
An Exploratory Study on a New Method for Nutritional Status Assessment in Patients with Chronic Kidney Disease
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
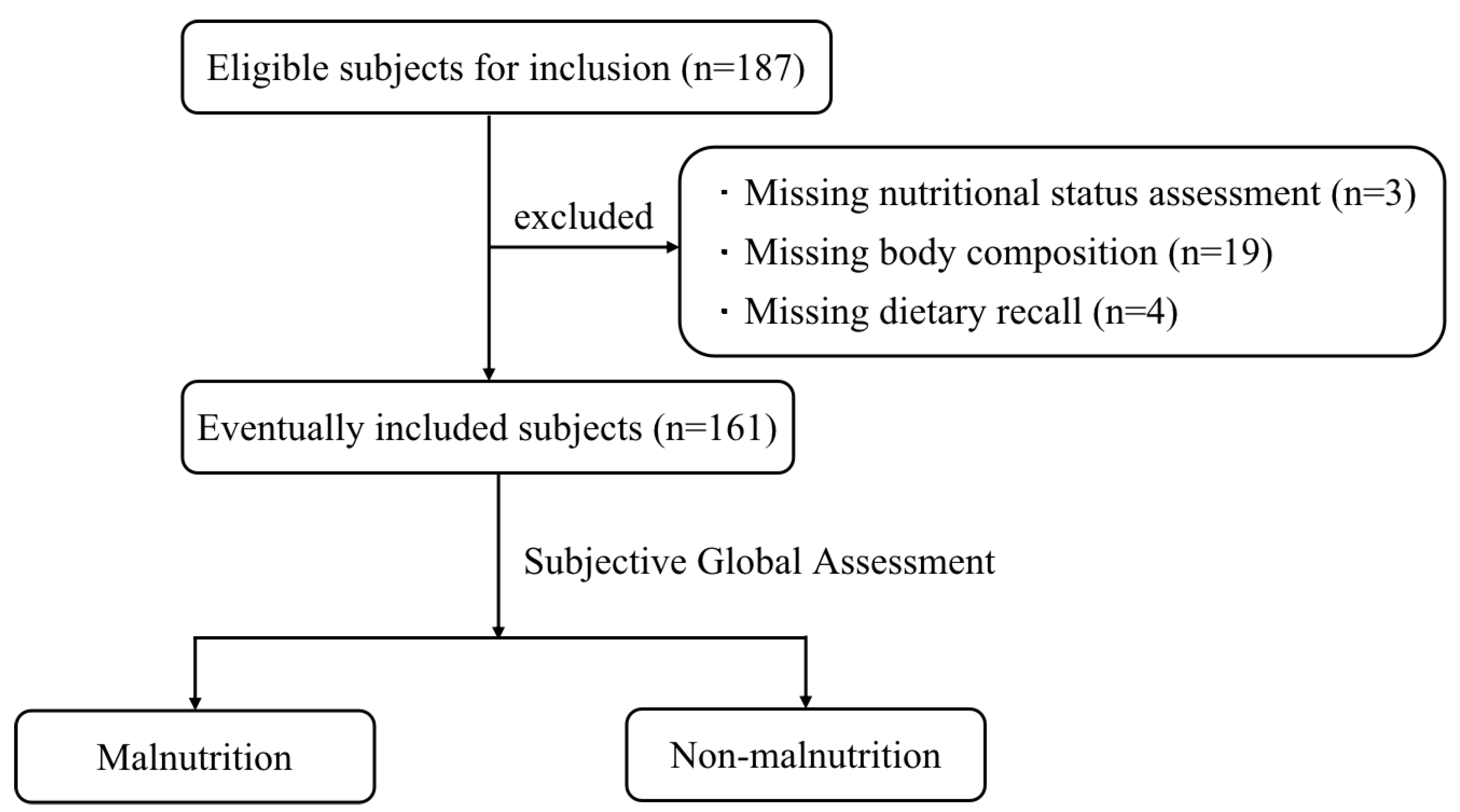
2.1. Study Population
2.2. Clinical Data Collection
2.3. Anthropometry and Body Composition Indicators
- BMI was calculated by dividing the weight (in kilograms) by the square of the height (in meters).
- HGS: According to the size of the subject’s hand, the handle of the handgrip dynamometer was adjusted, the subject was informed to take the standing position with the arm naturally sagging, and the handgrip dynamometer was grasped with the unilateral hand as hard as possible. The measurement was accurate to 0.1 kg and repeated three times with an interval of 1 min, and the highest value was taken as the HGS value.
- CC: The maximum circumference was measured with a tape measure at the right calf of the subject in a sitting position with feet on the floor and knees bent at 90°. The measurement was repeated twice and averaged with an accuracy of 0.1 cm.
- TSF: The subject’s arm was naturally pendulous, the surveyor pinched the sebum at the midpoint of the dorsal upper arm of the subject with the left thumb and index finger, and they then measured the skinfold thickness with a sebum skinfold caliper at a distance of 1 cm from the finger pinching site. The tip of the caliper was made to fully clamp the skinfold, the results after the pointer came to a complete stop were read and recorded immediately, and the measurements were repeated three times and averaged with an accuracy of 0.1 mm.
- The body composition indicators of the subjects were collected by the InbodyS10 body composition analyzer, including mid-arm circumference (MAC), MAMC, skeletal muscle mass index (SMI), body protein, body inorganic salts, body bone mineral content, body fat, BFP, and PhA. Before measurement, it was confirmed whether there was no pacemaker or metal implant in the subject, and the subject was informed to take the supine position, exposing the bilateral fingers and ankles. The relevant information of the subject was input on the instrument operation panel, the upper-limb electrode clips were clamped on the thumb and middle finger of the subject, the lower-limb electrode clips were clamped on the ankle of the subject, and the measurement was started after confirming that the electrode clips were properly clamped. After completion of the measurement, the electrode clips were removed, and the body composition report was read.
2.4. Nutritional Status Assessment
2.5. Statistical Analysis
3. Results
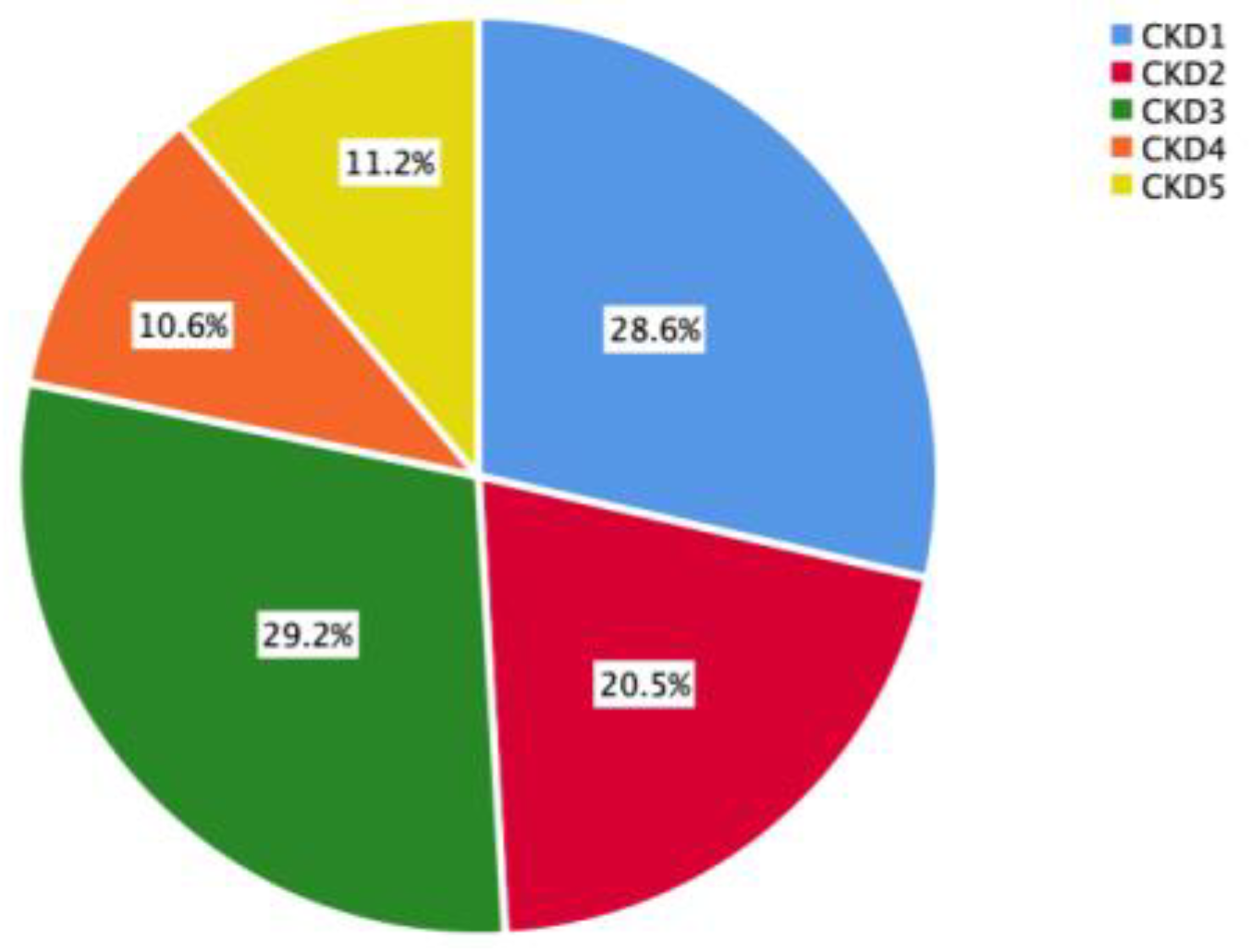
3.1. Subject Screening and CKD Staging
3.2. Assessment of Nutritional Status of the Study Population
3.3. Consistency Test between Renal iNUT and SGA and PEW
3.4. Comparison of Clinical Characteristics and Anthropometric Parameters of Malnutrition and Non-Malnutrition Subjects
3.5. Logistic Regression Analysis of Malnutrition in CKD
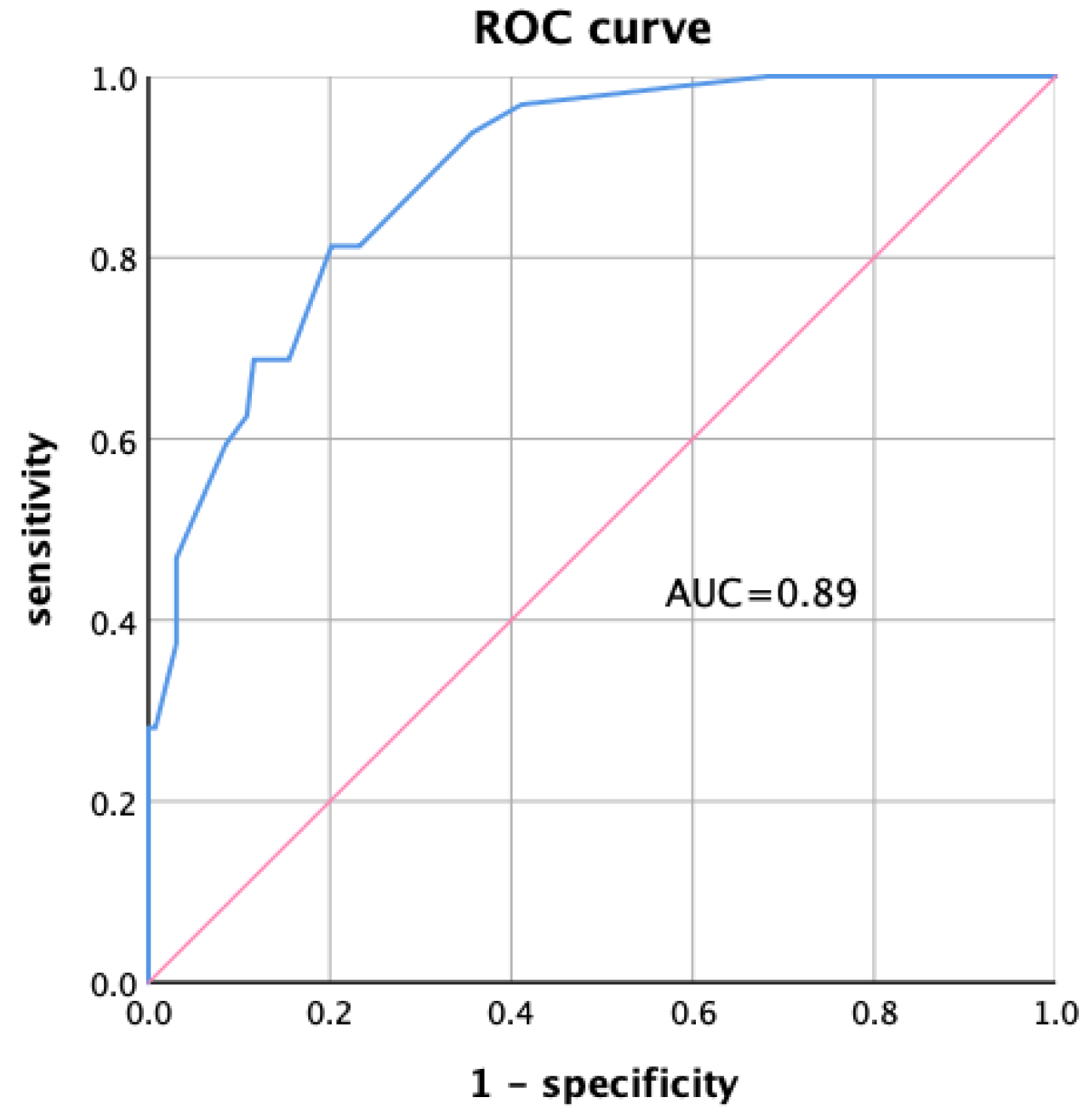
3.6. ROC Curve of Multiple Indicators Combined for the Diagnosis of CKD Malnutrition
+ 1.351 × neutrophil-lymphocyte ratio (≤2.62 = 0, >2.62 = 1)
+ 1.44 × transferrin (≥200 mg/dL = 0, <200 mg/dL = 1)
+ 2.012 × phase Angle (≥4.5° = 0, <4.5° = 1)
+ 2.951 × body fat percentage (≥10% = 0, <10% = 1)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| CKD Stage | SGA | |
|---|---|---|
| Malnutrition | Non-Malnutrition | |
| stage 1 | 6 (13%) | 40 (87%) |
| stage 2 | 7 (21.2%) | 26 (78.8%) |
| stage 3 | 8 (17%) | 39 (83%) |
| stage 4 | 5 (29.4%) | 12 (70.6%) |
| stage 5 | 6 (33.3%) | 12 (66.7%) |
| Variables | OR | 95%CI | p Value |
|---|---|---|---|
| Age | 1.066 | 1.03–1.10 | <0.001 |
| Gender | 0.762 | 0.348–1.669 | 0.497 |
| NLR | 1.402 | 1.015–1.938 | 0.04 |
| IL-6 | 1.109 | 0.998–1.233 | 0.055 |
| Hemoglobin | 0.973 | 0.956–0.99 | 0.003 |
| Albumin | 0.908 | 0.861–0.958 | <0.001 |
| Prealbumin | 0.935 | 0.882–0.992 | 0.025 |
| Transferrin | 0.98 | 0.97–0.991 | <0.001 |
| BUN | 1.11 | 1.029–1.197 | 0.007 |
| Cystatin C | 1.732 | 1.159–2.587 | 0.007 |
| Serum calcium | 0.028 | 0.002–0.371 | 0.007 |
| Serum phosphorus | 8.738 | 1.532–49.826 | 0.015 |
| BMI | 0.879 | 0.785–0.985 | 0.026 |
| CC | 0.88 | 0.778–0.995 | 0.041 |
| HGS | 0.94 | 0.898–0.985 | 0.009 |
| PhA | 0.37 | 0.242–0.566 | <0.001 |
| BFP | 0.957 | 0.915–1.001 | 0.054 |
| Variables | Assignment Method |
|---|---|
| Group | non-malnutrition = 0; malnutrition = 1 |
| Age | ≤60 years = 0; >60 years = 1 |
| Gender | female = 0; male = 1 |
| NLR | ≤2.62 = 0; >2.62 = 1 |
| IL-6 | ≤5.9 pg/mL = 0; >5.9 pg/mL = 1 |
| Hemoglobin | male ≤ 137 g/L, female ≤ 116 g/L = 0; male > 137 g/L, female > 116 g/L = 1 |
| Albumin | ≥35g/L = 0; <35g/L = 1 |
| Prealbumin | ≥20 mg/dL = 0; <20 mg/dL = 1 |
| Transferrin | ≥200 mg/dL = 0; <200 mg/dL = 1 |
| BUN | ≤7.5 mmol/L = 0; >7.5 mmol/L = 1 |
| Cystatin C | ≤1.25 mg/L = 0; >1.25 mg/L = 1 |
| Serum calcium | ≥2.09 mmol/L = 0; <2.09 mmol/L = 1 |
| Serum phosphorus | ≤1.12 mmol/L = 0; >1.12 mmol/L, ≤1.25 mmol/L = 1; >1.25 mmol/L, ≤1.4 mmol/L = 2; >1.4 mmol/L = 3 |
| BMI | ≥20 kg/m2 = 0; <20 kg/m2 = 1 |
| CC | male ≥ 34 cm, female ≥ 33 cm = 0; male < 34 cm, female < 33 cm = 1 |
| HGS | male ≥ 28 kg, female ≥ 18 kg = 0; male < 28 kg, female < 18 kg = 1 |
| PhA | ≥4.5° = 0; <4.5° = 1 |
| BFP | ≥10% = 0; <10% = 1 |
References
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franco, B.B.; Hopman, W.M.; Lamarche, M.C.; Holden, R.M. Protein energy wasting and long-term outcomes in nondialysis dependent chronic kidney disease. J. Ren. Care 2022, 48, 14–23. [Google Scholar] [CrossRef]
- Peev, V.; Nayer, A.; Contreras, G. Dyslipidemia, malnutrition, inflammation, cardiovascular disease and mortality in chronic kidney disease. Curr. Opin. Lipidol. 2014, 25, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, P.; Seres, D.; Lobo, D.N.; Gomes, F.; Kaegi-Braun, N.; Stanga, Z. Management of disease-related malnutrition for patients being treated in hospital. Lancet 2021, 398, 1927–1938. [Google Scholar] [CrossRef]
- Bellanti, F.; Lo Buglio, A.; Quiete, S.; Vendemiale, G. Malnutrition in Hospitalized Old Patients: Screening and Diagnosis, Clinical Outcomes, and Management. Nutrients 2022, 14, 910. [Google Scholar] [CrossRef]
- Fiaccadori, E.; Sabatino, A.; Barazzoni, R.; Carrero, J.J.; Cupisti, A.; De Waele, E.; Jonckheer, J.; Singer, P.; Cuerda, C. ESPEN guideline on clinical nutrition in hospitalized patients with acute or chronic kidney disease. Clin. Nutr. 2021, 40, 1644–1668. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; Kalantar-Zadeh, K.; Kopple, J.; Cano, N.; Chauveau, P.; Cuppari, L.; Franch, H.; Guarnieri, G.; Ikizler, T.A.; Kaysen, G.; et al. A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int. 2008, 73, 391–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikizler, T.A.; Cano, N.J.; Franch, H.; Fouque, D.; Himmelfarb, J.; Kalantar-Zadeh, K.; Kuhlmann, M.K.; Stenvinkel, P.; TerWee, P.; Teta, D.; et al. Prevention and treatment of protein energy wasting in chronic kidney disease patients: A consensus statement by the International Society of Renal Nutrition and Metabolism. Kidney Int. 2013, 84, 1096–1107. [Google Scholar] [CrossRef] [Green Version]
- Jackson, H.S.; MacLaughlin, H.L.; Vidal-Diez, A.; Banerjee, D. A new renal inpatient nutrition screening tool (Renal iNUT): A multicenter validation study. Clin. Nutr. 2019, 38, 2297–2303. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Bigogno, F.G.; Fetter, R.L.; Avesani, C.M. Applicability of subjective global assessment and malnutrition inflammation score in the assessment of nutritional status on chronic kidney disease. J. Bras. Nefrol. 2014, 36, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Kovesdy, C.P.; Anderson, J.E.; Kalantar-Zadeh, K. Paradoxical association between body mass index and mortality in men with CKD not yet on dialysis. Am. J. Kidney Dis. 2007, 49, 581–591. [Google Scholar] [CrossRef] [PubMed]
- Oladele, C.O.; Unuigbe, E.; Chukwuonye, I.I.; Obi, E.C.; Ohagwu, K.A.; Oladele, G.; Ojogwu, L.I. Assessment of nutritional status in patients with chronic kidney disease in Nigeria. Saudi J. Kidney Dis. Transplant. 2021, 32, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Moriconi, D.; D’Alessandro, C.; Giannese, D.; Panichi, V.; Cupisti, A. Diagnosis, Prevalence and Significance of Obesity in a Cohort of CKD Patients. Metabolites 2023, 13, 196. [Google Scholar] [CrossRef]
- Wu, L.W.; Lin, Y.Y.; Kao, T.W.; Lin, C.M.; Liaw, F.Y.; Wang, C.C.; Peng, T.C.; Chen, W.L. Mid-arm muscle circumference as a significant predictor of all-cause mortality in male individuals. PLoS ONE 2017, 12, e0171707. [Google Scholar] [CrossRef]
- Shen, F.C.; Chen, M.E.; Wu, W.T.; Kuo, I.C.; Niu, S.W.; Lee, J.J.; Hung, C.C.; Chang, J.M.; Hwang, S.J. Normal weight and waist obesity indicated by increased total body fat associated with all-cause mortality in stage 3–5 chronic kidney disease. Front. Nutr. 2022, 9, 982519. [Google Scholar] [CrossRef]
- Han, B.G.; Lee, J.Y.; Kim, J.S.; Yang, J.W. Clinical Significance of Phase Angle in Non-Dialysis CKD Stage 5 and Peritoneal Dialysis Patients. Nutrients 2018, 10, 1331. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.L.; Liang, S.; Zhu, F.L.; Liu, J.Q.; Chen, X.M.; Cai, G.Y. Association of the malnutrition-inflammation score with anthropometry and body composition measurements in patients with chronic kidney disease. Ann. Palliat. Med. 2019, 8, 596–603. [Google Scholar] [CrossRef]
- Han, B.G.; Lee, J.Y.; Kim, J.S.; Yang, J.W. Decreased Bioimpedance Phase Angle in Patients with Diabetic Chronic Kidney Disease Stage 5. Nutrients 2019, 11, 2874. [Google Scholar] [CrossRef] [Green Version]
- Stevens, P.E.; Levin, A.; Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Detsky, A.S.; McLaughlin, J.R.; Baker, J.P.; Johnston, N.; Whittaker, S.; Mendelson, R.A.; Jeejeebhoy, K.N. What is subjective global assessment of nutritional status? JPEN J. Parenter. Enter. Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Society, C.N. Dietary Reference Intakes for Chinese, 2013 ed.; Sciences Press: Beijing, China, 2015; p. 660. [Google Scholar]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic criteria for malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Carrero, J.J.; Thomas, F.; Nagy, K.; Arogundade, F.; Avesani, C.M.; Chan, M.; Chmielewski, M.; Cordeiro, A.C.; Espinosa-Cuevas, A.; Fiaccadori, E.; et al. Global Prevalence of Protein-Energy Wasting in Kidney Disease: A Meta-analysis of Contemporary Observational Studies from the International Society of Renal Nutrition and Metabolism. J. Ren. Nutr. 2018, 28, 380–392. [Google Scholar] [CrossRef]
- Anupama, S.H.; Abraham, G.; Alex, M.; Vijayan, M.; Subramanian, K.K.; Fernando, E.; Nagarajan, V.; Nageshwara Rao, P.K. A multicenter study of malnutrition status in chronic kidney disease stages I-V-D from different socioeconomic groups. Saudi J. Kidney Dis. Transplant. 2020, 31, 614–623. [Google Scholar]
- Chinese Medical Doctor Association Nephrologist Branch. Chinese association of integrated Chinese and western medicine kidney disease professional committee nutrition therapy guidelines expert collaboration group. Clinical practice guidelines for nutritional therapy of chronic kidney disease in China (2021 edition). Natl. Med. J. China 2021, 101, 539–559. [Google Scholar]
- Allard, J.P.; Keller, H.; Gramlich, L.; Jeejeebhoy, K.N.; Laporte, M.; Duerksen, D.R. GLIM criteria has fair sensitivity and specificity for diagnosing malnutrition when using SGA as comparator. Clin. Nutr. 2020, 39, 2771–2777. [Google Scholar] [CrossRef]
- Dent, E.; Hoogendijk, E.O.; Visvanathan, R.; Wright, O.R.L. Malnutrition Screening and Assessment in Hospitalised Older People: A Review. J. Nutr. Health Aging 2019, 23, 431–441. [Google Scholar] [CrossRef]
- Ahmed, T.; Haboubi, N. Assessment and management of nutrition in older people and its importance to health. Clin. Interv. Aging 2010, 5, 207–216. [Google Scholar]
- Windahl, K.; Faxen Irving, G.; Almquist, T.; Liden, M.K.; van de Luijtgaarden, M.; Chesnaye, N.C.; Voskamp, P.; Stenvinkel, P.; Klinger, M.; Szymczak, M.; et al. Prevalence and Risk of Protein-Energy Wasting Assessed by Subjective Global Assessment in Older Adults with Advanced Chronic Kidney Disease: Results from the EQUAL Study. J. Ren. Nutr. 2018, 28, 165–174. [Google Scholar] [CrossRef] [Green Version]
- Xi, W.Z.; Wu, C.; Liang, Y.L.; Wang, L.L.; Cao, Y.H. Analysis of malnutrition factors for inpatients with chronic kidney disease. Front. Nutr. 2022, 9, 1002498. [Google Scholar] [CrossRef]
- Song, M.; Graubard, B.I.; Rabkin, C.S.; Engels, E.A. Neutrophil-to-lymphocyte ratio and mortality in the United States general population. Sci. Rep. 2021, 11, 464. [Google Scholar] [CrossRef] [PubMed]
- Buonacera, A.; Stancanelli, B.; Colaci, M.; Malatino, L. Neutrophil to Lymphocyte Ratio: An Emerging Marker of the Relationships between the Immune System and Diseases. Int. J. Mol. Sci. 2022, 23, 3636. [Google Scholar] [CrossRef]
- Han, Q.; Lin, S.; He, F.; Zhang, R.; Xie, X.; Qing, F.; Huang, R.; Chen, C.; Yang, Q. A high neutrophil to lymphocyte ratio is associated with poor nutritional status in chronic kidney disease patients. Br. J. Nutr. 2022, 128, 1990–1996. [Google Scholar] [CrossRef] [PubMed]
- Ucha, I.; Mamven, M.; Adejumo, O.; Nwankwo, E.A. Malnutrition Inflammation Complex Syndrome in Pre-dialysis Chronic Kidney Disease Patients in a Nigerian Tertiary Hospital. West Afr. J. Med. 2022, 39, 1253–1259. [Google Scholar]
- Aggarwal, H.K.; Jain, D.; Chauda, R.; Bhatia, S.; Sehgal, R. Assessment of Malnutrition Inflammation Score in Different Stages of Chronic Kidney Disease. Pril Makedon Akad Nauk. Umet Odd Med. Nauk. 2018, 39, 51–61. [Google Scholar] [CrossRef] [Green Version]
- Giglio, J.; Kamimura, M.A.; Souza, N.C.; Bichels, A.V.; Cordeiro, A.C.; Pinho, N.; Avesani, C.M. Muscle mass assessment by computed tomography in chronic kidney disease patients: Agreement with surrogate methods. Eur. J. Clin. Nutr. 2019, 73, 46–53. [Google Scholar] [CrossRef]
- Cuppari, L.; Meireles, M.S.; Ramos, C.I.; Kamimura, M.A. Subjective global assessment for the diagnosis of protein-energy wasting in nondialysis-dependent chronic kidney disease patients. J. Ren. Nutr. 2014, 24, 385–389. [Google Scholar] [CrossRef]
- Low, S.; Pek, S.; Liu, Y.L.; Moh, A.; Ang, K.; Tang, W.E.; Lim, Z.; Subramaniam, T.; Sum, C.F.; Lim, C.L.; et al. Higher extracellular water to total body water ratio was associated with chronic kidney disease progression in type 2 diabetes. J. Diabetes Its Complicat. 2021, 35, 107930. [Google Scholar] [CrossRef] [PubMed]
- Bansal, N.; Zelnick, L.R.; Himmelfarb, J.; Chertow, G.M. Bioelectrical Impedance Analysis Measures and Clinical Outcomes in CKD. Am. J. Kidney Dis. 2018, 72, 662–672. [Google Scholar] [CrossRef] [PubMed]
- Barril, G.; Nogueira, A.; Alvarez-García, G.; Núñez, A.; Sánchez-González, C.; Ruperto, M. Nutritional Predictors of Mortality after 10 Years of Follow-Up in Patients with Chronic Kidney Disease at a Multidisciplinary Unit of Advanced Chronic Kidney Disease. Nutrients 2022, 14, 3848. [Google Scholar] [CrossRef] [PubMed]



| Assessment Tool | Item | Total (n, %) | Male (n, %) | Female (n, %) | p Value |
|---|---|---|---|---|---|
| SGA | Weight change | 11 (6.8%) | 6 (6.1%) | 5 (8.1%) | 0.75 |
| Dietary intake change | 20 (12.4%) | 15 (15.2%) | 5 (8.1%) | 0.185 | |
| Gastrointestinal symptoms | 13 (8.1%) | 6 (6.1%) | 7 (11.3%) | 0.236 | |
| Functional capacity | 67 (41.6%) | 38 (38.4%) | 29 (46.8%) | 0.293 | |
| Metabolic demand | 161 (100%) | 99 (100%) | 62 (100%) | – | |
| Subcutaneous fat loss | 61 (37.9%) | 36 (36.4%) | 25 (40.3%) | 0.614 | |
| Muscle wasting | 29 (18%) | 19 (19.2%) | 10 (16.1%) | 0.623 | |
| Edema | 38 (23.6%) | 22 (22.2%) | 16 (25.8%) | 0.602 | |
| Result of SGA | 32 (19.9%) | 18 (18.2%) | 14 (22.6%) | 0.496 | |
| PEW | Serum chemistry | 95 (59%) | 54 (54.5%) | 41 (66.1%) | 0.146 |
| Body mass | 55 (34.2%) | 26 (26.3%) | 29 (46.8%) | 0.008 | |
| Muscle mass | 17 (10.6%) | 10 (10.1%) | 7 (11.3%) | 0.811 | |
| Dietary intake | 116 (72%) | 68 (68.7%) | 48 (77.4%) | 0.23 | |
| Result of PEW | 32 (19.9%) | 17 (17.2%) | 15 (24.2%) | 0.277 | |
| Renal iNUT | Unintentional weight loss | 21 (13%) | 15 (15.2%) | 6 (9.7%) | 0.316 |
| BMI ≤ 20 kg/m2 | 16 (9.9%) | 3 (3%) | 13 (21%) | <0.001 | |
| Nutritional supplements | 85 (52.8%) | 47 (47.5%) | 38 (61.3%) | 0.087 | |
| Food intake | 20 (12.4%) | 15 (15.2%) | 5 (8.1%) | 0.185 | |
| Appetite | 18 (11.2%) | 12 (12.1%) | 6 (9.7%) | 0.632 | |
| Result of Renal iNUT | 35 (21.7%) | 21 (21.2%) | 14 (22.6%) | 0.838 |
| Renal iNUT | SGA | Sum | |
|---|---|---|---|
| Malnutrition | Non-Malnutrition | ||
| Malnutrition | 19 | 16 | 35 |
| Non-malnutrition | 13 | 113 | 126 |
| Sum | 32 | 129 | 161 |
| Renal iNUT | PEW | Sum | |
|---|---|---|---|
| PEW | Non-PEW | ||
| Malnutrition | 15 | 20 | 35 |
| Non-malnutrition | 17 | 109 | 126 |
| Sum | 32 | 129 | 161 |
| Variables | Non-Malnutrition (n = 129) | Malnutrition (n = 32) | p Value |
|---|---|---|---|
| Age (years) | 47 (37.5, 59) | 61.5 (54, 69) | <0.001 |
| Male, n (%) | 81 (62.8%) | 18 (56.3%) | 0.496 |
| CKD course (months) | 20 (9, 62) | 19.5 (9.25, 49.5) | 0.821 |
| Diabetes, n (%) | 57 (44.2%) | 18 (56.3%) | 0.221 |
| Hypertension, n (%) | 95 (73.6%) | 26 (81.3%) | 0.373 |
| WBC (×109/L) | 6.79 (5.71, 8.1) | 6.03 (4.98, 8.24) | 0.199 |
| NLR | 2.13 (1.58, 2.86) | 2.56 (1.81, 3.32) | 0.07 |
| CRP (mg/dL) | 0.09 (0.05, 0.16) | 0.1 (0.05, 0.21) | 0.625 |
| IL-6 (pg/mL) | 2.45 (2, 4.02) | 3.48 (2.06, 6.11) | 0.023 |
| Hemoglobin (g/L) | 121.04 ± 24.57 | 104.75 ± 18.59 | 0.001 |
| Total protein (g/L) | 58.59 ± 9.23 | 52.69 ± 10.01 | 0.002 |
| Albumin (g/L) | 37.4 (32.5, 41) | 31.05 (25.23, 35.95) | <0.001 |
| Prealbumin (mg/dL) | 29.18 (24.75, 33.55) | 25.6 (20.93, 31.43) | 0.034 |
| Transferrin (mg/dL) | 190.08 (168.5, 224.5) | 167 (143, 186.5) | <0.001 |
| Haptoglobin (mg/dL) | 128.03 (84.3, 161) | 125 (79.9, 172.5) | 0.912 |
| BUN (mmol/L) | 7.77 (5.41, 10.15) | 9.81 (6.14, 14.61) | 0.024 |
| Serum creatinine (umol/L) | 109.2 (74.75, 163.25) | 122.35 (78.6, 316.58) | 0.199 |
| eGFR (mL/min/1.73 m2) | 61.24 (35.46, 94.43) | 42.07 (16.53, 77) | 0.043 |
| Cystatin C (mg/L) | 1.52 (1.1, 1.9) | 1.8 (1.24, 2.91) | 0.015 |
| Uric acid (umol/L) | 377.07 ± 92.14 | 346.72 ± 101.06 | 0.104 |
| Total cholesterol (mmol/L) | 4.52 (3.83, 5.4) | 4.2 (3.45, 6.51) | 0.588 |
| Triglyceride (mmol/L) | 1.76 (1.23, 2.4) | 1.61 (1.22, 2) | 0.391 |
| FBG (mmol/L) | 4.64 (4.12, 5.25) | 4.8 (4.4, 5.5) | 0.164 |
| Serum calcium (mmol/L) | 2.18 (2.08, 2.27) | 2.09 (1.95, 2.25) | 0.017 |
| Serum potassium (mmol/L) | 3.89 (3.64, 4.08) | 3.85 (3.42, 4.61) | 0.997 |
| Serum phosphorus (mmol/L) | 1.24 ± 0.21 | 1.35 ± 0.27 | 0.012 |
| HDL-C (mmol/L) | 1.12 (0.92, 1.3) | 1.09 (0.9, 1.51) | 0.906 |
| LDL-C (mmol/L) | 2.66 (2.09, 3.35) | 2.54 (1.92, 4.12) | 0.719 |
| Dietary protein (g/kg/d) | 0.83 (0.64, 1.15) | 0.66 (0.55, 1.06) | 0.052 |
| Dietary energy (kcal/kg/d) | 19.33 (14.26, 25.85) | 16.38 (12.14, 21.04) | 0.044 |
| Variables | Non-Malnutrition (n = 129) | Malnutrition (n = 32) | p Value |
|---|---|---|---|
| BMI (kg/m2) | 25.18 ± 3.71 | 23.54 ± 3.38 | 0.024 |
| HGS (kg) | 30.24 ± 10.2 | 25.02 ± 8.08 | 0.008 |
| CC (cm) | 36.56 ± 3.49 | 35.17 ± 2.76 | 0.038 |
| TSF (cm) | 1.59 ± 0.5 | 1.46 ± 0.48 | 0.182 |
| MAC (cm) | 29.2 (27.45, 31.3) | 27.25 (26.1, 28.95) | 0.002 |
| MAMC (cm) | 26.1 (24.3, 27.65) | 24.05 (23.08, 25.68) | 0.002 |
| SMI (kg/m2) | 8.72 ± 1.4 | 8.83 ± 1.74 | 0.74 |
| Body protein (kg) | 10.61 ± 2.1 | 10.11 ± 2.21 | 0.229 |
| Body inorganic salts (kg) | 3.79 ± 0.76 | 3.61 ± 0.73 | 0.228 |
| Body bone mineral content (kg) | 3.11 (2.7, 3.53) | 2.83 (2.5, 3.34) | 0.091 |
| Body fat (kg) | 16.76 ± 7.12 | 12.96 ± 8.08 | 0.009 |
| BFP (%) | 23.2 ± 8.04 | 19.73 ± 12.08 | 0.131 |
| PhA (°) | 6.03 ± 1.03 | 4.88 ± 1.17 | <0.001 |
| Variables | B | P | OR | 95%CI | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Age | 1.914 | 0.001 | 6.78 | 2.252 | 20.413 |
| NLR | 1.351 | 0.012 | 3.862 | 1.344 | 11.104 |
| Transferrin | 1.44 | 0.036 | 4.222 | 1.099 | 16.218 |
| PhA | 2.012 | 0.001 | 7.478 | 2.229 | 25.093 |
| BFP | 2.951 | <0.001 | 19.119 | 4.404 | 83.003 |
| Constant | −4.675 | <0.001 | 0.009 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, Y.; Huang, H.; Wang, Q.; Lin, W.; Duan, S.; Zhou, J.; Huang, J.; Zhang, W.; Zheng, Y.; Tang, L.; et al. An Exploratory Study on a New Method for Nutritional Status Assessment in Patients with Chronic Kidney Disease. Nutrients 2023, 15, 2640. https://doi.org/10.3390/nu15112640
Luo Y, Huang H, Wang Q, Lin W, Duan S, Zhou J, Huang J, Zhang W, Zheng Y, Tang L, et al. An Exploratory Study on a New Method for Nutritional Status Assessment in Patients with Chronic Kidney Disease. Nutrients. 2023; 15(11):2640. https://doi.org/10.3390/nu15112640
Chicago/Turabian StyleLuo, Yayong, Hui Huang, Qian Wang, Wenwen Lin, Shuwei Duan, Jianhui Zhou, Jing Huang, Weiguang Zhang, Ying Zheng, Li Tang, and et al. 2023. "An Exploratory Study on a New Method for Nutritional Status Assessment in Patients with Chronic Kidney Disease" Nutrients 15, no. 11: 2640. https://doi.org/10.3390/nu15112640