
Associations between Delayed Introduction of Complementary Foods and Childhood Health Consequences in Exclusively Breastfed Children
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
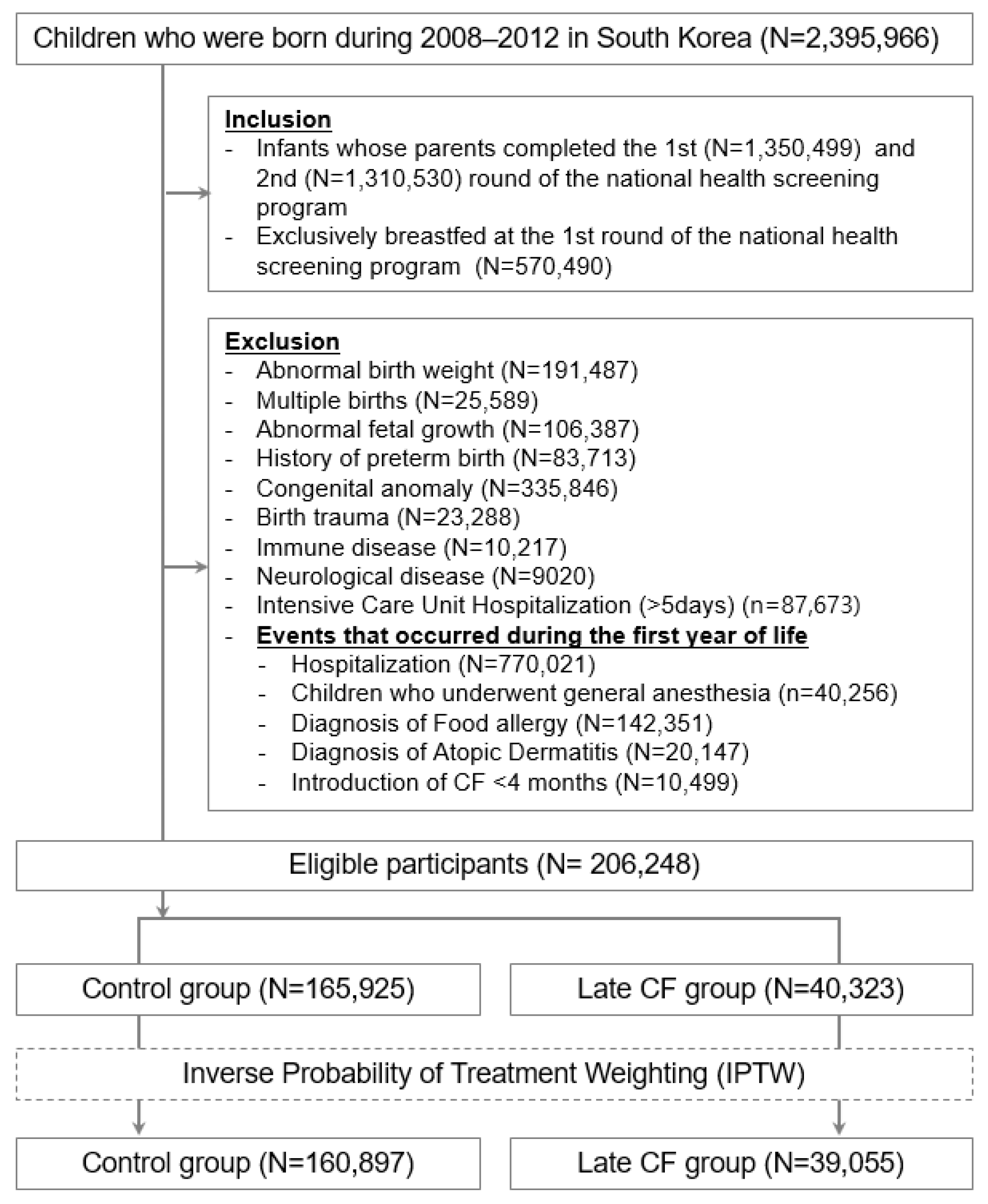
2.1. Study Population and Setting
2.2. Data Sources and Study Period
2.3. Exposure Measurements
2.4. Outcome Measurements
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Participating Children
3.2. Effect of Delayed CF Introduction on the Risk of Hospitalization and Death
3.3. Effect of Delayed CF Introduction on the Risk for Different Clinical Diseases
3.4. Effect of Delayed CF Introduction on the Risk for Excessive Weight Gain and Short Height
3.5. Effect of Delayed CF Introduction on the Frequency of Admission to the Hospital and ICU
4. Discussion
4.1. Principal Findings
4.2. Comparison with Other Studies
4.3. Clinical Implications
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Complementary Feeding. Available online: https://www.who.int/health-topics/complementary-feeding (accessed on 1 October 2021).
- Ha, E.K.; Kim, J.H.; Baek, H.S.; Lee, E.; Baek, J.H.; Shim, S.; Kim, Y.H.; Moreno, L.A.; Lee, S.W.; Han, M.Y. Association between complementary food introduction before age 4 months and body mass index at age 5-7 years: A retrospective population-based longitudinal cohort study. J. Hum. Nutr. Diet. 2023, 36, 787–797. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E. Effect of breastfeeding on infant and child mortality due to infectious diseases in less developed countries: A pooled analysis. WHO Collaborative Study Team on the Role of Breastfeeding on the Prevention of Infant Mortality. Lancet 2000, 355, 451–455. [Google Scholar]
- Lanigan, J.A.; Bishop, J.; Kimber, A.C.; Morgan, J. Systematic review concerning the age of introduction of complementary foods to the healthy full-term infant. Eur. J. Clin. Nutr. 2001, 55, 309–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duffy, D.M. How complementary feeding in infants affects allergies, chronic disease, and neurodevelopment. JAAPA 2020, 33, 14–18. [Google Scholar] [CrossRef] [Green Version]
- Martorell, R. Improved nutrition in the first 1000 days and adult human capital and health. Am. J. Hum. Biol. 2017, 29, e22952. [Google Scholar] [CrossRef] [Green Version]
- Hirvonen, K.; Wolle, A.; Laillou, A.; Vinci, V.; Chitekwe, S.; Baye, K. Understanding delays in the introduction of complementary foods in rural Ethiopia. Matern. Child. Nutr. 2021, e13247. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Verma, S.; Faridi, M. Complementary feeding—Reasons for inappropriateness in timing, quantity and consistency. Indian. J. Pediatr. 2008, 75, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Wells, J.C. Duration of exclusive breast-feeding: Introduction of complementary feeding may be necessary before 6 months of age. Br. J. Nutr. 2005, 94, 869–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brew, B.K.; Kull, I.; Garden, F.; Almqvist, C.; Bergstrom, A.; Lind, T.; Webb, K.; Wickman, M.; Marks, G.B. Breastfeeding, asthma, and allergy: A tale of two cities. Pediatr. Allergy Immunol. 2012, 23, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Shin, M.; Lee, B. Influence of age at complementary food introduction on the development of asthma and atopic dermatitis in Korean children aged 1-3 years. Clin. Exp. Pediatr. 2021, 64, 408–414. [Google Scholar] [CrossRef]
- Kim, J.H.; Lee, J.E.; Shim, S.M.; Ha, E.K.; Yon, D.K.; Kim, O.H.; Baek, J.H.; Koh, H.Y.; Chae, K.Y.; Lee, S.W.; et al. Cohort profile: National Investigation of Birth Cohort in Korea study 2008 (NICKs-2008). Clin. Exp. Pediatr. 2021, 64, 480–488. [Google Scholar] [CrossRef]
- Ha, E.K.; Lee, S.W.; Kim, J.H.; Shim, S.; Kim, Y.H.; Song, J.Y.; Koh, H.Y.; Shin, Y.H.; Han, M.Y. Neurodevelopmental Outcomes in Infants Fed with Soy Formula: A Retrospective, National Population-Based Observational Cohort Study. J. Nutr. 2021, 151, 3045–3052. [Google Scholar] [CrossRef]
- Bartick, M.; Reinhold, A. The burden of suboptimal breastfeeding in the United States: A pediatric cost analysis. Pediatrics 2010, 125, e1048–e1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.H.; Lee, S.W.; Lee, J.E.; Ha, E.K.; Han, M.Y.; Lee, E. Breastmilk Feeding during the First 4 to 6 Months of Age and Childhood Disease Burden until 10 Years of Age. Nutrients 2021, 13, 2824. [Google Scholar] [CrossRef]
- Kramer, M.S.; Kakuma, R. Optimal duration of exclusive breastfeeding. Cochrane Database Syst. Rev. 2012, CD003517. [Google Scholar] [CrossRef]
- WHO. Exclusive Breastfeeding for Six Months Best for Babies Everywhere. Available online: https://www.who.int/news/item/15-01-2011-exclusive-breastfeeding-for-six-months-best-for-babies-everywhere (accessed on 15 January 2011).
- Kim, J.H.; Yun, S.; Hwang, S.S.; Shim, J.O.; Chae, H.W.; Lee, Y.J.; Lee, J.H.; Kim, S.C.; Lim, D.; Yang, S.W.; et al. The 2017 Korean National Growth Charts for children and adolescents: Development, improvement, and prospects. Korean J. Pediatr. 2018, 61, 135–149. [Google Scholar] [CrossRef] [Green Version]
- Berry, J.G.; Hall, M.; Hall, D.E.; Kuo, D.Z.; Cohen, E.; Agrawal, R.; Mandl, K.D.; Clifton, H.; Neff, J. Inpatient growth and resource use in 28 children’s hospitals: A longitudinal, multi-institutional study. JAMA Pediatr. 2013, 167, 170–177. [Google Scholar] [CrossRef]
- Matriano, M.G.; Ivers, R.; Meedya, S. Factors that influence women’s decision on infant feeding: An integrative review. Women Birth 2021, 35, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Graffy, J.; Taylor, J. What information, advice, and support do women want with breastfeeding? Birth 2005, 32, 179–186. [Google Scholar] [CrossRef]
- Bae, S.P.; Lee, W.R.; Hahn, W.H.; Shin, H.J.; Ahn, Y.M.; Shin, S.M.; Kim, Y.J.; Kim, E.A.; Shin, Y.J.; Yi, D.Y.; et al. Survey of Korean pediatrician’s perceptions of barriers to and improvements in breastfeeding. Clin. Exp. Pediatr. 2022, 65, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Gingras, V.; Aris, I.M.; Rifas-Shiman, S.L.; Switkowski, K.M.; Oken, E.; Hivert, M.F. Timing of Complementary Feeding Introduction and Adiposity Throughout Childhood. Pediatrics 2019, 144, e20191320. [Google Scholar] [CrossRef] [PubMed]
- Quigley, M.A.; Kelly, Y.J.; Sacker, A. Breastfeeding and hospitalization for diarrheal and respiratory infection in the United Kingdom Millennium Cohort Study. Pediatrics 2007, 119, e837–e842. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.S.; Guo, T.; Platt, R.W.; Sevkovskaya, Z.; Dzikovich, I.; Collet, J.P.; Shapiro, S.; Chalmers, B.; Hodnett, E.; Vanilovich, I.; et al. Infant growth and health outcomes associated with 3 compared with 6 mo of exclusive breastfeeding. Am. J. Clin. Nutr. 2003, 78, 291–295. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Lee, E.; Ha, E.K.; Lee, G.C.; Shin, J.; Baek, H.S.; Choi, S.H.; Shin, Y.H.; Han, M.Y. Infant Feeding Pattern Clusters Are Associated with Childhood Health Outcomes. Nutrients 2023, 15, 3065. [Google Scholar] [CrossRef] [PubMed]
- Oddy, W.H.; Mori, T.A.; Huang, R.C.; Marsh, J.A.; Pennell, C.E.; Chivers, P.T.; Hands, B.P.; Jacoby, P.; Rzehak, P.; Koletzko, B.V.; et al. Early infant feeding and adiposity risk: From infancy to adulthood. Ann. Nutr. Metab. 2014, 64, 262–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenabi, E.; Bashirian, S.; Salehi, A.M.; Khazaei, S. Not breastfeeding and risk of autism spectrum disorders among children: A meta-analysis. Clin. Exp. Pediatr. 2023, 66, 28–31. [Google Scholar] [CrossRef]
- Shin, E.J.; Kim, Y.; Jeong, J.Y.; Jung, Y.M.; Lee, M.H.; Chung, E.H. The changes of prevalence and etiology of pediatric pneumonia from National Emergency Department Information System in Korea, between 2007 and 2014. Korean J. Pediatr. 2018, 61, 291–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.W.; Yon, D.K.; James, C.C.; Lee, S.; Koh, H.Y.; Sheen, Y.H.; Oh, J.-W.; Han, M.Y.; Sugihara, G. Short-term effects of multiple outdoor environmental factors on risk of asthma exacerbations: Age-stratified time-series analysis. J. Allergy Clin. Immunol. 2019, 144, 1542–1550.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, S.M.; Shin, J.Y.; Kim, M.H.; Lee, S.H.; Choi, S.; Park, B.J. Prevalence of antibiotic use for pediatric acute upper respiratory tract infections in Korea. J. Korean Med. Sci. 2015, 30, 617–624. [Google Scholar] [CrossRef] [Green Version]
- Ryoo, E. Causes of acute gastroenteritis in Korean children between 2004 and 2019. Clin. Exp. Pediatr. 2021, 64, 260–268. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Characteristic | Observed Data (N = 206,248) | Weighted Data (N = 199,952) c | ||||
|---|---|---|---|---|---|---|
| Non-Exposed (N = 165,925) | Exposed (N= 40,323) | SMD, % d | Non-Exposed (N = 160,897) | Exposed (N = 39,055) | SMD, % d | |
| Sex | 1 | 0 | ||||
| Male | 75,738 (45.6) | 18,259 (45.3) | 73,451 (45.6) | 17,837 (45.7) | ||
| Female | 90,187 (54.4) | 22,064 (54.7) | 108,153 (54.4) | 21,218 (54.3) | ||
| Birth year | ||||||
| 2008 | 25,365 (15.3) | 5229 (13.0) | 7 | 23,703 (14.7) | 5756 (14.7) | 0 |
| 2009 | 28,528 (17.2) | 7234 (17.9) | 2 | 27,702 (17.2) | 6726 (17.2) | 0 |
| 2010 | 34,236 (20.6) | 8752 (21.7) | 3 | 33,462 (20.8) | 8115 (20.8) | 0 |
| 2011 | 35,753 (21.6) | 8936 (22.2) | 2 | 35,089 (21.8) | 8501 (21.8) | 0 |
| 2012 | 42,043 (25.3) | 10,172 (25.2) | 0 | 40,941 (25.5) | 9957 (25.5) | 0 |
| Birth residence e | ||||||
| Seoul | 37,868 (22.8) | 8097 (20.1) | 7 | 35,895 (22.5) | 8712 (22.5) | 0 |
| Metropolitan | 37,863 (22.8) | 9378 (23.3) | 1 | 36,839 (23.1) | 8946 (23.1) | 0 |
| City | 79,493 (47.9) | 19,875 (49.3) | 3 | 77,562 (48.6) | 18,831 (48.6) | 0 |
| Rural | 9329 (5.6) | 2608 (6.5) | 4 | 9252 (5.8) | 2238 (5.8) | 0 |
| Income quintile f | ||||||
| 1 (Lowest) | 11,246 (6.8) | 3038 (7.5) | 3 | 11,075 (7.2) | 2694 (7.2) | 0 |
| 2 | 20,943 (12.6) | 5427 (13.5) | 3 | 20,540 (13.3) | 4987 (13.3) | 0 |
| 3 (Middle) | 42,233 (25.5) | 10,287 (25.5) | 0 | 40,992 (26.5) | 9951 (26.5) | 0 |
| 4 | 55,535 (33.5) | 12,942 (32.1) | 3 | 53,494 (34.6) | 12,983 (34.6) | 0 |
| 5 (Highest) | 29,433 (17.7) | 6985 (17.3) | 1 | 28,435 (18.4) | 6898 (18.4) | 0 |
| Observed Data (N = 206,248) | Weighted Data (N = 199,952) c | ||||
|---|---|---|---|---|---|
| Event d | Non-Exposed (N = 165,925) | Exposed (N = 40,323) | Non-Exposed (N = 160,897) | Exposed (N = 39,055) | Weighted IRR (95% CI) e |
| All-cause hospitalization | 55,268 (33.31) | 13,555 (33.62) | 53,758 (33.41) | 13,061 (33.44) | 1.00 (0.98 to 1.02) |
| All-cause ICU admission | 200 (0.12) | 66 (0.16) | 192 (0.12) | 63 (0.16) | 1.34 (1.01 to 1.79) |
| All-cause death | 66 (0.04) | 21 (0.05) | 65 (0.04) | 19 (0.05) | 1.21 (0.72 to 2.02) |
| Observed Data (N = 206,248) | Weighted Data (N = 199,952) c | Weighted IRR | |||
|---|---|---|---|---|---|
| Outcomes, N(%) a, b | Non-Exposed (N = 165,925) | Exposed (N = 40,323) | Non-Exposed (N = 160,897) | Exposed (N = 39,055) | (95% CI), % d |
| Pneumonia | 21,628 (13.03) | 5274 (13.08) | 21,048 (13.08) | 5065 (12.97) | 0.99 (0.96 to 1.02) |
| Asthma | 1460 (0.88) | 381 (0.94) | 1416 (0.88) | 366 (0.94) | 1.06 (0.95 to 1.19) |
| URTI | 8783 (5.29) | 2226 (5.51) | 8583 (5.33) | 2125 (5.44) | 1.02 (0.97 to 1.07) |
| Acute gastroenteritis | 10,995 (6.63) | 2768 (6.86) | 10,688 (6.64) | 2672 (6.84) | 1.03 (0.99 to 1.07) |
| Acute otitis media | 1314 (0.79) | 300 (0.74) | 1272 (0.79) | 293 (0.75) | 0.95 (0.84 to 1.08) |
| Tooth decay | 2181 (1.31) | 490 (1.22) | 2111 (1.31) | 474 (1.21) | 0.93 (0.84 to 1.03) |
| ADHD e | 648 (0.39) | 142 (0.35) | 626 (0.39) | 137 (0.35) | 0.90 (0.75 to 1.08) |
| Autism spectrum disorder | 276 (0.17) | 68 (0.17) | 258 (0.16) | 62 (0.16) | 1.00 (0.76 to 1.32) |
| Epilepsy | 579 (0.35) | 130 (0.32) | 562 (0.35) | 126 (0.32) | 0.92 (0.76 to 1.12) |
| Malignancy | 183 (0.11) | 49 (0.12) | 176 (0.11) | 47 (0.12) | 1.10 (0.79 to 1.51) |
| Observed Data (N = 206,248) | Weighted Data (N = 199,952) c | Weighted IRR | |||
|---|---|---|---|---|---|
| Outcomes, N(%) b | Non-Exposed (N =165,925) | Exposed (N = 40,323) | Non-Exposed (N = 160,897) | Exposed (N = 39,055) | (95% CI), % d |
| Overweight e | 24 596 (14.82) | 6457 (16.01) | 24 128 (15.00) | 5942 (15.21) | 1.01 (0.99 to 1.04) |
| Obesity f | 10 987 (6.62) | 3041 (7.54) | 10 802 (6.71) | 2764 (7.08) | 1.05 (1.01 to 1.09) |
| −1.64 < HAZ ≤ −1.03 g | 22 313 (13.45) | 5704 (14.15) | 21 377 (13.29) | 5742 (14.70) | 1.11 (1.08 to 1.14) |
| HZA ≤ −1.64 g | 6168 (3.72) | 1679 (4.16) | 5869 (3.65) | 1717 (4.40) | 1.21 (1.14 to 1.27) |
| Observed Data (N = 206,248) | Weighted Data (N = 199,952) c | Weighted OR | |||
|---|---|---|---|---|---|
| All-cause Hospitalization, N (%) b | Non-Exposed (N = 165,925) | Exposed (N = 40,323) | Non-Exposed (N = 160,897) | Exposed (N = 39,055) | (95% CI), % d |
| None | 110,657 (66.69) | 26,768 (66.38) | 107,139 (66.59) | 25,994(66.65) | Reference |
| 1–2 events | 40,692 (24.52) | 9819 (24.35) | 39,565 (24.59) | 9488 (24.29) | 0.99 (0.96 to 1.02) |
| 3–5 events | 11,204 (6.75) | 2750 (6.82) | 10,899 (6.77) | 2632 (6.74) | 1.00 (0.95 to 1.04) |
| ≥6 events | 3372 (2.03) | 986 (2.45) | 3294 (2.05) | 941 (2.41) | 1.18 (1.09 to 1.29) |
| All-cause ICU admission, N (%) b | |||||
| None | 165,725 (99.88) | 40,257 (99.84) | 160,705 (99.88) | 38,992 (99.8) | Reference |
| 1 event | 36 (0.02) | 12 (0.03) | 34 (0.02) | 12 (0.03) | 1.39 (0.71 to 2.71) |
| ≥2 events | 164 (0.1) | 54 (0.13) | 158 (0.1) | 51 (0.13) | 1.34 (0.97 to 1.83) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ha, E.K.; Lee, S.W.; Kim, J.H.; Lee, E.; Cha, H.R.; Han, B.E.; Shin, J.; Han, M.Y. Associations between Delayed Introduction of Complementary Foods and Childhood Health Consequences in Exclusively Breastfed Children. Nutrients 2023, 15, 3410. https://doi.org/10.3390/nu15153410
Ha EK, Lee SW, Kim JH, Lee E, Cha HR, Han BE, Shin J, Han MY. Associations between Delayed Introduction of Complementary Foods and Childhood Health Consequences in Exclusively Breastfed Children. Nutrients. 2023; 15(15):3410. https://doi.org/10.3390/nu15153410
Chicago/Turabian StyleHa, Eun Kyo, Seung Won Lee, Ju Hee Kim, Eun Lee, Hye Ryeong Cha, Bo Eun Han, Jeewon Shin, and Man Yong Han. 2023. "Associations between Delayed Introduction of Complementary Foods and Childhood Health Consequences in Exclusively Breastfed Children" Nutrients 15, no. 15: 3410. https://doi.org/10.3390/nu15153410