
An Evaluation of ¡Haz Espacio Para Papi!, a Culturally Tailored Nutrition and Physical Activity Pilot Program for Mexican-Heritage Fathers


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participant Recruitment
2.3. Program Delivery and Components
2.4. Data Collection and Measures
2.5. Treatment of Variables
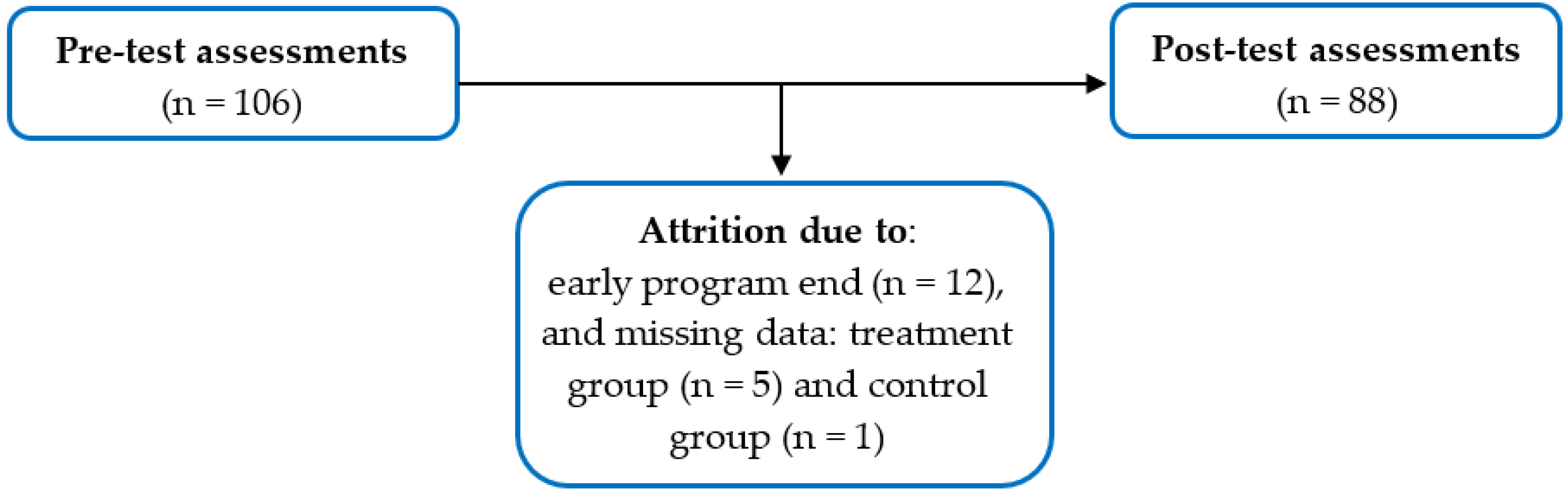
2.6. Analytic Sample
2.7. Statistical Analyses
3. Results
3.1. Sociodemographic Characteristics of HEPP Program Participants
3.2. Dietary Trends across Time for Treatment and Wait-Listed Control Comparison Groups
3.3. Comparisons of Fathers’ Objectively Measured Dietary Intake of Fruits and Vegetables Using Veggie Meter® Scores across Time and Between Groups
3.4. Comparisons of Fathers’ Weekly Average Self-Reported Dietary Intake of Fruits and Vegetables across Time and Between Groups
3.5. Comparisons of Fathers’ Weekly Average Healthy Dietary Behavior Scores across Time and Between Groups
3.6. Sociodemographic Effects on Program Outcomes
3.7. Analyses with Attrition
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rahill, S.; Kennedy, A.; Kearney, J. A review of the influence of fathers on children’s eating behaviours and dietary intake. Appetite 2020, 14, 104540. [Google Scholar] [CrossRef] [PubMed]
- Litchford, M.R.; Roskos, S.; Wengreen, H. Influence of fathers on the feeding practices and behaviors of children: A systematic review. Appetite 2020, 147, 104558. [Google Scholar] [CrossRef] [PubMed]
- Davison, K.K.; Lawson, H.A.; Coatsworth, J.D. The Family-Centered Action Model of Intervention Layout and Implementation (FAMILI): The example of childhood obesity. Health Promot. Pract. 2012, 13, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Ashton, L.M.; Morgan, P.J.; Grounds, J.A.; Young, M.D.; Rayward, A.T.; Barnes, A.T.; Pollock, E.R.; Kennedy, S.-L.; Saunders, K.L.; Collins, C.E. Dietary outcomes of the ‘Healthy Youngsters, Healthy Dads’ randomised controlled trial. Nutrients 2021, 13, 3306. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Lubans, D.R.; Plotnikoff, R.C.; Callister, R.; Burrows, T.; Fletcher, R.; Okely, A.D.; Young, M.D.; Miller, A.; Clay, V. ‘Healthy Dads, Healthy Kids’ community effectiveness trial: Study protocol of a community-based healthy lifestyle program for fathers and their children. BMC Public. Health 2011, 11, 876. [Google Scholar] [CrossRef] [PubMed]
- Sleddens, E.F.C.; Kremers, S.P.J.; Stafleu, A.; Dagnelie, P.C.; De Vries, N.K.; Thijs, C. Food parenting practices and child dietary behavior. Prospective relations and the moderating role of general parenting. Appetite 2014, 79, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, R.L.; Adamsons, K.; Mobley, A.R. Recruitment, engagement, and retention of fathers in nutrition education and obesity research. J. Nutr. Educ. Behav. 2019, 51, 1121–1125. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.M.; Sharkey, J.R.; Gómez, L. Latino fathers as catalistas (agents of change): Strategies to support Latino fathers in childhood obesity prevention. J. Nutr. Educ. Behav. 2021, 53, 540–545. [Google Scholar] [CrossRef]
- O’Connor, T.M.; Beltran, A.; Musaad, S.; Perez, O.; Flores, A.; Galdamez-Calderon, E.; Isbell, T.; Arrendondo, E.M.; Cardona, R.P.; Cabrera, N. Feasibility of targeting Hispanic fathers and children in an obesity intervention: Papás Saludables Niños Saludables. Child. Obes. 2020, 16, 379–392. [Google Scholar] [CrossRef]
- Zhang, Y.; Hurtado, G.A.; Reyes, A.P.; Brazys, P.A.; Perdue, L.; Alvarez de Davila, S.; Florex, R.; Manardez Popelka, J.M.; Reicks, M. Padres Preparados, Jóvenes Saludables, a family-based program to prevent obesity among Latino early adolescents: Pilot test findings. J. Hum. Sci. Ext. 2019, 7, 68–91. [Google Scholar] [CrossRef]
- Baltaci, A.; Hurtado; Choque, G.A.; Davey, C.; Reyes Peralta, A.; Alvarez de Davila, S.; Zhang, Y.; Gold, A.; Larson, N.; Reicks, M. Padres Preparados, Jóvenes Saludables: Intervention impact of a randomized controlled trial on Latino father and adolescent energy balance-related behaviors. BMC Public. Health 2022, 22, 1932. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.M.; Sharkey, J.R.; Umstattd Meyer, M.; Gómez, L.; Allicock, M.A.; Prochnow, T.; Beltrán, E.; Martinez, L. Designing for multilevel behavior change: A father-focused nutrition and physical activity program for Mexican-heritage families in South Texas border communities. Int. J. Environ. Res. Public. Health 2021, 18, 10117. [Google Scholar] [CrossRef]
- Schmied, E.; Parada, H.; Horton, L.; Ibarra, L.; Ayala, G. A process evaluation of an efficacious family-based intervention to promote healthy eating: The Entre Familia: Reflejos de Salud Study. Health Educ. Behav. 2015, 42, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, A.C.; Wallington, S.F.; Muñoz, M.A.; Greaney, M.L. A qualitative study conducted in the USA exploring Latino fathers’ beliefs, attitudes and practices related to their young children’s eating, physical activity and sedentary behaviours. Public Health Nutr. 2018, 21, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Ayala, G.; Ibarra, L.; Arrendondo, E.; Horton, L.A.; Hernandez, E.; Prada, H. Promoting healthy eating by strengthening family relations: Design and implementation of the Entre Familia: Reflejos de Salud intervention. In Cancer Disparities: Causes and Evidence-Based Solutions; Springer: New York, NY, USA, 2012; pp. 237–252. [Google Scholar]
- O’Connor, T.M.; Perez, O.; Beltran, A.; Colón García, I.; Arredondo, E.; Parra Cardona, R.; Cabrera, N.; Thompson, E.; Baranowski, T.; Morgan, P.J. Cultural adaptation of “Healthy Dads, Healthy Kids” for Hispanic families: Applying the ecological validity model. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 52. [Google Scholar] [CrossRef]
- Zhang, Y.; Hurtado, F.A.; Flores, R.; Alba-Meraz, A.; Reicks, M. Latino fathers’ perspectives and parenting practices regarding eating, physical activity, and screen time behaviors of early adolescent children: Focus group findings. J. Acad. Nutr. Diet. 2018, 118, 2070–2080. [Google Scholar] [CrossRef] [PubMed]
- Overcash, F.; Reicks, M. Diet quality and eating practices among Hispanic/Latino men and women: NHANES 2011-2016. Int. J. Environ. Res. Public Health 2021, 18, 1302. [Google Scholar] [CrossRef]
- Hee-Lee, S.; Moore, L.V.; Park, S.; Harris, D.M.; Blanck, H.M. Adults meeting fruit and vegetable intake recommendations—United States, 2019. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lee-Kwan, S.H.; Moore, L.V.; Blanck, H.M.; Harris, D.M.; Faluska, D. Disparities in state-specific adult fruit and vegetable consumption—United States, 2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 1241–1247. [Google Scholar] [CrossRef]
- Daviglus, M.L.; Pirzadaa, A.; Talavera, G.A. Cardiovascular disease risk factors in the Hispanic/Latino population: Lessons from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Prog. Cardiovasc. Dis. 2014, 57, 230–236. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Diabetes Statistics Report. 2022. Available online: https://www.cdc.gov/diabetes/data/statistics-report/index.html (accessed on 14 August 2022).
- Fryar, C.D.; Carroll, M.D.; Afful, J. Prevalence of Overweight, Obesity, and Severe Obesity Among Adults Aged 20 and Over: United States, 1960–1962 through 2017–2018. 2020. Available online: https://www.cdc.gov/nchs/data/hestat/obesity-adult-17-18/obesity-adult.html (accessed on 28 September 2021).
- Stok, F.M.; Renner, B.; Allan, J.; Boeing, H.; Ensenauer, R.; Issanchou, S.; Kiesswetter, E.; Lien, N.; Mazzocchi, M.; Monisvais, P.; et al. Dietary behavior: An interdisciplinary conceptual analysis and taxonomy. Front. Psychol. 2018, 9, 1689. [Google Scholar] [CrossRef] [PubMed]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025, 9th ed.; U.S. Department of Agriculture and U.S. Department of Health and Human Services: Washington, DC, USA, 2020. Available online: https://www.dietaryguidelines.gov (accessed on 14 August 2021).
- Prochnow, T.; Umstattd Meyer, M.R.; Johnson, C.M.; Delgado, H.; Gómez, L.; Sharkey, J.R. The development and pilot testing of the ¡Haz Espacio Para Papi! program physical activity curriculum for Mexican-heritage fathers and children. Am. J. Health Educ. 2021, 52, 145–153. [Google Scholar] [CrossRef]
- Sharkey, J.R.; Dean, W.R.; Johnson, C.M. Association of household and community characteristics with adult and child food insecurity among Mexican-origin households in colonias along the Texas-Mexico border. Int. J. Equity Health 2011, 10, 19. [Google Scholar] [CrossRef]
- Ramirez, A.G.; Thompson, I.M.; Vela, L. (Eds.) The South Texas Health Status Review: A Health Disparities Roadmap; Springer: Cham, Switzerland, 2013. [Google Scholar]
- Johnson, C.M.; Allicock, M.A.; Sharkey, J.R.; Renée Umstattd Meyer, M.; Gómez, L.; Prochnow, T.; Laviolette, C.; Beltrán, E.; Garza, L.M. Promotoras de salud in a father-focused nutrition and physical activity program for border communities: Approaches and lessons learned from collaboration. Int. J. Environ. Res. Public. Health 2022, 19, 11660. [Google Scholar] [CrossRef]
- Laviolette, C.; Johnson, C.M.; Butler, J.L.; Biediger-Friedman, L.; Sharkey, J.R. Nutrition effects of a family-centered health promotion program for Mexican-heritage children in the Lower Rio Grande Valley of Texas. Nutrients 2023, 15, 1600. [Google Scholar] [CrossRef]
- Hemming, K.; Haines, T.P.; Chilton, P.J.; Girling, A.J.; Lilford, R.J. The stepped wedge cluster randomised trial: Rationale, design, analysis, and reporting. BMJ 2015, 350, h391. [Google Scholar] [CrossRef] [PubMed]
- Diaz Rios, L.K.; Chapman-Novakofski, K. Latino/Hispanic participation in community nutrition research: An interplay of decisional balance, cultural competency, and formative Work. J. Acad. Nutr. Diet. 2018, 118, 1687–1699. [Google Scholar] [CrossRef]
- Mier, N.; Ory, M.G.; Medina, A.A. Anatomy of culturally sensitive interventions promoting nutrition and exercise in Hispanics: A critical examination of existing literature. Health Promot. Pract. 2010, 11, 541–554. [Google Scholar] [CrossRef]
- Longevity Link Corporation. The Veggie Meter® Non-Invasive Optical Biomarker for Personal Health. Available online: http://www.longevitylinkcorporation.com/home.html (accessed on 19 February 2023).
- Radtke, M.D.; Poe, M.; Stookey, J.; Jilcott, P.S.; Moran, N.E.; Landry, M.J.; Rubin, L.P.; Stage, V.C.; Scherr, R.E. Recommendations for the use of the Veggie Meter® for spectroscopy-based skin carotenoid measurements in the research setting. Curr. Dev. Nutr. 2021, 5, nzab104. [Google Scholar] [CrossRef]
- Jilcott, P.S.B.; Moran, N.E.; Wu, Q.; Harnack, L.; Craft, N.E.; Hanchard, N.; Bell, R.; Moe, S.G.; Johnson, N.; Obasohan, J.; et al. A non-invasive assessment of skin carotenoid status through reflection spectroscopy is a feasible, reliable, and potentially valid measure of fruit and vegetable consumption in a diverse community sample. Public. Health Nutr. 2018, 21, 1664–1670. [Google Scholar] [CrossRef] [PubMed]
- Nioa, J.D.; Gellermann, W. Use of the spectroscopy-based Veggie Meter® to objectively assess fruit and vegetable intake in low-income adults. Nutrients 2021, 13, 2270. [Google Scholar] [CrossRef] [PubMed]
- Jahns, L.; Johnson, L.A.K.; Mayne, S.T.; Cartmel, B.; Picklo Sr, M.J.; Ermakov, I.V.; Gellermann, W.; Whigham, L.D. Skin and plasma carotenoid response to a provided intervention diet high in vegetables and fruit: Uptake and depletion kinetics. Am. J. Clin. Nutr. 2014, 100, 930–937. [Google Scholar] [CrossRef] [PubMed]
- Ermakov, I.V.; Gellermann, W. Dermal carotenoid measurements via pressure mediated reflection spectroscopy. J. Biophotonics 2012, 5, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Obana, A.; Gohto, Y.; Gellermann, W.; Ermakov, I.V.; Sasano, H.; Seto, T.; Berstein, P. Skin carotenoid index in a large Japanese population sample. Sci. Rep. 2019, 9, 9318. [Google Scholar] [CrossRef] [PubMed]
- Nagao-Sato, S.; Baltaci, A.; Peralta Reyes, A.O.; Zhang, Y.; Hurtado Choque, G.A.; Reicks, M. Skin carotenoid scores assessed with reflection spectroscopy are associated with self-reported fruit and vegetable intake among Latino early adolescents. J. Acad. Nutr. Diet. 2021, 121, 1507–1514. [Google Scholar] [CrossRef] [PubMed]
- Stata Statistical Software: Release 17; [Computer Software]; Stata: College Station, TX, USA, 2021.
- Schmider, E.; Ziegler, M.; Danay, E.; Beyer, L.; Bühner, M. Is it really robust? Reinvestigating the robustness of ANOVA against violation of the normal distribution assumption. Methodology 2010, 6, 147–151. [Google Scholar] [CrossRef]
- Portney, L.G.; Watkins, M. Foundations of Clinical Research: Applications to Practice, 3rd ed.; F.A.: Davis Company: Philadelphia, PA, USA, 2015. [Google Scholar]
- Field-Fote, E.E. Mediators and moderators, confounders and covariates: Exploring the variables that illuminate or obscure the “active ingredients” in neurorehabilitation. J. Neurol. Phys. Ther. 2019, 43, 83–84. [Google Scholar] [CrossRef]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef]
- Fernandez, A.; Lozano, A.; Lee, T.K.; Messiah, S.E.; Prado, G. A healthy lifestyle intervention for Hispanic families: Moderating effects of education, income, nativity. J. Nutr. Educ. Behav. 2022, 54, 125–134. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods. 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Saracho, O.N.; Spodek, B. Demythologizing the Mexican American father. J. Hisp. High. Educ. 2008, 7, 79–96. [Google Scholar] [CrossRef]
- McCamgridgea, J.; Wittonb, J.; Elbourne, D.R. Systematic review of the Hawthorne effect: New concepts are needed to study research participation effects. J. Clin. Epidemiol. 2014, 67, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Coleman, K.J.; Ocana, L.L.; Walker, C.; Araujo, R.A.; Gutierrez, V.; Shordon, M.; Oratowski-Coleman, J.; Philis-Tsimikas, A. Outcomes from a culturally tailored diabetes prevention program in Hispanic families from a low-income school: Horton Hawks Stay Healthy (HHSH). Diabetes Educ. 2010, 3, 7784–7792. [Google Scholar] [CrossRef]
- Frank, G.C.; Nguyen Rodriguez, S.T.; Bird, M.; Garcia, M.; Gatdula, N.; Centinaje, E.; Rascón, M.; Rios-Ellis, B. Primary outcomes of a healthy lifestyle intervention for Latino families. Calif. J. Health Promot. 2020, 18, 29–38. [Google Scholar] [CrossRef]
- Prado, G.; Fernandez, A.; St George, S.; Tapia, M.I.; Velazquez, M.R.; Messiah, S.E. Results of a family-based intervention promoting healthy weight strategies in overweight Hispanic adolescents and parents: A RCT. Am. J. Prev. Med. 2020, 59, 658–668. [Google Scholar] [CrossRef] [PubMed]
- Gallo, S.; Jones, M.T.; Doig, A.C.; Kogan, K.; Fields, J.; Wonderlich, J.A.; Hansen, A.; LaCharite, K.; Mehlenbeck, R. Feasibility of a multidisciplinary and culturally adapted pediatric weight management program for Latino families: Results from the Vidas Activas y Familias Saludables pilot study. J. Nutr. Educ. Behav. 2020, 52, 55–63. [Google Scholar] [CrossRef]
- Perez, O.; Beltran, A.; Isbell, T.; Galdamez-Calderon, E.; Baranowski, T.; Morgan, P.J.; O’Connor, T.M. Papá Saludables, Niños Saludables: Perspectives from Hispanic parents and children in a culturally adapted father-focused obesity program. J. Nutr. Educ. Behav. 2020, 53, 246–253. [Google Scholar] [CrossRef]
- Macdiarmid, J.I. Seasonality and dietary requirements: Will eating seasonal food contribute to health and environmental sustainability? Proc. Nutr. Soc. 2013, 73, 368–375. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Weeks | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Clusters | 0 | 6 | 10 | 16 | 20 | 26 | 30 | 36 | 40 | 42 | |
| 1 | |||||||||||
| 2 | |||||||||||
| 3 | |||||||||||
| 4 | |||||||||||
| 5 | |||||||||||
| Sociodemographic Characteristic | Treatment (n = 42) | Control Comparison (n = 46) |
|---|---|---|
| Mean ± s.d. (Range) or n (%) | ||
| Age | 39.0 ± 7.3 (26–59) | 38.7 ± 8.9 (26–58) |
| Body mass index a | 30.5 ± 5.2 (22.1–46.1) | 31.3 ± 5.5 (22.1–49.7) |
| Marital status | ||
| Married | 27 (64.3) | 25 (54.4) |
| Living with spouse—not married | 15 (35.7) | 21 (45.7) |
| Education attainment | ||
| Did not go to school | 1 (2.4) | 1 (2.3) |
| Some school | 29 (69.1) | 34 (73.9) |
| GED or HS diploma | 10 (23.8) | 9 (19.6) |
| Some college | 2 (4.8) | 1 (2.2) |
| College degree | 0 (0.0) | 1 (2.2) |
| Total residents in household | 7.3 ± 2.4 (4–16) | 7.1 ± 2.0 (4–13) |
| Number of adults b | 2.6 ± 1.0 (2–5) | 2.7 ± 1.0 (2–6) |
| Number of children c | 4.7 ± 2.2 (2–13) | 4.4 ± 1.9 (2–9) |
| Ages of adults in household (years of age) | 36.6 ± 11.4 (18–79) | 37.3 ± 12.3 (26–77) |
| Ages of children in household (years of age) | 9.4 ± 4.2 (3 mo–17) | 9.3 ± 4.2 (3 mo–17) |
| Measure | Treatment (n = 42) | Control Comparison (n = 46) | ||||||
|---|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | Mean Change | p Value | Pre-Test | Post-Test | Mean Change | p Value | |
| Total fruit a | 3.9 ± 2.4 (0–10) | 4.0 ± 2.3 (1–10) | 0.12 ± 1.9 | 0.69 | 3.5 ± 3.2 (0–16) | 3.7 ± 2.4 (0–10) | 0.13 ± 3.6 | 0.81 |
| Fresh fruit | 2.7 ± 1.6 (0–7) | 2.8 ± 1.5 (0–8) | 0.17 ± 1.5 | 0.49 | 2.3 ± 2.6 (0–16) | 2.5 ± 1.6 (0–7) | 0.15 ± 3.0 | 0.73 |
| 100% fruit juice | 1.2 ± 1.5 (0–5) | 1.2 ± 1.4 (0–5) | −0.05 ± 1.4 | 0.82 | 1.2 ± 1.6 (0–7) | 1.2 ± 1.4 (0–5) | −0.22 ± 1.9 | 0.94 |
| Total veggies b | 5.4 ± 3.3 (1–17) | 5.9 ± 2.7 (0–12) | 0.45 ± 3.5 | 0.40 | 5.3 ± 4.4 (0–24) | 5.8 ± 3.3 (1–17) | 0.54 ± 5.4 | 0.50 |
| White potatoes | 1.6 ± 1.0 (0–4) | 1.8 ± 1.5 (0–6) | 0.17 ± 1.8 | 0.55 | 1.5 ± 1.4 (0–7) | 1.7 ± 1.0 (0–5) | 0.20 ± 1.6 | 0.40 |
| Lettuce | 2.0 ± 1.5 (0–7) | 1.7 ± 1.1 (0–3) | −0.29 ± 1.3 | 0.17 | 1.6 ± 1.6 (0–7) | 2.2 ± 1.5 (0–7) | 0.54 ± 2.0 | 0.07 |
| Other veggies | 1.8 ± 1.6 (0–7) | 2.3 ± 1.6 (0–7) | 0.57 ± 2.0 | 0.07 | 2.1 ± 3.2 (0–21) | 2.0 ± 1.5 (0–7) | −0.20 ± 3.7 | 0.72 |
| Total FV c | 9.2 ± 4.9 (2–27) | 9.9 ± 4.1 (3–20) | 0.57 ± 4.5 | 0.41 | 8.1 ± 5.4 (1–28) | 9.5 ± 4.6 (2–27) | 1.50 ± 6.3 | 0.12 |
| VM score d | 288.6 ± 45.7 (208–421) | 289.8 ± 60.6 (92.5–423) | 0.60 ± 46.9 | 0.47 | 276.9 ± 48.2 (179.5–388) | 279.8 ± 46.5 (139–376) | 3.00 ± 45.1 | 0.66 |
| HDBS e | 6.5 ± 2.1 (1–12) | 6.9 ± 1.6 (4–11) | 0.42 ± 1.8 | 0.11 | 5.8 ± 2.1 (0–11) | 6.6 ± 2.1 (1–12) | 0.80 ± 2.1 | 0.01 |
| Source of Variation | df | F-Value | p | η2 |
|---|---|---|---|---|
| Veggie Meter® scores | ||||
| Group | 1 | 1.22 | 0.27 | 0.01 |
| Time | 1 | 0.13 | 0.72 | <0.01 |
| Group × Time | 1 | 0.06 | 0.81 | <0.01 |
| Total | 175 | |||
| Total FV a | ||||
| Group | 1 | 0.85 | 0.36 | <0.01 |
| Time | 1 | 3.01 | 0.08 | 0.01 |
| Group × Time | 1 | 0.58 | 0.45 | <0.01 |
| Total | 174 | |||
| HDBS | ||||
| Group | 1 | 1.32 | 0.25 | 0.01 |
| Time | 1 | 8.88 | <0.01 * | 0.02 |
| Group × Time | 1 | 0.70 | 0.41 | <0.01 |
| Total | 175 |
| Source of Variation | df | F-Value | p | η2 |
|---|---|---|---|---|
| Age | ||||
| Group | 1 | 0.79 | 0.37 | <0.01 |
| Time | 1 | 7.96 | <0.01 * | 0.02 |
| Group × Time × Age | 1 | 0.10 | 0.75 | <0.01 |
| Total | 175 | |||
| Educational Attainment | ||||
| Group | 1 | 1.68 | 0.20 | 0.01 |
| Time | 1 | 8.40 | <0.01 * | 0.02 |
| Group × Time × Education | 1 | 3.41 | 0.07 | <0.01 |
| Total | 175 | |||
| Number of children in household | ||||
| Group | 1 | 0.91 | 0.34 | <0.01 |
| Time | 1 | 7.85 | <0.01 * | 0.02 |
| Group × Time × Children | 1 | 1.93 | 0.17 | <0.01 |
| Total | 175 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vahk, A.; Monsivais, P.; Johnson, C.M.; Sharkey, J.R. An Evaluation of ¡Haz Espacio Para Papi!, a Culturally Tailored Nutrition and Physical Activity Pilot Program for Mexican-Heritage Fathers. Nutrients 2024, 16, 1153. https://doi.org/10.3390/nu16081153
Vahk A, Monsivais P, Johnson CM, Sharkey JR. An Evaluation of ¡Haz Espacio Para Papi!, a Culturally Tailored Nutrition and Physical Activity Pilot Program for Mexican-Heritage Fathers. Nutrients. 2024; 16(8):1153. https://doi.org/10.3390/nu16081153
Chicago/Turabian StyleVahk, Annika, Pablo Monsivais, Cassandra M. Johnson, and Joseph R. Sharkey. 2024. "An Evaluation of ¡Haz Espacio Para Papi!, a Culturally Tailored Nutrition and Physical Activity Pilot Program for Mexican-Heritage Fathers" Nutrients 16, no. 8: 1153. https://doi.org/10.3390/nu16081153