Age-Dependent Changes in Resting Energy Expenditure (REE): Insights from Detailed Body Composition Analysis in Normal and Overweight Healthy Caucasians

Abstract
:1. Introduction
2. Materials and Methods
3. Results
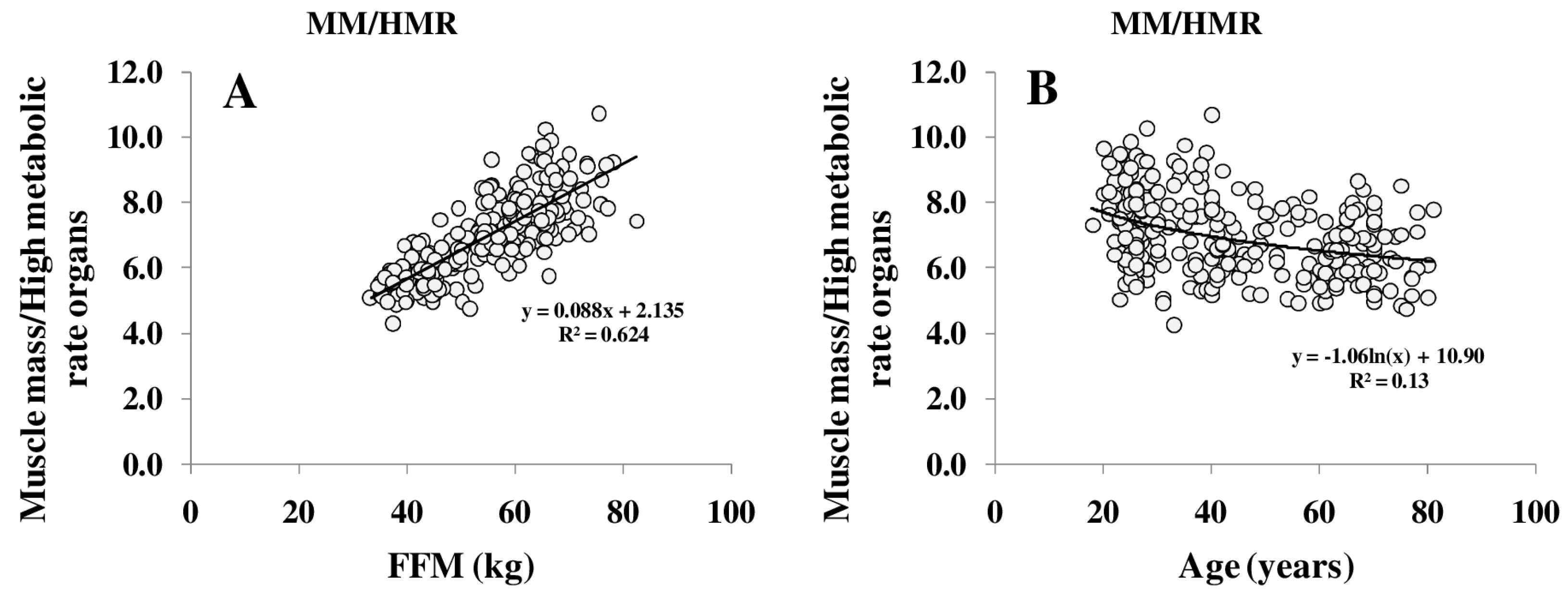
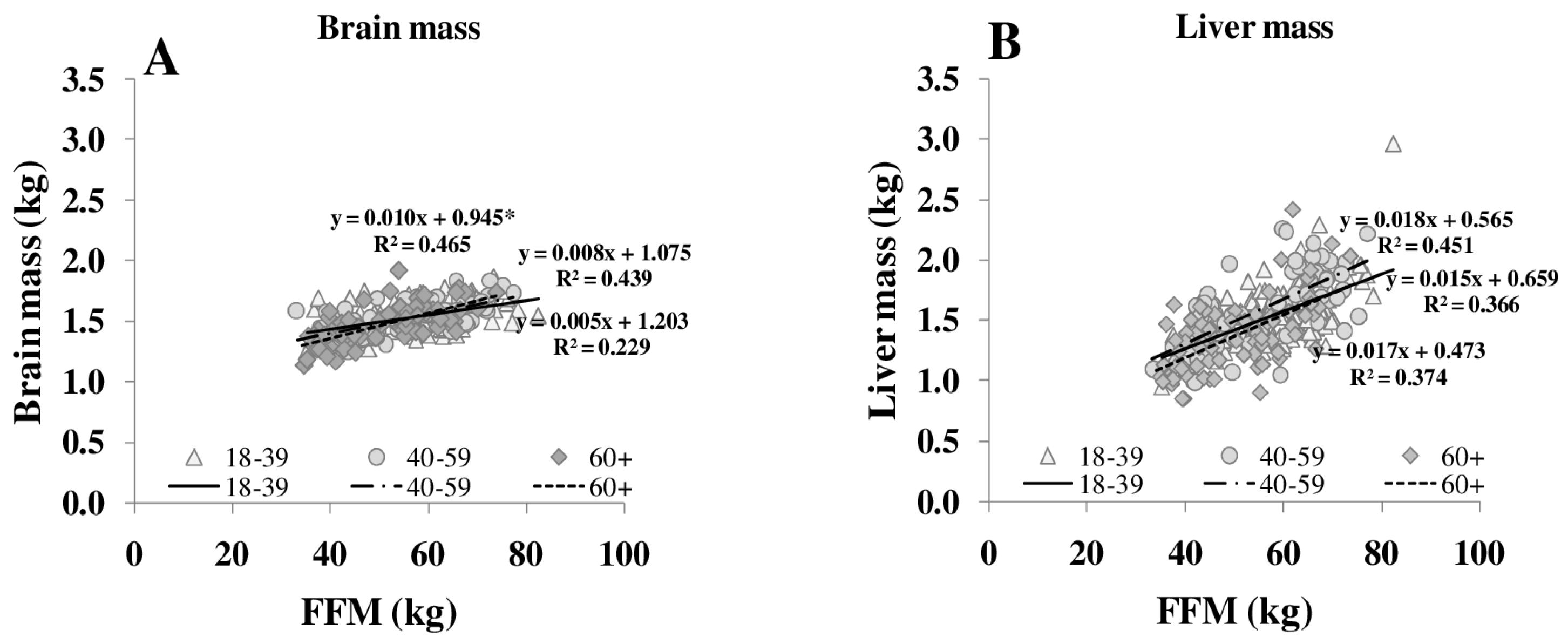
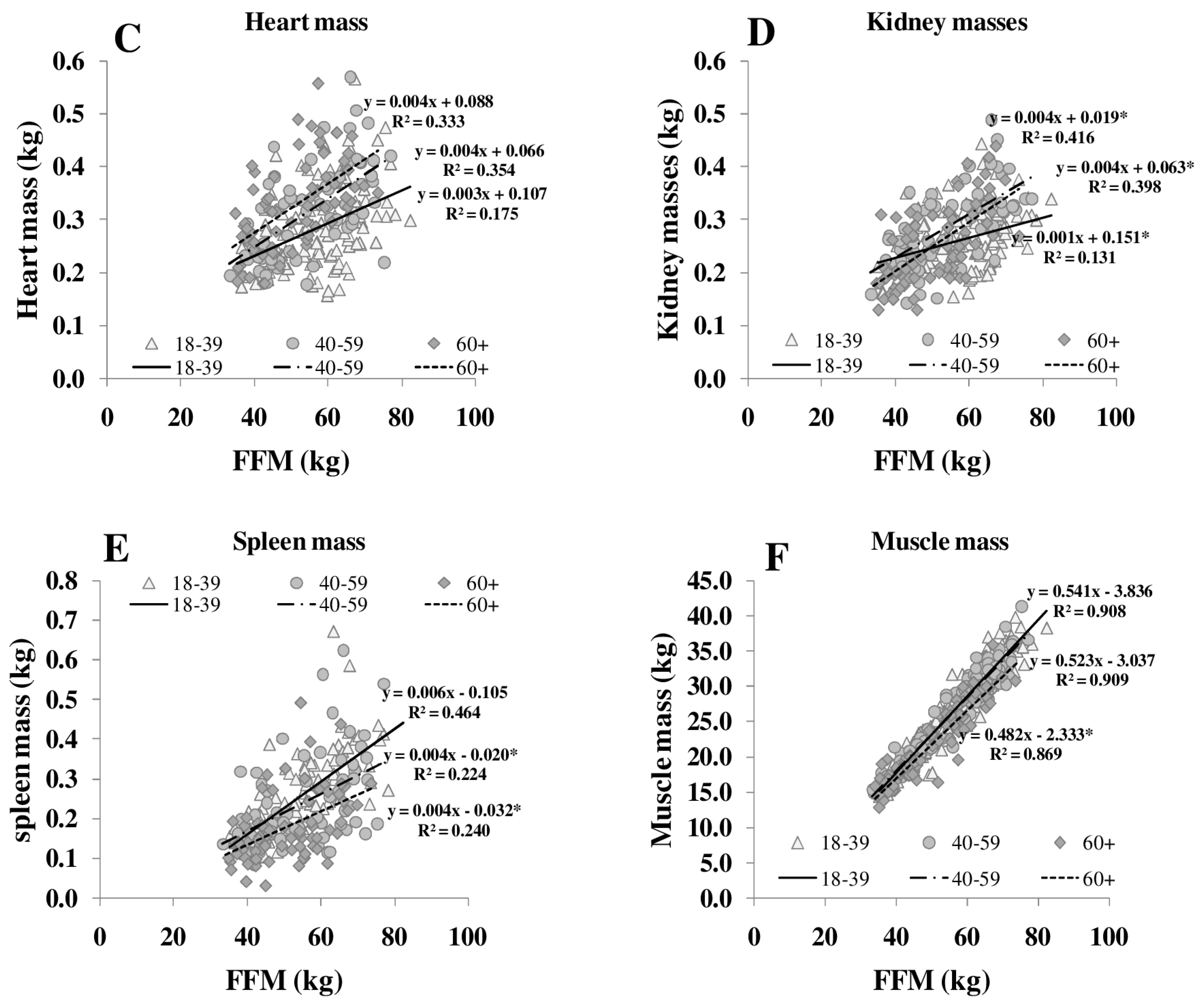
3.1. Body Composition
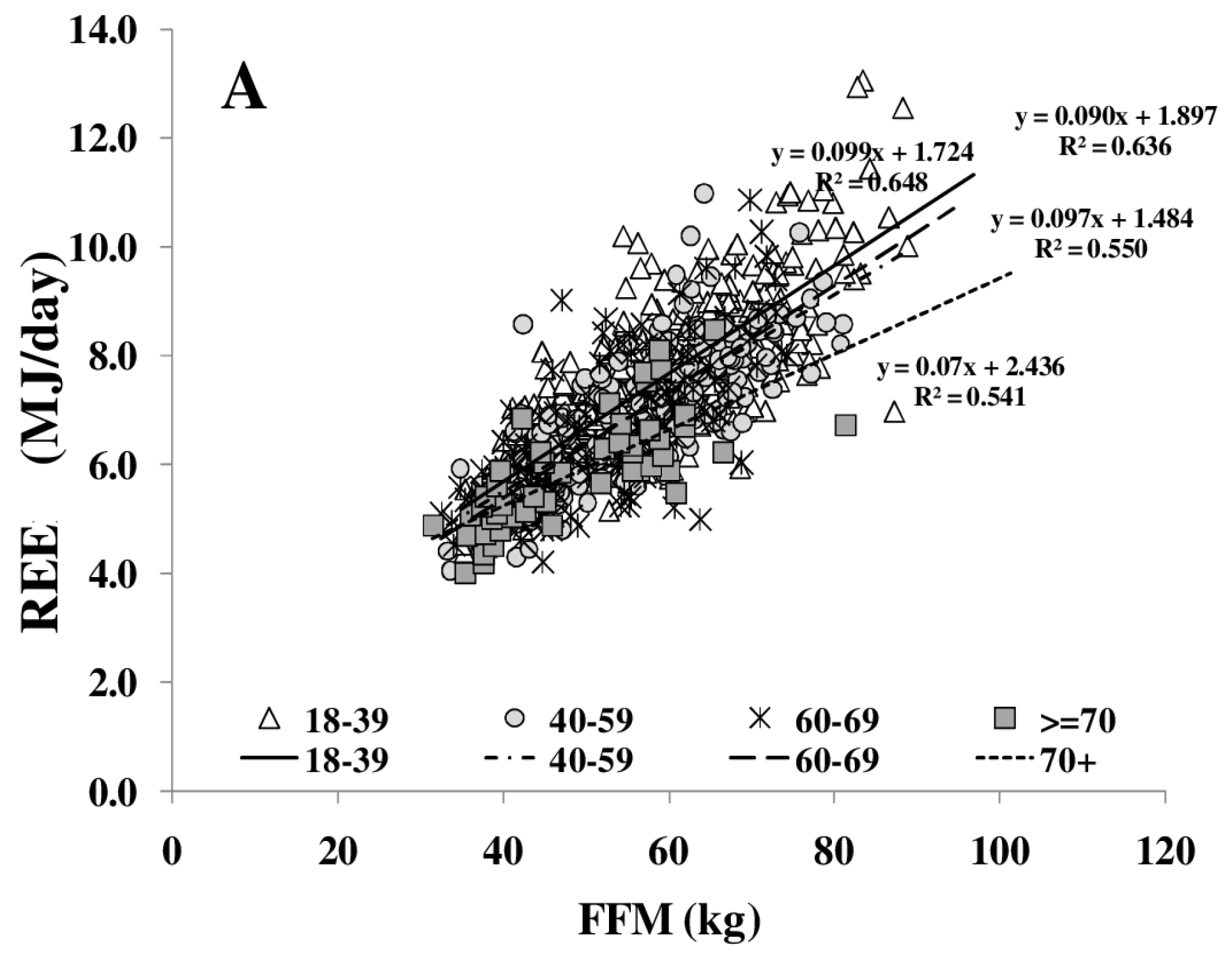
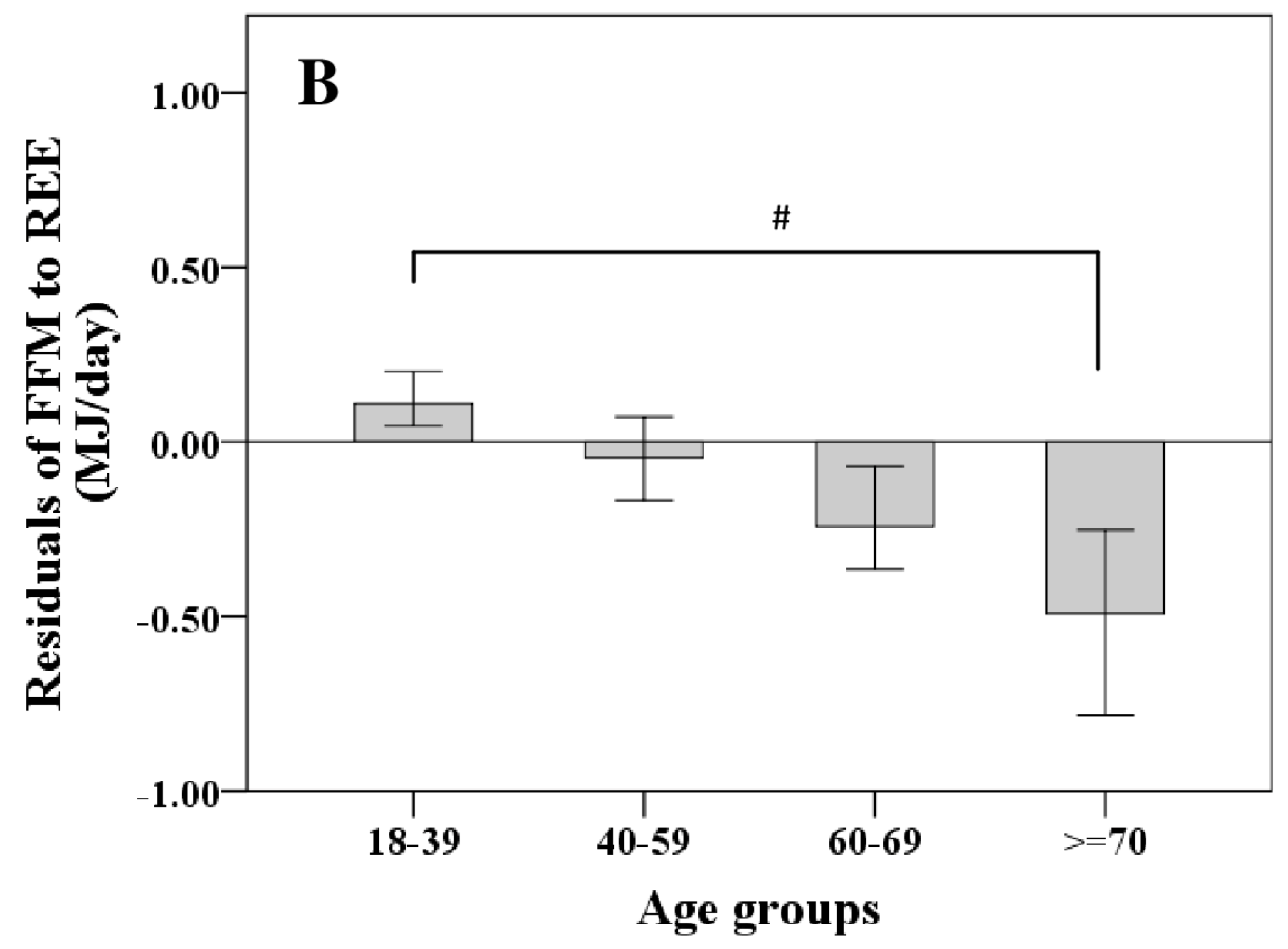
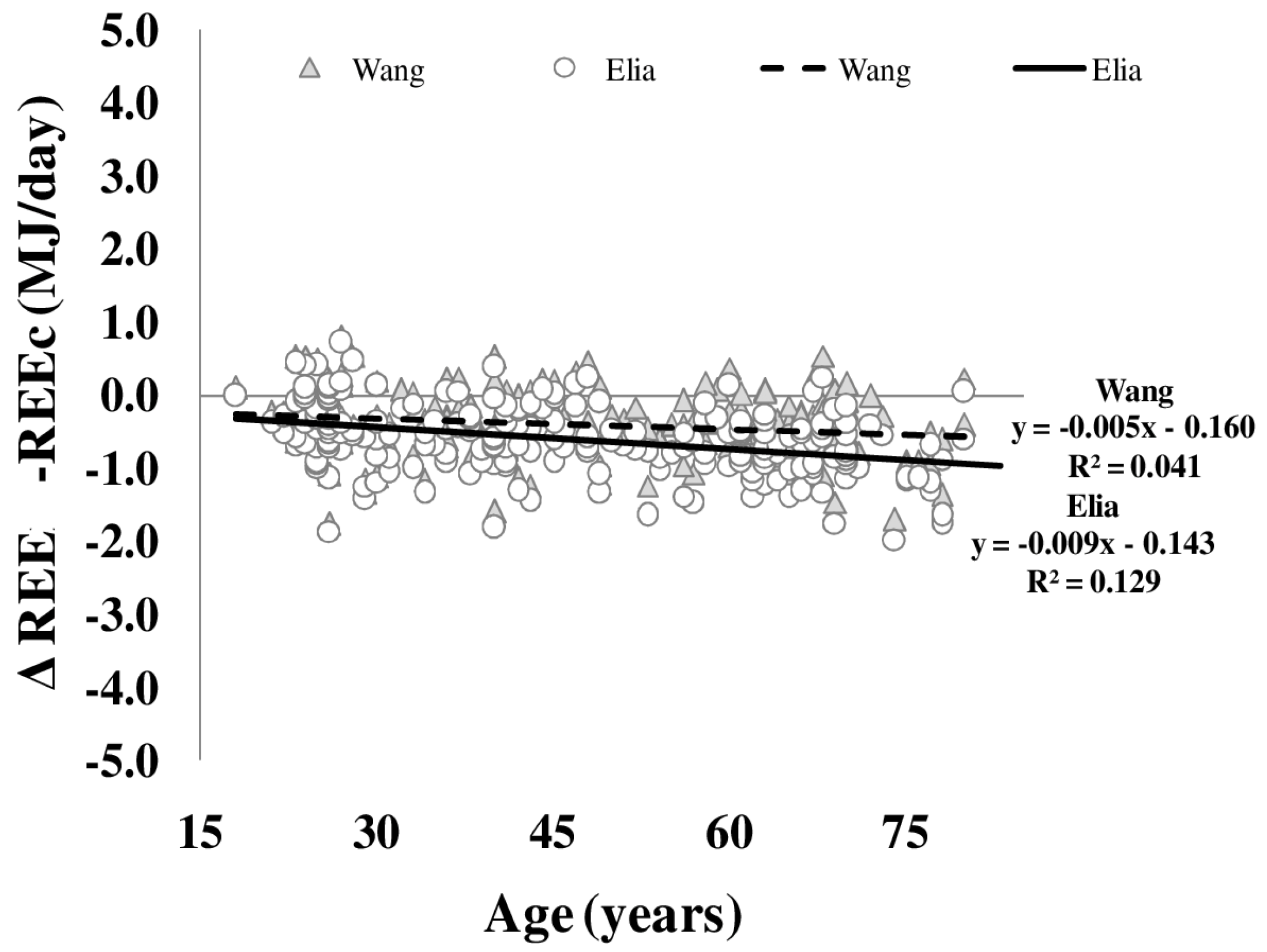
3.2. REE
3.3. Cardiometabolic Risk
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| BMCDXA | bone mineral content measured by dual energy X-ray absorptiometry |
| DXA | dual energy X-ray absorptiometry |
| FFM | fat free mass by DXA |
| FM | fat mass |
| MJ/day | mega joule per day |
| MM | skeletal muscle mass |
| MRI | magnetic resonance imaging |
| HMR | high metabolic rate organs |
| REE | measured resting energy expenditure |
| REEc | REE calculated from organ/tissue masses times their specific metabolic rates |
| ∆ REE-REEc | difference between measured resting energy expenditure and calculated resting energy expenditure |
References
- Elia, M.; Ritz, P.; Stubbs, R.J. Total energy expenditure in the elderly. Eur. J. Clin. Nutr. 2000, 54, S92–S103. [Google Scholar] [CrossRef] [PubMed]
- Molnar, D.; Schutz, Y. The effect of obesity, age, puberty and gender on resting metabolic rate in children and adolescents. Eur. J. Pediatr. 1997, 156, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Bosy-Westphal, A.; Eichhorn, C.; Kutzner, D.; Illner, K.; Heller, M.; Muller, M.J. The age-related decline in resting energy expenditure in humans is due to the loss of fat-free mass and to alterations in its metabolically active components. J. Nutr. 2003, 133, 2356–2362. [Google Scholar] [PubMed]
- Gallagher, D.; Allen, A.; Wang, Z.; Heymsfield, S.B.; Krasnow, N. Smaller organ tissue mass in the elderly fails to explain lower resting metabolic rate. Ann. N. Y. Acad. Sci. 2000, 904, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, D.; Belmonte, D.; Deurenberg, P.; Wang, Z.; Krasnow, N.; Pi-Sunyer, F.X.; Heymsfield, S.B. Organ-tissue mass measurement allows modeling of ree and metabolically active tissue mass. Am. J. Physiol. 1998, 275, E249–E258. [Google Scholar] [PubMed]
- Wang, Z.; Heshka, S.; Gallagher, D.; Boozer, C.N.; Kotler, D.P.; Heymsfield, S.B. Resting energy expenditure-fat-free mass relationship: New insights provided by body composition modeling. Am. J. Physiol. Endocrinol. Metab. 2000, 279, E539–E545. [Google Scholar] [PubMed]
- Bosy-Westphal, A.; Kossel, E.; Goele, K.; Later, W.; Hitze, B.; Settler, U.; Heller, M.; Gluer, C.C.; Heymsfield, S.B.; Muller, M.J. Contribution of individual organ mass loss to weight loss-associated decline in resting energy expenditure. Am. J. Clin. Nutr. 2009, 90, 993–1001. [Google Scholar] [CrossRef] [PubMed]
- Bosy-Westphal, A.; Reinecke, U.; Schlorke, T.; Illner, K.; Kutzner, D.; Heller, M.; Muller, M.J. Effect of organ and tissue masses on resting energy expenditure in underweight, normal weight and obese adults. Int. J. Obes. 2004, 28, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Heymsfield, S.B.; Gonzalez, M.C.; Shen, W.; Redman, L.; Thomas, D. Weight loss composition is one-fourth fat-free mass: A critical review and critique of this widely cited rule. Obes. Rev. 2014, 15, 310–321. [Google Scholar] [CrossRef] [PubMed]
- Muller, M.J.; Bosy-Westphal, A.; Kutzner, D.; Heller, M. Metabolically active components of fat free mass (ffm) and resting energy expenditure (ree) in humans. Forum. Nutr. 2003, 56, 301–303. [Google Scholar] [PubMed]
- Müller, M.J.; Wang, Z.; Heymsfield, S.B.; Schautz, B.; Bosy-Westphal, A. Advances in the understanding of specific metabolic rates of major organs and tissues in humans. Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Geisler, C.; Braun, W.; Pourhassan, M.; Schweitzer, L.; Gluer, C.C.; Bosy-Westphal, A.; Muller, M.J. Gender-specific associations in age-related changes in resting energy expenditure (ree) and mri measured body composition in healthy caucasians. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 20, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Ying, Z.; Bosy-Westphal, A.; Zhang, J.; Schautz, B.; Later, W.; Heymsfield, S.B.; Muller, M.J. Specific metabolic rates of major organs and tissues across adulthood: Evaluation by mechanistic model of resting energy expenditure. Am. J. Clin. Nutr. 2010, 92, 1369–1377. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, C.; Metter, E.J.; Melenovsky, V.; Cherubini, A.; Najjar, S.S.; Ble, A.; Senin, U.; Longo, D.L.; Ferrucci, L. High basal metabolic rate is a risk factor for mortality: The baltimore longitudinal study of aging. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Abizanda, P.; Romero, L.; Sánchez-Jurado, P.M.; Ruano, T.F.; Ríos, S.S.; Sánchez, M.F. Energetics of aging and frailty: The fradea study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2015. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, E.; An, Y.; Schrack, J.A.; Gonzalez-Freire, M.; Zoli, M.; Simonsick, E.M.; Guralnik, J.M.; Boyd, C.M.; Studenski, S.A.; Ferrucci, L. Energy metabolism and the burden of multimorbidity in older adults: Results from the baltimore longitudinal study of aging. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2015, 70, 1297–1303. [Google Scholar] [CrossRef] [PubMed]
- Luhrmann, P.M.; Edelmann-Schafer, B.; Neuhauser-Berthold, M. Changes in resting metabolic rate in an elderly german population: Cross-sectional and longitudinal data. J. Nutr. Health Aging 2010, 14, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Bosy-Westphal, A.; Muller, M.J.; Boschmann, M.; Klaus, S.; Kreymann, G.; Luhrmann, P.M.; Neuhauser-Berthold, M.; Noack, R.; Pirke, K.M.; Platte, P.; et al. Grade of adiposity affects the impact of fat mass on resting energy expenditure in women. Br. J. Nutr. 2009, 101, 474–477. [Google Scholar] [CrossRef] [PubMed]
- Bosy-Westphal, A.; Schautz, B.; Lagerpusch, M.; Pourhassan, M.; Braun, W.; Goele, K.; Heller, M.; Gluer, C.C.; Muller, M.J. Effect of weight loss and regain on adipose tissue distribution, composition of lean mass and resting energy expenditure in young overweight and obese adults. Int. J. Obes. 2013, 37, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.J.; Bosy-Westphal, A. Adaptive thermogenesis with weight loss in humans. Obesity 2013, 21, 218–228. [Google Scholar] [CrossRef] [PubMed]
- Siri, W.E. Body composition from fluid spaces and density: Analysis of methods. 1961. Nutrition 1993, 9, 480–491; discussion 480, 492. [Google Scholar] [PubMed]
- Muller, M.J.; Enderle, J.; Pourhassan, M.; Braun, W.; Eggeling, B.; Lagerpusch, M.; Gluer, C.C.; Kehayias, J.J.; Kiosz, D.; Bosy-Westphal, A. Metabolic adaptation to caloric restriction and subsequent refeeding: The minnesota starvation experiment revisited. Am. J. Clin. Nutr. 2015, 102, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Schautz, B.; Later, W.; Heller, M.; Muller, M.J.; Bosy-Westphal, A. Total and regional relationship between lean and fat mass with increasing adiposity—Impact for the diagnosis of sarcopenic obesity. Eur. J. Clin. Nutr. 2012, 66, 1356–1361. [Google Scholar] [CrossRef] [PubMed]
- Snyder, W.; Cook, M.J.; Nasset, E.S.; Karhausen, L.R.; Howells, G.P.; Tipton, I.H. Report of the Task Group on Reference Man; Pergamon Press: Oxford, UK, 1975. [Google Scholar]
- Muller, M.J.; Bosy-Westphal, A.; Klaus, S.; Kreymann, G.; Luhrmann, P.M.; Neuhauser-Berthold, M.; Noack, R.; Pirke, K.M.; Platte, P.; Selberg, O.; et al. World health organization equations have shortcomings for predicting resting energy expenditure in persons from a modern, affluent population: Generation of a new reference standard from a retrospective analysis of a german database of resting energy expenditure. Am. J. Clin. Nutr. 2004, 80, 1379–1390. [Google Scholar] [PubMed]
- Bader, N.; Bosy-Westphal, A.; Dilba, B.; Muller, M.J. Intra- and interindividual variability of resting energy expenditure in healthy male subjects—Biological and methodological variability of resting energy expenditure. Br. J. Nutr. 2005, 94, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Elia, M. Organ and tissue contribution to metabolic rate. In Energy Metabolism: Tissue Determinants and Cellular Corollaries; Kinney, J.M., Tucker, H.N., Eds.; Raven: New York, NY, USA, 1992; pp. 61–77. [Google Scholar]
- Heymsfield, S.B.; Gallagher, D.; Kotler, D.P.; Wang, Z.; Allison, D.B.; Heshka, S. Body-size dependence of resting energy expenditure can be attributed to nonenergetic homogeneity of fat-free mass. Am. J. Physiol. Endocrinol. Metab. 2002, 282, E132–E138. [Google Scholar] [PubMed]
- Haas, V.; Onur, S.; Paul, T.; Nutzinger, D.O.; Bosy-Westphal, A.; Hauer, M.; Brabant, G.; Klein, H.; Muller, M.J. Leptin and body weight regulation in patients with anorexia nervosa before and during weight recovery. Am. J. Clin. Nutr. 2005, 81, 889–896. [Google Scholar] [PubMed]
- Lagerpusch, M.; Enderle, J.; Eggeling, B.; Braun, W.; Johannsen, M.; Pape, D.; Muller, M.J.; Bosy-Westphal, A. Carbohydrate quality and quantity affect glucose and lipid metabolism during weight regain in healthy men. J. Nutr. 2013, 143, 1593–1601. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic Title | Women | Men | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All | 18–39 Years | 40–59 Years | 60–69 Years | 70+ Years | All | 18–39 Years | 40–59 Years | 60–69 Years | 70+ Years | |
| Number of subjects | 346 | 162 | 103 | 59 | 22 | 368 | 166 | 119 | 60 | 23 |
| Weight (kg) | 67.1 [60.3–72.8] * | 66.2 [59.1–731] | 68.3 [62.9–74.6] | 68.8 [62.6–72.7] | 61.7 [57.9–70.6] | 81.1 [73.3–88.6] | 79.1 [72.5–88.6] | 83.2 [76.8–90.1] | 79.6 [74.0–87.6] | 75.9 [71.5–83.6] # |
| Height (m) | 1.66 [1.62–1.72] * | 1.70 [1.64–1.73] | 1.66 [1.62–1.71] | 1.64 [1.60–1.67] | 1.61 [1.57–1.64] # | 1.79 [1.76–1.84] | 1.80 [1.77–1.86] | 1.81 [1.76–1.84] | 1.76 [1.72–1.79] | 1.74 [1.72–1.77] # |
| BMI (kg/m2) | 24.1 [21.7–26.7] * | 22.9 [21.1–25.6] | 24.8 [22.8–26.9] | 25.4 [23.3–27.3] | 23.9 [21.5–27.7] # | 25.0 [22.9–27.5] | 23.6 [22.2–26.8] | 25.6 [23.6–27.5] | 26.1 [24.9–28.4] | 24.6 [23.7–27.8] # |
| FFMADP(kg) | 44.6 [40.7–47.9] * | 46.1 [42.7–50.1] | 44.9 [41.5–49.2] | 42.2 [37.8–45.2] | 38.8 [37.4–41.9] # | 62.5 [57.9–67.5] | 64.8 [59.4–69.4] | 63.0 [59.4–67.5] | 58.9 [54.8–64.3] | 57.1 [54.1–59.4] # |
| FMADP (kg) | 22.4 [17.5–27.5] * | 20.3 [16.2–25.4] | 23.0 [17.8–23.3] | 26.3 [22.0–31.0] | 22.2 [18.6–30.5] # | 18.5 [12.9–23.1] | 14.2 [10.0–21.4] | 20.5 [15.4–25.0] | 20.8 [18.1–24.8] | 18.1 [15.4–27.5] # |
| Body density (kg/L) | 1.02 [1.01–1.03] * | 1.03 [1.02–1.03] | 1.02 [1.01–1.03] | 1.01 [1.00–1.02] | 1.01 [1.00–1.03] # | 1.04 [1.03–1.06] | 1.05 [1.04–1.07] | 1.04 [1.03–1.05] | 1.04 [1.03–1.05] | 1.04 [1.03–1.05] # |
| FFM hydration (L/kg) (n = 290) | 0.75 [0.73–0.78] * | 0.74 [0.71–0.76] | 0.75 [0.73–0.78] | 0.77 [0.72–0.79] | 0.79 [0.76–0.79] # | 0.73 [0.70–0.76] | 0.73 [0.70–0.76] | 0.73 [0.70–0.76] | 0.74 [0.71–0.76] | 0.74 [0.71–0.74] |
| Detailed body composition | ||||||||||
| Muscle massMRI (kg) (n = 369) | 19.6 [17.5–21.8] * | 20.7 [18.7–23.3] | 20.3 [18.5–22.3] | 17.5 [16.4–19.3] | 16.7 [15.2–17.5] # | 29.7 [26.9–32.8] | 31.7 [18.7–23.3] | 30.6 [27.8–32.3] | 27.1 [24.4–29.6] | 25.6 [22.2–27.1] # |
| % Muscle massMRI | 44.4 [42.4–46.7] * | 45.3 [43.1–47.7] | 44.5 [43.5–47.0] | 42.7 [41.3–45.5] | 39.9 [38.7–41.3] # | 47.4 [45.4–49.8] | 48.4 [46.2–50.6] # | 47.4 [45.8–50.4] | 45.8 [42.8–47.2] | 44.8 [40.8–46.1] # |
| Brain massMRI (kg) (n = 266) | 1.41 [1.35–1.48] * | 1.45 [1.39–1.51] | 1.44 [1.36–1.48] | 1.38 [1.35–1.41] | 1.25 [1.23–1.41] # | 1.57 [1.49–1.67] | 1.56 [1.49–1.67] | 1.65 [1.55–1.70] | 1.56 [1.47–1.63] | 1.54 [1.43–1.61] |
| % Brain massMRI | 3.20 [2.91–3.42] * | 3.10 [2.84–3.39] | 3.15 [2.85–3.44] | 3.26 [3.13–3.53] | 3.25 [3.05–3.61] # | 2.52 [2.33–2.72] | 2.45 [2.30–2.67] | 2.40 [2.30–2.65] | 2.62 [2.43–2.75] | 2.75 [2.41–2.98] # |
| Heart massMRI (kg) (n = 260) | 0.25 [0.21–0.32] * | 0.24 [0.22–0.29] | 0.25 [0.22–0.33] | 0.26 [0.23–0.33] | 0.21 [0.18–0.28] # | 0.32 [0.27–0.39] | 0.29 [0.25–0.33] | 0.33 [0.29–0.38] | 0.34 [0.29–0.39] | 0.39 [0.29–0.46] # |
| % Heart massMRI | 0.58 [0.49–0.69] * | 0.49 [0.44–0.60] | 0.58 [0.48–0.68] | 0.71 [0.55–0.77] | 0.60 [0.51–0.70] # | 0.51 [0.44–0.61] | 0.46 [0.38–0.58] | 0.54 [0.46–0.61] | 0.53 [0.49–0.63] | 0.66 [0.58–0.81] # |
| Liver massMRI (kg) (n = 266) | 1.36 [1.18–1.52] * | 1.42 [1.28–1.56] | 1.39 [1.23–1.54] | 1.14 [1.03–1.41] | 1.24 [1.02–1.37] # | 1.57 [1.39–1.81] | 1.57 [1.40–1.71] | 1.79 [1.49–1.97] | 1.54 [1.39–1.68] | 1.33 [1.22–1.49] # |
| % Liver massMRI | 3.01 [2.76–3.30] * | 3.01 [2.79–3.25] | 3.04 [2.77–3.43] | 2.8 [2.64–3.37] | 3.10 [2.68–3.36] | 2.55 [2.27–2.78] | 2.47 [2.24–2.69] | 2.72 [2.41–2.92] | 2.60 [2.38–2.84] | 2.34 [2.17–2.71] # |
| Kidney massesMRI (kg) (n = 265) | 0.22 [0.19–0.27] * | 0.24 [0.21–0.28] | 0.26 [0.21–0.28] | 0.19 [0.18–0.27] | 0.19 [0.16–0.21] # | 0.28 [0.23–0.33] | 0.26 [0.23–0.31] | 0.32 [0.28–0.33] | 0.31 [0.25–0.37] | 0.23 [0.21–0.29] # |
| % Kidney massesMRI | 0.51 [0.44–0.61] * | 0.50 [0.45–0.58] | 0.53 [0.45–0.64] | 0.51 [0.45–0.63] | 0.42 [0.39–0.54] | 0.45 [0.39–0.53] | 0.40 [0.35–0.48] | 0.50 [0.44–0.57] | 0.53 [0.45–0.59] | 0.40 [0.38–0.50] # |
| Spleen mass (kg) (n = 229) | 0.17 [0.14–0.21] * | 0.18 [0.16–0.24] | 0.18 [0.15–0.21] | 0.14 [0.10–0.17] | 0.12 [0.09–0.17] # | 0.27 [0.18–0.35] | 0.32 [0.24–0.39] | 0.28 [0.18–0.36] | 0.23 [0.16–0.28] | 0.15 [0.12–0.27] # |
| % Spleen massMRI | 0.37 [0.32–0.47] | 0.41 [0.34–0.48] | 0.37 [0.33–0.50] | 0.34 [0.27–0.38] | 0.29 [0.24–0.42] # | 0.40 [0.28–0.56] * | 0.51 [0.38–0.58] | 0.40 [0.25–0.55] | 0.35 [0.27–0.43] | 0.26 [0.21–0.43] # |
| Residual massMRI (kg) (n = 224) | 17.1 [14.3–19.8] * | 17.5 [15.9–20.4] | 18.9 [15.9–20.7] | 18.1 [15.6–24.9] | 27.0 [23.8–28.7] # | 22.8 [19.6–27.1] | 22.7 [19.9–25.6] | 24.7 [22.1–27.9] | 24.2 [19.9–28.1] | 39.0 [34.9–40.9] # |
| % Residual massMRI | 37.1 [32.9–42.9] | 33.7 [29.4–37.3] | 36.4 [32.6–39.7] | 41.6 [37.2–61.8] | 66.6 [60.4–68.9] # | 35.6 [31.9–39.8] | 31.4 [27.9–35.9] | 35.2 [32.5–37.8] | 38.1 [33.2–43.8] | 66.9 [48.8–71.1] # |
| Muscle mass/ Organ mass (n = 260) | 5.9 [5.5–6.4] * | 6.1 [5.6–6.7] | 6.2 [5.7–6.6] | 5.6 [5.4–5.9] | 5.6 [5.1–6.1] # | 7.7 [7.0–8.3] | 8.2 [7.6–8.8] | 7.4 [6.8–8.0] | 6.9 [6.6–7.5] | 6.9 [6.6–7.7] # |
| Adipose tissueMRI (L) (n = 369) | 23.5 [18.9–29.4] * | 22.9 [18.4–28.6] | 25.0 [20.5–33.7] | 23.9 [18.6–28.6] | 22.7 [17.8–28.5] # | 19.03 [14.4–24.1] | 15.8 [11.9–22.4] | 21.7 [18.1–25.9] | 20.9 [18.9–25.9] | 16.3 [14.1–20.3] # |
| Visceral adipose tissueMRI (L) (n = 369) | 1.24 [0.63–2.08] | 0.87 [0.45–1.43] | 1.33 [0.82–2.44] | 1.65 [1.12–2.54] | 1.95 [1.24–2.61] # | 2.71 [1.43–4.17] | 1.71 [0.84–3.35] | 2.96 [1.85–4.66] | 4.18 [3.74–6.08] | 3.11 [2.14–5.43] # |
| Bone mineralDXA (kg) (n = 329) | 4.2 [3.7–4.7] * | 4.4 [3.9–4.7] | 4.2 [3.7–4.6] | 3.8 [3.6–4.7] | 5.5 [3.8–6.4] # | 5.4 [4.8–5.9] | 5.4 [4.8–5.7] | 5.1 [4.8–5.7] | 5.6 [4.8–6.7] | 6.7 [5.5–7.5] # |
| %Bone mineralDXA | 9.3 [8.7–10.0] * | 9.3 [8.7–9.9] | 9.2 [8.6–9.8] | 9.1 [8.3–10.9] | 13.1 [10.1–14.7] # | 8.4 [7.9–8.9] | 8.2 [7.7–8.7] | 8.1 [7.8–8.5] | 8.8 [8.5–10.1] | 11.7 [9.7–12.9] # |
| Characteristic Title | Women | Men | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All | 18–39 Years | 40–59 Years | 60–69 Years | 70+ Years | All | 18–39 Years | 40–59 Years | 60–69 Years | 70+ Years | |
| Number of subjects | 346 | 162 | 103 | 59 | 22 | 368 | 166 | 119 | 60 | 23 |
| Resting energy expenditure | ||||||||||
| REE (MJ/day) (n = 714) | 5.8 [5.3–6.4] * | 6.1 [5.6–6.6] | 5.8 [5.4–6.4] | 5.5 [4.9–5.9] | 5.0 [4.7–5.3] # | 7.5 [6.8–8.3] | 7.8 [7.2–8.6] # | 7.7 [6.9–8.3] | 6.9 [6.1–7.8] | 6.3 [5.9–6.7] |
| REEFFM (MJ/day) (n = 714) | 5.8 [4.9–6.6] * | 6.2 [5.4–6.9] | 5.9 [4.9–6.8] | 5.3 [4.5–6.5] | 4.7 [3.9–5.1] # | 7.5 [6.2–8.8] | 7.9 [6.7–9.4] # | 7.7 [6.4–8.5] | 6.4 [5.5–7.8] | 5.7 [4.8–6.9] |
| REEc by Elia (MJ/day) (n = 217) | 5.9 [5.6–6.5] * | 6.0 [5.7–6.7] | 6.1 [5.7–6.6] | 5.7 [5.5–6.1] | 5.8 [5.4–6.0] | 7.6 [6.9–8.0] | 7.5 [6.9–7.9] | 7.9 [7.3–8.3] | 7.7 [6.7–8.0] | 7.5 [6.9–7.9] |
| ΔREE–REEc by Elia (MJ/day) (n = 217) | −0.56 [−0.78–0.29] * | −0.42 [−0.67–0.19] | −0.66 [−0.77–0.16] | −0.66 [−0.92–0.44] | −0.84 [−1.01–0.59] # | −0.63 [−1.04–0.37] | −0.48 [−0.88–0.03] # | −0.62 [−0.96–0.29] | −0.79 [−1.22–0.56] | −1.03 [−1.39–0.39] |
| REEc by Wang et al. (MJ/day) (n = 217) | 5.8 [5.4–6.3] * | 5.9 [5.4–6.3] | 5.9 [5.5–6.4] | 5.5 [5.2–5.8] | 5.6 [5.1–5.8] # | 7.4 [6.9–7.8] | 7.4 [6.8–7.8] | 7.7 [7.1–7.9] | 7.3 [6.4–7.7] | 7.2 [6.6–7.6] |
| ΔREE–REEc by Wang et al. (MJ/day) (n = 217) | −0.41 [−0.60–0.19] | −0.31 [−0.57–0.08] | −0.46 [−0.61–0.08] | −0.41 [−0.61–0.22] | −0.60 [−0.81–0.41] | −0.41 [−0.81–0.07] | −0.33 [−0.73–0.09] | −0.38 [−0.75–0.01] | −0.46 [−0.82–0.20] | −0.78 [−1.12–0.08] |
| Energy metabolism related hormones | ||||||||||
| Thyroid-stimulating hormone (mU/L) (n = 566) | 1.70 [1.16–2.49] * | 1.92 [1.31–2.76] | 1.43 [1.09–2.35] | 1.69 [1.05–2.69] | 1.46 [1.09–1.60] | 1.49 [1.04–2.25] | 1.83 [1.20-2.64] | 1.33 [0.94–1.85] | 1.39 [1.04-2.06] | 1.44 [1.04–2.06] # |
| Free triiodothryonin (pmol/L) (n = 566) | 3.63 [3.12–4.25] * | 3.69 [3.18–4.34] | 3.64 [3.04-4.22] | 3.46 [2.97–3.91] | 3.49 [2.83–4.13] | 3.90 [3.26–4.59] | 3.92 [3.20-4.67] | 4.01 [3.42–4.64] | 3.52 [3.19–4.04] | 3.60 [2.75-4.08] # |
| Free thyroxin (pmol/L) (n = 566) | 18.79 [12.19-15.82] * | 13.21 [12.09–14.95] | 14.30 [12.16-16.27] | 14.21 [12.38–19.37] | 17.41 [16.44–19.37] # | 14.52 [12.29–16.68] | 13.64 [10.50–16.04] | 15.40 [13.84–17.33] | 14.47 [12.21–17.46] | 16.16 [15.16–17.69] # |
| Characteristic Title | Women | Men | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All | 18–39 Years | 40–59 Years | 60–69 Years | 70+ Years | All | 18–39 Years | 40–59 Years | 60–69 Years | 70+ Years | |
| Number of subjects | 346 | 162 | 103 | 59 | 22 | 368 | 166 | 119 | 60 | 23 |
| Inflammation | ||||||||||
| CRP (mg/l) (n = 437) | 0.69 [0.20–1.75] | 0.92 [0.35–2.36] | 0.81 [0.25–1.53] | 0.41 [0.17–1.79] | 0.20 [0.10–0.35] # | 0.43 [0.16–1.29] | 0.32 [0.14–1.23] | 0.70 [0.28–1.67] | 0.63 [0.23–1.19] | 0.20 [0.10–0.78] |
| Insulin resistance | ||||||||||
| Glucose (mg/dl) (n = 551) | 90.6 [84.8–96.6] | 87.9 [83.9–92.4] | 91.6 [84.5–97.0] | 96.0 [92.0–103.0] | 93.5 [85.5–105.5] | 94.7 [87.4–101.9] | 90.0 [62.4–96.7] | 97.0 [91.9–104.6] | 99.5 [92.1–108.0] | 96.0 [89.8–102.5] |
| Insulin (mU/dl) (n = 530) | 8.8 [6.6–12.3] | 9.2 [6.9–12.8] | 7.8 [5.9–11.4] | 9.5 [6.9–12.5] | 8.9 [6.0–11.5] | 8.1 [6.3–10.9] | 8.2 [6.0–10.4] | 8.2 [6.4–12.1] | 7.8 [6.6–11.2] | 7.5 [5.9–11.3] |
| HOMA (n = 529) | 1.93 [1.38–2.80] | 2.06 [1.55–3.07] | 1.78 [1.09–2.59] | 2.04 [1.56–2.76] | 1.85 [1.29–2.81] | 1.73 [1.38–2.37] | 1.59 [1.19–2.16] | 1.95 [1.42–2.37] | 2.09 [1.66–3.31] | 1.91 [1.49–2.51] # |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geisler, C.; Braun, W.; Pourhassan, M.; Schweitzer, L.; Glüer, C.-C.; Bosy-Westphal, A.; Müller, M.J. Age-Dependent Changes in Resting Energy Expenditure (REE): Insights from Detailed Body Composition Analysis in Normal and Overweight Healthy Caucasians. Nutrients 2016, 8, 322. https://doi.org/10.3390/nu8060322
Geisler C, Braun W, Pourhassan M, Schweitzer L, Glüer C-C, Bosy-Westphal A, Müller MJ. Age-Dependent Changes in Resting Energy Expenditure (REE): Insights from Detailed Body Composition Analysis in Normal and Overweight Healthy Caucasians. Nutrients. 2016; 8(6):322. https://doi.org/10.3390/nu8060322
Chicago/Turabian StyleGeisler, Corinna, Wiebke Braun, Maryam Pourhassan, Lisa Schweitzer, Claus-Christian Glüer, Anja Bosy-Westphal, and Manfred J. Müller. 2016. "Age-Dependent Changes in Resting Energy Expenditure (REE): Insights from Detailed Body Composition Analysis in Normal and Overweight Healthy Caucasians" Nutrients 8, no. 6: 322. https://doi.org/10.3390/nu8060322