
Effects of a 16-Week Digital Intervention on Sports Nutrition Knowledge and Behavior in Female Endurance Athletes with Risk of Relative Energy Deficiency in Sport (REDs)
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
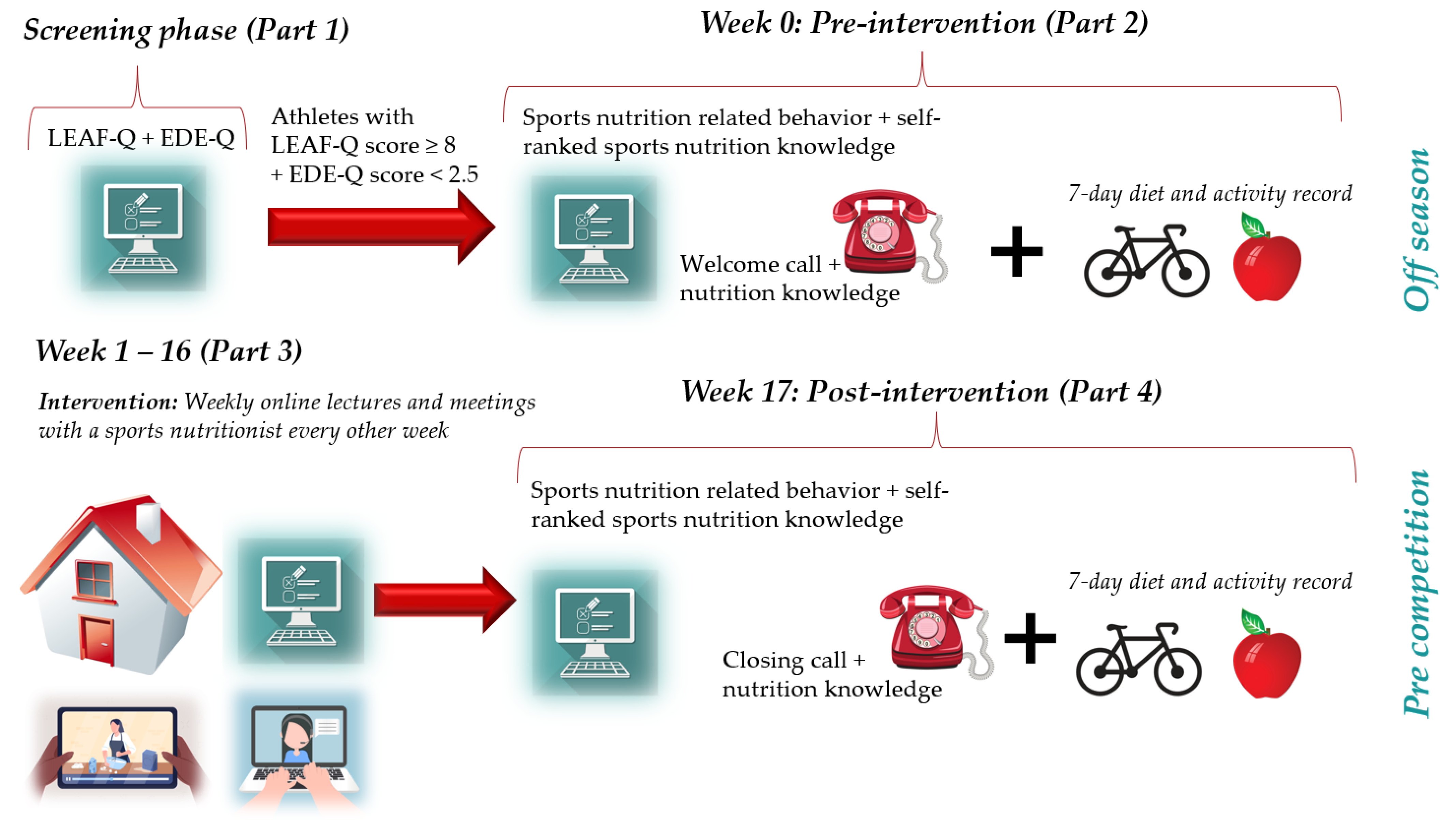
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
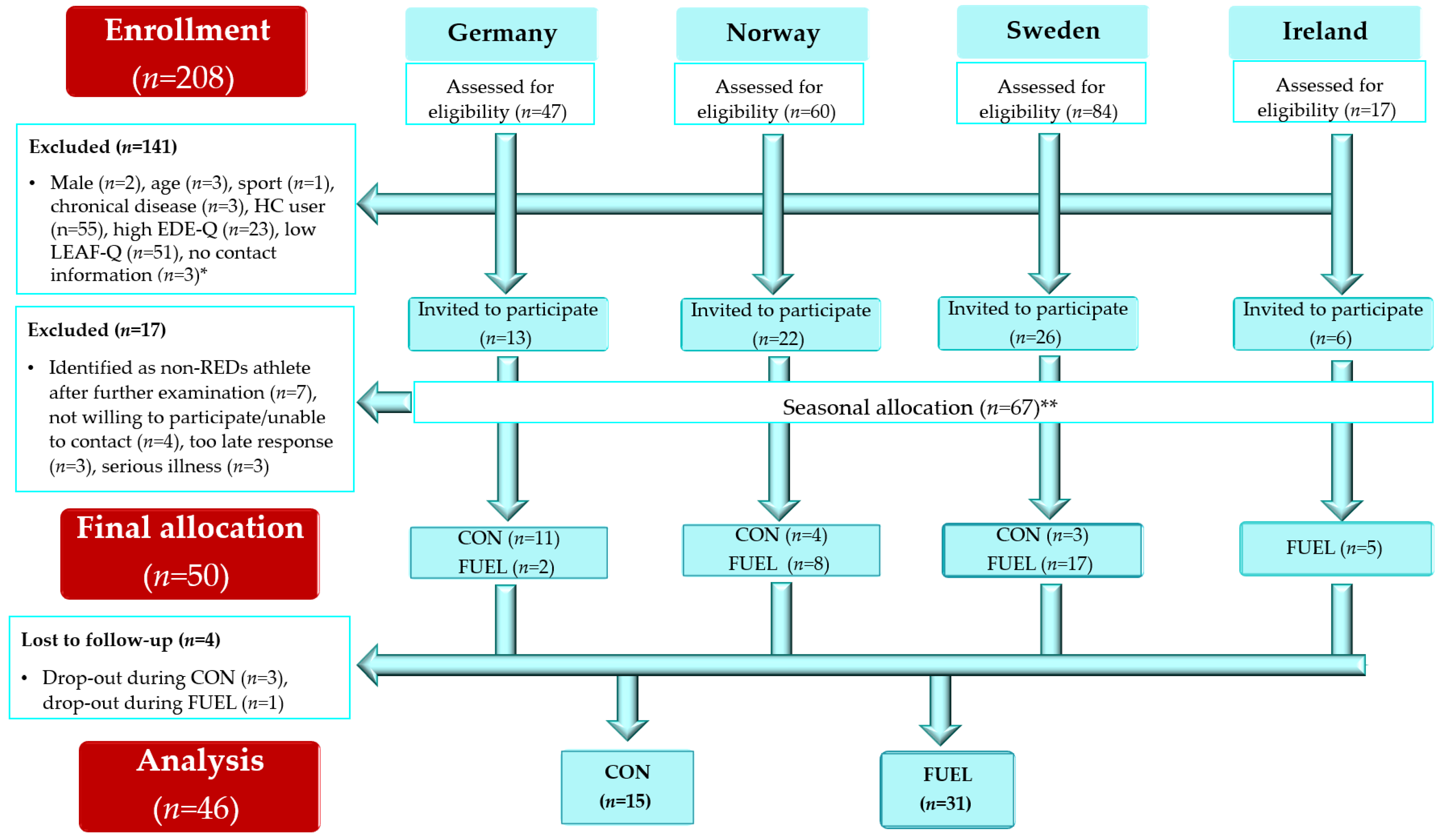
2.3. Recruitment and Eligibility
2.4. Nutrition Intervention
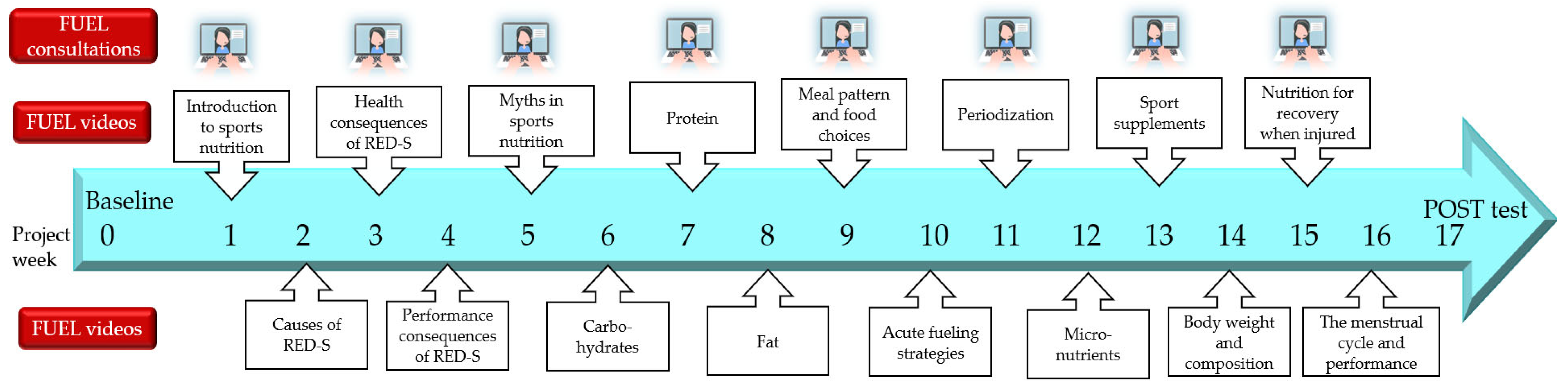
2.4.1. Sports Nutrition Lectures
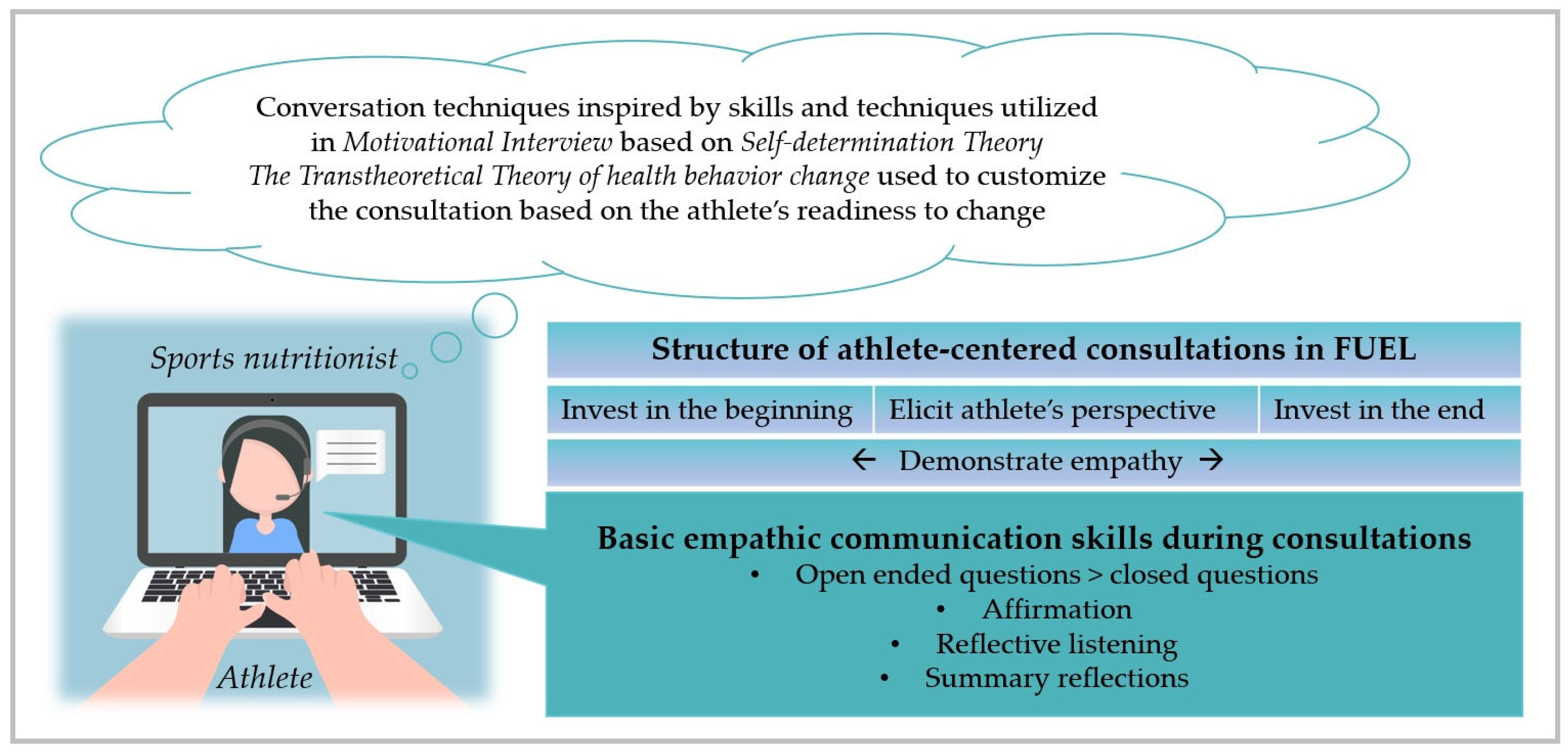
2.4.2. Athlete-Centered Nutrition Counseling
2.5. Sports Nutrition Knowledge
2.6. Sports Nutrition-Related Behavior and Dietary Intake
2.7. Physical Activity and Training
2.8. Statistics
3. Results
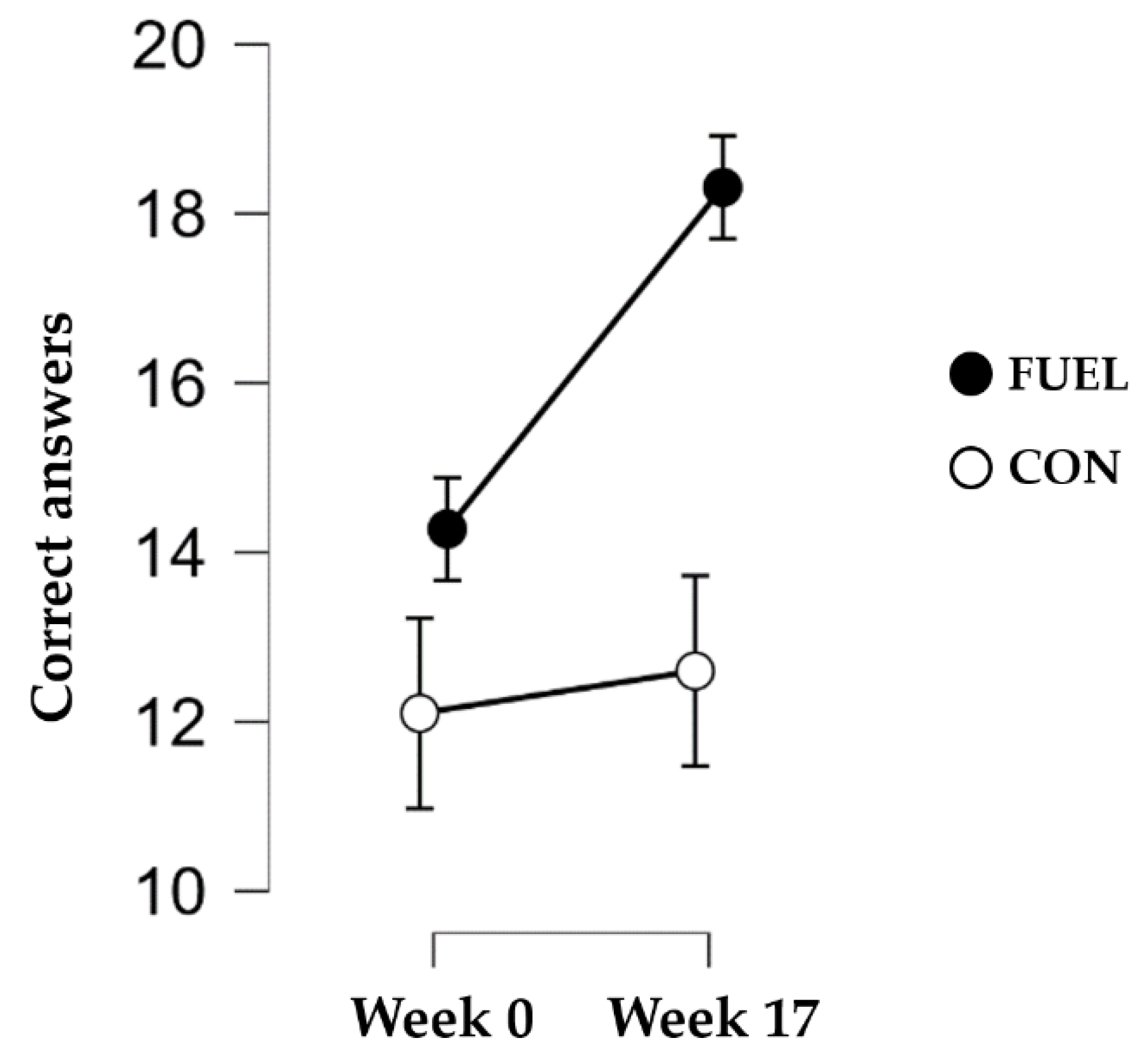
3.1. Sports Nutrition Knowledge
3.2. Sports Nutrition-Related Behavior, Overall Dietary Intake, and Physical Activity
4. Discussion
4.1. Strengths and Limitations
4.2. Future Directions
4.3. Practical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| BF | Bayes factor |
| BFincl | Bayes factor for inclusion of group x time interaction |
| BMI | Body mass index |
| CON | Control group |
| EDE-Q | Eating Disorder Examination Questionnaire |
| E% | Energy percentage |
| FUEL | Food and nUtrition for Endurance athletes—a Learning program |
| g | gram |
| HC | Hormonal contraceptives |
| kcal | Kilocalorie |
| kg | Kilogram |
| LEA | Low energy availability |
| LEAF-Q | Low Energy Availability in Females Questionnaire |
| RED-S | Relative Energy Deficiency in Sport |
| SD | Standard deviation |
| TSD | Services for Sensitive Data |
References
- Melin, A.; Tornberg, Å.B.; Skouby, S.; Faber, J.; Ritz, C.; Sjödin, A.; Sundgot-Borgen, J. The LEAF questionnaire: A screening tool for the identification of female athletes at risk for the female athlete triad. Br. J. Sport. Med. 2014, 48, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Mountjoy, M.; Sundgot-Borgen, J.K.; Burke, L.M.; Ackerman, K.E.; Blauwet, C.; Constantini, N.; Lebrun, C.; Lundy, B.; Melin, A.; Meyer, N.; et al. IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. Br. J. Sport. Med. 2018, 52, 687–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mountjoy, M.; Sundgot-Borgen, J.; Burke, L.; Carter, S.; Constantini, N.; Lebrun, C.; Meyer, N.; Sherman, R.; Steffen, K.; Budgett, R.; et al. The IOC consensus statement: Beyond the Female Athlete Triad-Relative Energy Deficiency in Sport (RED-S). Br. J. Sport. Med. 2014, 48, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Nattiv, A.; Loucks, A.B.; Manore, M.M.; Sanborn, C.F.; Sundgot-Borgen, J.; Warren, M.P. The female athlete triad. Med. Sci. Sport. Exerc. 2007, 39, 1867–1882. [Google Scholar] [CrossRef] [PubMed]
- Wasserfurth, P.; Palmowski, J.; Hahn, A.; Krüger, K. Reasons for and Consequences of Low Energy Availability in Female and Male Athletes: Social Environment, Adaptations, and Prevention. Sport. Med. Open 2020, 6, 44. [Google Scholar] [CrossRef]
- Melin, A.; Tornberg, Å.B.; Skouby, S.; Møller, S.S.; Sundgot-Borgen, J.; Faber, J.; Sidelmann, J.J.; Aziz, M.; Sjödin, A. Energy availability and the female athlete triad in elite endurance athletes. Scand. J. Med. Sci. Sport. 2015, 25, 610–622. [Google Scholar] [CrossRef]
- Fahrenholtz, I.L.; Melin, A.K.; Wasserfurth, P.; Stenling, A.; Logue, D.; Garthe, I.; Koehler, K.; Gräfnings, M.; Lichtenstein, M.B.; Madigan, S.; et al. Risk of Low Energy Availability, Disordered Eating, Exercise Addiction, and Food Intolerances in Female Endurance Athletes. Front. Sport. Act. Living 2022, 4, 869594. [Google Scholar] [CrossRef]
- Howe, S.M.; Hand, T.M.; Larson-Meyer, D.E.; Austin, K.J.; Alexander, B.M.; Manore, M.M. No effect of exercise intensity on appetite in highly-trained endurance women. Nutrients 2016, 8, 223. [Google Scholar] [CrossRef]
- Larson-Meyer, D.E.; Palm, S.; Bansal, A.; Austin, K.J.; Hart, A.M.; Alexander, B.M. Influence of running and walking on hormonal regulators of appetite in women. J. Obes. 2012, 2012, 730409. [Google Scholar] [CrossRef] [Green Version]
- Lodge, M.T.; Ackerman, K.E.; Garay, J. Knowledge of Triad and RED-S in Female Cross-Country Athletes and Support Staff. J. Athl. Train. 2021, 57, 385–392. [Google Scholar] [CrossRef]
- Logue, D.M.; Madigan, S.M.; Melin, A.; Delahunt, E.; Heinen, M.; Donnell, S.J.M.; Corish, C.A. Low Energy Availability in Athletes 2020: An Updated Narrative Review of Prevalence, Risk, Within-Day Energy Balance, Knowledge, and Impact on Sports Performance. Nutrients 2020, 12, 835. [Google Scholar] [CrossRef] [Green Version]
- Benardot, D. Fear of Calories-Part I. Peak Run. Perform. 2009, 18, 11–15. [Google Scholar]
- Coelho, G.; de Abreu Soares, E.; Innocencio da Silva Gomes, A.; Goncalves Ribeiro, B. Prevention of eating disorders in female athletes. Open Access J. Sport. Med. 2014, 5, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Jeukendrup, A.E.; Killer, S.C. The myths surrounding pre-exercise carbohydrate feeding. Ann. Nutr. Metab. 2011, 57 (Suppl. S2), 18–25. [Google Scholar] [CrossRef]
- Verhoef, S.J.; Wielink, M.C.; Achterberg, E.A.; Bongers, M.Y.; Goossens, S.M.T.A. Absence of menstruation in female athletes: Why they do not seek help. BMC Sport. Sci. Med. Rehabil. 2021, 13, 146. [Google Scholar] [CrossRef]
- Melin, A.; Tornberg, Å.; Skouby, S.; Møller, S.S.; Faber, J.; Sundgot-Borgen, J.; Sjödin, A. Low-energy density and high fiber intake are dietary concerns in female endurance athletes. Scand. J. Med. Sci. Sport. 2016, 26, 1060–1071. [Google Scholar] [CrossRef]
- Barron, E.; Cano Sokoloff, N.; Maffazioli, G.D.N.; Ackerman, K.E.; Woolley, R.; Holmes, T.M.; Anderson, E.J.; Misra, M. Diets High in Fiber and Vegetable Protein Are Associated with Low Lumbar Bone Mineral Density in Young Athletes with Oligoamenorrhea. J. Acad. Nutr. Diet. 2016, 116, 481–489. [Google Scholar] [CrossRef] [Green Version]
- Laughlin, G.A.; Yen, S.S. Nutritional and endocrine-metabolic aberrations in amenorrheic athletes. J. Clin. Endocrinol. Metab. 1996, 81, 4301–4309. [Google Scholar]
- Heikura, I.A.; Uusitalo, A.L.T.; Stellingwerff, T.; Bergland, D.; Mero, A.A.; Burke, L.M. Low Energy Availability is Difficult to Assess But Outcomes Have Large Impact on Bone Injury Rates in Elite Distance Athletes. Int. J. Sport Nutr. Exerc. Metab. 2017, 28, 403–411. [Google Scholar] [CrossRef] [Green Version]
- Matt, S.A.; Barrack, M.T.; Gray, V.B.; Cotter, J.A.; Van Loan, M.D.; Rauh, M.J.; McGowan, R.; Nichols, J.F. Adolescent Endurance Runners Exhibit Suboptimal Energy Availability and Intakes of Key Nutrients. J. Am. Coll. Nutr. 2021, 41, 551–558. [Google Scholar] [CrossRef]
- Carr, A.; McGawley, K.; Govus, A.; Andersson, E.P.; Shannon, O.M.; Mattsson, S.; Melin, A.K. Nutritional Intake in Elite Cross-Country Skiers During Two Days of Training and Competition. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Birkenhead, K.L.; Slater, G. A Review of Factors Influencing Athletes’ Food Choices. Sport. Med. 2015, 45, 1511–1522. [Google Scholar] [CrossRef] [PubMed]
- Trakman, G.; Forsyth, A.; Devlin, B.; Belski, R. A Systematic Review of Athletes’ and Coaches’ Nutrition Knowledge and Reflections on the Quality of Current Nutrition Knowledge Measures. Nutrients 2016, 8, 570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kettunen, O.; Heikkilä, M.; Linnamo, V.; Ihalainen, J.K. Nutrition Knowledge Is Associated with Energy Availability and Carbohydrate Intake in Young Female Cross-Country Skiers. Nutrients 2021, 13, 1769. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, K.E.; Stellingwerff, T.; Elliott-Sale, K.J.; Baltzell, A.; Cain, M.; Goucher, K.; Fleshman, L.; Mountjoy, M.L. #REDS (Relative Energy Deficiency in Sport): Time for a revolution in sports culture and systems to improve athlete health and performance. Br. J. Sport. Med. 2020, 54, 369–370. [Google Scholar]
- Gastrich, M.D.; Quick, V.; Bachmann, G.; Moriarty, A.M. Nutritional Risks among Female Athletes. J. Women’s Health 2020, 29, 693–702. [Google Scholar] [CrossRef]
- Nose-Ogura, S.; Yoshino, O.; Dohi, M.; Kigawa, M.; Harada, M.; Kawahara, T.; Osuga, Y.; Saito, S. Low Bone Mineral Density in Elite Female Athletes With a History of Secondary Amenorrhea in Their Teens. Clin. J. Sport. Med. 2018, 30, 245–250. [Google Scholar] [CrossRef]
- Keen, A.D.; Drinkwater, B.L. Irreversible bone loss in former amenorrheic athletes. Osteoporos. Int. 1997, 7, 311–315. [Google Scholar] [CrossRef]
- Heikkilä, M.; Valve, R.; Lehtovirta, M.; Fogelholm, M. Nutrition Knowledge Among Young Finnish Endurance Athletes and Their Coaches. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 522–527. [Google Scholar] [CrossRef]
- Logue, D.M.; Mahony, L.; Corish, C.A.; Tobin, D.; Doherty, R.; O’Higgins, G.; Madigan, S. Athletes’ and Coaches’ Perceptions of Nutritional Advice: Eating More Food for Health and Performance. Nutrients 2021, 13, 1925. [Google Scholar] [CrossRef]
- Pelly, F.E.; Thurecht, R.L.; Slater, G. Determinants of Food Choice in Athletes: A Systematic Scoping Review. Sport. Med.-Open 2022, 8, 77. [Google Scholar] [CrossRef]
- Tam, R.; Beck, K.L.; Manore, M.M.; Gifford, J.; Flood, V.M.; Connor, H.O. Effectiveness of Education Interventions Designed to Improve Nutrition Knowledge in Athletes: A Systematic Review. Sport. Med. 2019, 49, 1769–1786. [Google Scholar] [CrossRef]
- Kuikman, M.A.; Mountjoy, M.; Stellingwerff, T.; Burr, J.F. A Review of Nonpharmacological Strategies in the Treatment of Relative Energy Deficiency in Sport. Int. J. Sport Nutr. Exerc. Metab. 2021, 31, 268–275. [Google Scholar] [CrossRef]
- Robertson, S.; Mountjoy, M. A Review of Prevention, Diagnosis, and Treatment of Relative Energy Deficiency in Sport in Artistic (Synchronized) Swimming. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Joy, E.; de Souza, M.J.; Nattiv, A.; Misra, M.; Williams, N.I.; Mallinson, R.J.; Gibbs, J.; Olmsted, M.; Goolsby, M.; Matheson, G.; et al. 2014 Female Athlete Triad Coalition Consensus Statement on Treatment and Return to Play of the Female Athlete Triad. Curr. Sport. Med. Rep. 2014, 13, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Dueck, C.A.; Matt, K.S.; Manore, M.M.; Skinner, J.S. Treatment of athletic amenorrhea with a diet and training intervention program. Int. J. Sport Nutr. 1996, 6, 24–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopp-Woodroffe, S.A.; Manore, M.M.; Dueck, C.A.; Skinner, J.S.; Matt, K.S. Energy and nutrient status of amenorrheic athletes participating in a diet and exercise training intervention program. Int. J. Sport Nutr. 1999, 9, 70–88. [Google Scholar] [CrossRef] [PubMed]
- Mallinson, R.J.; Williams, N.I.; Olmsted, M.P.; Scheid, J.L.; Riddle, E.S.; De Souza, M.J. A case report of recovery of menstrual function following a nutritional intervention in two exercising women with amenorrhea of varying duration. J. Int. Soc. Sport. Nutr. 2013, 10, 34. [Google Scholar] [CrossRef] [Green Version]
- Cialdella-Kam, L.; Guebels, C.P.; Maddalozzo, G.F.; Manore, M.M. Dietary intervention restored menses in female athletes with exercise-associated menstrual dysfunction with limited impact on bone and muscle health. Nutrients 2014, 6, 3018–3039. [Google Scholar] [CrossRef] [Green Version]
- Łagowska, K.; Kapczuk, K.; Friebe, Z.; Bajerska, J. Effects of dietary intervention in young female athletes with menstrual disorders. J. Int. Soc. Sport. Nutr. 2014, 11, 21. [Google Scholar] [CrossRef] [Green Version]
- De Souza, M.J.; Mallinson, R.J.; Strock, N.C.A.; Koltun, K.J.; Olmsted, M.P.; Ricker, E.A.; Scheid, J.L.; Allaway, H.C.; Mallinson, D.J.; Don, P.K.; et al. Randomised controlled trial of the effects of increased energy intake on menstrual recovery in exercising women with menstrual disturbances: The ‘REFUEL’ study. Hum. Reprod. 2021, 36, 2285–2297. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Beglin, S.J. Assessment of eating disorder psychopathology: Interview or self-report questionnaire. Int. J. Eat. Disord. 1994, 16, 363–370. [Google Scholar] [CrossRef]
- Rø, Ø.; Reas, D.L.; Stedal, K. Eating Disorder Examination Questionnaire (EDE-Q) in Norwegian Adults: Discrimination between Female Controls and Eating Disorder Patients. Eur. Eat. Disord. Rev. 2015, 23, 408–412. [Google Scholar] [CrossRef]
- Kuikman, M.A.; Mountjoy, M.; Burr, J.F. Examining the Relationship between Exercise Dependence, Disordered Eating, and Low Energy Availability. Nutrients 2021, 13, 2601. [Google Scholar] [CrossRef]
- McKay, A.K.A.; Stellingwerff, T.; Smith, E.S.; Martin, D.T.; Mujika, I.; Goosey-Tolfrey, V.L.; Sheppard, J.; Burke, L.M. Defining Training and Performance Caliber: A Participant Classification Framework. Int. J. Sport. Physiol. Perform. 2022, 17, 317–331. [Google Scholar] [CrossRef]
- Burke, L.M.; Castell, L.M.; Casa, D.J.; Close, G.L.; Costa, R.J.S.; Desbrow, B.; Halson, S.L.; Lis, D.M.; Melin, A.K.; Peeling, P.; et al. International Association of Athletics Federations Consensus Statement 2019: Nutrition for Athletics. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance. Med. Sci. Sport. Exerc. 2016, 48, 543–568. [Google Scholar]
- Rollo, I.; Gonzalez, J.T.; Fuchs, C.J.; van Loon, L.J.C.; Williams, C. Primary, Secondary, and Tertiary Effects of Carbohydrate Ingestion During Exercise. Sport. Med. 2020, 50, 1863–1871. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The Behavior Change Technique Taxonomy (v1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Sheeran, P.; Wright, C.E.; Avishai, A.; Villegas, M.E.; Lindemans, J.W.; Klein, W.M.P.; Rothman, A.J.; Miles, E.; Ntoumanis, N. Self-determination theory interventions for health behavior change: Meta-analysis and meta-analytic structural equation modeling of randomized controlled trials. J. Consult. Clin. Psychol. 2020, 88, 726–737. [Google Scholar] [CrossRef]
- William, R.; Miller, S.R. Motivational Interviewing: Helping People Change, 3rd ed.; Guilford Press: New York, NY, USA, 2012; 482p. [Google Scholar]
- Norcross, J.C.; Krebs, P.M.; Prochaska, J.O. Stages of Change. In Psychotherapy Relationships That Work, 2nd ed.; Oxford University Press: Oxford, UK, 2011; pp. 279–300. [Google Scholar]
- Frankel, R.M.; Stein, T. Getting the Most out of the Clinical Encounter: The Four Habits Model. Perm. J. 1999, 3, 79–88. [Google Scholar] [CrossRef]
- Krupat, E.; Frankel, R.; Stein, T.; Irish, J. The Four Habits Coding Scheme: Validation of an instrument to assess clinicians’ communication behavior. Patient Educ. Couns. 2006, 62, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Mountjoy, M.; Sundgot-Borgen, J.; Burke, L.; Carter, S.; Constantini, N.; Lebrun, C.; Meyer, N.; Sherman, R.; Steffen, K.; Budgett, R.; et al. The IOC relative energy deficiency in sport clinical assessment tool (RED-S CAT). Br. J. Sport. Med. 2015, 49, 1354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heikkilä, M.; Valve, R.; Lehtovirta, M.; Fogelholm, M. Development of a nutrition knowledge questionnaire for young endurance athletes and their coaches. Scand. J. Med. Sci. Sport. 2018, 28, 873–880. [Google Scholar] [CrossRef]
- Kost och Näringsdata. Dietist Net Pro. Available online: http://www.kostdata.se/se/dietist-net/dietist-net-pro (accessed on 18 January 2023).
- Nutritics. Nutritics. Available online: https://www.nutritics.com/en/ (accessed on 18 January 2023).
- EBISpro. EBISpro. Available online: http://www.ebispro.de/ (accessed on 18 January 2023).
- Kerksick, C.M.; Wilborn, C.D.; Roberts, M.D.; Smith-ryan, A.; Kleiner, S.M.; Jäger, R.; Collins, R.; Cooke, M.; Davis, J.N.; Galvan, E. ISSN exercise & sports nutrition review update: Research & recommendations. J. Int. Soc. Sport. Nutr. 2018, 15, 38. [Google Scholar]
- Burke, L.M.; Hawley, J.A.; Wong, S.H.S.; Jeukendrup, A.E. Carbohydrates for training and competition. J. Sport. Sci. 2011, 29 (Suppl. S1), S17–S27. [Google Scholar] [CrossRef]
- Wagenmakers, E.J.; Marsman, M.; Jamil, T.; Ly, A.; Verhagen, J.; Love, J.; Selker, R.; Gronau, Q.F.; Šmíra, M.; Epskamp, S.; et al. Bayesian inference for psychology. Part I: Theoretical advantages and practical ramifications. Psychon. Bull. Rev. 2018, 25, 35–57. [Google Scholar] [CrossRef]
- Van de Schoot, R.; Kaplan, D.; Denissen, J.; Asendorpf, J.B.; Neyer, F.J.; van Aken, M.A.G. A Gentle Introduction to Bayesian Analysis: Applications to Developmental Research. Child Dev. 2014, 85, 842–860. [Google Scholar] [CrossRef]
- Van den Bergh, D.; van Doorn, J.; Marsman, M.; Draws, T.; van Kesteren, E.J.; Derks, K.; Dablander, F.; Gronau, Q.F.; Kucharský, Š.; Raj, A.; et al. A Tutorial on Conducting and Interpreting a Bayesian ANOVA in JASP. LAnnee Psychol. 2020, 120, 73–96. [Google Scholar] [CrossRef]
- Van Doorn, J.; van den Bergh, D.; Böhm, U.; Dablander, F.; Derks, K.; Draws, T.; Etz, A.; Evans, N.J.; Gronau, Q.F.; Haaf, J.M.; et al. The JASP guidelines for conducting and reporting a Bayesian analysis. Psychon. Bull. Rev. 2021, 28, 813–826. [Google Scholar] [CrossRef]
- Worsley, A. Nutrition knowledge and food consumption: Can nutrition knowledge change food behaviour? Asia Pac. J. Clin. Nutr. 2002, 11, S579–S585. [Google Scholar] [CrossRef] [Green Version]
- Bentley, M.R.N.; Mitchell, N.; Backhouse, S.H. Sports nutrition interventions: A systematic review of behavioural strategies used to promote dietary behaviour change in athletes. Appetite 2020, 150, 104645. [Google Scholar] [CrossRef]
- Heaney, S.; O’Connor, H.; Michael, S.; Gifford, J.; Naughton, G. Nutrition knowledge in athletes: A systematic review. Int. J. Sport Nutr. Exerc. Metab. 2011, 21, 248–261. [Google Scholar] [CrossRef] [Green Version]
- Heikkilä, M.; Lehtovirta, M.; Autio, O.; Fogelholm, M.; Valve, R. The Impact of Nutrition Education Intervention with and Without a Mobile Phone Application on Nutrition Knowledge Among Young Endurance Athletes. Nutrients 2019, 11, 2249. [Google Scholar] [CrossRef] [Green Version]
- Beggs, V.C.E.; Nolte, V.W.; Dickey, J.P. The Impact of Nutritional Counseling in Conjunction with Co-active Coaching on Behavior Change of Varsity Female Rowers. Sport. Nutr. Ther. 2016, 1, 1000112. [Google Scholar]
- Nordic Council of Ministers. Nordic Nutrition Recommendations 2012; Nordic Council of Ministers: Copenhagen, Denmark, 2008; Volume 5, pp. 1–3. [Google Scholar]
- Lagowska, K.; Kapczuk, K.; Jeszka, J. Nine-month nutritional intervention improves restoration of menses in young female athletes and ballet dancers. J. Int. Soc. Sport. Nutr. 2014, 11, 52. [Google Scholar] [CrossRef] [Green Version]
- Murimi, M.W.; Kanyi, M.; Mupfudze, T.; Amin, R.; Mbogori, T.; Aldubayan, K. Systematic Review Factors Influencing Efficacy of Nutrition Education Interventions: A Systematic Review. J. Nutr. Educ. Behav. 2017, 49, 142–165.e1. [Google Scholar] [CrossRef]
- Stickler, L.G.; Hoogenboom, B.J.; Brown, J. The Impact of Nutritional Intervention on Menstrual Dysfunction in Female Athletes: A Systematic Review. SN Compr. Clin. Med. 2019, 1, 669–676. [Google Scholar] [CrossRef] [Green Version]
- Tam, R.; Gifford, J.A.; Beck, K.L. Recent Developments in the Assessment of Nutrition Knowledge in Athletes. Curr. Nutr. Rep. 2022, 11, 241–252. [Google Scholar] [CrossRef]
- Jesus, F.; Sousa, M.; Nunes, C.L.; Francisco, R.; Rocha, P.; Minderico, C.S.; Sardinha, L.B.; Silva, A.M. Energy Availability Over One Athletic Season: An Observational Study Among Athletes From Different Sports. Int. J. Sport Nutr. Exerc. Metab. 2022, 32, 479–490. [Google Scholar] [CrossRef]
- Hamer, J.; Desbrow, B.; Irwin, C. Are Coaches of Female Athletes Informed of Relative Energy Deficiency in Sport? A Scoping Review. Women Sport Phys. Act. J. 2021, 29, 38–46. [Google Scholar] [CrossRef]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Preparation | Beginning | Work Part | Conclusion | Reflection |
|---|---|---|---|---|
|
|
|
|
|
| ← Maintain alliance ∙ Express empathy ∙ Support autonomy ∙ Support mastery ∙ Give information → | ||||
| FUEL (n = 31) | CON (n = 15) | |
|---|---|---|
| Age (years) | 24.1 ± 4.7 | 25.3 ± 4.8 |
| Height (cm) | 169.3 ± 6.2 | 171.2 ± 7.1 |
| Body weight (kg) | 59.5 ± 7.0 | 59.3 ± 5.0 |
| BMI (kg/m2) | 20.8 ± 2.1 | 20.3 ± 1.7 |
| Training volume (h/month) | 46.3 ± 16.7 | 48.6 ± 17.7 |
| Full-time athlete (%) | 16.1 | 20.0 |
| Occupation 1 | ||
| Full-time job (%) | 45.2 | 33.3 |
| Part-time job (%) | 0.0 | 0.0 |
| Studying (%) | 38.7 | 40.0 |
| Other (%) | 0.0 | 6.6 |
| Level of competition | ||
| Club (%) | 64.5 | 86.7 |
| National team (%) | 19.4 | 6.7 |
| Professional (%) | 9.7 | 6.7 |
| Other (%) | 6.5 | 0.0 |
| Level of education | ||
| Primary school (%) | 0.0 | 0.0 |
| Secondary school (%) | 25.8 | 46.7 |
| University/college < 4 years (%) | 48.4 | 20.0 |
| University/college ≥ 4 years (%) | 25.8 | 33.3 |
| FUEL | CON | ||||||
|---|---|---|---|---|---|---|---|
| Statements Rated on a Scale from 1 to 10 (1 = Totally Disagree, 10 = Fully Agree) | Week 0 | Week 17 | Within Group Difference | Week 0 | Week 17 | Within Group Difference | BFincl |
| I have great knowledge in the field of sports nutrition | 5.8 ± 1.9 | 8.1 ± 1.5 | 2.2 ± 1.6 | 7.0 ± 1.5 | 6.7 ± 1.9 | −0.3 ± 1.6 | 592.02 |
| I have followed all sports nutrition recommendations I can | 5.3 ± 1.8 | 7.6 ± 1.7 | 2.2 ± 2.0 | 5.8 ± 1.9 | 5.3 ± 1.8 | −0.4 ± 2.2 | 68.88 |
| There has been agreement between how I have eaten and my theoretical knowledge of sports nutrition | 6.4 ± 1.6 | 7.8 ± 1.4 | 1.4 ± 1.9 | 4.5 ± 1.4 | 4.8 ± 2.2 | 0.3 ± 2.8 | 0.94 |
| I have confidence in my nutrition routines | 6.0 ± 1.6 | 7.8 ± 1.4 | 1.8 ± 2.2 | 5.8 ± 2.0 | 5.8 ± 2.1 | 0.1 ± 2.8 | 9.38 |
| I have known where I should gather research-based information about sports nutrition | 5.3 ± 2.9 | 8.7 ± 1.6 | 3.5 ± 2.8 | 6.0 ± 2.9 | 6.8 ± 2.7 | 0.8 ± 3.1 | 8.70 |
| FUEL | CON | BFincl | |||||
|---|---|---|---|---|---|---|---|
| Dietary Intake | Week 0 | Week 17 | within Group Difference | Week 0 | Week 17 | within Group Difference | |
| Energy intake (kcal/day) | 2588 ± 528 | 2726 ± 547 | 138 ± 453 | 2455 ± 482 | 2300 ± 449 | −155 ± 396 | 1.03 |
| Carbohydrates (g/day) Carbohydrates (g/kg/day) Carbohydrates (E%) | 290 ± 68 | 326 ± 88 | 36 ± 74 | 285 ± 65 | 280 ± 74 | −6 ± 62 | 1.09 |
| 4.8 ± 1.0 | 5.5 ± 1.4 | 0.6 ± 1.3 | 4.8 ± 1.0 | 4.7 ± 1.2 | −0.1 ± 1.0 | 1.04 | |
| 47 ± 8 | 50 ± 8 | 2.7 ± 9.4 | 49 ± 5 | 51 ± 6 | 2.2 ± 5.4 | 0.38 | |
| Dietary fibers (g/day) | 37.5 ± 12.5 | 36.7 ± 12.7 | −1 ± 10 | 36 ± 9 | 37 ± 15 | 1 ± 12 | 0.37 |
| Dietary fibers (g/1000 kcal) | 14.4 ± 3.8 | 13.3 ± 3.1 | −1.1 ± 3.2 | 14.9 ± 3.6 | 15.9 ± 5.2 | 1.0 ± 4.7 | 0.88 |
| Protein (g/day) | 107 ± 30 | 115 ± 31 | 8 ± 22 | 95 ± 19 | 88 ± 24 | −7 ± 17 | 1.06 |
| Protein (g/kg/day) | 1.8 ± 0.5 | 1.9 ± 0.5 | 0.1 ± 0.4 | 1.6 ± 0.3 | 1.5 ± 0.4 | −0.1 ± 0.3 | 1.12 |
| Protein (E%) | 17 ± 4 | 18 ± 4 | 3 ± 3 | 17 ± 4 | 16 ± 4 | −1 ± 2 | 0.42 |
| Fat (g/day) | 106 ± 35 | 96 ± 26 | −10 ± 34 | 97 ± 24 | 88 ± 23 | −9 ± 23 | 0.36 |
| Fat (g/kg/day) | 1.8 ± 0.6 | 1.6 ± 0.4 | −0.2 ± 0.6 | 1.6 ± 0.3 | 1.4 ± 0.4 | −0.2 ± 0.4 | 0.38 |
| Fat (E%) | 37 ± 9 | 32 ± 6 | −5 ± 9 | 35 ± 5 | 34 ± 7 | −1 ± 7 | 1.43 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fahrenholtz, I.L.; Melin, A.K.; Garthe, I.; Hollekim-Strand, S.M.; Ivarsson, A.; Koehler, K.; Logue, D.; Lundström, P.; Madigan, S.; Wasserfurth, P.; et al. Effects of a 16-Week Digital Intervention on Sports Nutrition Knowledge and Behavior in Female Endurance Athletes with Risk of Relative Energy Deficiency in Sport (REDs). Nutrients 2023, 15, 1082. https://doi.org/10.3390/nu15051082
Fahrenholtz IL, Melin AK, Garthe I, Hollekim-Strand SM, Ivarsson A, Koehler K, Logue D, Lundström P, Madigan S, Wasserfurth P, et al. Effects of a 16-Week Digital Intervention on Sports Nutrition Knowledge and Behavior in Female Endurance Athletes with Risk of Relative Energy Deficiency in Sport (REDs). Nutrients. 2023; 15(5):1082. https://doi.org/10.3390/nu15051082
Chicago/Turabian StyleFahrenholtz, Ida L., Anna K. Melin, Ina Garthe, Siri Marte Hollekim-Strand, Andreas Ivarsson, Karsten Koehler, Danielle Logue, Petra Lundström, Sharon Madigan, Paulina Wasserfurth, and et al. 2023. "Effects of a 16-Week Digital Intervention on Sports Nutrition Knowledge and Behavior in Female Endurance Athletes with Risk of Relative Energy Deficiency in Sport (REDs)" Nutrients 15, no. 5: 1082. https://doi.org/10.3390/nu15051082