
Benefits and Harms of Edible Vegetable Oils and Fats Fortified with Vitamins A and D as a Public Health Intervention in the General Population: A Systematic Review of Interventions

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Selection Process
2.4. Data Collection
2.5. Risk of Bias Assessment
2.6. Effect Measures
2.7. Synthesis Methods
2.8. Reporting Bias Assessment
2.9. Certainty Assessment
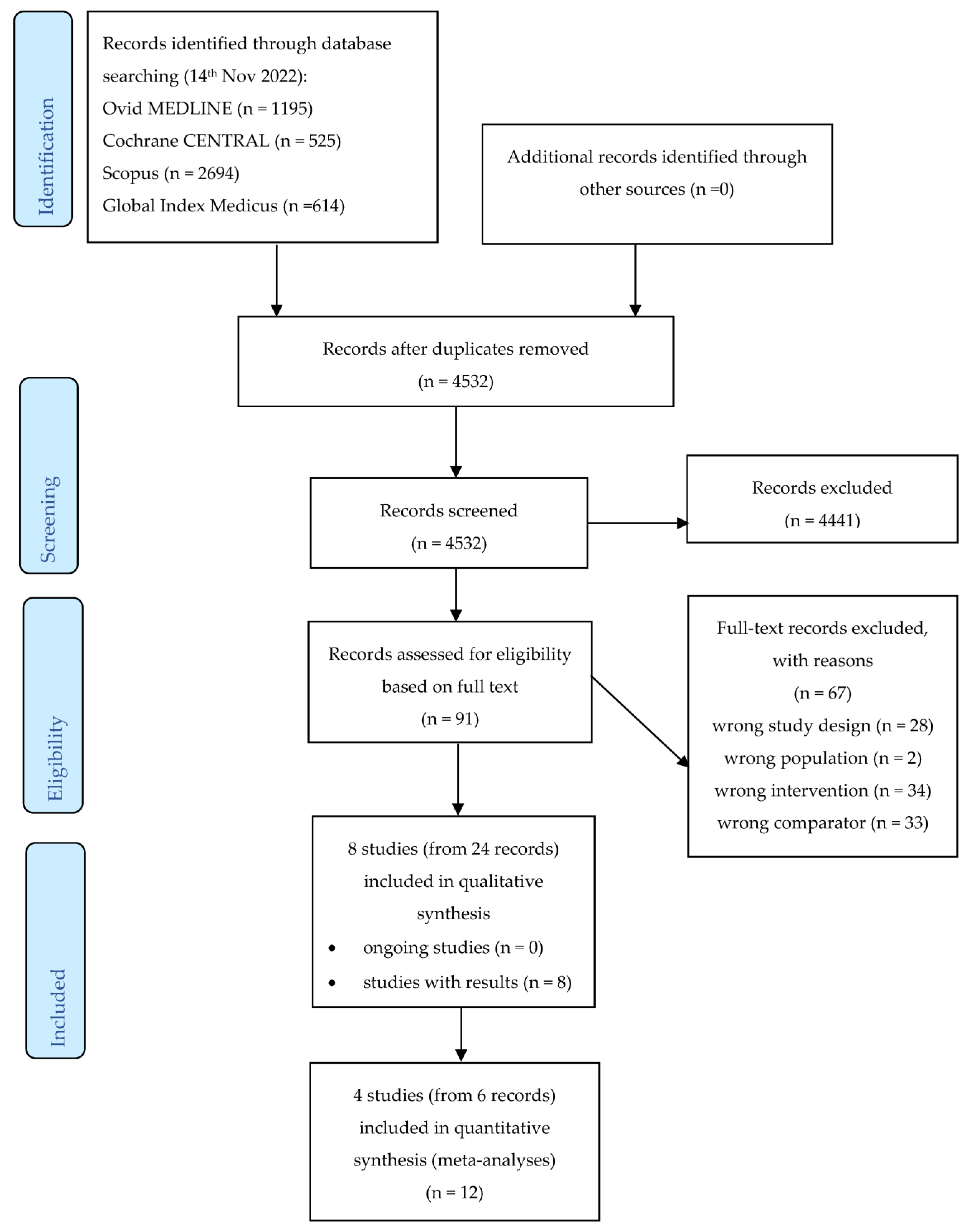
3. Results
3.1. Description of Included Studies
3.2. Risk of Bias in Included Studies
3.3. Primary Outcomes for Studies on Vitamin A Fortification versus No Fortification with Vitamin A

{kind=link}
| Study ID | References | Country | Study Design | Sample Size (n) | Age at Exposure | Age at Outcome Measurement | Fortified Product | Micronutrient(s) Added to the Fortified Products | Duration of Intervention | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|
| Ghasemifard 2020 | [33,34,35] | Iran | randomized controlled trial | 99 | 18–30 years | 18–30 years | Canola oil | Vitamin D | 12 weeks | Se levels of 25(OH)D, CTX, B-ALP, PTH, TC, LDL, HDL, TG; dietary intake of energy, protein, vitamin D, vitamin K, vitamin C, calcium, phosphorus, magnesium, zinc, |
| Stougaard 2018 | [35] | Denmark | birth cohort study | 73,237 | during pregnancy | NA | Margarine | Vitamin D | NA | Gestational hypertension, preeclampsia (including mild and unspecified preeclampsia and toxemia), eclampsia (including severe preeclampsia and eclampsia) |
| Danish study | [36] | Denmark | birth cohort study | 217,249 | during fetal life | NA | Margarine | Vitamin D | NA | Incidence of celiac disease |
| [37] | Denmark | birth cohort study | 217,249 | during fetal life | NA | Margarine | Vitamin D | NA | Incidence of IBD (including Crohn’s disease, ulcerative colitis, unidentified IBD) | |
| [38,39,40] | Denmark | birth cohort study | 28,871 | during fetal life | 20.6–27.5 years | Margarine | Vitamin D | NA | Incidence of gestational diabetes mellitus | |
| [41] | Denmark | birth cohort study | 222,247 | during fetal life | 0–9 years | Margarine | Vitamin D | NA | Incidence of childhood asthma (diagnoses from birth to the age of 9 years) | |
| [42,43] | Denmark | birth cohort study | 331,623 | during fetal life and during first postnatal year | 0–15 years | Margarine | Vitamin D | NA | Incidence of type 1 diabetes mellitus (before age of 15 years) | |
| [44] | Denmark | birth cohort study | 327,254 | during fetal life | 10–18 years | Margarine | Vitamin D | NA | Number of fracture events | |
| [45] | Denmark | birth cohort study | 30,004 | during fetal life | 0 year | Margarine | Vitamin D | NA | Birth weight, prevalence of low and high birth weight | |
| [46] | Denmark | birth cohort study | 30,004 | during fetal life | 7 years | Margarine | Vitamin D | NA | Birth weight, BMI, BMI Z-score, prevalence of overweight and obesity (at 7 years of age) | |
| [47] | Denmark | birth cohort study | 35,435 | during fetal life | 14.5–27.5 years | Margarine | Vitamin D | NA | Gestational hypertension, preeclampsia (including mild and unspecified preeclampsia and toxemia), eclampsia (including severe preeclampsia and eclampsia) |
| Certainty Assessment | No of Patients | Effect | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Vitamin A-Fortified Oils or Fats | Same Oils or Fats without Vitamin A | Relative (95% CI) | Absolute (95% CI) | ||
| Serum retinol (µmol/L)—Randomized Studies (follow-up: 6 months) | ||||||||||||
| 2 [27,28] | randomized trials | serious a | serious b | not serious | not serious c | none | 307 | 207 | - | MD 0.35 µmol/L higher(0.43 lower to 1.12 higher) | ⊕⊕◯◯ Low | CRITICAL |
| Serum retinol (µmol/L)— non-randomized studies (follow-up: between 2 and 5 months) | ||||||||||||
| 2 [31,32] | randomized trials | serious d | serious b | not serious | serious e | none | 102 | 103 | - | MD 0.31 µmol/L higher(0.18 lower to 0.8 higher) | ⊕◯◯◯ Very low | CRITICAL |
| Subclinical vitamin A deficiency (serum retinol ≤ 0.70 µmol/L)—randomized studies (follow-up: 6 months) | ||||||||||||
| 1 [27] | randomized trials | serious f | not serious | not serious | serious g | none | 0/268 (0.0%) | 0/144 (0.0%) | not estimable | ⊕⊕◯◯ Low | CRITICAL | |
| Subclinical vitamin A deficiency (serum retinol ≤ 0.70 µmol/L)—non-randomized studies (follow-up: 2 months) | ||||||||||||
| 1 [31] | randomized trials | serious f | not serious | not serious | very serious h | none | 0/15 (0.0%) | 2/16 (12.5%) | RR 0.21 (0.01 to 4.10) | 99 fewer per 1 000 (from 124 fewer to 387 more) | ⊕◯◯◯ Very low | CRITICAL |
| Clinical vitamin A deficiency (xerophthalmia, night blindness)—not measured | ||||||||||||
| - | - | - | - | - | - | - | - | CRITICAL | ||||
| All-cause morbidity—randomized studies (follow-up: 6 months) | ||||||||||||
| 2 [27,28] | randomized trials | very serious i | not serious | not serious | not serious | none | Out of two RCTs measuring morbidity, one (with 268 participants in the intervention and 144 in the control group) reported results as frequency and duration of illness. This study reported no significant differences between study groups. | ⊕⊕◯◯ Low | CRITICAL | |||
| All-cause morbidity—non-randomized studies (follow-up: 2 months) | ||||||||||||
| 1 [31] | randomized trials | Serious f | not serious j | not serious | very serious h | none | One CCT reported morbidity scores (defined as frequency of illness multiplied by duration of illness) and described no significant differences between study groups. | ⊕◯◯◯ Very low | CRITICAL | |||
| All-cause mortality—not measured | ||||||||||||
| - | - | - | - | - | - | - | - | CRITICAL | ||||
| Adverse effects (hypervitaminosis, liver toxicity)—not measured | ||||||||||||
| - | - | - | - | - | - | - | - | CRITICAL | ||||
3.4. Primary Outcomes for Studies on Vitamin D Fortification versus No Fortification with Vitamin D
3.5. Secondary Outcomes for Studies on Vitamin A Fortification versus No Fortification with Vitamin A
3.6. Secondary Outcomes for Studies on Vitamin D Fortification versus No Fortification with Vitamin D
4. Discussion
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Keats, E.C.; Neufeld, L.M.; Garrett, G.S.; Mbuya, M.N.N.; Bhutta, Z.A. Improved micronutrient status and health outcomes in low- and middle-income countries following large-scale fortification: Evidence from a systematic review and meta-analysis. Am. J. Clin. Nutr. 2019, 109, 1696–1708. [Google Scholar] [CrossRef] [PubMed]
- Stephensen, C.B. Vitamin A, infection, and immune function. Annu. Rev. Nutr. 2001, 21, 167–192. [Google Scholar] [CrossRef] [PubMed]
- Carazo, A.; Macakova, K.; Matousova, K.; Krcmova, L.K.; Protti, M.; Mladenka, P. Vitamin A Update: Forms, Sources, Kinetics, Detection, Function, Deficiency, Therapeutic Use and Toxicity. Nutrients 2021, 13, 1703. [Google Scholar] [CrossRef] [PubMed]
- Vijayaraghavan, K. National control programme against nutritional blindness due to vitamin A deficiency: Current status & future strategy. Indian J. Med. Res. 2018, 148, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Wirth, J.P.; Petry, N.; Tanumihardjo, S.A.; Rogers, L.M.; McLean, E.; Greig, A.; Garrett, G.S.; Klemm, R.D.; Rohner, F. Vitamin A Supplementation Programs and Country-Level Evidence of Vitamin A Deficiency. Nutrients 2017, 9, 190. [Google Scholar] [CrossRef] [PubMed]
- Sherwin, J.C.; Reacher, M.H.; Dean, W.H.; Ngondi, J. Epidemiology of vitamin A deficiency and xerophthalmia in at-risk populations. Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 205–214. [Google Scholar] [CrossRef]
- WHO. Global prevalence of vitamin A deficiency in populations at risk 1995–2005: WHO global database on vitamin A deficiency. Available online: https://www.who.int/publications/i/item/9789241598019 (accessed on 2 September 2023).
- Vanherwegen, A.S.; Gysemans, C.; Mathieu, C. Regulation of Immune Function by Vitamin D and Its Use in Diseases of Immunity. Endocrinol. Metab. Clin. N. Am. 2017, 46, 1061–1094. [Google Scholar] [CrossRef]
- DeLuca, H.F. Overview of general physiologic features and functions of vitamin D. Am. J. Clin. Nutr. 2004, 80, 1689S–1696S. [Google Scholar] [CrossRef]
- Roth, D.E.; Abrams, S.A.; Aloia, J.; Bergeron, G.; Bourassa, M.W.; Brown, K.H.; Calvo, M.S.; Cashman, K.D.; Combs, G.; De-Regil, L.M.; et al. Global prevalence and disease burden of vitamin D deficiency: A roadmap for action in low- and middle-income countries. Ann. N. Y. Acad. Sci. 2018, 1430, 44–79. [Google Scholar] [CrossRef]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid Biochem. Mol. Biol. 2014, 144 Pt A, 138–145. [Google Scholar] [CrossRef]
- Kimball, S.M.; Holick, M.F. Official recommendations for vitamin D through the life stages in developed countries. Eur. J. Clin. Nutr. 2020, 74, 1514–1518. [Google Scholar] [CrossRef]
- Lips, P.; de Jongh, R.T.; van Schoor, N.M. Trends in Vitamin D Status Around the World. JBMR Plus 2021, 5, e10585. [Google Scholar] [CrossRef]
- Prentice, A. Nutritional rickets around the world. J. Steroid Biochem. Mol. Biol. 2013, 136, 201–206. [Google Scholar] [CrossRef]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Kostenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines on Food Fortification with Micronutrients. 2006. Available online: https://apps.who.int/iris/handle/10665/43412 (accessed on 21 November 2023).
- FAO. World Food and Agriculture: Statistical Yearbook 2021. Rome. 2021. FIGURE 23: World Production of Vegetable Oils, Main Commodities. Available online: https://www.fao.org/documents/card/en/c/cb4477en (accessed on 21 November 2023).
- Hombali, A.S.; Solon, J.A.; Venkatesh, B.T.; Nair, N.S.; Pena-Rosas, J.P. Fortification of staple foods with vitamin A for vitamin A deficiency. Cochrane Database Syst. Rev. 2019, 5, CD010068. [Google Scholar] [CrossRef]
- Dunlop, E.; Kiely, M.E.; James, A.P.; Singh, T.; Pham, N.M.; Black, L.J. Vitamin D Food Fortification and Biofortification Increases Serum 25-Hydroxyvitamin D Concentrations in Adults and Children: An Updated and Extended Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Nutr. 2021, 151, 2622–2635. [Google Scholar] [CrossRef]
- Mendu, V.V.R.; Nair, K.P.M.; Athe, R. Systematic review and meta-analysis approach on vitamin A fortified foods and its effect on retinol concentration in under 10 year children. Clin. Nutr. ESPEN 2019, 30, 126–130. [Google Scholar] [CrossRef]
- Al Khalifah, R.; Alsheikh, R.; Alnasser, Y.; Alsheikh, R.; Alhelali, N.; Naji, A.; Al Backer, N. The impact of vitamin D food fortification and health outcomes in children: A systematic review and meta-regression. Syst. Rev. 2020, 9, 144. [Google Scholar] [CrossRef]
- Brandao-Lima, P.N.; Santos, B.D.C.; Aguilera, C.M.; Freire, A.R.S.; Martins-Filho, P.R.S.; Pires, L.V. Vitamin D Food Fortification and Nutritional Status in Children: A Systematic Review of Randomized Controlled Trials. Nutrients 2019, 11, 2766. [Google Scholar] [CrossRef]
- Souza, S.V.S.; Borges, N.; Vieira, E.F. Vitamin D-fortified bread: Systematic review of fortification approaches and clinical studies. Food Chem. 2022, 372, 131325. [Google Scholar] [CrossRef]
- Gasparri, C.; Perna, S.; Spadaccini, D.; Alalwan, T.; Girometta, C.; Infantino, V.; Rondanelli, M. Is vitamin D-fortified yogurt a value-added strategy for improving human health? A systematic review and meta-analysis of randomized trials. J. Dairy Sci. 2019, 102, 8587–8603. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Syn. Meth. 2020, 12, 55–61. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Candelaria, L.V.; Magsadia, C.R.; Velasco, R.E.; Pedro, M.R.; Barba, C.V.; Tanchoco, C.C. The effect of vitamin A-fortified coconut cooking oil on the serum retinol concentration of Filipino children 4–7 years old. Asia Pac. J. Clin. Nutr. 2005, 14, 43–53. [Google Scholar]
- Atalhi, N.; El Hamdouchi, A.; Barkat, A.; Elkari, K.; Hamrani, A.; El Mzibri, M.; Haskell, M.J.; Mokhtar, N.; Aguenaou, H. Combined consumption of a single high-dose vitamin A supplement with provision of vitamin A fortified oil to households maintains adequate milk retinol concentrations for 6 months in lactating Moroccan women. Appl. Physiol. Nutr. Metab. 2020, 45, 275–282. [Google Scholar] [CrossRef]
- Atalhi, N.; Choua, G.; Elhamdouchi, A.; Elhaloui, N.; Elmzibri, M.; Haskell, M.; Aguenaou, H.; Mokhtar, N. Impact of daily consumption of Vitamin A fortified oil on human milk Vitamin A concentration in lactating Moroccan women. Ann. Nutr. Metab. 2011, 58, 6. [Google Scholar] [CrossRef]
- PACTR201512001217212. Combined Consumption of a Single High-Dose Vitamin A Supplement and Provision of Vitamin A Fortified Oil to Households Maintains Adequate Milk Retinol. 2015. Available online: https://pactr.samrc.ac.za/TrialDisplay.aspx?TrialID=1217 (accessed on 21 November 2023).
- Marliyati, S.A.; Martianto, D.; Andarwulan, N.; Fauzi, S. Efficacy of non-branded cooking oil fortified with carotene from RPO on blood retinol and IgG of children aged 7–9 years. Pak. J. Nutr. 2016, 15, 419–426. [Google Scholar] [CrossRef]
- Wang, D.L.; Xiao, Q.M.; Hong, Y.; Li, S.T.; Chen, W.Q.; Cheng, Y.Y. Effects of vitamin A-fortified edible oil on improving the immune fuction of children. Acta Nutr. Sin. 2006, 28, 40–46. [Google Scholar]
- Keller, A.; Angquist, L.; Jacobsen, R.; Vaag, A.; Heitmann, B.L. A retrospective analysis of a societal experiment among the Danish population suggests that exposure to extra doses of vitamin A during fetal development may lower type 2 diabetes mellitus (T2DM) risk later in life. Br. J. Nutr. 2017, 117, 731–736. [Google Scholar] [CrossRef]
- Ghasemifard, N.; Nasimi, N.; Hassanzadeh-Rostami, Z.; Abbasi, A.; Faghih, S. Effects of vitamin D fortified canola oil on vitamin D and lipid profiles in healthy adults: A double-blind randomized trial. Iran. J. Nutr. Sci. Food Technol. 2020, 15, 28–35. [Google Scholar]
- Ghasemifard, N.; Hassanzadeh-Rostami, Z.; Abbasi, A.; Naghavi, A.M.; Faghih, S. Effects of vitamin D-fortified oil intake versus vitamin D supplementation on vitamin D status and bone turnover factors: A double blind randomized clinical trial. Clin. Nutr. ESPEN 2022, 47, 28–35. [Google Scholar] [CrossRef]
- Irct20180708040401N. Fortification and Supplementation Effect on Vitamin D Levels. 2018. Available online: https://trialsearch.who.int/Trial2.aspx?TrialID=IRCT20180708040401N1 (accessed on 21 November 2023).
- Stougaard, M.; Damm, P.; Frederiksen, P.; Jacobsen, R.; Heitmann, B.L. Extra vitamin D from fortification and the risk of preeclampsia: The D-tect Study. PLoS ONE 2018, 13, e0191288. [Google Scholar] [CrossRef]
- Moos, C.; Duus, K.S.; Frederiksen, P.; Heitmann, B.L.; Andersen, V. Exposure to the Danish Mandatory Vitamin D Fortification Policy in Prenatal Life and the Risk of Developing Coeliac Disease-The Importance of Season: A Semi Ecological Study. Nutrients 2020, 12, 1243. [Google Scholar] [CrossRef]
- Duus, K.S.; Moos, C.; Frederiksen, P.; Andersen, V.; Heitmann, B.L. Prenatal and Early Life Exposure to the Danish Mandatory Vitamin D Fortification Policy Might Prevent Inflammatory Bowel Disease Later in Life: A Societal Experiment. Nutrients 2021, 13, 1367. [Google Scholar] [CrossRef]
- Keller, A.; Stougard, M.; Frederiksen, P.; Thorsteinsdottir, F.; Vaag, A.; Damm, P.; Jacobsen, R.; Heitmann, B.L. In Utero exposure to extra vitamin D from food fortification and the risk of subsequent development of gestational diabetes: The D-tect study. Nutr. J. 2018, 17, 100. [Google Scholar] [CrossRef]
- NCT03330301. D-tecting Disease—From Exposure to Vitamin D During Critical Periods of Life. 2012. Available online: https://ClinicalTrials.gov/show/NCT03330301 (accessed on 21 November 2023).
- Jacobsen, R.; Abrahamsen, B.; Bauerek, M.; Holst, C.; Jensen, C.B.; Knop, J.; Raymond, K.; Rasmussen, L.B.; Stougaard, M.; Sorensen, T.I.; et al. The influence of early exposure to vitamin D for development of diseases later in life. BMC Public Health 2013, 13, 515. [Google Scholar] [CrossRef]
- Thorsteinsdottir, F.; Maslova, E.; Jacobsen, R.; Frederiksen, P.; Keller, A.; Backer, V.; Heitmann, B.L. Exposure to Vitamin D Fortification Policy in Prenatal Life and the Risk of Childhood Asthma: Results From the D-Tect Study. Nutrients 2019, 11, 24. [Google Scholar] [CrossRef]
- Jacobsen, R.; Hypponen, E.; Sorensen, T.I.; Vaag, A.A.; Heitmann, B.L. Gestational and Early Infancy Exposure to Margarine Fortified with Vitamin D through a National Danish Programme and the Risk of Type 1 Diabetes: The D-Tect Study. PLoS ONE 2015, 10, e0128631. [Google Scholar] [CrossRef]
- Jacobsen, R.; Moldovan, M.; Vaag, A.A.; Hypponen, E.; Heitmann, B.L. Vitamin D fortification and seasonality of birth in type 1 diabetic cases: D-tect study. J. Dev. Orig. Health Dis. 2016, 7, 114–119. [Google Scholar] [CrossRef]
- Handel, M.N.; Frederiksen, P.; Osmond, C.; Cooper, C.; Abrahamsen, B.; Heitmann, B.L. Prenatal exposure to vitamin D from fortified margarine and risk of fractures in late childhood: Period and cohort results from 222,000 subjects in the D-tect observational study. Br. J. Nutr. 2017, 117, 872–881. [Google Scholar] [CrossRef]
- Jensen, C.B.; Berentzen, T.L.; Gamborg, M.; Sorensen, T.I.; Heitmann, B.L. Does prenatal exposure to vitamin D-fortified margarine and milk alter birth weight? A societal experiment. Br. J. Nutr. 2014, 112, 785–793, Erratum in Br. J. Nutr. 2016, 116, 377–379. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.B.; Gamborg, M.; Berentzen, T.L.; Sørensen, T.I.A.; Heitmann, B.L. Prenatal exposure to vitamin-D from fortified margarine and milk and body size at age 7 years. Eur. J. Clin. Nutr. 2015, 69, 1169–1175. [Google Scholar] [CrossRef] [PubMed]
- Stougaard, M.; Damm, P.; Frederiksen, P.; Jacobsen, R.; Heitmann, B.L. Exposure to vitamin D from fortified margarine during fetal life and later risk of pre-eclampsia: The D-tect Study. Public Health Nutr. 2018, 21, 721–731. [Google Scholar] [CrossRef] [PubMed]
- Bjelakovic, G.; Gluud, L.L.; Nikolova, D.; Whitfield, K.; Wetterslev, J.; Simonetti, R.G.; Bjelakovic, M.; Gluud, C. Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst. Rev. 2014, 10, CD007470. [Google Scholar] [CrossRef] [PubMed]
- Black, L.J.; Seamans, K.M.; Cashman, K.D.; Kiely, M. An updated systematic review and meta-analysis of the efficacy of vitamin D food fortification. J. Nutr. 2012, 142, 1102–1108. [Google Scholar] [CrossRef]
- Nikooyeh, B.; Neyestani, T.R. The effects of vitamin D-fortified foods on circulating 25(OH)D concentrations in adults: A systematic review and meta-analysis. Br. J. Nutr. 2022, 127, 1821–1838. [Google Scholar] [CrossRef] [PubMed]
- Rohner, F.; Wirth, J.P.; Zeng, W.; Petry, N.; Donkor, W.E.S.; Neufeld, L.M.; Mkambula, P.; Groll, S.; Mbuya, M.N.; Friesen, V.M. Global Coverage of Mandatory Large-Scale Food Fortification Programs: A Systematic Review and Meta-Analysis. Adv. Nutr. 2023, 14, 1197–1210. [Google Scholar] [CrossRef]
- Stevens, G.A.; Beal, T.; Mbuya, M.N.N.; Luo, H.; Neufeld, L.M. Micronutrient deficiencies among preschool-aged children and women of reproductive age worldwide: A pooled analysis of individual-level data from population-representative surveys. Lancet. Glob. Health 2022, 10, e1590–e1599. [Google Scholar] [CrossRef]
- Van Schoor, N.; Lips, P. Global Overview of Vitamin D Status. Endocrinol. Metab. Clin. N. Am. 2017, 46, 845–870. [Google Scholar] [CrossRef]
- Cianferotti, L.; Marcocci, C. Subclinical vitamin D deficiency. Best Pract. Res. Clin. Endocrinol. Metab. 2012, 26, 523–537. [Google Scholar] [CrossRef]
- Mogire, R.M.; Mutua, A.; Kimita, W.; Kamau, A.; Bejon, P.; Pettifor, J.M.; Adeyemo, A.; Williams, T.N.; Atkinson, S.H. Prevalence of vitamin D deficiency in Africa: A systematic review and meta-analysis. Lancet. Glob. Health 2020, 8, e134–e142. [Google Scholar] [CrossRef] [PubMed]
- Bartley, J. Vitamin D: Emerging roles in infection and immunity. Expert Rev. Anti-Infect. Ther. 2010, 8, 1359–1369. [Google Scholar] [CrossRef] [PubMed]

| References | Country | Study Design | Sample Size (n) | Age at Exposure | Age at Outcome Measurement | Fortified Product | Micronutrient(s) Added to the Fortified Products | Duration of Intervention | Outcomes | |
|---|---|---|---|---|---|---|---|---|---|---|
| Marliyati 2016 | [31] | Indonesia | controlled clinical trial | 31 | 7–9 years | 7–9 years | Non-branded cooking oil | Carotene from red palm oil | 8 weeks | Se retinol; IgG level; sub-clinical vitamin A deficiency; dietary intake of energy, protein, fat, vitamin A; consumption of cooking oil; BMI; WAZ (results not reported); morbidity |
| Candelaria 2005 | [27] | Philippines | randomized controlled trail | 622 | 4–7 years | 4–7 years | Coconut oil | Vitamin A | 6 months | Se retinol; dietary intake of energy, protein, vitamin C, vitamin A; distribution of subjects by sources of vitamin A; sub-clinical vitamin A deficiency; WHZ (results not reported); proportion of children with low WHZ; morbidity; cooking practices; cooking oil use |
| Atalhi 2020 | [28,29,30] | Morocco | randomized controlled trial | 140 | 19–40 years | 19–40 years | Soy oil | Vitamin A | 6 months | Se retinol; retinol in breast milk; proportion of mothers with low concentrations of retinol in their breast milk; breast milk fat; CRP; proportion of mothers who consumed foods rich in vitamin A; morbidity (results not reported) |
| Keller 2020 | [33] | Denmark | birth cohort study | 193,803 | during fetal life | NA | Margarine | Vitamin A | NA | incidence of type 2 diabetes mellitus |
| Donglan 2006 | [32] | China | controlled clinical trial | 174 | 9–11 years | 9–11 years | Oil | Vitamin A | 5 months | Se levels of vitamin A, IgA, IgG, IgM, complement C3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szabó, É.; Csölle, I.; Felső, R.; Kuellenberg de Gaudry, D.; Nyakundi, P.N.; Ibrahim, K.; Metzendorf, M.-I.; Ferenci, T.; Lohner, S. Benefits and Harms of Edible Vegetable Oils and Fats Fortified with Vitamins A and D as a Public Health Intervention in the General Population: A Systematic Review of Interventions. Nutrients 2023, 15, 5135. https://doi.org/10.3390/nu15245135
Szabó É, Csölle I, Felső R, Kuellenberg de Gaudry D, Nyakundi PN, Ibrahim K, Metzendorf M-I, Ferenci T, Lohner S. Benefits and Harms of Edible Vegetable Oils and Fats Fortified with Vitamins A and D as a Public Health Intervention in the General Population: A Systematic Review of Interventions. Nutrients. 2023; 15(24):5135. https://doi.org/10.3390/nu15245135
Chicago/Turabian StyleSzabó, Éva, Ildikó Csölle, Regina Felső, Daniela Kuellenberg de Gaudry, Patrick Nyamemba Nyakundi, Kazahyet Ibrahim, Maria-Inti Metzendorf, Tamás Ferenci, and Szimonetta Lohner. 2023. "Benefits and Harms of Edible Vegetable Oils and Fats Fortified with Vitamins A and D as a Public Health Intervention in the General Population: A Systematic Review of Interventions" Nutrients 15, no. 24: 5135. https://doi.org/10.3390/nu15245135