
Human Papillomavirus Genotype Richness and the Biodiversity of Squamous and Glandular Cervical Dysplasias: A Cross-Sectional Study
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Human Papillomavirus DNA Detection and Genotyping
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bernard, H.-U.; Burk, R.D.; Chen, Z.; van Doorslaer, K.; zur Hausen, H.; de Villiers, E.-M. Classification of Papillomaviruses (PVs) Based on 189 PV Types and Proposal of Taxonomic Amendments. Virology 2010, 401, 70–79. [Google Scholar] [CrossRef]
- Walboomers, J.M.M.; Jacobs, M.V.; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K.V.; Snijders, P.J.F.; Peto, J.; Meijer, C.J.L.M.; Muñoz, N. Human Papillomavirus Is a Necessary Cause of Invasive Cervical Cancer Worldwide. J. Pathol. 1999, 189, 12–19. [Google Scholar] [CrossRef]
- IARC. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; International Agency for Research on Cancer: Lyon, France, 2007; Volume 90. [Google Scholar]
- Schiffman, M.; Castle, P.E.; Jeronimo, J.; Rodriguez, A.C.; Wacholder, S. Human Papillomavirus and Cervical Cancer. Lancet 2007, 370, 890–907. [Google Scholar] [CrossRef] [PubMed]
- Bonde, J.; Bottari, F.; Iacobone, A.D.; Cocuzza, C.E.; Sandri, M.-T.; Bogliatto, F.; Khan, K.S.; Ejegod, D.M.; Gary, D.S.; Andrews, J.C. Human Papillomavirus Same Genotype Persistence and Risk: A Systematic Review. J. Low. Genit. Tract. Dis. 2021, 25, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.M.; Smith, J.S.; Plummer, M.; Muñoz, N.; Franceschi, S. Human Papillomavirus Types in Invasive Cervical Cancer Worldwide: A Meta-Analysis. Br. J. Cancer 2003, 88, 63–73. [Google Scholar] [CrossRef] [PubMed]
- De Sanjose, S.; Quint, W.G.; Alemany, L.; Geraets, D.T.; Klaustermeier, J.E.; Lloveras, B.; Tous, S.; Felix, A.; Bravo, L.E.; Shin, H.-R.; et al. Human Papillomavirus Genotype Attribution in Invasive Cervical Cancer: A Retrospective Cross-Sectional Worldwide Study. Lancet Oncol. 2010, 11, 1048–1056. [Google Scholar] [CrossRef] [PubMed]
- Dunne, E.F.; Unger, E.R.; Sternberg, M.; McQuillan, G.; Swan, D.C.; Patel, S.S.; Markowitz, L.E. Prevalence of HPV Infection among Females in the United States. JAMA 2007, 297, 813. [Google Scholar] [CrossRef]
- Salazar, K.L.; Zhou, H.S.; Xu, J.; Peterson, L.E.; Schwartz, M.R.; Mody, D.R.; Ge, Y. Multiple Human Papilloma Virus Infections and Their Impact on the Development of High-Risk Cervical Lesions. Acta Cytol. 2015, 59, 391–398. [Google Scholar] [CrossRef]
- Burger, E.A.; Kim, J.J.; Sy, S.; Castle, P.E. Age of Acquiring Causal Human Papillomavirus (HPV) Infections: Leveraging Simulation Models to Explore the Natural History of HPV-Induced Cervical Cancer. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2017, 65, 893–899. [Google Scholar] [CrossRef]
- Chaturvedi, A.K.; Katki, H.A.; Hildesheim, A.; Rodríguez, A.C.; Quint, W.; Schiffman, M.; Van Doorn, L.-J.; Porras, C.; Wacholder, S.; Gonzalez, P.; et al. Human Papillomavirus Infection with Multiple Types: Pattern of Coinfection and Risk of Cervical Disease. J. Infect. Dis. 2011, 203, 910–920. [Google Scholar] [CrossRef]
- Dasgupta, S. A Review on Cervical Dysplasia: Etiology, Risk Factors, Diagnostic Biomarkers and Possible Nutritional Association. Asian Pac. J. Cancer Care 2022, 7, 555–563. [Google Scholar] [CrossRef]
- Camargo, M.; Del Río-Ospina, L.; Soto-De León, S.C.; Sánchez, R.; Pineda-Peña, A.C.; Sussmann, O.; Patarroyo, M.E.; Patarroyo, M.A. Association of HIV Status with Infection by Multiple HPV Types. Trop. Med. Int. Health 2018, 23, 1259–1268. [Google Scholar] [CrossRef] [PubMed]
- Trottier, H.; Mahmud, S.; Costa, M.C.; Sobrinho, J.P.; Duarte-Franco, E.; Rohan, T.E.; Ferenczy, A.; Villa, L.L.; Franco, E.L. Human Papillomavirus Infections with Multiple Types and Risk of Cervical Neoplasia. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1274–1280. [Google Scholar] [CrossRef] [PubMed]
- Spinillo, A.; Dal Bello, B.; Gardella, B.; Roccio, M.; Dacco’, M.D.; Silini, E.M. Multiple Human Papillomavirus Infection and High Grade Cervical Intraepithelial Neoplasia among Women with Cytological Diagnosis of Atypical Squamous Cells of Undetermined Significance or Low Grade Squamous Intraepithelial Lesions. Gynecol. Oncol. 2009, 113, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Bello, B.D.; Spinillo, A.; Alberizzi, P.; Cesari, S.; Gardella, B.; D’Ambrosio, G.; Roccio, M.; Silini, E.M. Cervical Infections by Multiple Human Papillomavirus (HPV) Genotypes: Prevalence and Impact on the Risk of Precancerous Epithelial Lesions. J. Med. Virol. 2009, 81, 703–712. [Google Scholar] [CrossRef] [PubMed]
- Fife, K.H.; Cramer, H.M.; Schroeder, J.M.; Brown, D.R. Detection of Multiple Human Papillomavirus Types in the Lower Genital Tract Correlates with Cervical Dysplasia. J. Med. Virol. 2001, 64, 550–559. [Google Scholar] [CrossRef]
- Herrero, R.; Castle, P.E.; Schiffman, M.; Bratti, M.C.; Hildesheim, A.; Morales, J.; Alfaro, M.; Sherman, M.E.; Wacholder, S.; Chen, S.; et al. Epidemiologic Profile of Type-Specific Human Papillomavirus Infection and Cervical Neoplasia in Guanacaste, Costa Rica. J. Infect. Dis. 2005, 191, 1796–1807. [Google Scholar] [CrossRef]
- Ah Lee, S.; Kang, D.; Soo Seo, S.; Kim Jeong, J.; Young Yoo, K.; Tark Jeon, Y.; Weon Kim, J.; Hyun Park, N.; Beom Kang, S.; Pyo Lee, H.; et al. Multiple HPV Infection in Cervical Cancer Screened by HPVDNAChipTM. Cancer Lett. 2003, 198, 187–192. [Google Scholar] [CrossRef]
- Pista, A.; Oliveira, A.; Verdasca, N.; Ribeiro, F. Single and Multiple Human Papillomavirus Infections in Cervical Abnormalities in Portuguese Women. Clin. Microbiol. Infect. 2011, 17, 941–946. [Google Scholar] [CrossRef]
- Wheeler, C.M.; Hunt, W.C.; Schiffman, M.; Castle, P.E.; Atypical Squamous Cells of Undetermined Significance/Low-Grade Squamous Intraepithelial Lesions Triage Study (ALTS) Group. Human Papillomavirus Genotypes and the Cumulative 2-Year Risk of Cervical Precancer. J. Infect. Dis. 2006, 194, 1291–1299. [Google Scholar] [CrossRef]
- Wentzensen, N.; Schiffman, M.; Dunn, S.T.; Zuna, R.E.; Gold, M.A.; Allen, R.A.; Zhang, R.; Sherman, M.E.; Wacholder, S.; Walker, J.; et al. Multiple HPV Genotype Infections in Cervical Cancer Progression in the Study to Understand Cervical Cancer Early Endpoints and Determinants (SUCCEED). Int. J. Cancer J. Int. Cancer 2009, 125, 2151–2158. [Google Scholar] [CrossRef] [PubMed]
- Cuschieri, K.S. Multiple High Risk HPV Infections Are Common in Cervical Neoplasia and Young Women in a Cervical Screening Population. J. Clin. Pathol. 2004, 57, 68–72. [Google Scholar] [CrossRef]
- Adcock, R.; Cuzick, J.; Hunt, W.C.; McDonald, R.M.; Wheeler, C.M.; Joste, N.E.; Kinney, W.; Wheeler, C.M.; Hunt, W.C.; McDonald, R.M.; et al. Role of HPV Genotype, Multiple Infections, and Viral Load on the Risk of High-Grade Cervical Neoplasia. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1816–1824. [Google Scholar] [CrossRef]
- Schmitt, M.; Depuydt, C.; Benoy, I.; Bogers, J.; Antoine, J.; Arbyn, M.; Pawlita, M.; on behalf of the VALGENT Study Group. Multiple Human Papillomavirus Infections with High Viral Loads Are Associated with Cervical Lesions but Do Not Differentiate Grades of Cervical Abnormalities. J. Clin. Microbiol. 2020, 51, 1458–1464. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Shi, X.; Liu, J.; Zhang, L. Correlation between Human Papillomavirus Viral Load and Cervical Lesions Classification: A Review of Current Research. Front. Med. 2023, 10, 1111269. [Google Scholar] [CrossRef]
- Heip, C.H.; Peter, H. Indices of Diversity and Richness. Océanis. 1998, 24, 61–87. [Google Scholar]
- Whittaker, R.J.; Willis, K.J.; Field, R. Scale and Species Richness: Towards a General, Hierarchical Theory of Species Diversity: Towards a General Theory of Diversity. J. Biogeogr. 2001, 28, 453–470. [Google Scholar] [CrossRef]
- Bosch, F.X.; Lorincz, A.; Munoz, N.; Meijer, C.J.L.M.; Shah, K.V. The Causal Relation between Human Papillomavirus and Cervical Cancer. J. Clin. Pathol. 2002, 55, 244–265. [Google Scholar] [CrossRef] [PubMed]
- van der Marel, J.; Berkhof, J.; Ordi, J.; Torné, A.; Del Pino, M.; van Baars, R.; Schiffman, M.; Wentzensen, N.; Jenkins, D.; Quint, W.G.V. Attributing Oncogenic Human Papillomavirus Genotypes to High-Grade Cervical Neoplasia: Which Type Causes the Lesion? Am. J. Surg. Pathol. 2015, 39, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Venetianer, R.; Clarke, M.A.; van der Marel, J.; Tota, J.; Schiffman, M.; Dunn, S.T.; Walker, J.; Zuna, R.; Quint, W.; Wentzensen, N. Identification of HPV Genotypes Causing Cervical Precancer Using Tissue-Based Genotyping. Int. J. Cancer 2020, 146, 2836–2844. [Google Scholar] [CrossRef]
- Bottari, F.; Passerini, R.; Renne, G.; Guerrieri, M.E.; Sandri, M.T.; Li, A.; Orlandini, A.; Iacobone, A.D. Onclarity Performance in Human Papillomavirus DNA Detection in Formalin-Fixed Paraffin-Embedded Cervical Samples. J. Low. Genit. Tract. Dis. 2021, 25, 216–220. [Google Scholar] [CrossRef]
- Basukala, O.; Banks, L. The Not-So-Good, the Bad and the Ugly: HPV E5, E6 and E7 Oncoproteins in the Orchestration of Carcinogenesis. Viruses 2021, 13, 1892. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Oštrbenk, A.; Poljak, M.; Arbyn, M. Assessment of the Roche Linear Array HPV Genotyping Test within the VALGENT Framework. J. Clin. Virol. 2018, 98, 37–42. [Google Scholar] [CrossRef]
- Quint, W.; Jenkins, D.; Molijn, A.; Struijk, L.; Van De Sandt, M.; Doorbar, J.; Mols, J.; Van Hoof, C.; Hardt, K.; Struyf, F.; et al. One Virus, One Lesion-Individual Components of CIN Lesions Contain a Specific HPV Type. J. Pathol. 2012, 227, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Ring, L.L.; Munk, C.; Galanakis, M.; Tota, J.E.; Thomsen, L.T.; Kjaer, S.K. Incidence of Cervical Precancerous Lesions and Cervical Cancer in Denmark from 2000 to 2019: Population Impact of Multi-Cohort Vaccination against Human Papillomavirus Infection. Int. J. Cancer 2023, 152, 1320–1327. [Google Scholar] [CrossRef]
- Benard, V.B.; Castle, P.E.; Jenison, S.A.; Hunt, W.C.; Kim, J.J.; Cuzick, J.; Lee, J.-H.; Du, R.; Robertson, M.; Norville, S.; et al. Population-Based Incidence Rates of Cervical Intraepithelial Neoplasia in the Human Papillomavirus Vaccine Era. JAMA Oncol. 2017, 3, 833. [Google Scholar] [CrossRef]
- Chan, P.K.S.; Chang, A.R.; Cheung, J.L.K.; Chan, D.P.C.; Xu, L.Y.; Tang, N.L.S.; Cheng, A.F. Determinants of Cervical Human Papillomavirus Infection: Differences between High- and Low-Oncogenic Risk Types. J. Infect. Dis. 2002, 185, 28–35. [Google Scholar] [CrossRef]
- Iacobone, A.D.; Bottari, F.; Radice, D.; Preti, E.P.; Franchi, D.; Vidal Urbinati, A.M.; Boveri, S.; Passerini, R.; Sandri, M.T. Distribution of High-Risk Human Papillomavirus Genotypes and Multiple Infections in Preneoplastic and Neoplastic Cervical Lesions of Unvaccinated Women: A Cross-Sectional Study. J. Low. Genit. Tract. Dis. 2019, 23, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Du, X.; Lu, M.; Zhang, W.; Sun, Z.; Li, L.; Ye, M.; Fan, W.; Jiang, S.; Liu, A.; et al. Prevalence Characteristics of Single and Multiple HPV Infections in Women with Cervical Cancer and Precancerous Lesions in Beijing, China. J. Med. Virol. 2019, 91, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Song, F.; Yan, P.; Huang, X.; Wang, C.; Du, H.; Qu, X.; Wu, R. Roles of Extended Human Papillomavirus Genotyping and Multiple Infections in Early Detection of Cervical Precancer and Cancer and HPV Vaccination. BMC Cancer 2022, 22, 42. [Google Scholar] [CrossRef]
- Depuydt, C.E.; Thys, S.; Beert, J.; Jonckheere, J.; Salembier, G.; Bogers, J.J. Linear Viral Load Increase of a Single HPV-Type in Women with Multiple HPV Infections Predicts Progression to Cervical Cancer. Int. J. Cancer 2016, 139, 2021–2032. [Google Scholar] [CrossRef]
- Spinillo, A.; Gardella, B.; Iacobone, A.D.; Cesari, S.; Alberizzi, P.; Silini, E.M. Multiple Papillomavirus Infection and Size of Colposcopic Lesions among Women with Cervical Intraepithelial Neoplasia. J. Low. Genit. Tract. Dis. 2016, 20, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Stoler, M.H.; Wright, T.C.; Parvu, V.; Yanson, K.; Cooper, C.K.; Andrews, J. Stratified Risk of High-Grade Cervical Disease Using Onclarity HPV Extended Genotyping in Women, ≥25 years of Age, with NILM Cytology. Gynecol. Oncol. 2019, 153, 26–33. [Google Scholar] [CrossRef]
- Zhong, F.; Yu, T.; Ma, X.; Wang, S.; Cong, Q.; Tao, X. Extensive HPV Genotyping Reveals High Association between Multiple Infections and Cervical Lesions in Chinese Women. Dis. Markers 2022, 2022, 8130373. [Google Scholar] [CrossRef] [PubMed]
- Bonde, J.; Bottari, F.; Parvu, V.; Pedersen, H.; Yanson, K.; Iacobone, A.D.; Kodsi, S.; Landoni, F.; Vaughan, L.; Ejegod, D.M.; et al. Bayesian Analysis of Baseline Risk of CIN2 and ≥CIN3 by HPV Genotype in a European Referral Cohort. Int. J. Cancer 2019, 145, 1033–1041. [Google Scholar] [CrossRef]
- Koeneman, M.M.; Hendriks, N.; Kooreman, L.F.; Winkens, B.; Kruitwagen, R.F.; Kruse, A.J. Prognostic Factors for Spontaneous Regression of High-Risk Human Papillomavirus-Positive Cervical Intra-Epithelial Neoplasia Grade 2. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2019, 29, 1003–1009. [Google Scholar] [CrossRef]
- Tainio, K.; Athanasiou, A.; Tikkinen, K.A.O.; Aaltonen, R.; Hernándes, J.C.; Glazer-Livson, S.; Jakobsson, M.; Joronen, K.; Kiviharju, M.; Louvanto, K.; et al. Clinical Course of Untreated Cervical Intraepithelial Neoplasia Grade 2 under Active Surveillance: Systematic Review and Meta-Analysis. BMJ 2018, 360, k499. [Google Scholar] [CrossRef]
- Bruno, M.T.; Scalia, G.; Cassaro, N.; Costanzo, M.; Boemi, S. Conservative Management of CIN2 P16 Positive Lesions in Women with Multiple HPV Infection. BMC Infect. Dis. 2020, 20, 801. [Google Scholar] [CrossRef] [PubMed]
- Höhn, A.K.; Brambs, C.E.; Hiller, G.G.R.; May, D.; Schmoeckel, E.; Horn, L.-C. 2020 WHO Classification of Female Genital Tumors. Geburtshilfe Frauenheilkd. 2021, 81, 1145–1153. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Cheng, X.; Ye, J.; Xu, X.; Hong, Y.; Sui, L.; You, Z.; Xie, X. Distribution of Human Papilloma Virus Genotype Prevalence in Invasive Cervical Carcinomas and Precancerous Lesions in the Yangtze River Delta Area, China. BMC Cancer 2018, 18, 487. [Google Scholar] [CrossRef] [PubMed]
- Pista, A.; de Oliveira, C.F.; Lopes, C.; Cunha, M.J.; CLEOPATRE Portugal Study Groupa. Human Papillomavirus Type Distribution in Cervical Intraepithelial Neoplasia Grade 2/3 and Cervical Cancer in Portugal: A CLEOPATRE II Study. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2013, 23, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Sigurdsson, K.; Taddeo, F.J.; Benediktsdottir, K.R.; Olafsdottir, K.; Sigvaldason, H.; Oddsson, K.; Rafnar, T. HPV Genotypes in CIN 2-3 Lesions and Cervical Cancer: A Population-Based Study. Int. J. Cancer 2007, 121, 2682–2687. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Statistics | |||||
|---|---|---|---|---|---|
| Mean (SD) | Median | IQR | p-Value | ||
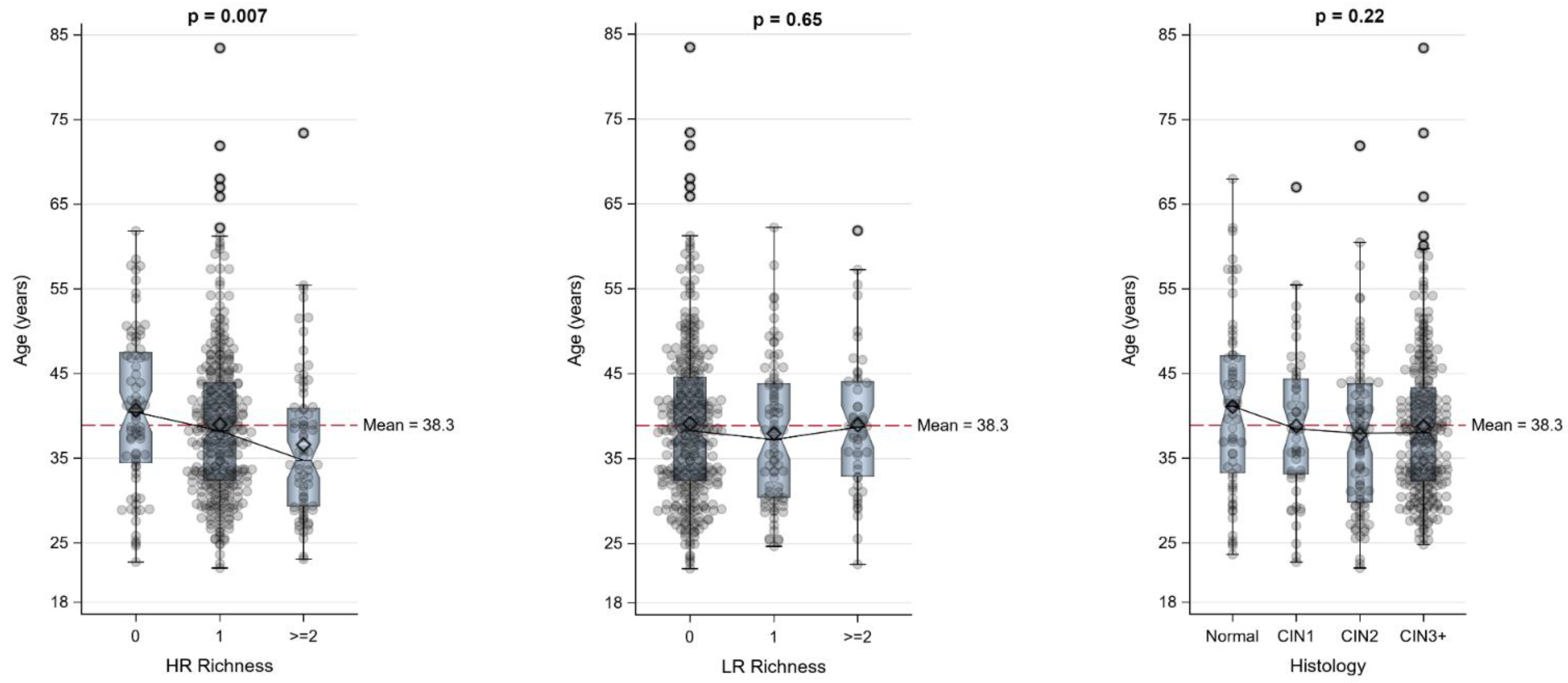
| HR Richness | |||||
| 0 | N = 76 | 40.7 (9.3) | 40.5 | 34,48 | |
| 1 | N = 321 | 39.0 (9.0) | 38.3 | 32,44 | |
| ≥2 | N = 72 | 36.6 (9.0) | 34.8 | 29,41 | 0.007 |
| LR Richness | |||||
| 0 | N = 335 | 39.1 (9.4) | 38.3 | 32,45 | |
| 1 | N = 83 | 37.9 (8.5) | 37.3 | 30,44 | |
| ≥2 | N = 51 | 39.0 (8.1) | 38.7 | 33,44 | 0.65 |
| Histology | |||||
| Normal | N = 62 | 41.1 (10.4) | 41.2 | 33,47 | |
| CIN1 | N = 50 | 38.8 (8.8) | 38.5 | 33,44 | |
| CIN2 | N = 91 | 37.8 (9.2) | 38.0 | 30,44 | |
| CIN3+ | N = 266 | 38.8 (8.7) | 38.0 | 32,43 | 0.22 |
| Histology, N (%) | ||||||
|---|---|---|---|---|---|---|
| All Patients N = 469 | Normal N = 62 | CIN1 N = 50 | CIN2 N = 91 | CIN3+ N = 266 | p-Value | |
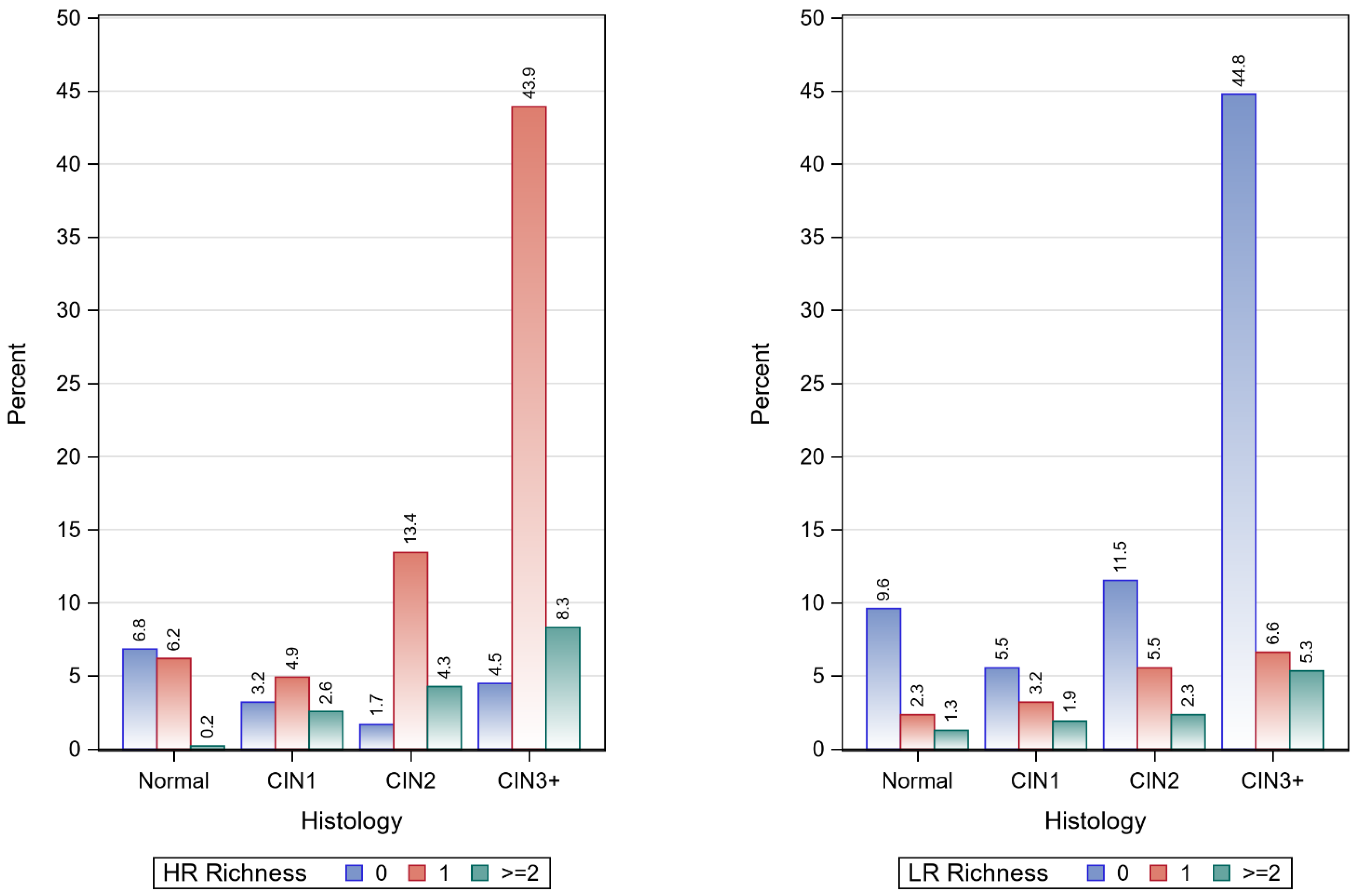
| HR Richness | ||||||
| 0 | 76 (16.2) | 32 (6.8) | 15 (3.2) | 8 (1.7) | 21 (4.5) | |
| 1 | 321 (68.4) | 29 (6.2) | 23 (4.9) | 63 (13.4) | 206 (43.9) | |
| ≥2 | 72 (15.4) | 1 (0.2) | 12 (2.6) | 20 (4.3) | 39 (8.3) | <0.001 |
| LR Richness | ||||||
| 0 | 335 (71.4) | 45 (9.6) | 26 (5.5) | 54 (11.5) | 210 (44.8) | |
| 1 | 83 (17.7) | 11 (2.4) | 15 (3.2) | 26 (5.5) | 31 (6.6) | |
| ≥2 | 51 (10.9) | 6 (1.3) | 9 (1.9) | 11 (2.4) | 25 (5.3) | <0.001 |
| LR Richness, N (%) | ||||||
|---|---|---|---|---|---|---|
| Histology | HR Richness | Row Total (%) | 0 | 1 | ≥2 | p-Value |
| Normal | 0 | 32 (53.1) | 26 (41.9) | 2 (3.2) | 4 (6.5) | |
| 1 | 29 (45.3) | 19 (30.7) | 8 (12.9) | 2 (3.2) | ||
| ≥2 | 1 (1.6) | 0 | 1 (1.6) | 0 | 0.04 | |
| CIN1 | 0 | 15 (30.0) | 8 (16.0) | 5 (10.0) | 2 (4.0) | |
| 1 | 23 (46.0) | 13 (26.0) | 5 (10.0) | 5 (10.0) | ||
| ≥2 | 12 (24.0) | 5 (10.0) | 5 (10.0) | 2 (4.0) | 0.79 | |
| CIN2 | 0 | 8 (8.8) | 3 (3.3) | 3 (3.3) | 2 (2.2) | |
| 1 | 63 (69.2) | 45 (49.5) | 14 (15.4) | 4 (4.4) | ||
| ≥2 | 20 (22.0) | 6 (6.6) | 9 (9.9) | 5 (5.5) | 0.004 | |
| CIN3+ | 0 | 21 (7.9) | 16 (6.0) | 2 (0.8) | 3 (1.1) | |
| 1 | 206 (77.4) | 163 (61.3) | 26 (9.8) | 17 (6.4) | ||
| ≥2 | 39 (14.7) | 31 (11.7) | 3 (1.1) | 5 (1.9) | 0.68 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gozzini, E.; Radice, D.; Bottari, F.; Boveri, S.; Guerrieri, M.E.; Preti, E.P.; Spolti, N.; Ghioni, M.; Ferrari, F.; Iacobone, A.D. Human Papillomavirus Genotype Richness and the Biodiversity of Squamous and Glandular Cervical Dysplasias: A Cross-Sectional Study. Pathogens 2023, 12, 1234. https://doi.org/10.3390/pathogens12101234
Gozzini E, Radice D, Bottari F, Boveri S, Guerrieri ME, Preti EP, Spolti N, Ghioni M, Ferrari F, Iacobone AD. Human Papillomavirus Genotype Richness and the Biodiversity of Squamous and Glandular Cervical Dysplasias: A Cross-Sectional Study. Pathogens. 2023; 12(10):1234. https://doi.org/10.3390/pathogens12101234
Chicago/Turabian StyleGozzini, Elisa, Davide Radice, Fabio Bottari, Sara Boveri, Maria Elena Guerrieri, Eleonora Petra Preti, Noemi Spolti, Mariacristina Ghioni, Federico Ferrari, and Anna Daniela Iacobone. 2023. "Human Papillomavirus Genotype Richness and the Biodiversity of Squamous and Glandular Cervical Dysplasias: A Cross-Sectional Study" Pathogens 12, no. 10: 1234. https://doi.org/10.3390/pathogens12101234