
Dietary Patterns and Alzheimer’s Disease: An Updated Review Linking Nutrition to Neuroscience



1
Department of Plant Biotechnology, Higher Institute of Biotechnology of Beja, University of Jendouba, Beja 382, Tunisia
2
Department of Nutrition and Integrative Physiology, Florida State University, Tallahassee, FL 32306, USA
3
Center for Translational Behavioral Science, Florida State University College of Medicine, Tallahassee, FL 32304, USA
4
Center for Advancing Exercise and Nutrition Research on Aging, Florida State University, Tallahassee, FL 32306, USA
*
Authors to whom correspondence should be addressed.
Nutrients 2023, 15(14), 3204; https://doi.org/10.3390/nu15143204
Submission received: 22 June 2023
/
Revised: 15 July 2023
/
Accepted: 17 July 2023
/
Published: 19 July 2023
(This article belongs to the Section Nutrition and Public Health)
Abstract
:Alzheimer’s disease (AD) is a growing concern for the aging population worldwide. With no current cure or reliable treatments available for AD, prevention is an important and growing area of research. A range of lifestyle and dietary patterns have been studied to identify the most effective preventive lifestyle changes against AD and related dementia (ADRD) pathology. Of these, the most studied dietary patterns are the Mediterranean, DASH, MIND, ketogenic, and modified Mediterranean-ketogenic diets. However, there are discrepancies in the reported benefits among studies examining these dietary patterns. We herein compile a narrative/literature review of existing clinical evidence on the association of these patterns with ADRD symptomology and contemplate their preventive/ameliorative effects on ADRD neuropathology in various clinical milieus. By and large, plant-based dietary patterns have been found to be relatively consistently and positively correlated with preventing and reducing the odds of ADRD. These impacts stem not only from the direct impact of specific dietary components within these patterns on the brain but also from indirect effects through decreasing the deleterious effects of ADRD risk factors, such as diabetes, obesity, and cardiovascular diseases. Importantly, other psychosocial factors influence dietary intake, such as the social connection, which may directly influence diet and lifestyle, thereby also impacting ADRD risk. To this end, prospective research on ADRD should include a holistic approach, including psychosocial considerations.
1. Introduction
Dementia is one of the most prevalent illnesses among older adults, with over 55 million people worldwide suffering from dementia. According to the World Health Organization (WHO), dementia is caused by diseases and injuries that affect the brain [1]. These diseases gradually destroy nerve cells and impair brain function over time, resulting in the deterioration of cognitive functioning beyond the normal effects of biological aging. This deterioration affects memory, thinking, processing speed, and the ability to engage in activities of daily living. Consequently, dementia leads to disability and an increasing level of dependency. Moreover, dementia imposes a significant physical, psychological, social, and economic burden on caregivers, families, and society. By 2030, the global population of older adults (aged ≥ 65 years old) is projected to reach 1 billion, accounting for 12% of the total population [2]. With an aging population, the rates of neurodegenerative diseases such as Alzheimer’s disease (AD) and related dementias (ADRD) will continue to increase.
Various cross-sectional, observational, and interventional studies, as discussed in the succeeding sections and tables, have independently linked specific dietary patterns, such as the Mediterranean diet, MIND diet, and DASH diet, to a reduced or delayed incidence or symptoms of ADRD. Therefore, our aim herein is to compile current clinical evidence concerning the associations among these dietary patterns and ADRD symptomology. Additionally, we will discuss the preventive and/or ameliorative effects of these dietary patterns on the incidence and neuropathology of AD in various clinical settings and cohorts.
2. Alzheimer’s Disease
According to the Centers for Disease Control and Prevention, AD is the most common form of dementia [3]. It is an incurable and progressive degenerative disease that initially manifests as mild memory loss. AD is characterized by the development of senile amyloid plaques and neurofibrillary tangles, which are associated with the gradual loss of neuronal synapses and pyramidal neurons, eventually leading to progressive neurodegeneration. The neurological regions, such as the hippocampus and neocortex, are particularly affected early in the disease [4].
The first clinical symptoms of AD typically appear around 20 years after the initial structural changes in the brain [5,6]. Additionally, this disease can result in reduced glucose metabolism, ultimately leading to brain atrophy [6,7,8]. As the disease progresses, it impairs the patient’s ability to engage in conversations and respond to the environment, primarily affecting the parts of the brain responsible for thought, memory, and language [7,8]. Several factors influence AD, including non-modifiable factors, such as genetics, sex, and age, and modifiable factors, like the level of education, physical activity, sleep, diet, smoking, and alcohol consumption, in addition to potentially modifiable factors, including metabolic syndrome during middle age [7,8].
In the United States, it is projected that by 2030, 8.2 million people will be diagnosed with AD, and this number is expected to increase to 14 million by 2060 [9,10]. Currently, AD is the sixth leading cause of death among adults aged 65 or older, and the number of deaths resulting from AD continues to rise [11]. Despite the significant economic burden and extensive research efforts to find a cure, AD remains incurable. There are currently no approved drugs available that can cure or effectively reverse AD. Consequently, there is great interest in preventive actions and interventions [12]. These interventions aim to promote healthy brain aging. Given that there are currently no treatment options for ADRD pathology, the manifestation of the disparity between cognition and the magnitude of pathology indicates the significance of exploring modifiable risk factors for improving cognitive health without specifically treating the ubiquitous aging-associated neuropathology [13,14,15]. One-third of AD cases involve certain modifiable risk factors and are preventable through dietary and lifestyle modification [16]. Scientific research indicates that regular physical activity and a healthy diet may have a beneficial effect on human cognitive function, thereby reducing the risk of developing AD. In this view, these factors may be considered preventive measures against the development or progression of AD [17,18]. Understanding the pathways underlying ADRD is crucial to improving preventative and therapeutic approaches, which are public health priorities [19]. Emerging epidemiological and clinical evidence supports the relationship between diet and ADRD development [20].
Emerging evidence suggests that prudent dietary patterns are associated with slower cognitive decline and reduced ADRD risk [20,21], although the mechanisms underlying these effects remain unclear. One possible mechanism is that specific dietary constituents may influence neural resources and enhance cognitive health and resilience [22,23]. For instance, healthier dietary patterns have been linked to the homeostatic formation of hippocampal neurons, which are found to be impaired in the early stages of ADRD [24]. Thus, by strengthening/improving cognitive resilience over time, healthier dietary elements may lead to improved late-life cognitive trajectories [25,26,27]. Indeed, understanding and exploiting the biological elements of ADRD risk factors (such as dietary factors) may inform the development of novel interventions for disease prevention.
3. Methodology
This narrative review encompasses clinical trials (longitudinal, cross-sectional, prospective cohorts, interventions) and meta-analyses on middle-aged and older adult populations diagnosed with or at higher risks of developing ADRD. A comprehensive literature search was conducted using various databases, including Pubmed, Medline, ScienceDirect, and Google Scholar (last accessed on 20 May 2023). The search utilized specific keywords, such as diet, dietary pattern, Mediterranean, DASH, MIND, ketogenic, modified ketogenic, vegetarian, vegan, Alzheimer’s, Alzheimer’s disease, cognitive impairment, and dementia. The search was further refined to include only English-language studies and human studies that incorporated a meta-analysis of clinical trials and cross-sectional studies. The primary aim of this review is to evaluate current evidence on dietary patterns and their effects on ADRD risk and progression.
4. Impact of Specific Dietary Patterns on ADRD Progression
The Western diet is known for its high content of refined grains, sugar, unhealthy fats, and salt while having an extremely low consumption of fruits and vegetables [28,29]. These components, both individually and collectively, have been linked to the obesity epidemic, cardiovascular diseases, cancer, osteoporosis, autoimmune diseases, type 2 diabetes, and other illnesses [30,31,32]. Another characteristic of the Western diet is the high consumption of ultra-processed foods and beverages. Based on the NOVA classification system, these products are characterized by high levels of hydrogenated and/or esterified oils, added sugars, carbohydrates, saturated fats, and various additives that enhance their palatability [33]. As a result, these nutritionally poor food products often lack fiber and can disrupt the gut microbiome, leading to immune alterations [34,35]. These immune system disturbances can eventually contribute to chronic inflammation [28,29]. Moreover, the excessive consumption of foods that have a high glycemic index, are rich in saturated fats, and have high sodium content may contribute to conditions such as hypercholesterolemia and insulin resistance, which impair vasoreactivity, hemodynamic function, and endothelial integrity, thereby impeding cerebral perfusion [36]. Vascular dysfunction has long been recognized as a contributing factor to ADRD [37].
Several studies have established a causal relationship between the Western diet and pathological brain aging [38,39]. Furthermore, the Western diet has been associated with poorer cognitive function, particularly at an older age [40,41]. Therefore, for overall health and well-being, the American Heart Association and the U.S. government’s Dietary Guidelines for Americans recommend a diet centered around plant-based foods, including fruits, vegetables, whole grains, nuts, and seeds, while also incorporating fish, low-fat dairy products, and lean meat. It is advised to limit or avoid red meat, sodium, saturated fats, sugar, and highly processed foods. This dietary pattern is associated with good cognitive health [10]. The diet has been suggested to play an important role, both directly and indirectly, in cognitive health and the development of dementia [42]. Nutrients found in the diet, such as vitamins, antioxidants, and fiber, can directly impact cognitive health through their antioxidative, anti-inflammatory, and endothelial and mitochondrial functions. These nutrients also have indirect effects, as they act on the cardiovascular-related effects of diabetes, dyslipidemia, hypertension, obesity, and/or homocysteine levels [10]. As these nutrients are consumed as part of a dietary pattern, it is crucial to explore the holistic effects of these dietary patterns on health [43]. A diet comprises all the individual foods and beverages consumed on a daily basis, but dietary patterns are the outcome of an individual’s dietary history, sociocultural identity, and demographic characteristics [10]. However, only a limited number of randomized controlled trials conducted to date have assessed the effects of specific foods or dietary patterns on cognitive health, particularly in relation to ADRD [44].
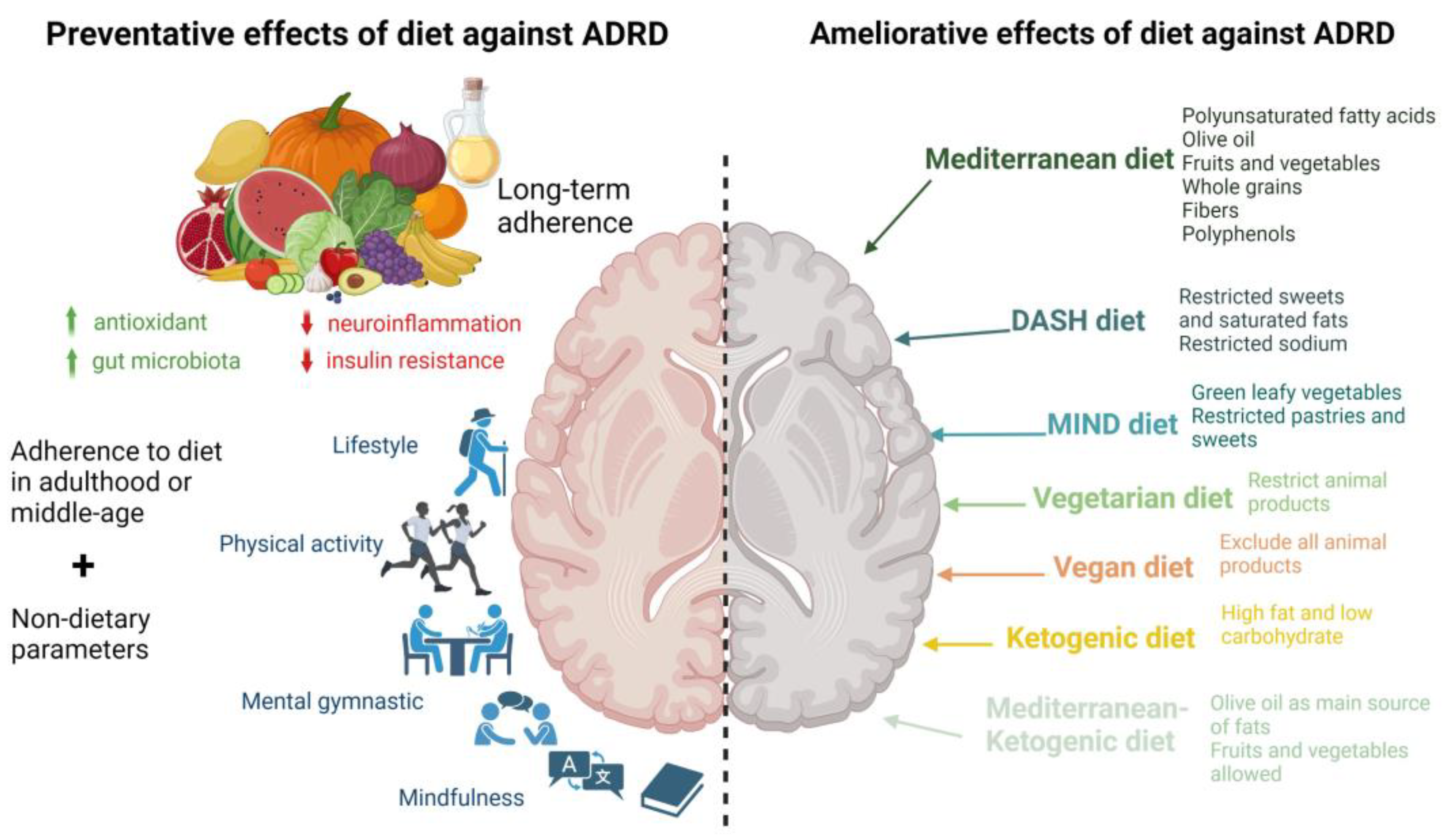
Hereafter, the different dietary patterns studied and their impacts on ADRD progression are presented (Figure 1).
4.1. Impact of Mediterranean Diet on ADRD Progression
The Mediterranean diet (MedD), created by an American couple in the 1960s, is inspired by the eating habits of people in Greece, Southern Italy, and Spain in the 1940s and 1950s [45]. These habits involve a high consumption of olive oil, unrefined cereals, fruits, and vegetables; a moderate to high consumption of fish; a moderate consumption of dairy products (mostly cheese and yogurt); moderate wine consumption; and a low consumption of red meat products [12]. The MedD consists of nutrient-dense foods that have been recognized as beneficial for overall health and healthy brain aging [9]. It has been associated with a lower risk of conversion from mild cognitive impairment to dementia [46,47,48,49], a reduction in dementia incidence [46,50,51,52,53,54,55,56], the maintenance of brain health [20,57], a lower risk of cognitive decline [41,58,59,60,61,62,63], and better cognition [64,65]. However, some inconsistencies are observed among studies regarding the benefits of the MedD on cognition and cognitive aging, particularly with regard to ADRD. Some studies did not find significant associations between the MedD and a decrease in ADRD incidence and/or conversion from mild cognitive impairment to dementia, which may be attributed to recruiting participants from outside the Mediterranean area [21,56,66,67,68,69,70,71,72,73,74]. There is evidence that the benefits of the MedD may be more prominent among individuals who have adhered to the MedD throughout their lives and reside in the Mediterranean region compared to those who adopt this dietary pattern later in life [75]. Another factor contributing to the contradictory results is the variation in the qualitative and quantitative food components prescribed in different studies. For example, some studies grouped all polyunsaturated fatty acids together, while others focused solely on olive oil. Additionally, the quantities of different components of the diet vary among studies. A randomized study, for instance, examined the impact of the MedD supplemented with olive oil or nuts and identified a significant improvement in global cognition and/or specific cognitive domains among a Spanish population with cardiovascular risk factors over a period of 6.5 years [76]. Furthermore, there is considerable variation in the scoring systems used across different studies, which can lead to disparities in estimating nutrient intake and compliance with the MedD [77]. It is important to consider potential sources of discrepancies in research findings, which may stem from differences in the studied populations, including factors such as gender (males or females only), the presence of obesity or cardiovascular diseases, and the duration of the studies. The timing of dietary adherence, whether it occurs during midlife or late life, also needs careful consideration. Table 1 provides a compilation of observational, longitudinal, and intervention studies conducted in the past 10 years examining the MedD and its association with ADRD risk factors.
In addition to cognitive outcomes associated with ADRD risk, recent research has examined the effect of the MedD on AD biomarkers, specifically β-amyloid and phosphorylated tau tangles. In a systematic review and meta-analysis conducted by Hill et al. [78], it was concluded that adherence to a Mediterranean-style dietary pattern was associated with a reduction in AD biomarkers (β-amyloid and tau tangle) and subsequent pathology. Specifically, in the latest published study by Agarwal et al. [79], which involved autopsied older adults, higher scores of adherence to the MedD were significantly associated with lower global AD pathology (p = 0.039). Even after adjusting the models for other covariates, such as physical activity, smoking, and vascular disease burden, the association remained significant (p = 0.027). When excluding the dietary assessments from the last year of life of the participants to account for events that might have altered their diet, greater overall adherence to the MedD for almost a decade remained significantly associated with reduced global AD pathology and β-amyloid load.
Furthermore, the MedD has shown potential in reducing the incidence of ADRD through its beneficial effects on blood pressure [80], mitochondrial structure and function [81], the preservation of white matter microstructure [82,83], the induction of cerebral blood flow [81], cortical thickness [84], and the accumulation of white matter hyperintensities [85]. The MedD can also act through a variety of mechanisms, including anti-inflammatory, antioxidant, and lipid-lowering actions [86,87], as well as its favorable impact on cardiovascular risk factors [87,88,89]. MedD has also been associated with higher total brain volume and cortical thickness and lower white matter hyperintensities [84,90,91,92,93]. All these factors can contribute to reducing ADRD (Figure 2).
It should be noted that adherence to the MedD may come with higher financial costs compared to other diets, as reported in studies conducted in the UK and Spain that highlighted this aspect [94,95]. Therefore, individuals with higher incomes have a higher likelihood of adhering to the MedD [96]. Future studies focusing on the MedD should consider the participants’ socioeconomic status as a covariate for dietary analysis [75], as well as other lifestyle factors, such as social contact and physical activity [97,98].
Figure 2.
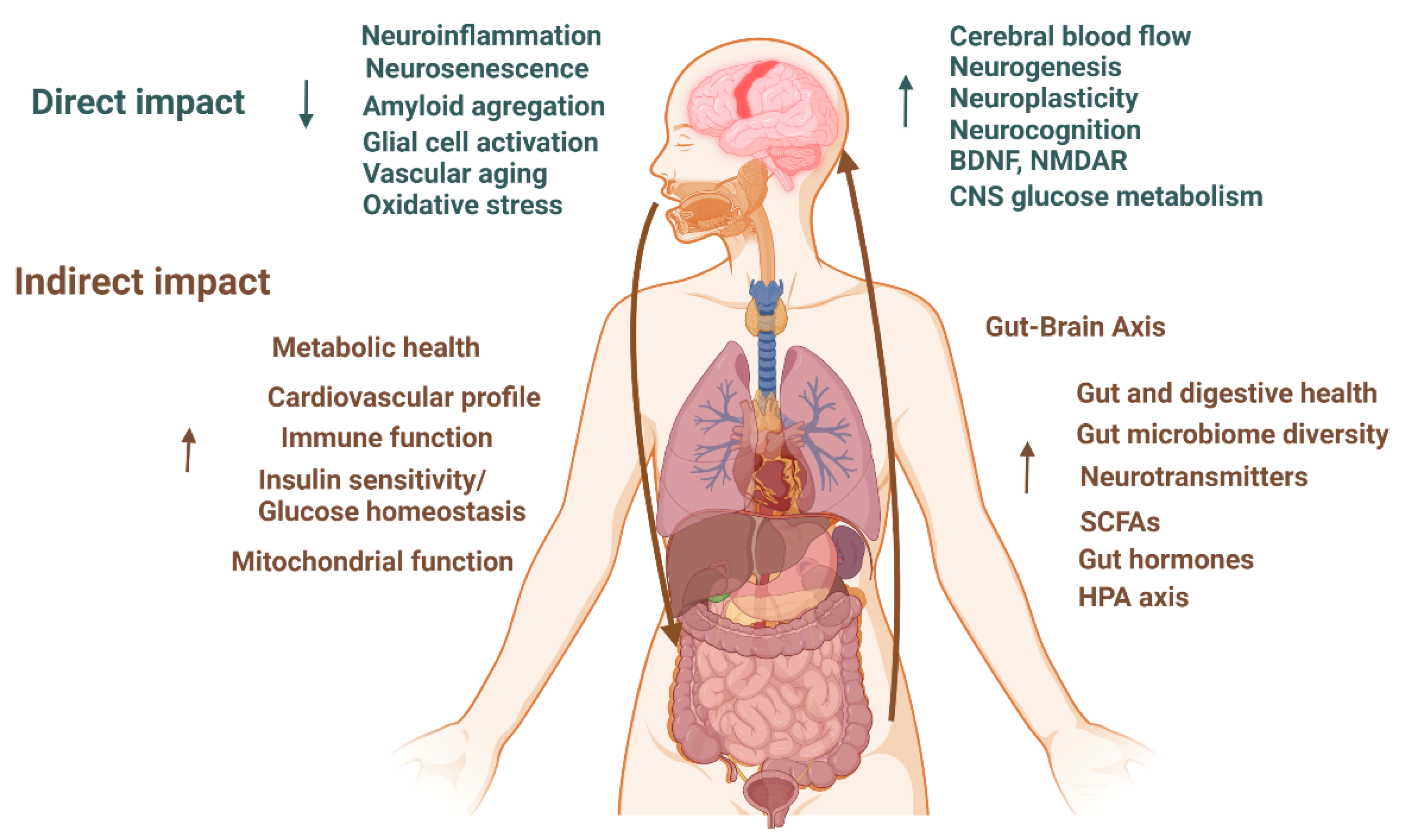
Hypothesized direct and indirect impacts of dietary patterns on ADRD [12,46,47,48,49,50,51,52,53,54,55,56,85,86,93,99,100,101,102,103]. BDNF: Brain-Derived Neurotrophic Factor; NMDR: N-methyl-D-aspartate receptor; CNS: central neural system; SCFAs: short-chain fatty acids; HPA: hypothalamic–pituitary–adrenal; ↑ higher; ↓ lower.
Figure 2.
Hypothesized direct and indirect impacts of dietary patterns on ADRD [12,46,47,48,49,50,51,52,53,54,55,56,85,86,93,99,100,101,102,103]. BDNF: Brain-Derived Neurotrophic Factor; NMDR: N-methyl-D-aspartate receptor; CNS: central neural system; SCFAs: short-chain fatty acids; HPA: hypothalamic–pituitary–adrenal; ↑ higher; ↓ lower.


{kind=link}
{kind=link}
Table 1.
A summary of clinical studies examining Mediterranean diet impact on ADRD.
| Study Design | Country | Population | Follow-Up | Exposure | Outcome | Results | Covariates | Reference |
|---|---|---|---|---|---|---|---|---|
| Longitudinal | US | Older adults in CCMS Age: ≥65 years n = 3580 | 10.6 years | 142-item FFQ, MedD score, DASH score, global cognition (3 MS) | Associations between DASH and MedD diets and age-related cognitive change. | Higher quintile of MedD score associated with better average cognition during follow-up but not with cognitive function rate of change. | Age, gender, education, BMI, frequency of moderate physical activity, multivitamin and mineral supplement use, history of drinking and smoking, and history of diabetes, heart attack, or stroke. | [104] |
| Longitudinal | US | Participants in United States Reasons for Geographic and Racial Differences in Stroke study n = 17,478 (7548 M 9930 F) Age: 64.4 years | 4 years | 98-item block FFQ, MedD score, cognitive impairment, six-item screener (SIS) | Higher adherence to MedD and likelihood of incident cognitive impairment (ICI) and the interaction of race and vascular risk factors. | High compared with low adherence to MedD significantly associated with lower risk of ICI. Higher tertile of MedD score significantly associated with lower risk of ICI. | Age, gender, race, region, educational level, income, number of packs smoked per year, weekly exercise, diabetes mellitus, hypercholesterolemia, atrial fibrillation, history of heart disease, BMI, waist circumference, systolic and diastolic blood pressure, ACE inhibitors/angiotensin receptor blockers, β-blockers, other antihypertensive medication, depressive symptoms, and self-reported health status. | [105] |
| Longitudinal | Sweden | Senior participants in Prospective Investigation of the Vasculature in Uppsala Seniors Age: 70.1 ± 0.01 years at enrollment n = 194 (101 M 93 F) cognitive assessment at 75 years | 5 years | 7-day food diary, adapted MedD score, dietary components, global cognition (7 MS), brain volume (3D T1-weighted MRI scan) | Association between dietary habits, cognitive functioning, and brain volumes in older individuals. | Continuous MedD score not significantly associated with global cognitive function after adjustment. Continuous MedD score not associated with gray or white matter volume or total brain volume. | Gender, energy intake, education, self-reported physical activity, low-density cholesterol, BMI, systolic blood pressure, and HOMA-IR. | [99] |
| Longitudinal | US | Subset of participants from the Women’s Health study n = 6174 (0 M 6174 F) Age: 72 years | 4 years | 131-item SFFQ, adapted MedD score, dietary components, global cognition (TICS, EBMT, CF) and verbal memory (EBMT, delayed recall of TICS 10-word list) | Association of adherence to MedD with cognitive function and decline. | MedD score quintile not significantly associated with better average global cognition or verbal memory nor with change in global cognition and verbal memory. | Treatment arm, age at initial cognitive testing, Caucasian race, high education, high income, energy intake, physical activity, BMI, smoking, diabetes, hypertension, hypercholesterolemia, hormone use, and depression. | [67] |
| Longitudinal | US | Women from the Nurses’ Health Study n = 16,058 (0 M 16,058 F) Age: 74.3 years | 6 years | 116-item SFFQ, adapted MedD score, dietary components, global cognition (TICS and composite score of TICS, EBMT, CF, DST backward), and verbal memory (immediate and delayed recalls of the EBMT and TICS) | Associations between long-term adherence to MedD and subsequent cognitive function and decline. | Long-term higher quintile MedD score at older age significantly associated with better performance on TICS, global cognition, and verbal memory. Quintile of average MedD score not significantly associated with change in TICS score, global cognition, or verbal memory. | Age, education, long-term physical activity and total energy intake, BMI, smoking, multivitamin use, and history of depression, diabetes, hypertension, hypercholesterolemia, or myocardial infarction. | [54] |
| Longitudinal | US | Subset of participants from The Supplementation with Vitamins and Mineral Antioxidants study n = 3083 (1655 M 1428 F) Age: 52.0 ± 4.6 years at enrollment | 13 years | 24 h food recalls (12: each year), MedD score, Mediterranean-Style Dietary Pattern Score (MSDPS), cognitive performance (episodic memory, lexical-semantic memory, short-term memory, working memory, mental flexibility | Association between midlife MedD adherence and cognitive performance assessed 13 years later. | Higher tertile of MedD score associated only with working memory span. Higher tertile of MSDPS significantly associated with semantic fluency on the phonemic fluency task, but not with global cognition, episodic memory, short-term memory, working memory, or mental flexibility. | Age, gender, education, follow-up time, supplementation group during the trial phase, number of 24 h dietary records, total energy intake, BMI, occupational status, smoking status, physical activity, memory difficulties at baseline, depressive symptoms concomitant with the cognitive function assessment, and history of diabetes, hypertension, or CVD. | [55] |
| Longitudinal | Italy | Subset of participants in TRELONG Study n = 309 (120 M 189 F) Age: 79.1 ± 9.65 y | 7 years | FFQ, MedD yes/no (based on cereal, fish, vegetable and fruit intake), global cognition (MMSE) | Association between risk factors (body mass index (BMI), depression, chronic diseases, smoking, and lifestyles) and cognitive decline in older adults. | Adherence compared to non-adherence to MedD not significantly associated with less cognitive decline | NS | [106] |
| Longitudinal | US | Older participants from the Memory and Aging Project cognitively normal at enrollment n = 826 (26%M) Age: 81.5 ± 7.1 years | 4.1 years | 144-item FFQ, battery of cognitive tests: episodic memory, semantic memory, working memory, perceptual speed, and visuospatial ability. | Association between DASH and MedD diets and slower cognitive decline. | A 1-unit higher MedD score associated with a 0.002 slower rate of global cognitive decline standardized units, after adjustment for covariates. | Age, gender, education, participation in cognitive activities, total energy intake (kcal), time, and the interaction between time and each covariate, physical activity, presence of APOE ε4 alleles, depression, hypertension, diabetes, and stroke. | [58] |
| Longitudinal | Greece | Older adults in European Prospective Investigation into Cancer and Nutrition (EPIC) n = 401 (144 M 257 F) Age at enrollment: 74 years | 6.6 years | 150-item SFFQ, MedD score, dietary components, global cognition (MMSE) | Association between adherence to MedD in a Mediterranean country and cognitive decline in older adults. | Higher tertile of MedD scores significantly associated with less mild cognitive decline and substantial cognitive decline. | Age, gender, years of education, BMI, physical activity, smoking status, diabetes, hypertension, cohabiting, total energy intake. | [49] |
| Longitudinal | China | Older adults in China Health and Nutrition Survey n = 1650 (820 M 831 F) Age: 63.5 years | 5.3 years | 3-day 24 h recall, adapted MedD score, dietary components, decline in global cognition, composite z-scores, and verbal memory (modified TICS) | Association between cognitive changes among Chinese older adults and either an adapted Mediterranean diet score or factor-analysis-derived dietary patterns. | Higher MedD score significantly associated with slower rate of decline in global cognitive, composite z-, and verbal memory scores only in participants ≥ 65 years. Higher tertile of MedD score significantly associated with less decline in global cognitive scores and verbal memory scores only in participants ≥ 65 years | Age, gender, education, region, urbanization index, annual household income per capita, total energy intake, physical activity, current smoking, time since baseline, BMI, hypertension, and time interactions with each covariate. | [61] |
| Longitudinal | Sweden | Older adults in Uppsala longitudinal study n = 1038 (1038 M 0 F) Age at enrollment: 70 years | 12 years | 7-day food diary, adapted MedD score, AD (based on NINCDS-ADRDA and DSM-IV criteria), dementia, and cognitive impairment (MMSE) | Associations between development of cognitive dysfunctions and different diets. (Healthy Diet Indicator), a Mediterranean-like diet, and a low-carbohydrate, high-protein diet. | Continuous MedD score not associated with a lower risk of AD, dementia, or cognitive impairment. Higher tertile of MedD score not associated with AD or cognitive impairment. Highest tertile of MedD score in participants with energy intake according to the Goldberg cut-off significantly associated with a lower risk of cognitive impairment. | Energy, education, presence of APOE ε4 allele, living alone, smoking, and physical activity. | [72] |
| Longitudinal | US | Participants of the Rush Memory and Aging Project (MAP) n = 923 (±24% M) Age: 58–98 years | 4.5 years | 144-item SFFQ, A-MedD, A-DASH, and MIND scores, AD (based on NINCDS-ADRDA criteria) | Association of MIND, a hybrid Mediterranean and DASH diet, with incident Alzheimer’s disease. | Highest tertile of A-MedD adherence significantly associated with lower risk of AD diagnosis. | Age, gender, education, presence of APOE ε4 allele, participation in cognitively stimulating activities, physical activity, total energy intake, and cardiovascular conditions. | [100] |
| Longitudinal | US | Older adults in Health, Aging, and Body Composition (Health ABC) n = 2326 (1109 M 1217 F) Age: 70–79 years | 7.9 years | 108-item block FFQ via interviews, A-MedD score (race-specific), global cognition (3 MS score) | Association of decreased risk of cognitive decline with MedD within a diverse population. | Among African American, but not among whites, A-MedD score significantly associated with less cognitive decline. | Age, gender, education, BMI, current smoking, physical activity, depression, diabetes, total energy intake, and socioeconomic status. | [60] |
| Longitudinal | Spain | Participants in Spanish SUN project n = 823 (597 M 223 F) Age: at enrollment, 61.9 ± 6.0 years | 6–8 years | 136-item SFFQ, MedD score, dietary components, cognitive function (TICS) | Association between adherence to MedD and cognitive function in a Spanish population. | Lower tertile of MedD score significantly associated with faster cognitive decline. | Age, gender, presence of APOE ε4 allele, follow-up time, total energy intake, BMI, smoking status, physical activity, diabetes, hypertension, hypercholesterolemia, history of CVD, and years of university education. | [59] |
| Longitudinal | US | Postmenopausal women enrolled in the Women’s Health Initiative Memory Study (WHIMS) n = 6425 (0%M) Age: 65–79 years | 9.11 years | FFQ, A-MedD score, DASH score, MCI (MMSE and battery of neuropsychological tests) | Association of dietary patterns with cognitive decline in older women and association of dietary patterns with risk of cognitive decline in women with hypertension. | A-MedD score quintile not significantly associated with reduced risk of MCI. Higher quintile of A-MedD score in a subset of white women with adjustment for APOE ε4 allele quintile significantly associated with a lower risk of MCI. | Age, race, education level, Women’s Health Initiative hormone trial randomization assignment, baseline 3 MS level, smoking status, physical activity, diabetes, hypertension, BMI, family income, depression, history of CVD, and total energy intake. | [73] |
| Longitudinal | Italy | Older adults in InCHIANTI study n = 832 (44% M) Age: 75.4 ± 7.6 y | 10.1 years | FFQ, MedD score, dietary components, global cognition (MMSE) | Association between MedD and trajectories of cognitive performance in the InCHIANTI study. | Continuous MedD score and higher tertile of MedD significantly associated lower risk of cognitive decline based on MMSE. | Age, gender, study site, chronic diseases, years of education, total energy intake, physical activity, BMI, presence of APOE ε4 allele, CRP, and IL-6. | [63] |
| Longitudinal | Sweden | Older adults in Swedish National study on Aging and Care n = 2223 (871 M 1352 F) Age: M: 69.5 ± 8.6 and F: 71.3 ± 9.1 years | 6 years | 98-item SFFQ, A-MedD, A-DASH, and MIND scores, dietary components, global cognition (MMSE) | Association between slower cognitive decline and dietary patterns: MIND, DASH, MedD, and a Nordic dietary pattern. | Higher A-MedD score significantly associated with less cognitive decline. A-MedD score not significantly associated with a lower risk of MMSE score ≤24. | Total caloric intake, age, gender, education, civil status, physical activity, smoking, BMI, vitamin/mineral supplement intake, vascular disorders, diabetes, cancer, depression, presence of APOE ε4 allele, and dietary components other than those included in each dietary index. | [41] |
| Longitudinal | US | Male health professional participants in Health Professionals Follow-up Study n = 27,842 (27,842 M 0 F) Age at baseline: 51 y | ±26 years | FFQ, MedD score, dietary components, subjective cognitive function (SCF) | Association between long-term adherence to MedD and self-reported subjective cognitive function. | Higher quintile of MedD score associated with a lower risk of both poor SCF and moderate SCF. | Age, smoking history, diabetes, hypertension, depression, hypercholesterolemia, physical activity level, BMI. | [62] |
| Longitudinal | Australia | Older Australian adults n= 1220 (50% men) Age: 60–64 years | 12 years | CSIRO-FFQ, MedD, and MIND scores, dietary components | Cognitive impairment: MCI/dementia (Winbald criteria, NINCDS-ADRDA criteria). | Higher tertile of MedD score not significantly associated with cognitive impairment. | Energy intake, age, sex, presence of APOE ε4 allele, education, mental activity, physical activity, smoking status, depression, diabetes, BMI, hypertension, heart disease, and stroke. | [74] |
| Longitudinal | US | Participants in the Cognitive Reserve (CR) study and the Reference Ability Neural Network (RANN) study n = 183 (89 M 94 F) Age: 53.19 ± 16.52 years | 5 years | FFQ, MedD score, brain MRI | Association of greater adherence to MedD with less accumulation of white matter hyperintensities (WMHs). | MedD adherence negatively associated with an increase in WMHs, adjusting for all covariates. Association between MedD and WMH change moderated by age. | Age, gender, and race/ethnicity. | [85] |
| Cross-sectional | Greece | Older adults n = 557 (237 M 320 F) Age > 65 years | NS | 157-item EPIC-Greek SFFQ, A-MedD score, cognitive impairment (MMSE) | Association of dietary habits with cognitive function among seniors. | Continuous MedD score significantly associated with less cognitive impairment in men but more cognitive impairment in women. | Age, GDS, education, social activity, smoking, metabolic syndrome. | [107] |
| Cross-sectional | Australia | Participants from Southern Australia n = 1183 (432 M 751 F) Age: 50.6 ± 5.8 years | NS | 215-item FFQ, MedD score, dietary components Self-reported cognitive function (CFQ) on mistakes in tasks, perception, memory, and motor function | Association of level of adherence to the MedD with cognitive function and psychological well-being. | MedD score not significantly associated with self-reported cognitive function. | Age, gender, education, BMI, exercise, smoking, and total energy intake. | [108] |
| Cross-sectional | China | Chinese older adults from Hong Kong n= 3670 (1926 M 1744 F) Age: >65 years | NS | 280-item FFQ, MedD score, cognitive function (CSI-D) | Association of a priori or a posteriori diet with risk of cognitive impairment. | No significant association between MedD score and cognitive function in men and women. | Age, BMI, PASE, energy intake, education level, Hong Kong community ladder, smoking status, alcohol use, number of ADLs, GDS category, and self-reported history of diabetes, hypertension, and CVD/stroke. | [66] |
| Cross-sectional | Scotland | Participants enrolled in 1936 n = 878 (±50% M) Age: 69.5 years | NS | 168-item FFQ, MedD (22 items), cognitive function (IQ (MHT), general cognition (WAIS-III LNS, MR, BD, DS, DST backward, SS), processing speed (SS, DS, SCRT, IT), memory LM and VPA immediate and delayed recalls, SSP forward and backward, LNS, DST backward, and verbal ability (NART, WTAR)) | Association between dietary patterns and better cognitive performance in later life, taking into consideration childhood intelligence quotient (IQ) and socioeconomic status. | MedD score positively associated with verbal ability only. | Age, gender, occupational social class, IQ at age of 11 years. | [109] |
| Cross-sectional | Poland | Older adults with high risk of metabolic syndrome n = 87 (31 M 56 F) Age: 70.0 ± 6.5 years | NS | FFQ, A-MedD score (high vs. low), dietary components, MCI, global cognition (MMSE), attention (TMT), visual memory (PRM), executive function (ST, SOC, SWM, SSP) | Association between adherence to MedD and cognitive function (CF), along with selected sociodemographic (SD) and clinical indices. | High MedD score significantly associated with lower prevalence of MCI and higher global cognition, but not with attention, visual memory, or executive function. | Gender, age, education level, smoking status, family status, leisure time physical activity, and existence of metabolic syndrome. | [48] |
| Cross-sectional | US | Participants in study of aging and dementia WHICAP n = 674 (220 M 454 F) Age: 80.1 ± 5.6 years | NS | FFQ, MedD score, MRI, total brain volume (TBV); total gray matter volume (TGMV); total white matter volume (TWMV), cortical thickness | Association of higher adherence to a MedD diet with larger MRI-measured brain volume or cortical thickness. | MedD adherence associated with less brain atrophy, with an effect similar to 5 years of aging. | Age at time of scan, gender, ethnicity, education, BMI, diabetes, mean cognitive z-score, presence of APOE ε4 allele, caloric intake, hypertension, heart disease, and stroke. | [90] |
| Cross-sectional | US | Older adults n = 5907 (40% men) Age: 67.8 years | NS | Cognitive performance (global cognition score based on immediate and delayed recall, backward counting, and serial seven subtraction) | Association between the MedD and MIND diets and cognition in a nationally representative population of older U.S. adults. | Higher tertile of A-MedD score significantly associated with better cognitive performance and lower risk of poor cognitive performance. | Age, gender, race, low education attainment, current smoking, obesity, total wealth, hypertension, diabetes mellitus, physical inactivity, depression, and total energy intake. | [65] |
| Cross-sectional | US | Older Spanish adults n = 79 (36 M 41 F) Age: 81.0 years | NS | 3-day 24 h diet recalls and a face-to- face interview, 14-item Mediterranean Diet Adherence Screener (MEDAS), global cognition (MMSE) | Association of adherence to MedD and cognitive status and depressive symptoms in older adults. | Higher tertile of MEDAS score significantly associated with better cognitive status. | NS | [64] |
| Cross-sectional | Greece | Older adults in Hellenic Longitudinal Investigation of Ageing and Diet n = 1864 (757 M 1107 F) Age: 73.0 ± 6.1 years | NS | SFFQ, A-MedD score, dietary components, cognitive status (dementia (DSM-IV, NINCDS/ADRDA criteria)) and cognitive performance (memory (GVLT), language (BNT, CIMS; categories: objects and the letter A), executive functioning (TMT, verbal fluency, months forward and backward), and visuospatial perception (TMT)) | Association of adherence to an a priori defined MedD and its components with dementia and specific aspects of cognitive function in a representative population cohort in Greece. | Continuous A-MedD score and A-MedD score quartile significantly associated with lower risk of dementia. A-MedD score significantly associated with composite z-score, memory, language, and executive functioning but not with visuospatial perception. | Age, gender, education, number of clinical comorbidities, and energy intake. | [52] |
| Cross-sectional | US | Clinically and cognitively normal participants who were enrolled in observational brain imaging studies n = 116 (44 M 72 F) Age: 50 ± 6 years | NS | FFQ, MedD score, memory (immediate and delayed recall), executive function (WAIS), language (WAIS vocabulary), and MRI-based cortical thickness | Effects of lifestyle and vascular-related risk factors for Alzheimer’s disease (AD) on in vivo MRI-based brain atrophy in asymptomatic young to middle-aged adults. | Continuous MedD score significantly positively associated with MRI-based cortical thickness of the posterior cingulate cortex. MedD score not significantly associated with memory, executive function, or language. | Age, gender, presence of APOE ε4 allele. | [84] |
| Cross-sectional | US | Older participants in study focusing on healthy brain aging and cardiovascular disease risk factors n = 82 (40 M 42 F) Age: 68.8 ± 6.88 years | NS | FFQ, MedD score, cognitive assessment: information processing, executive functioning, MRI scans | Associations between MedD and cognitive and neuroimaging phenotypes in a cohort of nondemented, nondepressed older adults. | After adjustment with all covariates, a significant effect of MedD score on the volume of the dentate gyrus. | Age, gender, education, BMI, and estimated daily calorie intake. | [101] |
Adapted from [20] and updated. ACE: angiotensin-converting enzyme; AD: Alzheimer’s disease; ADLs: activities of daily living; APOE: apolipoprotein E; BD: block design; BMI: body mass index; BNT: Boston Naming Test; CIMS: Complex Ideational Material Subtest; CF: category fluency; CRP: C-reactive protein; CSI-D: Community Screening Instrument for Dementia; CSIRO-FFQ: Commonwealth Scientific and Industrial Research Organization semi-quantitative food frequency questionnaire; CVD: cardiovascular disease; DS: Digit Symbol; DST: Digital Span Task; EBMT: East Boston Memory Test; FFQ: Food Frequency Questionnaire; GDS: Geriatric Depression Scale; GVLT: Greek Verbal Learning Test; IL-6: Interleukin 6; IT: Inspection Time; IQ: intelligence quotient; LM: logical memory; LNS: Letter Number Sequencing; MCI: mild cognitive impairment; MedD: Mediterranean diet; MHT: Moray House Test; MR: matrix reasoning; MRI: Magnetic Resonance Imaging; NS: not specified; NART: National Adult Reading Test; PASE: Physical Activity Scale for Elderly; PRM: pattern recognition memory; SFFQ: semi-quantitative food frequency questionnaire; SCRT: Simple and Choice Reaction Time; SOC: the Stockings of Cambridge Test; SS: Symbol Search; SSP: Spatial Span; ST: Stroop test; SWM: spatial working memory; RI: Rappel indicé; TICS: Telephone Interview for Cognitive Status; TMT: Trail Making Test; VPA: verbal paired associates; WAIS-III: Wechsler Adult Intelligence Scale-III; WTAR: Wechsler test of adult reading; 3 MS: Modified Mini-Mental State Examination; 7 MS: 7 min screening.
4.2. Impact of DASH Diet on ADRD Progression
The Dietary Approaches to Stop Hypertension (DASH) diet is a dietary pattern that aims at preventing and treating hypertension and improving cardiovascular health [110]. The DASH diet shares several similarities with the MedD, as both encourage a high intake of plant-based foods. However, the DASH diet also emphasizes the low consumption and/or limitation of dietary sodium, sweetened beverages, and red meats, and it does not recommend alcohol [12]. Similar to the MedD, the DASH diet has been shown to prevent several cardiovascular risk factors, including high blood pressure and LDL cholesterol, which are associated with the development of dementia and particularly ADRD. Additionally, the DASH diet can modulate oxidative stress, inflammation, and insulin resistance, which are involved in the pathological process of ADRD (Figure 2) [111]. Long-term adherence to the DASH diet has been associated with better cognitive function. For example, this association was found in older American women participating in a six-year follow-up study from the Nurses’ Health study [112], as well as in an observational study spanning 11 years involving older adult men and women in the Cache County Memory Study [104], and in participants of the Memory and Aging Project over 4.1 years, who exhibited slower rates of cognitive decline [58]. However, a cross-sectional study focusing on sedentary adults with cognitive impairment and cardiovascular disease risks reported mixed results regarding cognitive functions. While high adherence to the DASH diet was associated with better verbal memory, it had no effect on executive function, processing speed, or visual memory [102]. Another randomized trial concluded that combining the DASH diet with weight management significantly improved executive function and memory/learning (p = 0.008). When the DASH diet was implemented alone, it showed an improvement in psychomotor speed (p = 0.036) for hypertensive overweight adults in the U.S. after a 4-month intervention [103]. In the same study, when combining the DASH diet intervention with weight management, greater improvements were observed in executive function, memory, learning (p = 0.008), and psychomotor speed (p = 0.023).
Discrepancies have been reported, as other studies have not found a significant association between the DASH diet and cognition. For instance, a prospective longitudinal study among older women in the Women’s Health Initiative Memory Study by Haring et al. [73] concluded that the DASH diet had no significant association with cognitive decline, nor did a high DASH score have an impact on cognitive decline in older community participants (both men and women) in other longitudinal studies [41,113,114]. Another six-month randomized controlled trial with sedentary men and women concluded that the DASH diet alone did not improve cognitive impairment (p = 0.059), but when combined with aerobic exercise, a considerable improvement in executive function (p = 0.012) was observed [115]. These results suggest that the DASH diet, when combined with other non-dietary interventions, possibly synergistically, provides a neuroprotective effect. Table 2 summarizes the different clinical trials investigating the relationship between the DASH diet and ADRD and cognition in the last 10 years. The observed discrepancies in Table 2 may be attributed to differences in study design (RCT vs. observational or cross-sectional), the number and variety of participants (e.g., men only, specific age group, obese or lean individuals), the scoring systems used to define adherence to the DASH diet, and the food products considered in each study. Overall, while the existing evidence hints that the DASH diet might be beneficial for cognitive functioning, further research is needed to validate these findings and demonstrate the benefits of DASH for ADRD progression and risk.
4.3. Impact of MIND Diet on ADRD Progression
The MIND diet, which stands for Mediterranean-DASH Intervention for Neurogenerative Delay, combines elements from both the Mediterranean and DASH diets, with a specific focus on dietary components with neuroprotective effects [12]. Unlike the Mediterranean diet, the MIND diet emphasizes the consumption of berries and green leafy vegetables rather than a high intake of fruits. Numerous observational studies and clinical trials have examined the impact of the MIND diet on ADRD progression (Table 3), and all of these studies suggest a positive association with better cognition [20,41,100,116,117,118,119], lower risks of cognitive impairment [74], and a reduced risk of developing AD [100]. An observational study conducted by Morris et al. [100] over an average of 4.7 years highlighted that high adherence to the MIND diet was associated with less cognitive decline compared to low adherence (p < 0.0001), suggesting that the MIND diet may slow the rate of cognitive decline. Another cross-sectional study involving older U.S. citizens found that higher adherence to the MIND diet was associated with improved cognitive function in a dose–response manner (p < 0.001) [65]. Long-term adherence to the MIND diet was associated with moderately improved verbal memory in later life over a 12.9-year follow-up [120], and a longitudinal study with a 12-year follow-up concluded that the MIND diet reduced the risk of cognitive decline by 53% [74]. Additionally, a study on older adults with a 6-year follow-up on MIND diet adherence showed that a one-point increase in the MIND diet score was associated with a 14% reduction in the risk of subjective memory complaints [121]. Furthermore, a study on older adults highlighted a strong and significant association between MIND diet adherence and better cognitive functioning, even among those diagnosed with AD before or after death [122]. A systematic search conducted by Chu et al. [12] concluded that higher adherence to the MIND diet may be associated with a lower incidence of cognitive impairment and AD, while the MedD appears to provide greater neuroprotection against ADRD. Huang et al. [123] attempted to establish a Chinese version of the MIND diet that aligned with Chinese dietary characteristics and culture while also being more affordable. Moderate and high adherence to the developed Chinese MIND diet were both associated with lower odds of cognitive impairment and IADL disability (0.81 and 0.6, respectively), even after adjusting for covariates. In a recent study by Agarwal et al. [79], higher MIND diet scores were negatively correlated with lower global AD pathology (p = 0.047), and this association remained significant even after adjusting for other covariates (p = 0.047). Participants who had a one-unit higher MIND diet score showed amyloid loads similar to those of individuals who were four years younger [79]. This effect persisted even after adjusting for other lifestyle factors and the burden of vascular disease. A randomized controlled trial conducted over 3 months with a MIND diet intervention for postmenopausal women demonstrated a significant improvement in working memory and verbal recognition [124]. However, combining the MIND diet with different lifestyle components, particularly physical activity, may be more effective in slowing ADRD progression when diagnosed early, as indicated by a cross-sectional study involving both physical activity and the MIND diet in an older adult population [125]. Overall, the current evidence indicates that the MIND diet may be associated with a reduced risk of ADRD and slowed ADRD progression.
4.4. Impact of Ketogenic Diet on ADRD Progression
The ketogenic diet is characterized by high fat and low carbohydrate intake, which promotes ketone production for energy [12]. This diet has been successfully used to treat patients with refractory epilepsy [129], and growing evidence indicates that it may have benefits for cognitive functioning. In a recent case study conducted by Morrill and Gibas [130], the ketogenic diet was found to increase cognitive assessment scores in ApoE4-positive patients with mild AD. Chu et al. [12] extensively reviewed human studies linking the ketogenic diet to cognitive impairment and ADRD development. Out of the 15 identified studies, 14 indicated a significant improvement in cognitive function when ketogenic diets or ketone supplements were administrated to patients with mild cognitive impairment, mild-to-moderate AD, or AD. Grammatikopoulou et al. [131] identified 10 randomized controlled trials that focused on the impact of ketogenic therapies on improving cognitive function and delaying AD progression. The beneficial effects of the ketogenic diet were observed both after acute consumption and with long-term adherence, particularly in participants with mild cognitive impairment. One characteristic of the ketogenic diet is its level of restrictiveness compared to other ‘healthy’ diets, such as the Mediterranean, MIND, and DASH diets [12]. Individuals adhering to the ketogenic diet often experience adverse gastrointestinal events and hypoglycemic episodes during the initial phase [132]. Additionally, long-term compliance with the ketogenic diet presents challenges. For instance, for older adults with mild cognitive impairment or established ADRD health conditions, a drastic shift toward a high-fat dietary pattern can have detrimental effects on their cardiovascular health [12,130]. The potential benefits identified in current studies suggest that more research is needed to evaluate the long-term benefits and side effects, as well as research addressing adherence to this more restrictive eating pattern. It is important to note that, to the best of our knowledge, there are no large-scale RCTs examining ketogenic diet and cognition, so more research is needed in this area.
4.5. Impact of Modified Mediterranean-Ketogenic Diet on ADRD Progression
To meet the dietary requirements of the late-middle-aged population and mitigate the potential negative consequences of long-term adherence to the ketogenic diet, Taylor et al. [133] proposed making the ketogenic diet nutritionally dense. This led to the development of a new diet called the modified Mediterranean-ketogenic diet (MMKD), which combines key elements of the Mediterranean and ketogenic diets. The target macronutrient composition of the MMKD is approximately 5–10% carbohydrate, 60–65% fat, and 30% protein as a percentage of total caloric intake [134]. The diet encourages the consumption of protein sources low in saturated fats, such as fish and lean meats, along with healthy fats, with a particular emphasis on extra virgin olive oil as the main source of fats. It also promotes the intake of fruits, vegetables, and whole grains within certain limits and allows for the consumption of one glass of wine per day [135]. Since the MMKD is relatively new, a few studies have investigated its relationship with AD progression (Table 4). In a pilot study, Nagpal et al. [136] highlighted that the MMKD can modulate the gut microbiome and metabolites, which are associated with improved AD biomarkers in the cerebrospinal fluid. However, they reported an increase in cerebrospinal fluid Aβ42 but a decrease in tau at the end of the 6-week intervention. Similar observations were made in a randomized controlled trial conducted by Neth et al. [135]. A 12-week intervention with MMKD resulted in improved cognitive function and everyday functioning [137]. In a crossover trial investigating the impact of MMKD, a decrease in adiposity was found to be correlated with a similar decrease in cerebrospinal fluid biomarkers [134]. The latest review conducted by Wang et al. [138] addresses different diet patterns and individual food product intake and their respective impacts on ADRD. However, conducting more studies with a large number of participants will help uncover the hidden mechanisms and better understand the impacts of MMKD on individuals with mild cognitive impairment or ADRD.
4.6. Impact of Vegetarian Diet on ADRD Progression
A vegetarian diet is not just a plant-based diet that restricts animal products but is also characterized by a low consumption of saturated fat and a high intake of vegetables, fruits, whole grains, legumes, nuts and seeds, dairy products, and/or eggs [139,140]. The extent to which this diet includes discretionary foods, such as sugar-sweetened beverages, desserts, and potato chips, determines its classification as a ‘healthy’ plant-based food pattern [141]. The vegetarian diet has been associated with a lower risk of several chronic diseases and may have the potential to reduce the risk of cardiometabolic and neurodegenerative diseases (Figure 2) [142]. Despite the increasing number of individuals globally adopting a vegetarian diet, only a few studies have specifically investigated the relationship between this dietary pattern and cognitive impairment, particularly ADRD (Table 5). The Adventist Health Study-2 included older adults who followed a vegetarian or non-vegetarian diet. This cohort demonstrated that vegetarians had higher adherence to their dietary patterns constantly over decades, which was associated with better memory and language abilities [143]. Liu et al. [141] assessed the difference in cognition among different races and dietary patterns. They found that a healthy plant-based diet was associated with significantly slower rates of decline in global cognition (p = 0.032), perceptual speed (p = 0.04), and episodic memory (p = 0.04), specifically in African American participants. A large study conducted in Taiwan concluded that vegetarians had a reduced risk of developing dementia compared to non-vegetarians [144]. Despite the limited number of studies on vegetarian diets, existing evidence suggests that such diets may have a beneficial impact on slowing the progression of cognitive decline. The vegetarian diet is rich in nutrients known for their anti-inflammatory and antioxidant activities. However, it is important to note that patients with cognitive impairment and ADRD may still require a certain intake of animal-derived products, especially meat [145,146]. Indeed, older adults have high protein needs, which will present a challenge when restricting animal product consumption to adhere to a vegetarian diet. These products ensure an important supply of B vitamins that are highly and strictly related to AD development and progression [146].
4.7. Impact of Vegan Diet on ADRD Progression
What distinguishes the vegan diet from plant-based and vegetarian diets is that it excludes all animal products, not just meat. In fact, the vegan diet is not only free of meat but also eliminates all animal-derived products. When compared to an omnivorous diet, the vegan diet is richer in fiber, polyunsaturated fatty acids, and vitamins [147,148,149]. These individual components can potentially slow down AD pathophysiology. Despite the suspected beneficial impacts on AD, no studies have been conducted to investigate the specific impact of a vegan diet. However, it is important to pay special attention to the long-term effects of a vegan diet, as it may lead to deficiencies in essential micronutrients such as vitamin B12 and vitamin D. These deficiencies are closely associated with the development and progression of ADRD [150].
5. Impact of Specific Dietary Patterns on ADRD Prevention
The multiple dietary patterns reviewed here have shown potential for slowing the progression of ADRD and may also play a preventive role. However, it is important to determine when to start adhering to these dietary patterns, given that ADRD symptoms may manifest decades after the onset of brain changes. Current research evidence suggests that the first prodromal symptoms, such as changes in the synapse number, nutritional status, cognitive level, and neuropathological changes in the central nervous system, appear around the age of 50 years. Therefore, the ideal age to start taking preventive actions and implementing diet interventions seems to be around 50–60 years old or earlier, with impacts being assessed starting from 70 years old. This is due to the prevalence of long-term interventions rather than the acute effects of consumption on ADRD prevention. As a result, most proposed research studies target participants between the age of 50 and 70 years who do not show any symptoms of cognitive impairment but carry one or several risk factors. Some researchers recommend that dietary interventions last 4–8 years to enable long-term adherence effects to accumulate [151]. To make dietary patterns effective in preventing neurodegenerative diseases, the interventions need to be balanced and meet the dietary requirements of the target population. They should help maintain proper blood pressure and optimal cholesterol, glucose, and homocysteine levels. The proposed diet should also prevent overweight and obesity, which are increasing risk factors for AD [152]. The following sections present the dietary patterns that have been studied and linked to ADRD prevention (Figure 1 and Figure 2).
5.1. Impact of Mediterranean Diet on ADRD Prevention
Given the extensive research on the MedD in the management of ADRD, it is reasonable to explore whether it has the potential to prevent the onset of this disease as well. In a study conducted by Hoscheidt et al. [153], normal cognitive participants who adhered to the MedD showed a decrease in Aβ40 levels and a shift in the Aβ42/40 ratio, indicating a decreased risk of AD development. The results of an epidemiological study conducted by Andreu-Reinon et al. [87] suggest that over a 20-year follow-up period, participants with high adherence to the MedD had a 20% lower risk of dementia compared to those with low adherence. In fact, every 2-point increase in MedD adherence provided an 8% lower risk of developing AD. However, when examining the linear or non-linear trends between adherence to MedD and AD, no statistically significant associations were reported (p = 0.196, p = 0.353). Similarly, the studies conducted by Féart et al. [154] and Hu et al. [155] found no statistically significant association between adherence to the MedD and the incidence of ADRD (p = 0.72). High adherence to the MedD was not associated with a decreased risk of ADRD after 4.1 years of follow-up in an older French population [154] or after 12 years of follow-up in an older Swedish population [72]. On the other hand, the results of the Washington Heights-Inwood Columbia Aging Project conducted by Scarmeas et al. [50] concluded that a one-point increase in the MedD scale decreased the risk of ADRD by 9%. The latest meta-analysis performed by Solch et al. [9] demonstrated a 32% decreased risk of developing ADRD when adhering to the MedD compared to low adherence, with low heterogeneity between studies. The observed beneficial effects of the MedD are attributed to its anti-inflammatory and antioxidant capacities, as well as its high fiber and polyphenol contents, which impact the gut microbiota (Figure 2) [156,157]. The reported discrepancies may be attributed to variations in scoring systems used to define diet adherence, differences in the selected populations’ age, and differences in risk factors for developing AD, as well as the duration of the follow-up and the lack of an AD diagnosis at the beginning of the study period. Despite the reported non-significant effects on ADRD prevention, it is still plausible that some protection is provided through the various mechanisms mentioned earlier. To arrive at evidence-based conclusions, it is imperative to conduct numerous clinical trials, particularly randomized controlled trials, that examine the impact of adherence to the MedD on various AD biomarkers and imaging. Additionally, long-term observational studies starting with a middle-aged population and following them for 12–15+ years are necessary.
5.2. Impact of DASH Diet on ADRD Prevention
There is only one longitudinal study focusing on adherence to the DASH diet and its implication in the development of ADRD in U.S. participants [100]. The study concluded that high adherence to the DASH diet decreases the risk of developing AD by 39%. The observed positive impacts are expected to be the result of long-time use, particularly before the first symptoms appear [158]. To reach a unanimous conclusion about the prevention of ADRD development through the DASH diet, several studies are required, with a special focus on early adherence (in the middle-aged population) and long-term follow-ups (12–15+ years).
5.3. Impact of MIND Diet on ADRD Prevention
Only one longitudinal study conducted in an older adult population from the Memory and Aging Project evaluated the relationship between the MIND diet and the prevention of ADRD [100]. The study observed a 53% lower risk of ADRD after a 4.5-year follow-up period. Furthermore, moderate adherence to the MIND diet resulted in a 35% decrease in the risk of developing AD. Undoubtedly, more studies need to be conducted to arrive at evidence-based conclusions regarding the potential beneficial effects of the MIND diet, including the examination of adherence beginning in middle age.
6. Discussion
Across the literature, there is relatively strong evidence that adherence to the MedD, DASH, MIND, and MMKD diets may reduce the risk of developing ADRD and slow the rate of decline. These diets may be particularly beneficial for cognitive health based on common factors, such as increased polyunsaturated fat, higher fiber, and nutrients and compounds that have neuroprotective properties. Multiple studies have provided evidence linking the intake of certain nutrients common in these diets to preventive or therapeutic effects on AD specifically [12]. For instance, polyphenols have shown the ability to promote cognitive well-being through several pathways. They can improve cerebral blood flow, reduce oxidative stress, decrease neuroinflammation, enhance neurogenesis, and promote neuroplasticity. [159,160,161,162]. Whole grains, through their cardiometabolic and gastrointestinal benefits, as evidenced by the gut microbiota–brain axis, also contribute to cognitive improvement [136,163]. Omega-3 polyunsaturated fatty acids, especially those derived from marine sources, as well as mono- and polyunsaturated fatty acids found in nuts, contribute to brain protection through various effects, including anti-inflammatory action, blood pressure reduction, and endothelial enhancement [164,165,166]. Vitamins, such as B9, B12, and E, have been associated with neurogenesis in adults due to their antioxidant effects [167,168,169]. Many of these nutrients operate through mechanistic pathways that are associated with reducing metabolic syndromes, such as lowering blood pressure, decreasing insulin resistance, and reducing blood sugar and triglyceride levels, resulting in enhanced cognitive health [170,171,172,173]. It is also important to address the appropriate proportions of these nutrient intakes within the suggested dietary patterns. Furthermore, upcoming randomized controlled trials should focus on assessing the intake of these elements within these dietary patterns and their impact on ADRD progression and prevention, as their beneficial effects may be associated with their combined consumption rather than their individual intake. In addition, the amounts of deleterious foods and drinks, such as highly processed meat, refined grains, refined sugars, and beverages with high refined sugar content, need to be monitored in the proposed dietary patterns to be studied, as these products have been significantly linked to an increased risk of cognitive impairment and ADRD. Consuming them alongside the proposed diet may decrease the effectiveness of the studied dietary pattern and its components.
7. Parameters Affecting Food Intake in Older Adults
Older adults often have unique dietary needs and preferences. The quality and quantity of their dietary intake are impacted by various parameters, such as physiological, economic, and societal factors, which can become more pronounced with age [174]. Some of these factors are personal, encompassing sociodemographic and psychosocial aspects, as well as lifestyle factors [175,176,177]. In fact, diet quality has been strongly linked to marital status and living arrangement. Living with a partner or in a community allows older adults to have some social support and share food [178]. Furthermore, emerging evidence shows that the association between dietary elements and neurocognition depends on socioeconomic status, with the effects of diet being more pronounced in people with low socioeconomic status [179,180]. At the same time, older adults are subject to some conditions impacting their food intake, namely, loss of sensory perceptions (olfaction, taste bud loss, salivation decrease), poor oral health, and particularly mastication difficulties, which represent barriers to diet variety and a healthy diet. ADRD in particular can lead to sensory changes that can also lead to reduced appetite. Further, certain medications and medical treatments can increase deficiencies of some nutrients, which must be emphasized in their diet. Likewise, most older adults suffer dexterity loss with aging, which can lead to practical challenges related to cooking and food preparation [181].
8. Other Parameters Important for ADRD
Conducting research to understand how to prevent AD is valuable. It is a part of the science of risk reduction, aiming to gather evidence on noteworthy lifestyle changes. According to the Centers for Disease Control and Prevention, healthy lifestyle habits such as regular exercise and blood pressure management are among the noticeable factors that can lower the risk of dementia. Similarly, adopting healthy habits that reduce the prevalence of cancer, diabetes, and heart diseases may also be beneficial in preventing cognitive decline. Given the specific nature of neurodegenerative diseases, other factors should also be taken into consideration for daily habits, such as not smoking, stress reduction, and engaging in mental and physical activities [152]. Emerging evidence highlights that three lifestyle components, namely, social, mental, and physical factors, are inversely correlated with the risk and incidence of ADRD. In this context, maintaining a lifestyle with high levels of physical, mental, and social activities stands out as one of the important factors contributing to enhancing the quality and expectancy of life. Enhanced psychosocial engagement, in turn, lowers the risk of dementia and neurocognitive impairment in ADRD [182]. Additionally, other factors are associated with cognitive impairment and ADRD, such as marital status and frequent social contacts. Maintaining frequent social contacts can be achieved through numerous activities, including participating in social activities, having a larger social network, and receiving greater social support, thus promoting social engagement [183]. These social parameters vary among individuals as personal attributes, and they are highly affected by the place of residence of older adults. In recent years, there has been a growing interest in the new concept of lifestyle medicine, which is associated with optimal brain health and healthy aging. This concept is based on six pillars, namely, consuming whole foods and following plant-based dietary patterns, maintaining physical activity, managing stress through non-pharmaceutical means, avoiding risky substances, ensuring good-quality sleep, and maintaining social connections [184]. Indeed, the Western lifestyle is characterized by a sedentary nature, with sedentarity or physical inactivity defined as engaging in less than 30 min of moderate-intensity physical activity on a minimum of 5 days per week or at least 20 min of vigorous-intensity physical activity on a minimum of 3 days per week [185]. Research has shown that leading an active lifestyle is inversely related to the risk of cognitive decline, with aerobic exercise training being the most widely studied form of physical activity in relation to neurocognitive function and aging [186,187]. Simultaneously, other studies have highlighted the importance of participating in leisure activities and how it can result in better diet quality for older adults [188]. Ultimately, it has been found that multidomain programs, which include interventions related to diet, nutrition, exercise, neurocognitive exercises, and social activities, yield better outcomes in slowing down disease progression compared to single-domain interventions [189].
9. Conclusions
Considering the rapidly growing number of people with or at risk of developing ADRD in the upcoming decades, it is crucial to find low-cost and effective ways to prevent and/or ameliorate the development and progression of these diseases. Diet, indeed, appears to be one of the most important modifiable factors that influence ADRD risk. Despite the discrepancies revealed in this review due to differences in study populations, associated risk factors, geographical regions, and scoring methods, plant-based dietary patterns generally show a positive correlation with a reduction in AD advancement and the lowering of its incidence. The MedD, DASH, MIND, and MMKD diets have the greatest efficacy for their neuroprotective benefits. The precise cellular and molecular pathways underlying and mediating the preventive and ameliorative effects of these diets on ADRD are still unclear and need to be elucidated through prospective clinical and mechanistic studies. For future studies, it is advisable to consider holistic approaches that not only incorporate dietary patterns but also encompass factors related to physical, social, economic, and mental health components.
Author Contributions
I.E. and B.A. formulated the research questions and conceptualized and designed the review; I.E. conducted the literature search, screened the articles, extracted the data, and drafted the manuscript; R.N. helped in preparing tables and figures and reviewed and edited the manuscript; R.N. and J.S. provided critiques, review, and comments during manuscript drafting. All authors have read and agreed to the published version of the manuscript.
Funding
I.E. is supported by the Fulbright Visiting Scholar. J.S. is supported by the National Institutes of Health (NIH) FIRST award number U54CA267730-02, with funding from the Office of the Director, NIH (NCI). R.N. is supported by Florida State University (FSU) startup funds and FSU Council on Research & Creativity grant.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank Florida State University for providing the resources needed to carry out the review work.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization (WHO). 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 15 March 2023).
- He, Y.; Li, C.; Yang, Y.; Li, Y.; Wang, Y.; Yang, H.; Jin, T.; Chen, S. Meta-analysis of the rs2075650 polymorphism and risk of Alzheimer disease. Aging Clin. Exp. Res. 2016, 28, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Gaugler, J.; James, B.; Johnson, T.; Reimer, J.; Solis, M.; Weuve, J.; Buckley, R.F.; Hohman, T.J.; Alzheimer’s Association. Alzheimer’s Disease Facts and Figures. Alzheimer’s Dement. 2022, 18, 700–789. [Google Scholar]
- Francis, P.T.; Palmer, A.M.; Snape, M.; Wilcock, G.K. The cholinergic hypothesis of Alzheimer’s disease: A review of progress. J. Neurol. Neurosurg. Psychiatry 1999, 66, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Bagyinszky, E.; Youn, Y.C.; An, S.S.; Kim, S. The genetics of Alzheimer’s disease. Clin. Interv. Aging 2014, 9, 535–551. [Google Scholar] [CrossRef] [Green Version]
- Jalbert, J.J.; Daiello, L.A.; Lapane, K.L. Dementia of the Alzheimer Type. Epidemiol. Rev. 2008, 30, 15–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farlow, M.R. Etiology and pathogenesis of Alzheimer’s disease. Am. J. Health Syst. Pharm. 1998, 55 (Suppl. S2), S5–S10. [Google Scholar] [CrossRef]
- Hersi, M.; Irvine, B.; Gupta, P.; Gomes, J.; Birkett, N.; Krewski, D. Risk factors associated with the onset and progression of Alzheimer’s disease: A systematic review of the evidence. Neurotoxicology 2017, 61, 143–187. [Google Scholar] [CrossRef]
- Solch, R.J.; Aigbogun, J.O.; Voyiadjis, A.G.; Talkington, G.M.; Darensbourg, R.M.; O’Connell, S.; Pickett, K.M.; Perez, S.R.; Maraganore, D.M. Mediterranean diet adherence, gut microbiota, and Alzheimer’s or Parkinson’s disease risk: A systematic review. J. Neurol. Sci. 2022, 434, 120166. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). 2023. Available online: https://www.cdc.gov/aging/aginginfo/alzheimers.htm (accessed on 15 March 2023).
- Tejada-Vera, B. Mortality from Alzheimer’s Disease in the United States: Data for 2000 and 2010; NCHS Data Brief, No 116; Hyattsville, M.D., Ed.; National Center for Health Statistics: Hyattsville, MD, USA, 2013.
- Chu, C.Q.; Yu, L.L.; Qi, G.Y.; Mi, Y.S.; Wu, W.Q.; Lee, Y.K.; Zhai, Q.X.; Tian, F.W.; Chen, W. Can dietary patterns prevent cognitive impairment and reduce Alzheimer’s disease risk: Exploring the underlying mechanisms of effects. Neurosci. Biobehav. Rev. 2022, 135, 104556. [Google Scholar] [CrossRef]
- James, B.D.; Wilson, R.S.; Boyle, P.A.; Trojanowski, J.Q.; Bennett, D.A.; Schneider, J.A. TDP-43 stage, mixed pathologies, and clinical Alzheimer’s-type dementia. Brain 2016, 139, 2983–2993. [Google Scholar] [CrossRef] [Green Version]
- Dodge, H.H.; Zhu, J.; Woltjer, R.; Nelson, P.T.; Bennett, D.A.; Cairns, N.J.; Fardo, D.W.; Kaye, J.A.; Lyons, D.E.; Mattek, N.; et al. SMART data consortium. Risk of incident clinical diagnosis of Alzheimer’s disease-type dementia attributable to pathology-confirmed vascular disease. Alzheimers Dement. 2017, 13, 613–623. [Google Scholar] [CrossRef] [PubMed]
- Boyle, P.A.; Yu, L.; Leurgans, S.E.; Wilson, R.S.; Brookmeyer, R.; Schneider, J.A.; Bennett, D.A. Attributable risk of Alzheimer’s dementia attributed to age-related neuropathologies. Ann. Neurol. 2019, 85, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Norton, S.; Matthews, F.E.; Barnes, D.E.; Yaffe, K.; Brayne, C. Potential for primary prevention of Alzheimer’s disease: An analysis of population-based data. Lancet Neurol. 2014, 13, 788–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crous-Bou, M.; Minguillón, C.; Gramunt, N.; Molinuevo, J.L. Alzheimer’s disease prevention: From risk factors to early intervention. Alzheimers Res. Ther. 2017, 9, 71. [Google Scholar] [CrossRef] [Green Version]
- Dominguez, L.J.; Veronese, N.; Vernuccio, L.; Catanese, G.; Inzerillo, F.; Salemi, G.; Barbagallo, M. Nutrition, Physical Activity, and Other Lifestyle Factors in the Prevention of Cognitive Decline and Dementia. Nutrients 2021, 13, 4080. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Van den Brink, A.C.; Brouwer-Brolsma, E.M.; Berendsen, A.A.M.; van de Rest, O. The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diets Are Associated with Less Cognitive Decline and a Lower Risk of Alzheimer’s Disease-A Review. Adv. Nutr. 2019, 10, 1040–1065. [Google Scholar] [CrossRef] [Green Version]
- Scarmeas, N.; Anastasiou, C.A.; Yannakoulia, M. Nutrition and prevention of cognitive impairment. Lancet Neurol. 2018, 17, 1006–1015. [Google Scholar] [CrossRef]
- Stern, Y. Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol. 2012, 11, 1006–1012. [Google Scholar] [CrossRef] [Green Version]
- Song, S.; Stern, Y.; Gu, Y. Modifiable lifestyle factors and cognitive reserve: A systematic review of current evidence. Ageing Res. Rev. 2022, 74, 101551. [Google Scholar] [CrossRef]
- Zainuddin, M.S.; Thuret, S. Nutrition, adult hippocampal neurogenesis and mental health. Br. Med. Bull. 2012, 103, 89–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayden, K.M.; Reed, B.R.; Manly, J.J.; Tommet, D.; Pietrzak, R.H.; Chelune, G.J.; Yang, F.M.; Revell, A.J.; Bennett, D.A.; Jones, R.N. Cognitive decline in the elderly: An analysis of population heterogeneity. Age Ageing 2011, 40, 684–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, L.; Boyle, P.A.; Segawa, E.; Leurgans, S.; Schneider, J.A.; Wilson, R.S.; Bennett, D.A. Residual decline in cognition after adjustment for common neuropathologic conditions. Neuropsychology 2015, 29, 335–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, R.S.; Wang, T.; Yu, L.; Bennett, D.A.; Boyle, P.A. Normative Cognitive Decline in Old Age. Ann. Neurol. 2020, 87, 816–829. [Google Scholar] [CrossRef]
- Christ, A.; Lauterbach, M.; Latz, E. Western Diet and the Immune System: An Inflammatory Connection. Immunity 2019, 51, 794–811. [Google Scholar] [CrossRef]
- Statovci, D.; Aguilera, M.; MacSharry, J.; Melgar, S. The Impact of Western Diet and Nutrients on the Microbiota and Immune Response at Mucosal Interfaces. Front. Immunol. 2017, 8, 838. [Google Scholar] [CrossRef] [Green Version]
- Kanehara, R.; Goto, A.; Sawada, N.; Mizoue, T.; Noda, M.; Hida, A.; Iwasaki, M.; Tsugane, S. Association between sugar and starch intakes and type 2 diabetes risk in middle-aged adults in a prospective cohort study. Eur. J. Clin. Nutr. 2022, 76, 746–755. [Google Scholar] [CrossRef]
- Chareonrungrueangchai, K.; Wongkawinwoot, K.; Anothaisintawee, T.; Reutrakul, S. Dietary Factors and Risks of Cardiovascular Diseases: An Umbrella Review. Nutrients 2020, 12, 1088. [Google Scholar] [CrossRef] [Green Version]
- Gaesser, G.A. Whole Grains, Refined Grains, and Cancer Risk: A Systematic Review of Meta-Analyses of Observational Studies. Nutrients 2020, 12, 3756. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Moubarac, J.C.; Levy, R.B.; Canella, D.S.; Louzada, M.L.D.C.; Cannon, G. Household availability of ultra-processed foods and obesity in nineteen European countries. Public Health Nutr. 2018, 21, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Crittenden, A.N.; Schnorr, S.L. Current views on hunter-gatherer nutrition and the evolution of the human diet. Am. J. Phys. Anthropol. 2017, 162 (Suppl. S63), 84–109. [Google Scholar] [CrossRef] [PubMed]
- Requena, T.; Martínez-Cuesta, M.C.; Peláez, C. Diet and microbiota linked in health and disease. Food Funct. 2018, 9, 688–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelkman, C.L. Effects of the glycemic index of foods on serum concentrations of high-density lipoprotein cholesterol and triglycerides. Curr. Atheroscler. Rep. 2001, 3, 456–461. [Google Scholar] [CrossRef] [PubMed]
- De Roos, A.; van der Grond, J.; Mitchell, G.; Westenberg, J. Magnetic Resonance Imaging of Cardiovascular Function and the Brain: Is Dementia a Cardiovascular-Driven Disease? Circulation 2017, 135, 2178–2195. [Google Scholar] [CrossRef] [Green Version]
- Carlsson, C.M. Type 2 diabetes mellitus, dyslipidemia, and Alzheimer’s disease. J. Alzheimers Dis. 2010, 20, 711–722. [Google Scholar] [CrossRef]
- Kopp, W. How Western Diet and Lifestyle Drive the Pandemic of Obesity And Civilization Diseases. Diabetes Metab. Syndr. Obes. 2019, 12, 2221–2236. [Google Scholar] [CrossRef] [Green Version]
- Gardener, S.L.; Rainey-Smith, S.R.; Barnes, M.B.; Sohrabi, H.R.; Weinborn, M.; Lim, Y.Y.; Harrington, K.; Taddei, K.; Gu, Y.; Rembach, A.; et al. Dietary patterns and cognitive decline in an Australian study of ageing. Mol. Psychiatry 2015, 20, 860–866. [Google Scholar] [CrossRef]
- Shakersain, B.; Rizzuto, D.; Larsson, S.C.; Faxén-Irving, G.; Fratiglioni, L.; Xu, W.L. The Nordic Prudent Diet Reduces Risk of Cognitive Decline in the Swedish Older Adults: A Population-Based Cohort Study. Nutrients 2018, 10, 229. [Google Scholar] [CrossRef] [Green Version]
- Szczechowiak, K.; Diniz, B.S.; Leszek, J. Diet and Alzheimer’s dementia—Nutritional approach to modulate inflammation. Pharmacol. Biochem. Behav. 2019, 184, 172743. [Google Scholar] [CrossRef]
- Liu, X.; Morris, M.C.; Dhana, K.; Ventrelle, J.; Johnson, K.; Bishop, L.; Hollings, C.S.; Boulin, A.; Laranjo, N.; Stubbs, B.J.; et al. Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) study: Rationale, design and baseline characteristics of a randomized control trial of the MIND diet on cognitive decline. Contemp. Clin. Trials. 2021, 102, 106270. [Google Scholar] [CrossRef]
- Gutierrez, L.; Folch, A.; Rojas, M.; Cantero, J.L.; Atienza, M.; Folch, J.; Camins, A.; Ruiz, A.; Papandreou, C.; Bulló, M. Effects of Nutrition on Cognitive Function in Adults with or without Cognitive Impairment: A Systematic Review of Randomized Controlled Clinical Trials. Nutrients 2021, 13, 3728. [Google Scholar] [CrossRef] [PubMed]
- Keys, A.B.; Keys, M. How to Eat Well and Stay Well the Mediterranean Way; Doubleday: New York, NY, USA, 1975. [Google Scholar]
- Scarmeas, N.; Stern, Y.; Mayeux, R.; Manly, J.J.; Schupf, N.; Luchsinger, J.A. Mediterranean diet and mild cognitive impairment. Arch. Neurol. 2009, 66, 216–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, C.; Sommerlad, A.; Lyketsos, C.G.; Livingston, G. Modifiable predictors of dementia in mild cognitive impairment: A systematic review and meta-analysis. Am. J. Psychiatry 2015, 172, 323–334. [Google Scholar] [CrossRef] [Green Version]
- Bajerska, J.; Woźniewicz, M.; Suwalska, A.; Jeszka, J. Eating patterns are associated with cognitive function in the elderly at risk of metabolic syndrome from rural areas. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 3234–3245. [Google Scholar]
- Trichopoulou, A.; Kyrozis, A.; Rossi, M.; Katsoulis, M.; Trichopoulos, D.; La Vecchia, C.; Lagiou, P. Mediterranean diet and cognitive decline over time in an elderly Mediterranean population. Eur. J. Nutr. 2015, 54, 1311–1321. [Google Scholar] [CrossRef] [PubMed]
- Scarmeas, N.; Stern, Y.; Tang, M.X.; Mayeux, R.; Luchsinger, J.A. Mediterranean diet and risk for Alzheimer’s disease. Ann. Neurol. 2006, 59, 912–921. [Google Scholar] [CrossRef] [Green Version]
- van de Rest, O.; Berendsen, A.A.; Haveman-Nies, A.; de Groot, L.C. Dietary patterns, cognitive decline, and dementia: A systematic review. Adv. Nutr. 2015, 6, 154–168. [Google Scholar] [CrossRef] [Green Version]
- Anastasiou, C.A.; Yannakoulia, M.; Kosmidis, M.H.; Dardiotis, E.; Hadjigeorgiou, G.M.; Sakka, P.; Arampatzi, X.; Bougea, A.; Labropoulos, I.; Scarmeas, N. Mediterranean diet and cognitive health: Initial results from the Hellenic Longitudinal Investigation of Ageing and Diet. PLoS ONE 2017, 12, e0182048. [Google Scholar] [CrossRef] [Green Version]
- Loughrey, D.G.; Lavecchia, S.; Brennan, S.; Lawlor, B.A.; Kelly, M.E. The Impact of the Mediterranean Diet on the Cognitive Functioning of Healthy Older Adults: A Systematic Review and Meta-Analysis. Adv. Nutr. 2017, 8, 571–586. [Google Scholar] [CrossRef]
- Samieri, C.; Okereke, O.I.; EDevore, E.; Grodstein, F. Long-term adherence to the Mediterranean diet is associated with overall cognitive status, but not cognitive decline, in women. J. Nutr. 2013, 143, 493–499. [Google Scholar] [CrossRef] [Green Version]
- Kesse-Guyot, E.; Andreeva, V.A.; Lassale, C.; Ferry, M.; Jeandel, C.; Hercberg, S.; Galan, P. SU.VI.MAX 2 Research Group. Mediterranean diet and cognitive function: A French study. Am. J. Clin. Nutr. 2013, 97, 369–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tangney, C.C.; Kwasny, M.J.; Li, H.; Wilson, R.S.; Evans, D.A.; Morris, M.C. Adherence to a Mediterranean-type dietary pattern and cognitive decline in a community population. Am. J. Clin. Nutr. 2011, 93, 601–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SACN. SACN Statement on Diet, Cognitive Impairment and Dementia; Public Health England: London, UK, 2018.
- Tangney, C.C.; Li, H.; Wang, Y.; Barnes, L.; Schneider, J.A.; Bennett, D.A.; Morris, M.C. Relation of DASH- and Mediterranean-like dietary patterns to cognitive decline in older persons. Neurology 2014, 83, 1410–1416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galbete, C.; Toledo, E.; Toledo, J.B.; Bes-Rastrollo, M.; Buil-Cosiales, P.; Marti, A.; Guillén-Grima, F.; Martínez-González, M.A. Mediterranean diet and cognitive function: The SUN project. J. Nutr. Health Aging 2015, 19, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Koyama, A.; Houston, D.K.; Simonsick, E.M.; Lee, J.S.; Ayonayon, H.N.; Shahar, D.R.; Rosano, C.; Satterfield, S.; Yaffe, K. Association between the Mediterranean diet and cognitive decline in a biracial population. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 354–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, B.; Adair, L.S.; Plassman, B.L.; Batis, C.; Edwards, L.J.; Popkin, B.M.; Mendez, M.A. Dietary Patterns and Cognitive Decline Among Chinese Older Adults. Epidemiology 2015, 26, 758–768. [Google Scholar] [CrossRef] [Green Version]
- Bhushan, A.; Fondell, E.; Ascherio, A.; Yuan, C.; Grodstein, F.; Willett, W. Adherence to Mediterranean diet and subjective cognitive function in men. Eur. J. Epidemiol. 2018, 33, 223–234. [Google Scholar] [CrossRef]
- Tanaka, T.; Talegawkar, S.A.; Jin, Y.; Colpo, M.; Ferrucci, L.; Bandinelli, S. Adherence to a Mediterranean Diet Protects from Cognitive Decline in the Invecchiare in Chianti Study of Aging. Nutrients 2018, 10, 2007. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Galiot, A.; Goñi, I. Adherence to the Mediterranean diet pattern, cognitive status and depressive symptoms in an elderly non-institutionalized population. Nutr. Hosp. 2017, 34, 338–344. [Google Scholar] [CrossRef]
- McEvoy, C.T.; Guyer, H.; Langa, K.M.; Yaffe, K. Neuroprotective Diets Are Associated with Better Cognitive Function: The Health and Retirement Study. J. Am. Geriatr. Soc. 2017, 65, 1857–1862. [Google Scholar] [CrossRef] [Green Version]
- Chan, R.; Chan, D.; Woo, J. A cross sectional study to examine the association between dietary patterns and cognitive impairment in older Chinese people in Hong Kong. J. Nutr. Health Aging 2013, 17, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Samieri, C.; Grodstein, F.; Rosner, B.A.; Kang, J.H.; Cook, N.R.; Manson, J.E.; Buring, J.E.; Willett, W.C.; Okereke, O.I. Mediterranean diet and cognitive function in older age. Epidemiology 2013, 24, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Vercambre, M.N.; Grodstein, F.; Berr, C.; Kang, J.H. Mediterranean diet and cognitive decline in women with cardiovascular disease or risk factors. J. Acad. Nutr. Diet. 2012, 112, 816–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, R.O.; Geda, Y.E.; Cerhan, J.R.; Knopman, D.S.; Cha, R.H.; Christianson, T.J.; Pankratz, V.S.; Ivnik, R.J.; Boeve, B.F.; O’Connor, H.M.; et al. Vegetables, unsaturated fats, moderate alcohol intake, and mild cognitive impairment. Dement. Geriatr. Cogn. Disord. 2010, 29, 413–423. [Google Scholar] [CrossRef] [Green Version]
- Cherbuin, N.; Anstey, K.J. The Mediterranean diet is not related to cognitive change in a large prospective investigation: The PATH Through Life study. Am. J. Geriatr. Psychiatry 2012, 20, 635–639. [Google Scholar] [CrossRef]
- Gardener, S.; Gu, Y.; Rainey-Smith, S.R.; Keogh, J.B.; Clifton, P.M.; Mathieson, S.L.; Taddei, K.; Mondal, A.; Ward, V.K.; Scarmeas, N.; et al. Adherence to a Mediterranean diet and Alzheimer’s disease risk in an Australian population. Transl. Psychiatry 2012, 2, e164. [Google Scholar] [CrossRef] [Green Version]
- Olsson, E.; Karlström, B.; Kilander, L.; Byberg, L.; Cederholm, T.; Sjögren, P. Dietary patterns and cognitive dysfunction in a 12-year follow-up study of 70 year old men. J. Alzheimers Dis. 2015, 43, 109–119. [Google Scholar] [CrossRef]
- Haring, B.; Wu, C.; Mossavar-Rahmani, Y.; Snetselaar, L.; Brunner, R.; Wallace, R.B.; Neuhouser, M.L.; Wassertheil-Smoller, S. No Association between Dietary Patterns and Risk for Cognitive Decline in Older Women with 9-Year Follow-Up: Data from the Women’s Health Initiative Memory Study. J. Acad. Nutr. Diet. 2016, 116, 921–930.e1. [Google Scholar] [CrossRef] [Green Version]
- Hosking, D.E.; Eramudugolla, R.; Cherbuin, N.; Anstey, K.J. MIND not Mediterranean diet related to 12-year incidence of cognitive impairment in an Australian longitudinal cohort study. Alzheimers Dement. 2019, 15, 581–589. [Google Scholar] [CrossRef]
- Gregory, S.; Pullen, H.; Ritchie, C.W.; Shannon, O.M.; Stevenson, E.J.; Muniz-Terrera, G. Mediterranean diet and structural neuroimaging biomarkers of Alzheimer’s and cerebrovascular disease: A systematic review. Exp. Gerontol. 2023, 172, 112065. [Google Scholar] [CrossRef]
- Valls-Pedret, C.; Sala-Vila, A.; Serra-Mir, M.; Corella, D.; de la Torre, R.; Martínez-González, M.Á.; Martínez-Lapiscina, E.H.; Fitó, M.; Pérez-Heras, A.; Salas-Salvadó, J.; et al. Mediterranean Diet and Age-Related Cognitive Decline: A Randomized Clinical Trial. JAMA Intern. Med. 2015, 175, 1094–1103. [Google Scholar] [CrossRef] [Green Version]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [Green Version]
- Hill, E.; Goodwill, A.M.; Gorelik, A.; Szoeke, C. Diet and biomarkers of Alzheimer’s disease: A systematic review and meta-analysis. Neurobiol. Aging 2019, 76, 45–52. [Google Scholar] [CrossRef]
- Agarwal, P.; Leurgans, S.E.; Agarwal, S.; Aggarwal, N.; Cherian, L.J.; James, B.D.; Dhana, K.; Barnes, L.L.; Bennett, D.A.; Schneider, J.A. Association of Mediterranean-DASH Intervention for Neurodegenerative Delay and Mediterranean Diets with Alzheimer Disease Pathology. Neurology 2023, 10, 1212. [Google Scholar] [CrossRef]
- Cowell, O.R.; Mistry, N.; Deighton, K.; Matu, J.; Griffiths, A.; Minihane, A.M.; Mathers, J.C.; Shannon, O.M.; Siervo, M. Effects of a Mediterranean diet on blood pressure: A systematic review and meta-analysis of randomized controlled trials and observational studies. J. Hypertens. 2021, 39, 729–739. [Google Scholar] [CrossRef] [PubMed]
- Shannon, O.M.; Ashor, A.W.; Scialo, F.; Saretzki, G.; Martin-Ruiz, C.; Lara, J.; Matu, J.; Griffiths, A.; Robinson, N.; Lillà, L.; et al. Mediterranean diet and the hallmarks of ageing. Eur. J. Clin. Nutr. 2021, 75, 1176–1192. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, A.; Barul, C.; Féart, C.; Helmer, C.; Bernard, C.; Periot, O.; Dilharreguy, B.; Dartigues, J.F.; Allard, M.; Barberger-Gateau, P.; et al. Mediterranean diet and preserved brain structural connectivity in older subjects. Alzheimers Dement. 2015, 11, 1023–1031. [Google Scholar] [CrossRef]
- Rodrigues, B.; Coelho, A.; Portugal-Nunes, C.; Magalhães, R.; Moreira, P.S.; Castanho, T.C.; Amorim, L.; Marques, P.; Soares, J.M.; Sousa, N.; et al. Higher Adherence to the Mediterranean Diet Is Associated With Preserved White Matter Integrity and Altered Structural Connectivity. Front. Neurosci. 2020, 14, 786. [Google Scholar] [CrossRef]
- Mosconi, L.; Walters, M.; Sterling, J.; Quinn, C.; McHugh, P.; Andrews, R.E.; Matthews, D.C.; Ganzer, C.; Osorio, R.S.; Isaacson, R.S.; et al. Lifestyle and vascular risk effects on MRI-based biomarkers of Alzheimer’s disease: A cross-sectional study of middle-aged adults from the broader New York City area. BMJ Open 2018, 8, e019362. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Gaynor, A.M.; Cruz, E.; Lee, S.; Gazes, Y.; Habeck, C.; Stern, Y.; Gu, Y. Mediterranean Diet and White Matter Hyperintensity Change over Time in Cognitively Intact Adults. Nutrients 2022, 14, 3664. [Google Scholar] [CrossRef] [PubMed]
- Tuttolomondo, A.; Simonetta, I.; Daidone, M.; Mogavero, A.; Ortello, A.; Pinto, A. Metabolic and Vascular Effect of the Mediterranean Diet. Int. J. Mol. Sci. 2019, 20, 4716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreu-Reinón, M.E.; Chirlaque, M.D.; Gavrila, D.; Amiano, P.; Mar, J.; Tainta, M.; Ardanaz, E.; Larumbe, R.; Colorado-Yohar, S.M.; Navarro-Mateu, F.; et al. Mediterranean Diet and Risk of Dementia and Alzheimer’s Disease in the EPIC-Spain Dementia Cohort Study. Nutrients 2021, 13, 700. [Google Scholar] [CrossRef] [PubMed]
- Lourida, I.; Soni, M.; Thompson-Coon, J.; Purandare, N.; Lang, I.A.; Ukoumunne, O.C.; Llewellyn, D.J. Mediterranean diet, cognitive function, and dementia: A systematic review. Epidemiology 2013, 24, 479–489. [Google Scholar] [CrossRef]
- Shen, J.; Wilmot, K.A.; Ghasemzadeh, N.; Molloy, D.L.; Burkman, G.; Mekonnen, G.; Gongora, M.C.; Quyyumi, A.A.; Sperling, L.S. Mediterranean Dietary Patterns and Cardiovascular Health. Annu. Rev. Nutr. 2015, 35, 425–449. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Brickman, A.M.; Stern, Y.; Habeck, C.G.; Razlighi, Q.R.; Luchsinger, J.A.; Manly, J.J.; Schupf, N.; Mayeux, R.; Scarmeas, N. Mediterranean diet and brain structure in a multiethnic elderly cohort. Neurology 2015, 85, 1744–1751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croll, P.H.; Voortman, T.; Ikram, M.A.; Franco, O.H.; Schoufour, J.D.; Bos, D.; Vernooij, M.W. Better diet quality relates to larger brain tissue volumes: The Rotterdam Study. Neurology 2018, 90, e2166–e2173. [Google Scholar] [CrossRef]
- Staubo, S.C.; Aakre, J.A.; Vemuri, P.; Syrjanen, J.A.; Mielke, M.M.; Geda, Y.E.; Kremers, W.K.; Machulda, M.M.; Knopman, D.S.; Petersen, R.C.; et al. Mediterranean diet, micronutrients and macronutrients, and MRI measures of cortical thickness. Alzheimer’s Dement. 2017, 13, 168–177. [Google Scholar] [CrossRef] [Green Version]
- Gardener, H.; Scarmeas, N.; Gu, Y.; Boden-Albala, B.; Elkind, M.S.; Sacco, R.L.; DeCarli, C.; Wright, C.B. Mediterranean diet and white matter hyperintensity volume in the Northern Manhattan Study. Arch. Neurol. 2012, 69, 251–256. [Google Scholar] [CrossRef] [Green Version]
- Tong, T.Y.N.; Imamura, F.; Monsivais, P.; Brage, S.; Griffin, S.J.; Wareham, N.J.; Forouhi, N.G. Dietary cost associated with adherence to the Mediterranean diet, and its variation by socio-economic factors in the UK Fenland Study. Br. J. Nutr. 2018, 119, 685–694. [Google Scholar] [CrossRef] [Green Version]
- Pastor, R.; Pinilla, N.; Tur, J.A. The Economic Cost of Diet and Its Association with Adherence to the Mediterranean Diet in a Cohort of Spanish Primary Schoolchildren. Int. J. Environ. Res. Public Health 2021, 18, 1282. [Google Scholar] [CrossRef]
- Bonaccio, M.; Iacoviello, L.; de Gaetano, G.; Moli-Sani, I. The Mediterranean diet: The reasons for a success. Thromb. Res. 2012, 129, 401–404. [Google Scholar] [CrossRef]
- Gallaway, P.J.; Miyake, H.; Buchowski, M.S.; Shimada, M.; Yoshitake, Y.; Kim, A.S.; Hongu, N. Physical Activity: A Viable Way to Reduce the Risks of Mild Cognitive Impairment, Alzheimer’s Disease, and Vascular Dementia in Older Adults. Brain Sci. 2017, 7, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sommerlad, A.; Sabia, S.; Singh-Manoux, A.; Lewis, G.; Livingston, G. Association of social contact with dementia and cognition: 28-year follow-up of the Whitehall II cohort study. PLoS Med. 2019, 16, e1002862. [Google Scholar] [CrossRef] [Green Version]
- Titova, O.E.; Ax, E.; Brooks, S.J.; Sjögren, P.; Cederholm, T.; Kilander, L.; Kullberg, J.; Larsson, E.M.; Johansson, L.; Ahlström, H.; et al. Mediterranean diet habits in older individuals: Associations with cognitive functioning and brain volumes. Exp. Gerontol. 2013, 48, 1443–1448. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Bennett, D.A.; Aggarwal, N.T. MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimer’s Dement. 2015, 11, 1007–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karstens, A.J.; Tussing-Humphreys, L.; Zhan, L.; Rajendran, N.; Cohen, J.; Dion, C.; Zhou, X.J.; Lamar, M. Associations of the Mediterranean diet with cognitive and neuroimaging phenotypes of dementia in healthy older adults. Am. J. Clin. Nutr. 2019, 109, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, J.A.; Smith, P.J.; Mabe, S.; Hinderliter, A.; Welsh-Bohmer, K.; Browndyke, J.N.; Lin, P.H.; Kraus, W.; Doraiswamy, P.M.; Burke, J.; et al. Lifestyle and Neurocognition in Older Adults With Cardiovascular Risk Factors and Cognitive Impairment. Psychosom. Med. 2017, 79, 719–727. [Google Scholar] [CrossRef]
- Smith, P.J.; Blumenthal, J.A.; Babyak, M.A.; Craighead, L.; Welsh-Bohmer, K.A.; Browndyke, J.N.; Strauman, T.A.; Sherwood, A. Effects of the dietary approaches to stop hypertension diet, exercise, and caloric restriction on neurocognition in overweight adults with high blood pressure. Hypertension 2010, 55, 1331–1338. [Google Scholar] [CrossRef] [Green Version]
- Wengreen, H.; Munger, R.G.; Cutler, A.; Quach, A.; Bowles, A.; Corcoran, C.; Tschanz, J.T.; Norton, M.C.; Welsh-Bohmer, K.A. Prospective study of Dietary Approaches to Stop Hypertension- and Mediterranean-style dietary patterns and age-related cognitive change: The Cache County Study on Memory, Health and Aging. Am. J. Clin. Nutr. 2013, 98, 1263–1271. [Google Scholar] [CrossRef] [Green Version]
- Tsivgoulis, G.; Judd, S.; Letter, A.J.; Alexandrov, A.V.; Howard, G.; Nahab, F.; Unverzagt, F.W.; Moy, C.; Howard, V.J.; Kissela, B.; et al. Adherence to a Mediterranean diet and risk of incident cognitive impairment. Neurology 2013, 80, 1684–1692. [Google Scholar] [CrossRef] [Green Version]
- Gallucci, M.; Mazzuco, S.; Ongaro, F.; Di Giorgi, E.; Mecocci, P.; Cesari, M.; Albani, D.; Forloni, G.L.; Durante, E.; Gajo, G.B.; et al. Body mass index, lifestyles, physical performance and cognitive decline: The "Treviso Longeva (TRELONG)" study. J. Nutr. Health Aging 2013, 17, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Katsiardanis, K.; Diamantaras, A.A.; Dessypris, N.; Michelakos, T.; Anastasiou, A.; Katsiardani, K.P.; Kanavidis, P.; Papadopoulos, F.C.; Stefanadis, C.; Panagiotakos, D.B.; et al. Cognitive impairment and dietary habits among elders: The Velestino Study. J. Med. Food. 2013, 16, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Crichton, G.E.; Bryan, J.; Hodgson, J.M.; Murphy, K.J. Mediterranean diet adherence and self-reported psychological functioning in an Australian sample. Appetite 2013, 70, 53–59. [Google Scholar] [CrossRef]
- Corley, J.; Starr, J.M.; McNeill, G.; Deary, I.J. Do dietary patterns influence cognitive function in old age? Int. Psychogeriatr. 2013, 25, 1393–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soltani, S.; Chitsazi, M.J.; Salehi-Abargouei, A. The effect of dietary approaches to stop hypertension (DASH) on serum inflammatory markers: A systematic review and meta-analysis of randomized trials. Clin. Nutr. 2018, 37, 542–550. [Google Scholar] [CrossRef]
- Abbatecola, A.M.; Russo, M.; Barbieri, M. Dietary patterns and cognition in older persons. Curr. Opini. Clini. Nutri. Metabol. Care. 2018, 21, 10–13. [Google Scholar] [CrossRef]
- Berendsen, A.A.M.; Kang, J.H.; van de Rest, O.; Feskens, E.J.M.; de Groot, L.C.P.G.M.; Grodstein, F. The Dietary Approaches to Stop Hypertension Diet, Cognitive Function, and Cognitive Decline in American Older Women. J. Am. Med. Dir. Assoc. 2017, 18, 427–432. [Google Scholar] [CrossRef]
- Nishi, S.K.; Babio, N.; Gómez-Martínez, C.; Martínez-González, M.Á.; Ros, E.; Corella, D.; Castañer, O.; Martínez, J.A.; Alonso-Gómez, Á.M.; Wärnberg, J.; et al. Mediterranean, DASH, and MIND Dietary Patterns and Cognitive Function: The 2-Year Longitudinal Changes in an Older Spanish Cohort. Front. Aging Neurosci. 2021, 13, 782067. [Google Scholar] [CrossRef]
- Daniel, G.D.; Chen, H.; Bertoni, A.G.; Rapp, S.R.; Fitzpatrick, A.L.; Luchsinger, J.A.; Wood, A.C.; Hughes, T.M.; Burke, G.L.; Hayden, K.M. DASH diet adherence and cognitive function: Multi-ethnic study of atherosclerosis. Clin. Nutr. ESPEN 2021, 46, 223–231. [Google Scholar] [CrossRef]
- Blumenthal, J.A.; Smith, P.J.; Mabe, S.; Hinderliter, A.; Lin, P.H.; Liao, L.; Welsh-Bohmer, K.A.; Browndyke, J.N.; Kraus, W.E.; Doraiswamy, P.M.; et al. Lifestyle and neurocognition in older adults with cognitive impairments: A randomized trial. Neurology 2019, 92, e212–e223. [Google Scholar] [CrossRef] [Green Version]
- Cherian, L.; Wang, Y.; Fakuda, K.; Leurgans, S.; Aggarwal, N.; Morris, M. Mediterranean-Dash Intervention for Neurodegenerative Delay (MIND) Diet Slows Cognitive Decline After Stroke. J. Prev. Alzheimers Dis. 2019, 6, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Melo van Lent, D.; O’Donnell, A.; Beiser, A.S.; Vasan, R.S.; DeCarli, C.S.; Scarmeas, N.; Wagner, M.; Jacques, P.F.; Seshadri, S.; Himali, J.J.; et al. Mind Diet Adherence and Cognitive Performance in the Framingham Heart Study. J. Alzheimers Dis. 2021, 82, 827–839. [Google Scholar] [CrossRef]
- Boumenna, T.; Scott, T.M.; Lee, J.S.; Zhang, X.; Kriebel, D.; Tucker, K.L.; Palacios, N. MIND Diet and Cognitive Function in Puerto Rican Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2022, 77, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Tao, Y.; Chen, H.; Chen, X.; Shen, J.; Zhao, C.; Xu, X.; He, M.; Zhu, D.; Zhang, R.; et al. Mediterranean-Dietary Approaches to Stop Hypertension Intervention for Neurodegenerative Delay (MIND) Diet and Cognitive Function and its Decline: A Prospective Study and Meta-analysis of Cohort Studies. Am. J. Clin. Nutr. 2023, 118, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Berendsen, A.M.; Kang, J.H.; Feskens, E.J.M.; de Groot, C.P.G.M.; Grodstein, F.; van de Rest, O. Association of Long-Term Adherence to the MIND Diet with Cognitive Function and Cognitive Decline in American Women. J. Nutr. Health Aging 2018, 22, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Adjibade, M.; Assmann, K.E.; Julia, C.; Galan, P.; Hercberg, S.; Kesse-Guyot, E. Prospective association between adherence to the MIND diet and subjective memory complaints in the French NutriNet-Santé cohort. J. Neurol. 2019, 266, 942–952. [Google Scholar] [CrossRef]
- Dhana, K.; James, B.D.; Agarwal, P.; Aggarwal, N.T.; Cherian, L.J.; Leurgans, S.E.; Barnes, L.L.; Bennett, D.A.; Schneider, J.A. MIND Diet, Common Brain Pathologies, and Cognition in Community-Dwelling Older Adults. J. Alzheimers Dis. 2021, 83, 683–692. [Google Scholar] [CrossRef]
- Huang, X.; Aihemaitijiang, S.; Ye, C.; Halimulati, M.; Wang, R.; Zhang, Z. Development of the cMIND Diet and Its Association with Cognitive Impairment in Older Chinese People. J. Nutr. Health Aging 2022, 26, 760–770. [Google Scholar] [CrossRef]
- Arjmand, G.; Abbas-Zadeh, M.; Eftekhari, M.H. Effect of MIND diet intervention on cognitive performance and brain structure in healthy obese women: A randomized controlled trial. Sci. Rep. 2022, 12, 2871. [Google Scholar] [CrossRef]
- Ahn, S.; Lingerfelt, C.N.; Lee, C.E.; Lee, J.A.; Raynor, H.A.; Anderson, J.G. Association of adherence to high-intensity physical activity and the Mediterranean-dietary approaches to stop hypertension intervention for neurodegenerative delay diet with cognition: A cross-sectional study. Int. J. Nurs. Stud. 2022, 131, 104243. [Google Scholar] [CrossRef]
- Wesselman, L.M.P.; van Lent, D.M.; Schröder, A.; van de Rest, O.; Peters, O.; Menne, F.; Fuentes, M.; Priller, J.; Spruth, E.J.; Altenstein, S.; et al. Dietary patterns are related to cognitive functioning in elderly enriched with individuals at increased risk for Alzheimer’s disease. Eur. J. Nutr. 2021, 60, 849–860. [Google Scholar] [CrossRef] [PubMed]
- Calil, S.R.B.; Brucki, S.M.D.; Nitrini, R.; Yassuda, M.S. Adherence to the Mediterranean and MIND diets is associated with better cognition in healthy seniors but not in MCI or AD. Clin. Nutr. ESPEN 2018, 28, 201–207. [Google Scholar] [CrossRef]
- Munoz-Garcia, M.I.; Toledo, E.; Razquin, C.; Dominguez, L.J.; Maragarone, D.; Martinez-Gonzalez, J.; Martinez-Gonzalez, M.A. “A priori” dietary patterns and cognitive function in the SUN project. Neuroepidemiology 2020, 54, 45–57. [Google Scholar] [CrossRef]
- Nabbout, R.; Mazzuca, M.; Hubert, P.; Peudennier, S.; Allaire, C.; Flurin, V.; Aberastury, M.; Silva, W.; Dulac, O. Efficacy of ketogenic diet in severe refractory status epilepticus initiating fever induced refractory epileptic encephalopathy in school age children (FIRES). Epilepsia 2010, 51, 2033–2037. [Google Scholar] [CrossRef] [PubMed]
- Morrill, S.J.; Gibas, K.J. Ketogenic diet rescues cognition in ApoE4+ patient with mild Alzheimer’s disease: A case study. Diabetes Metab. Syndr. 2019, 13, 1187–1191. [Google Scholar] [CrossRef] [PubMed]
- Grammatikopoulou, M.G.; Goulis, D.G.; Gkiouras, K.; Theodoridis, X.; Gkouskou, K.K.; Evangeliou, A.; Dardiotis, E.; Bogdanos, D.P. To Keto or Not to Keto? A Systematic Review of Randomized Controlled Trials Assessing the Effects of Ketogenic Therapy on Alzheimer Disease. Adv. Nutr. 2020, 11, 1583–1602. [Google Scholar] [CrossRef]
- Lin, A.; Turner, Z.; Doerrer, S.C.; Stanfield, A.; Kossoff, E.H. Complications During Ketogenic Diet Initiation: Prevalence, Treatment, and Influence on Seizure Outcomes. Pediatr. Neurol. 2017, 68, 35–39. [Google Scholar] [CrossRef]
- Taylor, M.K.; Swerdlow, R.H.; Burns, J.M.; Sullivan, D.K. An Experimental Ketogenic Diet for Alzheimer Disease Was Nutritionally Dense and Rich in Vegetables and Avocado. Curr. Dev. Nutr. 2019, 3, nzz003. [Google Scholar] [CrossRef] [Green Version]
- Brinkley, T.E.; Leng, I.; Register, T.C.; Neth, B.J.; Zetterberg, H.; Blennow, K.; Craft, S. Changes in Adiposity and Cerebrospinal Fluid Biomarkers Following a Modified Mediterranean Ketogenic Diet in Older Adults at Risk for Alzheimer’s Disease. Front. Neurosci. 2022, 16, 906539. [Google Scholar] [CrossRef]
- Neth, B.J.; Mintz, A.; Whitlow, C.; Jung, Y.; Solingapuram Sai, K.; Register, T.C.; Kellar, D.; Lockhart, S.N.; Hoscheidt, S.; Maldjian, J.; et al. Modified ketogenic diet is associated with improved cerebrospinal fluid biomarker profile, cerebral perfusion, and cerebral ketone body uptake in older adults at risk for Alzheimer’s disease: A pilot study. Neurobiol. Aging 2020, 86, 54–63. [Google Scholar] [CrossRef]
- Nagpal, R.; Neth, B.J.; Wang, S.; Craft, S.; Yadav, H. Modified Mediterranean-ketogenic diet modulates gut microbiome and short-chain fatty acids in association with Alzheimer’s disease markers in subjects with mild cognitive impairment. EBioMedicine 2019, 47, 529–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, M.C.L.; Deprez, L.M.; Mortimer, G.M.N.; Murtagh, D.K.J.; McCoy, S.; Mylchreest, R.; Gilbertson, L.J.; Clark, K.M.; Simpson, P.V.; McManus, E.J.; et al. Randomized crossover trial of a modified ketogenic diet in Alzheimer’s disease. Alzheimers Res. Ther. 2021, 13, 51. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Niu, X.; Peng, D. Eat for better cognition in older adults at risk for Alzheimer’s disease. Nutrition 2023, 109, 111969. [Google Scholar] [CrossRef]
- Fraser, G.E. Vegetarian diets: What do we know of their effects on common chronic diseases? Am. J. Clin. Nutr. 2009, 89, 1607S–1612S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satija, A.; Hu, F.B. Plant-based diets and cardiovascular health. Trends Cardiovasc. Med. 2018, 28, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Dhana, K.; Barnes, L.L.; Tangney, C.C.; Agarwal, P.; Aggarwal, N.; Holland, T.M.; Beck, T.; Evans, D.A.; Rajan, K.B. A healthy plant-based diet was associated with slower cognitive decline in African American older adults: A biracial community-based cohort. Am. J. Clin. Nutr. 2022, 116, 875–886. [Google Scholar] [CrossRef]
- Mottaghi, T.; Amirabdollahian, F.; Haghighatdoost, F. Fruit and vegetable intake and cognitive impairment: A systematic review and meta-analysis of observational studies. Eur. J. Clin. Nutr. 2018, 72, 1336–1344. [Google Scholar] [CrossRef]
- Gatto, N.M.; Garcia-Cano, J.; Irani, C.; Jaceldo-Siegl, K.; Liu, T.; Chen, Z.; Paul, J.; Fraser, G.; Wang, C.; Lee, G.J. Vegetarian Dietary Patterns and Cognitive Function among Older Adults: The Adventist Health Study-2. J. Nutr. Gerontol. Geriatr. 2021, 40, 197–214. [Google Scholar] [CrossRef]
- Tsai, J.H.; Huang, C.F.; Lin, M.N.; Chang, C.E.; Chang, C.C.; Lin, C.L. Taiwanese Vegetarians Are Associated with Lower Dementia Risk: A Prospective Cohort Study. Nutrients 2022, 14, 588. [Google Scholar] [CrossRef]
- Foote, J.A.; Giuliano, A.R.; Harris, R.B. Older adults need guidance to meet nutritional recommendations. J. Am. Coll. Nutr. 2000, 19, 628–640. [Google Scholar] [CrossRef] [Green Version]
- Yeh, T.S.; Yuan, C.; Ascherio, A.; Rosner, B.A.; Blacker, D.; Willett, W.C. Long-term dietary protein intake and subjective cognitive decline in US men and women. Am. J. Clin. Nutr. 2022, 115, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Bakaloudi, D.R.; Halloran, A.; Rippin, H.L.; Oikonomidou, A.C.; Dardavesis, T.I.; Williams, J.; Wickramasinghe, K.; Breda, J.; Chourdakis, M. Intake and adequacy of the vegan diet. A systematic review of the evidence. Clin. Nutr. 2021, 40, 3503–3521. [Google Scholar] [PubMed]
- Neufingerl, N.; Eilander, A. Nutrient Intake and Status in Adults Consuming Plant-Based Diets Compared to Meat-Eaters: A Systematic Review. Nutrients 2021, 14, 29. [Google Scholar] [CrossRef] [PubMed]
- Weikert, C.; Trefflich, I.; Menzel, J.; Obeid, R.; Longree, A.; Dierkes, J.; Meyer, K.; Herter-Aeberli, I.; Mai, K.; Stangl, G.I.; et al. Vitamin and Mineral Status in a Vegan Diet. Dtsch. Ärzteblatt Int. 2020, 117, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Katonova, A.; Sheardova, K.; Amlerova, J.; Angelucci, F.; Hort, J. Effect of a Vegan Diet on Alzheimer’s Disease. Int. J. Mol. Sci. 2022, 23, 14924. [Google Scholar] [CrossRef] [PubMed]
- Tolppanen, A.M.; Solomon, A.; Kulmala, J.; Kåreholt, I.; Ngandu, T.; Rusanen, M.; Laatikainen, T.; Soininen, H.; Kivipelto, M. Leisure-time physical activity from mid- to late life, body mass index, and risk of dementia. Alzheimers Dement. 2015, 11, 434–443.e6. [Google Scholar] [CrossRef] [PubMed]
- Kępka, A.; Ochocińska, A.; Borzym-Kluczyk, M.; Chojnowska, S.; Skorupa, E.; Przychodzeń, M.; Waszkiewicz, N. Healthy Food Pyramid as Well as Physical and Mental Activity in the Prevention of Alzheimer’s Disease. Nutrients 2022, 14, 1534. [Google Scholar] [CrossRef]
- Hoscheidt, S.; Sanderlin, A.H.; Baker, L.D.; Jung, Y.; Lockhart, S.; Kellar, D.; Whitlow, C.T.; Hanson, A.J.; Friedman, S.; Register, T.; et al. Mediterranean and Western diet effects on Alzheimer’s disease biomarkers, cerebral perfusion, and cognition in mid-life: A randomized trial. Alzheimers Dement. 2022, 18, 457–468. [Google Scholar] [CrossRef]
- Féart, C.; Samieri, C.; Rondeau, V.; Amieva, H.; Portet, F.; Dartigues, J.F.; Scarmeas, N.; Barberger-Gateau, P. Adherence to a Mediterranean diet, cognitive decline, and risk of dementia. JAMA 2009, 302, 638–648. [Google Scholar] [CrossRef] [Green Version]
- Hu, E.A.; Wu, A.; Dearborn, J.L.; Gottesman, R.F.; Sharrett, A.R.; Steffen, L.M.; Coresh, J.; Rebholz, C.M. Adherence to Dietary Patterns and Risk of Incident Dementia: Findings from the Atherosclerosis Risk in Communities Study. J. Alzheimers Dis. 2020, 78, 827–835. [Google Scholar] [CrossRef]
- Benus, R.F.; van der Werf, T.S.; Welling, G.W.; Judd, P.A.; Taylor, M.A.; Harmsen, H.J.; Whelan, K. Association between Faecalibacterium prausnitzii and dietary fibre in colonic fermentation in healthy human subjects. Br. J. Nutr. 2010, 104, 693–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Mantrana, I.; Selma-Royo, M.; Alcantara, C.; Collado, M.C. Shifts on Gut Microbiota Associated to Mediterranean Diet Adherence and Specific Dietary Intakes on General Adult Population. Front. Microbiol. 2018, 9, 890. [Google Scholar] [CrossRef] [Green Version]
- Cremonini, A.L.; Caffa, I.; Cea, M.; Nencioni, A.; Odetti, P.; Monacelli, F. Nutrients in the Prevention of Alzheimer’s Disease. Oxid. Med. Cell Longev. 2019, 2019, 9874159. [Google Scholar] [CrossRef] [Green Version]
- Rajaram, S.; Jones, J.; Lee, G.J. Plant-Based Dietary Patterns, Plant Foods, and Age-Related Cognitive Decline. Adv. Nutr. 2019, 10 (Suppl. S4), S422–S436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammar, A.; Trabelsi, K.; Boukhris, O.; Bouaziz, B.; Müller, P.; MGlenn, J.; Bott, N.T.; Müller, N.; Chtourou, H.; Driss, T.; et al. Effects of Polyphenol-Rich Interventions on Cognition and Brain Health in Healthy Young and Middle-Aged Adults: Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 1598. [Google Scholar] [CrossRef] [PubMed]
- Travica, N.; D’Cunha, N.M.; Naumovski, N.; Kent, K.; Mellor, D.D.; Firth, J.; Georgousopoulou, E.N.; Dean, O.M.; Loughman, A.; Jacka, F.; et al. The effect of blueberry interventions on cognitive performance and mood: A systematic review of randomized controlled trials. Brain Behav. Immun. 2020, 85, 96–105. [Google Scholar] [CrossRef]
- Holland, T.M.; Agarwal, P.; Wang, Y.; Leurgans, S.E.; Bennett, D.A.; Booth, S.L.; Morris, M.C. Dietary flavonols and risk of Alzheimer dementia. Neurology 2020, 94, e1749–e1756. [Google Scholar] [CrossRef]
- Ozawa, M.; Shipley, M.; Kivimaki, M.; Singh-Manoux, A.; Brunner, E.J. Dietary pattern, inflammation and cognitive decline: The Whitehall II prospective cohort study. Clin. Nutr. 2017, 36, 506–512. [Google Scholar] [CrossRef] [Green Version]
- Lin, P.Y.; Chiu, C.C.; Huang, S.Y. SUKP A meta-analytic review of polyunsaturated fatty acid compositions in dementia. J. Clin. Psychiatry 2012, 73, 1245–1254. [Google Scholar] [CrossRef]
- Theodore, L.E.; Kellow, N.J.; McNeil, E.A.; Close, E.O.; Coad, E.G.; Cardoso, B.R. Nut Consumption for Cognitive Performance: A Systematic Review. Adv. Nutr. 2021, 12, 777–792. [Google Scholar] [CrossRef]
- Simonetto, M.; Infante, M.; Sacco, R.L.; Rundek, T.; Della-Morte, D. A Novel Anti-Inflammatory Role of Omega-3 PUFAs in Prevention and Treatment of Atherosclerosis and Vascular Cognitive Impairment and Dementia. Nutrients 2019, 11, 2279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulose, S.M.; Miller, M.G.; Scott, T.; Shukitt-Hale, B. Nutritional Factors Affecting Adult Neurogenesis and Cognitive Function. Adv. Nutr. 2017, 8, 804–811. [Google Scholar] [CrossRef] [Green Version]
- Farina, N.; Llewellyn, D.; Isaac, M.G.; Tabet, N. Vitamin E for Alzheimer’s dementia and mild cognitive impairment. Cochrane Database Syst. Rev. 2017, 1, CD002854. [Google Scholar] [PubMed]
- An, Y.; Feng, L.; Zhang, X.; Wang, Y.; Wang, Y.; Tao, L.; Qin, Z.; Xiao, R. Dietary intakes and biomarker patterns of folate, vitamin B6, and vitamin B12 can be associated with cognitive impairment by hypermethylation of redox-related genes NUDT15 and TXNRD1. Clin. Epigenetics 2019, 11, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Setola, E.; Monti, L.D.; Galluccio, E.; Palloshi, A.; Fragasso, G.; Paroni, R.; Magni, F.; Sandoli, E.P.; Lucotti, P.; Costa, S.; et al. Insulin resistance and endothelial function are improved after folate and vitamin B12 therapy in patients with metabolic syndrome: Relationship between homocysteine levels and hyperinsulinemia. Eur. J. Endocrinol. 2004, 151, 483–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Gueant-Rodriguez, R.M.; Quilliot, D.; Sirveaux, M.A.; Meyre, D.; Gueant, J.L.; Brunaud, L. Folate and vitamin B12 status is associated with insulin resistance and metabolic syndrome in morbid obesity. Clin. Nutr. 2018, 37, 1700–1706. [Google Scholar] [CrossRef]
- Wong, S.K.; Chin, K.Y.; Suhaimi, F.H.; Ahmad, F.; Ima-Nirwana, S. Vitamin E As a Potential Interventional Treatment for Metabolic Syndrome: Evidence from Animal and Human Studies. Front. Pharmacol. 2017, 8, 444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, K.; Luo, M.; Wei, S. The Bioprotective Effects of Polyphenols on Metabolic Syndrome against Oxidative Stress: Evidences and Perspectives. Oxid. Med. Cell Longev. 2019, 2019, 6713194. [Google Scholar] [CrossRef] [Green Version]
- Mak, T.N.; Caldeira, S. The Role of Nutrition in Active and Healthy Ageing. for Prevention and Treatment of Age-Related Diseases: Evidence So Far; Publications Office of the European Union: Luxembourg, 2014; Available online: https://publications.jrc.ec.europa.eu/repository/handle/JRC90454 (accessed on 1 April 2023).
- Han, Y.; Li, S.; Zheng, Y. Predictors of nutritional status among community-dwelling older adults in Wuhan, China. Public Health Nutr. 2009, 12, 1189–1196. [Google Scholar] [CrossRef] [Green Version]
- Bloom, I.; Edwards, M.; Jameson, K.A.; Syddall, H.E.; Dennison, E.; Gale, C.R.; Baird, J.; Cooper, C.; Aihie Sayer, A.; Robinson, S. Influences on diet quality in older age: The importance of social factors. Age Ageing 2017, 46, 277–283. [Google Scholar] [CrossRef] [Green Version]
- Host, A.; McMahon, A.T.; Walton, K.; Charlton, K. Factors Influencing Food Choice for Independently Living Older People-A Systematic Literature Review. J. Nutr. Gerontol. Geriatr. 2016, 35, 67–94. [Google Scholar] [CrossRef] [PubMed]
- Aravanis, C.; Corcondilas, A.; Dontas, A.S.; Lekos, D.; Keys, A. Coronary heart disease in seven countries. IX. The Greek islands of Crete and Corfu. Circulation 1970, 41 (Suppl. S4), I88–I100. [Google Scholar] [CrossRef] [PubMed]
- Parrott, M.D.; Shatenstein, B.; Ferland, G.; Payette, H.; Morais, J.A.; Belleville, S.; Kergoat, M.J.; Gaudreau, P.; Greenwood, C.E. Relationship between diet quality and cognition depends on socioeconomic position in healthy older adults. J. Nutr. 2013, 143, 1767–1773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weng, P.H.; Chen, J.H.; Chiou, J.M.; Tu, Y.K.; Chen, T.F.; Chiu, M.J.; Tang, S.C.; Yeh, S.J.; Chen, Y.C. The effect of lifestyle on late-life cognitive change under different socioeconomic status. PLoS ONE 2018, 13, e0197676. [Google Scholar] [CrossRef] [Green Version]
- Whitelock, E.; Ensaff, H. On Your Own: Older Adults’ Food Choice and Dietary Habits. Nutrients 2018, 10, 413. [Google Scholar] [CrossRef] [Green Version]
- Abbott, R.D.; White, L.R.; Ross, G.W.; Masaki, K.H.; Curb, J.D.; Petrovitch, H. Walking and dementia in physically capable elderly men. JAMA 2004, 292, 1447–1453. [Google Scholar] [CrossRef] [Green Version]
- Lenart-Bugla, M.; Łuc, M.; Pawłowski, M.; Szcześniak, D.; Seifert, I.; Wiegelmann, H.; Gerhardus, A.; Wolf-Ostermann, K.; Rouwette, E.A.J.A.; Ikram, M.A.; et al. What Do We Know about Social and Non-Social Factors Influencing the Pathway from Cognitive Health to Dementia? A Systematic Review of Reviews. Brain Sci. 2022, 12, 1214. [Google Scholar] [CrossRef]
- Jaqua, E.; Biddy, E.; Moore, C.; Browne, G. The Impact of the Six Pillars of Lifestyle Medicine on Brain Health. Cureus 2023, 15, e34605. [Google Scholar] [CrossRef]
- De la Rosa, A.; Olaso-Gonzalez, G.; Arc-Chagnaud, C.; Millan, F.; Salvador-Pascual, A.; García-Lucerga, C.; Blasco-Lafarga, C.; Garcia-Dominguez, E.; Carretero, A.; Correas, A.G.; et al. Physical exercise in the prevention and treatment of Alzheimer’s disease. J. Sport Health Sci. 2020, 9, 394–404. [Google Scholar] [CrossRef]
- Laurin, D.; Verreault, R.; Lindsay, J.; MacPherson, K.; Rockwood, K. Physical activity and risk of cognitive impairment and dementia in elderly persons. Arch. Neurol. 2001, 58, 498–504. [Google Scholar] [CrossRef] [Green Version]
- Sofi, F.; Valecchi, D.; Bacci, D.; Abbate, R.; Gensini, G.F.; Casini, A.; Macchi, C. Physical activity and risk of cognitive decline: A meta-analysis of prospective studies. J. Intern. Med. 2011, 269, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Mamalaki, E.; Anastasiou, C.A.; Kosmidis, M.H.; Dardiotis, E.; Hadjigeorgiou, G.M.; Sakka, P.; Scarmeas, N.; Yannakoulia, M. Social life characteristics in relation to adherence to the Mediterranean diet in older adults: Findings from the Hellenic Longitudinal Investigation of Aging and Diet (HELIAD) study. Public Health Nutr. 2020, 23, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Corsi, M.; Di Raimo, T.; Di Lorenzo, C.; Rapp-Ricciardi, M.; Archer, T.; Ricci, S.; Businaro, R. Cognitive disability in alzheimer’s disease and its management. Clin. Ter. 2016, 167, e123–e126. [Google Scholar] [PubMed]
Figure 1.
Preventive and ameliorative effects of dietary patterns against ADRD. Long-term adherence to prudent dietary patterns (left-side panel), in conjunction with a healthy lifestyle, may prevent ADRD via antioxidant/anti-inflammatory mechanisms and positive microbiome modulation, which are associated with lower predisposition to aging-associated neuroinflammation and insulin resistance, leading to improved lifestyle, cognitive abilities, and overall quality of life. Specific dietary patterns (right-side panel) may also ameliorate ADRD via different mechanisms, such as antioxidant/anti-inflammatory/microbiome-modulatory, attributed to specific macro- and micronutrients in these dietary patterns. ADRD: Alzheimer’s disease and related dementias; DASH: Dietary Approaches to Stop Hypertension dietary pattern; MIND: Mediterranean-DASH Intervention for Neurodegenerative Delay dietary patterns; ↑ higher; ↓ lower.
Figure 1.
Preventive and ameliorative effects of dietary patterns against ADRD. Long-term adherence to prudent dietary patterns (left-side panel), in conjunction with a healthy lifestyle, may prevent ADRD via antioxidant/anti-inflammatory mechanisms and positive microbiome modulation, which are associated with lower predisposition to aging-associated neuroinflammation and insulin resistance, leading to improved lifestyle, cognitive abilities, and overall quality of life. Specific dietary patterns (right-side panel) may also ameliorate ADRD via different mechanisms, such as antioxidant/anti-inflammatory/microbiome-modulatory, attributed to specific macro- and micronutrients in these dietary patterns. ADRD: Alzheimer’s disease and related dementias; DASH: Dietary Approaches to Stop Hypertension dietary pattern; MIND: Mediterranean-DASH Intervention for Neurodegenerative Delay dietary patterns; ↑ higher; ↓ lower.

Table 2.
A summary of clinical studies examining DASH diet impact on ADRD.
| Study Design | Country | Population | Follow-Up | Exposure | Outcome | Results | Covariates | Reference |
|---|---|---|---|---|---|---|---|---|
| Longitudinal | US | Older adults in CCMS study aged over 65 years n = 3580 | 10.6 years | 142-item FFQ, MeDi score, DASH score Global cognition (3 MS) | Associations between DASH and Mediterranean-style dietary patterns and age-related cognitive change. | Higher quintile compared to lower one of DASH score associated with better average cognition but not significantly associated with rate of change in cognitive function. | Age, gender, education, BMI, frequency of moderate physical activity, multivitamin and mineral supplement use, history of drinking and smoking, and history of diabetes, heart attack, or stroke. | [104] |
| Longitudinal | US | Older participants of Memory and Aging Project cognitively normal at enrollment n = 826 (26% M) Age: 81.5 ± 7.1 years | 4.1 years | 144-item FFQ, battery of cognitive tests: episodic memory, semantic memory, working memory, perceptual speed, and visuospatial ability | Association between DASH and Mediterranean diets with slower cognitive decline. | In models adjusted for covariates, a 1-unit increase in DASH score associated with slower rate of global cognitive decline, with a decrease of 0.007 standardized units. | Age, gender, education, participation in cognitive activities, total energy intake (kcal), time, and the interaction between time and each covariate, physical activity, presence of APOE ε4 allele, depression, hypertension, diabetes, and stroke. | [58] |
| Longitudinal | US | Participants of the Rush Memory and Aging Project (MAP) n = 923 (±24% M) Age: 58–98 years | 4.5 years | 144-item SFFQ, A-MeDi, -DASH, and MIND scores, AD (based on NINCDS-ADRDA criteria) | Association of MIND, a hybrid Mediterranean and DASH diet, with incident AD. | The highest tertile of DASH diet adherence significantly associated with lower risk of AD. | Age, gender, education, presence of APOE ε4 allele, participation in cognitively stimulating activities, physical activity, total energy intake, and cardiovascular conditions. | [100] |
| Longitudinal | US | Postmenopausal women enrolled in the Women’s Health Initiative Memory Study (WHIMS) n = 6425 (0% M) Age: 65–79 years | 9.11 years | FFQ, A-MeDi score, DASH score, MCI (MMSE and battery of neuropsychological tests) | Dietary patterns associated with cognitive decline in older women. Dietary patterns modified cognitive decline risk for women with hypertension. | Higher quintile of DASH score significantly associated with lower risk of MCI. | Age, race, education level, Women Health Initiative hormone trial randomization assignment, baseline 3 MS level, smoking status, physical activity, diabetes, hypertension, BMI, family income, depression, history of CVD, and total energy intake. | [73] |
| Longitudinal | US | Participants from Nurses’ Health Study, n = 16,144 Age: at first cognitive assessment, 74.3 ± 2.3 years | 4.1 years | 116-item SFFQ, DASH, global cognition, and verbal memory (immediate and delayed recalls) | Association between long-term adherence to DASH diet and cognitive function and decline in older American women. | Higher long-term adherence to DASH diet associated with better average global cognition, verbal memory, and TICS, but not with change in global cognition, verbal memory, or TICS score during follow-up. | Age, education, physical activity, caloric intake, alcohol intake, smoking status, multivitamin use, BMI, history of depression, high blood pressure, hypercholesterolemia, myocardial infarction, and diabetes mellitus. | [112] |
| Longitudinal | Sweden | Older community participants n = 2223 (39% men) Age: 69.5 years | 6 years | 98-item SFFQ, A-MedD, A-DASH and MIND scores, dietary components, global cognition (MMSE) | Comparison of association of the different dietary patterns with cognitive decline in an older Scandinavian population. | DASH score not associated with cognitive decline nor with risk of MMSE score ≤ 24. | Age, gender, education, civil status, total caloric intake, BMI, physical activity, smoking, vitamin/mineral supplement intake, vascular disorders, diabetes, cancer, depression, presence of APOE ε4 allele, and dietary components other than those included in each dietary index. | [41] |
| Longitudinal | Spain | Participants in PREDIMED-Plus trial n = 6647 (52% men) Age: 65 years | 2 years | 143-item FFQ, MedD, DASH diet and MIND diet scoring, battery of cognitive tests: MMSE, visuospatial and visuo-constructive capacity, verbal ability and executive function, short-term and working memory | Relationship between baseline adherence to MedD, DASH, and MIND diets with 2-year changes in cognitive performance in older adults with overweight or obesity and high cardiovascular disease risk. | Higher adherence to DASH diet not associated with better cognitive function over 2 years. | Age, gender, education level, and civil status, physical activity, dietary intake, and smoking habit, BMI, personal history of hypertension, hypercholesterolemia, type 2 diabetes, and depression. | [113] |
| Longitudinal | US | Participants in MESA cohort from six communities n= 4169 (1965 M 2204 F) Age: 60.4 ± 9.5 years | 2 years | 120-item FFQ, cognitive function assessment by Cognitive Abilities Screening Instrument (CASI), Digit Symbol Coding (DSC), and Digit Span (DS) | Association between DASH diet and cognitive function in MESA cohort. | DASH diet adherence not associated with cognitive performance or any decline. | Age, gender, race/ethnicity, education, income, acculturation status, presence of APOE ε4 allele, total energy intake, BMI, smoking, Center for Epidemiological Studies Depression (CES-D) scale score, total intentional exercise, diabetes categories, diabetes medication use, antihypertensive medication use, Alzheimer’s medication use, stroke diagnosis, hypertension, use of antihypertensive medications, alcohol intake. | [114] |
| Cross-sectional | US | Sedentary adults with cognitive impairment and CVD risk factors n = 160 (33% men) Age: 65.4 years | NS | FFQ and 4-day food diary, A-MedD and A-DASH scores, verbal memory, visual memory, and executive function/processing speed score | The relationship of lifestyle factors and neurocognitive functioning in older adults with vascular risk factors and cognitive impairment, no dementia. | Higher adherence to DASH diet associated with better verbal memory, but not with executive function/processing speed or visual memory. | Age, education, gender, ethnicity, total caloric intake, family history of dementia, and chronic use of anti-inflammatory medications. | [102] |
| Randomized controlled trial | US | Sedentary older adults n = 160 Aerobic Exercise (AE) + DASH group, n = 40 (14 M 26 F), Age: 64.9 ± 6.2 years AE no DASH, n = 41 (12 M 29 F), Age: 65.8 ± 7.3 years DASH group, n = 41 (15 M 26 F), Age: 66.0 ± 7.1 years HE: Health Education group, n = 38 (12 M 16 F), Age: 64.7 ± 6.6 years | 6 months | FFQ, DASH diet score, battery of tests: executive function, global executive function, cognitive and functional performance | Evaluation of independent and additive effects of AE and DASH diet on executive functioning in adults with cognitive impairments with no dementia. | Participants engaged in AE but not DASH diet demonstrated significant improvements in executive function. Combined AE and DASH diet associated with the largest improvements compared to receiving HE. | NS | [115] |
Adapted from [20] and updated. AD: Alzheimer’s disease; APOE: apolipoprotein E; BMI: body mass index; CVD: cardiovascular disease; FFQ: Food Frequency Questionnaire; MedD: Mediterranean diet; MMSE: Mini-Mental State Examination; SFFQ: semi-quantitative food frequency questionnaire; TICS: Telephone Interview for Cognitive Status; 3 MS: Modified Mini-Mental State Examination.
Table 3.
A summary of clinical studies examining MIND diet impact on ADRD.
| Study Design | Country | Population | Follow-Up | Exposure | Outcome | Results | Covariates | Reference |
|---|---|---|---|---|---|---|---|---|
| Longitudinal | US | Older adults n = 923 (±24% men) Age: 58–98 years | 4.5 years | 144-item SFFQ, A-MeDi, A-DASH, and MIND scores | AD (based on NINCDS-ADRDA criteria) | Middle and high tertiles of MIND diet score significantly associated with lower risk of AD. | Age, gender, education, presence of APOE ε4 allele, participation in cognitively stimulating activities, physical activity, total energy intake, and cardiovascular conditions. | [100] |
| Longitudinal | US | Older adults n = 960 (25% men) Age: 81.4 years | 4.7 years | 144-item SFFQ, MIND diet score | Global cognition, episodic memory, semantic memory, visuospatial ability, perceptual speed, and working memory | MIND diet score significantly associated with slower ↘ in global cognition; episodic memory; semantic memory; visuospatial ability; perceptual speed; and working memory. Higher tertile of MIND diet score significantly associated with slower ↘ in global cognitive score. | Age, gender, education, participation in cognitive activities, smoking history, physical activity hours per week, total energy intake, presence of APOE ε4 allele, time, history of stroke, myocardial infarction, diabetes, hypertension, and interaction terms between each covariate and time). | [100] |
| Longitudinal | Sweden | Older-adult community residents n = 2223 (39% men) Age: 69.5 years | 6 years | 98-item SFFQ, A-MeDi, A-DASH, and MIND scores, dietary components | Global cognition (MMSE) | Higher MIND score significantly associated with less cognitive decline and lower risk of MMSE score ≤ 24. | Total caloric intake, age, gender, education, civil status, physical activity, smoking, BMI, vitamin/mineral supplement intake, vascular disorders, diabetes, cancer, depression, presence of APOE ε4 allele, and dietary components other than main exposure in each model. | [41] |
| Longitudinal | US | Older women n = 16,058 (0% men) Age: 74.3 years | 12.9 years | 116-item FFQ, MIND score | Global cognition (TICS and composite score of TICS, EBMT) and verbal memory (immediate and delayed recalls). | Higher adherence to MIND diet not significantly associated with less ↘ in global cognition, verbal memory, or TICS score. | Age, education, physical activity, caloric intake, alcohol intake, smoking status, multivitamin use, BMI, depression, and history of hypertension, hypercholesterolemia, myocardial infarction, and diabetes mellitus. | [120] |
| Longitudinal | Australia | Older Australian adults n = 1220 (50% men) Age: 60–64 years | 12 years | CSIRO-FFQ, MeDi, A-MeDi, and MIND scores, dietary components | Cognitive impairment: MCI/dementia | Higher tertile of MIND score significantly associated with a lower risk of cognitive impairment. | Energy intake, age, gender, presence of APOE ε4 allele, education, mental activity, physical activity, smoking status, depression, diabetes, BMI, hypertension, heart disease, and stroke. | [74] |
| Longitudinal | US | Older adults with clinical history of stroke n = 106 (29 M 77 F) Age: 82.8 ± 7.1 years | 5.9 years | 144-item FFQ, neuropsychologic battery of tests/global cognitive decline: episodic memory, semantic memory, working memory, perceptual orientation, perceptual speed | Determination of whether the MIND diet is effective in preventing cognitive decline after stroke | Higher tertile compared with lowest one of MIND diet scores had slower rate of global cognitive ↘ and slower ↘ in semantic memory and perceptual speed. In continuous models, MIND diet associated with slower ↘ in cognitive function for global cognition and semantic memory. | Age, gender, education, total energy intake, presence of APOE ε4 allele, smoking, participation in cognitive and physical activities, depressive symptoms, BMI, chronic diseases. | [116] |
| Longitudinal | US | Population WRAP study n = 828 (268 M 560 F) Age: 57.7 ± 6.4 years, free of dementia and MCI at baseline | 6.3 years | 15-item questionnaire, neuropsychological battery of tests/ multidomain cognitive composite: immediate memory, delayed memory, executive function | Effect of MIND diet on multidomain cognitive composite and immediate/delayed memory and executive function composites | Higher MIND diet scores associated with slower ↘ in executive function. MIND diet not associated with PACC4, immediate memory, or delayed memory. | Age, gender, presence of APOE ε4 allele, cognitive activity, physical activity, education. | [117] |
| Longitudinal | Germany | Older adults from DELCODE study n= 389 (187 M 202 F), free of dementia Age: 69.4 ± 5.6 years Subjective Cognitive Decline group (SCD): n = 146 MCI group: n = 60 First-degree relatives of AD dementia patients: n = 35 Healthy controls: n = 148 | NS | 148-item FFQ neuropsychological battery of tests and MMSE tool/cognitive function: memory, language (verbal fluency), executive functioning, working memory, visuospatial functioning | Associations between dietary patterns and cognitive functioning in older adults free of dementia | Higher MIND diet score associated with better memory in total subjects and language functions in cognitively normal subjects. MIND diet not associated with executive functioning, working memory, or visuospatial functioning. | Age, gender, education, BMI, physical activity, smoking, total daily energy intake, presence of APOE ε4 allele. | [126] |
| Longitudinal | US | Decedent participants from Rush Memory and Aging Project (MAP) n = 569 (70% F), age at death 91 years | NS | Dietary data, cognitive testing proximate to death, and complete autopsy data at the time of the analyses | Examination of whether the association of MIND diet with cognition is independent of common brain pathologies | Higher MIND diet score associated with better global cognitive functioning proximate to death, even after adjustment for AD and other brain pathologies. MIND diet–cognition relationship remained significant when analysis restricted to individuals without MCI at baseline or postmortem diagnosed with AD. | Age at death, gender, years of education, presence of APOE ε4 allele, cognitive activities, and total energy intake. | [121] |
| Cross-sectional | US | Community-dwelling adults n = 5907 (40% men) Age: 67.8 years | NS | 163-item SFFQ, A-MeDi score, MIND diet score | Cognitive performance: immediate and delayed recall, backward counting, and serial seven subtraction | Higher MIND diet scores associated with slower ↘ in executive function. MIND diet not associated with PACC4, immediate memory, or delayed memory. | Gender, age, race, low education attainment, current smoking, obesity, total wealth, hypertension, diabetes mellitus, physical inactivity, depression, and total energy intake. | [65] |
| Cross-sectional | Brazil | Senior participants with different cognition Control: n = 36 (7 M 29 F) Age ≥ 75 years 12% MCI: n = 30 (9 M 21 F) Age ≥ 75 years 50% AD: n = 30 (11 M 19 F) Age ≥ 75 years 63.3% | NS | 98-item FFQ, neuropsychiatric battery of tests and MMSE tool/ cognitive performance: naming, incidental memory, immediate memory, learning, delayed recall and recognition | Impact of MIND diet adherence on cognitive performance for different cognitive profiles seniors | Moderate adherence to MIND diet associated with higher MMSE scores. High adherence to MIND diet associated with learning score in healthy older adults but not in MCI or AD. No association between the other cognitive variables and the MIND score. | Age, education, income, marital status, BMI, chronic diseases, having undergone nutritional care, motor or sensory impairments. | [127] |
| Cross-sectional | China | Older adults from the Chinese Longitudinal Healthy Longevity Study n = 11,245 (45.3% M) Age: 84.06 ± 11.46 years | 2 to 3 years | 12-items FFQ, Chinese MIND (cMIND)diet score | Cognitive impairment and IADL disability | Moderate and high adherence to cMIND diet associated with lower likelihood of cognitive impairment (higher MMSE score) and IADL disability, even after adjusting for covariates. Higher cMIND diet score associated with better cognitive function and IADL. | Age, gender, residence, education, BMI, diabetes, hearing impairment, hypertension, depression, smoking, drinking, exercise, and social engagement. | [123] |
| Cross-sectional | US | Data from University of Michigan Health and Retirement Study n = 3463 Age: 68.0 ± 10.0 years | NS | 163-item FFQ, MIND diet scores, episodic memory (im- mediate and delayed recall), working memory, attention/processing speed | Association of combination of high-intensity physical activity (PA) and MIND diet with better cognition compared with PA or MIND diet alone or neither | MIND diet alone associated with better global cognition and lower likelihood of cognitive decline. Combining PA and MIND diet predicted better global cognition and lower likelihood of cognitive decline, but did not predict lower odds of cognitive decline compared to PA alone. | Age, gender, race, education, annual income, smoking history, hypertension, diabetes mellitus, depression, and obesity. | [125] |
| Randomized controlled trial | Iran | Healthy obese women (MMSE = 24) n = 37 MIND group: n = 22 Age 48.95 ± 1.07 years Control group: n = 15 Age 48.86 ± 1.56 years | 3 months | 168-item FFQ and 3-day food recall, neuropsychological test battery and MMSE tool/verbal short memory, working memory, attention and visual scanning, verbal recognition memory, executive function and task switching, ability to inhibit cognitive interference | Impact of 3 months MIND diet on body composition and cognition | MIND group compared with control had improved working memory, verbal recognition memory, and attention. ↗ in the surface area of inferior frontal gyrus in MIND diet group. | Pregnancy, metabolic complications, severe untreated medical, neurological, psychiatric diseases, or gastrointestinal problems. | [124] |
| Prospective cohort | Spain | Older adults from “Seguimiento Universidad de Navarra” n= 806 (562 M 244 F) without cognitive impairment at baseline Age: 61 ± 6 years | 6 ± 3 years | 136-item FFQ, telephone-based interview of MMSE/Spanish TICS (orientation, memory, attention/calculation, and language) | Compare association of dietary patterns with cognitive function | Higher adherence to MIND diet associated with upward 6-year changes in Spanish TICS scores. Each 1-point ↗ in the MIND score ↗ Spanish TICS score by 0.27 points. In adjusted linear mixed model, MIND diet score associated with 0.038 rate of change in STICS scores over 5.6 years. | Age, gender, presence of APOE ε4 allele, smoking, education, total energy intake, physical activity, BMI, alcohol intake, depression, chronic diseases, high cholesterol, low HDL cholesterol. | [128] |
| Prospective cohort | France | Older Adults in NutriNet-Santé n = 6011 (2384 M 3627 F) without SMC at enrollment | 6 years | FFQ, SMC measured with French version of the validated self-administered cognitive difficulties scale | Impact of MIND diet adherence on SMC | MIND diet score not significantly associated with SMC in adults aged 60–69 years. Adherence to MIND diet for >70 years without depressive symptoms associated with SMC. One-point increase in MIND diet score associated with 14% ↘ in SMC risk. | Age, gender, marital status, education, occupation, smoking, income, BMI, physical activity, depressive symptoms, chronic diseases, energy intake. | [121] |
| Prospective cohort | US | Older population of Framingham Heart Study n = 2092 (956 M 1036 F) Age: 61 ± 9 years | 6.6 ± 1.1 years | FFQ, neuropsychological testing, and brain MRI scans (n = 1904). | Association between the MIND diet and measures of brain volume, silent brain infarcts (SBIs), or brain atrophy in the community-based Framingham Heart Study | Higher MIND diet scores associated with better global cognitive function, verbal memory, visual memory, processing speed, and verbal comprehension/reasoning and with larger total brain volume following adjustments. Higher MIND diet scores not associated with other brain MRI measures or cognitive decline. | Age, gender, presence of APOE ε4 allele, total energy intake, education, the time interval between completion of the FFQ and the measurement of the neuropsychological and MRI outcomes, BMI, physical activity, smoking status, cardiometabolic factors, and high level of depressive symptoms. | [117] |
| Cross-sectional and longitudinal | US | Adults from Boston Puerto Rican Health Study n= 1502 (378 M 1124 F) Age: 45–75 years at baseline | 8 years | FFQ over 5-year follow-ups, neuropsychological tests, MMSE | Association between long-term adherence to MIND diet and cognitive function in Puerto Rican adults | In cross-sectional and longitudinal analyses, the highest compared to lowest MIND quintile associated with better cognition function, but not with cognitive trajectory over 8 years. | Income-to-poverty ratio, education level, and job complexity score. | [118] |
| Longitudinal study and meta-analysis | China | Participants from the China Health and Nutrition Survey (CHNS) n = 4066 participants Meta-analysis: results from the longitudinal study and 7 other MIND diet and cognitive effect studies n = 26,103 | 3-day 24 h dietary recall, battery of cognitive tests, immediate and delayed recall memory, attention, and calculation abilities | Median 3 years | Relationship between MIND diet and cognitive function and its decline among middle-aged and older adults | Higher MIND diet scores were significantly associated with better global cognitive function. Each increment of 3 points in MIND diet score has adjusted difference in global cognitive function z-score approximately equivalent to being one year younger in age. In the meta-analysis of 26,103 participants, 1 standardized deviation MIND score increment associated with 0.042-unit higher global cognitive function z-score and 0.014-unit slower annual cognitive decline. | Age, gender, education, annual household income per capita, residence, region, smoking, alcohol drinking, BMI, total energy intake, physical activity, history of chronic diseases included self-reported hypertension, diabetes, and myocardial infarction diagnosis, and use of antihypertensive and anti-diabetic medications. | [119] |
Adapted from [20] and updated. AD: Alzheimer’s disease; APOE: apolipoprotein E; BMI: body mass index; CSIRO-FFQ: Commonwealth Scientific and Industrial Research Organization semi-quantitative food frequency questionnaire; EBMT: East Boston Memory Test; FFQ: Food Frequency Questionnaire; HDL: High-Density Lipoprotein; IADL: Instrumental Activities of Daily Living; MCI: mild cognitive impairment; MMSE: Mini-Mental State Examination; MRI: Magnetic Resonance Imaging; PA: high-intensity physical activity; PACC4: Preclinical Alzheimer’s Cognitive Composite 4; SBI: silent brain infarcts; SFFQ: semi-quantitative food frequency questionnaire; SMC: subjective memory complaints; TICS: Telephone Interview for Cognitive Status; ↘: decline; ↗: increase.
Table 4.
A summary of clinical studies examining modified Mediterranean-ketogenic diet impact on ADRD.
Table 4.
A summary of clinical studies examining modified Mediterranean-ketogenic diet impact on ADRD.
| Study Design | Country | Population | Follow-Up | Exposure | Outcome | Results | Covariates | Reference |
|---|---|---|---|---|---|---|---|---|
| Randomized, double-blind, crossover single-center pilot study | US | n = 17 Age: 64.6 ± 6.4 years Participants with MCI n = 11 Participants with normal cognitive function n = 6 | 6-week interventions: MMKD and AHA diet separated by 6-week washout | Gut microbiome, fecal short-chain fatty acids, markers of AD in cerebrospinal fluid | Change in gut microbial signature, fecal short-chain fatty acids, and AD biomarkers after each diet intervention. | MMKD associated with improved metabolic indices and AD biomarkers in CSF profile. | NS | [136] |
| Randomized crossover trial | US | Participants with MCI n= 9 (3 M 6 F) Age: 63.4 ± 4.0 years Participants with SMC n= 11 (2 M 9 F) Age: 64.9 ± 7.9 years | MMKD diet and AHA diet for 6 weeks followed by 6-week washout | Immediate and delayed memory, general cognition, plasma biomarkers, CSF biomarkers, and MRI | Compare effects of MMKD and AHA diet on AD biomarkers in CSF, neuroimaging measures, peripheral metabolism, and cognition. | MMKD associated with ↗ CSF Ab42 and ↘ t-tau. | Age, presence of APOE ε4 allele, and order of diet intervention. | [135] |
| Randomized controlled trial | New Zealand | Participants with diagnosed AD n= 26 (16 M 10 F) Age: 69.8 ± 6.0 years | 12-week intervention and 10-week washout, low-fat diet and MMKD | FFQ, cognition by ACE-III, daily function by ADCS-ADL, quality of life by QOL-AD | Change in cognition, daily function, or quality of life in AD patients after 12 weeks of MMKD. | Improvement in cognitive function, everyday functioning, and quality of life for MMKD group participants compared with the low-fat diet ones. | NS | [137] |
| Crossover trial | US | Participants with MCI n = 9 (3 M 6 F) Age: 63.4 ± 4.0 Participants with SMC n = 11 (2 M 9 F) Age: 64.9 ± 7.89 years | MMKD and AHA diet for 6 weeks with a 6-week washout period | Dual-energy X-ray absorptiometry for adiposity and CSF biomarkers | Effects of MMKD compared to AHA diet on body weight, body composition, and body fat distribution and their association with AD biomarkers in CSF. | ↘ in body fat on the MMKD related to changes in Aβ biomarkers. | Age and diet order | [134] |
ACE-III: Addenbrookes Cognitive Examination-III; ADCS-ADL: Alzheimer’s Disease Cooperative Study—Activities of Daily Living; AD: Alzheimer’s disease; AHA: American Heart Association; APOE: apolipoprotein E; CSF: cerebrospinal fluid; MCI: mild cognitive impairment; MMKD: modified Mediterranean-ketogenic diet; MRI: Magnetic Resonance Imaging; PET: Positron Emission Tomography; SCFA: short-chain fatty acids; SMC: subjective memory complaints; QOL-AD: Quality of Life in Alzheimer’s Disease questionnaire; ↘: decline; ↗: increase.
Table 5.
A summary of clinical studies examining vegetarian diet impact on ADRD.
| Study Design | Country | Population | Follow-Up | Exposure | Outcome | Results | Covariates | Reference |
|---|---|---|---|---|---|---|---|---|
| NS | US and Canada | Vegetarian, n= 72 (32 M 40 F) (62 white, 10 non-white) Age: 76.6 ± 8.3 years Non-vegetarian, n = 60 (24 M 36 F) (44 white, 16 non-white) Age: 73.5 ± 7.7 years | 10 years | FFQ, historic dietary habits survey instrument | Verbal learning, memory, attention, processing speed, executive function, visuospatial abilities, language, global cognitive functioning, MMSE, AMNART, and GDS | Vegetarian diet not associated with lower mild memory impairment likelihood. More stable diet associated with better memory/language. | Age, education | [143] |
| Prospective cohort study | Taiwan | Buddhist Tzu Chi Foundation volunteers Non-vegetarian, n = 3154 (1345 M 1809 F) Age: 57.8 ± 6.3 years Vegetarian, n = 1737 (461 M 1276 F) Age: 58.1 ± 6.5 years | Average 9.2 years | Baseline questionnaires to assess dietary pattern, overall plant-based diet index | MCI and dementia diagnosis | Vegetarians associated with less risk of dementia compared with non-vegetarians after adjusting for covariates. | Gender, age, smoking, drinking, education level, marital status, regular exercise, comorbidities | [144] |
| Longitudinal | US | n = 3337 (1200 M 2137 F) Age: 73.7 ± 5.72 years African American (AA), n = 2012; white, n = 1325 | NS | FFQ | Episodic memory, perceptual speed, and MMSE | ↗ plant-based diet associated with slower ↘ in GC, PS, and EM in AA but not in white participants. AA in the highest quintile of high plant-based diet had significantly slower rates of GC, PS, and EM than individuals in the lowest quintile. | Age, gender, presence of apolipoprotein E4 (APOE ε4) allele, lifestyle factors (education, cognitive activities, smoking, calorie intake, risk factors for cardiovascular disease, time and interaction time × each covariate) | [141] |
AMNART: American National Adult Reading Test; APOE: apolipoprotein E; EM: episodic memory; FFQ: Food Frequency Questionnaire; GC: global cognition; GDS: Geriatric Depression Scale; MCI: mild cognitive impairment; MMSE: Mini-Mental State Examination; NS: not specified; PS: perceptual speed; VIQ: estimated verbal intelligence; ↘: decline; ↗: increase.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ellouze, I.; Sheffler, J.; Nagpal, R.; Arjmandi, B. Dietary Patterns and Alzheimer’s Disease: An Updated Review Linking Nutrition to Neuroscience. Nutrients 2023, 15, 3204. https://doi.org/10.3390/nu15143204
AMA Style
Ellouze I, Sheffler J, Nagpal R, Arjmandi B. Dietary Patterns and Alzheimer’s Disease: An Updated Review Linking Nutrition to Neuroscience. Nutrients. 2023; 15(14):3204. https://doi.org/10.3390/nu15143204
Chicago/Turabian StyleEllouze, Ines, Julia Sheffler, Ravinder Nagpal, and Bahram Arjmandi. 2023. "Dietary Patterns and Alzheimer’s Disease: An Updated Review Linking Nutrition to Neuroscience" Nutrients 15, no. 14: 3204. https://doi.org/10.3390/nu15143204
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.