
Vitamin D Deficiency and Cardiovascular Mortality: Retrospective Analysis “Siena Osteoporosis” Cohort

 ,
, 
Abstract
:1. Introduction
2. Aim of the Study
3. Materials and Methods
3.1. Study Population
3.2. Biochemical Analyses
3.3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sizar, O.; Khare, S.; Goyal, A.; Givler, A. Vitamin D Deficiency; StatPearls: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK532266/ (accessed on 5 May 2023).
- Zittermann, A. Vitamin D in preventive medicine: Are we ignoring the evidence? Br. J. Nutr. 2003, 89, 552–572. [Google Scholar] [CrossRef] [Green Version]
- Bouillon, R.; Carmeliet, G.; Daci, E.; Segaert, S.; Verstuyf, A. Vitamin D metabolism and action. Osteoporos. Int. 1998, 8, S13–S19. [Google Scholar] [CrossRef]
- Mensah, G.A.; Wei, G.S.; Sorlie, P.D.; Fine, L.J.; Rosenberg, Y.; Kaufmann, P.G.; Mussolino, M.E.; Hsu, L.L.; Addou, E.; Engelgau, M.M.; et al. Decline in Cardiovascular Mortality. Circ. Res. 2017, 120, 366–380. [Google Scholar] [CrossRef]
- Tishkoff, D.X.; Nibbelink, K.A.; Holmberg, K.H.; Dandu, L.; Simpson, R.U. Functional Vitamin D Receptor (VDR) in the T-Tubules of Cardiac Myocytes: VDR Knockout Cardiomyocyte Contractility. Endocrinology 2007, 149, 558–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connell, T.D. Immunochemical identification of the 1,25-dihydroxyvitamin d3receptor protein in human heart. Cell Biol. Int. 1996, 20, 621–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosentino, N.; Campodonico, J.; Milazzo, V.; De Metrio, M.; Brambilla, M.; Camera, M.; Marenzi, G. Vitamin D and Cardiovascular Disease: Current Evidence and Future Perspectives. Nutrients 2021, 13, 3603. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. Med. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Bertoldo, F.; Cianferotti, L.; Di Monaco, M.; Falchetti, A.; Fassio, A.; Gatti, D.; Gennari, L.; Giannini, S.; Girasole, G.; Gonnelli, S.; et al. Definition, Assessment, and Management of Vitamin D Inadequacy: Suggestions, Recommendations, and Warnings from the Italian Society for Osteoporosis, Mineral Metabolism and Bone Diseases (SIOMMMS). Nutrients 2022, 14, 4148. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar] [CrossRef]
- Nair, R.; Maseeh, A. Vitamin D: The “sunshine” vitamin. J. Pharmacol. Pharmacother. 2012, 3, 118–126. [Google Scholar]
- McKenna, M.J. Differences in vitamin D status between countries in young adults and the elderly. Am. J. Med. 1992, 93, 69–77. [Google Scholar] [CrossRef]
- Gennari, L.; Merlotti, D.; Figura, N.; Mingiano, C.; Franci, M.B.; Lucani, B.; Picchioni, T.; Alessandri, M.; Campagna, M.S.; Gonnelli, S.; et al. Infection by CagA-Positive Helicobacter pylori Strains and Bone Fragility: A Prospective Cohort Study. J. Bone Miner. Res. 2021, 36, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Montomoli, M.; Gonnelli, S.; Giacchi, M.; Mattei, R.; Cuda, C.; Rossi, S.; Gennari, C. Validation of a food frequency questionnaire for nutritional calcium intake assessment in Italian women. Eur. J. Clin. Nutr. 2002, 56, 21–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: http://www.qualitalaboratorilombardia.it/public/razionale_ormoniemarcatoritumorali.pdf (accessed on 19 June 2023).
- Sutherland, B.N.M.; Zhou, A.; Hyppönen, E. Vitamin D Deficiency Increases Mortality Risk in the UK Biobank. Ann. Intern. Med. 2022, 175, 1552–1559. [Google Scholar] [CrossRef]
- Lin, X.; Chen, X.; Liu, S.; Deng, Y.; Wang, Y.; Lu, Q.; Li, R.; Ou, Y.; Tian, Q.; Liao, Y.; et al. Associations of Serum 25(OH)D with Risk of Recurrent Cardiovascular Events in Individuals with Coronary Heart Disease. J. Clin. Endocrinol. Metab. 2023, 6, dgad339. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.C.; Kong, J.; Wei, M.; Chen, Z.-F.; Liu, S.Q.; Cao, L.-P. 1,25-Dihydroxyvitamin D3 is a negative endocrine regulator of the renin-angiotensin system. J. Clin. Investig. 2002, 110, 229–238. [Google Scholar] [CrossRef]
- Xu, J.; Yang, J.; Chen, J.; Luo, Q.; Zhang, Q.; Zhang, H. Vitamin D alleviates lipopolysaccharide-induced acute lung injury via regulation of the renin-angiotensin system. Mol. Med. Rep. 2017, 16, 7432–7438. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.J.; Pencina, M.J.; Booth, S.L.; Jacques, P.F.; Ingelsson, E.; Lanier, K.; Benjamin, E.J.; D’Agostino, R.B.; Wolf, M.; Vasan, R.S. Vitamin D Deficiency and Risk of Cardiovascular Disease. Circulation 2008, 117, 503–511. [Google Scholar] [CrossRef] [Green Version]
- Andrukhova, O.; Slavic, S.; Zeitz, U.; Riesen, S.C.; Heppelmann, M.S.; Ambrisko, T.D.; Markovic, M.; Kuebler, W.M.; Erben, R.G. Vitamin D Is a Regulator of Endothelial Nitric Oxide Synthase and Arterial Stiffness in Mice. Mol. Endocrinol. 2014, 28, 53–64. [Google Scholar] [CrossRef] [Green Version]
- Yin, K.; You, Y.; Swier, V.; Tang, L.; Radwan, M.M.; Pandya, A.N.; Agrawal, D.K. Vitamin D Protects Against Atherosclerosis via Regulation of Cholesterol Efflux and Macrophage Polarization in Hypercholesterolemic Swine. Arter. Thromb. Vasc. Biol. 2015, 35, 2432–2442. [Google Scholar] [CrossRef] [Green Version]
- Hiemstra, T.F.; Lim, K.; Thadhani, R.; Manson, J.E. Vitamin D and Atherosclerotic Cardiovascular Disease. J. Clin. Endocrinol. Metab. 2019, 104, 4033–4050. [Google Scholar] [CrossRef]
- Zhu, Y.; Mahon, B.D.; Froicu, M.; Cantorna, M.T. Calcium and 1?,25-dihydroxyvitamin?D3 target the TNF-? pathway to suppress experimental inflammatory bowel disease. Eur. J. Immunol. 2005, 35, 217–224. [Google Scholar] [CrossRef]
- Mathieu, C.; Adorini, L. The coming of age of 1,25-dihydroxyvitamin D3 analogs as immunomodulatory agents. Trends Mol. Med. 2002, 8, 174–179. [Google Scholar] [CrossRef]
- Roffe-Vazquez, D.N.; Huerta-Delgado, A.S.; Castillo, E.C.; Villarreal-Calderón, J.R.; Gonzalez-Gil, A.M.; Enriquez, C.; Garcia-Rivas, G.; Elizondo-Montemayor, L. Correlation of Vitamin D with Inflammatory Cytokines, Atherosclerotic Parameters, and Lifestyle Factors in the Setting of Heart Failure: A 12-Month Follow-Up Study. Int. J. Mol. Sci. 2019, 20, 5811. [Google Scholar] [CrossRef] [Green Version]
- Wöbke, T.K.; Sorg, B.L.; Steinhilber, D. Vitamin D in inflammatory diseases. Front. Physiol. 2014, 5, 244. [Google Scholar] [CrossRef] [Green Version]
- Koyama, T.; Shibakura, M.; Ohsawa, M.; Kamiyama, R.; Hirosawa, S. Anticoagulant effects of 1alpha,25-dihydroxyvitamin D3 on human myelogenous leukemia cells and monocytes. Blood 1998, 92, 160–167. [Google Scholar] [CrossRef]
- Coppini, R.; Ferrantini, C.; Mugelli, A.; Poggesi, C.; Cerbai, E. Altered Ca2+ and Na+ Homeostasis in Human Hypertrophic Cardiomyopathy: Implications for Arrhythmogenesis. Front. Physiol. 2018, 9, 1391. [Google Scholar] [CrossRef]
- Soto, M.E.; Pérez-Torres, I.; Rubio-Ruiz, M.E.; Cano-Martínez, A.; Manzano-Pech, L.; Guarner-Lans, V. Frailty and the Interactions between Skeletal Muscle, Bone, and Adipose Tissue-Impact on Cardiovascular Disease and Possible Therapeutic Measures. Int. J. Mol. Sci. 2023, 24, 4534. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, H.; Hendrickse, P.W.; Pereira, M.G.; Bowen, T.S. Skeletal muscle atrophy, regeneration, and dysfunction in heart failure: Impact of exercise training. J. Sport Health Sci. 2023. [Google Scholar] [CrossRef] [PubMed]
- Latic, N.; Erben, R.G. Vitamin D and Cardiovascular Disease, with Emphasis on Hypertension, Atherosclerosis, and Heart Failure. Int. J. Mol. Sci. 2020, 21, 6483. [Google Scholar] [CrossRef] [PubMed]
- Carbone, L.; Bůžková, P.; Fink, H.A.; Lee, J.S.; Chen, Z.; Ahmed, A.; Parashar, S.; Robbins, J.R. Hip fractures and heart failure: Findings from the Cardiovascular Health Study. Eur. Heart J. 2009, 31, 77–84. [Google Scholar] [CrossRef]
- Fohtung, R.B.; Brown, D.L.; Koh, W.J.H.; Bartz, T.M.; Carbone, L.D.; Civitelli, R.; Stein, P.K.; Chaves, P.H.M.; Kestenbaum, B.R.; Kizer, J.R. Bone Mineral Density and Risk of Heart Failure in Older Adults: The Cardiovascular Health Study. J. Am. Heart Assoc. 2017, 6, e004344. [Google Scholar] [CrossRef] [Green Version]
- Jankowska, E.A.; Jakubaszko, J.; Cwynar, A.; Majda, J.; Ponikowska, B.; Kustrzycka-Kratochwil, D.; Reczuch, K.; Borodulin-Nadzieja, L.; Banasiak, W.; Poole-Wilson, P.A.; et al. Bone mineral status and bone loss over time in men with chronic systolic heart failure and their clinical and hormonal determinants. Eur. J. Heart Fail. 2009, 11, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Loncar, G.; Cvetinovic, N.; Lainscak, M.; Isaković, A.; Von Haehling, S. Bone in heart failure. J. Cachex-Sarcopenia Muscle 2020, 11, 381–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maas, A.; Appelman, Y. Gender differences in coronary heart disease. Neth. Heart J. 2010, 18, 598–603. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Control Group | Heart Failure Group | p Value |
|---|---|---|---|
| Females | 797 (83.9%) | 39 (76.5%) | |
| Males | 153 (16.1%) | 12 (23.5%) | |
| Age at baseline (yrs) | 63.14 ± 6.76 | 62.95 ± 7.12 | |
| BMI (Kg/m2) | 25.72 ± 4.2 | 25.9 ± 3.18 | n.s. |
| Obesity (BMI > 30 Kg/m2) | 123 (12.9%) | 3 (5.9%) | |
| Smoke (%) | 127 (13.4%) | 6 (11.8%) | |
| Hypertension (%) | 166 (17.5%) | 12 (23.5%) | |
| Ipercholesterolemia (%) | 291 (30.6%) | 20 (39.2%) | |
| Diabetes (%) | 43 (4.5%) | 6 (11.8%) | |
| Chronic Kidney Disease (%) | 12 (1.3%) | 1 (2%) | |
| Calcium Intake (mg/day) | 837.07 ± 319.43 | 836.40 ± 345.68 | n.s. |
| Calcium (mg/dL) | 9.27 ± 0.58 | 9.34 ± 0.66 | n.s. |
| Phosphorus (mg/dL) | 3.42 ± 0.55 | 3.41 ± 0.59 | n.s. |
| Alkaline Phosphatase (UI/L) | 180.57 ± 85.07 | 181.94 ± 64.84 | n.s. |
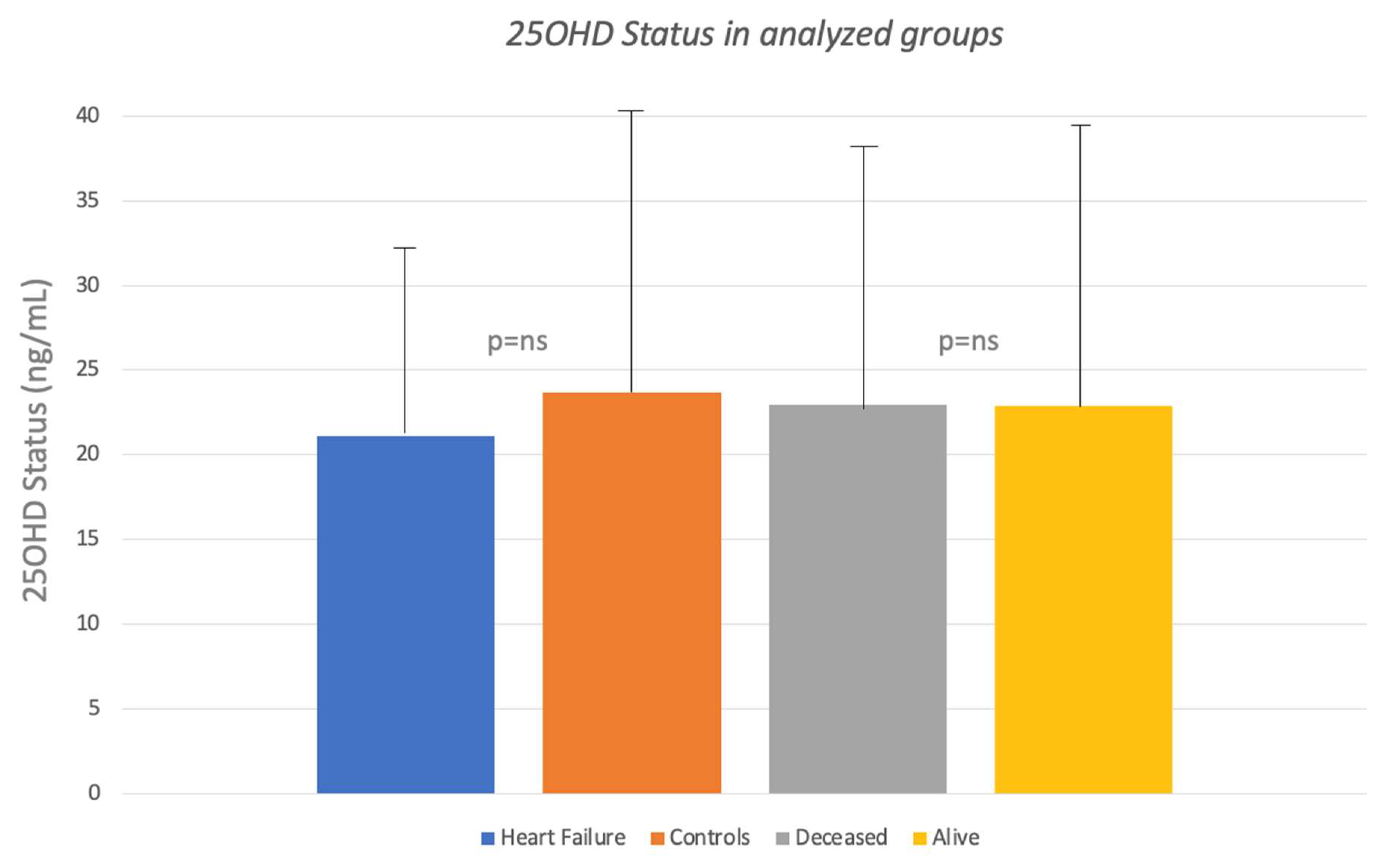
| 25OH Vitamin D (ng/mL) | 23.65 ±16.5 | 21.08 ± 12.4 | n.s. |
| n | Alive Subjects | Deceased Subjects | p Value |
|---|---|---|---|
| Females (%) | 812 (87.2%) | 144 (77%) | |
| Males (%) | 119 (12.3%) | 43 (23%) | |
| Age at baseline (yrs) | 62.21 ± 6.31 | 66.4 ± 6.41 | <0.05 |
| BMI (Kg/m2) | 25.61 ± 4.17 | 25.81 ± 4.35 | n.s |
| Obesity (BMI > 30 Kg/m2) | 101 (10.8%) | 25 (13.4%) | |
| Smoke (%) | 113 (12.1%) | 31 (16.6%) | |
| Hypertension (%) | 151 (15.2%) | 32 (17.1%) | |
| Ipercholesterolemia (%) | 270 (29%) | 56 (29.9%) | |
| Diabetes (%) | 40 (4.3%) | 10 (5.3%) | |
| Chronic Kidney Disease (%) | 8 (0.9%) | 5 (2.7%) | |
| Calcium Intake (mg/day) | 842.52 ± 329.71 | 806.72 ± 276.07 | n.s |
| Calcium (mg/dL) | 9.29 ± 0.59 | 9.25 ± 0.56 | n.s |
| Phosphorus (mg/dL) | 3.44 ± 0.55 | 3.35 ± 0.54 | |
| Alkaline Phosphatase (UI/L) | 178.63 ± 86.29 | 187.23 ± 57.76 | n.s |
| Creatinine (mg/dL) | 0.91 ± 0.33 | 0.96 ± 0.21 | <0.05 |
| 25OH Vitamin D (ng/mL) | 22.89 ± 16.7 | 22.96 ± 14.8 | n.s |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pirrotta, F.; Cavati, G.; Mingiano, C.; Merlotti, D.; Nuti, R.; Gennari, L.; Palazzuoli, A. Vitamin D Deficiency and Cardiovascular Mortality: Retrospective Analysis “Siena Osteoporosis” Cohort. Nutrients 2023, 15, 3303. https://doi.org/10.3390/nu15153303
Pirrotta F, Cavati G, Mingiano C, Merlotti D, Nuti R, Gennari L, Palazzuoli A. Vitamin D Deficiency and Cardiovascular Mortality: Retrospective Analysis “Siena Osteoporosis” Cohort. Nutrients. 2023; 15(15):3303. https://doi.org/10.3390/nu15153303
Chicago/Turabian StylePirrotta, Filippo, Guido Cavati, Christian Mingiano, Daniela Merlotti, Ranuccio Nuti, Luigi Gennari, and Alberto Palazzuoli. 2023. "Vitamin D Deficiency and Cardiovascular Mortality: Retrospective Analysis “Siena Osteoporosis” Cohort" Nutrients 15, no. 15: 3303. https://doi.org/10.3390/nu15153303