
The Relationships between Parenting Practices and Child Health-Related Behaviors in Children with Intellectual Disability: The Moderating Role of Child Body Weight Status
 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Methods
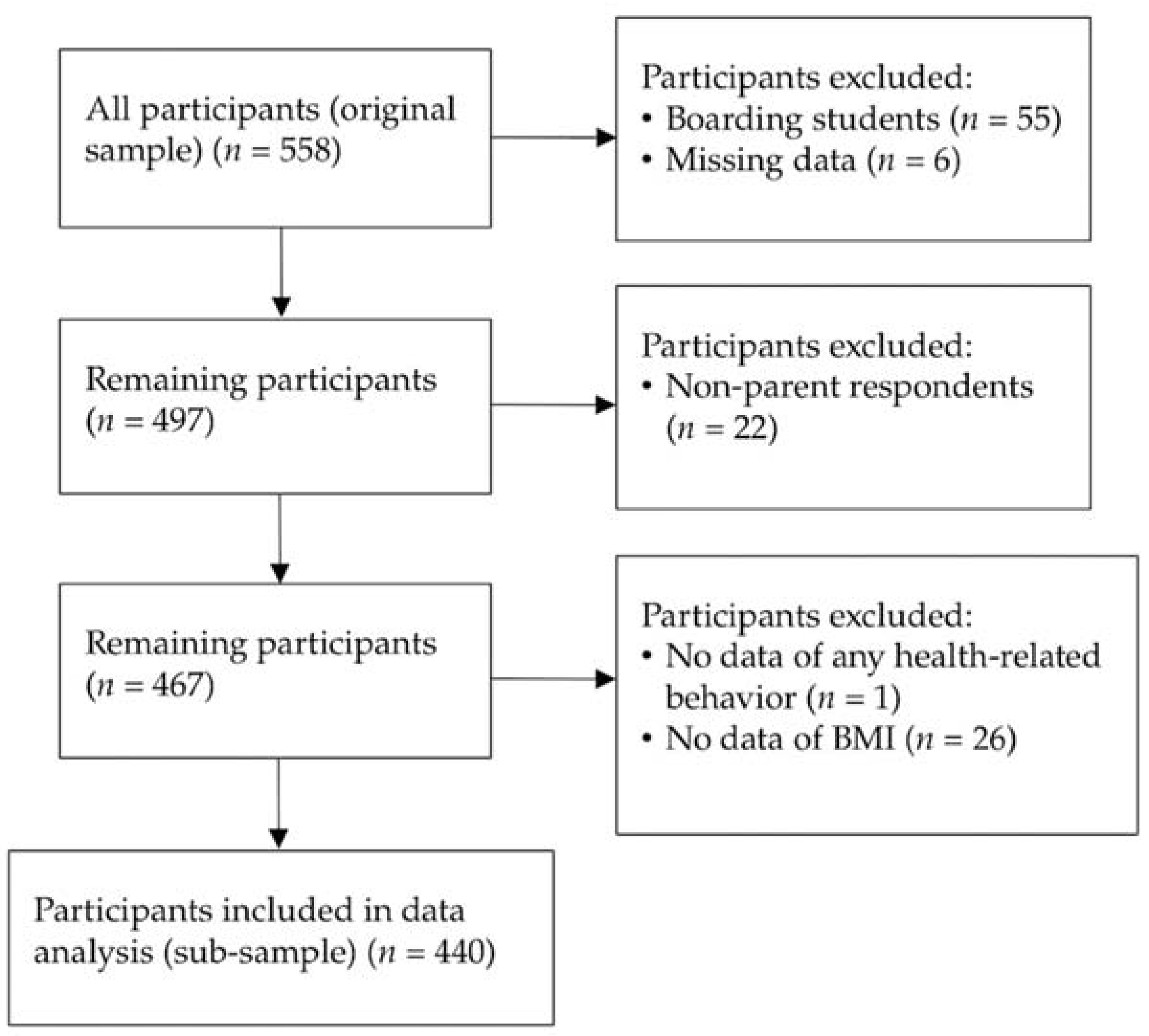
2.1. Study Design and Participants
2.2. Measures
2.2.1. Background Characteristics of the Participants
2.2.2. Parenting Practices
2.2.3. Children’s Health-Related Behaviors
2.2.4. Child Body Weight Status
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hinckson, E.A.; Curtis, A. Measuring physical activity in children and youth living with intellectual disabilities: A sys-tematic review. Res. Dev. Disabil. 2013, 34, 72–86. [Google Scholar] [CrossRef] [PubMed]
- Rimmer, J.H.; Yamaki, K.; Lowry, B.M.D.; Wang, E.; Vogel, L.C. Obesity and obesity-related secondary conditions in adolescents with intellectual/developmental disabilities. J. Intellect. Disabil. Res. 2010, 54, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.Q.; Liu, Y.; Wang, M.J.; Hou, X.; Zhang, S.H.; Wang, X.L.; Han, Y.N.; Sang, P.; Bian, Y.; Roswal, G. Prevalence of overweight and obesity in children and adolescents with intellectual disabilities in China. J. Intellect. Disabil. Res. 2021, 65, 655–665. [Google Scholar] [CrossRef] [PubMed]
- Krahn, G.L.; Hammond, L.; Turner, A. A cascade of disparities: Health and health care access for people with intellectual disabilities. Ment. Retard. Dev. Disabil. Res. Rev. 2006, 12, 70–82. [Google Scholar] [CrossRef] [PubMed]
- Census and Statistics Department. Special Topics Report No.62, in Persons with Disabilities and Chronic Diseases; Census and Statistics Department: Hong Kong, China, 2014; pp. 249–250.
- Wang, J.; Gao, Y.; Kwok, H.H.; Huang, W.Y.; Li, S.; Li, L. Children with Intellectual Disability Are Vulnerable to Overweight and Obesity: A Cross-Sectional Study among Chinese Children. Child. Obes. 2018, 14, 316–326. [Google Scholar] [CrossRef] [PubMed]
- Yamaki, K.; Rimmer, J.H.; Lowry, B.D.; Vogel, L.C. Prevalence of obesity-related chronic health conditions in overweight adolescents with disabilities. Res. Dev. Disabil. 2011, 32, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Mikulovic, J.; Vanhelst, J.; Salleron, J.; Marcellini, A.; Compte, R.; Fardy, P.S.; Bui-Xuan, G. Overweight in intellectually-disabled pop-ulation: Physical, behavioral and psychological characteristics. Res. Dev. Disabil. 2014, 35, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Golan, M.; Crow, S. Parents are key players in the prevention and treatment of weight-related problems. Nutr Rev. 2004, 62, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Beighton, C.; Wills, J. How parents describe the positive aspects of parenting their child who has intellectual disa-bilities: A systematic review and narrative synthesis. J. Appl. Res. Intellect. Disabil. 2019, 32, 1255–1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyd, M.J.; Iacono, T.; McDonald, R. The Perceptions of Fathers About Parenting a Child with Developmental Disability: A Scoping Review. J. Policy Pract. Intellect. Disabil. 2019, 16, 312–324. [Google Scholar] [CrossRef]
- Darling, N.; Steinberg, L. Parenting style as context: An integrative model. Psychol Bull. 1993, 113, 487. [Google Scholar] [CrossRef]
- Kiefner-Burmeister, A.; Hoffmann, D.; Zbur, S.; Musher-Eizenman, D. Implementation of parental feeding practices: Does parenting style matter? Public Health Nutr. 2016, 19, 2410–2414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loth, K.A. Associations Between Food Restriction and Pressure-to-Eat Parenting Practices and Dietary Intake in Children: A Selective Review of the Recent Literature. Curr. Nutr. Rep. 2016, 5, 61–67. [Google Scholar] [CrossRef]
- Faith, M.S.; Scanlon, K.S.; Birch, L.L.; Francis, L.A.; Sherry, B. Parent-Child Feeding Strategies and Their Relationships to Child Eating and Weight Status. Obes. Res. 2004, 12, 1711–1722. [Google Scholar] [CrossRef]
- Kiefner-Burmeister, A.E.; Hoffmann, D.A.; Meers, M.R.; Koball, A.M.; Musher-Eizenman, D.R. Food consumption by young children: A function of parental feeding goals and practices. Appetite 2014, 74, 6–11. [Google Scholar] [CrossRef]
- Peters, J.; Dollman, J.; Petkov, J.; Parletta, N. Associations between parenting styles and nutrition knowledge and 2–5-year-old children’s fruit, vegetable and non-core food consumption. Public Health Nutr. 2013, 16, 1979–1987. [Google Scholar] [CrossRef] [Green Version]
- Gevers, D.W.; van Assema, P.; Sleddens, E.F.; de Vries, N.K.; Kremers, S.P. Associations between general parenting, restrictive snacking rules, and adolescent’s snack intake. The roles of fathers and mothers and interparental congruence. Appetite 2015, 87, 184–191. [Google Scholar] [CrossRef]
- Villa, J.K.D.; Santos, T.S.S.; Ribeiro, A.Q.; e Silva, A.R.; Sant’Ana, L.F.D.R.; Pessoa, M.C. Dietary patterns of children and socioeconomical, behavioral and maternal determinants. Rev. Paul. Pediatr. 2015, 33, 302–309. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Dalton, W.T.; Schetzina, K.E.; Fulton-Robinson, H.; Holt, N.; Ho, A.L.; Tudiver, F.; Wu, T. Home food environment, dietary intake, and weight among overweight and obese children in Southern Appalachia. South Med. J. 2013, 106, 550–557. [Google Scholar] [CrossRef]
- Van Der Horst, K.; Kremers, S.; Ferreira, I.; Singh, A.; Oenema, A.; Brug, J. Perceived parenting style and practices and the consumption of sugar-sweetened beverages by adolescents. Health Educ. Res. 2006, 22, 295–304. [Google Scholar] [CrossRef]
- Sleddens, E.F.; Kremers, S.P.; de Vries, N.K.; Thijs, C. Relationship between parental feeding styles and eating behaviors of Dutch children aged 6–7. Appetite 2010, 54, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Arredondo, E.M.; Elder, J.P.; Ayala, G.X.; Campbell, N.; Baquero, B.; Duerksen, S. Is parenting style related to children’s healthy eating and physical activity in Latino families? Health Educ. Res. 2006, 21, 862–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vereecken, C.; Rovner, A.; Maes, L. Associations of parenting styles, parental feeding practices and child characteristics with young children’s fruit and vegetable consumption. Appetite 2010, 55, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.A.; Ogden, J.; Vögele, C.; Gibson, E.L. The role of parental control practices in explaining children’s diet and BMI. Appetite 2008, 50, 252–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salmon, J.; Timperio, A.; Telford, A.; Carver, A.; Crawford, D. Association of family environment with children’s television viewing and with low level of physical activity. Obes Res. 2005, 13, 1939–1951. [Google Scholar] [CrossRef] [PubMed]
- Spurrier, N.J.; Magarey, A.A.; Golley, R.; Curnow, F.; Sawyer, M.G. Relationships between the home environment and physical activity and dietary patterns of preschool children: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 31. [Google Scholar] [CrossRef] [Green Version]
- He, M.; Piché, L.; Beynon, C.; Harris, S. Screen-related sedentary behaviors: Children’s and parents’ attitudes, motivations, and practices. J. Nutr. Educ. Behav. 2010, 42, 17–25. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, I.; van der Horst, K.; Wendel-Vos, W.; Kremers, S.; Van Lenthe, F.J.; Brug, J. Environmental correlates of physical activity in youth? A review and update. Obes. Rev. 2007, 8, 129–154. [Google Scholar] [CrossRef]
- Gubbels, J.S.; Kremers, S.P.J.; Stafleu, A.; de Vries, S.I.; Goldbohm, R.A.; Dagnelie, P.C.; de Vries, N.K.; van Buuren, S.; Thijs, C. Association between parenting practices and children’s dietary intake, activity behavior and development of body mass index: The KOALA Birth Cohort Study. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 18. [Google Scholar] [CrossRef] [Green Version]
- Gubbels, J.S.; Kremers, S.P.; Stafleu, A.; Dagnelie, P.C.; Goldbohm, R.A.; de Vries, N.K.; Thijs, C. Diet-related restrictive parenting practices. Impact on dietary intake of 2-year-old children and interactions with child characteristics. Appetite 2009, 52, 423–429. [Google Scholar] [CrossRef]
- Min, J.; Wang, V.H.; Xue, H.; Mi, J.; Wang, Y. Maternal perception of child overweight status and its association with weight-related parenting practices, their children’s health behaviours and weight change in China. Public Health Nutr. 2017, 20, 2096–2103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, H.; Cuskelly, M.; Gilmore, L.; Sullivan, K. Authoritative Parenting of Chinese Mothers of Children with and without Intellectual Disability. J. Child Fam. Stud. 2016, 26, 1173–1183. [Google Scholar] [CrossRef] [Green Version]
- WHO. Better Health, Better Lives: Children and Young People with Intellectual Disabilities and Their Families; The Case for Change; WHO: Geneva, Switzerland, 2010.
- Buehler, J.; Rothman, K.; Greenland, S. Modern Epidemiology; Lippencott-Raven: Philadelphia, PA, USA, 1998. [Google Scholar]
- Rowlands, A.V.; Eston, R.G.; Louie, L.; Ingledew, D.K.; Tong, K.K.; Fu, F.H. Physical Activity Levels of Hong Kong Chinese Children: Relationship with Body Fat. Pediatr. Exerc. Sci. 2002, 14, 286–296. [Google Scholar] [CrossRef]
- Pan, W.-H.; Yeh, W.-T. How to define obesity? Evidence-based multiple action points for public awareness, screening, and treatment: An extension of Asian-Pacific recommendations. Asia Pac. J. Clin. Nutr. 2008, 17, 370. [Google Scholar] [PubMed]
- Wen, X.; Hui, S.S.-C. Parenting Style as a Moderator of the Association Between Parenting Behaviors and the Weight Status of Adolescents. J. Early Adolesc. 2010, 32, 252–268. [Google Scholar] [CrossRef]
- WHO. Global Physical Activity Surveillance. 2014. Available online: https://www.who.int/teams/noncommunicable-diseases/surveillance/systems-tools/physical-activity-surveillance (accessed on 24 May 2022).
- WHO. WHO Guidelines on Physical Activity and Sedentary Behavior. 2020. Available online: https://www.who.int/publications/i/item/9789240015128 (accessed on 20 January 2022).
- A Qualitative Study on Dietary and Exercise Practice People in Hong Kong. 2005. Available online: http://www.ssrc.hku.hk/files/reports/health/grp-pmpdb-focus_group_e.pdf (accessed on 24 May 2022).
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [Green Version]
- Frazier, P.A.; Tix, A.P.; Barron, K.E. Testing moderator and mediator effects in counseling psychology research. J. Couns Psychol. 2004, 51, 115. [Google Scholar] [CrossRef]
- Scheffer, J. Dealing with missing data. Res. Lett. Inf. Math. Sci. 2002, 3, 153–160. [Google Scholar]
- Loth, K.A.; MacLehose, R.F.; Fulkerson, J.A.; Crow, S.; Neumark-Sztainer, D. Food-related parenting practices and ado-lescent weight status: A population-based study. Pediatrics 2013, 131, e1443–e1450. [Google Scholar] [CrossRef] [Green Version]
- Tschann, J.M.; Gregorich, S.E.; Penilla, C.; Pasch, L.A.; De Groat, C.L.; Flores, E.; Deardorff, J.; Greenspan, L.C.; Butte, N.F. Parental feeding practices in Mexican American families: Initial test of an expanded measure. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 6. [Google Scholar] [CrossRef] [Green Version]
- Jansen, P.W.; Roza, S.J.; Jaddoe, V.W.; Mackenbach, J.; Raat, H.; Hofman, A.; Verhulst, F.C.; Tiemeier, H. Children’s eating behavior, feeding practices of parents and weight problems in early childhood: Results from the population-based Generation R Study. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 130. [Google Scholar] [CrossRef] [PubMed]
- May, A.L.; Donohue, M.; Scanlon, K.S.; Sherry, B.; Dalenius, K.; Faulkner, P.; Birch, L.L. Child-feeding strategies are associated with maternal concern about children becoming overweight, but not children’s weight status. J. Am. Diet. Assoc. 2007, 107, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Savage, J.S.; Fisher, J.O.; Birch, L.L. Parental Influence on Eating Behavior: Conception to Adolescence. J. Law Med. Ethic- 2007, 35, 22–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherry, B.; McDivitt, J.; Birch, L.L.; Cook, F.H.; Sanders, S.; Prish, J.L.; Francis, L.A.; Scanlon, K.S. Attitudes, practices, and concerns about child feeding and child weight status among socioeconomically diverse white, Hispanic, and African-American mothers. J. Am. Diet. Assoc. 2004, 104, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Fang, K.; Mu, M.; Liu, K.; He, Y. Screen time and childhood overweight/obesity: A systematic review and meta-analysis. Child: Care Health Dev. 2019, 45, 744–753. [Google Scholar] [CrossRef]
- Liberali, R.; Kupek, E.; De Assis, M.A.A. Dietary Patterns and Childhood Obesity Risk: A Systematic Review. Child. Obes. 2020, 16, 70–85. [Google Scholar] [CrossRef]
- Olvera-Ezzell, N.; Power, T.G.; Cousins, J.H. Cousins, Maternal socialization of children’s eating habits: Strategies used by obese Mexican-American mothers. Child. Dev. 1990, 61, 395–400. [Google Scholar] [CrossRef]
- Moens, E.; Braet, C.; Soetens, B. Observation of family functioning at mealtime: A comparison between families of children with and without overweight. J. Pediatr. Psychol. 2007, 32, 52–63. [Google Scholar] [CrossRef] [Green Version]
- Vereecken, C.A.; Keukelier, E.; Maes, L. Influence of mother’s educational level on food parenting practices and food habits of young children. Appetite 2004, 43, 93–103. [Google Scholar] [CrossRef]
- Fisher, J.O.; Mitchell, D.C.; Smiciklas-Wright, H.; Birch, L.L. Parental influences on young girls’ fruit and vegetable, mi-cronutrient, and fat intakes. J. Am. Diet. Assoc. 2002, 102, 58–64. [Google Scholar] [CrossRef]
- Lee, H.; Keller, K.L. Children Who Are Pressured to Eat at Home Consume Fewer High-Fat Foods in Laboratory Test Meals. J. Acad. Nutr. Diet. 2012, 112, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Stang, J.; Rehorst, J.; Golicic, M. Parental feeding practices and risk of childhood overweight in girls: Implications for dietetics practice. J. Am. Diet. Assoc. 2004, 104, 1076–1079. [Google Scholar] [CrossRef] [PubMed]
- Loth, K.; Fulkerson, J.A.; Neumark-Sztainer, D. Food-related parenting practices and child and adolescent weight and weight-related behaviors. Clin. Pract. 2014, 11, 207–220. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n | % | |
|---|---|---|
| Children’s characteristics | ||
| Gender | ||
| Male | 307 | 69.8 |
| Female | 133 | 30.2 |
| Age group | ||
| 6–12 years | 241 | 54.8 |
| 13–21 years | 199 | 45.2 |
| ID level | ||
| Mild (IQ: 55–69) | 309 | 72.4 |
| Moderate (IQ: 35–54) | 118 | 27.6 |
| Autism | ||
| No | 170 | 38.9 |
| Yes | 267 | 61.1 |
| ADHD | ||
| No | 289 | 66.1 |
| Yes | 148 | 33.9 |
| Down Syndrome | ||
| No | 403 | 92.2 |
| Yes | 34 | 7.8 |
| Epilepsy | ||
| No | 401 | 91.8 |
| Yes | 36 | 8.2 |
| Body weight status a | ||
| Non-overweight/obese | 301 | 68.4 |
| Overweight/obese | 139 | 31.6 |
| Respondents’ characteristics | ||
| Relationship with the children | ||
| Mothers | 348 | 79.1 |
| Fathers | 92 | 20.9 |
| Age groups of the respondents | ||
| <40 years | 94 | 21.8 |
| 40–49 years | 237 | 54.9 |
| ≥50 years | 101 | 23.4 |
| Parental characteristics | ||
| Paternal education | ||
| Junior secondary and below | 128 | 29.7 |
| Senior secondary | 161 | 37.4 |
| College or above | 142 | 32.9 |
| Maternal education | ||
| Junior secondary and below | 125 | 29.0 |
| Senior secondary | 188 | 43.6 |
| College or above | 118 | 27.4 |
| Paternal occupation | ||
| Administrators and Professionals | 181 | 42.8 |
| Others | 242 | 57.2 |
| Maternal occupation | ||
| Housewives | 214 | 49.9 |
| Administrators and Professionals | 91 | 21.2 |
| Others | 124 | 28.9 |
| Parental marital status | ||
| Married/cohabiting | 376 | 86.2 |
| Divorced/separated/widowed | 60 | 13.8 |
| Paternal obesity b | ||
| No | 186 | 42.3 |
| Yes | 200 | 45.5 |
| Missing | 54 | 12.3 |
| Maternal obesity b | ||
| No | 297 | 67.5 |
| Yes | 119 | 27.0 |
| All (n = 440) | Child Body Weight Status | p-Value | ||
|---|---|---|---|---|
| Non-Overweight/Obese (n = 301) | Overweight/Obese (n = 139) | |||
| mean ± SD | mean ± SD | mean ± SD | p-value a | |
| Subscale of parenting practices (averaged score range: 1–5) | ||||
| Diet and PA monitoring (MO) | 3.73 ± 0.65 | 3.73 ± 0.63 | 3.73 ± 0.70 | 0.987 |
| Restricting access to unhealthy food and sedentary behaviors (RA) | 3.68 ± 0.80 | 3.70 ± 0.80 | 3.64 ± 0.81 | 0.474 |
| Pressure to eat more (PE) | 3.05 ± 0.65 | 3.18 ± 0.63 | 2.75 ± 0.61 | <0.001 *** |
| Reinforcement (RF) | 4.25 ± 0.58 | 4.24 ± 0.59 | 4.27 ±0.57 | 0.669 |
| Use food or sedentary behaviors as rewards (UR) | 3.13 ± 0.81 | 3.10 ± 0.85 | 3.18 ± 0.74 | 0.368 |
| n (%) | n (%) | n (%) | p-value b | |
| Unhealthy behaviors | ||||
| Insufficient MVPA (<60 min/day) | 406 (93.8) | 280 (94.3) | 126 (92.6) | 0.525 |
| More sedentary behaviors (≥4 h/day) | 196 (47.7) | 126 (44.5) | 70 (54.7) | 0.070 † |
| Lower fruit consumption (<2 servings/day) | 331 (75.7) | 237 (79.3) | 94 (68.1) | 0.016 * |
| Lower vegetable consumption (<3 servings/day) | 378 (86.5) | 261 (87.3) | 117 (84.8) | 0.547 |
| Higher fried food consumption (≥once/day) | 86 (19.7) | 48 (16.1) | 38 (27.5) | 0.007 ** |
| Higher sweetened drink consumption (≥once/day) | 200 (45.7) | 128 (42.7) | 72 (52.2) | 0.079 † |
| Higher snack consumption (≥twice/day) | 104 (23.9) | 66 (22.1) | 38 (27.5) | 0.229 |
| Breakfast skipping (≤6 times/week) | 89 (20.4) | 62 (20.8) | 27 (19.6) | 0.800 |
| Insufficient MVPA (<60 min/day) | More Sedentary Behaviors (≥4 h/day) | Lower Fruit Consumption (<2 Servings/day) | Lower Vegetable Consumption (<3 Servings/day) | Higher Fried Food Consumption (≥Once/day) | Higher Sweetened Drink Consumption (≥Once/day) | Higher Snack Consumption (≥Twice/day) | Breakfast Skipping (≤6 Times/week) | |
|---|---|---|---|---|---|---|---|---|
| Children’s characteristics | ||||||||
| Gender | ||||||||
| Male | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Female | 0.99 (0.42, 2.33) | 1.44 (0.94, 2.21) † | 1.28 (0.78, 2.08) | 1.19 (0.64, 2.20) | 0.76 (0.46, 1.30) | 0.83 (0.55, 1.25) | 0.54 (0.32, 0.91) * | 1.70 (1.04, 2.76) * |
| Age group | ||||||||
| 6–12 years | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| 13–21 years | 0.64 (0.29, 1.41) | 1.16 (0.79, 1.72) | 0.55 (0.35, 0.85) ** | 0.61 (0.35, 1.06) † | 1.13 (0.71, 1.82) | 1.00 (0.69, 1.46) | 0.51 (0.32, 0.81) ** | 1.33 (0.83, 2.12) |
| Body weight status a | ||||||||
| Non-overweight | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Overweight/obese | 0.77 (0.34, 1.72) | 1.50 (0.99, 2.29) † | 0.56 (0.36, 0.88) * | 0.81 (0.46, 1.44) | 1.98 (1.22, 3.21) ** | 1.47 (0.98, 2.20) † | 1.34 (0.84, 2.12) | 0.93 (0.56, 1.53) |
| ID level | ||||||||
| Mild (IQ: 55–69) | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Moderate (IQ: 35–54) | 3.16 (0.93, 10.73) † | 0.91 (0.59, 1.42) | 0.67 (0.41, 1.08) † | 0.61 (0.34, 1.09) † | 1.16 (0.68, 1.95) | 1.07 (0.70, 1.65) | 1.81 (1.12, 2.93) * | 0.96 (0.56, 1.63) |
| Autism | ||||||||
| No | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 0.44 (0.18, 1.12) † | 0.73 (0.49, 1.08) | 0.74 (0.47, 1.18) | 0.86 (0.49, 1.53) | 1.38 (0.84, 2.28) | 1.69 (1.14, 2.50) ** | 2.10 (1.29, 3.43) ** | 0.78 (0.49, 1.26) |
| ADHD | ||||||||
| No | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 1.24 (0.53, 2.90) | 0.85 (0.56, 1.28) | 0.61 (0.39, 0.95) * | 0.78 (0.44, 1.37) | 1.37 (0.84, 2.23) | 1.13 (0.76, 1.68) | 1.64 (1.04, 2.59) * | 0.88 (0.53, 1.45) |
| Down Syndrome | ||||||||
| No | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 2.32 (0.31, 17.64) | 1.62 (0.79, 3.29) | 1.93 (0.73, 5.11) | 0.90 (0.34, 2.43) | 0.11 (0.02, 0.83) * | 0.18 (0.07, 0.48) ** | -- | 0.83 (0.33, 2.07) |
| Epilepsy | ||||||||
| No | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | -- | 0.69 (0.33, 1.42) | 0.61 (0.29, 1.26) | 0.43 (0.19, 0.97) * | 1.62 (0.75, 3.51) | 0.83 (0.41, 1.65) | 0.62 (0.25, 1.53) | 0.77 (0.31, 1.91) |
| Parental characteristics | ||||||||
| Respondents’ relationship with the children | ||||||||
| Mothers | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Fathers | 0.90 (0.35, 2.30) | 0.94 (0.58, 1.52) | 1.62 (0.90,2.93) | 1.52 (0.72, 3.21) | 1.40 (0.81, 2.43) | 1.00 (0.63, 1.59) | 1.00 (0.59, 1.72) | 1.54 (0.90, 2.64) |
| Age group of the respondents | ||||||||
| <40 years | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| 40–49 years | 0.65 (0.21, 2.02) | 0.73 (0.44, 1.20) | 0.92 (0.51, 1.65) | 0.85 (0.40, 1.82) | 1.20 (0.64, 2.25) | 1.16 (0.72, 1.88) | 0.57 (0.34, 0.97) * | 1.30 (0.71, 2.39) |
| ≥50 years | 0.49 (0.14, 1.70) | 0.97 (0.54, 1.75) | 0.54 (0.28, 1.05) † | 0.57 (0.25, 1.31) | 1.28 (0.62, 2.63) | 0.67 (0.38, 1.19) | 0.33 (0.17, 0.67) ** | 0.98 (0.47, 2.04) |
| Paternal education | ||||||||
| Junior secondary and below | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Senior secondary | 1.48 (0.58, 3.75) | 0.74 (0.46, 1.21) | 1.01 (0.59, 1.74) | 0.74 (0.35, 1.57) | 1.01 (0.57, 1.79) | 1.03 (0.64, 1.64) | 1.38 (0.78, 2.42) | 0.54 (0.31, 0.93) * |
| College or above | 1.48 (0.57, 3.88) | 1.06 (0.65, 1.74) | 1.04 (0.59, 1.81) | 0.45 (0.22, 0.93) * | 0.77 (0.41, 1.42) | 0.72 (0.44, 1.16) | 1.36 (0.76, 2.42) | 0.31 (0.16, 0.58) *** |
| Maternal education | ||||||||
| Junior secondary and below | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Senior secondary | 0.70 (0.26, 1.90) | 1.06 (0.66, 1.71) | 0.92 (0.53, 1.59) | 0.67 (0.32, 1.43) | 1.04 (0.59, 1.82) | 1.15 (0.73, 1.80) | 1.42 (0.80, 2.51) | 0.46 (0.27, 0.79) ** |
| College or above | 0.72 (0.24, 2.15) | 0.91 (0.54, 1.53) | 0.70 (0.39, 1.25) | 0.43 (0.20, 0.93) * | 0.74 (0.38, 1.43) | 0.64 (0.38, 1.08) † | 1.82 (0.99, 3.35) † | 0.28 (0.12, 0.48) *** |
| Paternal occupation | ||||||||
| Administrators and Professionals | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Others | 0.77 (0.34, 1.72) | 0.82 (0.55, 1.22) | 0.75 (0.48, 1.18) | 1.27 (0.72, 2.23) | 1.32 (0.80, 2.17) | 1.48 (1.00, 2.19) * | 0.71 (0.45, 1.11) | 2.01 (1.20, 3.37) ** |
| Maternal occupation | ||||||||
| Housewives | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Administrators and Professionals | 0.41 (0.16, 1.02) † | 0.69 (0.42, 1.15) | 0.79 (0.46, 1.38) | 0.71 (0.37, 1.39) | 1.00 (0.53, 1.91) | 1.03 (0.63, 1.69) | 1.29 (0.73, 2.27) | 0.49 (0.24, 1.00) † |
| Others | 0.84 (0.31, 2.28) | 0.64 (0.40, 1.01) † | 1.14 (0.67, 1.93) | 1.20 (0.60, 2.37) | 1.59 (0.92, 2.72) † | 1.30 (0.83, 2.02) | 1.16 (0.68, 1.96) | 1.06 (0.62, 1.80) |
| Parental marital status | ||||||||
| Married/cohabiting | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Divorced/separated/widowed | 0.93 (0.31, 2.78) | 1.19 (0.67, 2.12) | 1.69 (0.82, 3.45) | 3.36 (1.02, 11.09) * | 1.48 (0.78, 2.80) | 0.83 (0.48, 1.44) | 0.88 (0.45, 1.69) | 1.39 (0.74, 2.64) |
| Paternal obesity b | ||||||||
| No | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 0.78 (0.35, 1.74) | 0.96 (0.63, 1.44) | 1.18 (0.74, 1.88) | 0.74 (0.41, 1.33) | 0.71 (0.43, 1.19) | 0.77 (0.52, 1.15) | 0.80 (0.50, 1.27) | 0.77 (0.46, 1.28) |
| Missing | 3.18 (0.40, 25.22) | 1.08 (0.56, 2.10) | 1.21 (0.59, 2.48) | 1.06 (0.41, 2.78) | 1.20 (0.59, 2.46) | 0.76 (0.41, 1.40) | 0.46 (0.20, 1.05) † | 1.61 (0.81, 3.19) |
| Maternal obesity b | ||||||||
| No | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 0.60 (0.26, 1.36) | 1.11 (0.71, 1.72) | 0.89 (0.55, 1.47) | 0.78 (0.43, 1.44) | 2.32 (1.40, 3.85) ** | 1.28 (0.83, 1.97) | 1.19 (0.73, 1.93) | 1.41 (0.84, 2.37) |
| More Sedentary Behaviors (≥4 h/day) | Lower Fruit Consumption (<2 Servings/day) | Lower Vegetable Consumption (<3 Servings/day) | Higher Fried Food Consumption (≥Once/day) | Higher Sweetened Drink Consumption (≥Once/day) | Higher Snack Consumption (≥Twice/day) | Breakfast Skipping (≤6 Times/week) | |
|---|---|---|---|---|---|---|---|
| Main effects | |||||||
| Body weight status of the children | |||||||
| Non-overweight/obese | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Overweight/obese | 1.51 (1.02, 2.24) * | 0.65 (0.43, 0.99) * | 0.81 (0.46, 1.42) | 1.96 (1.24, 3.12) ** | 1.73 (1.16, 2.57) ** | 1.56 (1.01, 2.41) * | 0.86 (0.52, 1.42) |
| Parenting practices | |||||||
| MO | 0.80 (0.50, 1.28) | 0.62 (0.37, 1.05) | 0.58 (0.27, 1.24) | 0.59 (0.33, 1.5) | 0.64 (0.39, 1.04) | 0.73 (0.43, 1.24) | 0.58 (0.33, 1.03) |
| RA | 1.38 (0.93, 2.04) | 1.16 (0.76, 1.78) | 0.71 (0.38, 1.33) | 0.63 (0.40, 1.00) * | 0.64 (0.43, 0.96) * | 0.90 (0.59, 1.38) | 0.69 (0.43, 1.01) |
| PE | 1.01 (0.75, 1.37) | 1.04 (0.74, 1.45) | 1.19 (0.75, 1.88) | 1.05 (0.71, 1.56) | 1.03 (0.75, 1.40) | 1.16 (0.82, 1.64) | 1.14 (0.77, 1.70) |
| RF | 0.86 (0.63, 1.17) | 0.99 (0.70, 1.41) | 0.96 (0.58,1.57) | 0.83 (0.56, 1.22) | 0.88 (0.63, 1.22) | 0.96 (0.68, 1.37) | 0.96 (0.66, 1.39) |
| UR | 0.95 (0.76, 1.20) | 0.90 (0.70, 1.17) | 0.86 (0.61, 1.21) | 1.43 (1.04, 1.95) * | 1.51 (1.18, 1.94) ** | 1.60 (1.21, 2.11) ** | 1.28 (0.93, 1.75) * |
| Interactions | |||||||
| Body weight status * RA | -- | -- | -- | 0.33 (0.12, 0.96) * | 0.32 (0.12, 0.88) * | -- | 0.19 (0.06, 0.63) * |
| Body weight status * UR | -- | -- | 2.34 (1.10, 5.00) * | 2.33 (1.07, 4.20) * | -- | -- | -- |
| Non-Overweight/Obese Children | Overweight/Obese Children | |||
|---|---|---|---|---|
| AOR (95% CI) | p Value | AOR (95% CI) | p Value | |
| Lower vegetable consumption (<3 servings/day) | ||||
| UR | 0.68 (0.44, 0.98) | 0.040 * | 1.58 (0.83, 3.02) | 0.170 |
| Higher fried food consumption (≥ once/day) | ||||
| RA | 0.89 (0.51, 1.57) | 0.700 | 0.28 (0.11, 0.71) | 0.007 ** |
| UR | 1.15 (0.79, 1.68) | 0.460 | 2.50 (1.36, 4.60) | 0.003 ** |
| Higher sweetened drink consumption (≥ once/day) | ||||
| RA | 0.83 (0.52, 1.31) | 0.410 | 0.24 (0.09, 0.64) | 0.004 ** |
| Breakfast skipping (≤6 times/week) | ||||
| RA | 1.01 (0.59, 1.75) | 0.960 | 0.17 (0.06, 0.55) | 0.003 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, Y.; Supriya, R.; Gao, Y.; Yu, S.; Wang, A.; Ou, X.; Tao, D.; Baker, J.S. The Relationships between Parenting Practices and Child Health-Related Behaviors in Children with Intellectual Disability: The Moderating Role of Child Body Weight Status. Nutrients 2022, 14, 5206. https://doi.org/10.3390/nu14245206
Sun Y, Supriya R, Gao Y, Yu S, Wang A, Ou X, Tao D, Baker JS. The Relationships between Parenting Practices and Child Health-Related Behaviors in Children with Intellectual Disability: The Moderating Role of Child Body Weight Status. Nutrients. 2022; 14(24):5206. https://doi.org/10.3390/nu14245206
Chicago/Turabian StyleSun, Yan, Rashmi Supriya, Yang Gao, Siyue Yu, Aiwei Wang, Xiaoting Ou, Dan Tao, and Julien S. Baker. 2022. "The Relationships between Parenting Practices and Child Health-Related Behaviors in Children with Intellectual Disability: The Moderating Role of Child Body Weight Status" Nutrients 14, no. 24: 5206. https://doi.org/10.3390/nu14245206