
Vitamin D Deficiency in COVID-19 Patients and Role of Calcifediol Supplementation



Abstract
:1. Background
2. Materials and Methods
2.1. Study Population
2.2. 25OHD Measurement
2.3. Calcifediol Supplementation
2.4. Statistical Analysis
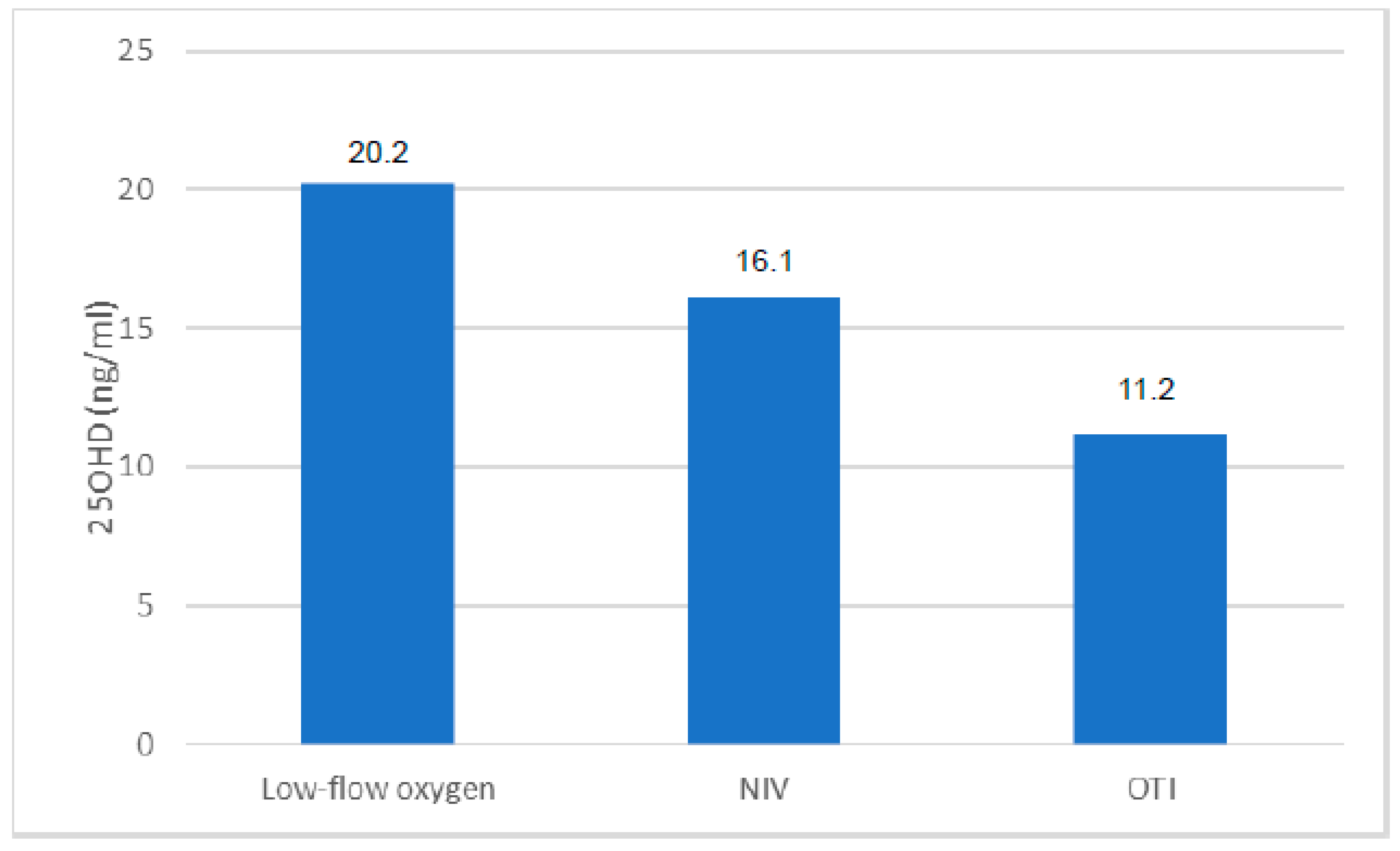
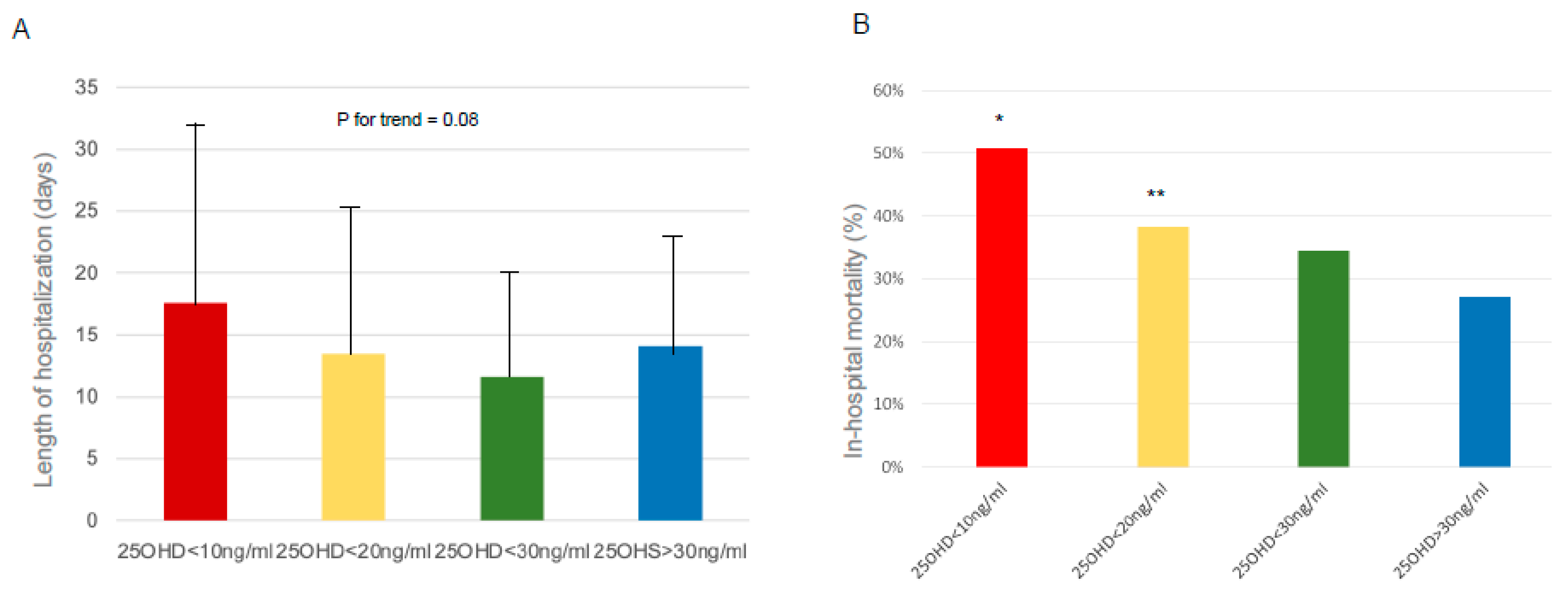
3. Results
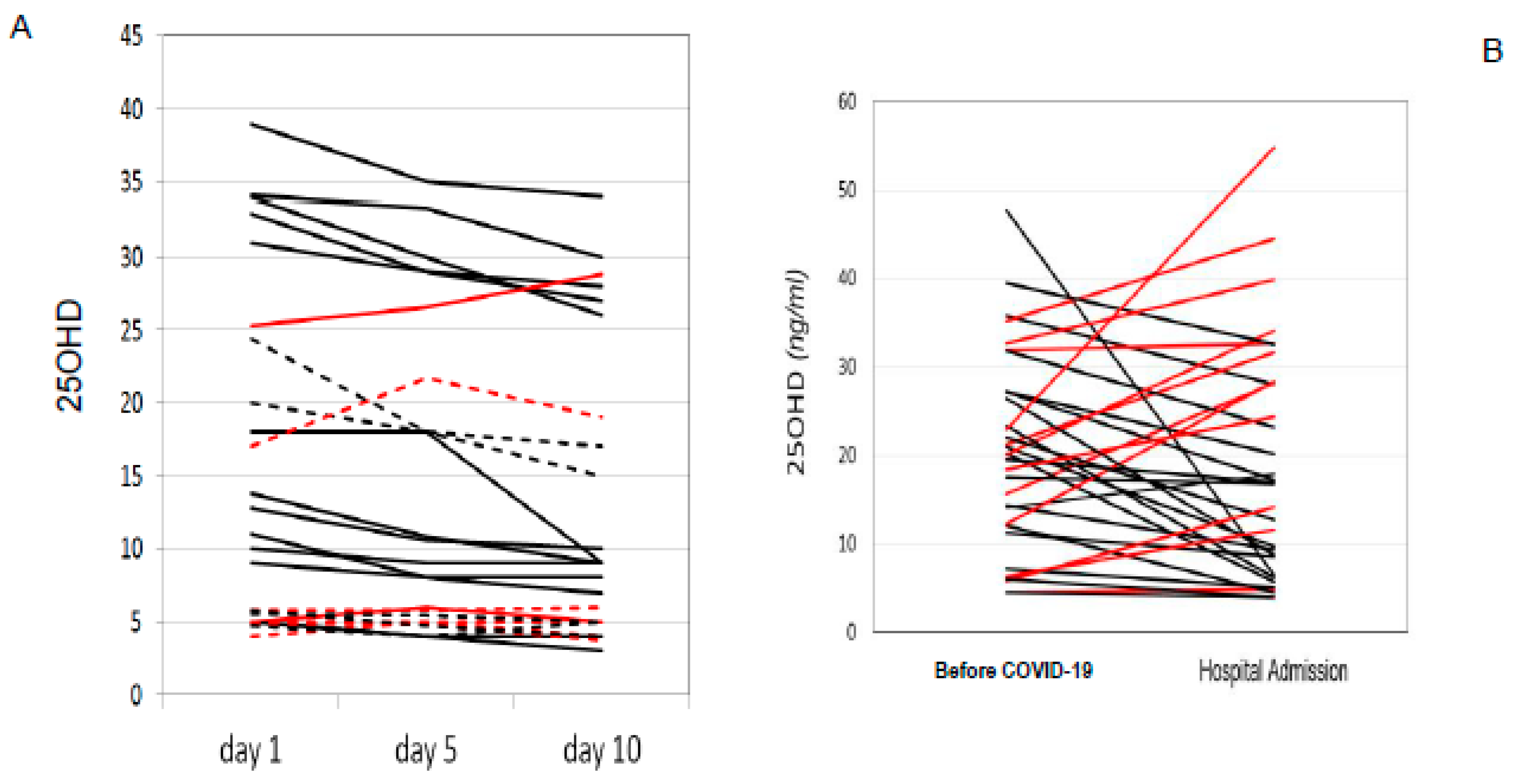
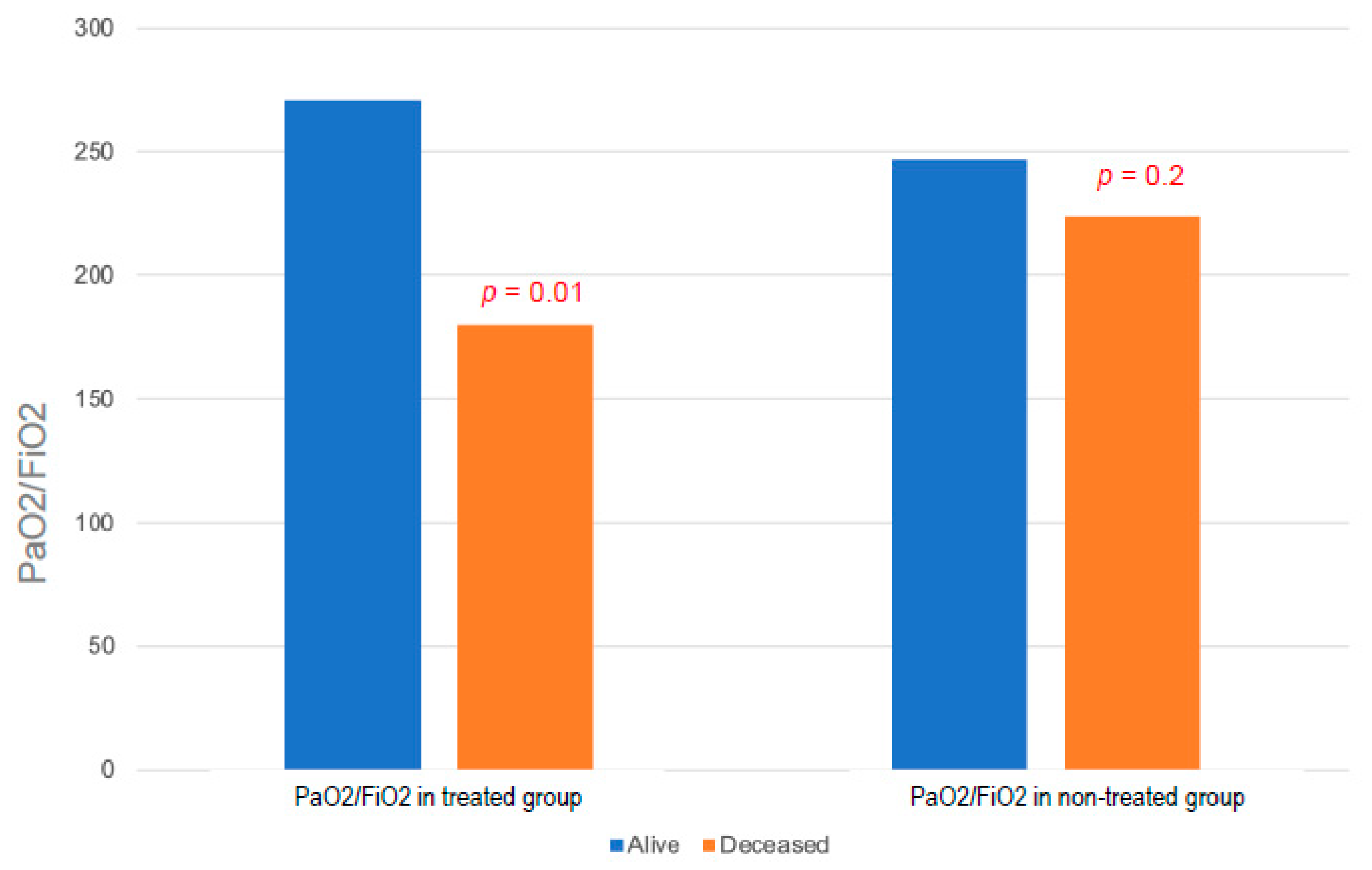
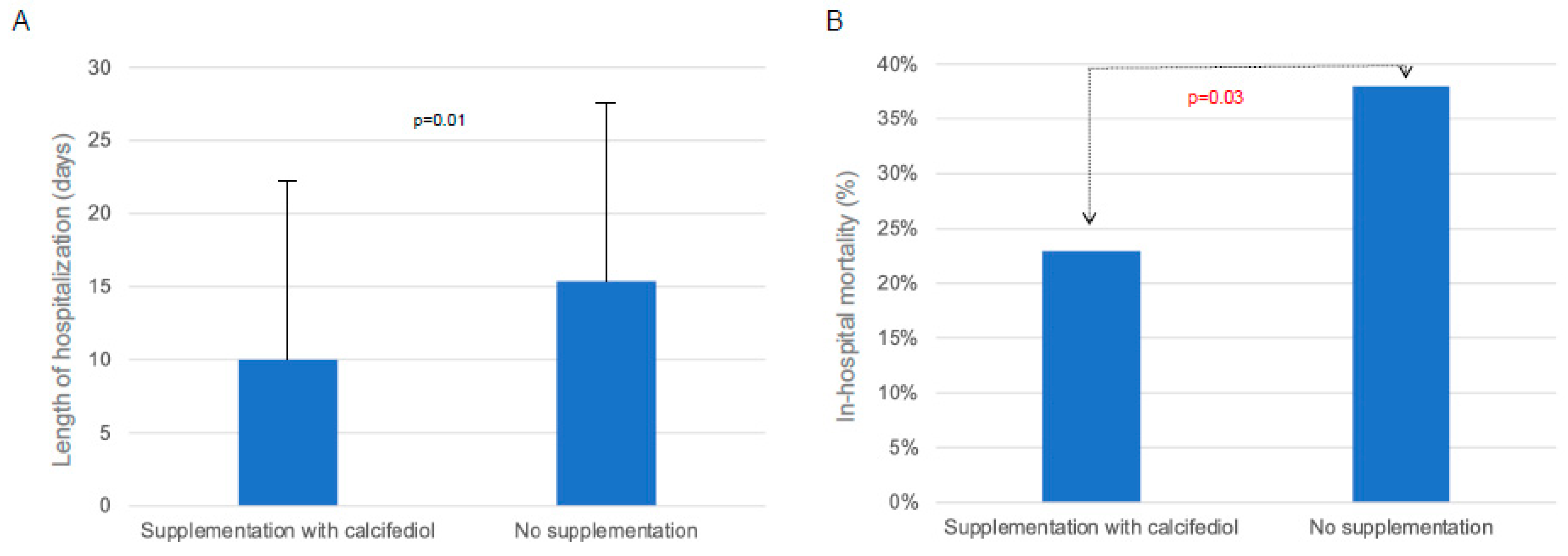
Effects of Calcifediol Supplementation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Cai, H. Sex difference and smoking predisposition in patients with COVID-19. Lancet Respir. Med. 2020, 8, e20. [Google Scholar] [CrossRef] [PubMed]
- Sha, J.; Qie, G.; Yao, Q.; Sun, W.; Wang, C.; Zhang, Z.; Wang, X.; Wang, P.; Jiang, J.; Bai, X.; et al. Sex Differences on Clinical Characteristics, Severity, and Mortality in Adult Patients With COVID-19: A Multicentre Retrospective Study. Front. Med. 2021, 8, 607059. [Google Scholar] [CrossRef] [PubMed]
- Charoenngam, N.; Shirvani, A.; Holick, M.F. Vitamin D for skeletal and non-skeletal health: What we should know. J. Clin. Orthop. Trauma. 2019, 6, 1082–1093. [Google Scholar] [CrossRef]
- Wang, Y.; Zhu, J.; DeLuca, H.F. Where is the vitamin D receptor? Arch. Biochem. Biophys. 2012, 523, 123–133. [Google Scholar] [CrossRef]
- Haussler, M.R.; Jurutka, P.W.; Mizwicki, M.; Norman, A.W. Vitamin D receptor (VDR)-mediated actions of 1α,25(OH)₂vitamin D₃: Genomic and non-genomic mechanisms. Best. Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 543–559. [Google Scholar] [CrossRef]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; et al. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 356, i6583. [Google Scholar] [CrossRef] [Green Version]
- Jolliffe, D.A.; Camargo, C.A., Jr.; Sluyter, J.D.; Aglipay, M.; Aloia, J.F.; Ganmaa, D.; Bergman, P.; Bischoff-Ferrari, H.A.; Borzutzky, A.; Damsgaard, C.T.; et al. Vitamin D supplementation to prevent acute respiratory infections: A systematic review and meta-analysis of aggregate data from randomised controlled trials. Lancet Diabetes Endocrinol. 2021, 9, 276–292. [Google Scholar] [CrossRef]
- Kundu, R.; Chain, B.M.; Coussens, A.K.; Khoo, B.; Noursadeghi, M. Regulation of CYP27B1 and CYP24A1 hydroxylases limits cell-autonomous activation of vitamin D in dendritic cells. Eur. J. Immunol. 2014, 44, 1781–1790. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.T.; Stenger, S.; Li, H.; Wenzel, L.; Tan, B.H.; Krutzik, S.R.; Ochoa, M.T.; Schauber, J.; Wu, K.; Meinken, C.; et al. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science 2006, 311, 1770–1773. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.T.; Schenk, M.; Walker, V.P.; Dempsey, P.W.; Kanchanapoomi, M.; Wheelwright, M.; Vazirnia, A.; Zhang, X.; Steinmeyer, A.; Zügel, U.; et al. Convergence of IL-1beta and VDR activation pathways in human TLR2/1-induced antimicrobial responses. PLoS ONE 2009, 4, e5810. [Google Scholar] [CrossRef] [Green Version]
- Watkins, R.R.; Lemonovich, T.L.; Salata, R.A. An update on the association of vitamin D deficiency with common infectious diseases. Can. J. Physiol. Pharmacol. 2015, 93, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.E.; Finney-Hayward, T.K.; Quint, J.K.; Thomas, C.M.; Tudhope, S.J.; Wedzicha, J.A.; Barnes, P.J.; Donnelly, L.E. Defective macrophage phagocytosis of bacteria in COPD. Eur. Respir. J. 2010, 35, 1039–1047. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, G.B.; Kleijwegt, F.S.; Waelkens, E.; Lage, K.; Nikolic, T.; Hansen, D.A.; Workman, C.T.; Roep, B.O.; Overbergh, L.; Mathieu, C. Differential protein pathways in 1,25-dihydroxyvitamin D3 and dexamethasone modulated tolerogenic human dendritic cells. J. Proteome Res. 2012, 11, 941–971. [Google Scholar] [CrossRef]
- Gombart, A.F.; Borregaard, N.; Koeffler, H.P. Human cathelicidin antimicrobial peptide (CAMP) gene is a direct target of the vitamin D receptor and is strongly up-regulated in myeloid cells by 1,25-dihydroxyvitamin D3. FASEB J. 2005, 19, 1067–1077. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Wang, S.; Li, D.; Chen, P.; Han, S.; Zhao, G.; Chen, Y.; Zhao, J.; Xiong, J.; Qiu, J.; et al. Human Cathelicidin Inhibits SARS-CoV-2 Infection: Killing Two Birds with One Stone. ACS Infect. Dis. 2021, 7, 1545–1554. [Google Scholar] [CrossRef]
- Jeffery, L.E.; Wood, A.M.; Qureshi, O.S.; Hou, T.Z.; Gardner, D.; Briggs, Z.; Kaur, S.; Raza, K.; Sansom, D.M. Availability of 25-hydroxyvitamin D3 to APCs controls the balance between regulatory and inflammatory T cell responses. J. Immunol. 2012, 189, 5155–5164. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, U.; Wakita, D.; Ohkuri, T.; Chamoto, K.; Kitamura, H.; Iwakura, Y.; Nishimura, T. 1α,25-Dihydroxyvitamin D3 and all-trans retinoic acid synergistically inhibit the differentiation and expansion of Th17 cells. Immunol. Lett. 2010, 134, 7–16. [Google Scholar] [CrossRef]
- Palmer, M.T.; Lee, Y.K.; Maynard, C.L.; Oliver, J.R.; Bikle, D.D.; Jetten, A.M.; Weaver, C.T. Lineage-specific effects of 1,25-dihydroxyvitamin D3 on the development of effector CD4 T cells. J. Biol. Chem. 2011, 286, 997–1004. [Google Scholar] [CrossRef] [Green Version]
- Vanherwegen, A.S.; Gysemans, C.; Mathieu, C. Vitamin D endocrinology on the cross-road between immunity and metabolism. Mol. Cell Endocrinol. 2017, 453, 52–67. [Google Scholar] [CrossRef]
- Ali, N. Role of vitamin D in preventing of COVID-19 infection, progression and severity. J. Infect. Public Health 2020, 13, 1373–1380. [Google Scholar] [CrossRef] [PubMed]
- Saponaro, F.; Franzini, M.; Okoye, C.; Antognoli, R.; Campi, B.; Scalese, M.; Neri, T.; Carrozzi, L.; Monzani, F.; Zucchi, R.; et al. Is There a Crucial Link Between Vitamin D Status and Inflammatory Response in Patients with COVID-19? Front. Immunol. 2022, 12, 1664–3224. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, N.M.; Junker, T.G.; Boelt, S.G.; Cohen, A.S.; Munger, K.L.; Stenager, E.; Ascherio, A.; Boding, L.; Hviid, A. Vitamin D status and severity of COVID-19. Sci. Rep. 2022, 12, 19823. [Google Scholar] [CrossRef]
- Nguyen, N.N.; Raju, M.N.P.; da Graca, B.; Wang, D.; Mohamed, N.A.; Mutnal, M.B.; Rao, A.; Bennett, M.; Gokingco, M.; Pham, H.; et al. 25-hydroxyvitamin D is a predictor of COVID-19 severity of hospitalized patients. PLoS ONE 2022, 17, e0268038. [Google Scholar] [CrossRef] [PubMed]
- Güven, M.; Gültekin, H. Association of 25-Hydroxyvitamin D Level with COVID-19-Related in-Hospital Mortality: A Retrospective Cohort Study. J. Am. Nutr. Assoc. 2022, 41, 577–586. [Google Scholar] [CrossRef]
- Davoudi, A.; Najafi, N.; Aarabi, M.; Tayebi, A.; Nikaeen, R.; Izadyar, H.; Salar, Z.; Delavarian, L.; Vaseghi, N.; Daftarian, Z.; et al. Lack of association between vitamin D insufficiency and clinical outcomes of patients with COVID-19 infection. BMC Infect. Dis. 2021, 21, 450. [Google Scholar] [CrossRef]
- Chiodini, I.; Gatti, D.; Soranna, D.; Merlotti, D.; Mingiano, C.; Fassio, A.; Adami, G.; Falchetti, A.; Eller-Vainicher, C.; Rossini, M.; et al. Vitamin D Status and SARS-CoV-2 Infection and COVID-19 Clinical Outcomes. Front. Public Health 2021, 9, 736665. [Google Scholar] [CrossRef]
- Yisak, H.; Ewunetei, A.; Kefale, B.; Mamuye, M.; Teshome, F.; Ambaw, B.; Yideg Yitbarek, G. Effects of Vitamin D on COVID-19 Infection and Prognosis: A Systematic Review. Risk Manag. Healthc. Policy 2021, 14, 31–38. [Google Scholar] [CrossRef]
- Pereira, M.; Dantas Damascena, A.; Galvão Azevedo, L.M.; de Almeida Oliveira, T.; da Mota Santana, J. Vitamin D deficiency aggravates COVID-19: Systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2022, 62, 1308–1316. [Google Scholar] [CrossRef]
- Akbar, M.R.; Wibowo, A.; Pranata, R.; Setiabudiawan, B. Low Serum 25-hydroxyvitamin D (Vitamin D) Level Is Associated with Susceptibility to COVID-19, Severity, and Mortality: A Systematic Review and Meta-Analysis. Front. Nutr. 2021, 8, 660420. [Google Scholar] [CrossRef]
- Tentolouris, N.; Samakidou, G.; Eleftheriadou, I.; Tentolouris, A.; Jude, E.B. The effect of vitamin D supplementation on mortality and intensive care unit admission of COVID-19 patients. A systematic review, meta-analysis and meta-regression. Diabetes Metab. Res. Rev. 2022, 38, e3517. [Google Scholar] [CrossRef]
- Shah, K.; Saxena, D.; Mavalankar, D. Vitamin D supplementation, COVID-19 and disease severity: A meta-analysis. QJM 2021, 114, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Stroehlein, J.K.; Wallqvist, J.; Iannizzi, C.; Mikolajewska, A.; Metzendorf, M.I.; Benstoem, C.; Meybohm, P.; Becker, M.; Skoetz, N.; Stegemann, M.; et al. Vitamin D supplementation for the treatment of COVID-19: A living systematic review. Cochrane Database Syst. Rev. 2021, 5, CD015043. [Google Scholar] [CrossRef] [PubMed]
- Nogues, X.; Ovejero, D.; Pineda-Moncusí, M.; Bouillon, R.; Arenas, D.; Pascual, J.; Ribes, A.; Guerri-Fernandez, R.; Villar-Garcia, J.; Rial, A.; et al. Calcifediol Treatment and COVID-19-Related Outcomes. J. Clin. Endocrinol. Metab. 2021, 106, e4017–e4027. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo, M.E.; Costa, L.M.; Barrios, J.M.; Díaz, J.F.; Miranda, J.L.; Bouillon, R.; Gomez, J.M. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef] [PubMed]
- Bakaloudi, D.R.; Chourdakis, M. A critical update on the role of mild and serious vitamin D deficiency prevalence and the COVID-19 epidemic in Europe. Nutrition 2022, 93, 111441. [Google Scholar] [CrossRef]
- Reid, D.; Toole, B.J.; Knox, S.; Talwar, D.; Harten, J.; O’Reilly, D.S.; Blackwell, S.; Kinsella, J.; McMillan, D.C.; Wallace, A.M. The relation between acute changes in the systemic inflammatory response and plasma 25-hydroxyvitamin D concentrations after elective knee arthroplasty. Am. J. Clin. Nutr. 2011, 93, 1006–1011. [Google Scholar] [CrossRef] [Green Version]
- Smolders, J.; van den Ouweland, J.; Geven, C.; Pickkers, P.; Kox, M. Letter to the Editor: Vitamin D deficiency in COVID-19: Mixing up cause and consequence. Metabolism 2021, 115, 154434. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Schuit, F.; Antonio, L.; Rastinejad, F. Vitamin D Binding Protein: A Historic Overview. Front. Endocrinol. 2020, 10, 910. [Google Scholar] [CrossRef] [PubMed]
- Demir, M.; Demir, F.; Aygun, H. Vitamin D deficiency is associated with COVID-19 positivity and severity of the disease. J. Med. Virol. 2021, 93, 2992–2999. [Google Scholar] [CrossRef]
- Merlotti, D.; Rendina, D.; Muscariello, R.; Picchioni, T.; Alessandri, M.; De Filippo, G.; Materozzi, M.; Bianciardi, S.; Franci, M.B.; Lucani, B.; et al. Preventive Role of Vitamin D Supplementation for Acute Phase Reaction after Bisphosphonate Infusion in Paget’s Disease. J. Clin. Endocrinol. Metab. 2020, 105, dgz138. [Google Scholar] [CrossRef]
- Mathieu, C. Vitamin D and the immune system: Getting it right. IBMS BoneKey 2011, 8, 178–186. [Google Scholar] [CrossRef]
- Channappanavar, R.; Perlman, S. Pathogenic human coronavirus infections: Causes and consequences of cytokine storm and immunopathology. Semin. Immunopathol. 2017, 39, 529–539. [Google Scholar] [CrossRef] [Green Version]
- Campi, I.; Gennari, L.; Merlotti, D.; Mingiano, C.; Frosali, A.; Giovanelli, L.; Torlasco, C.; Pengo, M.F.; Heilbron, F.; Soranna, D.; et al. Vitamin D and COVID-19 severity and related mortality: A prospective study in Italy. BMC Infect. Dis. 2021, 21, 566. [Google Scholar] [CrossRef]
- Quesada-Gomez, J.M.; Lopez-Miranda, J.; Entrenas-Castillo, M.; Casado-Díaz, A.; Nogues, Y.; Solans, X.; Mansur, J.L.; Bouillon, R. Vitamin D Endocrine System and COVID-19: Treatment with Calcifediol. Nutrients 2022, 14, 2716. [Google Scholar] [CrossRef]
- De Niet, S.; Trémège, M.; Coffiner, M.; Rousseau, A.F.; Calmes, D.; Frix, A.N.; Gester, F.; Delvaux, M.; Dive, A.F.; Guglielmi, E.; et al. Positive Effects of Vitamin D Supplementation in Patients Hospitalized for COVID-19: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2022, 14, 3048. [Google Scholar] [CrossRef]
- Wimalawansa, S.J. Rapidly Increasing Serum 25(OH)D Boosts the Immune System, against Infections-Sepsis and COVID-19. Nutrients 2022, 14, 2997. [Google Scholar] [CrossRef]
- Maghbooli, Z.; Sahraian, M.A.; Jamalimoghadamsiahkali, S.; Asadi, A.; Zarei, A.; Zendehdel, A.; Varzandi, T.; Mohammadnabi, S.; Alijani, N.; Karimi, M.; et al. Treatment With 25-Hydroxyvitamin D3 (Calcifediol) Is Associated with a Reduction in the Blood Neutrophil-to-Lymphocyte Ratio Marker of Disease Severity in Hospitalized Patients with COVID-19: A Pilot Multicenter, Randomized, Placebo-Controlled, Double-Blinded Clinical Trial. Endocr. Pract. 2022, 27, 1242–1251. [Google Scholar] [CrossRef]
- Bičíková, M.; Máčová, L.; Hill, M. Vitamin D as a Possible COVID-19 Prevention Strategy. Int. J. Mol. Sci. 2022, 23, 10532. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Alive (n = 206) | Deceased (n = 82) | p-Value |
|---|---|---|---|
| Age (yrs) | 69.4 (±14.7) | 83.1 (±8) | <0.001 |
| Gender (M/F) | 144/62 | 46/36 | 0.02 |
| BMI (kg/m2) | 27.6 (±4) | 29.4 (±15) | 0.1 |
| Number of comorbidity | 1.3 (±1.1) | 2.13 (±1.3) | <0.001 |
| Charlson comorbidity index | 3.1 (±2.1) | 5.9 (±2.1) | <0.001 |
| Laboratory Tests | Alive (n = 206) | Deceased | p-Value |
|---|---|---|---|
| Hb (g/dL) | 13.3 (±2) | 12.5 (±2) | <0.001 |
| Platelets (U/microL) | 240 (±110) | 200 (±90) | 0.004 |
| WBC (103) | 7.6 (±4) | 8.7 (±5) | 0.06 |
| Neutrophils (103/L) | 6.1 (±4) | 7.5 (±5) | 0.01 |
| Lymphocytes (103/L) | 1.1 (±1) | 0.7(±1) | 0.03 |
| INR ratio | 1.2 (±0.6) | 1.3 (±0.5) | 0.2 |
| PTT (s) | 30.1 (±4) | 28.9 (±5) | 0.06 |
| D-dimer (ng/mL) | 2769 (±5929) | 6218 (±10,928) | <0.001 |
| Fibrinogen (mg/dL) media (SD) | 641 (±111) | 612 (±93) | 0.04 |
| D-d/Fibrinogen media (SD) | 0.6 (±0.5) | 0.9 (±0.2) | <0.001 |
| Creatinine (mg/dL) media (SD) | 0.96 (±1) | 1.8 (±1) | <0.001 |
| AST (mU/mL) media (SD) | 46 (±33) | 123 (±539) | 0.04 |
| ALT (mU/mL) media (SD) | 35.9 (±40) | 55.9 (±197) | 0.2 |
| LDH (U/L) media (SD) | 291 (±114) | 364 (±153.4) | <0.001 |
| PCR (mg/dL) media (SD) | 8.1 (±7) | 11.5 (±7) | <0.001 |
| IL-6 (pg/mL) media (SD) | 29.5 (±46) | 68.1 (±76) | <0.001 |
| Troponin (ng/mL) media (SD) | 40.4 (±60) | 283.9 (±762) | <0.001 |
| BNP (pg/mL) media (SD) | 280 (±1339) | 532.3 (±519) | 0.09 |
| Uremia (mg/dL) | 48.1 (±28) | 93.5 (±54) | <0.001 |
| ALP (U/L) media (SD) | 67 (±26) | 161 (±384) | <0.001 |
| 25OHD (ng/mL) media (SD) | 19.6 (±14) | 15.9 (±14) | 0.06 |
| Characteristics | Treated with Calcifediol (n = 56) | Not Treated with Calcifediol (n = 232) | p-Value |
|---|---|---|---|
| Age (years) | 71.8 (±16.4) | 74.9 (±13.4) | 0.1 |
| BMI | 29.2 (±11.5) | 26.7 (±4.1) | 0.008 |
| Number of comorbidities | 1.6 (±1.29) | 1.6 (±1.24) | >0.9 |
| CRP (mg/dL) | 9.8 (±7.6) | 8.6 (±7.2) | 0.3 |
| LDH (mU/mL) | 323.2 (±148.5) | 305 (±119.4) | 0.3 |
| D-dimer (ng/mL) | 3812 (±8174) | 3601 (±7438) | 0.8 |
| INR ratio | 1.32 (±0.6) | 1.23 (±1.23) | 0.6 |
| Lymphocytes (103/L) | 1.01 (±0.9) | 1 (±0.7) | 0.4 |
| 25OHD (ng/mL) | 17.3 (±11.4) | 18.9 (±14.3) | 0.4 |
| SpO2/FiO2 | 314.8 (±126.3) | 333.3 (±121.3) | 0.3 |
| PaO2/FiO2 | 247.6 (±111.7) | 239.6 (±90.9) | 0.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mingiano, C.; Picchioni, T.; Cavati, G.; Pirrotta, F.; Calabrese, M.; Nuti, R.; Gonnelli, S.; Fortini, A.; Frediani, B.; Gennari, L.; et al. Vitamin D Deficiency in COVID-19 Patients and Role of Calcifediol Supplementation. Nutrients 2023, 15, 3392. https://doi.org/10.3390/nu15153392
Mingiano C, Picchioni T, Cavati G, Pirrotta F, Calabrese M, Nuti R, Gonnelli S, Fortini A, Frediani B, Gennari L, et al. Vitamin D Deficiency in COVID-19 Patients and Role of Calcifediol Supplementation. Nutrients. 2023; 15(15):3392. https://doi.org/10.3390/nu15153392
Chicago/Turabian StyleMingiano, Christian, Tommaso Picchioni, Guido Cavati, Filippo Pirrotta, Marco Calabrese, Ranuccio Nuti, Stefano Gonnelli, Alberto Fortini, Bruno Frediani, Luigi Gennari, and et al. 2023. "Vitamin D Deficiency in COVID-19 Patients and Role of Calcifediol Supplementation" Nutrients 15, no. 15: 3392. https://doi.org/10.3390/nu15153392