinho, J.R.R.; Malta, F.d.M.; Gomes-Gouvêa, M.S.; et al. Efficacy of Sofosbuvir as Treatment for Yellow Fever: Protocol for a Randomised Controlled Trial in Brazil (SOFFA Study). BMJ Open 2019, 9, e027207. [Google Scholar] [CrossRef] [PubMed]
- Sbrana, E.; Xiao, S.-Y.; Guzman, H.; Ye, M.; Travassos da Rosa, A.P.A.; Tesh, R.B. Efficacy of Post-Exposure Treatment of Yellow Fever with Ribavirin in a Hamster Model of the Disease. Am. J. Trop. Med. Hyg. 2004, 71, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Plourde, A.R.; Bloch, E.M. A Literature Review of Zika Virus. Emerg. Infect. Dis. 2016, 22, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Musso, D.; Roche, C.; Robin, E.; Nhan, T.; Teissier, A.; Cao-Lormeau, V.-M. Potential Sexual Transmission of Zika Virus. Emerg. Infect. Dis. 2015, 21, 359–361. [Google Scholar] [CrossRef] [PubMed]
- Musso, D.; Nhan, T.; Robin, E.; Roche, C.; Bierlaire, D.; Zisou, K.; Shan Yan, A.; Cao-Lormeau, V.M.; Broult, J. Potential for Zika Virus Transmission through Blood Transfusion Demonstrated during an Outbreak in French Polynesia, November 2013 to February 2014. Euro Surveill. 2014, 19, 20761. [Google Scholar] [CrossRef] [PubMed]
- Dick, G.W.A.; Kitchen, S.F.; Haddow, A.J. Zika Virus. I. Isolations and Serological Specificity. Trans. R. Soc. Trop. Med. Hyg. 1952, 46, 509–520. [Google Scholar] [CrossRef]
- de Oliveira, W.K.; de França, G.V.A.; Carmo, E.H.; Duncan, B.B.; de Souza Kuchenbecker, R.; Schmidt, M.I. Infection-Related Microcephaly after the 2015 and 2016 Zika Virus Outbreaks in Brazil: A Surveillance-Based Analysis. Lancet 2017, 390, 861–870. [Google Scholar] [CrossRef]
- Duffy, M.R.; Chen, T.-H.; Hancock, W.T.; Powers, A.M.; Kool, J.L.; Lanciotti, R.S.; Pretrick, M.; Marfel, M.; Holzbauer, S.; Dubray, C.; et al. Zika Virus Outbreak on Yap Island, Federated States of Micronesia. N. Engl. J. Med. 2009, 360, 2536–2543. [Google Scholar] [CrossRef]
- Muñoz, L.S.; Barreras, P.; Pardo, C.A. Zika Virus-Associated Neurological Disease in the Adult: Guillain-Barré Syndrome, Encephalitis, and Myelitis. Semin. Reprod. Med. 2016, 34, 273–279. [Google Scholar] [CrossRef]
- Leonhard, S.E.; Bresani-Salvi, C.C.; Lyra Batista, J.D.; Cunha, S.; Jacobs, B.C.; Brito Ferreira, M.L.; P Militão de Albuquerque, M.d.F. Guillain-Barré Syndrome Related to Zika Virus Infection: A Systematic Review and Meta-Analysis of the Clinical and Electrophysiological Phenotype. PLoS Negl. Trop. Di.s 2020, 14, e0008264. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.A.; Staples, J.E.; Dobyns, W.B.; Pessoa, A.; Ventura, C.V.; da Fonseca, E.B.; Ribeiro, E.M.; Ventura, L.O.; Neto, N.N.; Arena, J.F.; et al. Characterizing the Pattern of Anomalies in Congenital Zika Syndrome for Pediatric Clinicians. JAMA Pediatr. 2017, 171, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Troumani, Y.; Touhami, S.; Jackson, T.L.; Ventura, C.V.; Stanescu-Segall, D.M.; Errera, M.-H.; Rousset, D.; Bodaghi, B.; Cartry, G.; David, T.; et al. Association of Anterior Uveitis With Acute Zika Virus Infection in Adults. JAMA Ophthalmol. 2021, 139, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Cerbino-Neto, J.; Mesquita, E.C.; Souza, T.M.L.; Parreira, V.; Wittlin, B.B.; Durovni, B.; Lemos, M.C.F.; Vizzoni, A.; Bispo de Filippis, A.M.; Sampaio, S.A.; et al. Clinical Manifestations of Zika Virus Infection, Rio de Janeiro, Brazil, 2015. Emerg. Infect. Dis. 2016, 22, 1318–1320. [Google Scholar] [CrossRef] [PubMed]
- Parke, D.W.; Almeida, D.R.P.; Albini, T.A.; Ventura, C.V.; Berrocal, A.M.; Mittra, R.A. Serologically Confirmed Zika-Related Unilateral Acute Maculopathy in an Adult. Ophthalmology 2016, 123, 2432–2433. [Google Scholar] [CrossRef] [PubMed]
- Kodati, S.; Palmore, T.N.; Spellman, F.A.; Cunningham, D.; Weistrop, B.; Sen, H.N. Bilateral Posterior Uveitis Associated with Zika Virus Infection. Lancet 2017, 389, 125–126. [Google Scholar] [CrossRef] [PubMed]
- Ventura, C.V.; Ventura, L.O. Ophthalmologic Manifestations Associated with Zika Virus Infection. Pediatrics 2018, 141, S161–S166. [Google Scholar] [CrossRef] [PubMed]
- Ventura, C.V.; Maia, M.; Travassos, S.B.; Martins, T.T.; Patriota, F.; Nunes, M.E.; Agra, C.; Torres, V.L.; van der Linden, V.; Ramos, R.C.; et al. Risk Factors Associated with the Ophthalmoscopic Findings Identified in Infants with Presumed Zika Virus Congenital Infection. JAMA Ophthalmol. 2016, 134, 912–918. [Google Scholar] [CrossRef]
- Labib, B.A.; Chigbu, D.I. Pathogenesis and Manifestations of Zika Virus-Associated Ocular Diseases. Trop. Med. Infect. Dis. 2022, 7, 106. [Google Scholar] [CrossRef]
- Ventura, C.V.; Maia, M.; Bravo-Filho, V.; Góis, A.L.; Belfort, R. Zika Virus in Brazil and Macular Atrophy in a Child with Microcephaly. Lancet 2016, 387, 228. [Google Scholar] [CrossRef] [PubMed]
- Marquezan, M.C.; Ventura, C.V.; Sheffield, J.S.; Golden, W.C.; Omiadze, R.; Belfort, R.; May, W. Ocular Effects of Zika Virus-a Review. Surv. Ophthalmol. 2018, 63, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Ventura, C.V.; Ventura, L.O.; Bravo-Filho, V.; Martins, T.T.; Berrocal, A.M.; Gois, A.L.; de Oliveira Dias, J.R.; Araújo, L.; Escarião, P.; van der Linden, V.; et al. Optical Coherence Tomography of Retinal Lesions in Infants with Congenital Zika Syndrome. JAMA Ophthalmol. 2016, 134, 1420–1427. [Google Scholar] [CrossRef] [PubMed]
- Zin, A.A.; Tsui, I.; Rossetto, J.; Vasconcelos, Z.; Adachi, K.; Valderramos, S.; Halai, U.-A.; Pone, M.V.d.S.; Pone, S.M.; Silveira Filho, J.C.B.; et al. Screening Criteria for Ophthalmic Manifestations of Congenital Zika Virus Infection. JAMA Pediatr. 2017, 171, 847–854. [Google Scholar] [CrossRef] [PubMed]
- de Paula Freitas, B.; de Oliveira Dias, J.R.; Prazeres, J.; Sacramento, G.A.; Ko, A.I.; Maia, M.; Belfort, R. Ocular Findings in Infants with Microcephaly Associated with Presumed Zika Virus Congenital Infection in Salvador, Brazil. JAMA Ophthalmol. 2016, 134, 529–535. [Google Scholar] [CrossRef]
- Vasconcelos, G.C.; Macedo Pereira, C.M.; Toledo de Paula, C.H.; de Souza Haueisen Barbosa, P.; Machado de Souza, D.; Coelho, L.M. Corneal Ectasia and High Ametropia in an Infant with Microcephaly Associated with Presumed Zika Virus Congenital Infection: New Ocular Findings. J. AAPOS 2019, 23, 354–356. [Google Scholar] [CrossRef] [PubMed]
- Yepez, J.B.; Murati, F.A.; Pettito, M.; Peñaranda, C.F.; de Yepez, J.; Maestre, G.; Arevalo, J.F.; Johns Hopkins Zika Center. Ophthalmic Manifestations of Congenital Zika Syndrome in Colombia and Venezuela. JAMA Ophthalmol. 2017, 135, 440–445. [Google Scholar] [CrossRef]
- Fernandez, M.P.; Parra Saad, E.; Ospina Martinez, M.; Corchuelo, S.; Mercado Reyes, M.; Herrera, M.J.; Parra Saavedra, M.; Rico, A.; Fernandez, A.M.; Lee, R.K.; et al. Ocular Histopathologic Features of Congenital Zika Syndrome. JAMA Ophthalmol. 2017, 135, 1163–1169. [Google Scholar] [CrossRef]
- Agrawal, R.; Oo, H.H.; Balne, P.K.; Ng, L.; Tong, L.; Leo, Y.S. Zika Virus and the Eye. Ocul. Immunol. Inflamm. 2018, 26, 654–659. [Google Scholar] [CrossRef]
- Gouel-Cheron, A.; Lumbard, K.; Hunsberger, S.; Arteaga-Cabello, F.J.; Beigel, J.; Belaunzarán-Zamudio, P.F.; Caballero-Sosa, S.; Escobedo-López, K.; Ibarra-González, V.; Nájera-Cancino, J.G.; et al. Serial Real-Time RT-PCR and Serology Measurements Substantially Improve Zika and Dengue Virus Infection Classification in a Co-Circulation Area. Antivir. Res. 2019, 172, 104638. [Google Scholar] [CrossRef]
- Brasil, P.; Calvet, G.A.; Siqueira, A.M.; Wakimoto, M.; de Sequeira, P.C.; Nobre, A.; Quintana, M.d.S.B.; de Mendonça, M.C.L.; Lupi, O.; de Souza, R.V.; et al. Zika Virus Outbreak in Rio de Janeiro, Brazil: Clinical Characterization, Epidemiological and Virological Aspects. PLoS Negl. Trop. Dis. 2016, 10, e0004636. [Google Scholar] [CrossRef] [PubMed]
- Bingham, A.M.; Cone, M.; Mock, V.; Heberlein-Larson, L.; Stanek, D.; Blackmore, C.; Likos, A. Comparison of Test Results for Zika Virus RNA in Urine, Serum, and Saliva Specimens from Persons with Travel-Associated Zika Virus Disease—Florida, 2016. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 475–478. [Google Scholar] [CrossRef] [PubMed]
- Gourinat, A.-C.; O’Connor, O.; Calvez, E.; Goarant, C.; Dupont-Rouzeyrol, M. Detection of Zika Virus in Urine. Emerg. Infect. Dis. 2015, 21, 84–86. [Google Scholar] [CrossRef]
- Rabe, I.B.; Staples, J.E.; Villanueva, J.; Hummel, K.B.; Johnson, J.A.; Rose, L.; Hills, S.; Wasley, A.; Fischer, M.; Powers, A.M. Interim Guidance for Interpretation of Zika Virus Antibody Test Results. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 543–546. [Google Scholar] [CrossRef] [PubMed]
- Sadeer, N.B.; El Kalamouni, C.; Khalid, A.; Abdalla, A.N.; Zengin, G.; Khoa Bao, L.V.; Mahomoodally, M.F. Secondary Metabolites as Potential Drug Candidates against Zika Virus, an Emerging Looming Human Threat: Current Landscape, Molecular Mechanism and Challenges Ahead. J. Infect. Public Health 2023, 16, 754–770. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Xu, M.; Lee, E.M.; Gorshkov, K.; Shiryaev, S.A.; He, S.; Sun, W.; Cheng, Y.-S.; Hu, X.; Tharappel, A.M.; et al. Emetine Inhibits Zika and Ebola Virus Infections through Two Molecular Mechanisms: Inhibiting Viral Replication and Decreasing Viral Entry. Cell Discov. 2018, 4, 31. [Google Scholar] [CrossRef]
- Wang, Y.; Ling, L.; Zhang, Z.; Marin-Lopez, A. Current Advances in Zika Vaccine Development. Vaccines 2022, 10, 1816. [Google Scholar] [CrossRef]
- Burgomaster, K.E.; Foreman, B.M.; Aleshnick, M.A.; Larman, B.C.; Gordon, D.N.; Maciejewski, S.; Morabito, K.M.; Ledgerwood, J.E.; Gaudinski, M.R.; Chen, G.L.; et al. Limited Flavivirus Cross-Reactive Antibody Responses Elicited by a Zika Virus Deoxyribonucleic Acid Vaccine Candidate in Humans. J. Infect. Dis. 2021, 224, 1550–1555. [Google Scholar] [CrossRef]
- Richner, J.M.; Himansu, S.; Dowd, K.A.; Butler, S.L.; Salazar, V.; Fox, J.M.; Julander, J.G.; Tang, W.W.; Shresta, S.; Pierson, T.C.; et al. Modified mRNA Vaccines Protect against Zika Virus Infection. Cell 2017, 168, 1114–1125.e10. [Google Scholar] [CrossRef]
- Haut Conseil de la Sante Publique. Statement on the Medical Care Provided for and the Monitoring of New-Borns and Infants Having Been Exposed to the Zika Virus in Utero or Present. 2017. Available online: https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=675 (accessed on 2 August 2018).
- Adebanjo, T.; Godfred-Cato, S.; Viens, L.; Fischer, M.; Staples, J.E.; Kuhnert-Tallman, W.; Walke, H.; Oduyebo, T.; Polen, K.; Peacock, G.; et al. Update: Interim Guidance for the Diagnosis, Evaluation, and Management of Infants with Possible Congenital Zika Virus Infection—United States, October 2017. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 1089–1099. [Google Scholar] [CrossRef]
- Yakob, L.; Hu, W.; Frentiu, F.D.; Gyawali, N.; Hugo, L.E.; Johnson, B.; Lau, C.; Furuya-Kanamori, L.; Magalhaes, R.S.; Devine, G. Japanese Encephalitis Emergence in Australia: The Potential Population at Risk. Clin. Infect. Dis. 2023, 76, 335–337. [Google Scholar] [CrossRef] [PubMed]
- Solomon, T. Control of Japanese Encephalitis--within Our Grasp? N. Engl. J. Med. 2006, 355, 869–871. [Google Scholar] [CrossRef] [PubMed]
- Buescher, E.L.; Scherer, W.F.; Rosenberg, M.Z.; Gresser, I.; Hardy, J.L.; Bullock, H.R. Ecologic Studies of Japanese Encephalitis Virus in Japan. II. Mosquito Infection. Am. J. Trop. Med. Hyg. 1959, 8, 651–664. [Google Scholar] [CrossRef] [PubMed]
- Fischer, M.; Lindsey, N.; Staples, J.E.; Hills, S.; Centers for Disease Control and Prevention (CDC). Japanese Encephalitis Vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm. Rep. 2010, 59, 1–27. [Google Scholar] [PubMed]
- Hills, S.L.; Netravathi, M.; Solomon, T. Japanese Encephalitis among Adults: A Review. Am. J. Trop. Med. Hyg. 2023, 108, 860–864. [Google Scholar] [CrossRef] [PubMed]
- Turtle, L.; Solomon, T. Japanese Encephalitis—The Prospects for New Treatments. Nat. Rev. Neurol. 2018, 14, 298–313. [Google Scholar] [CrossRef] [PubMed]
- Solomon, T.; Dung, N.M.; Kneen, R.; Gainsborough, M.; Vaughn, D.W.; Khanh, V.T. Japanese Encephalitis. J. Neurol. Neurosurg. Psychiatry 2000, 68, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Fang, S.-T.; Chu, S.-Y.; Lee, Y.-C. Ischaemic Maculopathy in Japanese Encephalitis. Eye 2006, 20, 1439–1441. [Google Scholar] [CrossRef]
- Van, K.; Korman, T.M.; Nicholson, S.; Troutbeck, R.; Lister, D.M.; Woolley, I. Case Report: Japanese Encephalitis Associated with Chorioretinitis after Short-Term Travel to Bali, Indonesia. Am. J. Trop. Med Hyg. 2020, 103, 1691–1693. [Google Scholar] [CrossRef]
- Chanama, S.; Sukprasert, W.; Sa-ngasang, A.; A-nuegoonpipat, A.; Sangkitporn, S.; Kurane, I.; Anantapreecha, S. Detection of Japanese Encephalitis (JE) Virus-Specific IgM in Cerebrospinal Fluid and Serum Samples from JE Patients. Jpn. J. Infect. Dis. 2005, 58, 294–296. [Google Scholar]
- Swami, R.; Ratho, R.K.; Mishra, B.; Singh, M.P. Usefulness of RT-PCR for the Diagnosis of Japanese Encephalitis in Clinical Samples. Scand. J. Infect. Dis. 2008, 40, 815–820. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, A.; Taraphdar, D.; Mukhopadhyay, S.K.; Chakrabarti, S.; Chatterjee, S. Serological and Molecular Diagnosis of Japanese Encephalitis Reveals an Increasing Public Health Problem in the State of West Bengal, India. Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 15–19. [Google Scholar] [CrossRef]
- Sarkar, A.; Datta, S.; Pathak, B.K.; Mukhopadhyay, S.K.; Chatterjee, S. Japanese Encephalitis Associated Acute Encephalitis Syndrome Cases in West Bengal, India: A Sero-Molecular Evaluation in Relation to Clinico-Pathological Spectrum. J. Med. Virol. 2015, 87, 1258–1267. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, A. Control of Japanese Encephalitis in Japan: Immunization of Humans and Animals, and Vector Control. Curr. Top. Microbiol. Immunol. 2002, 267, 139–152. [Google Scholar] [CrossRef] [PubMed]
- Yun, S.-I.; Lee, Y.-M. Japanese Encephalitis: The Virus and Vaccines. Hum. Vaccin. Immunother. 2014, 10, 263–279. [Google Scholar] [CrossRef] [PubMed]
- Erlanger, T.E.; Weiss, S.; Keiser, J.; Utzinger, J.; Wiedenmayer, K. Past, Present, and Future of Japanese Encephalitis. Emerg. Infect. Dis. 2009, 15, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.Z.; Jabbar, B.; Ahmed, N.; Rehman, A.; Nasir, H.; Nadeem, S.; Jabbar, I.; Rahman, Z.U.; Azam, S. Epidemiology, Pathogenesis, and Control of a Tick-Borne Disease-Kyasanur Forest Disease: Current Status and Future Directions. Front. Cell. Infect. Microbiol. 2018, 8, 149. [Google Scholar] [CrossRef] [PubMed]
- Work, T.H.; Trapido, H.; Murthy, D.P.N.; Rao, R.L.; Bhatt, P.N.; Kulkarni, K.G. Kyasanur Forest Disease. III. A Preliminary Report on the Nature of the Infection and Clinical Manifestations in Human Beings. Indian J. Med. Sci. 1957, 11, 619–645. [Google Scholar]
- Chakraborty, S.; Andrade, F.C.D.; Ghosh, S.; Uelmen, J.; Ruiz, M.O. Historical Expansion of Kyasanur Forest Disease in India From 1957 to 2017: A Retrospective Analysis. Geohealth 2019, 3, 44–55. [Google Scholar] [CrossRef]
- Sadanandane, C.; Gokhale, M.D.; Elango, A.; Yadav, P.; Mourya, D.T.; Jambulingam, P. Prevalence and Spatial Distribution of Ixodid Tick Populations in the Forest Fringes of Western Ghats Reported with Human Cases of Kyasanur Forest Disease and Monkey Deaths in South India. Exp. Appl. Acarol. 2018, 75, 135–142. [Google Scholar] [CrossRef]
- Pattnaik, P. Kyasanur Forest Disease: An Epidemiological View in India. Rev. Med. Virol. 2006, 16, 151–165. [Google Scholar] [CrossRef]
- Ocular Manifestations of Kyasanur Forest Disease (a Clinical Study). Indian J. Ophthalmol. 1983, 31, 700–702.
- Iyer, C.G.; Laxmana Rao, R.; Work, T.H.; Narasimha Murthy, D.P. Kyasanur Forest Disease VI. Pathological Findings in Three Fatal Human Cases of Kyasanur Forest Disease. Indian J. Med. Sci. 1959, 13, 1011–1022. [Google Scholar]
- Mourya, D.T.; Yadav, P.D.; Mehla, R.; Barde, P.V.; Yergolkar, P.N.; Kumar, S.R.P.; Thakare, J.P.; Mishra, A.C. Diagnosis of Kyasanur Forest Disease by Nested RT-PCR, Real-Time RT-PCR and IgM Capture ELISA. J. Virol. Methods 2012, 186, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Cook, B.W.M.; Ranadheera, C.; Nikiforuk, A.M.; Cutts, T.A.; Kobasa, D.; Court, D.A.; Theriault, S.S. Limited Effects of Type I Interferons on Kyasanur Forest Disease Virus in Cell Culture. PLoS Negl. Trop. Dis. 2016, 10, e0004871. [Google Scholar] [CrossRef] [PubMed]
- Kiran, S.K.; Pasi, A.; Kumar, S.; Kasabi, G.S.; Gujjarappa, P.; Shrivastava, A.; Mehendale, S.; Chauhan, L.S.; Laserson, K.F.; Murhekar, M. Kyasanur Forest Disease Outbreak and Vaccination Strategy, Shimoga District, India, 2013–2014. Emerg. Infect. Dis. 2015, 21, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Kasabi, G.S.; Murhekar, M.V.; Sandhya, V.K.; Raghunandan, R.; Kiran, S.K.; Channabasappa, G.H.; Mehendale, S.M. Coverage and Effectiveness of Kyasanur Forest Disease (KFD) Vaccine in Karnataka, South India, 2005–2010. PLoS Negl. Trop. Dis. 2013, 7, e2025. [Google Scholar] [CrossRef] [PubMed]
- Srikanth, U.G.K.; Marinaik, C.B.; Gomes, A.R.; Rathnamma, D.; Byregowda, S.M.; Isloor, S.; Munivenkatarayappa, A.; Venkatesha, M.D.; Rao, S.; Rizwan, A.; et al. Evaluation of Safety and Potency of Kyasanur Forest Disease (KFD) Vaccine Inactivated with Different Concentrations of Formalin and Comparative Evaluation of In Vitro and In Vivo Methods of Virus Titration in KFD Vaccine. Biomedicines 2023, 11, 1871. [Google Scholar] [CrossRef]
- Ogden, N.H.; Bigras-Poulin, M.; O’Callaghan, C.J.; Barker, I.K.; Lindsay, L.R.; Maarouf, A.; Smoyer-Tomic, K.E.; Waltner-Toews, D.; Charron, D. A Dynamic Population Model to Investigate Effects of Climate on Geographic Range and Seasonality of the Tick Ixodes Scapularis. Int. J. Parasitol. 2005, 35, 375–389. [Google Scholar] [CrossRef]
- Satish, K.V.; Saranya, K.R.L.; Reddy, C.S.; Krishna, P.H.; Jha, C.S.; Rao, P.V.V.P. Geospatial Assessment and Monitoring of Historical Forest Cover Changes (1920–2012) in Nilgiri Biosphere Reserve, Western Ghats, India. Environ. Monit. Assess. 2014, 186, 8125–8140. [Google Scholar] [CrossRef]
Figure 1.
Schematic representation of a flavivirus viral particle (A) and genome (B). Adapted from https://viralzone.expasy.org/24 (accessed on 1 January 2011) with authorization [12].
Figure 1.
Schematic representation of a flavivirus viral particle (A) and genome (B). Adapted from https://viralzone.expasy.org/24 (accessed on 1 January 2011) with authorization [12].

Figure 2.
Fluorescein angiogram of the right eye of a 33-year-old woman presenting with sudden loss of vision 1 week after the onset of dengue hemorrhagic fever showing dengue maculopathy, manifesting as severe retinal vasculitis with prominent vascular leakage (Courtesy of Pr Soon Phaik Chee).
Figure 2.
Fluorescein angiogram of the right eye of a 33-year-old woman presenting with sudden loss of vision 1 week after the onset of dengue hemorrhagic fever showing dengue maculopathy, manifesting as severe retinal vasculitis with prominent vascular leakage (Courtesy of Pr Soon Phaik Chee).

Figure 3.
(A) Red-free fundus photograph of the left eye of a patient with dengue fever shows a subretinal round, yellowish lesion at the fovea (white arrow). (B) Optical coherence tomography through the lesion demonstrates conical foveal elevation (yellow arrow) with focal outer neurosensory retinal pigment epithelium thickening (Courtesy of Pr Soon Phaik Chee).
Figure 3.
(A) Red-free fundus photograph of the left eye of a patient with dengue fever shows a subretinal round, yellowish lesion at the fovea (white arrow). (B) Optical coherence tomography through the lesion demonstrates conical foveal elevation (yellow arrow) with focal outer neurosensory retinal pigment epithelium thickening (Courtesy of Pr Soon Phaik Chee).

Figure 4.
Color fundus photographs (A) and fluorescein angiograms (B) of the left eye of a diabetic patient with WNV infection show inactive multifocal chorioretinitis with typical linear clustering and the ‘target-like appearance’ of chorioretinal lesions (white arrowheads) with central hypofluorescence and peripheral hyperfluorescence (yellow arrowheads). Note the presence of associated moderate to severe non-proliferative diabetic retinopathy.
Figure 4.
Color fundus photographs (A) and fluorescein angiograms (B) of the left eye of a diabetic patient with WNV infection show inactive multifocal chorioretinitis with typical linear clustering and the ‘target-like appearance’ of chorioretinal lesions (white arrowheads) with central hypofluorescence and peripheral hyperfluorescence (yellow arrowheads). Note the presence of associated moderate to severe non-proliferative diabetic retinopathy.

Figure 5.
Fundus photograph of the left eye of a newborn with congenital Zika virus syndrome shows macular, well-delineated atrophic lesions (Courtesy of Pr Rubens Belfort).
Figure 5.
Fundus photograph of the left eye of a newborn with congenital Zika virus syndrome shows macular, well-delineated atrophic lesions (Courtesy of Pr Rubens Belfort).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Zina, S.M.; Hoarau, G.; Labetoulle, M.; Khairallah, M.; Rousseau, A. Ocular Manifestations of Flavivirus Infections. Pathogens 2023, 12, 1457. https://doi.org/10.3390/pathogens12121457
AMA Style
Zina SM, Hoarau G, Labetoulle M, Khairallah M, Rousseau A. Ocular Manifestations of Flavivirus Infections. Pathogens. 2023; 12(12):1457. https://doi.org/10.3390/pathogens12121457
Chicago/Turabian StyleZina, Sourour Meziou, Gautier Hoarau, Marc Labetoulle, Moncef Khairallah, and Antoine Rousseau. 2023. "Ocular Manifestations of Flavivirus Infections" Pathogens 12, no. 12: 1457. https://doi.org/10.3390/pathogens12121457
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.