
Dietary Patterns Associated with Abnormal Glucose Tolerance following Gestational Diabetes Mellitus: The MyNutritype Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Dietary Assessment
2.3. Diagnosis of Abnormal Glucose Tolerance
2.4. Other Variables
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 2. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes—2023. Diabetes Care 2023, 46, S19–S40. [Google Scholar] [CrossRef]
- Buchanan, T.A.; Xiang, A.H.; Page, K.A. Gestational Diabetes Mellitus: Risks and Management during and after Pregnancy. Nat. Rev. Endocrinol. 2012, 8, 639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nouhjah, S.; Shahbazian, H.; Shahbazian, N.; Jahanshahi, A.; Jahanfar, S.; Cheraghian, B. Incidence and Contributing Factors of Persistent Hyperglycemia at 6–12 Weeks Postpartum in Iranian Women with Gestational Diabetes: Results from LAGA Cohort Study. J. Diabetes Res. 2017, 2017, 9786436. [Google Scholar] [CrossRef] [PubMed]
- Jang, E.H.; Kwon, H.S. β-Cell Dysfunction and Insulin Resistance in Gestational Glucose Intolerance. Korean J. Intern. Med. 2013, 28, 294–296. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Newton, K.M.; Knopp, R.H. Gestational diabetes and the incidence of type 2 diabetes: A systematic review. Diabetes Care 2002, 25, 1862–1868. [Google Scholar] [CrossRef] [Green Version]
- Kramer, C.K.; Campbell, S.; Retnakaran, R. Gestational diabetes and risk of cardiovascular disease in women: A systematic review and meta-analysis. Diabetologia 2019, 62, 905–914. [Google Scholar] [CrossRef] [Green Version]
- Matheus, A.S.D.M.; Tannus, L.R.M.; Cobas, R.A.; Palma, C.C.S.; Negrato, C.A.; Gomes, M.D.B. Impact of Diabetes on Cardiovascular Disease: An Update. Int. J. Hypertens. 2013, 2013, 653789. [Google Scholar] [CrossRef] [Green Version]
- Li, N.; Yang, Y.; Cui, D.; Li, C.; Ma, R.C.W.; Li, J.; Yang, X. Effects of lifestyle intervention on long-term risk of diabetes in women with prior gestational diabetes: A systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2021, 22, e13122. [Google Scholar] [CrossRef]
- D’Arcy, E.; Rayner, J.; Hodge, A.; Ross, L.J.; Schoenaker, D.A.J.M. The Role of Diet in the Prevention of Diabetes among Women with Prior Gestational Diabetes: A Systematic Review of Intervention and Observational Studies. J. Acad. Nutr. Diet. 2020, 120, 69–85. [Google Scholar] [CrossRef] [Green Version]
- Andersson-Hall, U.; Carlsson, N.G.; Sandberg, A.S.; Holmäng, A. Circulating Linoleic Acid Is Associated with Improved Glucose Tolerance in Women after Gestational Diabetes. Nutrients 2018, 10, 1629. [Google Scholar] [CrossRef] [Green Version]
- Bao, W.; Chavarro, J.E.; Tobias, D.K.; Bowers, K.; Li, S.; Hu, F.B.; Zhang, C. Long-term risk of type 2 diabetes in relation to habitual iron intake in women with a history of gestational diabetes: A prospective cohort study. Am. J. Clin. Nutr. 2016, 103, 375–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, W.; Li, S.; Chavarro, J.E.; Tobias, D.K.; Zhu, Y.; Hu, F.B.; Zhang, C. Low Carbohydrate-Diet Scores and Long-term Risk of Type 2 Diabetes among Women with a History of Gestational Diabetes Mellitus: A Prospective Cohort Study. Diabetes Care 2016, 39, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.H.; Kim, M.Y.; Yang, J.H.; Park, S.Y.; Yim, C.H.; Han, K.O.; Yoon, H.K.; Park, S. Nutritional risk factors of early development of postpartum prediabetes and diabetes in women with gestational diabetes mellitus. Nutrition 2011, 27, 782–788. [Google Scholar] [CrossRef]
- Mercier, R.; Perron, J.; Weisnagel, S.J.; Robitaille, J. Associations between fruit and vegetables intake and abnormal glucose tolerance among women with prior gestational diabetes mellitus. Eur. J. Nutr. 2019, 58, 689–696. [Google Scholar] [CrossRef]
- Tobias, D.K.; Clish, C.; Mora, S.; Li, J.; Liang, L.; Hu, F.B.; Manson, J.A.E.; Zhang, C. Dietary Intakes and Circulating Concentrations of Branched-Chain Amino Acids in Relation to Incident Type 2 Diabetes Risk among High-Risk Women with a History of Gestational Diabetes Mellitus. Clin. Chem. 2018, 64, 1203–1210. [Google Scholar] [CrossRef]
- Cespedes, E.M.; Hu, F.B. Dietary patterns: From nutritional epidemiologic analysis to national guidelines. Am. J. Clin. Nutr. 2015, 101, 899–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Tapsell, L.C.; Neale, E.P.; Satija, A.; Hu, F.B. Foods, nutrients, and dietary patterns: Interconnections and implications for dietary guidelines. Adv. Nutr. 2016, 7, 445–454. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Rahman, M.L.; Wu, J.; DIng, M.; Chavarro, J.E.; Lin, Y.; Ley, S.H.; Bao, W.; Grunnet, L.G.; Hinkle, S.N.; et al. Genetic factors and risk of type 2 diabetes among women with a history of gestational diabetes: Findings from two independent populations. BMJ Open Diabetes Res. Care 2020, 8, e000850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tobias, D.K.; Hu, F.B.; Chavarro, J.; Rosner, B.; Mozaffarian, D.; Zhang, C. Healthful Dietary Patterns and Type 2 Diabetes Mellitus Risk among Women with a History of Gestational Diabetes Mellitus. Arch. Intern. Med. 2012, 172, 1566–1572. [Google Scholar] [CrossRef] [Green Version]
- Sanders, H.; Tripkovic, L.; Wilson, L.; Hart, K.; Lanham-New, S. Comparison of reported dietary intakes between Caucasian and South Asian women and extent of under-reporting. Proc. Nutr. Soc. 2015, 74, E148. [Google Scholar] [CrossRef] [Green Version]
- Yau, A.; Adams, J.; White, M.; Nicolaou, M. Differences in diet quality and socioeconomic patterning of diet quality across ethnic groups: Cross-sectional data from the HELIUS Dietary Patterns study. Eur. J. Clin. Nutr. 2020, 74, 387–396. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Li, Z.; Gao, Q.; Zhao, H.; Chen, S.; Huang, L.; Wang, W.; Wang, T. A Review of Statistical Methods for Dietary Pattern Analysis. Nutr. J. 2021, 20, 37. [Google Scholar] [CrossRef]
- Zaini, A. Where is Malaysia in the midst of the Asian epidemic of diabetes mellitus? Diabetes Res. Clin. Pract. 2000, 50 (Suppl. S2), S23–S28. [Google Scholar] [CrossRef] [PubMed]
- Hirschman, C. The making of race in colonial Malaya: Political economy and racial ideology. Sociol. Forum 1986, 1, 330–361. [Google Scholar] [CrossRef]
- Hatin, W.I.; Nur-Shafawati, A.R.; Zahri, M.K.; Xu, S.; Jin, L.; Tan, S.G.; Rizman-Idid, M.; Zilfalil, B.A.; HUGO Pan-Asian SNP Consortium. Population genetic structure of peninsular Malaysia Malay sub-ethnic groups. PLoS ONE 2011, 6, e18312. [Google Scholar] [CrossRef] [Green Version]
- Ali, A.; Margetts, B.M.; Zainuddin, A.A. Exploration of the principal component analysis (PCA) approach in synthesizing the diet quality of the Malaysian population. Nutrients 2021, 13, 70. [Google Scholar] [CrossRef]
- Hasbullah, F.Y.; Yusof, B.N.M.; Ghani, R.A.; Daud, Z.; ’Azuan, M.; Appannah, G.; Abas, F.; Shafie, N.H.; Khir, H.I.M.; Murphy, H.R. Dietary Patterns, Metabolomic Profile, and Nutritype Signatures Associated with Type 2 Diabetes in Women with Postgestational Diabetes Mellitus: MyNutritype Study Protocol. Metabolites 2022, 12, 843. [Google Scholar] [CrossRef]
- Hasbullah, F.Y.; Mohd Yusof, B.N.; Abdul Ghani, R.; Mat Daud, Z.; ‘Azuan, M.; Appannah, G.; Abas, F.; Shyam, S. Maternal and Dietary Factors Are Associated with Metabolic Syndrome in Women with a Previous History of Gestational Diabetes Mellitus. Int. J. Environ. Res. Public Health 2020, 19, 16797. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Malaysia; Malaysian Endocrine & Metabolic Society; Perinatal Society of Malaysia; Family Medicine Specialists Association of Malaysia; Academy of Medicine Malaysia. Clinical Practice Guidelines Management of Diabetes in Pregnancy. Ministry of Health Malaysia: Putrajaya, Malaysia, 2017. [Google Scholar]
- Institute for Public Health. National Health and Morbidity Survey 2014: Malaysian Adult Nutrition Survey (MANS). Volume I: Methodology and General Findings; Institute for Public Health: Kuala Lumpur, Malaysia, 2014.
- Suzana, S.; Nik Shanita, S.; Zahara, A.M. Atlas of Food Exchanges and Portion Sizes, 3rd ed.; MDC Publishers: Kuala Lumpur, Malaysia, 2015. [Google Scholar]
- Norimah, A.K.; Safiah, M.; Jamal, K.; Haslinda, S.; Zuhaida, H.; Rohida, S.; Norazlin, S.; Poh, B.K.; Kandiah, M.; Zalilah, M.S.; et al. Food Consumption Patterns: Findings from the Malaysian Adult Nutrition Survey (MANS). Malays. J. Nutr. 2008, 14, 25–39. [Google Scholar] [PubMed]
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Ministry of Health Malaysia. Malaysian Food Composition Database (MyFCD). Available online: https://myfcd.moh.gov.my/index.html (accessed on 2 February 2022).
- Ministry of Health Singapore. Energy and Nutrient Composition of Food. Available online: https://focos.hpb.gov.sg/eservices/ENCF/ (accessed on 2 February 2022).
- U.S. Department of Agriculture, Agricultural Research Service. Food Data Central. Available online: https://fdc.nal.usda.gov (accessed on 2 February 2022).
- Shyam, S.; Khor, G.L.; Ambak, R.; Mahadir, B.; Hasnan, M.; Ambu, S.; Chu, W.L.; Aris, T. Association between dietary patterns and overweight risk among Malaysian adults: Evidence from nationally representative surveys. Public Health Nutr. 2020, 23, 319–328. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Multivariate Data Analysis, 4th ed.; Prentice-Hall Inc.: Hoboken, NJ, USA, 2007. [Google Scholar]
- Pérez-Rodrigo, C.; Gil, Á.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Aranceta-Bartrina, J. Clustering of Dietary Patterns, Lifestyles, and Overweight among Spanish Children and Adolescents in the ANIBES Study. Nutrients 2015, 8, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fakhruddin, N.N.I.N.M.; Malaysia, U.K.; Shahar, S.; Rajikan, R.; Omar, M.A.; Din, N.C.; Razali, R.; Harith, S.; Mohamed, H.J.J.; Hakim, B.N.A.; et al. Identification of dietary patterns associated with characteristics of successful aging. Malays. J. Nutr. 2019, 25, 47–57. [Google Scholar] [CrossRef]
- Ministry of Health Malaysia; Malaysian Endocrine & Metabolic Society; Perinatal Society of Malaysia; Family Medicine Specialists Association of Malaysia. Clinical Practice Guidelines Management of Type 2 Diabetes Mellitus, 6th ed.; Ministry of Health Malaysia: Putrajaya, Malaysia, 2020.
- Department of Statistics Malaysia. Household Income Estimates and Incidence of Poverty Report, Malaysia. 2020. Available online: https://www.dosm.gov.my (accessed on 16 January 2023).
- World Health Organization; International Association for The Study of Obesity; International Obesity TaskForce. The Asia Pacific Perspective: Redefining Obesity and Its Treatment; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Am. Coll. Sport. Med. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- The IPAQ Group. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ)—Short and Long Forms. Available online: https://www.researchgate.net/file.PostFileLoader.html?id=5641f4c36143250eac8b45b7&assetKey=AS%3A294237418606593%401447163075131 (accessed on 10 January 2023).
- Gao, D.; Ning, N.; Wang, C.; Wang, Y.; Li, Q.; Meng, Z.; Liu, Y.; Li, Q. Dairy Products Consumption and Risk of Type 2 Diabetes: Systematic Review and Dose-Response Meta-Analysis. PLoS ONE 2013, 8, e73965. [Google Scholar] [CrossRef]
- Pereira, M.A.; Kartashov, A.I.; Ebbeling, C.B.; Van Horn, L.; Slattery, M.L.; Jacobs, D.R., Jr.; Ludwig, D.S. Fast-food habits, weight gain, and insulin resistance (the CARDIA study): 15-year prospective analysis. Lancet 2005, 365, 36–42. [Google Scholar] [CrossRef]
- Balasubramanian, G.V.; Chuah, K.-A.; Khor, B.-H.; Sualeheen, A.; Yeak, Z.-W.; Chinna, K.; Sundram, K.; Karupaiah, T. Associations of Eating Mode Defined by Dietary Patterns with Cardiometabolic Risk Factors in the Malaysia Lipid Study Population. Nutrients 2020, 12, 2080. [Google Scholar] [CrossRef]
- Allister Price, C.; Stanhope, K.L. Understanding the Impact of Added Sugar Consumption on Risk for Type 2 Diabetes. J. Calif. Dent. Assoc. 2016, 44, 619–626. [Google Scholar] [CrossRef]
- Grillo, A.; Salvi, L.; Coruzzi, P.; Salvi, P.; Parati, G. Sodium Intake and Hypertension. Nutrients 2019, 11, 1970. [Google Scholar] [CrossRef] [Green Version]
- Mohamad Kasim, N.; Ahmad, M.H.; Azli Baharudin, S.; Naidu, B.M.; Chan, Y.Y.; Aris, T. Food Choices among Malaysian Adults: Findings from Malaysian Adults Nutrition Survey (MANS) 2003 and MANS 2014. Malays. J. Nutr. 2018, 24, 63–75. [Google Scholar]
- Jannasch, F.; Kröger, J.; Schulze, M.B. Dietary Patterns and Type 2 Diabetes: A Systematic Literature Review and Meta-Analysis of Prospective Studies. J. Nutr. 2017, 147, 1174–1182. [Google Scholar] [CrossRef] [Green Version]
- Villegas, R.; Gao, Y.T.; Yang, G.; Li, H.L.; Elasy, T.A.; Zheng, W.; Shu, X.O. Legume and soy food intake and the incidence of type 2 diabetes in the Shanghai Women’s Health Study. Am. J. Clin. Nutr. 2008, 87, 162–167. [Google Scholar] [CrossRef]
- Ren, G.; Qi, J.; Zou, Y. Association between intake of white rice and incident type 2 diabetes—An updated meta-analysis. Diabetes Res. Clin. Pract. 2021, 172, 108651. [Google Scholar] [CrossRef]
- Yu, J.; Balaji, B.; Tinajero, M.; Jarvis, S.; Khan, T.; Vasudevan, S.; Ranawana, V.; Poobalan, A.; Bhupathiraju, S.; Sun, Q.; et al. White rice, brown rice and the risk of type 2 diabetes: A systematic review and meta-analysis. BMJ Open 2022, 12, e065426. [Google Scholar] [CrossRef] [PubMed]
- Osman, M.H.; Mohd Yusof, B.N.; Ismail, A. Glycaemic index and glycaemic load of foods and food products in Malaysia: A review. Int. Food Res. J. 2020, 28, 217–229. [Google Scholar] [CrossRef]
- Riccardi, G.; Rivellese, A.A.; Giacco, R. Role of glycemic index and glycemic load in the healthy state, in prediabetes, and in diabetes. Am. J. Clin. Nutr. 2008, 87, 269S–274S. [Google Scholar] [CrossRef] [Green Version]
- Hasbullah, F.Y.; Mohd Yusof, B.N.; Shariff, Z.M.; Rejali, Z.; Yong, H.Y.; Mitri, J. Factors associated with dietary glycemic index and glycemic load in pregnant women and risk for gestational diabetes mellitus. Int. J. Food Sci. Nutr. 2020, 71, 516–524. [Google Scholar] [CrossRef]
- Odegaard, A.O.; Koh, W.P.; Butler, L.M.; Duval, S.; Gross, M.D.; Yu, M.C.; Yuan, J.M.; Pereira, M.A. Dietary patterns and incident type 2 diabetes in Chinese men and women: The Singapore Chinese Health study. Diabetes Care 2011, 34, 880–885. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Zähringer, J.; Beyerbach, J.; Werner, S.W.; Heseker, H.; Koletzko, B.; Meerpohl, J.J. Total Dietary Fat Intake, Fat Quality, and Health Outcomes: A Scoping Review of Systematic Reviews of Prospective Studies. Ann. Nutr. Metab. 2021, 77, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Schwab, U.; Lauritzen, L.; Tholstrup, T.; Haldorssoni, T.; Riserus, U.; Uusitupa, M.; Becker, W. Effect of the amount and type of dietary fat on cardiometabolic risk factors and risk of developing type 2 diabetes, cardiovascular diseases, and cancer: A systematic review. Food Nutr. Res. 2014, 58, 25145. [Google Scholar] [CrossRef] [Green Version]
- Moazzami, A.A.; Shrestha, A.; Morrison, D.A.; Poutanen, K.; Mykkänen, H. Metabolomics reveals differences in postprandial responses to breads and fasting metabolic characteristics associated with postprandial insulin demand in postmenopausal women. J. Nutr. 2014, 144, 807–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oluwagbemigun, K.; Foerster, J.; Watkins, C.; Fouhy, F.; Stanton, C.; Bergmann, M.M.; Boeing, H.; Nöthlings, U. Dietary Patterns Are Associated with Serum Metabolite Patterns and Their Association Is Influenced by Gut Bacteria among Older German Adults. J. Nutr. 2019, 150, 149–158. [Google Scholar] [CrossRef] [Green Version]
- Floegel, A.; von Ruesten, A.; Drogan, D.; Schulze, M.B.; Prehn, C.; Adamski, J.; Pischon, T.; Boeing, H. Variation of serum metabolites related to habitual diet: A targeted metabolomic approach in EPIC-Potsdam. Eur. J. Clin. Nutr. 2013, 67, 1100–1108. [Google Scholar] [CrossRef] [Green Version]
- Lynch, C.J.; Adams, S.H. Branched-chain amino acids in metabolic signalling and insulin resistance. Nat. Rev. Endocrinol. 2014, 10, 723–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, X.; Han, Q.; Liu, Y.; Sun, C.; Gang, X.; Wang, G. The Relationship between Branched-Chain Amino Acid Related Metabolomic Signature and Insulin Resistance: A Systematic Review. J. Diabetes Res. 2016, 2016, 2794591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bountziouka, V.; Tzavelas, G.; Polychronopoulos, E.; Constantinidis, T.C.; Panagiotakos, D.B. Validity of dietary patterns derived in nutrition surveys using a priori and a posteriori multivariate statistical methods. Int. J. Food Sci. Nutr. 2011, 62, 617–627. [Google Scholar] [CrossRef]
- Panagiotakos, D. α-priori versus α-posterior methods in dietary pattern analysis: A review in nutrition epidemiology. Nutr. Bull. 2008, 33, 311–315. [Google Scholar] [CrossRef]
- Tapsell, L.C.; Neale, E.P.; Probst, Y. Dietary Patterns and Cardiovascular Disease: Insights and Challenges for Considering Food Groups and Nutrient Sources. Curr. Artheroscler. Rep. 2019, 21, 9. [Google Scholar] [CrossRef] [Green Version]
- Guasch-Ferre, M.; Bhupathiraju, S.N.; Hu, F.B. Use of Metabolomics in Improving Assessment of Dietary Intake. Clin. Chem. 2018, 64, 82–98. [Google Scholar] [CrossRef] [Green Version]
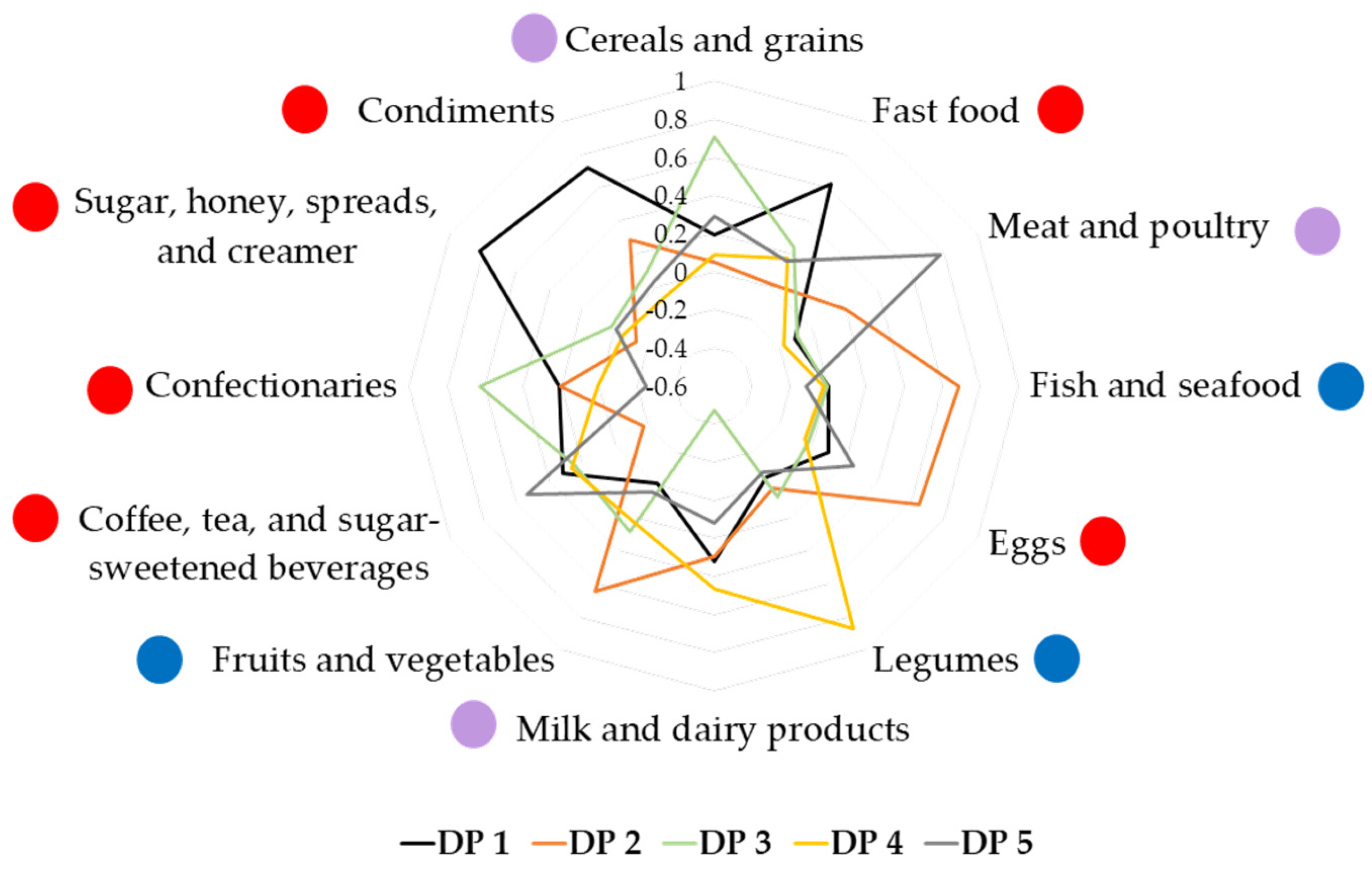
 : food group perceived to be healthy; blue circle
: food group perceived to be healthy; blue circle  : food group perceived to be unhealthy; purple circle
: food group perceived to be unhealthy; purple circle  : food group consisting of healthy and unhealthy food items.
: food group perceived to be healthy; blue circle : food group perceived to be unhealthy; purple circle : food group consisting of healthy and unhealthy food items.
: food group consisting of healthy and unhealthy food items.
: food group perceived to be healthy; blue circle : food group perceived to be unhealthy; purple circle : food group consisting of healthy and unhealthy food items.


{kind=link}
{kind=link}
| Variables | NGT (n = 100) | AGT (n = 57) | p-Value |
|---|---|---|---|
| Mean ± SD or n (%) | |||
| Sociodemographic background | |||
| Age (years) | 34.3 ± 5.9 | 35.6 ± 5.1 | 0.188 |
| Age distribution | |||
| 18–24 | 1 (1.0) | 2 (3.5) | 0.134 |
| 25–34 | 56 (56.0) | 22 (38.6) | |
| 35–44 | 38 (38.0) | 30 (52.6) | |
| 45–49 | 5 (5.0) | 3 (5.3) | |
| Ethnicity | |||
| Malay | 82 (82.0) | 49 (86.0) | |
| Chinese | 11 (11.0) | 2 (3.5) | 0.225 a |
| Indian | 4 (4.0) | 5 (8.8) | |
| Others | 3 (3.0) | 1 (1.8) | |
| Marital status | |||
| Married | 99 (99.0) | 56 (98.2) | 0.999 a |
| Divorced/widowed | 1 (1.0) | 1 (1.8) | |
| Education level | |||
| Primary education | 1 (1.0) | 0 (0.0) | |
| Secondary education | 42 (42.0) | 32 (56.1) | 0.151 a |
| Tertiary education | 57 (57.0) | 25 (43.9) | |
| Working status | |||
| Not working (housewife/student) | 27 (27.0) | 23 (40.4) | 0.084 |
| Working (employed/self-employed) | 73 (73.0) | 34 (59.6) | |
| Monthly household income (RM) | 6300 ± 3889 | 6211 ± 4568 | 0.898 |
| Low-income group (<RM4850) | 35 (35.0) | 26 (45.6) | |
| Middle-income group (RM4850–10,959) | 56 (56.0) | 25 (43.9) | 0.327 |
| High-income group (>RM10,959) | 9 (9.0) | 6 (10.5) | |
| Household size | 4 ± 1 | 5 ± 1 | 0.005 * |
| General obstetric history | |||
| Family history of diabetes | 68 (68.0) | 45 (78.9) | 0.142 |
| Gravidity | 3 ± 2 | 4 ± 2 | 0.037 * |
| Parity | 2 ± 1 | 3 ± 1 | 0.004 * |
| GDM recurrence | 16 (16.0) | 18 (31.6) | 0.023 * |
| Obstetric history during index GDM | |||
| Duration since index GDM (years) | 2.6 ± 3.6 | 2.4 ± 3.4 | 0.810 |
| Pre-pregnancy BMI (kg/m2) | 23.6 ± 4.0 | 26.3 ± 5.0 | 0.001 * |
| BMI categories | |||
| Underweight (<18.5 kg/m2) | 10 (10.0) | 2 (3.5) | |
| Normal (18.5–22.9 kg/m2) | 32 (32.0) | 12 (21.1) | 0.010 * |
| Overweight (23.0–24.9 kg/m2) | 27 (27.0) | 10 (17.5) | |
| Obese (≥25.0 kg/m2) | 31 (31.0) | 33 (57.9) | |
| Gestational weight gain (kg) | 10.8 ± 7.0 | 9.9 ± 5.5 | 0.413 |
| Postpartum weight retention (kg) | 5.1 ± 6.8 | 4.1 ± 6.0 | 0.365 |
| Gestational age during diagnosis (weeks) | 20.3 ± 7.7 | 18.6 ± 7.3 | 0.189 |
| Delivery method | |||
| Spontaneous vaginal delivery | 66 (66.0) | 35 (61.4) | 0.454 |
| Caesarean section | 32 (32.0) | 22 (38.6) | |
| Treatment | |||
| Diet control only | 87 (87.0) | 47 (82.5) | 0.439 |
| Diet control with metformin/insulin | 13 (13.0) | 10 (17.5) | |
| Breastfeeding status | |||
| Never breastfed | 0 (0.0) | 1 (1.8) | |
| Stopped breastfeeding | 34 (34.0) | 26 (45.6) | 0.119 a |
| Still breastfeeding | 64 (64.0) | 30 (52.6) | |
| Infant birth weight (kg) | 3.05 ± 0.51 | 3.14 ± 0.52 | 0.313 |
| Presence of macrosomia (>4.0 kg) | 3 (3.0) | 4 (7.0) | 0.424 a |
| Anthropometric and clinical measurements | |||
| Height (m) | 1.57 ± 0.06 | 1.56 ± 0.05 | 0.815 |
| Current weight (kg) | 63.3 ± 13.4 | 68.7 ± 13.5 | 0.016 * |
| Current BMI (kg/m2) | 25.7 ± 5.0 | 27.9 ± 4.7 | 0.007 * |
| BMI categorization | 0.014 * | ||
| Underweight (<18.5 kg/m2) | 7 (7.0) | 1 (1.8) | |
| Normal (18.5–22.9 kg/m2) | 21 (21.0) | 8 (14.0) | |
| Overweight (23.0–24.9 kg/m2) | 24 (24.0) | 6 (10.5) | |
| Obese (≥25.0 kg/m2) | 48 (48.0) | 42 (73.7) | |
| Waist circumference (cm) | 85.5 ± 10.1 | 89.9 ± 11.5 | 0.012 * |
| Within recommendation (<80 cm) | 30 (30.0) | 11 (19.3) | |
| Abdominal obesity (≥80 cm) | 70 (70.0) | 46 (80.7) | 0.142 |
| Hip circumference (cm) | 104.7 ± 10.3 | 108.2 ± 9.8 | 0.040 * |
| Waist-to-hip ratio | 0.83 ± 0.14 | 0.83 ± 0.06 | 0.935 |
| Within recommendation (≤0.8) | 40 (40.0) | 18 (31.6) | |
| Abdominal obesity (>0.8) | 60 (60.0) | 39 (68.4) | 0.293 |
| Systolic blood pressure (mmHg) | 111 ± 15 | 112 ± 15 | 0.706 |
| Diastolic blood pressure (mmHg) | 79 ± 11 | 81 ± 9 | 0.422 |
| Blood pressure category | |||
| Normal | 52 (52.0) | 27 (47.4) | |
| Pre-hypertension | 6 (6.0) | 1 (1.8) | 0.532 a |
| Stage 1 hypertension | 26 (26.0) | 19 (33.3) | |
| Stage 2 hypertension | 16 (16.0) | 10 (17.5) | |
| Biochemical profile | |||
| Fasting plasma glucose (mmol/L) | 4.55 ± 0.43 | 5.32 ± 1.71 | <0.001 * |
| 2-h plasma glucose (mmol/L) | 5.51 ± 1.18 | 8.15 ± 3.18 | <0.001 * |
| HbA1c (%) | 5.3 ± 0.2 | 6.0 ± 1.2 | <0.001 * |
| Fasting insulin (uIU/mL) | 6.44 ± 4.48 | 10.65 ± 9.01 | <0.001 * |
| Total cholesterol (mmol/L) | 5.14 ± 0.81 | 5.50 ± 1.01 | 0.024 * |
| Triglycerides (mmol/L) | 1.03 ± 0.57 | 1.32 ± 0.76 | 0.015 * |
| HDL cholesterol (mmol/L) | 1.59 ± 0.43 | 1.44 ± 0.36 | 0.021 * |
| LDL cholesterol (mmol/L) | 3.07 ± 0.74 | 3.46 ± 0.96 | 0.010 * |
| Non-HDL cholesterol (mmol/L) | 3.55 ± 0.80 | 4.07 ± 0.98 | 0.001 * |
| Total to HDL cholesterol ratio | 3.4 ± 0.9 | 4.0 ± 1.0 | <0.001 * |
| Physical activity | |||
| Total physical activity level (MET-min/week) | 2088 ± 401 | 1951 ± 387 | 0.822 |
| Vigorous-intensity (MET-min/week) | 482 ± 146 | 368 ± 98 | 0.584 |
| Moderate-intensity (MET-min/week) | 822 ± 183 | 768 ± 168 | 0.844 |
| Walking (MET-min/week) | 783 ± 188 | 814 ± 308 | 0.928 |
| Sitting duration (minutes/day) | 372 ± 20 | 363 ± 26 | 0.795 |
| Dietary Variables | NGT (n = 97) | AGT (n = 53) | p-Value |
|---|---|---|---|
| Energy and nutrient intakes | |||
| Total energy intake (TEI) (kcal/day) | 1738 ± 682 | 1681 ± 695 | 0.631 |
| Carbohydrate intake | |||
| Total amount (g/day) | 232 ± 99 | 235 ± 104 | 0.856 |
| As part of TEI (%) | 54 ± 9 | 56 ± 8 | 0.113 |
| Protein intake | |||
| Total amount (g/day) | 83 ± 40 | 80 ± 39 | 0.627 |
| As part of TEI (%) | 19 ± 5 | 19 ± 5 | 0.867 |
| Fat intake | |||
| Total amount (g/day) | 54 ± 26 | 48 ± 23 | 0.153 |
| As part of TEI (%) | 27 ± 6 | 25 ± 6 | 0.033 * |
| Saturated fat intake (g/day) | 13 ± 7 | 11 ± 6 | 0.043 * |
| Fiber intake (g/day) | 6 ± 7 | 6 ± 7 | 0.960 |
| Sugar intake (g/day) | 35 ± 28 | 36 ± 28 | 0.833 |
| Food group intake | |||
| Cereals and cereal products (g/day) | 401 ± 190 | 399 ± 188 | 0.964 |
| Fast food (g/day) | 46 ± 5 | 56 ± 8 | 0.294 |
| Meat and poultry (g/day) | 156 ± 14 | 139 ± 21 | 0.489 |
| Fish and seafood (g/day) | 68 ± 8 | 71 ± 10 | 0.776 |
| Eggs (g/day) | 34 ± 33 | 25 ± 3 | 0.034 * |
| Legumes (g/day) | 14 ± 4 | 15 ± 3 | 0.817 |
| Milk and dairy products (g/day) | 112 ± 14 | 65 ± 12 | 0.012 * |
| Vegetables (g/day) | 36 ± 3 | 50 ± 7 | 0.076 |
| Fruits (g/day) | 217 ± 24 | 238 ± 44 | 0.641 |
| Beverages (g/day) | 353 ± 36 | 345 ± 51 | 0.895 |
| Confectionaries (g/day) | 42 ± 6 | 45 ± 5 | 0.772 |
| Bread spreads (g/day) | 3 ± 0.4 | 3 ± 1 | 0.983 |
| Condiments (g/day) | 20 ± 2 | 23 ± 3 | 0.442 |
| Energy and Macronutrient Intakes | DP 1 (Unhealthy) | DP 2 (Fish-Eggs-Fruits-Vegetables) | DP 3 (Cereals-Confectionaries) | DP 4 (Legumes-Dairy) | DP 5 (Meat-Sugar-Sweetened Beverages) |
|---|---|---|---|---|---|
| TEI (kcal/day) | 0.413 *** | 0.450 *** | 0.466 *** | 0.240 ** | 0.424 *** |
| Carbohydrate (g/day) | 0.438 *** | 0.304 *** | 0.634 *** | 0.270 ** | 0.225 * |
| Protein (g/day) | 0.189 * | 0.571 *** | 0.188 * | 0.111 | 0.545 *** |
| Total fat (g/day) | 0.414 *** | 0.420 *** | 0.191 * | 0.221 ** | 0.528 *** |
| Saturated fat (g/day) | 0.414 *** | 0.354 *** | 0.035 | 0.273 ** | 0.610 *** |
| Fiber (g/day) | 0.136 | 0.514 *** | 0.237 ** | 0.373 *** | 0.089 |
| Sugar (g/day) | 0.379 *** | 0.409 *** | 0.297 *** | 0.355 *** | 0.099 |
| Dietary Pattern | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| DP 1 (Mostly unhealthy) | 1.060 | 0.761, 1.476 | 1.035 | 0.723, 1.481 | 1.054 | 0.697, 1.595 |
| DP 2 (Fish-eggs-fruits-vegetables) | 0.886 | 0.624, 1.260 | 0.879 | 0.604, 1.278 | 0.857 | 0.565, 1.300 |
| DP 3 (Cereals-confectionaries) | 1.281 | 0.912, 1.800 | 1.406 | 0.971, 2.036 | 1.536 * | 1.002, 2.354 |
| DP 4 (Legumes-dairy) | 0.937 | 0.657, 1.336 | 0.985 | 0.694, 1.398 | 0.986 | 0.692, 1.406 |
| DP 5 (Meat-sugar-sweetened beverages) | 0.812 | 0.571, 1.155 | 0.825 | 0.565, 1.205 | 0.794 | 0.522, 1.206 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasbullah, F.Y.; Mohd Yusof, B.-N.; Shyam, S.; Abdul Ghani, R.; Mohamed Khir, H.I. Dietary Patterns Associated with Abnormal Glucose Tolerance following Gestational Diabetes Mellitus: The MyNutritype Study. Nutrients 2023, 15, 2819. https://doi.org/10.3390/nu15122819
Hasbullah FY, Mohd Yusof B-N, Shyam S, Abdul Ghani R, Mohamed Khir HI. Dietary Patterns Associated with Abnormal Glucose Tolerance following Gestational Diabetes Mellitus: The MyNutritype Study. Nutrients. 2023; 15(12):2819. https://doi.org/10.3390/nu15122819
Chicago/Turabian StyleHasbullah, Farah Yasmin, Barakatun-Nisak Mohd Yusof, Sangeetha Shyam, Rohana Abdul Ghani, and Hannah Izzati Mohamed Khir. 2023. "Dietary Patterns Associated with Abnormal Glucose Tolerance following Gestational Diabetes Mellitus: The MyNutritype Study" Nutrients 15, no. 12: 2819. https://doi.org/10.3390/nu15122819