
Antibacterial and Anti-Biofilm Properties of Diopside Powder Loaded with Lysostaphin
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Production and Purification of Lysostaphin
2.2. Diopside Synthesis and Characterization
2.3. Loading of Diopside with Lysostaphin
2.4. Release of Lysostaphin from Diopside
2.5. ELISA
2.6. Determination of Minimum Inhibitory Concentration (MIC) and Minimum Bactericidal Concentration (MBC)
2.7. Determination of Activity of Lysostaphin Released from Diopside
2.8. Cultivation of Biofilms
2.9. Determination of Anti-Biofilm Activity of Diopside Loaded with Lysostaphin
2.10. Statistical Analysis
3. Results
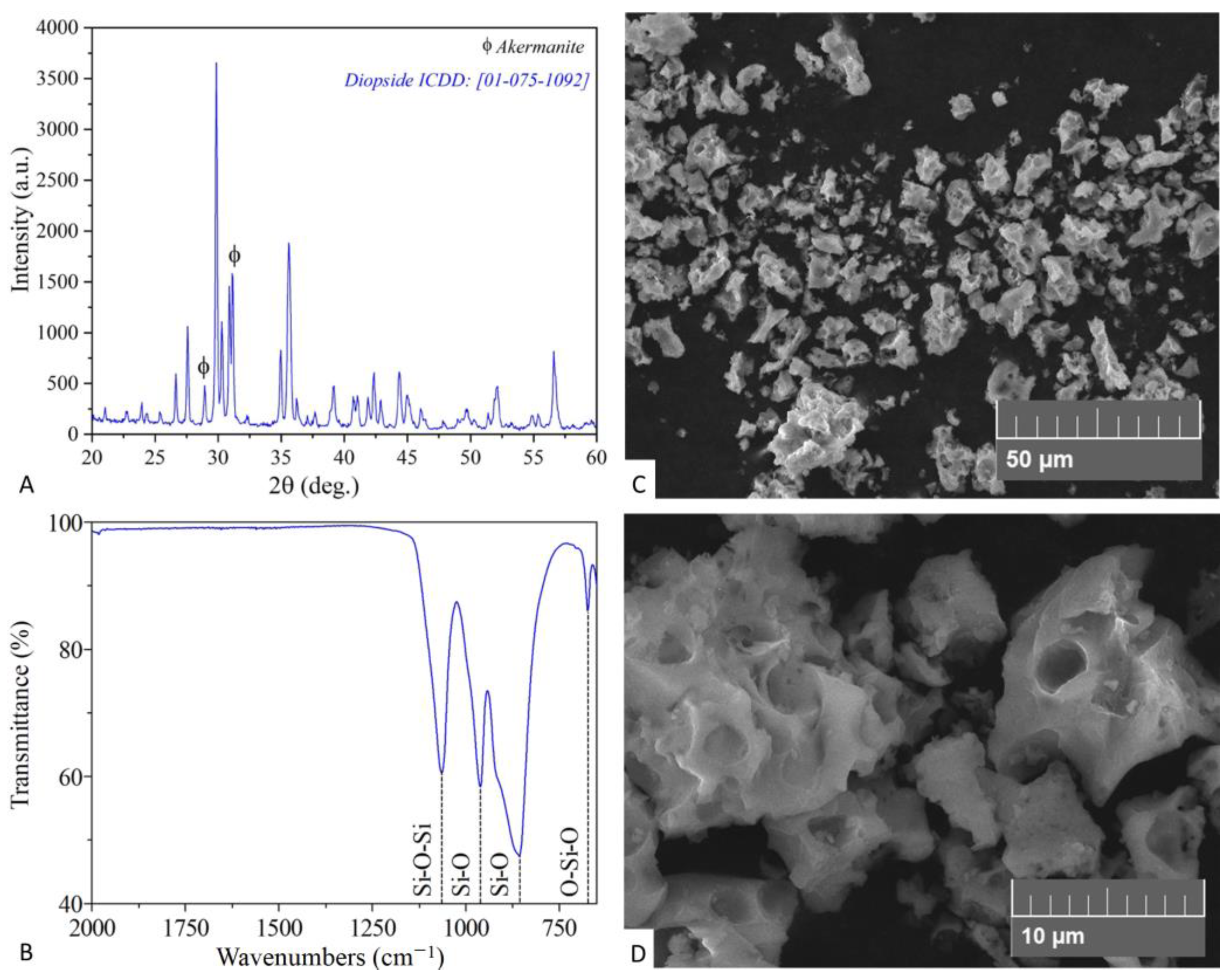
3.1. Characterization of Diopside Powder
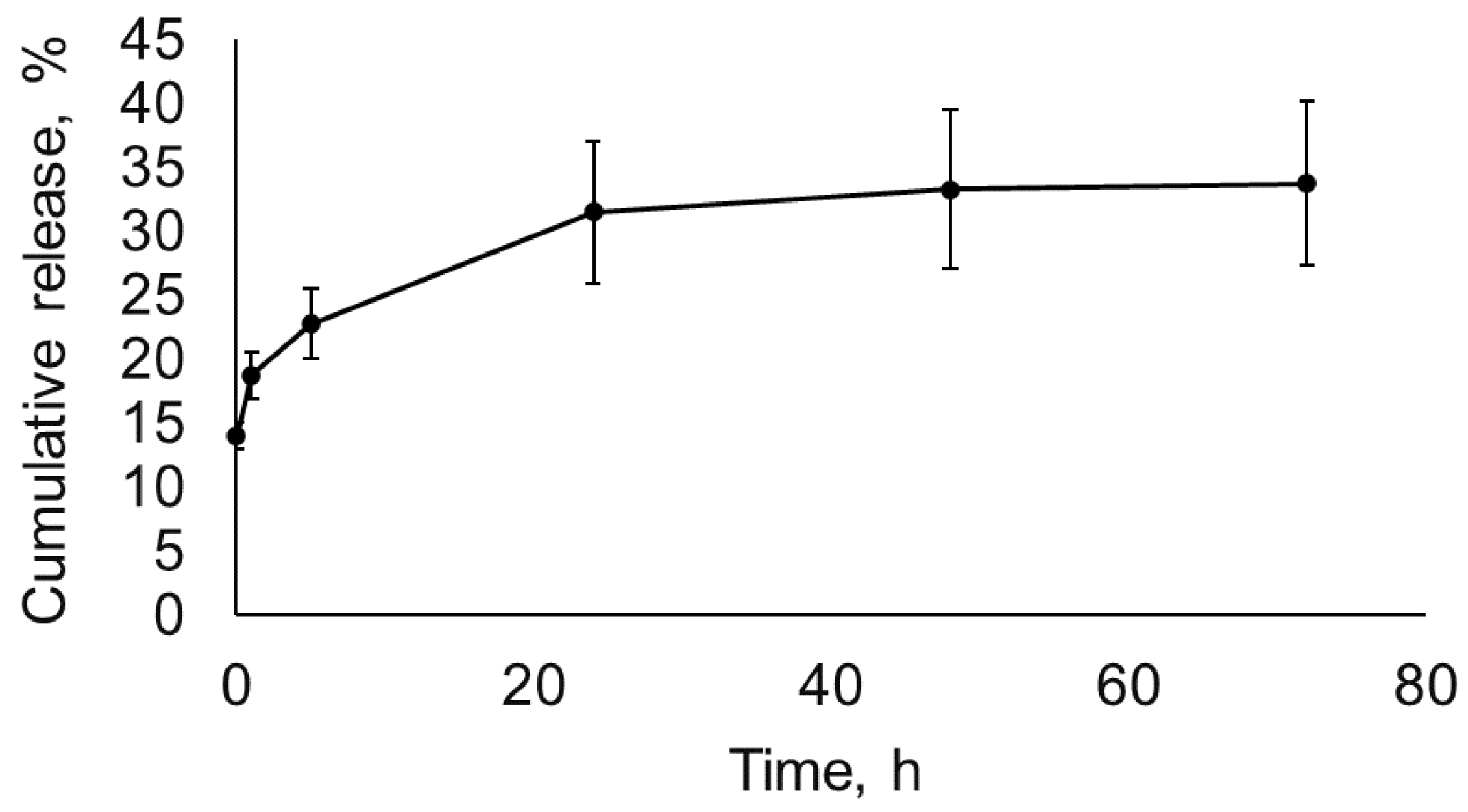
3.2. Lysostaphin Adsorption to and Release from Diopside
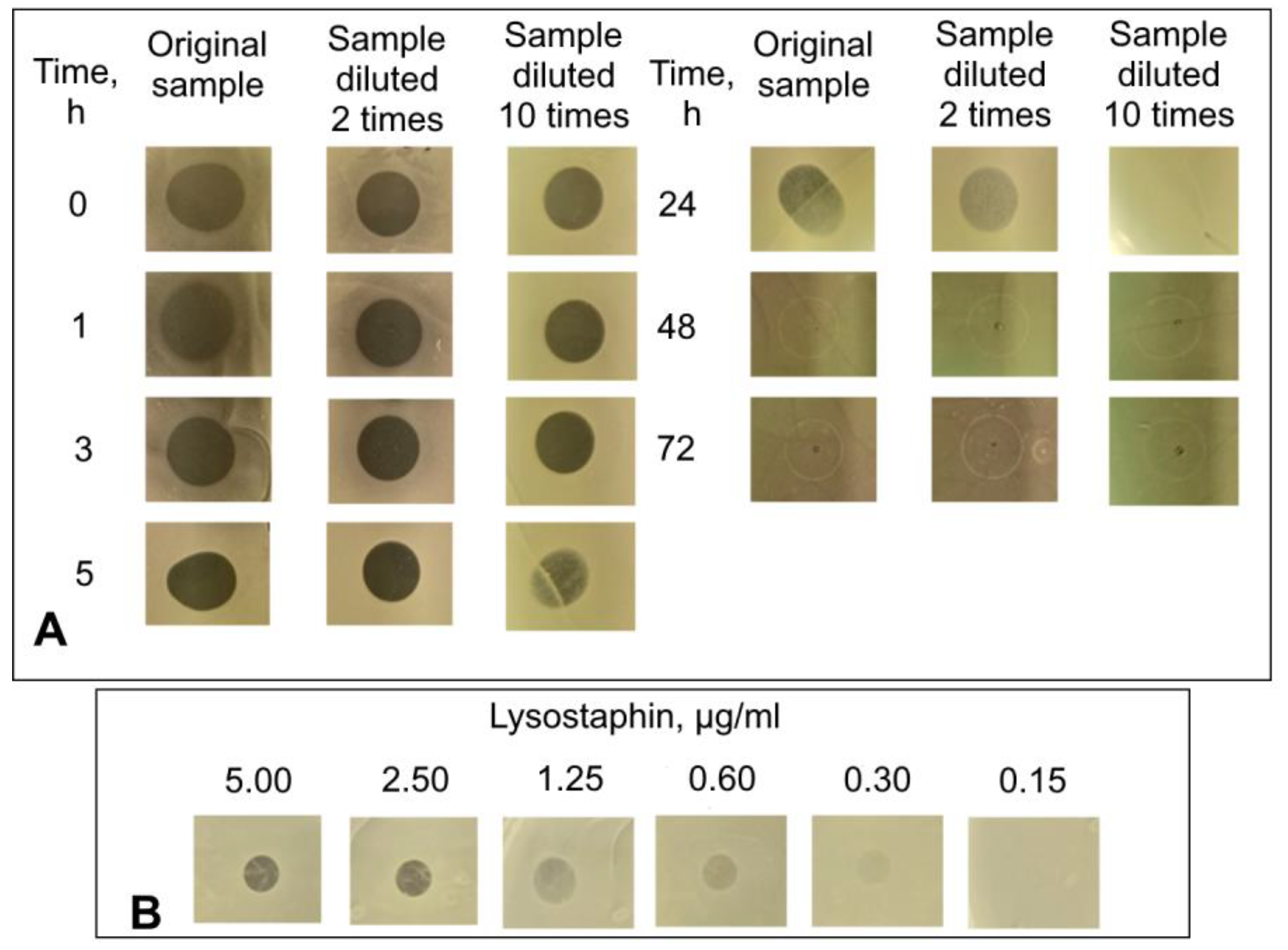
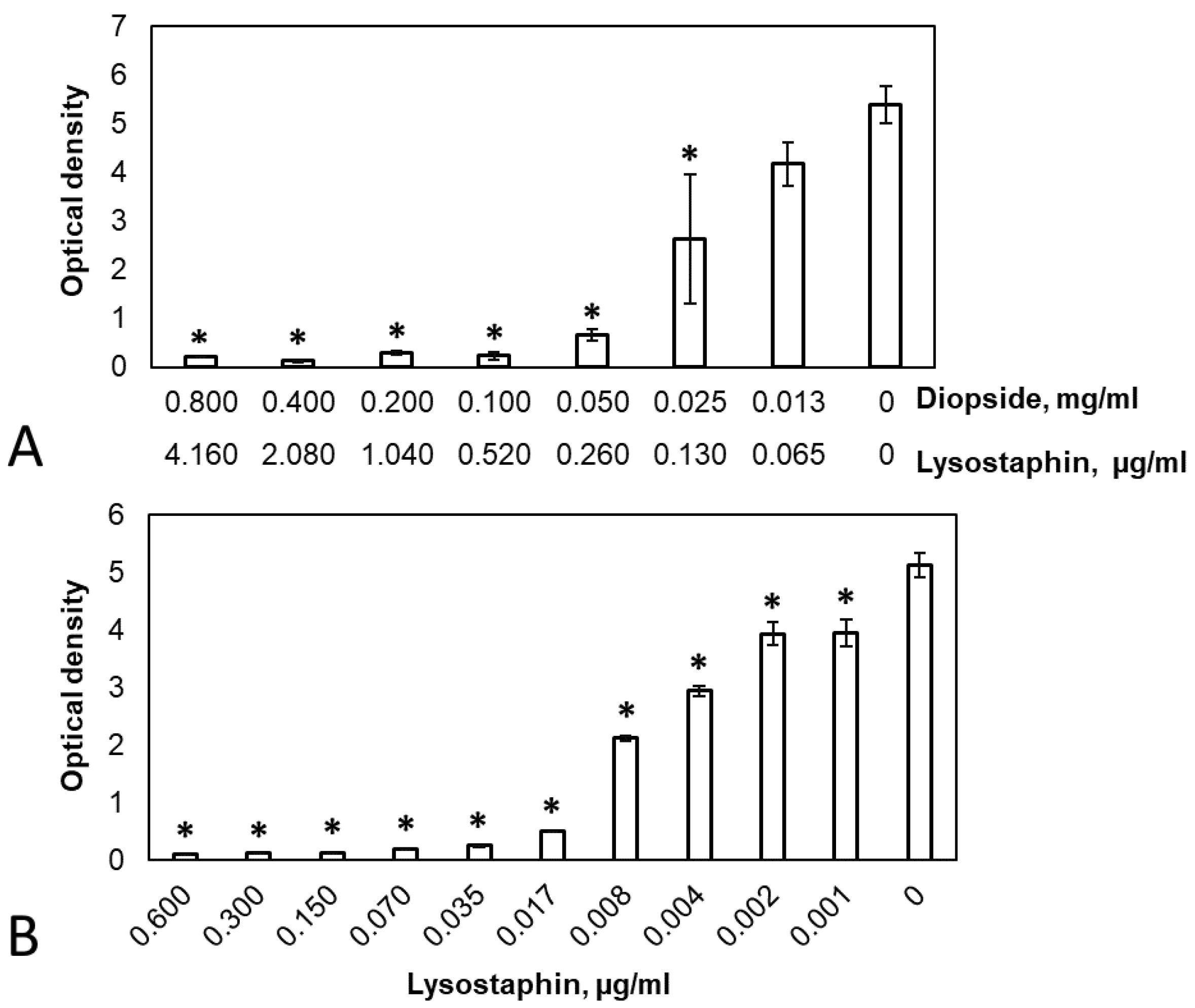
3.3. Antibacterial and Anti-Biofilm Activity of Diopside Loaded with Lysostaphin
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Palmer, M.P.; Altman, D.T.; Altman, G.T.; Sewecke, J.J.; Ehrlich, G.D.; Hu, F.Z.; Nistico, L.; Melton-Kreft, R.; Gause, T.M.; Costerton, J.W. Can We Trust Intraoperative Culture Results in Nonunions? J. Orthop. Trauma 2014, 28, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Urish, K.L.; Cassat, J.E. Staphylococcus aureus Osteomyelitis: Bone, Bugs, and Surgery. Infect. Immun. 2020, 88, e00932-19. [Google Scholar] [CrossRef] [PubMed]
- Darouiche, R.O. Treatment of Infections Associated with Surgical Implants. N. Engl. J. Med. 2004, 350, 1422–1429. [Google Scholar] [CrossRef] [PubMed]
- Tice, A.D.; Hoaglund, P.A.; Shoultz, D.A. Outcomes of Osteomyelitis among Patients Treated with Outpatient Parenteral Antimicrobial Therapy. Am. J. Med. 2003, 114, 723–728. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A.; Berendt, A.R.; Deery, H.G.; Embil, J.M.; Joseph, W.S.; Karchmer, A.W.; LeFrock, J.L.; Lew, D.P.; Mader, J.T.; Norden, C.; et al. Diagnosis and Treatment of Diabetic Foot Infections. Plast. Reconstr. Surg. 2006, 117, 212S–238S. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, E.M.; Parvizi, J.; Gehrke, T.; Aiyer, A.; Battenberg, A.; Brown, S.A.; Callaghan, J.J.; Citak, M.; Egol, K.; Garrigues, G.E.; et al. 2018 International Consensus Meeting on Musculoskeletal Infection: Research Priorities from the General Assembly Questions. J. Orthop. Res. 2019, 37, 997–1006. [Google Scholar] [CrossRef]
- Sancineto, C.F.; Barla, J.D. Treatment of Long Bone Osteomyelitis With a Mechanically Stable Intramedullar Antibiotic Dispenser: Nineteen Consecutive Cases with a Minimum of 12 Months Follow-Up. J. Trauma Inj. Infect. Crit. Care 2008, 65, 1416–1420. [Google Scholar] [CrossRef]
- Hutson, J.J.; Dayicioglu, D.; Oeltjen, J.C.; Panthaki, Z.J.; Armstrong, M.B. The Treatment of Gustilo Grade IIIB Tibia Fractures with Application of Antibiotic Spacer, Flap, and Sequential Distraction Osteogenesis. Ann. Plast. Surg. 2010, 64, 541–552. [Google Scholar] [CrossRef]
- Back, D.A.; Bormann, N.; Calafi, A.; Zech, J.; Garbe, L.A.; Müller, M.; Willy, C.; Schmidmaier, G.; Wildemann, B. Testing of antibiotic releasing implant coatings to fight bacteria in combat-associated osteomyelitis—An in-vitro study. Int. Orthop. 2016, 40, 1039–1047. [Google Scholar] [CrossRef]
- Qin, C.; Xu, L.; Liao, J.; Fang, J.; Hu, Y. Management of Osteomyelitis-Induced Massive Tibial Bone Defect by Monolateral External Fixator Combined with Antibiotics-Impregnated Calcium Sulphate: A Retrospective Study. BioMed Res. Int. 2018, 2018, 9070216. [Google Scholar] [CrossRef]
- Guo, Y.; Song, G.; Sun, M.; Wang, J.; Wang, Y. Prevalence and Therapies of Antibiotic-Resistance in Staphylococcus aureus. Front. Cell. Infect. Microbiol. 2020, 10, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qvortrup, K.; Hultqvist, L.D.; Nilsson, M.; Jakobsen, T.H.; Jansen, C.U.; Uhd, J.; Andersen, J.B.; Nielsen, T.E.; Givskov, M.; Tolker-Nielsen, T. Small Molecule Anti-Biofilm Agents Developed on the Basis of Mechanistic Understanding of Biofilm Formation. Front. Chem. 2019, 7, 742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastos, M.D.C.D.F.; Coutinho, B.G.; Coelho, M.L.V. Lysostaphin: A Staphylococcal Bacteriolysin with Potential Clinical Applications. Pharmaceuticals 2010, 3, 1139–1161. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.A.; Kusuma, C.; Mond, J.J.; Kokai-Kun, J.F. Lysostaphin Disrupts Staphylococcus aureus and Staphylococcus Epidermidis Biofilms on Artificial Surfaces. Antimicrob. Agents Chemother. 2003, 47, 3407–3414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kusuma, C.M.; Kokai-Kun, J.F. Comparison of Four Methods for Determining Lysostaphin Susceptibility of Various Strains of Staphylococcus aureus. Antimicrob. Agents Chemother. 2005, 49, 3256–3263. [Google Scholar] [CrossRef] [Green Version]
- Wittekind, M.; Schuch, R. Cell Wall Hydrolases and Antibiotics: Exploiting Synergy to Create Efficacious New Antimicrobial Treatments. Curr. Opin. Microbiol. 2016, 33, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Windolf, C.D.; Lögters, T.; Scholz, M.; Windolf, J.; Flohé, S. Lysostaphin-Coated Titan-Implants Preventing Localized Osteitis by Staphylococcus aureus in a Mouse Model. PLoS ONE 2014, 9, e115940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, C.T.; Wroe, J.A.; Agarwal, R.; Martin, K.E.; Guldberg, R.E.; Donlan, R.M.; Westblade, L.F.; García, A.J. Hydrogel Delivery of Lysostaphin Eliminates Orthopedic Implant Infection by Staphylococcus aureus and Supports Fracture Healing. Proc. Natl. Acad. Sci. USA 2018, 115, E4960–E4969. [Google Scholar] [CrossRef] [Green Version]
- Johnson, C.T.; Sok, M.C.P.; Martin, K.E.; Kalelkar, P.P.; Caplin, J.D.; Botchwey, E.A.; García, A.J. Lysostaphin and BMP-2 Co-Delivery Reduces S. aureus Infection and Regenerates Critical-Sized Segmental Bone Defects. Sci. Adv. 2019, 5, eaaw1228. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.; Zhou, C.; Hong, Y.; Zhang, X. A Review of Protein Adsorption on Bioceramics. Interface Focus 2012, 2, 259–277. [Google Scholar] [CrossRef]
- Fosca, M.; Rau, J.V.; Uskoković, V. Factors Influencing the Drug Release from Calcium Phosphate Cements. Bioact. Mater. 2022, 7, 341–363. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, R.; Venkatraman, S.K.; Chatterjee, A.; Vecstaudza, J.; Yáñez-Gascón, M.J.; Pérez-Sánchez, H.; Locs, J.; Abraham, J.; Swamiappan, S. Biomineralization, Antibacterial Activity and Mechanical Properties of Biowaste Derived Diopside Nanopowders. Adv. Powder Technol. 2019, 30, 1950–1964. [Google Scholar] [CrossRef]
- Wu, C.; Chang, J. A Review of Bioactive Silicate Ceramics. Biomed. Mater. 2013, 8, 032001. [Google Scholar] [CrossRef]
- Wu, C.; Chang, J. Degradation, Bioactivity, and Cytocompatibility of Diopside, Akermanite, and Bredigite Ceramics. J. Biomed. Mater. Res. B Appl. Biomater. 2007, 83B, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Ramaswamy, Y.; Zreiqat, H. Porous Diopside (CaMgSi2O6) Scaffold: A Promising Bioactive Material for Bone Tissue Engineering. Acta Biomater. 2010, 6, 2237–2245. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Li, J.; Liu, X.; Wei, L.; Wang, G.; Meng, F. Proliferation and Gene Expression of Osteoblasts Cultured in DMEM Containing the Ionic Products of Dicalcium Silicate Coating. Biomed. Pharmacother. 2009, 63, 650–657. [Google Scholar] [CrossRef]
- Karyagina, A.S.; Boksha, I.S.; Grunina, T.M.; Demidenko, A.V.; Poponova, M.S.; Sergienko, O.V.; Lyashchuk, A.M.; Galushkina, Z.M.; Soboleva, L.A.; Osidak, E.O.; et al. Two Variants of Recombinant Human Bone Morphogenetic Protein-2 (RhBMP-2) with Additional Protein Domains: Synthesis in an Escherichia Coli Heterologous Expression System. Biochemistry 2017, 82, 613–624. [Google Scholar] [CrossRef]
- Karyagina, A.; Orlova, P.; Poponova, M.; Bulygina, I.; Choudhary, R.; Zhulina, A.; Grunina, T.; Nikitin, K.; Strukova, N.; Generalova, M.; et al. Hybrid Implants Based on Calcium-Magnesium Silicate Ceramics Diopside as a Carrier of Recombinant BMP-2 and Demineralized Bone Matrix as a Scaffold: Dynamics of Reparative Osteogenesis in a Mouse Craniotomy Model. Biochemistry 2022, 87, 1277–1291. [Google Scholar] [CrossRef]
- Boksha, I.S.; Lavrova, N.V.; Grishin, A.V.; Demidenko, A.V.; Lyashchuk, A.M.; Galushkina, Z.M.; Ovchinnikov, R.S.; Umyarov, A.M.; Avetisian, L.R.; Chernukha, M.I.; et al. Staphylococcus Simulans Recombinant Lysostaphin: Production, Purification, and Determination of Antistaphylococcal Activity. Biochemistry 2016, 81, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Konstantinova, S.; Grishin, A.; Lyashchuk, A.; Vasina, I.; Karyagina, A.; Lunin, V. Influence of NaCl and PH on Lysostaphin Catalytic Activity, Cell Binding, and Bacteriolytic Activity. Appl. Microbiol. Biotechnol. 2022, 106, 6519–6534. [Google Scholar] [CrossRef]
- Grishin, A.V.; Lavrova, N.V.; Lyashchuk, A.M.; Strukova, N.V.; Generalova, M.S.; Ryazanova, A.V.; Shestak, N.V.; Boksha, I.S.; Polyakov, N.B.; Galushkina, Z.M.; et al. The Influence of Dimerization on the Pharmacokinetics and Activity of an Antibacterial Enzyme Lysostaphin. Molecules 2019, 24, 1879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grishin, A.V.; Shestak, N.V.; Lavrova, N.V.; Lyashchuk, A.M.; Popova, L.I.; Strukova, N.V.; Generalova, M.S.; Ryazanova, A.V.; Polyakov, N.B.; Galushkina, Z.M.; et al. Fusion of Lysostaphin to an Albumin Binding Domain Prolongs Its Half-Life and Bactericidal Activity in the Systemic Circulation. Molecules 2019, 24, 2892. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013; Available online: http://www.R-project.org/ (accessed on 31 October 2022).
- Venkatraman, S.K.; Choudhary, R.; Krishnamurithy, G.; Balaji Raghavendran, H.R.; Murali, M.R.; Kamarul, T.; Suresh, A.; Abraham, J.; Praharaj, S.; Swamiappan, S. Comparative Investigation on Antibacterial, Biological and Mechanical Behaviour of Monticellite and Diopside Derived from Biowaste for Bone Regeneration. Mater. Chem. Phys. 2022, 286, 126157. [Google Scholar] [CrossRef]
- Mah, T.F. Establishing the minimal bactericidal concentration of an antimicrobial agent for planktonic cells (MBC-P) and biofilm cells (MBC-B). J. Vis. Exp. 2014, 83, e50854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zirak, N.; Bolandparvaz Jahromi, A.; Salahinejad, E. Vancomycin Release Kinetics from Mg–Ca Silicate Porous Microspheres Developed for Controlled Drug Delivery. Ceram Int. 2020, 46, 508–512. [Google Scholar] [CrossRef]
- Wu, C.; Zreiqat, H. Porous Bioactive Diopside (CaMgSi2O6) Ceramic Microspheres for Drug Delivery. Acta Biomater. 2010, 6, 820–829. [Google Scholar] [CrossRef]
- Walsh, S.; Shah, A.; Mond, J. Improved Pharmacokinetics and Reduced Antibody Reactivity of Lysostaphin Conjugated to Polyethylene Glycol. Antimicrob. Agents Chemother. 2003, 47, 554–558. [Google Scholar] [CrossRef] [Green Version]
- Abdelkader, K.; Gerstmans, H.; Saafan, A.; Dishisha, T.; Briers, Y. The Preclinical and Clinical Progress of Bacteriophages and Their Lytic Enzymes: The Parts Are Easier than the Whole. Viruses 2019, 11, 96. [Google Scholar] [CrossRef] [Green Version]
- Zirak, N.; Maadani, A.M.; Salahinejad, E.; Abbasnezhad, N.; Shirinbayan, M. Fabrication, Drug Delivery Kinetics and Cell Viability Assay of PLGA-Coated Vancomycin-Loaded Silicate Porous Microspheres. Ceram. Int. 2022, 48, 48–54. [Google Scholar] [CrossRef]
- Ba, Z.; Chen, Z.; Huang, Y.; Feng, D.; Zhao, Q.; Zhu, J.; Wu, D. Nanoporous diopside modulates biocompatibility, degradability and osteogenesis of bioactive scaffolds of gliadin-based composites for new bone formation. Int. J. Nanomed. 2018, 13, 3883–3896. [Google Scholar] [CrossRef]
- Schmelcher, M.; Donovan, D.M.; Loessner, M.J. Bacteriophage Endolysins as Novel Antimicrobials. Future Microbiol. 2012, 7, 1147–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gondil, V.S.; Harjai, K.; Chhibber, S. Endolysins as Emerging Alternative Therapeutic Agents to Counter Drug-Resistant Infections. Int. J. Antimicrob. Agents 2020, 55, 105844. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lysostaphin, µg/mL | Diopside, mg/mL (In Brackets—The Respective Amount of Adsorbed Lysostaphin, µg/mL) | |
|---|---|---|
| MIC | 0.10 | 0.06 (0.31) |
| MBC | 0.10 | 0.13 (0.68) |
| CV 1 | 0.02 | 0.10 (0.52) |
| MBC-P | 0.07 | 0.20 (1.04) |
| MBC-B | 0.07 | 0.10 (0.52) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kudinova, A.; Grishin, A.; Grunina, T.; Poponova, M.; Bulygina, I.; Gromova, M.; Choudhary, R.; Senatov, F.; Karyagina, A. Antibacterial and Anti-Biofilm Properties of Diopside Powder Loaded with Lysostaphin. Pathogens 2023, 12, 177. https://doi.org/10.3390/pathogens12020177
Kudinova A, Grishin A, Grunina T, Poponova M, Bulygina I, Gromova M, Choudhary R, Senatov F, Karyagina A. Antibacterial and Anti-Biofilm Properties of Diopside Powder Loaded with Lysostaphin. Pathogens. 2023; 12(2):177. https://doi.org/10.3390/pathogens12020177
Chicago/Turabian StyleKudinova, Alina, Alexander Grishin, Tatiana Grunina, Maria Poponova, Inna Bulygina, Maria Gromova, Rajan Choudhary, Fedor Senatov, and Anna Karyagina. 2023. "Antibacterial and Anti-Biofilm Properties of Diopside Powder Loaded with Lysostaphin" Pathogens 12, no. 2: 177. https://doi.org/10.3390/pathogens12020177