

The Role of Diet and Nutritional Interventions for the Infant Gut Microbiome
by
 , ,
, ,
Giulia Catassi
1,2,
Marina Aloi
2,
Valentina Giorgio
3,
Antonio Gasbarrini
1,4,5,
Giovanni Cammarota
1,4,5 and
Gianluca Ianiro
1,4,5,* 1
Department of Translational Medicine and Surgery, Università Cattolica del Sacro Cuore, 00168 Rome, Italy
2
Pediatric Gastroenterology and Liver Unit, Sapienza University of Rome, Umberto I Hospital, 00161 Rome, Italy
3
Department of Woman and Child Health and Public Health, UOC Pediatria, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, 00168 Rome, Italy
4
Department of Medical and Surgical Sciences, UOC Gastroenterologia, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, 00168 Rome, Italy
5
Department of Medical and Surgical Sciences, UOC CEMAD Centro Malattie dell’Apparato Digerente, Medicina Interna e Gastroenterologia, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, 00168 Rome, Italy
*
Author to whom correspondence should be addressed.
Nutrients 2024, 16(3), 400; https://doi.org/10.3390/nu16030400
Submission received: 14 December 2023
/
Revised: 14 January 2024
/
Accepted: 19 January 2024
/
Published: 30 January 2024
(This article belongs to the Special Issue Diet and Nutritional Intervention for the Infant Gut Microbiome—2nd Edition)
{kind=link}
{kind=link}
Abstract
:The infant gut microbiome plays a key role in the healthy development of the human organism and appears to be influenced by dietary practices through multiple pathways. First, maternal diet during pregnancy and infant nutrition significantly influence the infant gut microbiota. Moreover, breastfeeding fosters the proliferation of beneficial bacteria, while formula feeding increases microbial diversity. The timing of introducing solid foods also influences gut microbiota composition. In preterm infants the gut microbiota development is influenced by multiple factors, including the time since birth and the intake of breast milk, and interventions such as probiotics and prebiotics supplementation show promising results in reducing morbidity and mortality in this population. These findings underscore the need for future research to understand the long-term health impacts of these interventions and for further strategies to enrich the gut microbiome of formula-fed and preterm infants.
1. Introduction
The infant gut microbiome is the collection of microorganisms residing in the gastrointestinal tract of newborns and infants (i.e., children between 1 and 23 months of age) [1]. This microbial community is composed of different microorganisms, including bacteria, viruses, fungi, parasites, archaea, and other microbes. Bacteria are the most abundant and diverse group within the gut microbiome [2,3].
Generally, the human gut microbiome is fundamental in shaping the health and well-being of individuals throughout their lifespan [4]. The critical role of this microbial community is even more pronounced during infancy, the period that lays the groundwork for an individual’s long-term health trajectory [5,6]. Multiple recent research works have underscored the significance of the gut microbiome in infants concerning different facets of health and illness [7,8], shedding light on the intricate interactions among microbial populations, nutrition, genetics, and the body’s immune mechanisms [5,6].
The quantitative and qualitative composition of the gut microbiome is heavily dependent on the diet. This is particularly true during the first two years of life due to the many changes that take place during this period of life, including breast and/or formula feeding, weaning and gradual introduction of different solid foods [9,10,11].
This narrative review aims to thoroughly assess the existing scientific literature regarding the impact of diet and nutritional interventions on the infant gut microbiome, exploring the impact of dietary factors on the composition, diversity, and functionality of the gut microbial community in early life. We aim to investigate how specific nutrients, dietary patterns, feeding practices and nutritional intervention (prebiotics, probiotics, and dietary supplements) can influence the establishment and development of a healthy gut microbiome in infants, both in healthy term-newborns and in infants requiring special care (e.g., preterm, very low birth weight, etc.). Finally, we will identify current research gaps and highlight potential areas for future investigation.
2. Methods
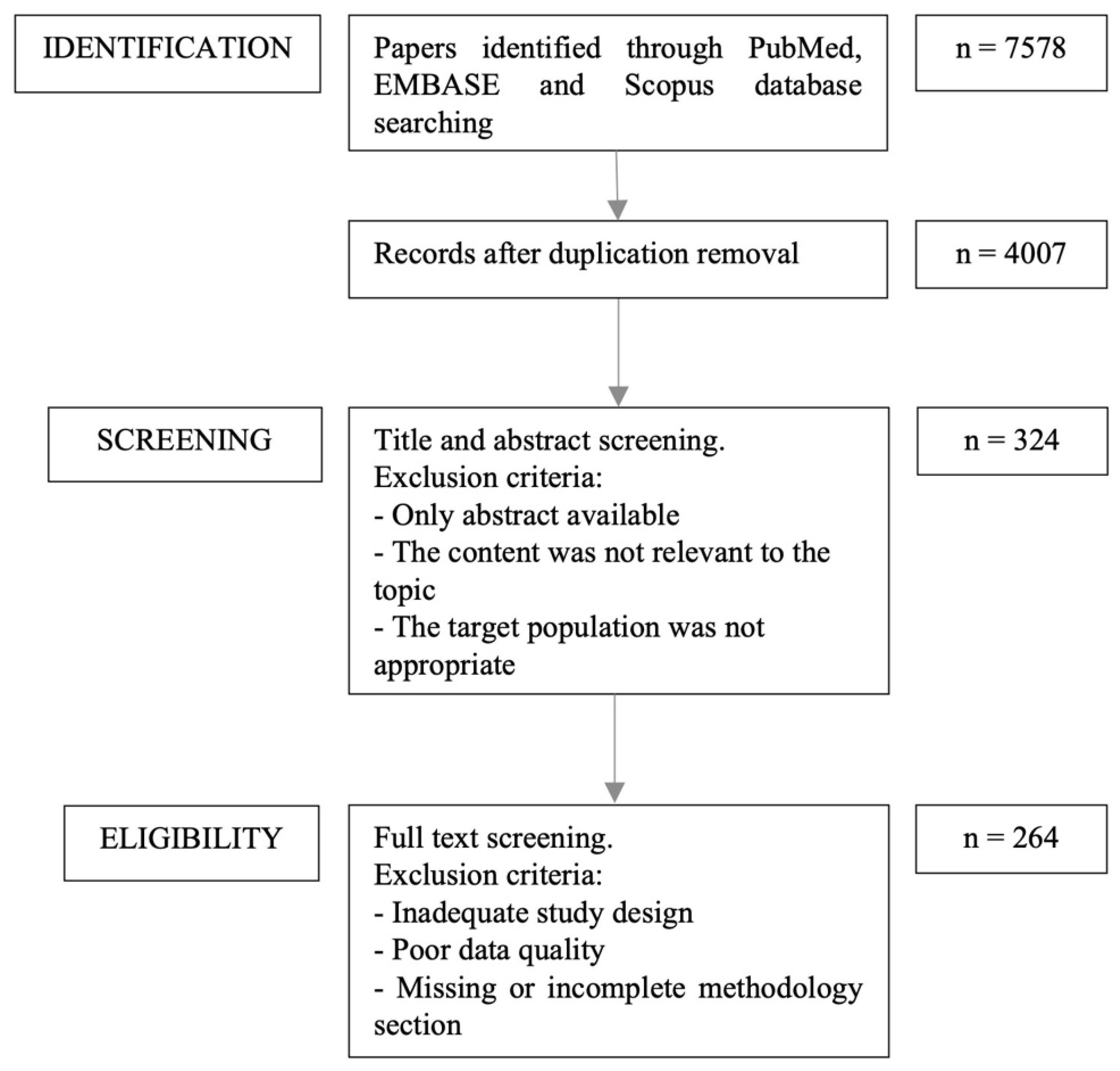
The authors independently identified the most pertinent published papers that examined the effect of diet on infant gut microbiota. These included observational, retrospective, and prospective studies, as well as case-control, cohort studies, systematic reviews, and meta-analyses. The search was limited to English-language studies published during the last 20 years (2003–2023) and was conducted on PubMed, EMBASE, and Scopus, using the following MeSH-terms: “infant” and “diet” or “food” or “nutrition” and “gastrointestinal microbiome”. The search included all articles that provided sufficient information on the relationship between infant gut microbiota, nutritional interventions, and diet. For every search conducted, the titles of the papers were examined to determine their relevance to the subject. The abstracts of these pertinent papers were then acquired and reviewed, leading to the selection of a subset for a comprehensive review of the entire manuscript. The flow diagram of the article selection process is shown in Figure 1.
3. Development of Infant Gut Microbiome and Early Dietary Changes
At birth, the gut of the newborn is considered to be relatively sterile, but it quickly becomes colonized by microorganisms acquired from the environment [12,13]. Studies challenge the sterility dogma of the fetus in utero, revealing bacterial presence in meconium, amniotic fluid, and the placenta [14,15,16], implying a process of maternal-to-offspring microbial transfer in utero [16]. Nevertheless, the crucial colonization phase occurs soon after birth [17].
The consolidation of a steady gut microbiota in humans is typically associated with two major transitions during infancy [18]: the initial transition takes place shortly after birth, during the lactation phase, characterized by the predominance of Bifidobacterium. During this phase, the beta diversity is initially pronounced, and the gut microbiota exhibits instability and decreased resistance to alterations compared to the gut microbiota observed in adults [12,18,19]. The subsequent shift ensues during the weaning stage when solid foods are introduced alongside the continuation of milk consumption. This second transition leads to the emergence of an intricate, adult-like microbiome, predominantly populated by the bacterial phyla Bacteroidetes and Firmicutes [12,19,20]. Following this period, the infant gut microbiota evolves into a more complex, diverse and stable ecosystem [21].
However, prior to reaching this stabilized state, the gut microbiota is more vulnerable to modifications induced by external variables [1,18,20,22]. Elements that contribute to the development of an infant’s gut microbiota include mode of delivery (vaginal birth vs. cesarean section), feeding method (breastfeeding vs. formula feeding), antibiotic exposure, and other environmental factors [8,23,24]. Early-life dietary habits in infants are recognized as significant factors influencing the initial formation of gut microbiota [25,26,27]. This early-life microbial inoculation is of pivotal importance, as these initial colonizers lay the groundwork for future microbial interactions [7,23].
Optimal infant nutrition is crucial for promoting growth and health [28,29]. The World Health Organization (WHO) and the United Nations International Children’s Emergency Fund (UNICEF) have provided specific guidelines for achieving this nutritional goal. They suggest that breastfeeding should commence within the first hour after birth and continue exclusively for the initial six months [30,31]. Beyond this period, breastfeeding should be sustained until the infant reaches two years of age or even longer. Moreover, it is recommended that a complementary diet be incorporated into the infant’s feeding regime no later than when they are six months old [30,31].
4. Diet and Nutritional Interventions during Pregnancy
4.1. Maternal Diet during Pregnancy
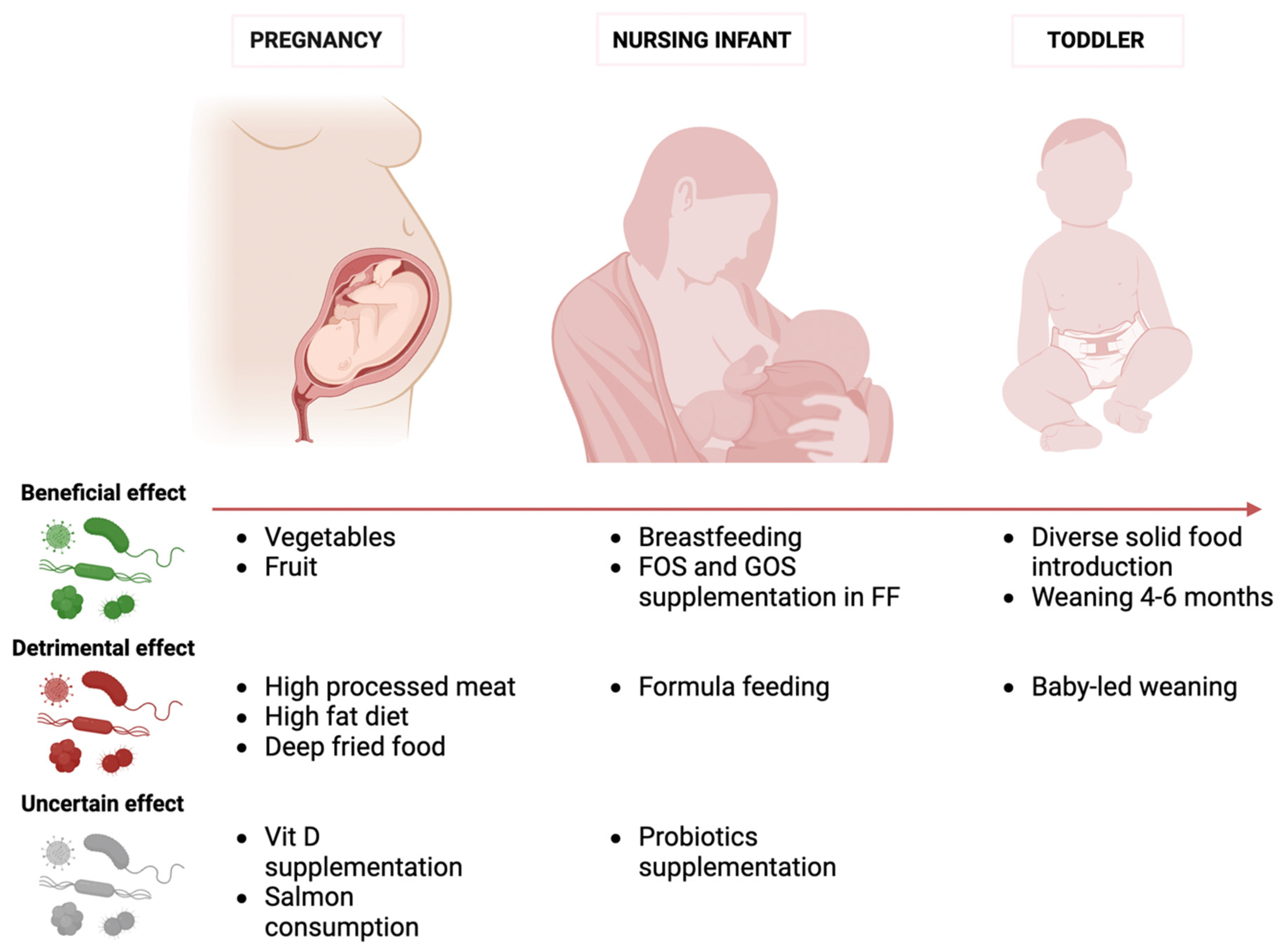
Scientists are increasingly intrigued by the impact of dietary and nutritional interventions during pregnancy on the development of the infant gut microbiome. Figure 2 summarizes the effects of different microbiome modulators at different stages of the infant’s life. According to the Developmental Origins of Health and Disease Hypothesis (DOHaD), neonatal gastrointestinal colonization during the first 1000 days after birth is an essential stage in growth and development, strongly impacted by maternal diet [32]. Numerous research projects have examined the relationship between a mother’s diet and her baby’s intestinal microbiota using food frequency questionnaires, yielding inconsistent findings [33,34]. The dietary elements analyzed in mothers included general eating habits as well as particular nutritional elements [32,35,36,37]. After adjusting for variables like demographics, delivery mode, and breastfeeding status, no significant independent impact on the infant microbiome was found [33]. Urwin et al. [38] discovered that a mother’s bi-weekly intake of salmon did not notably affect the gut microbiota of both the mother and her child. In this context, a study by Garcia Mantrana et al. [39] explored the specific relationship between maternal diet during pregnancy and the composition of both maternal and neonatal gut microbiota, employing 16S rRNA gene sequencing. This study revealed that dietary components such as fiber, lipids, and proteins were linked to specific clusters of gut microbiota in both mothers and their children. A considerable body of evidence comes from studies investigating the role of vitamin D during pregnancy. Using data from the same group of the Vitamin D Antenatal Asthma Reduction Trial (VDAART), it was observed that prenatal dietary habits classified as “healthy”—marked by abundant vegetable consumption and minimal intake of processed meats and deep-fried foods—were associated with a higher alpha diversity in the gut microbiota of newborns. Yet, these variations lost statistical significance upon demographic adjustments and consideration of the infant’s feeding mode [40,41]. In a distinct study, the VDAART team discovered no relation between supplementation of vitamin D during pregnancy and the diversity of gut microbes in infants aged between three to six months [42]. The KOALA birth cohort research also reported negligible connections between mothers’ vitamin D supplementation and 25-hydroxyvitamin D concentration and their infants’ intestinal microbiota. The only exception noted was an increase in Bifidobacteria counts in the stools of one-month-old babies following maternal vitamin D supplementation. No further significant links were evident in the models after adjustments [43].
Additionally, a high-fat diet appears to play a role in the infant microbiome. Chu and colleagues observed that regardless of the mother’s weight, babies born to mothers with a high-fat dietary intake exhibited a different meconium composition and a lower proportion of Bacteroides a few weeks after birth in comparison to those in the control group [44].
A key component of a mother’s diet that seems to have a notable impact on her baby’s intestinal microbiota is the consumption of fruits and vegetables [45]. Lundgren et al. [46] noted a substantial link between a mother’s fruit intake and the makeup of her baby’s fecal microbiome at six weeks, but this connection was only evident in babies born through vaginal delivery and who were solely breastfed. In line with this, a pilot study by Fan et al. [47] found a significant correlation between the level of maternal fruit and vegetable consumption and the infant gut microbiome composition at two months of age. It is indeed important to recognize that the gut microbiome’s structure is affected by the consumption of dietary fibers, which certain bacteria metabolize to produce short-chain fatty acids (SCFAs), including acetate, propionate, and butyrate [48,49,50]. In line with this, this study showed a pronounced increase in Cutibacterium, Parabacteroides, and Lactococcus in the intestinal microflora of infants exposed to a diet rich in fruits and vegetables during gestation. Conversely, an increased occurrence of inflammatory strains, like Sutterella, was associated with a lower intake of these foods [47].
4.2. Probiotics and Prebiotics during Pregnancy and Lactation
The scientific community has shown growing interest in the potential benefits of altering the infant gut microbiome by adding probiotics or prebiotics during pregnancy and breastfeeding. An extensive review of 17 interventional trials investigated the effects of administering probiotics to mothers during pregnancy on the newborn’s intestinal microbiota [32]. Supplementation was carried out using probiotics containing at least one species of Lactobacillus and/or Bifidobacterium, delivered in various forms, such as capsules, powder, milk, yogurt, or oil droplets. The supplementation was given to women during their second or third trimester of pregnancy. This review showed that the administration of probiotics to pregnant and lactating mothers has a significant impact on establishing the newborn’s gut ecosystem and influencing the microbial composition of maternal breast milk. However, there is scarce evidence that this intervention determines sustained colonization or can significantly influence the overall diversity of the infant microbiome [51,52,53]. While some studies report a higher abundance of supplemented species at the time of intervention [52,53,54,55,56,57], other research indicated no notable changes in the abundance of species added through supplementation following the discontinuation of the probiotic treatment [58,59,60,61]. A recent metanalysis of seven studies affirms that supplementing mothers with probiotics during pregnancy and breastfeeding leads to the infant’s gut being colonized by the species provided [51]. The abundance of these species reached its zenith during the first month of life, prior to a consistent decline, potentially attributed to the competitive interplay with other emergent bacterial populations. Overall, in a couple of randomized studies evaluating changes in ecological metrics after treatment with probiotics, no notable statistical variances were observed in alpha and beta diversity at various intervals when comparing probiotic supplementation with placebo [53,62].
Only a few (but well-designed) studies evaluated the effect of prebiotics, mainly galactooligosaccharides (GOS) and long-chain fructooligosaccharides (lcFOS), on infant gut microbiota [51,63]. A placebo-controlled RCT of 52 pregnant women explored the possible effects of GOS supplementation on maternal intestinal microbiota, inflammation and energy pathway [64]. Individuals receiving GOS had an increased level of Paraprevotella and Dorea but less Lachnospiraceae compared to those in the placebo group [64]. Another RCT found a positive correlation between maternal FOS intake and bifidobacterial count in the mothers but not in the neonates [65]. By contrast, a further RCT found no differences in Bifidobacteria and Lactobacilli abundances, alpha and beta diversity between mothers receiving GOS/lcFOS and those receiving placebo [66].
In conclusion, there is currently insufficient evidence to support the practice of maternal supplementation with probiotics or prebiotics to modulate the infant gut microbiome, also considering that these interventions appear to have only a temporary colonization effect that does not remain following the termination of treatment [32,67].
5. Diet and Nutritional Interventions in Early Life
5.1. Milk Feeding in Early Life
The maturation of the gut microbiota in early life is deeply influenced by the methods of infant nutrition, which are breast milk and formula feeding [68]. The type of feeding significantly influences the composition and function of the infant gut microbiota mainly because of differences in nutrient composition, particularly related to the Human Milk Oligosaccharides (HMOs) [69].
5.2. Role of Breastfeeding in Shaping the Infant Gut Microbiome
The primary role of breast feeding in establishing a healthy infant gut microbiome has been increasingly recognized in recent years [5]. Breast milk contains different components, including proteins, fats, carbohydrates, and immunoglobulins [70]. A significant component of breast milk is the HMOs, such as GOS, which undergo only partial digestion in the small intestine, mainly reaching the colon [71]. In the colon, HMOs are fermented, largely by Bifidobacteria, resulting in the production of SCFAs [72] that inhibit the growth of opportunistic pathogens, specifically belonging to the Clostridiaceae, Enterobacteriaceae, and Staphylococcaceae families [25,73,74]. Sakurama and colleagues showed that Bifidobacteria produce an enzyme, lacto-N-biosidase, that contributes to the digestion of GOS [75]. As shown by Matsuki et al. [76], Bifidobacterium numbers increase, HMO content in stool decreases, and the levels of acetic and lactic acid increase in one-month-old infants. Consequently, HMOs exhibit a pronounced prebiotic impact by selectively fostering the growth of a Bifidobacterium-dense microbiota.
Bifidobacteria, particularly the Bifidobacterium infantis, exhibit a direct correlation with the levels of mucosal Immunoglobulin A (IgA) secreted by the gut [77]. Additionally, this bacterium is known for its anti-inflammatory properties.
Therefore, the synergy between HMOs and Bifidobacteria not only enhances the variety and equilibrium of the baby’s intestinal microbiota but is also crucial in supporting the host’s immune system and general well-being. Moreover, remnants of HMO metabolism, such as fucose, lactate, and 1,2 propanediol, as well as aromatic amino acid-derived co-HMO metabolism products like indolelactate and 4-hydroxypheyllactate, are typically present in breastfed (BF) infants [1,78].
Additionally, human milk is also a source of bacteria that colonize the infant gut [79]. Mother-to-infant transmission studies, accounting for both cultured and non-cultured bacteria, provide strong evidence that this bacterial transfer takes place through breastfeeding [24,80]. This transmission has been verified by detecting the same bacterial strains in both maternal milk and the stool of breastfed infants [81]. Furthermore, research by Pannaraj and colleagues [82] suggests that bacterial transmission via breast milk has a more profound influence on the early bacterial colonization of a newborn than the bacteria from the areolar skin.
Human breast milk is comprised of a diverse array of microbiota, encompassing both skin-related and non-skin-related Gram-positive bacterial strains [83]. Notably, Streptococci (specifically S. mitis and S. salivarius) and coagulase-negative Staphylococci prevail in both human milk and stool of breastfed babies [84]. These microorganisms can compete with undesirable pathobionts, such as Staphylococcus aureus, for space and resources within the infant gut.
The origin of the microbial population in breast milk remains uncertain. The entero-mammary pathway theory suggests that immune cells selectively transport bacteria from the gut to the mammary gland [85]. This idea is supported by data indicating a resemblance in the bacterial profiles of a mother’s feces and her breast milk [86]. This hypothesis is further supported by clinical studies finding probiotic strains previously ingested by the mother in her breast milk [87,88].
Infant feeding also influences significantly the host gene expression, as demonstrated by transcriptomic studies conducted on intestinal epithelial cells [89]. It has been observed that breastfeeding increases the transcription of genes related to immunological processes and metabolic functions [89]. Breastfeeding plays a key role in rectifying disruptions in the infant’s gut microbiota resulting from cesarean birth, highlighting its essential function in forming a robust intestinal microbiota, regardless of the method of delivery [90].
5.3. Impact of Breastfeeding Duration and Exclusivity
The duration and exclusivity of breastfeeding are major drivers of infant gut microbiota composition [91]. Both exclusive breastfeeding (EBF), defined as the consumption of only breast milk without any additional formula milk, food, or drink, not even water, and its duration, shape specifically the infant gut microbiota [91,92,93,94]. A meta-analysis of seven studies revealed that during the first 6 months of life non-exclusively breastfed infants exhibited consistently higher gut bacterial diversity and microbiota age compared to exclusively breastfed infants [92]. Furthermore, relative abundances of Bacteroidetes and Firmicutes and their respective energy pathway were consistently higher in non-exclusively breastfed infants [92]. These differences persisted until 2 years of age. In the CHILD study [91], the relationship between exclusive breastfeeding and duration of EBF and the prevalence and relative abundance of different bacteria in the infant gut, represented by amplicon sequencing variants (ASVs), was analyzed, with notable differences in the overall relative abundance of ASVs at 3 and 12 months in exclusive vs. non-exclusive BF. In a recent work by Chichlowski [94], the gut microbiome of EBF infants was less diverse but more stable compared to formula-fed infants. Bifidobacterium, known for selectively using HMOs as growth substrates, was the dominant genus in the infants’ stools at all points in time, regardless of EBF duration. Infants who experienced EBF for more than six months exhibited a greater relative abundance of Bifidobacterium bifidum compared to those who were EBF for less than three months [94].
Laursen identified a positive correlation between the duration of breastfeeding and the occurrence of Bifidobacterium, Veillonella, Megasphaera, Haemophilus, lactic acid bacteria, and Enterobacteriaceae. Conversely, longer breastfeeding duration had a negative effect on the abundance of Lachnospiraceae and Ruminococcaceae, bacteria known for breaking down complex carbohydrates [95].
5.4. Role of Formula Feeding in Shaping the Infant Gut Microbiome
Formula-fed (FF) infants show more diverse colonization compared to their breastfed counterparts [96]. Infants who are FF show a greater prevalence of Clostridiales and Proteobacteria in their gut microbiome [79]. Additionally, the gut microbiota of these infants tends to have a higher concentration of Atopobium and Bacteroides but less Bifidobacteria compared to breastfed infants [97]. Formula feeding has also been observed to decrease the overall quantity of gut bacteria while simultaneously increasing the diversity within the gut microbiome [94,98].
This difference in microbiota composition is primarily attributed to the absence of HMOs and the increased protein content in formula milk. Infant formulas often contain supplemental FOS and/or GOS, but these are not as selective as HMOs [99]. They can stimulate the growth of various bacterial species, leading to a significantly different microbiota composition compared to that seen in breastfed infants [100,101].
Interestingly, the gut microbiota of FF infants, even when the formula contains GOS, show a predominance of proteolytic over saccharolytic metabolism [102,103]. This is evidenced by the elevated concentrations of protein breakdown byproducts [97]. Unfortunately, some of these metabolites can be converted in the liver into detrimental metabolites, such as p-cresol-sulfate and phenylacetateglutamine; these compounds can contribute to enterocyte toxicity, promote inflammation and increased gut permeability and disrupt normal metabolic functions by competing with other substances for sulfation in the liver, a pathway used to detoxify a variety of compounds [104,105].
5.5. How Changes in the Composition of Infant Formula Can Modulate Infant Gut Microbiota
Efforts to promote the development of a gut microbiome in FF infants that closely resembles that of a breastfed infant in order to emulate health advantages conferred by breast milk include the supplementation of infant formula with prebiotics, probiotics or symbiotics [106,107,108], which are synergistic combinations of both.
5.6. Prebiotics
Numerous research efforts have been conducted to explore the impact of prebiotic addition on the composition of the infant gut microbiome [99,109]. Research has demonstrated the advantages of enriching infant formula with HMOs like 2′ fucosyllactose and lacto-N-neotetraose [110]. The goal of this strategy is to replicate the positive impacts that breast milk has on the intestinal microbiota. Initial studies have shown promising results, as the gut microbiota of infants fed with HMO-supplemented formula showed a greater resemblance to that of breastfed infants [111]. These supplements not only support optimal growth in infants, but also promote the growth of beneficial Bifidobacteria, achieving a gut microbial composition closer to that of breastfed infants. The supplementation of infant formula with GOS and FOS can lead to an increased abundance of Bifidobacteria and lower fecal pH, mirroring attributes of breastfed infants [112].
Although infant formula products are engineered to replicate the macronutrient profile of human milk, currently, the majority of them do not incorporate substantial levels of prebiotics and/or probiotics, as reported by Salminen et al. in 2020 [113]. Babies fed with formula enhanced with HMOs exhibited increased Bifidobacteria and decreased Enterobacteriaceae and Peptostreptococcaceae [107]. A study by Borewicz [99] compared the fecal microbiota composition in infants who were breastfed with that of babies fed with an infant formula fortified with prebiotics (GOS and/or FOS) or receiving mixed feeding. These findings were compared with those from infants who were given conventional formulas. By next-generation sequencing analysis, this study demonstrated a bifidogenic effect of prebiotic-fortified formulas as compared to traditional formulas. Infants who were fed formulas fortified with prebiotics showed gut microbiota compositions that were more similar to those found in breastfed babies. This was not the case in formula-fed infants who were given formulas without any added prebiotics. This study also demonstrated lower bifidogenic activity in formulas combined with breastmilk feeding, suggesting a possible interference between the components of the two [99].
The addiction of bovine milk-derived oligosaccharides (MOS) to infant formula was evaluated in a three-arm RCT including a control group fed on regular cow milk-based formula, an experimental group receiving the same formula but with added MOS, and a reference group of exclusively breast milk-fed infants [114]. The overall gut microbiota composition in the experimental group showed more similarities with that of breast milk-fed infants than with the control group. Bifidobacteria were found in higher abundance in the experimental group compared to the control group. Moreover, infants born via cesarean in the experimental group also showed a microbiota composition that was more similar to breast milk-fed and vaginally born infants than to the control group infants. By the age of 4 months, counts of harmful bacteria, Clostridioides difficile and Clostridium perfringens, were significantly reduced in the experimental group than in the control group. The experimental group also showed twice the amount of fecal secretory IgA compared to the control group.
Two comprehensive systematic reviews carried out by Rao et al. [109] and Mugambi [115] examined the effects of adding prebiotics to formula milk. Both showed higher stool colony counts of Bifidobacteria, regardless of differences in dosage, duration of supplementation, and method of reporting results. However, three specific studies using supplementation with GOS, FOS or a GOS/FOS mix found no difference in Bifidobacteria levels between the infant formula-supplemented groups and their controls [116,117,118]. Prebiotic supplementation had an inconsistent impact on [117,118,119,120] while decreasing the levels of C. difficile [121,122]. A double-blinded RCT comparing an infant formula supplemented with a symbiotic composed of bovine MOS and the probiotic Bifidobacterium animalis vs. the same formula alone caused a significant increase in Bifidobacteria abundance and lower microbiota diversity in the experimental group vs. controls, similarly to breastfed infant [123].
5.7. Probiotics
Currently, the most frequently examined and utilized probiotic species belong to the Lactobacillus, Bifidobacterium, and Saccharomyces genera [124,125]. Researchers are also exploring the potential application of bacteria extracted from breast milk to develop infant formulas that closely resemble the nutritional composition of natural breast milk [5]. Supplementation of the formula with Bifidobacterium species and/or lactic acid bacteria, such as Lactobacillus strains, is deemed secure and generally accepted [126,127,128] and may potentially enhance their immune response [129,130].
Studies investigating the effect of probiotic supplementation of infant formulas did not find a strong correlation between fecal Bifidobacterium concentration and Bifidobacterium supplementation [131,132,133]. Bifidobacteria colonization in the infant gut was indeed found to be unstable over time, most likely due to competition among members of the gut microbial [134,135]. This finding has been supported by a systematic review [120] of 12 RCTs, reporting that supplementation of probiotics did not increase the counts of Bifidobacteria or Lactobacilli nor decreased the levels of pathogens such as Bacteroides and E. coli. [115].
In a recent observational study, neonates undergoing varied probiotic administration for six months showed an elevation in stool Bifidobacteria levels only during the first week after birth, implying that probiotics might potentially expedite the initial colonization of this taxon, together with a concomitant reduction in the Enterobacteriaceae family, without differences in alpha diversity [136]. Regardless of the probiotic species, fecal Lactobacillus levels were higher in infants supplemented with a probiotic [136,137]. Another investigation revealed that healthy infants given formula supplemented with Lactobacillus rhamnosus GG (LGG) showed a greater frequency of Lactobacilli colonization compared to those who were fed with a standard formula [138]. Additionally, in very low birth weight infants, the supplementation of Bifidobacterium breve Bb12 favored gut colonization by the added bacteria and expedited the growth of Lactobacilli compared to those infants who did not receive the probiotic supplement [139].
To foster a beneficial gut microbiota, the most opportune time for administering probiotics is prior to the establishment and colonization of individual microbial taxa [140]. This crucial window is typically within the initial months of life. Nonetheless, the colonization timings vary across different microbial taxa [141]. Therefore, identifying these specific periods of opportunity for each taxon is of paramount importance. However, the optimal duration of probiotic supplementation required to guarantee a protracted beneficial impact on gut microbiota remains unclear.
5.8. Introduction of Complementary Foods
During the fourth month of life, the infant’s renal and gastrointestinal systems reach physiological maturation, enabling them to process non-milk alimentary substances [142]. Upon reaching the sixth month, the nutritional and energetic benefits procured solely from breast milk become insufficient to meet the growing metabolic demands of the infant [143]. Thus, the inclusion of complementary food is needed for the appropriate somatic and neurodevelopmental trajectory [142,144].
The implementation of complementary feeding presents a heterogeneous pattern across Europe and worldwide. Certain European regions, exemplified by the UK and Sweden, adhere to the World Health Organization’s endorsement of starting such feeding regimens from six months. However, other territories, including Belgium and Spain, advocate for the initiation of these diets between the fourth and sixth month, a strategy that is in alignment with the guidelines of the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition [145]. According to this committee, the introduction of complementary alimentary substances should not precede the fourth month and should not be delayed beyond the sixth month, including those containing potential allergenic substances.
5.9. Diversity of Solid Food Introduction
Despite remarkable advancements in our knowledge of early-life gut microbial interaction and our growing understanding of the microbial capacity to metabolize various dietary compounds, the understanding of the effects of diet on gut microbiota during the complementary feeding period is still limited [146].
The shift from exclusive milk feeding to the inclusion of family foods in the infant’s diet corresponds with substantial changes in the gut microbiota [147]. During this period, the alpha diversity increases, with a shift from Bifidobacterium-dominant community to Bacteroidetes- and Firmicutes-dominant communities [148]. For instance, there is a rapid decrease in the population of Bifidobacterium species that can degrade HMO [20,149]. Simultaneously, there is a significant increase in diversity and the emergence of Bacteroidaceae, Lachnospiraceae, and Ruminococcaceae species, reflecting the more complex diet that comes with the introduction of fibers and new proteins [150,151]. A longitudinal study by Stewart et al. [152] reported a clear increase in gut microbial diversity after the introduction of solid foods. Further, this increased diversity correlated with enhanced immunological and metabolic development in infants, suggesting the potential health benefits of diverse solid food introduction. A recent study by Pannaraj et al. [82] provided similar findings, reporting the association of diversified solid food intake with the enrichment of specific microbial groups, particularly Bifidobacterium and Bacteroides.
Diverse solid foods act as new sources of microbiota-accessible carbohydrates, therefore stimulating the growth of beneficial taxa such as Bifidobacterium, Lactobacillus, and Bacteroides [153]. These microbes produce SCFAs, such as butyrate, propionate, and acetate, promoting a healthy gut environment and influencing the immune system [154]. The introduction of fruits and vegetables, rich in fermentable fibers, leads to an increase in beneficial microbes like Bacteroides and Bifidobacterium [155]. On the other hand, protein-rich foods like meats and eggs can stimulate proteolytic microbes such as Clostridium and Streptococcus [156]. Hence, the introduction of a diverse diet could ensure a balance between these microbes, leading to a more resilient and healthier gut microbiota.
Since gut microbes primarily derive their energy from dietary fibers and secondarily from proteins/peptides, these macronutrients are likely to have the greatest influence on the microbial composition [49,157]. The primary outputs of metabolizing dietary fiber include SCFAs like acetate, butyrate, and propionate [158,159]. High levels of acetate are generated during the initial stages of infancy, whereas the levels of butyrate and propionate start at a markedly reduced state, subsequently elevating as the infant grows older [9]. Correspondingly, the products of protein degradation, notably branched-chain fatty acids (BCFAs), remain essentially unobservable during the lactation period yet exhibit a parallel trajectory of augmentation with advancing age [95]. These changes align with the beginning of solid food intake and the end of breastfeeding [160]. In agreement with the typical gut microbiota developmental pattern, key species within the Lachnospiraceae and Ruminococcaceae families produce butyrate, while Bacteroides species are common propionate producers [161]. These species possess a comprehensive array of enzymes for breaking down dietary fibers into these SCFAs [162]. Moreover, certain species more abundant in older infants, such as Bacteroides and Clostridium, might employ a range of amino acids derived from dietary proteins to produce BCFAs [163]. Thus, complementary feeding might have a causative effect on microbiota composition and metabolism [69,164].
In a study of nine-month-olds infants, the diversity of gut microbiota was found to increase with the introduction of solid food, particularly fibers and protein, independent of whether the infants were breastfed or formula-fed [165]. A study by Marrs [26] suggests that the introduction of allergenic food, in conjunction with continued breastfeeding between 3 to 6 months of age, resulted in the increase of the overall gut microbiota Shannon diversity. Specifically, this diversification was characterized by the emergence of various microbial taxa, notably Prevotellaceae and Escherichia/Shigella. Of note, the presence of Prevotella has been linked with high-fiber diets [150].
Elevated protein intake has been associated with a heightened abundance of Lachnospiraceae and a decrease in saccharolytic organisms, such as those in the Bifidobacteriaceae family [166]. Simultaneously, the consumption of fiber was linked to an increase in the proportions of Prevotellaceae [167,168].
5.10. Timing of Solid Food Introduction
The timing of complementary food introduction is known to influence gut microbiota composition. A study by Bäckhed et al. [169] suggests that the delayed introduction of solid food could cause a lag in microbial maturation and increase susceptibility to allergies and obesity. On the other hand, an earlier introduction could expose infants to potential pathogens and allergens [170,171,172]. Hence, the timing of solid food introduction should balance between these risks and benefits.
Differding and coworkers found that the introduction of complementary feeding before 3 months of age can lead to enhanced microbial diversity and a higher concentration of fecal butyrate and that these effects may continue up to the age of 12 months [148]. In an RCT comparing traditional spoon feeding to a baby-led approach (involving self-feeding with complementary “finger foods”), the authors found that babies weaned through a baby-led approach were introduced to solid foods approximately 20 days beyond the initial six months (at the age of seven months) [173]. At this age, their consumption of both vegetables and fibrous nutrients was markedly reduced.
By contrast, Laursen and colleagues discovered that the length of time infants were breastfed had a greater influence on both the variety and the proportion of intestinal microbiota and their overall microbial richness at the age of nine months than when they began eating solid complements [147]. This conclusion aligns with the latest findings from Bäckhed et al. [169], which indicate an increase in Lachnospiraceae populations correlating with increased consumption of household meals, as opposed to a decline in Bifidobacteriaceae numbers. This alteration likely mirrors the dietary shift from mother’s milk, which is rich in Bifidobacteriaceae, to solid foods typical of late infancy that are abundant in fiber and protein, thus supporting the growth of Lachnospiraceae species [147].
In another study, Differding and coworkers [174] investigated how the timing of introducing complementary foods can significantly affect the infant’s gut microbiota composition, in turn potentially impacting their gut health and overall nutrition: Ruminococcus bromii, which is able to digest resistant starches [19] was found in greater amounts in infants who were breastfed for less than four months and given complementary foods early. In infants fed with a diet rich in resistant starches, R. bromii could potentially outperform other commensal bacteria that are not as efficient in energy extraction, potentially causing a shift in metabolic processes and dysbiosis. Additionally, these infants had a reduced number of Bifidobacterium animalis, a dominant bacterial species in young gut ecosystems, which generally diminishes with the infant’s growth and the onset of weaning [152,174]. An increased presence of Bifidobacterium animalis may be advantageous for the gastrointestinal health of infants, as indicated by a randomized controlled trial which demonstrated that its supplementation reduced the levels of fecal calprotectin (an indicator of gut inflammation) and decreased gastrointestinal leakiness in infants born before term [175].
6. The Effect of Diet and Nutritional Interventions on Gut Microbiota in Preterm Infants
Preterm infants born earlier than 32 weeks of gestation experience an atypical beginning of life. Their conditions often require placement in nearly sterile incubators, greater frequency of cesarean deliveries, and antibiotic use, combined with the inability to breastfeed, necessitating complex nutritional supplementation and parenteral nutrition that circumvents the gastrointestinal tract [176].
While these measures are crucial for maximizing survival in this susceptible population, they invariably result in an abnormal gut microbiome and altered microbial-host interaction, as compared to full-term infants [177,178]. Preterm infants also have an immature gastrointestinal tract that is abruptly exposed to a wide variety of microbes following birth [178]. Early colonization of the gut in these infants differs significantly from that in term infants, often characterized by lower microbial diversity, lower abundance of Bifidobacteria and Bacteroidetes, higher abundance of Proteobacteria, and greater colonization by pathogens [164,179]. Premature babies greatly benefit from maternal breast milk, which significantly reduces the risk of necrotizing enterocolitis (NEC), a common gastrointestinal disorder among preterm infants [180,181]. However, this does not entirely eliminate the risk, indicating that various other factors, including the variability in the composition of human milk, also play a role. Extremely premature newborns are unable to engage in direct breastfeeding, which leads to the necessity for extracting, cooling, and tube-feeding breast milk. This procedure, unfortunately, can result in an accumulation of harmful bacteria while simultaneously diminishing the presence of protective Bifidobacterium [182,183,184]. Appropriate nutrition, especially in the early stages, is vital for these infants. Studies have shown that early and higher nutrient provision, particularly through the mother’s own milk, not only supports growth [185] but also positively influences clinical outcomes like neurodevelopment and reduces the risk of complications typical of this condition, such as the bronchopulmonary dysplasia and retinopathy of prematurity [186,187,188]. In this context, a secondary analysis of a randomized controlled trial provides further insight into the impact of early versus delayed initiation of enteral feeding on the gut microbiome of extremely preterm infants [189]. This study found that early enteral feeding was associated with an increased presence of three specific bacterial genera in the gut: Bilophila, Veillonella, and Lactococcus. Bilophila species, which can proliferate with dietary changes, have been linked to both beneficial and potentially harmful effects. Veillonella spp., known as colonizers of the oral cavity and gastrointestinal tract, are generally considered harmless and potentially beneficial. Lactococcus, a lactic acid-producing bacteria, is noted for its potential as a probiotic, particularly in reducing the risk of NEC in preterm infants. However, the study did not find evidence that early human milk diets enhance the diversity of the gut microbiome in these infants, possibly due to minimal differences in feeding volumes between early and delayed feeding groups [189].
A prospective longitudinal study [164] evaluated the gut microbiome patterns in preterm infants during their first 30 days of life in the neonatal intensive care unit, finding that the composition of the gut microbiome varied significantly between individuals, with Proteobacteria being the most prevalent phylum. During the first 30 days post-birth, the gut microbiome of these preterm infants demonstrated an initially low diversity index that gradually increased daily. This pattern of microbial community was marked by an increased presence of Clostridium and Bacteroides and a corresponding decline in Staphylococcus and Haemophilus over time [164].
Two primary factors influence the gut microbiome development in preterm infants: time (days since birth) and the intake of breastmilk from their own mothers [190].
Alterations or delayed maturation of gut microbiota, primarily characterized by an increase in Proteobacteria and Firmicutes, have been associated with conditions such as NEC and late-onset sepsis in preterm infants [191].
Infants who are fed their mother’s breast milk have significantly more diverse gut microbiota and a greater abundance of Clostridiales and Lactobacillales than infants who are fed human donor milk and/or formula [164]. Conversely, those infants fed non-mothers breast milk displayed a distinct microbiome community, predominantly marked by Enterobacteriales during their initial 30 days of life [192].
Preterm infants fed by mother’s breast milk do not show a significant increase in Bifidobacteria but display a higher abundance of Firmicutes bacteria [193]. This finding could be explained by the fact that the breast milk produced by mothers of preterm infants differs significantly from that of mothers of full-term infants, which might influence the premature gut differently [194]. Moreover, preterm infants may respond to HMOs in a distinct way compared to full-term infants [195].
The same findings are reported in a study conducted by Cong et al. [164]; they discovered that infants fed with breast milk displayed increased populations of Clostridiales, Lactobacillales, and Bacillales while exhibiting decreased numbers of Enterobacteriaceae. Conversely, infants who were fed with donor human milk and formula milk showed an elevated proportion of Enterobacteriaceae. The study revealed that infants who were breastfed exhibited notably higher alpha diversity in their gut microbiota. In terms of beta diversity, the method of feeding emerged as the primary factor influencing variation, followed by other variables such as gender, gestational age, postnatal age, antibiotic usage, and premature membrane rupture.
6.1. The Role of Diet in Shaping the Gut Microbiota in Preterm Babies
Human milk contains a variety of HMOs that are not found in standard preterm formulas [195]. HMOs have been shown to have critical roles in epithelial function and immune development [196,197]. For instance, disialyllacto-N-tetraose (DSLNT), an HMO, has been associated with protection against NEC [198]. Furthermore, another HMO, 2′-fucosyllactose (2′FL), has been shown to suppress inflammation [105]. Given the crucial role of the gut microbiome in NEC and advancements in sequencing technologies, several studies tried to identify specific bacteria or bacterial combinations associated with NEC onset [199]. However, no consistent bacterial association has been found, although a pattern of higher Proteobacteria abundance and lower Bifidobacterium spp. diversity appears to be frequent in infants with NEC [200].
Recent research correlating the HMO composition in human milk with changes in microbiota evolution shows that low concentrations of DSLNT in the milk are associated with slower progression of microbial maturation, that are typically abundant in Bifidobacterium spp. [198]. These studies underscore the significance of the diet-microbe-host interaction, though it remains challenging to establish causality from observational studies.
A meta-analysis revealed a reduced occurrence of NEC in preterm babies when donor human milk (DHM) was used as the exclusive feed compared to formula milk [201]. Of the two most important RCTs, one indicated a lower incidence of NEC with the use of DHM, while the other reported no notable difference. In a recent RCT by Embleton and coworkers [202], 126 preterm babies were randomly assigned to pasteurized human milk and human milk-derived fortifiers or bovine formula and bovine-derived fortifier, without significant differences in terms of microbiome composition and alpha diversity and in the incidence of NEC or any other key neonatal health problems.
6.2. Effect of Probiotics or Prebiotics to Prevent Morbidity and Mortality in Preterm Infants
Supplementation of probiotics in preterm infants is seen as a potential strategy to assist the initial colonization of the neonatal intestine [203,204]. In addition, probiotic supplementation was reported to have numerous beneficial and anti-inflammatory effects [205,206].
According to a recent systematic review of 67 RCTs and a recent metanalysis of 70 studies, supplementation with probiotics, specifically those containing B. infantis, significantly reduced the risk of NEC, Late-Onset Sepsis (LOS), and all-cause mortality in preterm infants [207,208]. This aligns with the results of another systematic review by Beghetti and coworkers, who observed that a strain of probiotics, B. lactis Bb-12/B94, was associated with reduced risk of NEC in both exclusively human-milk-fed and non-exclusively milk-fed; more favorable results were seen in infants fed exclusively with human milk [203]. However, some concerns and challenges have been identified. There have been rare reports of fungal infections caused by probiotic contamination, indicating a need for stringent pharmaceutical standards for probiotic production and maintenance [205,209].
A systematic review and network meta-analysis [210] highlighted that both single- and multiple-strain probiotics exhibit superior effectiveness compared to a placebo in mitigating mortality and morbidity rates in premature infants, especially a blend of at least one Lactobacillus species and one Bifidobacterium species is the optimal strategy for preventing all-cause mortality and stage II NEC [210].
A meta-analysis conducted by Chi et al. compared the efficacy of different probiotics in premature infants, finding that the combined administration of Lactobacillus, Bifidobacterium, and prebiotics may help to decrease the mortality and morbidity rates associated with NEC and sepsis [211]. Regardless of the potential benefits, specific strains’ safety and effectiveness must be thoroughly evaluated before administration to preterm neonates, due to their vulnerable health status [212].
The American Academy of Pediatrics does not support the regular administration of probiotics in premature infants, citing a lack of conclusive evidence and the absence of FDA regulation, underlining the need for further research to optimize probiotic use in this population [213]. For preterm infants, the Committee on Nutrition of the ESPGHAN and its Working Group on Probiotics and Prebiotics advise the utilization of L. rhamnosus GG (LGG) ATCC 53103 (with daily doses between 1 × 109 CFU to 6 × 109 CFU) and a combination of B. infantis Bb-02, B. lactis Bb-12, and S. thermophilus TH-4 (daily dose of 3.0 to 3.5 × 108 CFU for each strain), as these may lower the incidence of NEC stage 2 or 3 in preterm newborns (though with low certainty in evidence). However, there’s no definitive conclusion on their impact on mortality and sepsis [113,212].
The creation of minimal or synthetic microbiotas, mirroring those found in human milk, is proposed as an innovative strategy to shield the premature infant group from NEC and sepsis, thereby enhancing the survival prospects of preterm babies at earlier stages of gestation [214].
To summarize, probiotics, prebiotics, and symbiotics represent promising interventions to reduce morbidity and mortality among preterm infants [207,210,215,216]. Despite encouraging results, the optimal strains, dosages, and routes of administration remain under investigation. Ongoing research will be crucial in consolidating the role of these therapies, developing precise guidelines for their use, and ultimately improving health outcomes for preterm infants.
7. Conclusions
The infant gut microbiome, a diverse ecosystem of microorganisms, is fundamental to health and well-being throughout life. This complex microbial community is established early in life and undergoes significant changes during infancy. The composition of the infant gut microbiome is influenced by several factors, mostly by diet and other nutrition strategies.
There is increasing evidence that the maternal diet during pregnancy may influence the initial seeding of the infant gut microbiome. While supplementation with probiotics and prebiotics during pregnancy may have some initial effects, it does not appear to have a long-lasting impact on the infant’s gut microbiota. This suggests that a balanced, nutritionally adequate maternal diet may be more important for healthy infant gut microbiome development rather than supplementation alone. Feeding methods in infancy are critical in shaping the gut microbiota. Breastfeeding promotes the growth of Bifidobacteria, contributing to the health of the infant, while formula-fed infants exhibit a more diverse but less stable microbiome, often featuring a higher prevalence of Clostridiales and Proteobacteria. Advances in formula composition, such as the addition of HMOs and prebiotics, are closing this gap, with some formulas resulting in gut microbiota that more closely resemble those of breastfed infants.
When it comes to the introduction of complementary foods, the timing and diversity of foods are of key importance. The transition from a Bifidobacterium-dominant community to one dominated by Bacteroidetes and Firmicutes aligns with this dietary shift. Hence, introducing a diverse range of solid foods can contribute to a well-balanced gut microbiota.
Preterm infants appear to be a specific niche in this context. Born earlier than 32 weeks of gestation, they exhibit lower microbial diversity and a higher abundance of Proteobacteria. However, when fed their mother’s breast milk, the gut microbiota of preterm infants becomes more diverse and abundant in beneficial bacteria such as Bifidobacteria and Lactobacilli. This suggests that breast milk plays a critical role in fostering a healthier gut microbiota, even in preterm infants.
Existing research in this field has several limitations. One significant constraint is the heterogeneity of the studies, which includes variations in the methods used for microbiota determination, dietary recording and the countries involved. Additionally, studies often lack longitudinal designs that would allow for understanding the long-term impacts of early microbiome development. There is also a need for more diverse and large-scale population studies to better understand the variations in gut microbiota across different ethnicities, geographies, and lifestyles. Furthermore, the mechanistic links between the gut microbiome and specific health outcomes in infants are still not fully understood. This diversity in study designs and methodologies presents a challenge in synthesizing a comprehensive understanding of the subject, thus representing another limitation to our current knowledge base. Taken together, these findings and future research directions underscore the need for nutritional guidance during pregnancy, the promotion of breastfeeding where possible, careful consideration of formula composition, and the thoughtful introduction of solid foods. For preterm infants, encouraging maternal breast milk feeding could significantly improve gut microbiota development. Further research should focus on these areas to enhance our understanding and develop effective interventions.
Author Contributions
Conceptualization, G.C. (Giulia Catassi) and G.I.; methodology, G.C. (Giulia Catassi); validation, G.I.; data curation, G.C. (Giulia Catassi) and G.I.; writing—original draft preparation, G.C. (Giulia Catassi) and G.I.; writing—review and editing, G.C. (Giulia Catassi), G.I., M.A., V.G., G.C. (Giovanni Cammarota) and A.G. All authors have read and agreed to the published version of the manuscript.
Funding
The staff of the Fondazione Policlinico Gemelli IRCCS thank the Fondazione Roma for the invaluable support of their scientific research. This work was supported by the Ricerca Finalizzata Giovani Ricercatori 2018 of the Italian Ministry of Health (project GR-2018-12365734) and by the Fondo Italiano per la Scienza 2021 of the Italian Ministry of University and Research (project FIS_00001711) to G.I.; by the BIOMIS grant of the Italian Ministry of Research to A.G., G.C. (Giovanni Cammarota) and G.I. The funders had no role in study design, data collection, and analysis, the decision to publish, or the preparation of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
A.G. reports personal fees for consultancy for Eisai S.r.l., 3PSolutions, Real Time Meeting, Fondazione Istituto Danone, Sinergie S.r.l. Board MRGE and Sanofi S.p.A; personal fees for acting as a speaker for Takeda S.p.A, AbbVie and Sandoz S.p.A; and personal fees for acting on advisory boards for VSL3 and Eisai. G.I. has received personal fees for acting as the speaker for Alfa Sigma, Biocodex, Illumina, Malesci, Sofar and Tillotts Pharma and for acting as consultant/adviser for Biocodex, Malesci, and Tillots Pharma. The other authors have no potential competing interest to disclose.
References
- Tanaka, M.; Nakayama, J. Development of the gut microbiota in infancy and its impact on health in later life. Allergol. Int. 2017, 66, 515–522. [Google Scholar] [CrossRef]
- Turroni, F.; Milani, C.; Duranti, S.; Lugli, G.A.; Bernasconi, S.; Margolles, A.; Di Pierro, F.; Van Sinderen, D.; Ventura, M. The infant gut microbiome as a microbial organ influencing host well-being. Ital. J. Pediatr. 2020, 46, 16. [Google Scholar] [CrossRef]
- Mehta, S.; Huey, S.L.; McDonald, D.; Knight, R.; Finkelstein, J.L. Nutritional Interventions and the Gut Microbiome in Children. Annu. Rev. Nutr. 2021, 41, 479–510. [Google Scholar] [CrossRef] [PubMed]
- Kho, Z.Y.; Lal, S.K. The Human Gut Microbiome—A Potential Controller of Wellness and Disease. Front. Microbiol. 2018, 9, e01835. [Google Scholar] [CrossRef] [PubMed]
- Davis, E.C.; Castagna, V.P.; Sela, D.A.; Hillard, M.A.; Lindberg, S.; Mantis, N.J.; Seppo, A.E.; Järvinen, K.M. Gut microbiome and breast-feeding: Implications for early immune development. J. Allergy Clin. Immunol. 2022, 150, 523–534. [Google Scholar] [CrossRef]
- Yang, I.; Corwin, E.J.; Brennan, P.A.; Jordan, S.; Murphy, J.R.; Dunlop, A. The Infant Microbiome: Implications for Infant Health and Neurocognitive Development. Nurs. Res. 2016, 65, 76–88. [Google Scholar] [CrossRef] [PubMed]
- Ahearn-Ford, S.; Berrington, J.E.; Stewart, C.J. Development of the gut microbiome in early life. Exp. Physiol. 2022, 107, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Kapourchali, F.R.; Cresci, G.A.M. Early-Life Gut Microbiome—The Importance of Maternal and Infant Factors in Its Establishment. Nutr. Clin. Pract. 2020, 35, 386–405. [Google Scholar] [CrossRef]
- Di Profio, E.; Magenes, V.C.; Fiore, G.; Agostinelli, M.; La Mendola, A.; Acunzo, M.; Francavilla, R.; Indrio, F.; Bosetti, A.; D’Auria, E.; et al. Special Diets in Infants and Children and Impact on Gut Microbioma. Nutrients 2022, 14, 3198. [Google Scholar] [CrossRef] [PubMed]
- Layuk, N.; Sinrang, A.W.; Asad, S. Early initiation of breastfeeding and gut microbiota of neonates: A literature review. Med. Clínica Práctica 2021, 4, 100222. [Google Scholar] [CrossRef]
- Homann, C.M. Evaluating the Relationship between Dietary Intake at the Time Immediately before and after the Introduction of Solid Foods and the Gut Microbiome in Full-Term Infants: A Longitudinal Study. Published Online 2020. Available online: https://macsphere.mcmaster.ca/handle/11375/25499 (accessed on 25 July 2023).
- Beller, L.; Deboutte, W.; Falony, G.; Vieira-Silva, S.; Tito, R.Y.; Valles-Colomer, M.; Rymenans, L.; Jansen, D.; Van Espen, L.; Papadaki, M.I.; et al. Successional Stages in Infant Gut Microbiota Maturation. mBio 2021, 12, e01857-21. [Google Scholar] [CrossRef]
- Gritz, E.C.; Bhandari, V. The human neonatal gut microbiome: A brief review. Front. Pediatr. 2015, 3, 17. [Google Scholar] [CrossRef] [PubMed]
- Penders, J.; Thijs, C.; Vink, C.; Stelma, F.F.; Snijders, B.; Kummeling, I.; van den Brandt, P.A.; Stobberingh, E.E. Factors influencing the composition of the intestinal microbiota in early infancy. Pediatrics 2006, 118, 511–521. [Google Scholar] [CrossRef]
- Chong, C.Y.L.; Bloomfield, F.H.; O’Sullivan, J.M. Factors Affecting Gastrointestinal Microbiome Development in Neonates. Nutrients 2018, 10, 274. [Google Scholar] [CrossRef] [PubMed]
- Collado, M.C.; Rautava, S.; Aakko, J.; Isolauri, E.; Salminen, S. Human gut colonisation may be initiated in utero by distinct microbial communities in the placenta and amniotic fluid. Sci. Rep. 2016, 6, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Q.; Li, T.; Chen, W.; Huo, Y.; Mou, X.; Zhao, W. Microbial regulation of offspring diseases mediated by maternal-associated microbial metabolites. Front. Microbiol. 2022, 13, 955297. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Cai, X.; Ye, Y.; Wang, F.; Chen, F.; Zheng, C. The Role of Microbiota in Infant Health: From Early Life to Adulthood. Front. Immunol. 2021, 12, 708472. [Google Scholar] [CrossRef]
- Xiao, L.; Wang, J.; Zheng, J.; Li, X.; Zhao, F. Deterministic transition of enterotypes shapes the infant gut microbiome at an early age. Genome Biol. 2021, 22, 243. [Google Scholar] [CrossRef]
- McKeen, S.; Roy, N.C.; Mullaney, J.A.; Eriksen, H.; Lovell, A.; Kussman, M.; Young, W.; Fraser, K.; Wall, C.R.; McNabb, W.C. Adaptation of the infant gut microbiome during the complementary feeding transition. PLoS ONE 2022, 17, e0270213. [Google Scholar] [CrossRef]
- Lugli, G.A.; Mancabelli, L.; Milani, C.; Fontana, F.; Tarracchini, C.; Alessandri, G.; van Sinderen, D.; Turroni, F.; Ventura, M. Comprehensive insights from composition to functional microbe-based biodiversity of the infant human gut microbiota. NPJ Biofilms Microbiomes 2023, 9, 25. [Google Scholar] [CrossRef]
- Avershina, E.; Lundgård, K.; Sekelja, M.; Dotterud, C.; Storrø, O.; Øien, T.; Johnsen, R.; Rudi, K. Transition from infant- to adult-like gut microbiota. Environ. Microbiol. 2016, 18, 2226–2236. [Google Scholar] [CrossRef]
- Coker, M.O.; Laue, H.E.; Hoen, A.G.; Hilliard, M.; Dade, E.; Li, Z.; Palys, T.; Morrison, H.G.; Baker, E.; Karagas, M.R.; et al. Infant Feeding Alters the Longitudinal Impact of Birth Mode on the Development of the Gut Microbiota in the First Year of Life. Front. Microbiol. 2021, 12, 642197. [Google Scholar] [CrossRef]
- Yang, L.; Sakandar, H.A.; Sun, Z.; Zhang, H. Recent advances of intestinal microbiota transmission from mother to infant. J. Funct. Foods. 2021, 87, 104719. [Google Scholar] [CrossRef]
- Laursen, M.F. Gut Microbiota Development: Influence of Diet from Infancy to Toddlerhood. Ann. Nutr. Metab. 2021, 77 (Suppl. 3), 21–34. [Google Scholar] [CrossRef]
- Marrs, T.; Jo, J.H.; Perkin, M.R.; Rivett, D.W.; Witney, A.A.; Bruce, K.D.; Logan, K.; Craven, J.; Radulovic, S.; Versteeg, S.A.; et al. Gut microbiota development during infancy: Impact of introducing allergenic foods. J. Allergy Clin. Immunol. 2021, 147, 613–621.e9. [Google Scholar] [CrossRef]
- Wernroth, M.L.; Peura, S.; Hedman, A.M.; Hetty, S.; Vicenzi, S.; Kennedy, B.; Fall, K.; Svennblad, B.; Andolf, E.; Pershagen, G.; et al. Development of gut microbiota during the first 2 years of life. Sci. Rep. 2022, 12, 9080. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Bahl, R.; Barros, A.J.; França, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [PubMed]
- Rollins, N.C.; Bhandari, N.; Hajeebhoy, N.; Horton, S.; Lutter, C.K.; Martines, J.C.; Piwoz, E.G.; Richter, L.M.; Victora, C.G. Why invest, and what it will take to improve breastfeeding practices? Lancet 2016, 387, 491–504. [Google Scholar] [CrossRef]
- World Health Organization. Infant and Young Child Feeding. Published Online 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding (accessed on 20 December 2023).
- UNICEF. Breastfeeding, A Mother’s Gift, for Every Child. Published Online 2018. Available online: https://www.unicef.org/media/48046/file/UNICEF_Breastfeeding_A_Mothers_Gift_for_Every_Child.pdf (accessed on 1 January 2018).
- Grech, A.; Collins, C.E.; Holmes, A.; Lal, R.; Duncanson, K.; Taylor, R.; Gordon, A. Maternal exposures and the infant gut microbiome: A systematic review with meta-analysis. Gut Microbes 2021, 13, 1897210. [Google Scholar] [CrossRef] [PubMed]
- Maher, S.E.; O’Brien, E.C.; Moore, R.L.; Byrne, D.F.; Geraghty, A.A.; Saldova, R.; Murphy, E.F.; Van Sinderen, D.; Cotter, P.D.; McAuliffe, F.M. The association between the maternal diet and the maternal and infant gut microbiome: A systematic review. Br. J. Nutr. 2020, 129, 1491–1499. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.; Keane, D.; Borrego, P.; Arcaro, K. Effect of Maternal Diet on Maternal Milk and Breastfed Infant Gut Microbiomes: A Scoping Review. Nutrients 2023, 15, 1420. [Google Scholar] [CrossRef]
- Sindi, A.S.; Stinson, L.F.; Lean, S.S.; Chooi, Y.H.; Leghi, G.E.; Netting, M.J.; Wlodek, M.E.; Muhlhausler, B.S.; Geddes, D.T.; Payne, M.S. Effect of a reduced fat and sugar maternal dietary intervention during lactation on the infant gut microbiome. Front. Microbiol. 2022, 13, 900702. [Google Scholar] [CrossRef] [PubMed]
- Cortes-Macías, E.; Selma-Royo, M.; García-Mantrana, I.; Calatayud, M.; González, S.; Martínez-Costa, C.; Collado, M.C. Maternal Diet Shapes the Breast Milk Microbiota Composition and Diversity: Impact of Mode of Delivery and Antibiotic Exposure. J. Nutr. 2021, 151, 330–340. [Google Scholar] [CrossRef] [PubMed]
- Simione, M.; Harshman, S.G.; Castro, I.; Linnemann, R.; Roche, B.; Ajami, N.J.; Petrosino, J.F.; Raspini, B.; Portale, S.; Camargo, C.A., Jr.; et al. Maternal Fish Consumption in Pregnancy Is Associated with a Bifidobacterium-Dominant Microbiome Profile in Infants. Curr. Dev. Nutr. 2020, 4, nzz133. [Google Scholar] [CrossRef] [PubMed]
- Urwin, H.J.; Miles, E.A.; Noakes, P.S.; Kremmyda, L.S.; Vlachava, M.; Diaper, N.D.; Godfrey, K.M.; Calder, P.C.; Vulevic, J.; Yaqoob, P. Effect of salmon consumption during pregnancy on maternal and infant faecal microbiota, secretory IgA and calprotectin. Br. J. Nutr. 2014, 111, 773–784. [Google Scholar] [CrossRef] [PubMed]
- García-Mantrana, I.; Selma-Royo, M.; González, S.; Parra-Llorca, A.; Martínez-Costa, C.; Collado, M.C. Distinct maternal microbiota clusters are associated with diet during pregnancy: Impact on neonatal microbiota and infant growth during the first 18 months of life. Gut Microbes 2020, 11, 962–978. [Google Scholar] [CrossRef] [PubMed]
- Litonjua, A.A.; Lange, N.E.; Carey, V.J.; Brown, S.; Laranjo, N.; Harshfield, B.J.; O’Connor, G.T.; Sandel, M.; Strunk, R.C.; Bacharier, L.B.; et al. The Vitamin D Antenatal Asthma Reduction Trial (VDAART): Rationale, design, and methods of a randomized, controlled trial of vitamin D supplementation in pregnancy for the primary prevention of asthma and allergies in children. Contemp. Clin. Trials 2014, 38, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Savage, J.H.; Lee-Sarwar, K.A.; Sordillo, J.E.; Lange, N.E.; Zhou, Y.; O’Connor, G.T.; Sandel, M.; Bacharier, L.B.; Zeiger, R.; Sodergren, E.; et al. Diet during Pregnancy and Infancy and the Infant Intestinal Microbiome. J. Pediatr. 2018, 203, 47–54.e4. [Google Scholar] [CrossRef]
- Litonjua, A.A.; Carey, V.J.; Laranjo, N.; Stubbs, B.J.; Mirzakhani, H.; O’Connor, G.T.; Sandel, M.; Beigelman, A.; Bacharier, L.B.; Zeiger, R.S.; et al. Six-Year Follow-up of a Trial of Antenatal Vitamin D for Asthma Reduction. N. Engl. J. Med. 2020, 382, 525–533. [Google Scholar] [CrossRef]
- Scheepers, L.E.J.M.; Penders, J.; Mbakwa, C.A.; Thijs, C.; Mommers, M.; Arts, I.C.W. The intestinal microbiota composition and weight development in children: The KOALA Birth Cohort Study. Int. J. Obes. 2014, 39, 16–25. [Google Scholar] [CrossRef]
- Chu, D.M.; Antony, K.M.; Ma, J.; Prince, A.L.; Showalter, L.; Moller, M.; Aagaard, K.M. The early infant gut microbiome varies in association with a maternal high-fat diet. Genome Med. 2016, 8, 1–2. [Google Scholar] [CrossRef]
- Al Rubaye, H.; Adamson, C.C.; Jadavji, N.M. The role of maternal diet on offspring gut microbiota development: A review. J. Neurosci. Res. 2021, 99, 284–293. [Google Scholar] [CrossRef]
- Lundgren, S.N.; Madan, J.C.; Emond, J.A.; Morrison, H.G.; Christensen, B.C.; Karagas, M.R.; Hoen, A.G. Maternal diet during pregnancy is related with the infant stool microbiome in a delivery mode-dependent manner. Microbiome 2018, 6. [Google Scholar] [CrossRef] [PubMed]
- Fan, H.Y.; Tung, Y.T.; Yang, Y.C.; Hsu, J.B.; Lee, C.Y.; Chang, T.H.; Su, E.C.; Hsieh, R.H.; Chen, Y.C. Maternal Vegetable and Fruit Consumption during Pregnancy and Its Effects on Infant Gut Microbiome. Nutrients 2021, 13, 1559. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.; Dissertation, K.; Zivkovic, A.M.; Steinberg, F.M.; German, J.B. The Role of Targeted Prebiotics for Improving Gut Microbiome Composition and Function in Individuals Consuming Diets Low in Fiber, and Individuals at Risk for Chronic Disease; University of California: Davis, CA, USA, 2022. [Google Scholar]
- Calatayud, M.; Van den Abbeele, P.; Ghyselinck, J.; Marzorati, M.; Rohs, E.; Birkett, A. Comparative Effect of 22 Dietary Sources of Fiber on Gut Microbiota of Healthy Humans in vitro. Front. Nutr. 2021, 8, 700571. [Google Scholar] [CrossRef] [PubMed]
- Fusco, W.; Lorenzo, M.B.; Cintoni, M.; Porcari, S.; Rinninella, E.; Kaitsas, F.; Lener, E.; Mele, M.C.; Gasbarrini, A.; Collado, M.C.; et al. Short-Chain Fatty-Acid-Producing Bacteria: Key Components of the Human Gut Microbiota. Nutrients 2023, 15, 2211. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, A.Z.; Moore, S.E.; Okala, S.G. Impact of maternal nutritional supplementation during pregnancy and lactation on the infant gut or breastmilk microbiota: A systematic review. Nutrients 2021, 13, 1137. [Google Scholar] [CrossRef] [PubMed]
- Sanz, Y. Gut microbiota and probiotics in maternal and infant health. Am. J. Clin. Nutr. 2011, 94, S2000–S2005. [Google Scholar] [CrossRef] [PubMed]
- Dotterud, C.K.; Avershina, E.; Sekelja, M.; Simpson, M.R.; Rudi, K.; Storrø, O.; Johnsen, R.; Øien, T. Does maternal perinatal probiotic supplementation alter the intestinal microbiota of mother and child? J. Pediatr. Gastroenterol. Nutr. 2015, 61, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Rutten, N.B.M.M.; Gorissen, D.M.W.; Eck, A.; Niers, L.E.M.; Vlieger, A.M.; Besseling-Van Der Vaart, I.; Budding, A.E.; Savelkoul, P.H.M.; Van Der Ent, C.K.; Rijkers, G.T. Long Term Development of Gut Microbiota Composition in Atopic Children: Impact of Probiotics. PLoS ONE 2015, 10, e0137681. [Google Scholar] [CrossRef]
- Murphy, R.; Morgan, X.; Wang, X.; Wickens, K.; Purdie, G.; Fitzharris, P.; Otal, A.; Lawley, B.; Stanley, T.; Barthow, C.; et al. Eczema-protective probiotic alters infant gut microbiome functional capacity but not composition: Sub-sample analysis from a RCT. Benef. Microbes 2019, 10, 5–17. [Google Scholar] [CrossRef]
- Grönlund, M.M.; Grzeskowiak, Ł.; Isolauri, E.; Salminen, S. Influence of mother’s intestinal microbiota on gut colonization in the infant. Gut Microbes 2011, 2, 227–233. [Google Scholar] [CrossRef]
- Wickens, K.; Black, P.N.; Stanley, T.V.; Mitchell, E.; Fitzharris, P.; Tannock, G.W.; Purdie, G.; Crane, J. A differential effect of 2 probiotics in the prevention of eczema and atopy: A double-blind, randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 2008, 122, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.L.; Geraghty, A.A.; Feehily, C.; Saldova, R.; Murphy, E.F.; Van Sinderen, D.; Cotter, P.D.; McAuliffe, F.M. Can a probiotic supplement in pregnancy result in transfer to the neonatal gut: A systematic review. Acta Obstet. Gynecol. Scand. 2020, 99, 1269–1277. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Li, Z.; Tye, K.D.; Chan, S.N.; Tang, X.; Luo, H.; Wang, D.; Zhou, J.; Duan, X.; Xiao, X. Probiotic supplementation during pregnancy alters gut microbial networks of pregnant women and infants. Front. Microbiol. 2022, 13, 1042846. [Google Scholar] [CrossRef]
- Kristensen, N.B.; Bryrup, T.; Allin, K.H.; Nielsen, T.; Hansen, T.H.; Pedersen, O. Alterations in fecal microbiota composition by probiotic supplementation in healthy adults: A systematic review of randomized controlled trials. Genome Med. 2016, 8, 1–11. [Google Scholar] [CrossRef]
- Singh, A.; Sarangi, A.N.; Goel, A.; Srivastava, R.; Bhargava, R.; Gaur, P.; Aggarwal, A.; Aggarwal, R. Effect of administration of a probiotic preparation on gut microbiota and immune response in healthy women in India: An open-label, single-arm pilot study. BMC Gastroenterol. 2018, 18, 85. [Google Scholar] [CrossRef] [PubMed]
- Ismail, I.H.; Oppedisano, F.; Joseph, S.J.; Boyle, R.J.; Robins-Browne, R.M.; Tang, M.L.K. Prenatal administration of Lactobacillus rhamnosus has no effect on the diversity of the early infant gut microbiota. Pediatr. Allergy Immunol. 2012, 23, 255–258. [Google Scholar] [CrossRef]
- Hughes, R.L.; Arnold, C.D.; Young, R.R.; Ashorn, P.; Maleta, K.; Fan, Y.-M.; Ashorn, U.; Chaima, D.; Malamba-Banda, C.; Kable, M.E.; et al. Infant gut microbiota characteristics generally do not modify effects of lipid-based nutrient supplementation on growth or inflammation: Secondary analysis of a randomized controlled trial in Malawi. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Wan, J.; An, L.; Ren, Z.; Wang, S.; Yang, H.; Ma, J. Effects of galactooligosaccharides on maternal gut microbiota, glucose metabolism, lipid metabolism and inflammation in pregnancy: A randomized controlled pilot study. Front. Endocrinol. 2023, 14, 1034266. [Google Scholar] [CrossRef]
- Jinno, S.; Toshimitsu, T.; Nakamura, Y.; Kubota, T.; Igoshi, Y.; Ozawa, N.; Suzuki, S.; Nakano, T.; Morita, Y.; Arima, T.; et al. Maternal Prebiotic Ingestion Increased the Number of Fecal Bifidobacteria in Pregnant Women but Not in Their Neonates Aged One Month. Nutrients 2017, 9, 196. [Google Scholar] [CrossRef]
- Shadid, R.; Haarman, M.; Knol, J.; Theis, W.; Beermann, C.; Rjosk-Dendorfer, D.; Schendel, D.J.; Koletzko, B.V.; Krauss-Etschmann, S. Effects of galactooligosaccharide and long-chain fructooligosaccharide supplementation during pregnancy on maternal and neonatal microbiota and immunity—A randomized, double-blind, placebo-controlled study. Am. J. Clin. Nutr. 2007, 86, 1426–1437. [Google Scholar] [CrossRef]
- Cuinat, C.; Stinson, S.E.; Ward, W.E.; Comelli, E.M. Maternal Intake of Probiotics to Program Offspring Health. Curr. Nutr. Rep. 2022, 11, 537–562. [Google Scholar] [CrossRef]
- Rey-Mariño, A.; Francino, M.P. Nutrition, Gut Microbiota, and Allergy Development in Infants. Nutrients 2022, 14, 4316. [Google Scholar] [CrossRef]
- Laursen, M.F.; Bahl, M.I.; Michaelsen, K.F.; Licht, T.R. First Foods and Gut Microbes. Front. Microbiol. 2017, 8, 356. [Google Scholar] [CrossRef] [PubMed]
- Ballard, O.; Morrow, A.L. Human milk composition: Nutrients and bioactive factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [PubMed]
- Cuxart, I.; Coines, J.; Esquivias, O.; Faijes, M.; Planas, A.; Biarnés, X.; Rovira, C. Enzymatic Hydrolysis of Human Milk Oligosaccharides. The Molecular Mechanism of Bifidobacterium Bifidum Lacto-N-biosidase. ACS Catal. 2022, 12, 4737–4743. [Google Scholar] [CrossRef] [PubMed]
- Lawson, M.A.E.; O’neill, I.J.; Kujawska, M.; Javvadi, S.G.; Wijeyesekera, A.; Flegg, Z.; Chalklen, L.; Hall, L.J. Breast milk-derived human milk oligosaccharides promote Bifidobacterium interactions within a single ecosystem. ISME J. 2019, 14, 635–648. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, S.; Toh, H.; Hase, K.; Oshima, K.; Nakanishi, Y.; Yoshimura, K.; Tobe, T.; Clarke, J.M.; Topping, D.L.; Suzuki, T.; et al. Bifidobacteria can protect from enteropathogenic infection through production of acetate. Nature 2011, 469, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Sakurama, H.; Kiyohara, M.; Wada, J.; Honda, Y.; Yamaguchi, M.; Fukiya, S.; Yokota, A.; Ashida, H.; Kumagai, H.; Kitaoka, M.; et al. Lacto-N-biosidase Encoded by a Novel Gene of Bifidobacterium longum Subspecies longum Shows Unique Substrate Specificity and Requires a Designated Chaperone for Its Active Expression. J. Biol. Chem. 2013, 288, 25194–25206. [Google Scholar] [CrossRef] [PubMed]
- Wada, J.; Ando, T.; Kiyohara, M.; Ashida, H.; Kitaoka, M.; Yamaguchi, M.; Kumagai, H.; Katayama, T.; Yamamoto, K. Bifidobacterium bifidum Lacto-N-Biosidase, a Critical Enzyme for the Degradation of Human Milk Oligosaccharides with a Type 1 Structure. Appl. Environ. Microbiol. 2008, 74, 3996. [Google Scholar] [CrossRef]
- Matsuki, T.; Yahagi, K.; Mori, H.; Matsumoto, H.; Hara, T.; Tajima, S.; Ogawa, E.; Kodama, H.; Yamamoto, K.; Yamada, T.; et al. A key genetic factor for fucosyllactose utilization affects infant gut microbiota development. Nat. Commun. 2016, 7, 1–12. [Google Scholar] [CrossRef]
- Wickramasinghe, S.; Pacheco, A.R.; Lemay, D.G.; Mills, D.A. Bifidobacteria grown on human milk oligosaccharides downregulate the expression of inflammation-related genes in Caco-2 cells. BMC Microbiol. 2015, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Saturio, S.; Nogacka, A.M.; Alvarado-Jasso, G.M.; Salazar, N.; Reyes-Gavilán, C.G.d.L.; Gueimonde, M.; Arboleya, S. Role of Bifidobacteria on Infant Health. Microorganisms 2021, 9, 2415. [Google Scholar] [CrossRef] [PubMed]
- Boudry, G.; Charton, E.; Le Huerou-Luron, I.; Ferret-Bernard, S.; Le Gall, S.; Even, S.; Blat, S. The Relationship between Breast Milk Components and the Infant Gut Microbiota. Front. Nutr. 2021, 8, 629740. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, P.; Pasolli, E.; Tett, A.; Asnicar, F.; Gorfer, V.; Fedi, S.; Armanini, F.; Truong, D.T.; Manara, S.; Zolfo, M.; et al. Mother-to-Infant Microbial Transmission from Different Body Sites Shapes the Developing Infant Gut Microbiome. Cell Host Microbe 2018, 24, 133–145.e5. [Google Scholar] [CrossRef] [PubMed]
- Yassour, M.; Jason, E.; Hogstrom, L.J.; Arthur, T.D.; Tripathi, S.; Siljander, H.; Selvenius, J.; Oikarinen, S.; Hyöty, H.; Virtanen, S.M.; et al. Strain-Level Analysis of Mother-to-Child Bacterial Transmission during the First Few Months of Life. Cell Host Microbe 2018, 24, 146–154.e4. [Google Scholar] [CrossRef] [PubMed]
- Pannaraj, P.S.; Li, F.; Cerini, C.; Bender, J.M.; Yang, S.; Rollie, A.; Adisetiyo, H.; Zabih, S.; Lincez, P.J.; Bittinger, K.; et al. Association Between Breast Milk Bacterial Communities and Establishment and Development of the Infant Gut Microbiome. JAMA Pediatr. 2017, 171, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Notarbartolo, V.; Giuffrè, M.; Montante, C.; Corsello, G.; Carta, M. Composition of Human Breast Milk Microbiota and Its Role in Children’s Health. Pediatr. Gastroenterol. Hepatol. Nutr. 2022, 25, 194–210. [Google Scholar] [CrossRef]
- Guo, W.; Liu, S.; Khan, M.Z.; Wang, J.; Chen, T.; Alugongo, G.M.; Li, S.; Cao, Z. Bovine milk microbiota: Key players, origins, and potential contributions to early-life gut development. J. Adv. Res. 2023. ISSN 2090-1232. [Google Scholar] [CrossRef]
- Selvamani, S.; Dailin, D.J.; Gupta, V.K.; Wahid, M.; Keat, H.C.; Natasya, K.H.; Malek, R.A.; Haque, S.; Sayyed, R.Z.; Abomoelak, B.; et al. An Insight into Probiotics Bio-Route: Translocation from the Mother’s Gut to the Mammary Gland. Appl. Sci. 2021, 11, 7247. [Google Scholar] [CrossRef]
- Rodríguez, J.M. The Origin of Human Milk Bacteria: Is There a Bacterial Entero-Mammary Pathway during Late Pregnancy and Lactation? Adv. Nutr. 2014, 5, 779. [Google Scholar] [CrossRef] [PubMed]
- Simpson, M.R.; Avershina, E.; Storrø, O.; Johnsen, R.; Rudi, K.; Øien, T. Breastfeeding-associated microbiota in human milk following supplementation with Lactobacillus rhamnosus GG, Lactobacillus acidophilus La-5, and Bifidobacterium animalis ssp. lactis Bb-12. J. Dairy Sci. 2018, 101, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, H.; Rodríguez, J.M.; Salminen, S.; Szajewska, H. Probiotics in human milk and probiotic supplementation in infant nutrition: A workshop report. Br. J. Nutr. 2014, 112, 1119–1128. [Google Scholar] [CrossRef]
- Komatsu, Y.; Kumakura, D.; Seto, N.; Izumi, H.; Takeda, Y.; Ohnishi, Y.; Nakaoka, S.; Aizawa, T. Dynamic Associations of Milk Components With the Infant Gut Microbiome and Fecal Metabolites in a Mother–Infant Model by Microbiome, NMR Metabolomic, and Time-Series Clustering Analyses. Front. Nutr. 2022, 8, 813690. [Google Scholar] [CrossRef]
- Liu, Y.; Qin, S.; Song, Y.; Feng, Y.; Lv, N.; Xue, Y.; Liu, F.; Wang, S.; Zhu, B.; Ma, J.; et al. The Perturbation of Infant Gut Microbiota Caused by Cesarean Delivery Is Partially Restored by Exclusive Breastfeeding. Front. Microbiol. 2019, 10, 598. [Google Scholar] [CrossRef]
- Fehr, K.; Moossavi, S.; Sbihi, H.; Boutin, R.C.; Bode, L.; Robertson, B.; Yonemitsu, C.; Field, C.J.; Becker, A.B.; Mandhane, P.J.; et al. Breastmilk Feeding Practices Are Associated with the Co-Occurrence of Bacteria in Mothers’ Milk and the Infant Gut: The CHILD Cohort Study. Cell Host Microbe 2020, 28, 285–297.e4. [Google Scholar] [CrossRef]
- Ho, N.T.; Li, F.; Lee-Sarwar, K.A.; Tun, H.M.; Brown, B.; Pannaraj, P.S.; Bender, J.M.; Azad, M.B.; Thompson, A.L.; Weiss, S.T.; et al. Meta-analysis of effects of exclusive breastfeeding on infant gut microbiota across populations. Nat. Commun. 2018, 9, 1–13. [Google Scholar] [CrossRef]
- Li, Y.; Ren, L.; Wang, Y.; Li, J.; Zhou, Q.; Peng, C.; Li, Y.; Cheng, R.; He, F.; Shen, X. The Effect of Breast Milk Microbiota on the Composition of Infant Gut Microbiota: A Cohort Study. Nutrients 2022, 14, 5397. [Google Scholar] [CrossRef]
- Chichlowski, M.; van Diepen, J.A.; Prodan, A.; Olga, L.; Ong, K.K.; Kortman, G.A.M.; Dunger, D.B.; Gross, G. Early development of infant gut microbiota in relation to breastfeeding and human milk oligosaccharides. Front. Nutr. 2023, 10, 1003032. [Google Scholar] [CrossRef]
- Laursen, M.F.; Sakanaka, M.; von Burg, N.; Mörbe, U.; Andersen, D.; Moll, J.M.; Pekmez, C.T.; Rivollier, A.; Michaelsen, K.F.; Mølgaard, C.; et al. Bifidobacterium species associated with breastfeeding produce aromatic lactic acids in the infant gut. Nat. Microbiol. 2021, 6, 1367–1382. [Google Scholar] [CrossRef]
- Hascoët, J.; Hubert, C.; Rochat, F.; Legagneur, H.; Gaga, S.; Emady-Azar, S.; Steenhout, P.G. Effect of formula composition on the development of infant gut microbiota. J. Pediatr. Gastroenterol. Nutr. 2011, 52, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Li, Z.; Zhang, W.; Zhang, C.; Zhang, Y.; Mei, H.; Zhuo, N.; Wang, H.; Wang, L.; Wu, D. Comparison of gut microbiota in exclusively breast-fed and formula-fed babies: A study of 91 term infants. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Fabiano, V.; Indrio, F.; Verduci, E.; Calcaterra, V.; Pop, T.L.; Mari, A.; Zuccotti, G.V.; Cokugras, F.C.; Pettoello-Mantovani, M.; Goulet, O. Term Infant Formulas Influencing Gut Microbiota: An Overview. Nutrients 2021, 13, 4200. [Google Scholar] [CrossRef] [PubMed]
- Borewicz, K.; Suarez-Diez, M.; Hechler, C.; Beijers, R.; de Weerth, C.; Arts, I.; Penders, J.; Thijs, C.; Nauta, A.; Lindner, C.; et al. The effect of prebiotic fortified infant formulas on microbiota composition and dynamics in early life. Sci. Rep. 2019, 9, 1–13. [Google Scholar] [CrossRef]
- Hill, C.J.; Lynch, D.B.; Murphy, K.; Ulaszewska, M.; Jeffery, I.B.; O’shea, C.A.; Watkins, C.; Dempsey, E.; Mattivi, F.; Tuohy, K.; et al. Evolution of gut microbiota composition from birth to 24 weeks in the INFANTMET Cohort. Microbiome 2017, 5, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Béghin, L.; Tims, S.; Roelofs, M.; Rougé, C.; Oozeer, R.; Rakza, T.; Chirico, G.; Roeselers, G.; Knol, J.; Rozé, J.C.; et al. Fermented infant formula (with Bifidobacterium breve C50 and Streptococcus thermophilus O65) with prebiotic oligosaccharides is safe and modulates the gut microbiota towards a microbiota closer to that of breastfed infants. Clin. Nutr. 2021, 40, 778–787. [Google Scholar] [CrossRef]
- He, X.; Parenti, M.; Grip, T.; Lönnerdal, B.; Timby, N.; Domellöf, M.; Hernell, O.; Slupsky, C.M. Fecal microbiome and metabolome of infants fed bovine MFGM supplemented formula or standard formula with breast-fed infants as reference: A randomized controlled trial. Sci. Rep. 2019, 9, 11589. [Google Scholar] [CrossRef]
- Chow, J.; Panasevich, M.R.; Alexander, D.; Boler, B.M.V.; Serao, M.C.R.; Faber, T.A.; Bauer, L.L.; Fahey, G.C. Fecal Metabolomics of Healthy Breast-Fed versus Formula-Fed Infants before and during In Vitro Batch Culture Fermentation. J. Proteome Res. 2014, 13, 2534–2542. [Google Scholar] [CrossRef]
- Roager, H.M.; Stanton, C.; Hall, L.J. Microbial metabolites as modulators of the infant gut microbiome and host-microbial interactions in early life. Gut Microbes 2023, 15, 2192151. [Google Scholar] [CrossRef]
- Yao, Q.; Li, H.; Gao, Y.; Zheng, N.; Delcenserie, V.; Wang, J. The Milk Active Ingredient, 2′-Fucosyllactose, Inhibits Inflammation and Promotes MUC2 Secretion in LS174T Goblet Cells In Vitro. Foods 2023, 12, 186. [Google Scholar] [CrossRef] [PubMed]
- Lemoine, A.; Tounian, P.; Adel-Patient, K.; Thomas, M. Pre-, pro-, syn-, and Postbiotics in Infant Formulas: What Are the Immune Benefits for Infants? Nutrients 2023, 15, 1231. [Google Scholar] [CrossRef] [PubMed]
- Holst, A.Q.; Myers, P.; Rodríguez-García, P.; Hermes, G.D.A.; Melsaether, C.; Baker, A.; Jensen, S.R.; Parschat, K. Infant Formula Supplemented with Five Human Milk Oligosaccharides Shifts the Fecal Microbiome of Formula-Fed Infants Closer to That of Breastfed Infants. Nutrients 2023, 15, 3087. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Li, L.Q.; Liu, F.; Wu, J.Y. Human milk oligosaccharides and infant gut microbiota: Molecular structures, utilization strategies and immune function. Carbohydr. Polym. 2022, 276, 118738. [Google Scholar] [CrossRef]
- Rao, S.; Srinivasjois, R.; Patole, S. Prebiotic supplementation in full-term neonates: A systematic review of randomized controlled trials. Arch. Pediatr. Adolesc. Med. 2009, 163, 755–764. [Google Scholar] [CrossRef]
- Dinleyici, M.; Barbieur, J.; Dinleyici, E.C.; Vandenplas, Y. Functional effects of human milk oligosaccharides (HMOs). Gut Microbes 2023, 15, 2186115. [Google Scholar] [CrossRef]
- Natividad, J.M.; Marsaux, B.; Rodenas, C.L.; Rytz, A.; Vandevijver, G.; Marzorati, M.; Van den Abbeele, P.; Calatayud, M.; Rochat, F. Human Milk Oligosaccharides and Lactose Differentially Affect Infant Gut Microbiota and Intestinal Barrier In Vitro. Nutrients 2022, 14, 2546. [Google Scholar] [CrossRef]
- Ben, X.M.; Zhou, X.Y.; Zhao, W.H.; Yu, W.L.; Pan, W.; Zhang, W.L.; Wu, S.M.; Beusekom, C.M.; Schaafsma, A. Supplementation of milk formula with galacto-oligosaccharides improves intestinal micro-flora and fermentation in term infants. Chin. Med. J. Engl. 2004, 117, 927–931. [Google Scholar]
- Salminen, S.; Stahl, B.; Vinderola, G.; Szajewska, H. Infant Formula Supplemented with Biotics: Current Knowledge and Future Perspectives. Nutrients 2020, 12, 1952. [Google Scholar] [CrossRef]
- Estorninos, E.; Lawenko, R.B.; Palestroque, E.; Sprenger, N.; Benyacoub, J.; Kortman, G.A.M.; Boekhorst, J.; Bettler, J.; Cercamondi, C.I.; Berger, B. Term infant formula supplemented with milk-derived oligosaccharides shifts the gut microbiota closer to that of human milk-fed infants and improves intestinal immune defense: A randomized controlled trial. Am. J. Clin. Nutr. 2022, 115, 142–153. [Google Scholar] [CrossRef]
- Mugambi, M.N.; Musekiwa, A.; Lombard, M.; Young, T.; Blaauw, R. Probiotics, prebiotics infant formula use in preterm or low birth weight infants: A systematic review. Nutr. J. 2012, 11, 58. [Google Scholar] [CrossRef] [PubMed]
- Giovannini, M.; Verduci, E.; Gregori, D.; Ballali, S.; Soldi, S.; Ghisleni, D.; Riva, E. Prebiotic effect of an infant formula supplemented with galacto-oligosaccharides: Randomized multicenter trial. J. Am. Coll. Nutr. 2014, 33, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Xia, Q.; Williams, T.; Hustead, D.; Price, P.; Morrison, M.; Yu, Z. Quantitative analysis of intestinal bacterial populations from term infants fed formula supplemented with fructo-oligosaccharides. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Vivatvakin, B.; Mahayosnond, A.; Theamboonlers, A.; Steenhout, P.G.; Conus, N.J. Effect of a whey-predominant starter formula containing LCPUFAs and oligosaccharides (FOS/GOS) on gastrointestinal comfort in infants. Asia Pac. J. Clin. Nutr. 2010, 19, 473–480. [Google Scholar] [PubMed]
- Salminen, S.; Endo, A.; Isolauri, E.; Scalabrin, D. Early Gut Colonization With Lactobacilli and Staphylococcus in Infants: The Hygiene Hypothesis Extended. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Salvini, F.; Riva, E.; Salvatici, E.; Boehm, G.; Jelinek, J.; Banderali, G.; Giovannini, M. A specific prebiotic mixture added to starting infant formula has long-lasting bifidogenic effects. J. Nutr. 2011, 141, 1335–1339. [Google Scholar] [CrossRef]
- Holscher, H.D.; Faust, K.L.; Czerkies, L.A.; Litov, R.; Ziegler, E.E.; Lessin, H.; Hatch, T.; Sun, S.; Tappenden, K.A. Effects of prebiotic-containing infant formula on gastrointestinal tolerance and fecal microbiota in a randomized controlled trial. JPEN J. Parenter. Enteral. Nutr. 2012, 36 (Suppl. 1), 95S–105S. [Google Scholar] [CrossRef]
- Huet, F.; Abrahamse-Berkeveld, M.; Tims, S.; Simeoni, U.; Beley, G.; Savagner, C.; Vandenplas, Y.; Hourihane, J.O. Partly Fermented Infant Formulae With Specific Oligosaccharides Support Adequate Infant Growth and Are Well-Tolerated. J. Pediatr. Gastroenterol. Nutr. 2016, 63, e43–e53. [Google Scholar] [CrossRef]
- Simeoni, U.; Berger, B.; Junick, J.; Blaut, M.; Pecquet, S.; Rezzonico, E.; Grathwohl, D.; Sprenger, N.; Brüssow, H.; Szajewska, H.; et al. Gut microbiota analysis reveals a marked shift to bifidobacteria by a starter infant formula containing a synbiotic of bovine milk-derived oligosaccharides and Bifidobacterium animalis subsp. lactis CNCM I-3446. Environ. Microbiol. 2016, 18, 2185–2195. [Google Scholar] [CrossRef] [PubMed]
- Das, T.K.; Pradhan, S.; Chakrabarti, S.; Mondal, K.C.; Ghosh, K. Current status of probiotic and related health benefits. Appl. Food Res. 2022, 2, 100185. [Google Scholar] [CrossRef]
- Fijan, S. Microorganisms with Claimed Probiotic Properties: An Overview of Recent Literature. Int. J. Environ. Res. Public Health 2014, 11, 4745. [Google Scholar] [CrossRef]
- Gil-Campos, M.; López, M.; Rodriguez-Benítez, M.V.; Romero, J.; Roncero, I.; Linares, M.D.; Maldonado, J.; López-Huertas, E.; Berwind, R.; Ritzenthaler, K.L.; et al. Lactobacillus fermentum CECT 5716 is safe and well tolerated in infants of 1–6 months of age: A Randomized Controlled Trial. Pharmacol. Res. 2012, 65, 231–238. [Google Scholar] [CrossRef]
- Scalabrin, D.; Harris, C.; Johnston, W.; Berseth, C. Long-term safety assessment in children who received hydrolyzed protein formulas with Lactobacillus rhamnosus GG: A 5-year follow-up. Eur. J. Pediatr. 2017, 176, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Maldonado-Lobón, J.; Gil-Campos, M.; Maldonado, J.; López-Huertas, E.; Flores-Rojas, K.; Valero, A.; Rodríguez-Benítez, M.; Bañuelos, O.; Lara-Villoslada, F.; Fonollá, J.; et al. Long-term safety of early consumption of Lactobacillus fermentum CECT5716: A 3-year follow-up of a randomized controlled trial. Pharmacol. Res. 2015, 95–96, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Rautava, S.; Kalliomäki, M.; Isolauri, E. Probiotics during pregnancy and breast-feeding might confer immunomodulatory protection against atopic disease in the infant. J. Allergy Clin. Immunol. 2002, 109, 119–121. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, J.; Cañabate, F.; Sempere, L.; Vela, F.; Sánchez, A.R.; Narbona, E.; López-Huertas, E.; Geerlings, A.; Valero, A.D.; Olivares, M.; et al. Human milk probiotic Lactobacillus fermentum CECT5716 reduces the incidence of gastrointestinal and upper respiratory tract infections in infants. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Horigome, A.; Hisata, K.; Odamaki, T.; Iwabuchi, N.; Xiao, J.Z.; Shimizu, T. Colonization of Supplemented Bifidobacterium breve M-16V in Low Birth Weight Infants and Its Effects on Their Gut Microbiota Weeks Post-administration. Front. Microbiol. 2021, 12, 610080. [Google Scholar] [CrossRef] [PubMed]
- Yan, W.; Luo, B.; Zhang, X.; Ni, Y.; Tian, F. Association and Occurrence of Bifidobacterial Phylotypes Between Breast Milk and Fecal Microbiomes in Mother–Infant Dyads During the First 2 Years of Life. Front. Microbiol. 2021, 12, 669442. [Google Scholar] [CrossRef]
- Alander, M.; Mättö, J.; Kneifel, W.; Johansson, M.; Kögler, B.; Crittenden, R.; Mattila-Sandholm, T.; Saarela, M. Effect of galacto-oligosaccharide supplementation on human faecal microflora and on survival and persistence of Bifidobacterium lactis Bb-12 in the gastrointestinal tract. Int. Dairy J. 2001, 11, 817–825. [Google Scholar] [CrossRef]
- Lin, C.; Lin, Y.; Zhang, H.; Wang, G.; Zhao, J.; Zhang, H.; Chen, W. Intestinal ‘Infant-Type’ Bifidobacteria Mediate Immune System Development in the First 1000 Days of Life. Nutrients 2022, 14, 1498. [Google Scholar] [CrossRef]
- Frese, S.A.; Hutton, A.A.; Contreras, L.N.; Shaw, C.A.; Palumbo, M.C.; Casaburi, G.; Xu, G.; Davis, J.C.C.; Lebrilla, C.B.; Henrick, B.M.; et al. Persistence of Supplemented Bifidobacterium longum subsp. infantis EVC001 in Breastfed Infants. mSphere 2017, 2, e00501–e00517. [Google Scholar] [CrossRef]
- Quin, C.; Estaki, M.; Vollman, D.M.; Barnett, J.A.; Gill, S.K.; Gibson, D.L. Probiotic supplementation and associated infant gut microbiome and health: A cautionary retrospective clinical comparison. Sci. Rep. 2018, 8, 1–16. [Google Scholar] [CrossRef]
- Alcon-Giner, C.; Dalby, M.J.; Caim, S.; Ketskemety, J.; Shaw, A.; Sim, K.; Lawson, M.A.; Kiu, R.; LeClaire, C.; Chalklen, L.; et al. Microbiota Supplementation with Bifidobacterium and Lactobacillus Modifies the Preterm Infant Gut Microbiota and Metabolome: An Observational Study. Cell Rep. Med. 2020, 1, 100077. [Google Scholar] [CrossRef]
- Vendt, N.; Grünberg, H.; Tuure, T.; Malminiemi, O.; Wuolijoki, E.; Tillmann, V.; Sepp, E.; Korpela, R. Growth during the first 6 months of life in infants using formula enriched with Lactobacillus rhamnosus GG: Double-blind, randomized trial. J. Hum. Nutr. Diet 2006, 19, 51–58. [Google Scholar] [CrossRef]
- Li, Y.; Shimizu, T.; Hosaka, A.; Kaneko, N.; Ohtsuka, Y.; Yamashiro, Y. Effects of bifidobacterium breve supplementation on intestinal flora of low birth weight infants. Pediatr. Int. 2004, 46, 509–515. [Google Scholar] [CrossRef]
- van Best, N.; Trepels-Kottek, S.; Savelkoul, P.; Orlikowsky, T.; Hornef, M.W.; Penders, J. Influence of probiotic supplementation on the developing microbiota in human preterm neonates. Gut Microbes 2020, 12, 1–16. [Google Scholar] [CrossRef]
- Milani, C.; Duranti, S.; Bottacini, F.; Casey, E.; Turroni, F.; Mahony, J.; Belzer, C.; Delgado Palacio, S.; Arboleya Montes, S.; Mancabelli, L.; et al. The First Microbial Colonizers of the Human Gut: Composition, Activities, and Health Implications of the Infant Gut Microbiota. Microbiol. Mol. Biol. Rev. 2017, 81, e00036-17. [Google Scholar] [CrossRef]
- Abate, A.D.; Hassen, S.L.; Temesgen, M.M. Timely initiation of complementary feeding practices and associated factors among children aged 6–23 months in Dessie Zuria District, Northeast Ethiopia: A community-based cross-sectional study. Front. Pediatr. 2023, 11, 1062251. [Google Scholar] [CrossRef] [PubMed]
- Berti, C.; Socha, P. Infant and Young Child Feeding Practices and Health. Nutrients 2023, 15, 1184. [Google Scholar] [CrossRef] [PubMed]
- Campoy, C.; Leis, R. Methods of introduction of complementary feeding in the first year of life. An. Pediatría Engl. Ed. 2023, 98, 247–248. [Google Scholar] [CrossRef]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Mis, N.F.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.; Matz, K.L.; Berman, L.M.; Davis, K.N.; Melanson, E.L.; Frank, D.N.; Hendricks, A.E.; Krebs, N.F. Effects of Complementary Feeding With Different Protein-Rich Foods on Infant Growth and Gut Health: Study Protocol. Front. Pediatr. 2021, 9, 793215. [Google Scholar] [CrossRef] [PubMed]
- Laursen, M.F.; Andersen, L.B.B.; Michaelsen, K.F.; Mølgaard, C.; Trolle, E.; Bahl, M.I.; Licht, T.R. Infant Gut Microbiota Development Is Driven by Transition to Family Foods Independent of Maternal Obesity. mSphere 2016, 1, e00069-15. [Google Scholar] [CrossRef] [PubMed]
- Differding, M.K.; Benjamin-Neelon, S.E.; Hoyo, C.; Østbye, T.; Mueller, N.T. Timing of complementary feeding is associated with gut microbiota diversity and composition and short chain fatty acid concentrations over the first year of life. BMC Microbiol. 2020, 20, 56. [Google Scholar] [CrossRef]
- Tang, M.; Frank, D.; Hendricks, A.; Ir, D.; Krebs, N. Protein Intake During Early Complementary Feeding Affects the Gut Microbiota in U.S. Formula-fed Infants (FS04-03-19). Curr. Dev. Nutr. 2019, 3 (Suppl. 1), nzz048.FS04-03-19. [Google Scholar] [CrossRef]
- Fu, J.; Zheng, Y.; Gao, Y.; Xu, W. Dietary Fiber Intake and Gut Microbiota in Human Health. Microorganisms 2022, 10, 2507. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Martín, M.; Saturio, S.; Arboleya, S.; Herrero-Morín, D.; Calzón, M.; López, T.; González, S.; Gueimonde, M. Association between diet and fecal microbiota along the first year of life. Food Res. Int. 2022, 162, 111994. [Google Scholar] [CrossRef]
- Stewart, C.J.; Ajami, N.J.; O’brien, J.L.; Hutchinson, D.S.; Smith, D.P.; Wong, M.C.; Ross, M.C.; Lloyd, R.E.; Doddapaneni, H.; Metcalf, G.A.; et al. Temporal development of the gut microbiome in early childhood from the TEDDY study. Nature 2018, 562, 583–588. [Google Scholar] [CrossRef]
- Neri-Numa, I.A.; Pastore, G.M. Novel insights into prebiotic properties on human health: A review. Food Res. Int. 2020, 131, 108973. [Google Scholar] [CrossRef]
- Suriano, F.; Nyström, E.E.L.; Sergi, D.; Gustafsson, J.K. Diet, microbiota, and the mucus layer: The guardians of our health. Front. Immunol. 2022, 13, 953196. [Google Scholar] [CrossRef]
- Simpson, H.L.; Campbell, B.J. Review article: Dietary fibre–microbiota interactions. Aliment. Pharmacol. Ther. 2015, 42, 158. [Google Scholar] [CrossRef]
- Wu, S.; Bhat, Z.F.; Gounder, R.S.; Ahmed, I.A.M.; Al-Juhaimi, F.Y.; Ding, Y.; Bekhit, A.E. Effect of Dietary Protein and Processing on Gut Microbiota—A Systematic Review. Nutrients 2022, 14, 453. [Google Scholar] [CrossRef] [PubMed]
- Makki, K.; Deehan, E.C.; Walter, J.; Bäckhed, F. The Impact of Dietary Fiber on Gut Microbiota in Host Health and Disease. Cell Host Microbe 2018, 23, 705–715. [Google Scholar] [CrossRef]
- Huang, Z.; Boekhorst, J.; Fogliano, V.; Capuano, E.; Wells, J.M. Impact of High-Fiber or High-Protein Diet on the Capacity of Human Gut Microbiota To Produce Tryptophan Catabolites. J. Agric. Food Chem. 2023, 71, 6956–6966. [Google Scholar] [CrossRef]
- Murga-Garrido, S.M.; Hong, Q.; Cross, T.-W.L.; Hutchison, E.R.; Han, J.; Thomas, S.P.; Vivas, E.I.; Denu, J.; Ceschin, D.G.; Tang, Z.-Z.; et al. Gut microbiome variation modulates the effects of dietary fiber on host metabolism. Microbiome 2021, 9, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.; Lee, G.; Son, H.; Koh, H.; Kim, E.S.; Unno, T.; Shin, J.H. Butyrate producers, “The Sentinel of Gut”: Their intestinal significance with and beyond butyrate, and prospective use as microbial therapeutics. Front. Microbiol. 2023, 13, 1103836. [Google Scholar] [CrossRef] [PubMed]
- Tsukuda, N.; Yahagi, K.; Hara, T.; Watanabe, Y.; Matsumoto, H.; Mori, H.; Higashi, K.; Tsuji, H.; Matsumoto, S.; Kurokawa, K.; et al. Key bacterial taxa and metabolic pathways affecting gut short-chain fatty acid profiles in early life. ISME J. 2021, 15, 2574–2590. [Google Scholar] [CrossRef]
- Alsharairi, N.A. Therapeutic Potential of Gut Microbiota and Its Metabolite Short-Chain Fatty Acids in Neonatal Necrotizing Enterocolitis. Life 2023, 13, 561. [Google Scholar] [CrossRef]
- Akhtar, M.; Chen, Y.; Ma, Z.; Zhang, X.; Shi, D.; Khan, J.A.; Liu, H. Gut microbiota-derived short chain fatty acids are potential mediators in gut inflammation. Anim. Nutr. 2022, 8, 350–360. [Google Scholar] [CrossRef]
- Cong, X.; Xu, W.; Janton, S.; Henderson, W.A.; Matson, A.; McGrath, J.M.; Maas, K.; Graf, J. Gut Microbiome Developmental Patterns in Early Life of Preterm Infants: Impacts of Feeding and Gender. PLoS ONE 2016, 11, e0152751. [Google Scholar] [CrossRef]
- Gondolf, U.H.; Tetens, I.; Michaelsen, K.F.; Trolle, E. Dietary habits of partly breast-fed and completely weaned infants at 9 months of age. Public Health Nutr. 2012, 15, 578–586. [Google Scholar] [CrossRef]
- Hughes, R.L.; Holscher, H.D. Fueling Gut Microbes: A Review of the Interaction between Diet, Exercise, and the Gut Microbiota in Athletes. Adv. Nutr. 2021, 12, 2190. [Google Scholar] [CrossRef]
- Li, L.; Ryan, J.; Ning, Z.; Zhang, X.; Mayne, J.; Lavallée-Adam, M.; Stintzi, A.; Figeys, D. A functional ecological network based on metaproteomics responses of individual gut microbiomes to resistant starches. Comput. Struct. Biotechnol. J. 2020, 18, 3833–3842. [Google Scholar] [CrossRef] [PubMed]
- Cronin, P.; Joyce, S.A.; O’toole, P.W.; O’connor, E.M. Dietary Fibre Modulates the Gut Microbiota. Nutrients 2021, 13, 1655. [Google Scholar] [CrossRef] [PubMed]
- Bäckhed, F.; Roswall, J.; Peng, Y.; Feng, Q.; Jia, H.; Kovatcheva-Datchary, P.; Li, Y.; Xia, Y.; Xie, H.; Zhong, H.; et al. Dynamics and Stabilization of the Human Gut Microbiome during the First Year of Life. Cell Host Microbe 2015, 17, 690–703. [Google Scholar] [CrossRef] [PubMed]
- Caffarelli, C.; Di Mauro, D.; Mastrorilli, C.; Bottau, P.; Cipriani, F.; Ricci, G. Solid Food Introduction and the Development of Food Allergies. Nutrients 2018, 10, 1790. [Google Scholar] [CrossRef] [PubMed]
- Koukou, Z.; Papadopoulou, E.; Panteris, E.; Papadopoulou, S.; Skordou, A.; Karamaliki, M.; Diamanti, E. The Effect of Breastfeeding on Food Allergies in Newborns and Infants. Children 2023, 10, 1046. [Google Scholar] [CrossRef] [PubMed]
- Du Toit, G.; Foong, R.X.M.; Lack, G. Prevention of food allergy—Early dietary interventions. Allergol. Int. 2016, 65, 370–377. [Google Scholar] [CrossRef]
- Leong, C.; Haszard, J.J.; Lawley, B.; Otal, A.; Taylor, R.W.; Szymlek-Gay, E.A.; Fleming, E.A.; Daniels, L.; Fangupo, L.J.; Tannock, G.W.; et al. Mediation analysis as a means of identifying dietary components that differentially affect the fecal microbiota of infants weaned by modified baby-led and traditional approaches. Appl. Environ. Microbiol. 2018, 84. [Google Scholar] [CrossRef]
- Differding, M.K.; Doyon, M.; Bouchard, L.; Perron, P.; Guérin, R.; Asselin, C.; Massé, E.; Hivert, M.; Mueller, N.T. Potential interaction between timing of infant complementary feeding and breastfeeding duration in determination of early childhood gut microbiota composition and BMI. Pediatr. Obes. 2020, 15, e12642. [Google Scholar] [CrossRef]
- Szajewska, H.; Guandalini, S.; Morelli, L.; Van Goudoever, J.B.; Walker, A. Effect of Bifidobacterium animalis subsp lactis supplementation in preterm infants: A systematic review of randomized controlled trials. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 203–209. [Google Scholar] [CrossRef]
- Bin-Nun, A.; Kassirer, Y.; Jarallah, Y.; Barg, M.; Mimouni, F.B.; Hammerman, C.; Sela, H.Y. Early breast expression for very low birth infants admitted to neonatal intensive care unit: The challenges of cesarean deliveries. J. Matern. Fetal Neonatal Med. 2022, 35, 8249–8256. [Google Scholar] [CrossRef]
- Henderickx, J.G.E.; Zwittink, R.D.; van Lingen, R.A.; Knol, J.; Belzer, C. The Preterm Gut Microbiota: An Inconspicuous Challenge in Nutritional Neonatal Care. Front. Cell Infect. Microbiol. 2019, 9, 85. [Google Scholar] [CrossRef]
- Jia, Q.; Yu, X.; Chang, Y.; You, Y.; Chen, Z.; Wang, Y.; Liu, B.; Chen, L.; Ma, D.; Xing, Y.; et al. Dynamic Changes of the Gut Microbiota in Preterm Infants With Different Gestational Age. Front. Microbiol. 2022, 13, 923273. [Google Scholar] [CrossRef]
- Derrien, M.; Alvarez, A.S.; de Vos, W.M. The Gut Microbiota in the First Decade of Life. Trends Microbiol. 2019, 27, 997–1010. [Google Scholar] [CrossRef]
- Altobelli, E.; Angeletti, P.M.; Verrotti, A.; Petrocelli, R. The Impact of Human Milk on Necrotizing Enterocolitis: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 1322. [Google Scholar] [CrossRef] [PubMed]
- Huston, R.K.; Markell, A.M.; McCulley, E.A.; Pathak, M.; Rogers, S.P.; Sweeney, S.L.; Dolphin, N.G.; Gardiner, S.K. Decreasing Necrotizing Enterocolitis and Gastrointestinal Bleeding in the Neonatal Intensive Care Unit: The Role of Donor Human Milk and Exclusive Human Milk Diets in Infants ≤1500 g Birth Weight. Infant Child Adolesc. Nutr. 2014, 6, 86–93. [Google Scholar] [CrossRef]
- Xu, W.; Judge, M.P.; Maas, K.; Hussain, N.; McGrath, J.M.; Henderson, W.A.; Cong, X. Systematic Review of the Effect of Enteral Feeding on Gut Microbiota in Preterm Infants. J. Obstet. Gynecol. Neonatal Nurs. 2018, 47, 451–463. [Google Scholar] [CrossRef]
- Cai, C.; Zhang, Z.; Morales, M.; Wang, Y.; Khafipour, E.; Friel, J. Feeding practice influences gut microbiome composition in very low birth weight preterm infants and the association with oxidative stress: A prospective cohort study. Free Radic. Biol. Med. 2019, 142, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.J. Importance of the Gut Microbiome in Preterm Infants. Nestle Nutr. Inst. Workshop Ser. 2021, 96, 141–148. [Google Scholar] [CrossRef]
- Ehrenkranz, R.A. Nutrition, Growth and Clinical Outcomes. World Rev Nutr Diet. 2014, 110, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Stephens, B.E.; Vohr, B.R. Neurodevelopmental Outcome of the Premature Infant. Pediatr. Clin. N. Am. 2009, 56, 631–646. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.L.; Sorita, A.; Carey, W.A.; Colby, C.E.; Murad, M.H.; Alahdab, F. Interventions To Prevent Retinopathy of Prematurity: A Meta-analysis. Pediatrics 2016, 137. [Google Scholar] [CrossRef] [PubMed]
- Stoltz Sjöström, E.; Lundgren, P.; Öhlund, I.; Holmström, G.; Hellström, A.; Domellöf, M. Low energy intake during the first 4 weeks of life increases the risk for severe retinopathy of prematurity in extremely preterm infants. Arch. Dis. Child Fetal Neonatal Ed. 2016, 101, F108–F113. [Google Scholar] [CrossRef]
- Salas, A.A.; Willis, K.A.; Carlo, W.A.; Yi, N.; Zhang, L.; Van Der Pol, W.J.; Younge, N.E.; Lefkowitz, E.J.; Lal, C.V. The gut microbiome of extremely preterm infants randomized to the early progression of enteral feeding. Pediatr. Res. 2021, 92, 799–804. [Google Scholar] [CrossRef]
- Timmerman, H.M.; Rutten, N.B.M.M.; Boekhorst, J.; Saulnier, D.M.; Kortman, G.A.M.; Contractor, N.; Kullen, M.; Floris, E.; Harmsen, H.J.M.; Vlieger, A.M.; et al. Intestinal colonisation patterns in breastfed and formula-fed infants during the first 12 weeks of life reveal sequential microbiota signatures. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef]
- Hosny, M.; Cassir, N.; La Scola, B. WITHDRAWN: Updating on gut microbiota and its relationship with the occurrence of necrotizing enterocolitis (Review). Hum. Microb. J. 2017, 4, 1–6. [Google Scholar] [CrossRef]
- Gregory, K.E.; Samuel, B.S.; Houghteling, P.; Shan, G.; Ausubel, F.M.; Sadreyev, R.I.; Walker, W.A. Influence of maternal breast milk ingestion on acquisition of the intestinal microbiome in preterm infants. Microbiome 2016, 4, 68. [Google Scholar] [CrossRef]
- Wang, Z.; Neupane, A.; Vo, R.; White, J.; Wang, X.; Marzano, S.Y.L. Comparing Gut Microbiome in Mothers’ Own Breast Milk- and Formula-Fed Moderate-Late Preterm Infants. Front. Microbiol. 2020, 11, 891. [Google Scholar] [CrossRef]
- Vass, R.A.; Kiss, G.; Bell, E.F.; Roghair, R.D.; Miseta, A.; Bódis, J.; Funke, S.; Ertl, T. Breast Milk for Term and Preterm Infants—Own Mother’s Milk or Donor Milk? Nutrients 2021, 13, 424. [Google Scholar] [CrossRef]
- Austin, S.; De Castro, C.A.; Sprenger, N.; Binia, A.; Affolter, M.; Garcia-Rodenas, C.L.; Beauport, L.; Tolsa, J.-F.; Fumeaux, C.J.F. Human Milk Oligosaccharides in the Milk of Mothers Delivering Term versus Preterm Infants. Nutrients 2019, 11, 1282. [Google Scholar] [CrossRef]
- Plaza-Díaz, J.; Fontana, L.; Gil, A. Human Milk Oligosaccharides and Immune System Development. Nutrients 2018, 10, 1038. [Google Scholar] [CrossRef]
- Rousseaux, A.; Brosseau, C.; Le Gall, S.; Piloquet, H.; Barbarot, S.; Bodinier, M. Human Milk Oligosaccharides: Their Effects on the Host and Their Potential as Therapeutic Agents. Front. Immunol. 2021, 12, 680911. [Google Scholar] [CrossRef]
- Masi, A.C.; Embleton, N.D.; A Lamb, C.; Young, G.; Granger, C.L.; Najera, J.; Smith, D.P.; Hoffman, K.L.; Petrosino, J.F.; Bode, L.; et al. Human milk oligosaccharide DSLNT and gut microbiome in preterm infants predicts necrotising enterocolitis. Gut 2021, 70, 2273–2282. [Google Scholar] [CrossRef]
- Coggins, S.A.; Wynn, J.L.; Weitkamp, J.H. Infectious Causes of Necrotizing Enterocolitis. Clin. Perinatol. 2015, 42, 133–154. [Google Scholar] [CrossRef]
- Lee, J.K.F.; Tan, L.T.H.; Ramadas, A.; Mutalib, N.S.A.; Lee, L.H. Exploring the Role of Gut Bacteria in Health and Disease in Preterm Neonates. Int. J. Environ. Res. Public Health 2020, 17, 6963. [Google Scholar] [CrossRef]
- McGuire, W. Donor human milk versus formula for preventing necrotising enterocolitis in preterm infants: Systematic review. Arch. Dis. Child Fetal Neonatal Ed. 2003, 88, 11F–14F. [Google Scholar] [CrossRef]
- Embleton, N.D.; Sproat, T.; Uthaya, S.; Young, G.R.; Garg, S.; Vasu, V.; Masi, A.C.; Beck, L.; Modi, N.; Stewart, C.J.; et al. Effect of an Exclusive Human Milk Diet on the Gut Microbiome in Preterm Infants. JAMA Netw. Open 2023, 6, e231165. [Google Scholar] [CrossRef] [PubMed]
- Beghetti, I.; Panizza, D.; Lenzi, J.; Gori, D.; Martini, S.; Corvaglia, L.; Aceti, A. Probiotics for Preventing Necrotizing Enterocolitis in Preterm Infants: A Network Meta-Analysis. Nutrients 2021, 13, 192. [Google Scholar] [CrossRef] [PubMed]
- Zhou, K.Z.; Wu, K.; Deng, L.X.; Hu, M.; Luo, Y.X.; Zhang, L.Y. Probiotics to prevent necrotizing enterocolitis in very low birth weight infants: A network meta-analysis. Front. Pediatr. 2023, 11, 1095368. [Google Scholar] [CrossRef] [PubMed]
- Underwood, M.A.; Umberger, E.; Patel, R.M. Safety and Efficacy of Probiotic Administration to Preterm Infants: Ten Common Questions. Pediatr. Res. 2020, 88 (Suppl. 1), 48. [Google Scholar] [CrossRef]
- Guitor, A.K.; Yousuf, E.I.; Raphenya, A.R.; Hutton, E.K.; Morrison, K.M.; McArthur, A.G.; Wright, G.D.; Stearns, J.C. Capturing the antibiotic resistome of preterm infants reveals new benefits of probiotic supplementation. Microbiome 2022, 10, 1–16. [Google Scholar] [CrossRef]
- Batta, V.K.; Rao, S.C.; Patole, S.K. Bifidobacterium infantis as a probiotic in preterm infants: A systematic review and meta-analysis. Pediatr. Res. 2023, 94, 1887–1905. [Google Scholar] [CrossRef]
- Wang, H.; Meng, X.; Xing, S.; Guo, B.; Chen, Y.; Pan, Y.Q. Probiotics to prevent necrotizing enterocolitis and reduce mortality in neonates: A meta-analysis. Medicine 2023, 102, E32932. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, M.; Patole, S. Prophylactic Probiotic Supplementation for Preterm Neonates—A Systematic Review and Meta-Analysis of Nonrandomized Studies. Adv. Nutr. 2021, 12, 1411–1423. [Google Scholar] [CrossRef]
- Morgan, R.L.; Preidis, G.A.; Kashyap, P.C.; Weizman, A.V.; Sadeghirad, B. Probiotics Reduce Mortality and Morbidity in Preterm, Low-Birth-Weight Infants: A Systematic Review and Network Meta-analysis of Randomized Trials. Gastroenterology 2020, 159, 467–480. [Google Scholar] [CrossRef] [PubMed]
- Chi, C.; Li, C.; Buys, N.; Wang, W.; Yin, C.; Sun, J. Effects of Probiotics in Preterm Infants: A Network Meta-analysis. Pediatrics 2021, 147. [Google Scholar] [CrossRef] [PubMed]
- Akker, C.H.v.D.; van Goudoever, J.B.; Shamir, R.; Domellöf, M.; Embleton, N.D.; Hojsak, I.; Lapillonne, A.; Mihatsch, W.A.; Canani, R.B.; Bronsky, J.; et al. Probiotics and Preterm Infants: A Position Paper by the European Society for Paediatric Gastroenterology Hepatology and Nutrition Committee on Nutrition and the European Society for Paediatric Gastroenterology Hepatology and Nutrition Working Group for Probiotics and Prebiotics. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 664–680. [Google Scholar] [CrossRef] [PubMed]
- Poindexter, B.; Cummings, J.; Hand, I.; Adams-Chapman, I.; Aucott, S.W.; Puopolo, K.M.; Goldsmith, J.P.; Kaufman, D.; Martin, C.; Mowitz, M.; et al. Use of Probiotics in Preterm Infants. Pediatrics 2021, 147. [Google Scholar] [CrossRef] [PubMed]
- Cacho, N.T.; Harrison, N.A.; Parker, L.A.; Padgett, K.A.; Lemas, D.J.; Marcial, G.E.; Li, N.; Carr, L.E.; Neu, J.; Lorca, G.L. Personalization of the Microbiota of Donor Human Milk with Mother’s Own Milk. Front. Microbiol. 2017, 8, 1470. [Google Scholar] [CrossRef] [PubMed]
- Sadeghirad, B.; Florez, I.D.; Morgan, R.L.; Foroutan, F.; Chang, Y.; Zeraatkar, D. Probiotics, Prebiotics, and Synbiotics for Prevention of Mortality and Morbidity in Preterm Infants: A Systematic Review and Network Meta-Analysis of Randomized Trials. SSRN Electron. J. 2019. [Google Scholar] [CrossRef]
- Thomas, D.; Sharma, A.; Sankar, M.J. Probiotics for the prevention of mortality and sepsis in preterm very low birth weight neonates from low- and middle-income countries: A Bayesian network meta-analysis. Front. Nutr. 2023, 10, 1133293. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram of article selection process.

Figure 2.
Effects of different microbiome modulators at different stages of the infant life. FOS, fructooligosaccharides; GOS, galactooligosaccharides; FF, formula feeding.
Figure 2.
Effects of different microbiome modulators at different stages of the infant life. FOS, fructooligosaccharides; GOS, galactooligosaccharides; FF, formula feeding.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Catassi, G.; Aloi, M.; Giorgio, V.; Gasbarrini, A.; Cammarota, G.; Ianiro, G. The Role of Diet and Nutritional Interventions for the Infant Gut Microbiome. Nutrients 2024, 16, 400. https://doi.org/10.3390/nu16030400
AMA Style
Catassi G, Aloi M, Giorgio V, Gasbarrini A, Cammarota G, Ianiro G. The Role of Diet and Nutritional Interventions for the Infant Gut Microbiome. Nutrients. 2024; 16(3):400. https://doi.org/10.3390/nu16030400
Chicago/Turabian StyleCatassi, Giulia, Marina Aloi, Valentina Giorgio, Antonio Gasbarrini, Giovanni Cammarota, and Gianluca Ianiro. 2024. "The Role of Diet and Nutritional Interventions for the Infant Gut Microbiome" Nutrients 16, no. 3: 400. https://doi.org/10.3390/nu16030400
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.