
A Case of Gastroallergic and Intestinal Anisakiasis in Italy: Diagnosis Based on Double Endoscopy and Molecular Identification
 , , , , and
, , , , and 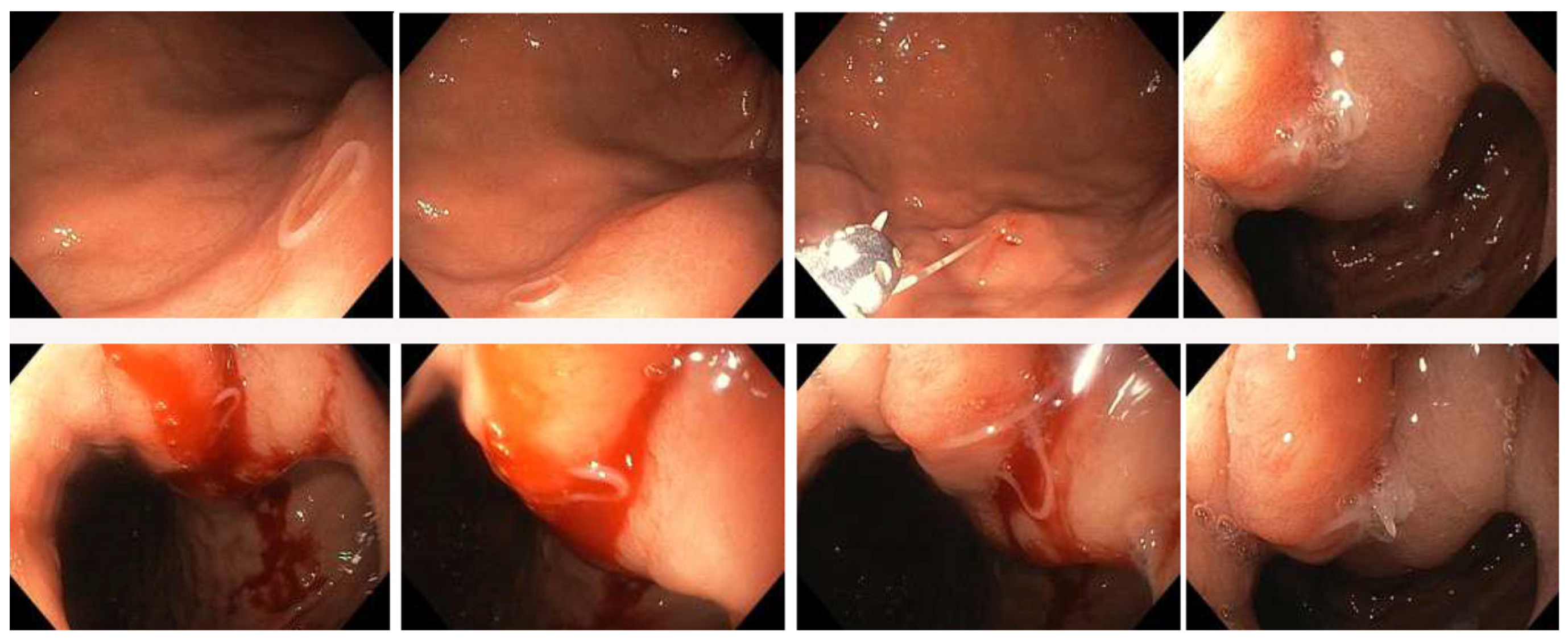{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
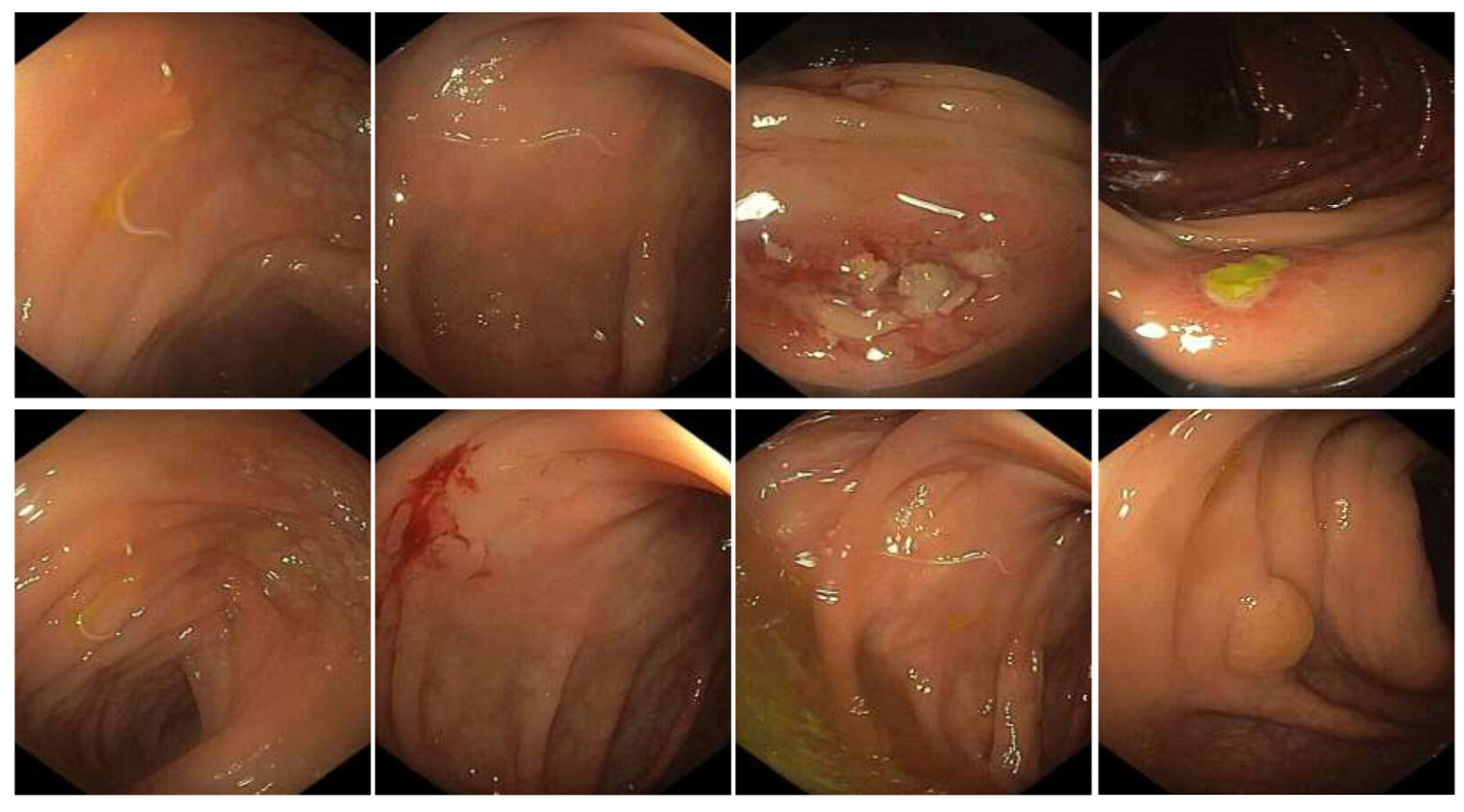
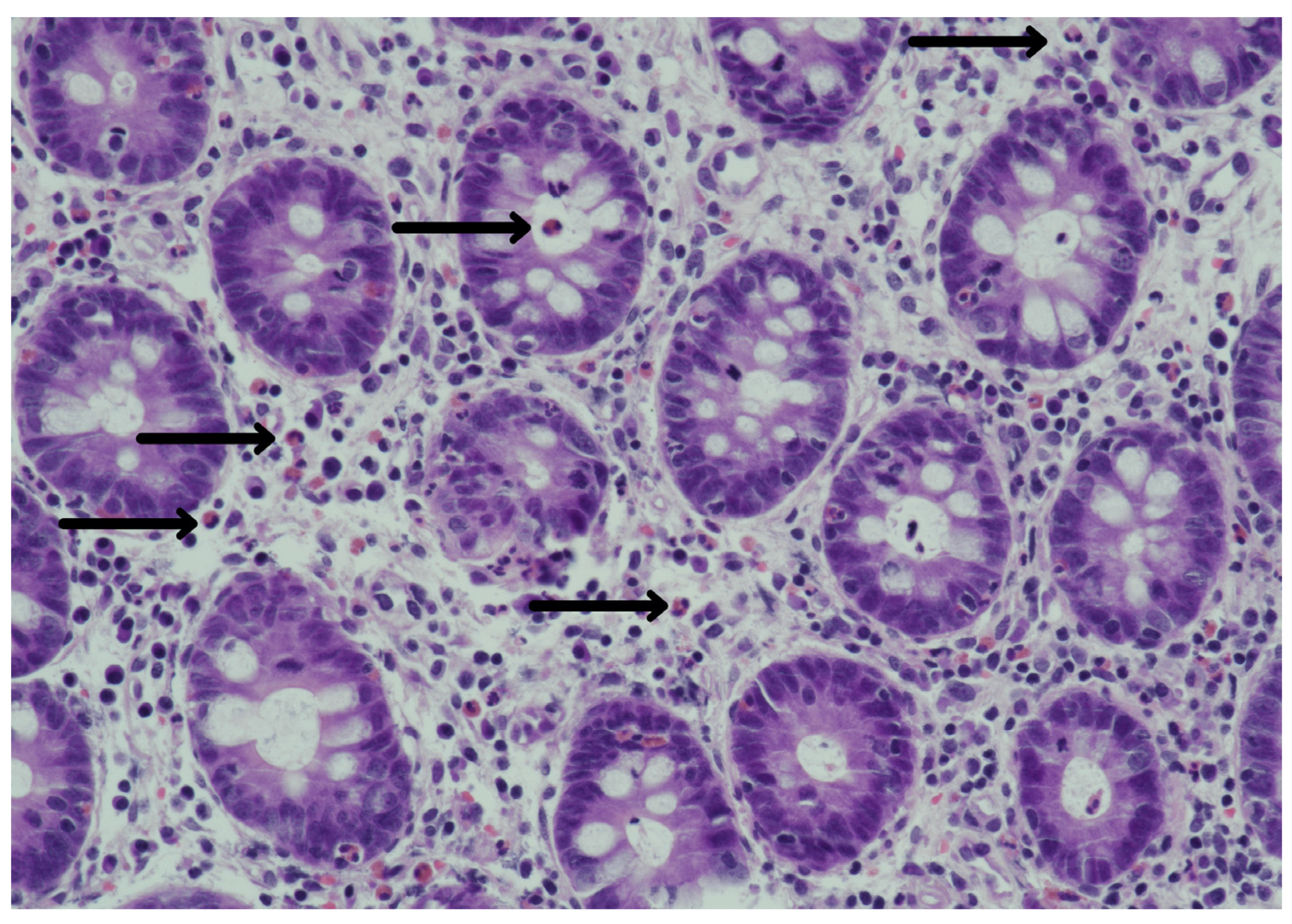
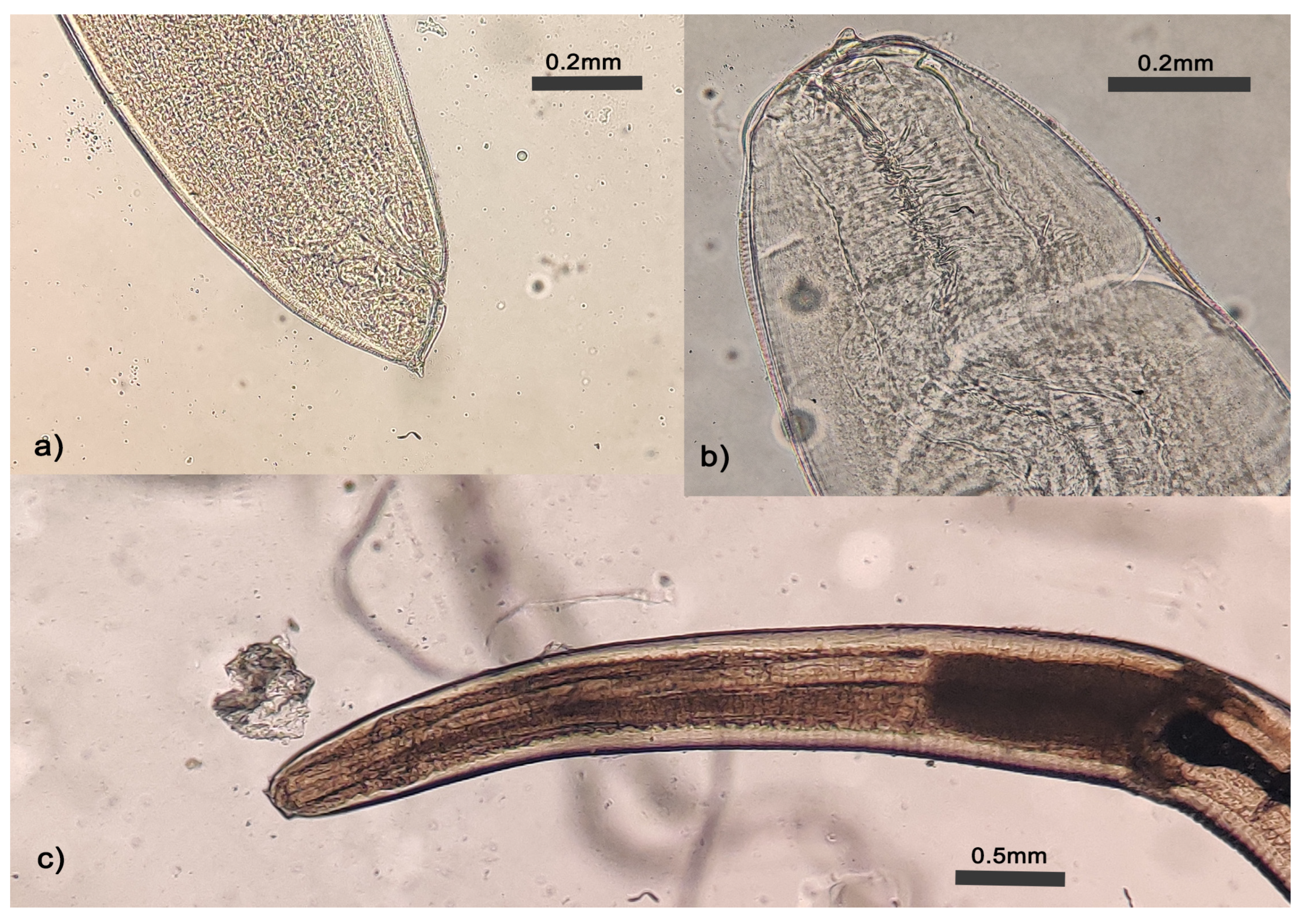
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Panel EFSA. On biological hazards (BIOHAZ) scientific opinion on risk assessment of parasites in fishery products. EFSA J. 2010, 8, 1543. [Google Scholar]
- Audicana, M.T.; Ansotegui, I.J.; de Corres, L.F.; Kennedy, M.W. Anisakis simplex: Dangerous—Dead and alive? Trends Parasitol. 2002, 18, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Nogami, Y.; Fujii-Nishimura, Y.; Banno, K.; Suzuki, A.; Susumu, N.; Hibi, T.; Murakami, K.; Yamada, T.; Sugiyama, H.; Morishima, Y.; et al. Anisakiasis mimics cancer recurrence: Two cases of extragastrointestinal anisakiasis suspected to be recurrence of gynecological cancer on PET-CT and molecular biological investigation. BMC Med. Imaging 2016, 16, 31. [Google Scholar] [CrossRef] [PubMed]
- Mattiucci, S.; Palomba, M.; Cavallero, S.; D’Amelio, S. Anisakiasis. In Helminth Infections and Their Impact on Global Public Health; Bruschi, F., Ed.; Springer: Cham, Switzerland, 2022. [Google Scholar] [CrossRef]
- Sugiyama, H.; Shiroyama, M.; Yamamoto, I.; Ishikawa, T.; Morishima, Y. Anisakiasis Annual Incidence and Causative Species, Japan, 2018–2019. Emerg. Infect. Dis. 2022, 28, 2105–2108. [Google Scholar] [CrossRef]
- Shamsi, S.; Barton, D.P. A critical review of anisakidosis cases occurring globally. Parasitol. Res. 2023, 122, 1733–1745. [Google Scholar] [CrossRef]
- Cavallero, S.; Martini, A.; Migliara, G.; De Vito, C.; Iavicoli, S.; D’Amelio, S. Anisakiasis in Italy: Analysis of hospital discharge records in the years 2005–2015. PLoS ONE 2018, 13, e0208772. [Google Scholar] [CrossRef]
- D’Amelio, S.; Mathiopoulos, K.D.; Santos, C.P.; Pugachev, O.N.; Webb, S.C.; Picanço, M.; Paggi, L. Genetic markers in ribosomal DNA for the identification of members of the genus Anisakis (Nematoda: Ascaridoidea) defined by polymerase-chain-reaction-based restriction fragment length polymorphism. Int. J. Parasitol. 2000, 25, 21. [Google Scholar] [CrossRef]
- Stallone, O.; Paggi, L.; Balestrazzi, A.; Mattiucci, S.; Montinari, M. Gastric Anisakiasis in Italy: Case report. Mediterr. J. Surg. Med. 1996, 4, 13–16. [Google Scholar]
- Guardone, L.; Armani, A.; Nucera, D.; Costanzo, F.; Mattiucci, S.; Bruschi, F. Human anisakiasis in Italy: A retrospective epidemiological study over two decades. Parasite 2018, 25, 41. [Google Scholar] [CrossRef]
- D’Amelio, S.; Mathiopoulos, K.D.; Brandonisio, O.; Lucarelli, G.; Doronzo, F.; Paggi, L. Diagnosis of a case of gastric anisakidosis by PCR-based restriction fragment length polymorphism analysis. Parassitologia 1999, 41, 591–593. [Google Scholar]
- Cavallero, S.; Scribano, D.; D’Amelio, S. First case report of invasive pseudoterranoviasis in Italy. Parasitol. Int. 2016, 65, 488–490. [Google Scholar] [CrossRef] [PubMed]
- Takasaki, T.; Yamada, T.; Kinoshita, J.; Motomura, Y. Asymptomatic Colonic Anisakiasis: Is It So Rare? Case Rep. Gastroenterol. 2020, 14, 593–597. [Google Scholar] [CrossRef] [PubMed]
- Fornell Pérez, R.; Urizar Gorosarri, M.; Pérez Bea, M. Anisakiasis: Imaging findings. Radiol. Engl. Ed. 2022, 64, 245–255. [Google Scholar] [CrossRef]
- Daschner, A.; Alonso-Gómez, A.; Cabañas, R.; Suarez-de-Parga, J.M.; López-Serrano, M.C. Gastroallergic anisakiasis: Borderline between food allergy and parasitic disease-clinical and allergologic evaluation of 20 patients with confirmed acute parasitism by Anisakis simplex. J. Allergy Clin. Immunol. 2000, 105, 176–181. [Google Scholar] [CrossRef]
- Kim, T.; Song, H.J.; Jeong, S.U.; Choi, E.K.; Cho, Y.K.; Kim, H.U.; Song, B.C.; Kim, K.S.; Kim, B.S.; Kim, Y.R. Comparison of the clinical characteristics of patients with small bowel and gastric anisakiasis in jeju island. Gut Liver. 2013, 7, 23–29. [Google Scholar] [CrossRef]
- Iwasaki, K.; Torisu, M. Anisakis and eosinophil. Clin. Immunol. Immunopathol. 1982, 23, 593–605. [Google Scholar] [CrossRef] [PubMed]
- Ishikura, H.; Namiki, M. Gastric Anisakiasis in Japan: Epidemiology, Diagnosis, Treatment; Springer Science & Business Media: Berlin, Germany, 2012. [Google Scholar]
- Kang, D.B.; Park, W.C.; Lee, J.K. Chronic gastric anisakiasis provoking a bleeding gastric ulcer. Ann. Surg. Treat. Res. 2014, 86, 270–273. [Google Scholar] [CrossRef]
- Takeuchi, K.; Hanai, H.; Iida, T.; Suzuki, S.; Isobe, S. A bleeding gastric ulcer on a vanishing tumor caused by anisakiasis. Gastrointest. Endosc. 2000, 52, 549–551. [Google Scholar] [CrossRef]
- Lash, R.H.; Genta, R.M.; Schuler, C.M. Sessile serrated adenomas: Prevalence of dysplasia and carcinoma in 2139 patients. J. Clin. Pathol. 2010, 63, 681–686. [Google Scholar] [CrossRef]
- Hochberg, N.S.; Hamer, D.H.; Hughes, J.M.; Wilson, M.E. Anisakidosis: Perils of the Deep. Clin. Infect. Dis. 2010, 51, 806–812. [Google Scholar] [CrossRef]
- Garcia-Perez, J.C.; Rodríguez-Perez, R.; Ballestero, A.; Zuloaga, J.; Fernandez-Puntero, B.; Arias-Díaz, J.; Caballero, M.L. Previous Exposure to the Fish Parasite Anisakis as a Potential Risk Factor for Gastric or Colon Adenocarcinoma. Medicine 2015, 94, e1699. [Google Scholar] [CrossRef] [PubMed]
- Hiramatsu, K.; Kamiyamamoto, S.; Ogino, H.; Satomura, Y.; Konishi, K.; Miwa, A.; Demachi, H.; Noda, Y. A Case of Acute Gastric Anisakiasis Presenting with Malignant Tumor-like Features: A Large Gastric Vanishing Tumor Accompanied by Local Lymph Node Swelling. Dig. Dis. Sci. 2004, 49, 965–969. [Google Scholar] [CrossRef] [PubMed]
- Sonoda, H.; Yamamoto, K.; Ozeki, K.; Inoye, H.; Toda, S.; Maehara, Y. An Anisakis larva attached to early gastric cancer: Report of a case. Surg. Today 2015, 45, 1321–1325. [Google Scholar] [CrossRef] [PubMed]
- Mineta, S.; Shimanuki, K.; Sugiura, A.; Tsuchiya, Y.; Kaneko, M.; Sugiyama, Y.; Akimaru, K.; Tajiri, T. Chronic anisakiasis of the ascending colon associated with carcinoma. J. Nippon. Med. Sch. 2006, 73, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, D.A.; Chambers, H.F.; Saag, M.S. The Sanford Guide to Antimicrobial Therapy 2023; Antimicrobial Therapy, Inc.: Sperryville, VA, USA, 2023. [Google Scholar]
- World Health Organization. WHO Model Prescribing Information: Drugs Used in Parasitic Diseases; World Health Organization: Geneva, Switzerland, 1995; 150p. [Google Scholar]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Amelio, S.; Bellini, I.; Chiovoloni, C.; Magliocco, C.; Pronio, A.; Di Rocco, A.; Pentassuglio, I.; Rosati, M.; Russo, G.; Cavallero, S. A Case of Gastroallergic and Intestinal Anisakiasis in Italy: Diagnosis Based on Double Endoscopy and Molecular Identification. Pathogens 2023, 12, 1172. https://doi.org/10.3390/pathogens12091172
D’Amelio S, Bellini I, Chiovoloni C, Magliocco C, Pronio A, Di Rocco A, Pentassuglio I, Rosati M, Russo G, Cavallero S. A Case of Gastroallergic and Intestinal Anisakiasis in Italy: Diagnosis Based on Double Endoscopy and Molecular Identification. Pathogens. 2023; 12(9):1172. https://doi.org/10.3390/pathogens12091172
Chicago/Turabian StyleD’Amelio, Stefano, Ilaria Bellini, Claudia Chiovoloni, Cristina Magliocco, Annamaria Pronio, Arianna Di Rocco, Ilaria Pentassuglio, Marco Rosati, Gianluca Russo, and Serena Cavallero. 2023. "A Case of Gastroallergic and Intestinal Anisakiasis in Italy: Diagnosis Based on Double Endoscopy and Molecular Identification" Pathogens 12, no. 9: 1172. https://doi.org/10.3390/pathogens12091172